")
Back to Journals » International Medical Case Reports Journal » Volume 15
Type 2 Diabetes Mellitus in a 7 Year Old Girl
Authors Haris B, Stafrace S, Hussain K
Received 28 February 2022
Accepted for publication 20 April 2022
Published 12 May 2022 Volume 2022:15 Pages 245—250
DOI https://doi.org/10.2147/IMCRJ.S364424
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ronald Prineas
Basma Haris,1 Samuel Stafrace,2 Khalid Hussain1
1Department of Pediatric Endocrinology, Sidra Medicine, Doha, Qatar; 2Department of Diagnostic Imaging, Sidra Medicine, Doha, Qatar
Correspondence: Khalid Hussain, Department of Pediatric Medicine, Sidra Medicine, OPC, C6-340|PO Box 26999, Al Luqta Street, Doha, Qatar, Tel +974-4003-7608 ; +974-30322007, Email [email protected]
Abstract: Type 2 diabetes is a chronic disease due to insulin resistance resulting in hyperglycemia. The prevalence of type 2 diabetes is increasing worldwide in the pediatric population. In the pediatric population, type 2 diabetes typically develops around adolescence; however, patients with a younger age of onset are now being reported. Earlier onset of type 2 diabetes is associated with a more aggressive course of disease and earlier comorbidities, although data on this is limited. We report a child from Qatar with type 2 diabetes that was diagnosed at 7 years of age, along obesity with a BMI of 26.8 kg/m2. Elevated liver enzymes, c-peptide, and insulin levels were observed along with fatty liver on an ultrasound. The child had severe acanthosis nigricans with increased appetite. There was a positive family history for type 2 diabetes. Testing for type 1 diabetes autoantibodies, monogenic obesity, and monogenic diabetes screening was negative. This is the second youngest child reported to have type 2 diabetes. Accurate diagnosis, early reporting, and long-term follow-up of such cases is necessary to bring more attention to the subgroup of type 2 diabetes in very young patients.
Keywords: pediatric diabetes, type 2 diabetes, insulin resistance, early-onset diabetes mellitus
Introduction
Diabetes mellitus is on the rise in adults as well as in the pediatric population, with an estimated 3% rise annually.1 Although type 1 diabetes is the most common type of diabetes in children, the incidence of type 2 diabetes, which was thought to be uncommon in children, is also increasing.2 Sweden, which is one of the countries with the highest prevalence of children with diabetes in the world, reported the incidence of type 2 diabetes in children as 3.1 per 100,000 per year.3 In Qatar, the reported prevalence is 23.7 per 100,000 for children with type 2 diabetes living in the country and an incidence of 2.51 in 2020.4 In 2019, the US reported 283,000 individuals under 20 years diagnosed with type 2 diabetes and an incidence of 5,800 new cases in 2014–2015.5
In the pediatric population, the onset of type 2 diabetes is most often around the adolescence period, however, there are rare reports of type 2 diabetes developing in children as young as 5 and 8 years of age.6,7 The cause of such early onset type 2 diabetes in childhood is not yet known but might be related to the increasing obesity epidemic seen all over the world, the sedentary lifestyle, possible underlying genetic factors, or as yet unknown factors. The SEARCH for Diabetes in Youth study estimated an overall increase of 30.5% in the prevalence of type 2 diabetes in youth. Out of all children with type 2 diabetes in the 2009 SEARCH database, 2.4% were <10 years of age.8
Here we report the youngest patient with type 2 diabetes from Qatar, with the age of onset at 7 years of age, and describe the clinical and biochemical findings observed.
Case Presentation
We present an 8 year old girl of Sri Lankan ethnicity. She was born at term with a birth weight of 2.45 kg and length of 49 cm. There was no history of any complications including gestational diabetes during the pregnancy. There were no medical concerns in the postnatal or early childhood phases. At the age of 6 years of age the patient was diagnosed with obesity after the parents noted that the child was gaining weight rapidly and getting tired very easily. There was also a history of snoring at night but no apnoea. She presented to the hospital at 7 years of age for these symptoms and was found to have hyperglycemia. The random blood glucose level was 7.8 mmol/L There were no symptoms of polyuria or polydipsia. The child was on a normal diet without excessive calories. There is a family history of type 2 diabetes in grandparents which started at 30 years of age. On examination, she had severe acanthosis nigricans on the neck, axilla and groin area but no dysmorphic features. She was noted to experience shortness of breath on exertion. Her weight was 53.6 kg (99.86 percentile/+2.99 SD) with a BMI of 26.8 kg/m2 (99 percentile). Her height was 141.5 cm (99.28 percentile/+2.45 SD).
Investigations
Liver function tests revealed elevated ALP (359 IU/L) and ALT (63 IU/L). She also had a reduced HDL level of 0.8 mmol/L and triglyceride level of 2 mmol/L. Ultrasound abdomen was performed and it showed hepatomegaly with fatty infiltration suggesting NAFLD (Non-Alcoholic Fatty Liver Disease). All four type 1 diabetes autoantibodies, namely GAD, IAA, IA-2A, and ZnT8, were measured and found to be negative. Diagnosis of type 2 diabetes was thus confirmed. Genetic testing was also performed for the monogenic obesity gene panel which was negative for all known causes of obesity. Some of the important genes tested were ADCT3, ALMS, BBS, CPE, DYRK1B, GNAS, KSR2, LEP, LEPR, MAGEL2, MC3R, MC4R, MCHR1, MRAP2, POMC, PPARG, SH2B1, SIM1, TUB, and UCP3. Thyroid function tests were normal. The monogenic diabetes genes, namely ABCC8, APPL1, BLK, GCK, HNF1A, HNF1B, HNF4A, KCNJ11, KLF11, NEUROD1, PAX4, PDX1, WFS1, INS, and CEL, were also tested and found to be negative. Table 1 shows the laboratory tests done on this patient. Figure 1 shows the liver ultrasound images showing fatty liver.
 |
Table 1 Laboratory Tests Performed with Reference Range |
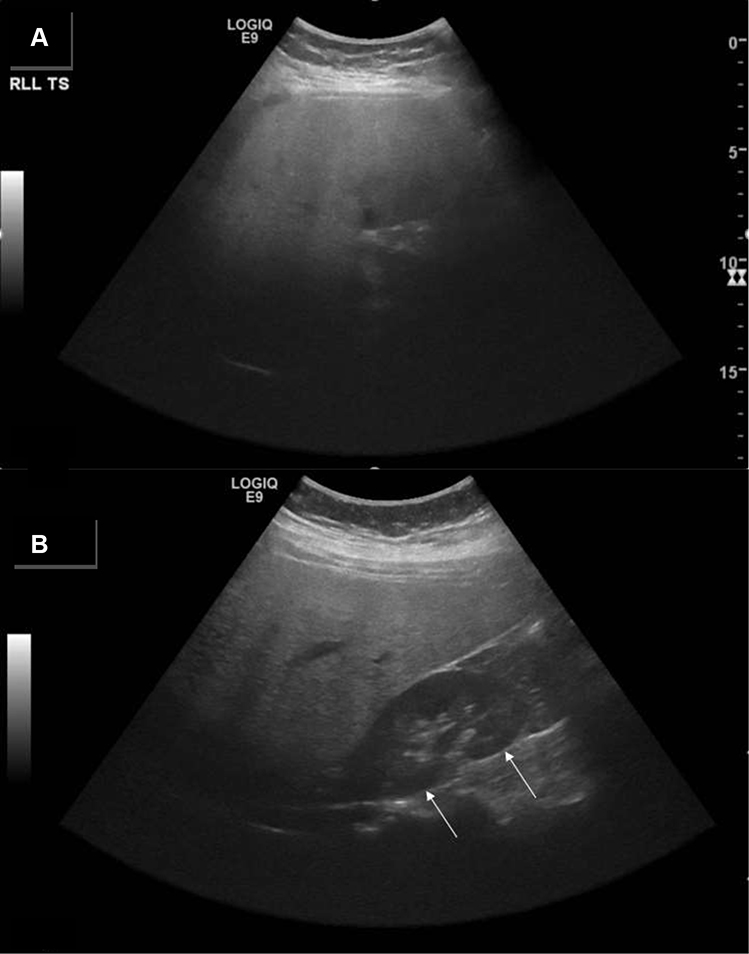 |
Figure 1 Liver ultrasound images in keeping with non-alcoholic fatty liver disease (NAFLD). Axial (A) and longitudinal (B) images of the liver demonstrating a diffuse increase in echogenicity with loss of appreciation of the intrahepatic vasculature and loss of appreciation of the deeper aspects of the liver. The liver is more echogenic than the adjacent kidney (arrows). Appearances are in keeping with non-alcoholic fatty liver disease (NAFLD). |
Treatment and Follow-Up
The patient is being treated with Metformin 500 mg BD and has been advised on lifestyle modifications. She has been followed up for 1 year with good glycemic control and no further deterioration of the disease yet; however, no reduction in weight was observed. Given the age of the patient, only limited options for medical therapy are available and GLP-1 agonists or surgical bypass is not indicated. This could suggest a genetic component to the underlying diagnosis.
Discussion
The global burden of diabetes mellitus is increasing rapidly with a projected average increase in the prevalence of 3–4% per year.9,10 A lower age of onset of the disease is also being observed worldwide, especially in developed countries. Type 2 diabetes, which was thought to be relatively rare in children, also has an increasing incidence globally.2
In children and adolescents, obesity is the main risk factor for developing type 2 diabetes. In a young Pima Indian cohort with diabetes, 85% of the patients were found to be obese.11 Qatar also reported 90% of their children with type 2 diabetes were obese.12 Ethnicity is also recognized as an important risk factor and the influence is more strong in children when compared to adults with higher prevalences seen in Asians, African Americans, Hispanics, and Indigenous people.13
The most common age of onset of type 2 diabetes in children is in the teenage years, but there is only limited data about the incidence in children below 10 years of age. One reason for this could be that young children with diabetes are assumed to have type 1 diabetes and accurate classification is not done. Some previous studies have also reported the presence of beta-cell autoantibodies youth onset type 2 diabetes.14,15 Moreover, obesity can also be seen in many type 1 diabetes patients now, which further complicates the accurate initial diagnosis. Genetic testing for obesity can be useful for detecting if the diabetes is a complication of obesity or a separate condition, since the majority of patients with type 2 diabetes are also obese. The mean age at diagnosis for individuals with NIDDM was 13.9 ± 0.4 years, with a range from 8 to 19 years.7
Nonalcoholic fatty liver disease (NAFLD) is a common comorbidity found in adults with type 2 diabetes. However, studies have reported adolescents with type 2 diabetes also have a higher incidence of NAFLD.16 In one study almost 30% of type 2 diabetic children were associated with NAFLD.17 This is true in our patient as well who was only 7 years old at diagnosis. There is also data that shows that younger children with type 2 diabetes have a more aggressive course of the disease when compared to other types of diabetes and adults.13,18 We observed liver enzyme abnormalities, reduced HDL, and elevated triglycerides in our patient along with NAFLD, suggesting a very advanced course of the disease. Diabetic nephropathy and hypertension are also observed in some children with early onset type 2 diabetes.19 Hence immediate attention for accurate diagnosis of type 2 diabetes is warranted in all children with compatible phenotype and more strict control of HbA1c is required. Close surveillance of comorbidities and complications of diabetes is to be ensured in this group of patients.
The American Diabetes Association recommends screening all youth with BMI >85% and any two risk factors such as a family history of diabetes, gestational diabetes in mother, signs of insulin resistance, certain ethnicities, etc., beginning at 10 years of age or earlier, as well as rescreening every 3 years subsequently.20 Screening criteria should also include polycystic ovary syndrome, hypertension, or dyslipidemia. Screening for microvascular and macrovascular complications should also be performed at diagnosis and in follow-up.21 A large epidemiological study found proliferative retinopathy in 9.1% of children with type 2 diabetes.22
The youngest child with type 2 diabetes reported was a 5 year old Hispanic male who presented with obesity, acanthosis nigricans, and hyperglycemia. Similar to our patient, type 1 diabetes autoantibodies and monogenic diabetes genetic testing were negative. However, this patient received insulin therapy initially due to elevated liver enzymes. Our subject has been on metformin only and monogenic obesity screening was also conducted and ruled out.6
A study done to evaluate genetic risk variants for type 2 diabetes in a cohort of subjects of Sri Lankan descent found that the risk variants identified in Europeans have similar effects in Sri Lankans. TCF7L2, SLC30A8, PROX1, PPARG, and FTO were found to be significant in this cohort. However, this study was done in adults and no similar studies were found in children of Sri Lankan ethnicity.23 There are no reports of any one gene causing type 2 diabetes in children which suggests a more polygenic mechanism. The pathophysiology of early onset type 2 diabetes remains unclear but appears to be multigenic, with environmental and lifestyle influences. There are many treatment options available for type 2 diabetes like glucagon-like peptide-1 (GLP-1) receptor agonists and sodium-glucose cotransporter-2 inhibitors.24 However, the most commonly used option still remains metformin in most countries. Newer therapies like salutary adipokine adiponectin and the hepatokine fibroblast growth factor (FGF) 21, have been extensively researched but have not yielded the expected clinical impact. Bariatric surgery in conjunction with drug therapies may provide better glycemic control and bodyweight reduction when compared with drugs alone.24
To the best of our knowledge, this is the second youngest patient with type 2 diabetes who has been extensively worked up and studied. There is a paucity of reports about long-term outcomes of patients with very early onset type 2 diabetes like the one described here, hence we have to carefully study the outcomes and complications to have a better understanding and form guidelines for accurate diagnosis and management.
Ethics Statement
The protocol for this research project has been approved by the ”Institutional Review Board (IRB) for the protection of human subjects” in Sidra Medicine, Qatar (IRB reference number 1702007592). It conforms to the provisions of the Declaration of Helsinki. Informed consent to take part in the study and publish findings was obtained from the subject(s) and/or guardian(s) prior to study commencement.
Funding
This research was supported by the Qatar National Research Fund (QNRF-NPRP 10-6100017-AXX) awarded to Professor Khalid Hussain.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Patterson CC, Karuranga S, Salpea P, et al. Worldwide estimates of incidence, prevalence and mortality of type 1 diabetes in children and adolescents: results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res Clin Pract. 2019;157:107842. doi:10.1016/j.diabres.2019.107842
2. Candler TP, Mahmoud O, Lynn RM, Majbar AA, Barrett TG, Shield JPH. Continuing rise of type 2 diabetes incidence in children and young people in the UK. Diabet Med. 2018;35(6):737–744. doi:10.1111/dme.13609
3. Thunander M, Petersson C, Jonzon K, et al. Incidence of type 1 and type 2 diabetes in adults and children in Kronoberg, Sweden. Diabetes Res Clin Pract. 2008;82(2):247–255. doi:10.1016/j.diabres.2008.07.022
4. Haris B, Saraswathi S, Al-Khawaga S, et al. Epidemiology, genetic landscape and classification of childhood diabetes mellitus in the State of Qatar. J Diabetes Investig. 2021;12(12):2141–2148. doi:10.1111/jdi.13610
5. Statistics about diabetes [Internet]. USA. Available from: https://www.diabetes.org/about-us/statistics/about-diabetes.
6. Hutchins J, Barajas RA, Hale D, Escaname E, Lynch J. Type 2 diabetes in a 5-year-old and single center experience of type 2 diabetes in youth under 10. Pediatr Diabetes. 2017;18(7):674–677. doi:10.1111/pedi.12463
7. Scott CR, Smith JM, Cradock MM, Pihoker C. Characteristics of youth-onset noninsulin-dependent diabetes mellitus and insulin-dependent diabetes mellitus at diagnosis. Pediatrics. 1997;100(1):84–91. doi:10.1542/peds.100.1.84
8. Pettitt DJ, Talton J, Dabelea D, et al. Prevalence of diabetes in U.S. youth in 2009: the SEARCH for diabetes in youth study. Diabetes Care. 2014;37(2):402–408. doi:10.2337/dc13-1838
9. Ogurtsova K, da Rocha Fernandes JD, Huang Y, et al. IDF diabetes atlas: global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res Clin Pract. 2017;128:40–50. doi:10.1016/j.diabres.2017.03.024
10. Tuomilehto J. The emerging global epidemic of type 1 diabetes. Curr Diab Rep. 2013;13(6):795–804. doi:10.1007/s11892-013-0433-5
11. Dabelea D, Pettitt DJ, Hanson RL, Imperatore G, Bennett PH, Knowler WC. Birth weight, type 2 diabetes, and insulin resistance in Pima Indian children and young adults. Diabetes Care. 1999;22(6):944–950. doi:10.2337/diacare.22.6.944
12. Ahmed SM, Haris B, Saraswathi S, et al. The epidemiology, clinical, biochemical, immunological and radiological features of youth onset type 2 diabetes mellitus in the state of Qatar. Diabetol Int. 2022;13(2):381–386. doi:10.1007/s13340-021-00548-9
13. American Diabetes Association. American Diabetes Association: type 2 diabetes in children and adolescents. Diabetes Care. 2000;23:381–389. doi:10.2337/diacare.23.3.381
14. Umpaichitra V, Banerji MA, Castells S. Autoantibodies in children with type 2 diabetes mellitus. J Pediatr Endocrinol Metab. 2002;15(Suppl 1):525–530.
15. Reinehr T, Schober E, Wiegand S, Thon A, Holl R; DPV-Wiss Study Group. Beta-cell autoantibodies in children with type 2 diabetes mellitus: subgroup or misclassification? Arch Dis Child. 2006;91(6):473–477. doi:10.1136/adc.2005.088229
16. Hecht L, Weiss R. Nonalcoholic fatty liver disease and type 2 diabetes in obese children. Curr Diab Rep. 2014;14(1):448. doi:10.1007/s11892-013-0448-y
17. Newton KP, Hou J, Crimmins NA, et al. Prevalence of prediabetes and type 2 diabetes in children with nonalcoholic fatty liver disease. JAMA Pediatr. 2016;170(10):e161971. doi:10.1001/jamapediatrics.2016.1971
18. Taheri S, Zaghloul H, Chagoury O, et al. Effect of intensive lifestyle intervention on bodyweight and glycaemia in early type 2 diabetes (DIADEM-I): an open-label, parallel-group, randomised controlled trial. Lancet Diabetes Endocrinol. 2020;8(6):477–489. doi:10.1016/S2213-8587(20)30117-0
19. Wong J, Constantino M, Yue DK. Morbidity and mortality in young-onset type 2 diabetes in comparison to type 1 diabetes: where are we now? Curr Diab Rep. 2015;15(1):566. doi:10.1007/s11892-014-0566-1
20. American Diabetes Association. Classification and diagnosis of diabetes: standards of medical care in diabetes-2019. Diabetes Care. 2019;42(Suppl 1):S13–S28. doi:10.2337/dc19-S002
21. Dileepan K, Feldt MM. Type 2 diabetes mellitus in children and adolescents. Pediatr Rev. 2013;34(12):541–548. doi:10.1542/pir.34-12-541
22. Jaiswal M, Divers J, Dabelea D, et al. Prevalence of and risk factors for diabetic peripheral neuropathy in youth with type 1 and type 2 diabetes: SEARCH for diabetes in Youth Study. Diabetes Care. 2017;40(9):1226–1232. doi:10.2337/dc17-0179
23. Hassanali N, De Silva NM, Robertson N, et al. Evaluation of common type 2 diabetes risk variants in a South Asian population of Sri Lankan descent. PLoS One. 2014;9(6):e98608. doi:10.1371/journal.pone.0098608
24. Nauck MA, Wefers J, Meier JJ. Treatment of type 2 diabetes: challenges, hopes, and anticipated successes. Lancet Diabetes Endocrinol. 2021;9(8):525–544. PMID: 34181914. doi:10.1016/S2213-8587(21)00113-3
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.