Back to Journals » Clinical Ophthalmology » Volume 15
Ultrasound Biomicroscopy for Zonular Evaluation in Eyes with Ocular Trauma
Authors Bhatt V, Bhatt D, Barot R, Sheth J ![]()
Received 10 June 2021
Accepted for publication 27 July 2021
Published 7 August 2021 Volume 2021:15 Pages 3285—3291
DOI https://doi.org/10.2147/OPTH.S323349
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Vaidehi Bhatt,1 Deepak Bhatt,2 Rakesh Barot,1 Jay Sheth3
1Department of Ophthalmology, Rajiv Gandhi Medical College and Chhatrapati Shivaji Memorial Hospital, Thane, Maharashtra, India; 2Department of Imaging, UBM Institute, Mumbai, Maharashtra, India; 3Department of Vitreoretinal, Surya Eye Institute and Research Center, Mumbai, Maharashtra, India
Correspondence: Jay Sheth
Department of Vitreoretinal, Surya Eye Institute and Research Center, Mumbai, Maharashtra, India
Tel +91 9961167200
Email [email protected]
Purpose: To evaluate the role of ultrasound biomicroscopy (UBM) in detecting zonular abnormalities in eyes with ocular trauma.
Patients and Methods: Prospective study of 143 eyes of 143 patients with ocular trauma and having opaque media was evaluated using a UBM. The presence or absence of zonular damage (zonular tears and/or zonular stretching) was examined and the clock-hour involvement was noted.
Results: One-hundred and one eyes had blunt trauma (70.63%; group 1), while 42 eyes had penetrating trauma (29.37%; group 2) The mean age of the patient population was 48.01± 17.93 years with a male:female ratio of 2.11:1. Group 1 had significantly greater visual acuity than group 2 (p = 0.03). Zonular damage was present in 79 (55.2%) eyes, including zonular tears (48 eyes; 33.6%) and zonular stretching (31 eyes; 21.7%). Zonular damage was seen significantly more in eyes with blunt trauma (64.28%) as compared to penetrating trauma (25.74%) (p = 0.015). On quantitative analysis, zonular damage between 3 and 6 clock hours was most frequent, both in eyes having zonular tears (70.83%) and zonular stretching (96.77%). Additionally, 3– 6 clock hours of zonular stretching was seen significantly more in blunt trauma as compared to penetrating trauma (p = 0.015).
Conclusion: UBM is an effective imaging modality to diagnose zonular abnormalities in patients with ocular trauma having opaque media. The ability to detect the presence of zonular weakness and their quantification by performing a UBM is critical to formulate the optimal surgical approach and avoid any untoward surgical complications.
Keywords: ultrasound biomicroscopy, ocular trauma, zonular tears, zonular stretching
Introduction
Ocular trauma is a major public health concern because it frequently causes visual impairment or blindness in people who are younger and more productive.1–3 Trauma can damage all regions of the eye as well as the adnexa to varying degrees. A thorough clinical evaluation and related investigations are required for optimum therapy. However, it is not uncommon to come across clinical scenarios of hazy ocular media which makes visualization of intraocular tissues problematic. In such a scenario, performing ocular ultrasonography provides excellent real-time images of the eye with good contrast.4–6 Amongst them, the technology of Ultrasound Biomicroscopy which was first developed by Pavlin, Sherer, and Foster in the early part of the 1990s provides an excellent platform for subsurface visualization of the anterior segment.4,7
After blunt ocular trauma, the incidence of zonular injuries is believed to be roughly 14%.8 The resultant subluxation of the lens usually transpires once 25% of zonules are damaged.9 Although phacodonesis is a symptom of zonular weakening, subtle injury to the zonules can readily go undetected on clinical examination.10 Furthermore, the extent of zonular weakening is difficult to assess clinically in all cases, particularly when the media is opaque.10 Gimbel et al performed a UBM analysis of 14 eyes with ocular trauma. They noted the presence of zonular weakness in only 6 out of 14 cases pre-operatively, while in the remaining 8 cases, it was noted during the time of surgery.11 Ozdal et al used UBM to examine 109 eyes with ocular trauma and found zonular damage in 64.2% of closed-globe injuries and 54.8% of open-globe injuries.12
During surgery for traumatic cataracts, the presence of zonular damage raises the risk of vitreous loss and posterior dislocation of the lens into the vitreous cavity.10,13 Thus, UBM is critical for zonular status analysis before surgery in individuals with a history of ocular damage. With the help of a UBM, we can accurately identify not only the presence of any zonular defects but also quantify the same. The precise location of the zonular damage and the area of clock-hour involvement is imperative before proceeding with cataract surgery in eyes with ocular trauma. This can help to formulate the optimal surgical plan and avoid any untoward surgical complications. The purpose of this study was to evaluate the utility of UBM to detect zonular abnormalities in eyes with ocular trauma and opaque media. We also describe the various UBM features of these zonular irregularities.
Materials and Methods
It was a Non-Randomized Prospective Study of 143 eyes of 143 consecutive patients with Ocular Trauma who presented to the vitreoretinal services of a tertiary eye care center between August 2018 and April 2021. The inclusion criteria were: 1). Patient having Open globe/closed globe injury; 2). Presence of opaque ocular media precluding zonular analysis; 3). Underwent UBM evaluation. All patients with clear ocular media in presence of ocular trauma and those patients in whom UBM could not be performed due to poor cooperation or severe sickness were excluded from the study. The study was conducted in accordance with the tenets of the Declaration of Helsinki and was approved by the Institutional Review Board of the Rajiv Gandhi Medical College and Chhatrapati Shivaji Memorial Hospital, India. Written informed consent was obtained from each patient.
At baseline, all patients underwent detailed clinical evaluation, including assessment of best-corrected visual acuity (BCVA) on Snellen chart, intraocular pressure measurement (IOP) by Goldmann applanation tonometry, along with anterior segment and fundus evaluation by slit-lamp biomicroscopy and indirect ophthalmoscopy.
UBM Evaluation
The UBM evaluation was performed after a minimum of 10 days following a primary globe repair for open-globe injuries. In closed-globe injuries, the UBM was performed after a minimum of three days following the injury. The UBM evaluation was performed by a single specialist (DB). Before the procedure, written informed consent was taken from the patient, and details of the procedure were duly explained. It was done using the Sonomed VuMax UD UBM machine (Lake Success, NY, USA) with the patient in a supine position. Eyecup of appropriate size was used with a coupling fluid such as saline or 2.5% methylcellulose. First, the eye with trauma was examined followed by the other normal eye for anatomical comparison. A 50 MHz probe was utilized for performing the UBM evaluation.
Various modes were utilized during the UBM procedure. The “high-resolution mode” was used for detailed analysis and the “angle mode” was utilized for identifying zonular or angle pathologies. The “gain” was adjusted to obtain artifact-free images. Inbuilt tools such as calipers and A-scan mode were applied for further image analysis. A thorough zonular evaluation was performed and the presence of zonular tears and/or zonular stretching was noted. A zonular stretch was defined as an appearance of increased zonular length as compared to a normal UBM zonular structure. A zonular tear was defined as any discontinuity along the zonular structure extending from the ciliary body to the lens capsule. The quantum of zonular abnormality was documented based on the total number of clock hours involved. The interpretation of the UBM image was performed by a single imaging expert (DB) with over 30 years of experience in ocular imaging, and over 21 years of experience in performing UBM evaluation (Approximately 400–500 UBMs/year).
Details of history, clinical examination, and UBM analysis were recorded in a Microsoft Excel sheet. For analysis, the groups were divided into blunt trauma (Group 1) and penetrating trauma (Group 2), respectively. The Statistical analysis was performed by SPSS 23.0 version. Visual acuity was converted to LogMAR for statistical analysis. Continuous variables were described as mean and variation of each observation from the mean value (Standard deviation) represented as mean ± SD. Paired data in comparison with baseline were analyzed with Wilcoxon signed-rank test (for non-normal distribution). Categorical variables were described by taking percentages and were analyzed using the chi-square test. Variables with a p-value <0.05 were considered statistically significant.
Results
One hundred and forty-three eyes of 143 patients with ocular trauma underwent UBM analysis. Of these, 101 eyes had blunt trauma (70.63%) while 42 eyes had penetrating trauma (29.37%) (Table 1). The mean age of the patient population was 48.01 ± 17.93 years (Table 1). There was no significant difference in age between group 1 and group 2 (Table 1). More than two-thirds of the patients were male (67.8%) while around one-third were females (32.2%) respectively (Table 1). The mean visual acuity of group 1 was significantly better than group 2 (p = 0.03) (Table 1).
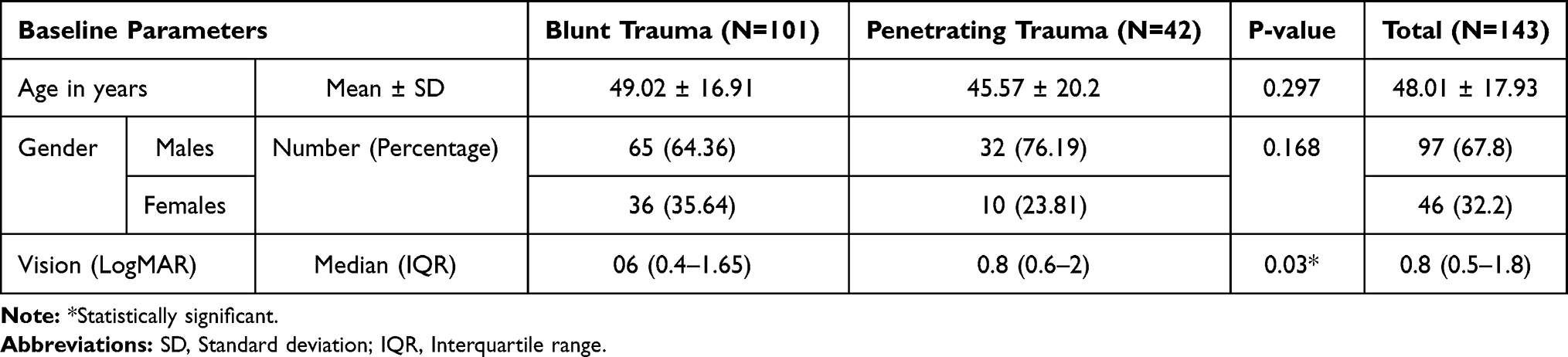 |
Table 1 Showing a Comparison of Baseline Parameters Between the Two Groups |
On UBM analysis, zonular damage was noted in 79 (55.2%) out of the 143 eyes. Forty-eight (33.6%) of these eyes had zonular tears while stretching of zonules was observed in 31 eyes (21.7%). On the detailed evaluation of eyes with a zonular tear, 70.83% had 3–6 clock hours of tear, 20.83% had > 6 clock hours of tear while 8.33% had a total zonular tear, respectively. Amongst eyes with zonular stretching, 96.77% had 3–6 clock hour involvement while 3.23% had < 3 clock hour involvement. None of the eyes had > 6 clock hours of zonular stretching. On subgroup analysis, a significantly greater number of eyes with blunt trauma had zonular damage (64 eyes; 64.28%) as compared to penetrating trauma (15 eyes; 36.63%) (p = 0.015). Also, zonular stretching between 3 and 6 clock hours was noted significantly more in blunt trauma (26 eyes; 25.74%) as compared to penetrating trauma (2 eyes; 4.76%) (p = 0.015). The details of zonular analysis on UBM are provided in Table 2. Figures 1Figures 2Figures 3Figures 4Figures–5 illustrate the various zonular and associated ocular abnormalities noted on UBM.
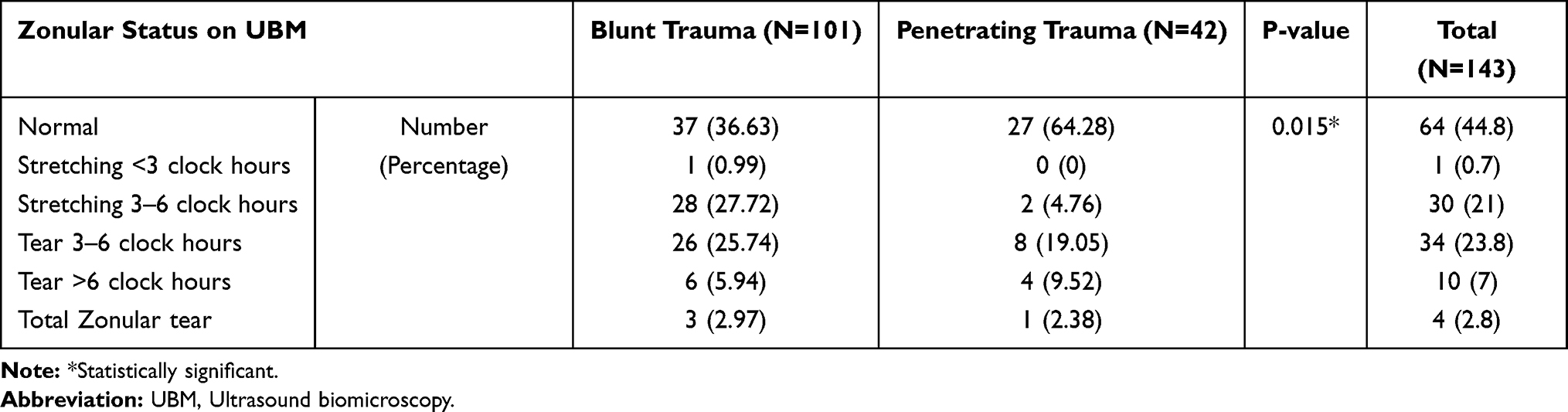 |
Table 2 Showing a Comparison of Zonular Status on Ultrasound Biomicroscopic Evaluation Between the Two Groups |
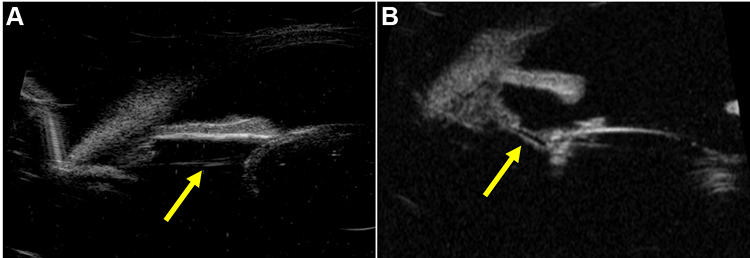 |
Figure 1 (A) An ultrasound biomicroscopic (UBM) image illustrating zonular stretching and thinning (Yellow arrow) with a normal crystalline lens in a 26-year-old patient with blunt trauma. (B) An ultrasound biomicroscopic (UBM) image illustrating zonular stretching (Yellow arrow) in a 55-year-old pseudophakic patient with blunt trauma. |
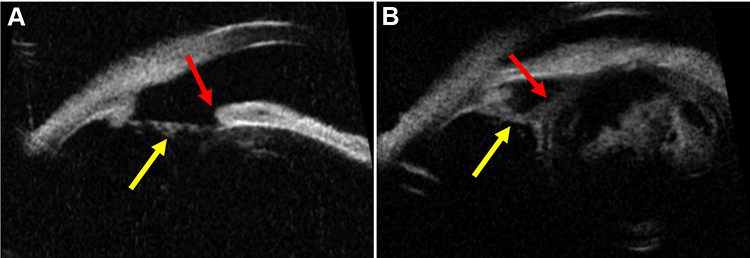 |
Figure 2 Ultrasound biomicroscopic (UBM) images illustrating zonular stretching ((A and B) Yellow arrow) in the presence of iridodialysis (A; Red arrow) in a 63-year-old patient with blunt trauma and anterior subluxation of the cataractous lens (B; Red arrow) in a 33-year-old patient with blunt trauma. |
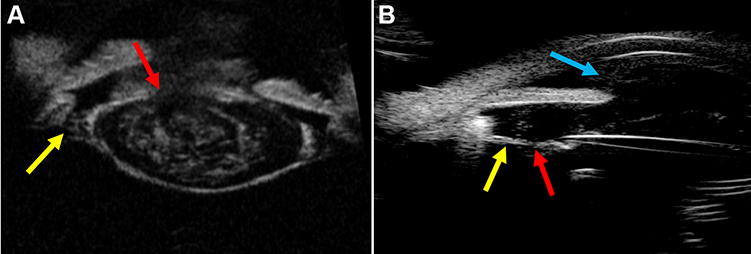 |
Figure 3 (A) An ultrasound biomicroscopic (UBM) image illustrating zonular stretching (Yellow arrow) with ruptured anterior capsule (Red arrow) in a 24-year-old patient with blunt trauma. (B) An ultrasound biomicroscopic (UBM) image illustrating zonular stretching (Yellow arrow) with zonular tear (Red arrow) along with vitreous in the anterior chamber (Blue arrow) in a 45-year-old patient with penetrating trauma. |
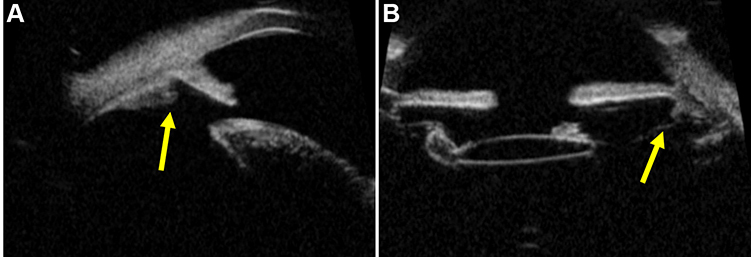 |
Figure 4 Ultrasound biomicroscopic (UBM) images demonstrating zonular tear ((A and B) Yellow arrow) in the presence of crystalline lens (A) in a 36-year-old patient with blunt trauma and posterior chamber intraocular lens (B) in a 22-year-old patient with blunt trauma respectively. |
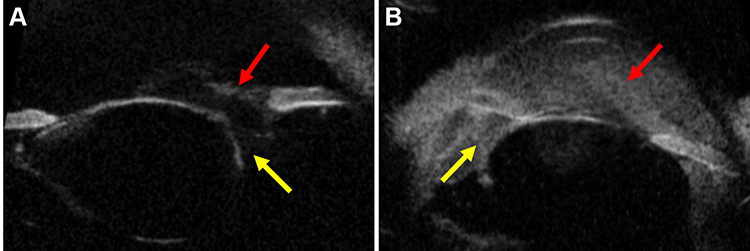 |
Figure 5 (A) An ultrasound biomicroscopic (UBM) image illustrating zonular tear (Yellow arrow) along with vitreous in the anterior chamber (Red arrow) in a 27-year-old patient with penetrating trauma. (B) An ultrasound biomicroscopic (UBM) image illustrating zonular tear (Yellow arrow) with dense hyphema in the anterior chamber (Red arrow) in a 36-year-old patient with blunt trauma. |
Discussion
In the present study, we performed a detailed evaluation of the zonules on UBM in 143 eyes with ocular trauma and opaque media. On clinical examination, the zonules were not visualized in any of the study eyes due to the media opacity. However, on UBM, 55.2% of the eyes illustrated some form of zonular damage. Of these, 60.76% had zonular tears while 39.24% had zonular stretching. Interestingly, eyes with blunt trauma had significantly more zonular damage as compared to penetrating trauma eyes.
There were 141 eyes evaluated and 101 (70.63%) had blunt trauma and 42 (29.37%) had penetrating trauma. This is slightly higher than the figure reported by Tripathy et al, who found blunt trauma in 61.7% of their patients presenting to casualty eye care, but only 15.43% of eyes had penetrating trauma.14 Males made up 67.8% of the population in our survey, while females made up 32.2%. This is consistent with the findings of Ozdal et al, who found that males are more frequently implicated in ocular trauma than females12 When compared to other research, such as Danenberg et al15 where males made up 97% of the study population, our study has a lower male population participation rate. The male to female ratio in this study was 2.11:1, which is lower than the 5.5:1 reported by Cillino et al.16
In our study, we had included both penetrating and blunt trauma cases. In their study of eyes presenting to the casualty department, Tripathy et al found that penetrating trauma has worse visual results than blunt trauma.13 Unlike their study, we did a direct comparison of baseline visual acuities between the groups and found that penetrating trauma eyes had a considerably worse visual outcome. This is comprehensible because penetrating injuries cause more tissue damage and, as a result, are more likely to cause visual problems.
The zonular fibers, also known as Zinn zonules, are important supporting structures that keep the lens in its natural position.17 Any weakness in these zonules can cause phacodonesis, which can be mild or severe depending on the degree of zonular injury.9,10 Lens subluxation or dislocation, iridodonesis, and an uneven anterior chamber are all symptoms of zonular weakening.18,19 Despite a meticulous clinical evaluation, subtle zonular damage can easily be missed even by an experienced clinician. Such situations are frequently encountered as intraoperative surprises, necessitating a change in surgical care. In the absence of any visualization of the zonules due to opaque media in cases of ocular trauma, the likelihood of such surprises increases enormously. This is where imaging, in the form of UBM, plays an unrivaled role. It provides excellent real-time images of the eye with good contrast.4–7 These are achievable at an affordable cost and in patients with opaque media. Zonular assessment can be performed efficiently and accurately on a UBM by an experienced imaging specialist. The presence of zonular remains on the lens capsule in the equatorial region, as well as the absence of zonular fibers and stretching of zonules, are all clear signs of zonular damage.20 On UBM, traits such as increased lens-ciliary body distance and increased crystalline lens sphericity are a few indirect indicators of traumatic zonular injury.20
Ozdal et al performed a landmark study to evaluate the indications for UBM in 109 eyes of ocular trauma.14 61.5% of the eyes in their study had a closed-globe injury, whereas 38.5% had an open-globe injury.14 In comparison to their study, we found a marginally higher rate of closed-globe injury/blunt trauma (70.63%) while eyes having penetrating trauma/open-globe injury were lower to some extent (29.37%). The most common indication for performing a UBM was zonular examination before cataract surgery, accounting for 56.7% of cases studied by Ozdal et al.12 This was followed by detection of foreign body (24.5%), assessment of ocular hypotony (13.2%), and anterior segment evaluation in presence of hyphema and corneal blood staining (6.6%).12 They noted a zonular deficiency in 64.2% of closed globe injury patients and 54.8% of open-globe injury patients. Although the incidence of zonular damage in blunt trauma was very similar in our study (64.28%), we noted fewer cases of penetrating trauma with zonular damage (36.63%) as compared to Ozdal et al.12 Furthermore, when comparing blunt versus penetrating trauma, the difference in zonular involvement was much higher in eyes with blunt trauma. Our zonular abnormality rate is also higher than that reported by McWhae et al,10 who found occult zonular defects in 21 of 42 (42.9%) eyes with anterior segment trauma.
A comprehensive UBM assessment illustrated a zonular involvement in the form of tears (48 eyes) and stretching (31 eyes) in our patient population. Pavlin et al used UBM to examine 18 eyes that had clinically suspicious zonular abnormalities.20 The most common cause of the zonular defect was trauma, which was followed by pseudoexfoliation, surgical procedures, congenital spherophakia, and Marfan syndrome.20 On UBM, they found zonular damage in the form of missing zonules as well as zonular stretch in an equal number of eyes (11 each).20 In contrast, we noted an almost 50% higher incidence of zonular tears (33.6% eyes) as compared to zonular stretching (21.7% eyes). This is also in contrast to Ozdal et al who did not report zonular stretching in their results, while all eyes had zonular deficiency ie, zonular tears.14 Furthermore, we also quantified the area of zonular damage in terms of clock hours involved, which was lacking in the studies by Pavlin et al20 and Ozdal et al.14 We found that zonular tears occurred between 3 and 6 clock hours in 23.8% of cases and zonular stretching occurred between 3 and 6 clock hours in 21% of cases, respectively. There was no significant difference in the number of zonular tears between the blunt and penetrating trauma groups on subgroup analysis. Penetrating trauma, on the other hand, had a considerably higher prevalence of zonular stretching between 3 and 6 clock hours than blunt trauma.
The lack of follow-up information for the patients is one of the study’s major limitations. However, the primary aim of our study was to assess how effective UBM is at detecting zonular abnormalities in ocular trauma eyes with opaque media. Nonetheless, we recommend long-term follow-up studies to evaluate the role of UBM in the assessment of zonular anomalies secondary to ocular trauma to acquire a better understanding of the visual and anatomical results. Also, while our study was based on a single grader UBM analysis, the grader is an experienced imaging specialist with over twenty-one years in this field and performing an average of 400–500 UBMs annually. Despite these limitations, the results reported here represent the largest prospective series on UBM analysis in eyes with ocular trauma with opaque media. Moreover, it is a singular real-world study to perform a detailed qualitative and quantitative assessment of zonular abnormalities on a UBM in trauma. Prior knowledge of the existing zonular weakness can aid the surgeon in developing a surgical strategy for such complicated cases. The surgeon can approach such challenging cases with greater confidence, lowering the likelihood of complications including vitreous loss, posterior displacement of the lens/posterior chamber intraocular lens (PCIOL) into the vitreous cavity, and progressive PCIOL decentration post-operatively.21,22
Conclusion
In conclusion, our study demonstrates that zonular abnormalities are commonly seen after ocular trauma, being more frequent in blunt trauma as compared to penetrating trauma. UBM analysis is very critical for the detection of subtle findings related to zonular involvement in such cases, especially since clinical evaluation is not feasible due to opaque media. Using an eyecup during the UBM evaluation will help to reduce globe pressure, especially in open-globe injuries following primary repair. We recommend incorporating UBM analysis as an integral part of the work-up of patients with ocular trauma especially with opaque media for optimal patient management and outcomes.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Aghadoost D. Ocular trauma: an overview. Arch Trauma Res. 2014;3(2):e21639. doi:10.5812/atr.21639
2. Thylefors B. Epidemiological patterns of ocular trauma. Aust N Z J Ophthalmol. 1992;20(2):95–98. doi:10.1111/j.1442-9071.1992.tb00718.x
3. Négrel AD, Thylefors B. The global impact of eye injuries. Ophthalmic Epidemiol. 1998;5(3):143–169. doi:10.1076/opep.5.3.143.8364
4. Pavlin CJ, Harasiewicz K, Sherar MD, Foster FS. Clinical use of ultrasound biomicroscopy. Ophthalmology. 1991;98(3):287–295. doi:10.1016/S0161-6420(91)32298-X
5. Pavlin CJ, Foster FS. Ultrasound biomicroscopy: high-frequency ultrasound imaging of the eye at microscopic resolution. Radiol Clin North Am. 1998;36(6):1047–1058. doi:10.1016/S0033-8389(05)70230-X
6. Ishikawa H, Schuman JS. Anterior segment imaging: ultrasound biomicroscopy. Ophthalmol Clin North Am. 2004;17(1):7–20. doi:10.1016/j.ohc.2003.12.001
7. Silverman RH. High-resolution ultrasound imaging of the eye - a review. Clin Exp Ophthalmol. 2009;37(1):54–67. doi:10.1111/j.1442-9071.2008.01892.x
8. Arques DM, Marques FF, Osher RH. Subtle signs of zonular damage. J Cataract Refract Surg. 2004;30(6):1295–1299. doi:10.1016/j.jcrs.2003.09.071
9. Mieler W. Overview of Ocular Trauma. Albert & Jakobiec’s Principles and Practice of Ophthalmology. Philadelphia: Saunders/Elsevier; 2008.
10. McWhae JA, Crichton AC, Rinke M. Ultrasound biomicroscopy for the assessment of zonules after ocular trauma. Ophthalmology. 2003;110(7):1340–1343. doi:10.1016/S0161-6420(03)00464-0
11. Gimbel HV, Sun R, Heston JP. Management of zonular dialysis in phacoemulsification and IOL implantation using the capsular tension ring. Ophthalmic Surg Lasers. 1997;28(4):273–281. doi:10.3928/1542-8877-19970401-03
12. Ozdal MP, Mansour M, Deschênes J. Ultrasound biomicroscopic evaluation of the traumatized eyes. Eye (Lond). 2003;17(4):467–472. doi:10.1038/sj.eye.6700382
13. Trikha S, Agrawal S, Saffari SE, Jayaswal R, Yang YF. Visual outcomes in patients with zonular dialysis following cataract surgery. Eye (Lond). 2016;30(10):1331–1335. doi:10.1038/eye.2016.108
14. Tripathy K, Chawla R, Venkatesh P, Vohra R, Sharma YR. Clinical profile of medicolegal cases presenting to the eye casualty in a tertiary care center in India. Indian J Ophthalmol. 2016;64(6):422–426. doi:10.4103/0301-4738.187656
15. Dannenberg AL, Parver LM, Brechner RJ, Khoo L. Penetrating eye injuries in the workplace: the National Eye Trauma System Registry. Arch Ophthalmol. 1992;110(6):843–848. doi:10.1001/archopht.1992.01080180115038
16. Cillino S, Casuccio A, Di Pace F, Pillitteri F, Cillino G. A five-year retrospective study of the epidemiological characteristics and visual outcomes of patients hospitalized for ocular trauma in a Mediterranean area. BMC Ophthalmol. 2008;8:1–9. doi:10.1186/1471-2415-8-6
17. Bassnett S. Zinn’s zonule. Prog Retin Eye Res. 2020;100902. Available from: https://www.sciencedirect.com/science/article/abs/pii/S1350946220300744.
18. Bartholomew RS. Phakodonesis. A sign of incipient lens displacement. Br J Ophthalmol. 1970;54(10):663–666. doi:10.1136/bjo.54.10.663
19. Liu XW, Wang Z, Yu WH, et al. Idiopathic phacodonesis in senile cataract patients in Qinghai, China. Int J Ophthalmol. 2011;4(5):508–512.
20. Pavlin CJ, Buys YM, Pathmanathan T. Imaging zonular abnormalities using ultrasound biomicroscopy. Arch Ophthalmol. 1998;116(7):854–857. doi:10.1001/archopht.116.7.854
21. Gimbel HV, Sun R. Role of capsular tension rings in preventing capsule contraction. J Cataract Refract Surg. 2000;26(6):791–792. doi:10.1016/S0886-3350(00)00505-8
22. Werner L, Zaugg B, Neuhann T, Burrow M, Tetz M. In-the-bag capsular tension ring and intraocular lens subluxation or dislocation: a series of 23 cases. Ophthalmology. 2012;119(2):266–271. doi:10.1016/j.ophtha.2011.08.016
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.