Back to Journals » Journal of Inflammation Research » Volume 19
Two-Dimensional PCR for Simultaneous Detection of Fecal Bacterial Markers in the Diagnosis and Management of Inflammatory Bowel Disease
Received 18 October 2025
Accepted for publication 24 January 2026
Published 4 February 2026 Volume 2026:19 566519
DOI https://doi.org/10.2147/JIR.S566519
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Nadia Andrea Andreani
Yueying Li, Hui Guo, Weiwei Liu
Department of Laboratory Medicine, Longhua Hospital, Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China
Correspondence: Weiwei Liu, Department of Laboratory Medicine, Longhua Hospital, Shanghai University of Traditional Chinese Medicine, 725 South Wanping Road, Shanghai, 200032, People’s Republic of China, Tel +86-13162640870, Email [email protected]
Background: Inflammatory bowel disease (IBD) is showing an increasing incidence in China, posing a significant threat to public health. IBD patients exhibit gut microbiota dysbiosis, and detection of IBD-associated gut microbes can aid in diagnosis and management.
Methods: We developed a 2D-PCR method based on base-quenching probe technology, which allowed closed-tube, single-tube simultaneous detection of four IBD-associated microbes: Ruminococcus gnavus, Veillonella spp. Ruminococcus torques, and Clostridioides difficile. Clinical fecal samples were tested including 224 IBD patients, 112 patients with other digestive diseases, and 57 healthy controls.
Results: The 2D-PCR method was demonstrated a detection limit of 10 copies/μL and no cross-reactivity between primers. The combination of R. gnavus and Veillonella spp. along with fecal occult blood test (FOBT), distinguished IBD patients from healthy controls (AUC = 0.9224, 95% CI [0.8747– 0.9701], p < 0.0001, Se = 85.11%, Sp = 92.59%) and IBD from other digestive diseases (AUC = 0.7984, 95% CI [0.7132– 0.8837], p < 0.0001, Se = 66.67%, Sp = 84.95%). R. torques was exclusively detected in Crohn’s disease patients (8.33% positivity), suggesting its potential as a specific diagnostic marker, albeit with limited sensitivity. C. difficile was detected in 8.93% of IBD patients and identifying such infections can guide antibiotic therapy and improve patient outcomes.
Conclusion: The 2D-PCR method is cost-effective and suitable for widespread clinical application with low technical and instrumental requirements. These detected microbial markers could aid in IBD diagnosis, differential diagnosis, and treatment guidance, serving as noninvasive biomarkers and expanding the clinical utility of gut microbiota in IBD management.
Keywords: inflammatory bowel disease, microbiology, PCR, molecular diagnostics
Introduction
Inflammatory bowel disease (IBD) is a group of chronic, nonspecific inflammatory disorders of the gastrointestinal tract, primarily including two subtypes: ulcerative colitis (UC) and Crohn’s disease (CD). IBD is showing an increasing incidence world while, which lacks a definitive cure and is characterized by chronic relapse and persistent symptoms, significantly impairing patients’ quality of life.1–3 Diagnosis of IBD lacks a gold standard and is primarily based on a combination of epidemiological data, clinical manifestations, laboratory tests, gastrointestinal endoscopy, imaging studies, histopathological examinations, and microbiological analyses.4 Colonoscopy with mucosal biopsy remains the conventional first-line diagnostic approach for IBD and serves as the primary basis for diagnosis. However, its drawbacks, including time-consuming procedures, invasiveness, and patient reluctance due to discomfort, make it less suitable for repeated assessments in chronic disease management.5 Therefore, developing noninvasive diagnostic techniques and methods is critical for improving clinical practice.
The pathogenesis of IBD involves a complex interplay of immune dysregulation, genetic predisposition, microbial factors, and environmental triggers.6–8 Most IBD patients exhibit gut dysbiosis, marked by an overabundance of harmful bacteria and a depletion of beneficial species.9 This microbial imbalance triggers immune responses that exacerbate inflammation. In turn, the inflammatory environment further disrupts the gut microbiota and its metabolic products, creating a vicious cycle where immune activation perpetuates chronic inflammation.10,11 Currently, the potential of gut microbiota in diagnosing and managing digestive diseases is increasingly being recognized. Fecal microbes closely mirror the composition of the intestinal microbiota and can be directly extracted from stool samples in a noninvasive manner. This positions gut microbiota as a promising noninvasive biomarker in IBD diagnosis.
To identify a panel of gut microbes for IBD diagnosis and treatment, we searched and analyzed fecal microbial data from IBD patients (including CD and UC) and healthy controls in the human gut metagenomic database GMrepo (Data Repository for Human Gut Microbiota).12 Elevated abundances of Ruminococcus gnavus, Clostridioides difficile, and some members of the Veillonella genus in IBD patients were reported previously. It has been reported that R. gnavus is elevated in IBD, and various molecules including methylation-controlled J, glucopolysaccharides, ursodeoxycholic acid, interleukin-10, interleukin-17, and capric acid have been proposed as potential contributors to the link between R. gnavus and IBD.13,14 Abundance of Veillonella spp. was reported to be higher than that in healthy controls. Proinflammatory diet may drive the increase of Veillonella spp. and calprotectin, which could contribute to the relapse of IBD.15,16 It also has been reported that patients with IBD have a higher incidence of C. difficile infection (CDI), and C. difficile may be an important factor in IBD exacerbation.17–19 Vancomycin and fidaxomicin are the preferred agents for the management of CDI in IBD, which can reduce hospitalization time.20 Detection of C. difficile and diagnosis of CDI can guide the timely treatment of IBD-CDI.21 Ruminococcus torques showed increased abundance in CD but decreased abundance in UC, suggesting its potential for differentiating between IBD subtypes. The accurate detection of these microbial biomarkers may enable earlier diagnosis and targeted intervention of IBD and ultimately improve patient prognosis.
Culture-based method is a fundamental tool for the detection of gut microbiota, however, it is constrained by low throughput, low coverage and time consumption. 16S rRNA sequencing, while enabling high-throughput analysis, offers limited taxonomic resolution. Metagenomic next-generation sequencing is cost-ineffective and involves complex data analysis, which limits its widespread application. Two-dimensional PCR (2D-PCR) is a multiplex PCR technique that combines base-quenched probe technology with melting curve analysis.22 Tag sequences were designed according to probe sequences, which were homologous to the probe sequence but containing several single nucleotide polymorphisms. Addition of tag sequences to upstream of the forward primers for different targets generates variations in the melting temperature (Tm) of the amplified products. The results are then interpreted based on the melting curve peaks at corresponding temperatures. This method is simple to operate, requires minimal expertise and instrument specifications, and is cost-effective, making it suitable for widespread clinical application.
In previous study, we constructed a 2D-PCR method and applied it to the detection of Clostridium cluster XVIII solely for the auxiliary diagnosis of IBD.22 In this study, by redesigning the tag and primer sequences and reconfigured the reaction system, we adjusting the microbial profiling to R. gnavus, Veillonella spp., C. difficile, and R. torques. We aimed to assess the diagnostic performance of constructed 2D-PCR method for simultaneous detection of IBD-related fecal bacteria and investigate its potential role in disease differentiation and therapeutic guidance.
Materials and Methods
Fluorescent Probe and Tagged Primer Design
FAM probe (from 5′ to 3′): FAM-CCATTACCAACCTTATACACTTCCAC-P) was used for signal detection. Tags were designed by changing a few bases in the probe sequence. Designed tags were added to the 5′ terminus of the forward primer, so that the Tm of each primer would be distinctive according to the sequence of corresponding tags. When amplification occurred, the products of each tagged primer could be distinguished by melting curves with different Tms. 16S rRNA sequences of C. difficile, R. gnavus, Veillonella spp., and R. torques were retrieved from National Center for Biotechnology Information (NCBI), and primers were designed using its online tools. An internal control primer was designed based on the shared conserved sequences at 16S rRNA of all bacteria to monitor the effect of stool DNA extraction (16S rRNA). FAM probe and primers were constructed from sequences from Sangon Biotech (Shanghai) Co. Ltd. (Table 1).
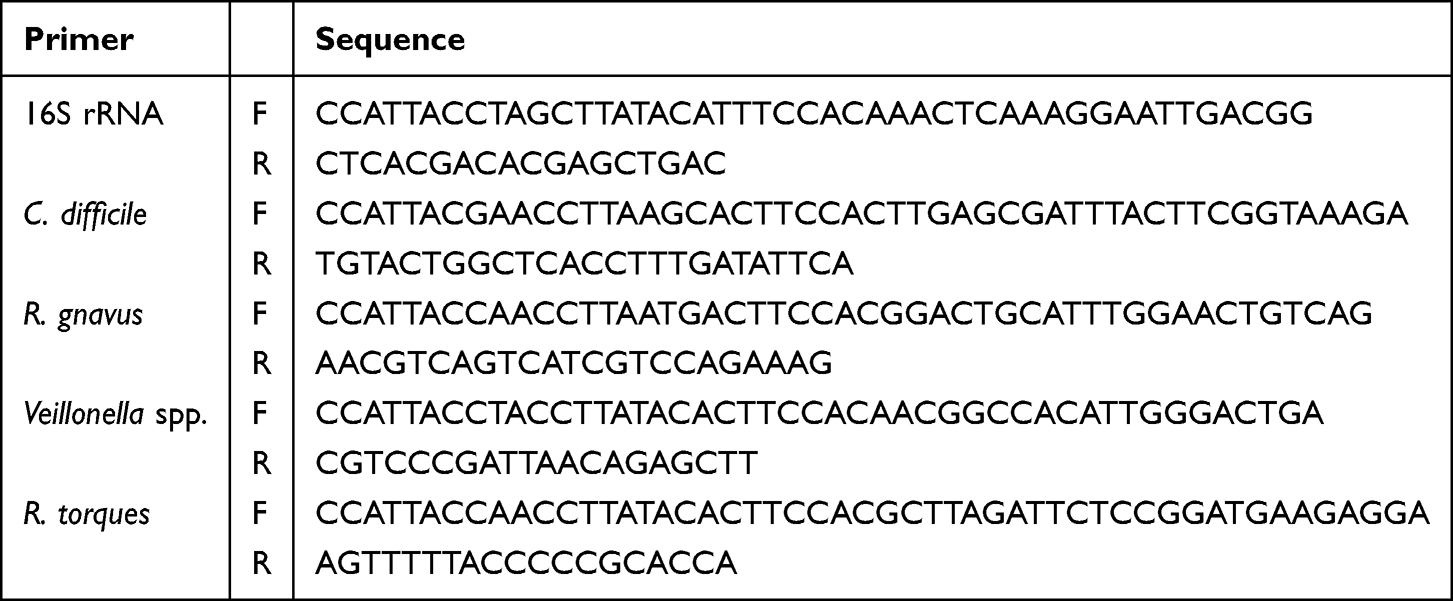 |
Table 1 Sequences of Tagged Forward and Reverse Primers |
Construction of 2D-PCR System
The volume of the 2D-PCR system was 25 μL, which was constructed with 10 × PCR Buffer (containing Tris-HCl and KCl, Mg2+ free) (Takara Biomedical Technology (Beijing) Co. Ltd.), 2.5 μL; 25 mM MgCl2 (Takara), 1.5 μL; 4 × 2.5 mM dNTPs (Takara), 0.7 μL; 5 U/μL hot Taq DNA polymerase (Takara), 0.5 μL; 10 μmol/L FAM probe, 0.4 μL; 10 μmol/L tagged forward primers, 0.1 μL, respectively; 10 μmol/L reverse primers, 0.6 μL, respectively; DNA template, 2 μL; and deionized distilled water, 13.9 μL (to 25 μL). Stool-extracted DNA or synthetic plasmids were used as DNA templates. 2D-PCR amplification procedure was: (1) 95°C, 10 min; (2) 95°C, 10 s; 60°C, 40 s; 40 cycles; (3) 95°C, 1 min; heated from 30°C to 80°C in increments of 0.5°C, with each lasting 4 s, while fluorescence intensity was detected; 40°C, 30 s. Melting curves were obtained in step (3), and the presence of distinct peaks at the target-specific melting temperature (Tm) indicates a positive detection result.
Performance Validation of 2D-PCR Method
Sequences of forward and reverse primers of 16S rRNA, C. difficile, R. gnavus, Veillonella spp., and R. torques were retrieved from the NCBI database, and were attached to the pUC57 vector to construct corresponding plasmids. Plasmids were obtained from Sangon Biotech (Shanghai) Co. Ltd. Plasmids were dissolved and diluted as a series of concentration gradients: 108, 107, 106, 105, 104, 1000, 100, and 10 copies/μL. These gradients were used to verify the minimum detection limits for each target. Plasmids with a concentration of 105 copies/μL were used to verify the cross-reaction among the primers.
Patients and Samples
We included patients diagnosed with IBD in Longhua Hospital Shanghai University of Traditional Chinese Medicine, who were admitted to hospital between January 2023 and December 2024 and underwent laboratory tests. All IBD patients were endoscopically and histopathologically diagnosed with CD or UC according to the generally accepted international diagnostic criteria. Healthy individuals or patients without any digestive diseases comprised the control group. Patients with other digestive diseases (including colorectal cancer, anal fistula, colon polyps, and stomach polyps) comprised the other digestive diseases group. All patients were randomly divided into the training cohort and validation cohort. Stool samples of all individuals were collected after testing in the department of laboratory medicine, underwent immediate visual quality control and promptly stored at –80°C, with a maximum storage duration of 6 months prior to analysis to prevent DNA degradation.
Stool DNA Extraction
Stool DNA was extracted using TIANamp Stool DNA Kit (Tiangen Biotech Co. Ltd., Beijing, China). Firstly, 200 mg stool samples were used for DNA extraction; 500 μL Buffer SA, 100 μL Buffer SC, 15 μL Proteinase K, and 0.25 g beads were added and mixed with samples. The mixed samples were incubated at 70°C for 15 min until lysed thoroughly. Lysed samples were centrifuged at 12,000 rpm for 3 min, and the supernatant was transferred into a new tube with 10 μL RNase A, shaken, mixed, and allowed to stand for 5 min. Then, 200 μL Buffer SH was added to the mix, which was shaken, mixed, and allowed to stand for 5 min. Samples were centrifuged at 12,000 rpm for 3 min. The supernatant was transferred to a new tube and an equal volume of Buffer GFA was added to the tube, shaken, mixed, and transferred to a CR2 adsorption column, which was placed in a companion collection tube. The CR2 adsorption column and collection tube were centrifuged at 12,000 rpm for 30 s and the waste liquids in the collection tube were discarded. DNA was absorbed in the CR2 adsorption column and washed once with 500 μL Buffer GD followed by two washes with 700 μL Buffer PW. After the last wash and discarding the waste liquid, the CR2 adsorption column was placed in the collection tube without any liquid added and centrifuged at 12,000 rpm for 2 min. The CR2 adsorption column was placed in a new tube, which was left open for a few minutes. Then, 50 μL Buffer TB was added to the CR2 adsorption column. The column was allowed to stand for 3 min and centrifuged at 12,000 rpm for 2 min. DNA solution was collected into new tubes under the CR2 adsorption column, stored at –20°C, no more than 1 month for further detection. To avoid contamination, all procedures were performed in a biological safety cabinet using certified DNA-free reagents and consumables. Negative controls were processed in parallel with each batch of samples to confirm the absence of exogenous DNA contamination.
Statistical Analysis and Construction of Diagnostic Models
Statistical analyses were performed using SPSS version 25 (IBM Corp., Chicago, IL, USA), GraphPad Prism version 7.0 (San Diego, CA, USA), R version 4.4.3 (R Foundation for Statistical Computing) and RStudio version 2025.09.2+418. To investigate combined use of bacteria and clinical indicators, multivariate analyses based on binary logistic regression analyses were performed to identify independent predictors of each individual marker for various panels. Corresponding receiver operating characteristic (ROC) curves for each combination were calculated using SPSS and plotted using GraphPad. Area under the ROC curve (AUC) was used to assess the diagnostic efficacy of each panel. The diagnostic value of each panel in the validation cohort was also determined by ROC curve analysis. Kappa consistency analysis was employed to assess the inter-batch consistency of the detection method. K-fold cross-validation was performed using the “caret” package in R, and calibration curve validation was performed using the “rms” package in R.
Results
Construction of 2D-PCR Method
Sequences of tagged forward and reverse primers are shown in Table 1. 2D-PCR was first performed in a single-primer system in which only one pair of primers was added: 10 × PCR Buffer (Mg2+ free), 2.5 μL; 25 mM Mg2+, 1.5 μL; 4 × 2.5 mM dNTPs, 0.7 μL; 5 U/μL hot Taq DNA polymerase, 0.5 μL; 10 μmol/L FAM probe, 0.4 μL; 10 μmol/L tagged forward primers, 0.1 μL; 10 μmol/L reverse primers, 0.6 μL; DNA template, 2 μL; deionized distilled water, 16.7 μL (to 25 μL). The melting curves of five primers were distributed at five distinctive temperatures (Figure 1). The Tm of 16S rRNA, C. difficile, R. gnavus, Veillonella spp., and R. torques was 43°C, 47°C, 52°C, 58°C, and 63°C, respectively (Figure 1A–E), which could be separated completely (Figure 1F).
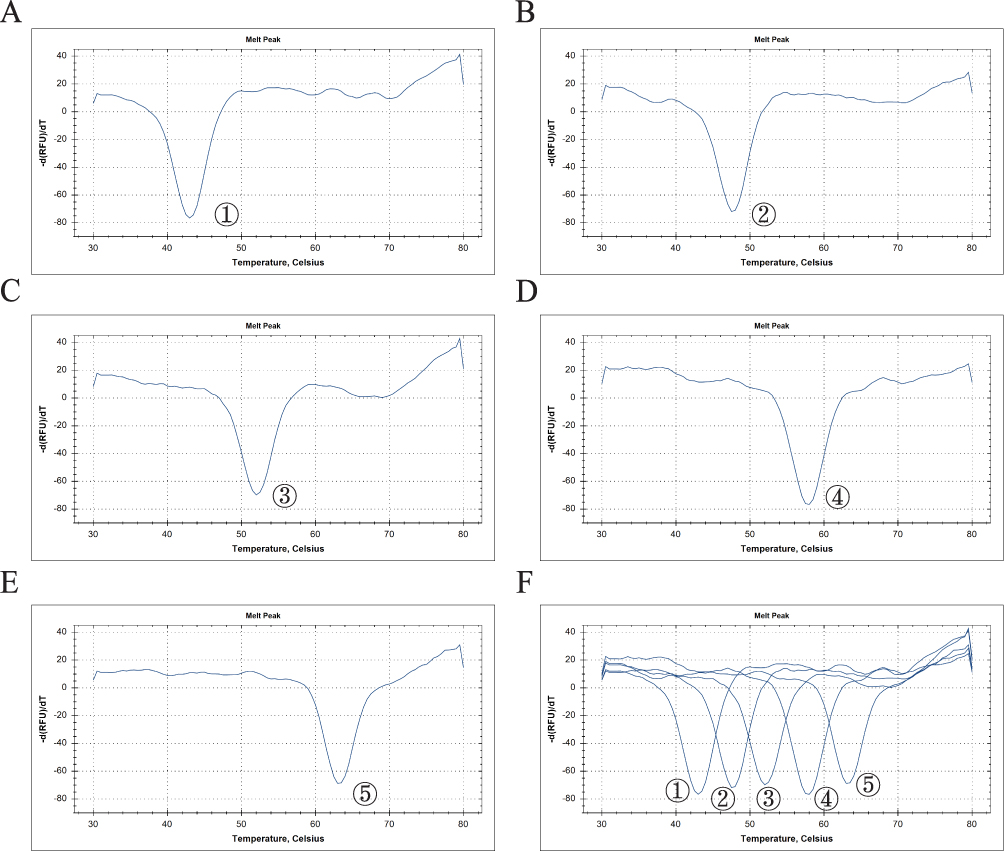 |
Figure 1 Melting curves of five tagged primers with different Tm. (A) 16S rRNA (Tm = 43°C). (B) C. difficile (Tm = 48°C). (C) R. gnavus (Tm = 52°C). (D) Veillonella spp. (Tm = 58°C). (E) R. torques (Tm = 63°C). (F) Five melting curves with distinctive Tm. |
Performance Validation of 2D-PCR Method
To exclude the nonspecific cross-reactivity among primers, we performed 2D-PCR based on a single-primer system. Five single-primer systems were used, each with a different plasmid as the DNA template (at a concentration of 105 copies/μL). The results confirmed that each target primer only reacted with its corresponding primer, with no cross-reactivity observed among primers (Figure 2). A single-primer system was used, with serially diluted plasmids (108, 107, 106, 105, 104, 1000, 100, and 10 copies/μL) as templates. The lowest concentration that produced a detectable melting curve peak was determined as the minimum detection limit. The minimum detection limits for R. gnavus, Veillonella spp., R. torques, C. difficile, and the internal control were 100, 10, 1000, 10, and 10 copies/μL, respectively (Figure 3).
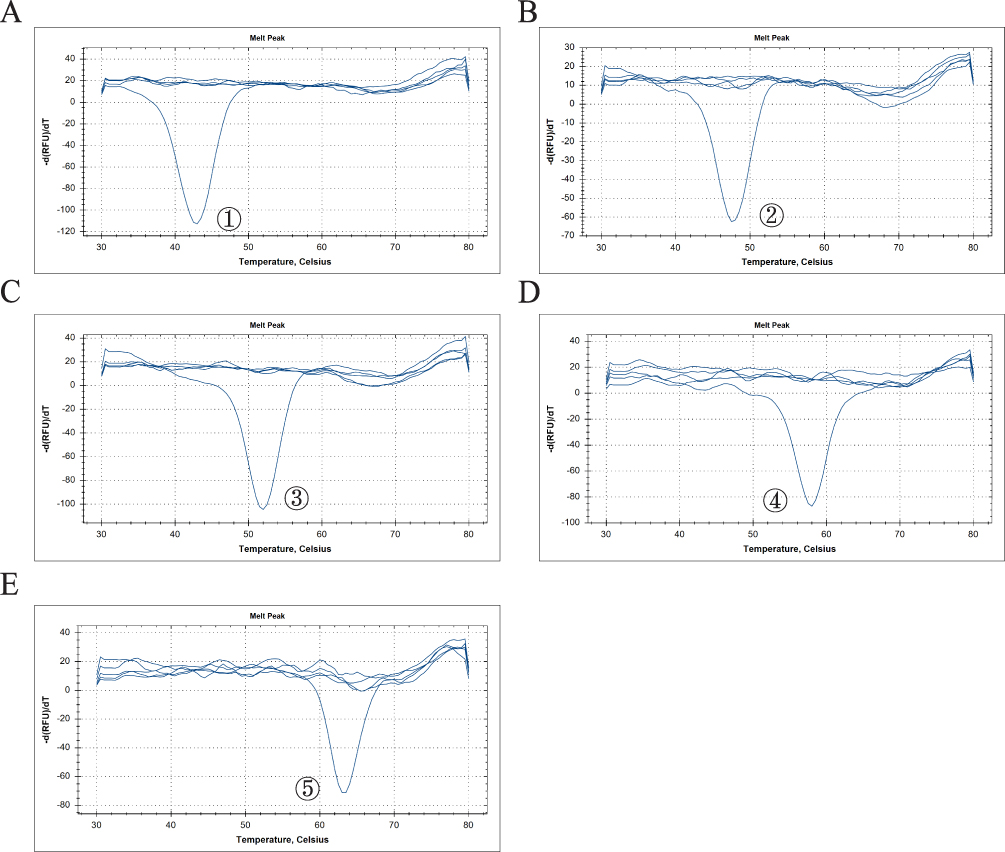 |
Figure 2 No cross-reaction among primers and primers only amplified with their corresponding plasmids. (A) 16S rRNA. (B) C. difficile. (C) R. gnavus. (D) Veillonella spp. (E) R. torques. |
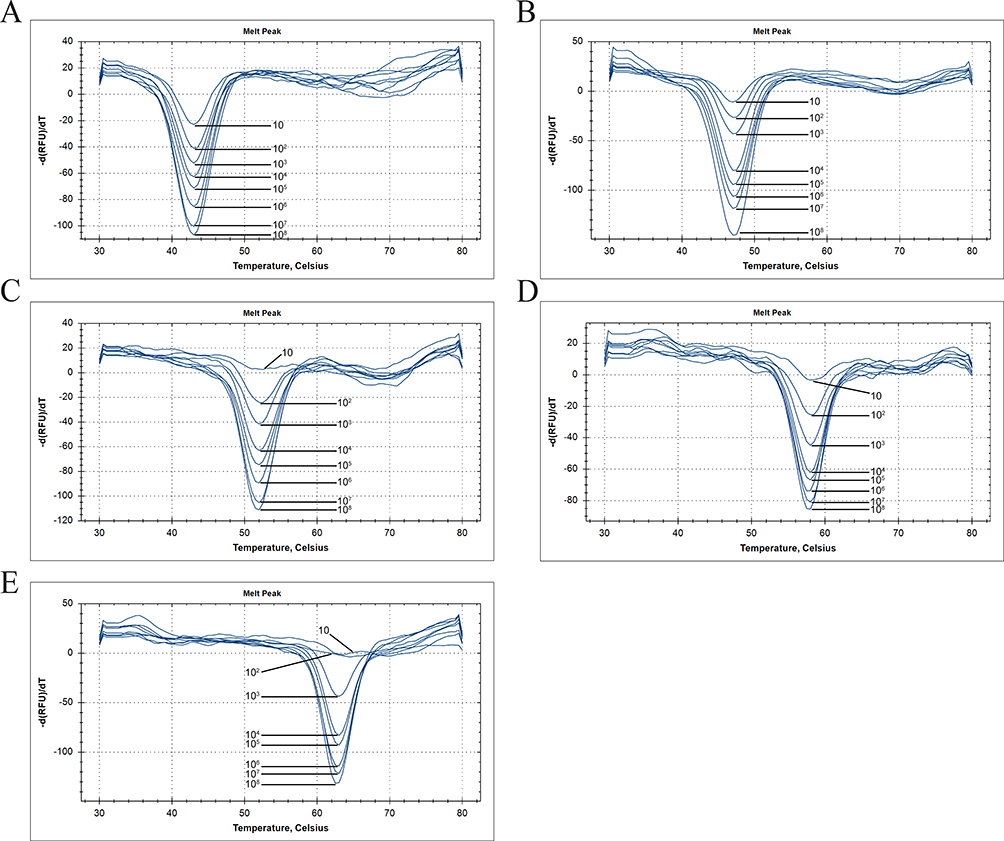 |
Figure 3 Minimum detection limits for each target. (A) 16S rRNA, 10 copies/μL. (B) C. difficile, 10 copies/μL. (C) R. gnavus, 100 copies/μL. (D) Veillonella spp., 10 copies/μL. (E) R. torques, 1000 copies/μL. |
Construction of 2D-PCR Mixed System
A mixed reaction system containing five pairs of primers was established and the DNA template used was a mixture of five plasmids; each at a concentration of 105 copies/μL, to simulate a mixed-infection sample. The 2D-PCR mixed system demonstrated simultaneous detection of four microbial targets and the internal control, with distinct melting curve peaks for each target (Figure 4). Tm of internal control, C. difficile, R. gnavus, Veillonella spp., and R. torques was 41°C, 46°C, 51°C, 58°C, and 63°C, respectively, which may be lower than that in the single primer system.
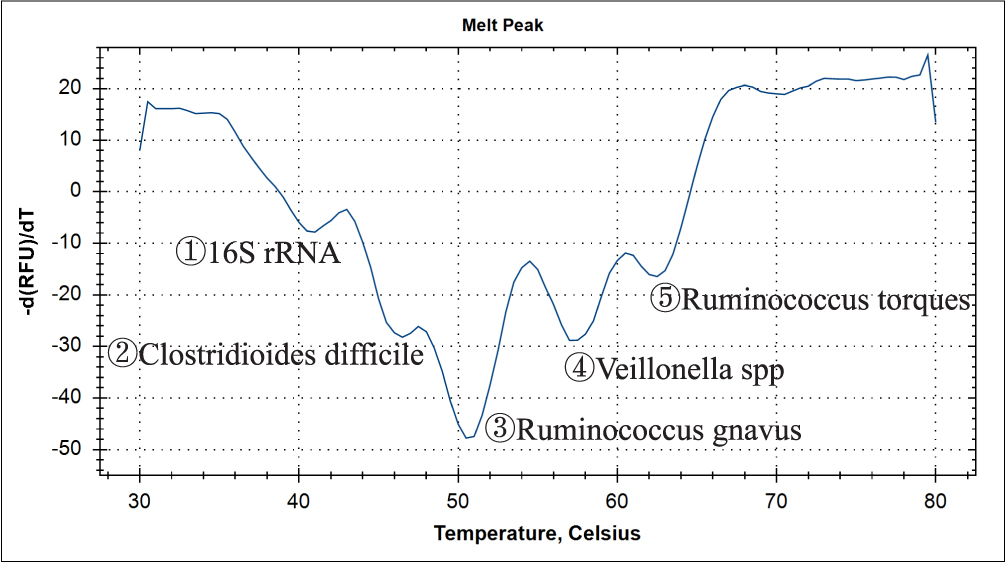 |
Figure 4 Melting curves of five primers detected simultaneously by single tube. Tm of 16S rRNA, C. difficile, R. gnavus, Veillonella spp., and R. torques was 41°C, 46°C, 51°C, 57°C, and 63°C, respectively, which may be lower than that in the single primer system. |
Characteristics of Patients
There were 114 patients with IBD (60 with CD and 54 with UC), 29 controls, 55 patients with other digestive diseases included in the training cohort, and 110 patients with IBD (60 with CD and 50 with UC), 28 controls, and 57 patients with other digestive diseases included in the validation cohort. Clinical and biochemical parameters, including sex, age, C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), fecal calprotectin (FC), and fecal occult blood test (FOBT), were collected and used for the construction of the diagnostic model. Characteristics of patients in the training and validation cohorts are showed in Tables S1 and S2, respectively.
Detection of Clinical Samples
DNA was extracted from stool samples. The 2D-PCR mixed system was utilized to detect four microbial targets, and representative results are shown in Figure 5. A dual-replicate design was performed for each sample over two separate batches. The intra-batch concordance rate was 100%. Kappa consistency test demonstrated great inter-batch consistency with kappa value of 0.882, 0.903, 0.787 and 0.773 in C. difficile, R. gnavus, Veillonella spp., and R. torques, respectively (Table S3). Only samples with a positive internal control were used for further analysis. Internal control negative samples were re-extracted and retested. Positive rates of C. difficile, R. gnavus, Veillonella spp., and R. torques in IBD patients were 9.6%, 56.1%, 39.4%, and 3.5% (only CD), respectively, in the training cohort (Table 2), and 8.2%, 59.1%, 41.8%, and 5.5% (only CD) in the validation cohort (Table 3). Positive rates of C. difficile and R. torques were both <10%, and they were excluded from construction of the diagnostic model. Positive rates of R. gnavus and Veillonella spp. in IBD patients were both higher than in the control group (31% and 6.9% in training cohort; 35.7% and 10.7% in validation cohort) and other digestive diseases group (43.6% and 21.8% in training cohort; 29.8% and 19.3% in validation cohort). These were used for construction of the diagnostic model.
 |
Table 2 Positive Rate of 4 Microbes in IBD, Other Digestive Diseases and Controls in the Training Cohort |
 |
Table 3 Positive Rate of 4 Microbes in IBD, Other Digestive Diseases and Controls in the Validation Cohort |
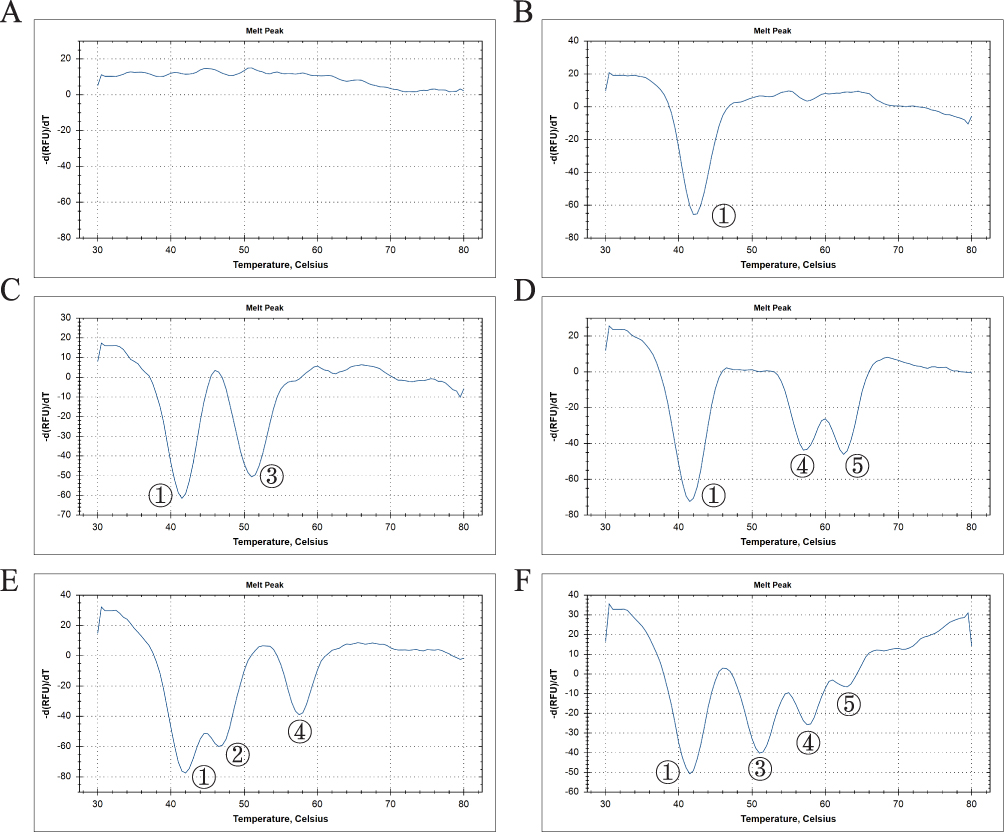 |
Figure 5 Examples of clinical sample detection. (A) Invalid result of failed fecal DNA extraction. (B) Negative result. (C) Positive result of R. gnavus. (D) Positive result of Veillonella spp. and R. torques. (E) Positive result of C. difficile and Veillonella spp. (F) Positive result of R. gnavus, Veillonella spp., and R. torques. |
Construction of Diagnostic Model to Differentiate IBD from Control Group
R. gnavus and Veillonella spp. were used for construction of the diagnostic model. Through binary logistic regression analysis, a diagnostic model based on two markers was constructed to differentiate the IBD group from the control group. ROC curve and AUC were used to evaluate the diagnostic performance of the model. The AUC of the R. gnavus+Veillonella spp. model was 0.7129 with a 95% confidence interval (CI) of 0.6191–0.8068 in the training cohort (p < 0.001) (Figure 6A), which was validated in an independent validation cohort with an AUC of 0.7076 (95% CI 0.6099–0.8053, p < 0.001) (Figure 6D). The integration of FOBT enhanced the diagnostic efficacy of the model, achieving an AUC of 0.8719 (95% CI 0.8029–0.9408, p < 0.0001) (Figure 6B) in the training cohort and 0.9224 (95% CI 0.8747–0.9701, p < 0.0001) (Figure 6E) in the validation cohort. Under the optimal cutoff value, sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) of R. gnavus+Veillonella spp.+FOBT model were 85.11%, 92.59%, 91.99% and 86.14%, respectively. Key diagnostic indices of all models were shown in Table 4. K-fold cross-validation showed that accuracy of R. gnavus+Veillonella spp.+FOBT model for IBD diagnosis was 0.8318 (kappa value 0.5002). Calibration curve validation indicated that the model has a high predictive accuracy for IBD diagnosis with mean absolute error of 0.034 (Figure S1A). When combined with CRP and ESR, the diagnostic performance of model improved slightly but not significantly (Figure 6C and F), suggesting that the combination may be unnecessary.
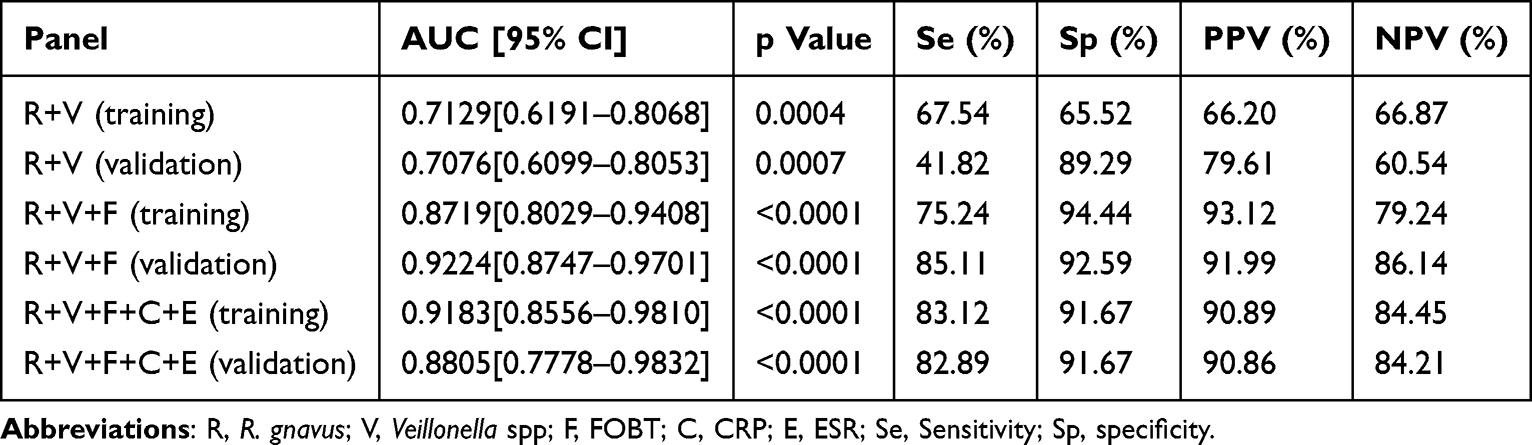 |
Table 4 Performances of Models Distinguishing IBD from Control Group in Training and Validation Cohorts |
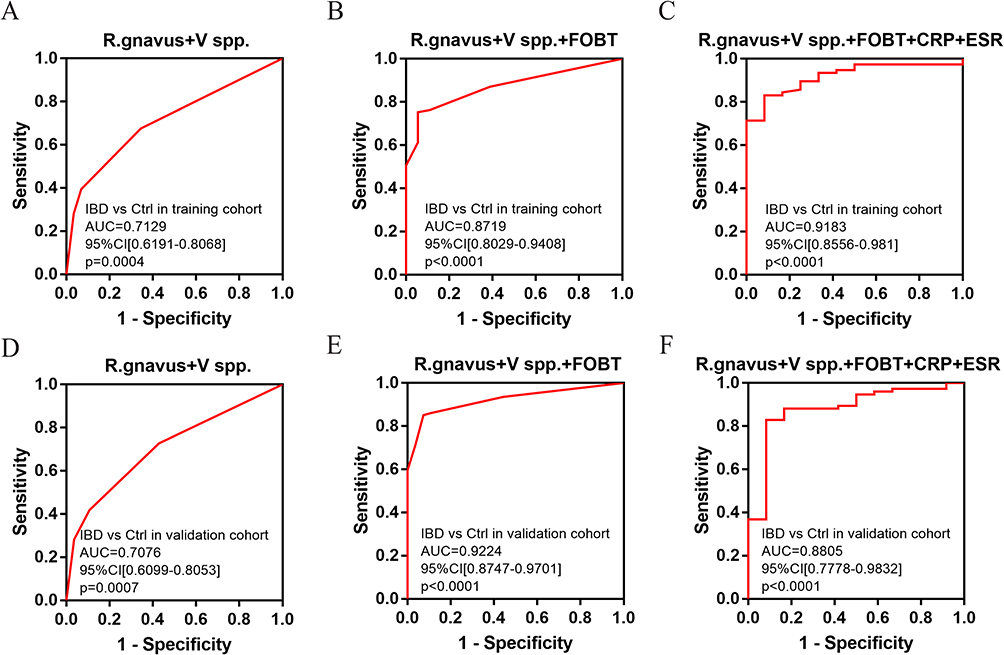 |
Figure 6 ROC curves for models distinguishing IBD from control group in training and validation cohorts. (A) R. gnavus+V spp. in training cohort (AUC = 0.7129, Se = 67.54%, Sp = 65.52%). (B) R. gnavus+V spp.+FOBT in training cohort (AUC = 0.8719, Se = 75.24%, Sp = 94.44%). (C) R. gnavus+V spp.+FOBT+CRP+ESR in training cohort (AUC = 0.9183, Se = 83.12%, Sp = 91.67%). (D) R. gnavus+V spp. in validation cohort (AUC = 0.7076, Se = 41.82%, Sp = 89.29%). (E) R. gnavus+V spp.+FOBT in validation cohort (AUC = 0.9224, Se = 85.11%, Sp = 92.59%). (F) R. gnavus+V spp.+FOBT+CRP+ESR in validation cohort (AUC = 0.8805, Se = 82.89%, Sp = 91.67%). Abbreviations: V spp., Veillonella spp.; Se, Sensitivity; Sp, specificity. |
Construction of Diagnostic Model to Differentiate IBD from Other Digestive Diseases
C. difficile and R. torques were excluded from the diagnostic model because of their low positivity rate. R. gnavus and Veillonella spp. were used for construction of the diagnostic model through binary logistic regression analysis. For differentiating IBD from other digestive diseases, the diagnostic performance of the R. gnavus+V spp. model was poor, with an AUC of 0.61 (95% CI 0.5215–0.6984, p < 0.05) (Figure 7A) in the training cohort and 0.6864 (95% CI 0.6013–0.7714, p < 0.0001) (Figure 7D) in the validation cohort. When combined with FOBT, AUC was enhanced to 0.7164 (95% CI 0.6265–0.8063, p < 0.0001) (Figure 7B) in the training cohort and 0.7984 (95% CI 0.7132–0.8837, p < 0.0001) (Figure 7E) in the validation cohort. Under the optimal cutoff value, sensitivity, specificity, and predictive values of models were also shown in Table 5. K-fold cross-validation showed that accuracy of R. gnavus+Veillonella spp.+FOBT model differentiating IBD from other digestive diseases was 0.7346 (kappa value 0.3420). Calibration curve validation indicated that the model has a high predictive accuracy for IBD with mean absolute error of 0.022 (Figure S1A). Similarly, integration of CRP did not enhance the diagnostic efficacy significantly (Figure 7C and F).
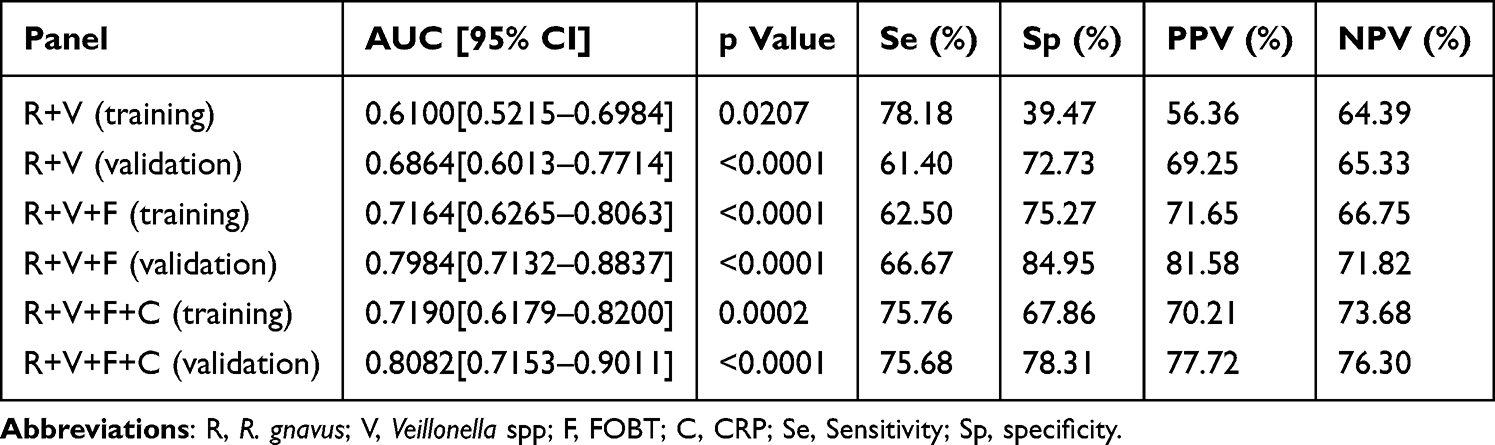 |
Table 5 Performances of Models Distinguishing IBD from Other Digestive Diseases in Training and Validation Cohorts |
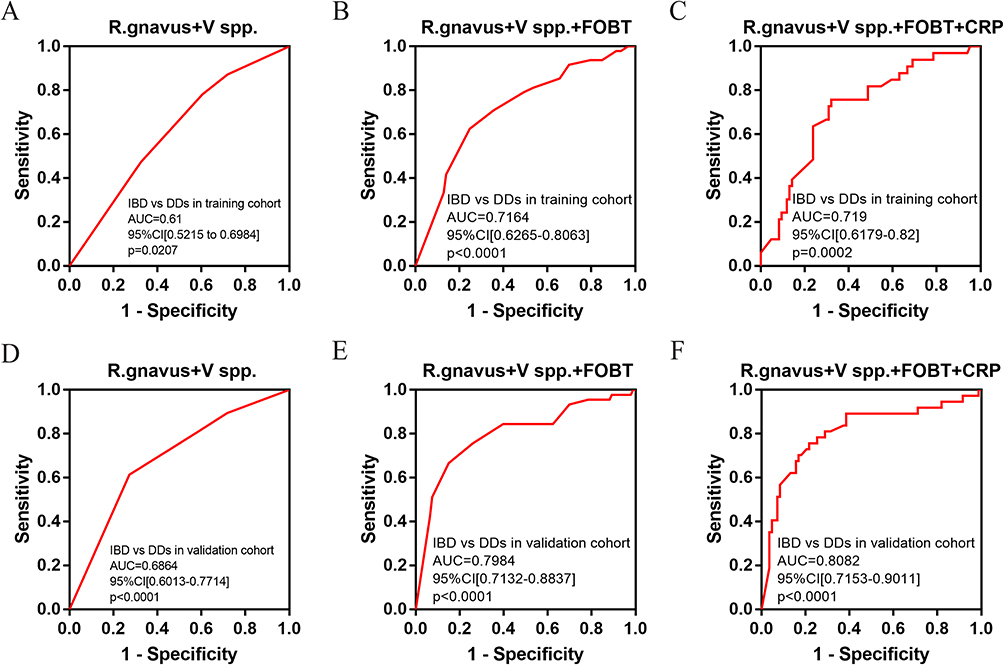 |
Figure 7 ROC curves for models distinguishing IBD from other digestive diseases in training and validation cohorts. (A) R. gnavus+V spp. in training cohort (AUC = 0.61, Se = 78.18%, Sp = 39.47%). (B) R. gnavus+V spp.+FOBT in training cohort (AUC = 0.7164, Se = 62.50%, Sp = 75.27%). (C) R. gnavus+V spp.+FOBT+CRP in training cohort (AUC = 0.719, Se = 75.76%, Sp = 67.86%). (D) R. gnavus+V spp. in validation cohort (AUC = 0.6864, Se = 61.40%, Sp = 72.73%). (E) ROC curve for combination of R. gnavus+V spp.+FOBT in validation cohort (AUC = 0.7984, Se = 66.67%, Sp = 84.95%). (F) ROC curve for combination of R. gnavus+V spp.+FOBT+CRP in validation cohort (AUC = 0.8082, Se = 75.68%, Sp = 78.31%). Abbreviations: V spp., Veillonella spp.; Se, Sensitivity; Sp, specificity. |
Application of R. torques in CD Diagnosis
R. torques was positive in 4.91% (10/224) of IBD patients included in the training and validation cohorts, but negative in the control group and other digestive diseases group (Tables 2 and 3). In the IBD patients, R. torques was detected exclusively in CD patients (10/120, 8.33%) and was negative in UC patients, suggesting its potential as a specific biomarker for CD. To investigate the performance of R. torques combined with clinical laboratory indicators, we performed binary logistic regression analysis in CD and UC patients. Combination of R. torques, FOBT, and ESR distinguished CD from UC with an AUC of 0.7503 (95% CI 0.6433–0.8573, p < 0.001) (Figure 8A) in the training cohort and 0.6957 (95% CI 0.5821–0.8093, p < 0.01) (Figure 8B) in the validation cohort, which can be used as an IBD differential diagnosis model.
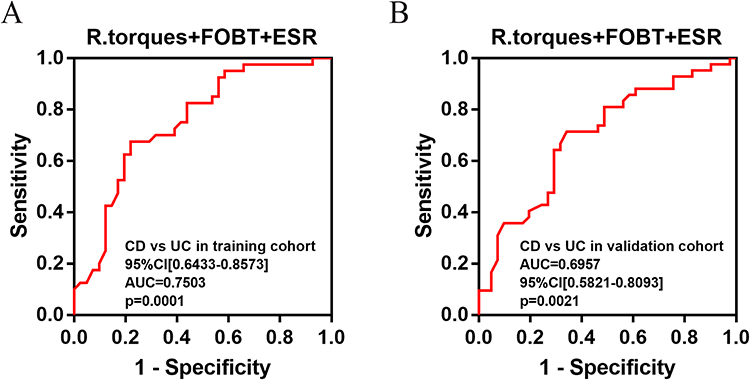 |
Figure 8 ROC curves of R. torques+FOBT+ESR model for distinguishing CD from UC in IBD patients. (A) AUC = 0.7503 (p < 0.001) in training cohort; (B) AUC = 0.6957 (p < 0.01) in validation cohort. |
Treatment Strategy Based on C. difficile Detection
Positive rate of C. difficile was 8.93% (20/224) in IBD patients included in the training and validation cohorts. Among 20 patients positive for C. difficile, medical records of nine were available. Two patients received antibiotic therapy including latamoxef, nalanxin, imipenem or sulperazon, and three were treated with immunosuppressants, including ustekinumab, vedolizumab or upadacitinib, which were recognized as risk factors for concurrent CDI. Four patients underwent C. difficile testing using culture and identification methods during the medical visit, but only one result was positive. One patient exhibited typical symptoms of CDI with observed pseudomembrane formation in the intestines; however, the result of C. difficile testing based on culture and identification was still negative, which may have led to a delay in treatment. The 2D-PCR method can enhance the detection rate of CDI to optimize IBD management, including application of vancomycin or fidaxomicin and adjustment to the application of biologics or immunomodulators. This could contribute to improved efficacy of IBD treatment.
Discussion
Gut microbiota dysbiosis plays an important role in the pathogenesis and progression of IBD. It disrupts intestinal barrier integrity, promotes aberrant immune activation, and sustains chronic inflammation through altered microbial metabolites and dysregulated host-microbe interactions. These processes collectively drive disease initiation, exacerbation, and clinical relapse in susceptible individuals.10,11 Gut microbiota detection is valuable for the diagnosis and monitoring of IBD. In this study, we constructed a 2D-PCR method based on base-quenched probe technology and melting curve analysis, which can be used to detect R. gnavus, Veillonella spp., R. torques, and C. difficile from stool samples in a single-tube system. Compared to 16S rRNA sequencing and metagenomic next-generation sequencing, 2D-PCR method is more accurate and cost-effective. In addition, it provides the benefits of direct interpretation of results, clear readability, low technical and instrumental requirements, which make it suitable for widespread clinical application.
R. gnavus and Veillonella spp. combined with FOBT were used to construct the diagnostic model for IBD. R. torques combined with FOBT and ESR was used as a specific diagnostic marker for CD as well as UC/CD differentiation. As a direction for future research, more IBD-related indicators such as fecal calprotectin could be considered to involving in the diagnostic model for IBD monitoring and recurrence prediction. The current assay requires enhanced sensitivity to reliably detect low abundance of R. torques, which was 1000 copies/μL, which was poorer than for other targets. In addition, for CD-specific diagnosis, the performance of the combined R. torques+FOBT+ESR model was not ideal, with an AUC of 0.7503 and 0.6957 only. This was partly due to the low positive rate of R. torques. A lower limit of R. torques detection may enhance its positive rate in CD patients and its efficacy for CD diagnosis. System optimization based on primer redesign or higher template input will be considered.
C. difficile detection contributed to clinical diagnosis and timely treatment of IBD-CDI. IBD is an independent risk factor for CDI and suggests a globally increased prevalence and severity of C. difficile coinfection in IBD patients (CDI-IBD). Studies have revealed that glucocorticoids, immunosuppressive agents, and biological agents, which may increase the risk of systemic infection and immunosuppression, and antibiotics, nonsteroidal anti-inflammatory drugs, and proton pump inhibitors, which may damage the intestinal flora and gastric acid barrier, also increase the risk of CDI-IBD. In this study, 2D-PCR enhanced the positive rate of CDI in IBD patients, among our positive patients.20 Five of nine patients were exposed to risk factors including immunosuppressive agents or antibiotics, consistent with the literature.20 The symptoms of CDI closely resemble those of active IBD, but the treatment approaches differ significantly. The low clinical detection rate of C. difficile may lead to delayed treatment. Detection based on 2D-PCR can guide CDI treatment and improve diagnostic–therapeutic efficiency.
Before construction of the diagnostic model, several stool samples were excluded because of failed DNA extraction, which may be attributed to improper sample collection or preservation. The quality of clinical samples is one of the most important factors for good test results. Preanalytical variability including stool handling, DNA degradation may influence detection rates of microbes, which should be optimized and standardized further. To facilitate the widespread clinical application of the method, we will further investigate the impact of sample processing methods, including preservative solutions. The development and utilization of fecal biomarkers in IBD diagnosis and management remain insufficient, lagging behind blood-based indicators. Non-standardized sampling and testing procedures are some of the major limiting factors for their clinical application. From this perspective, standardized protocols for sample collection and preservation should be implemented.
Conclusion
In summary, we established a 2D-PCR method that detected R. gnavus, Veillonella spp., R. torques, and C. difficile simultaneously in a single closed tube. The procedure is simple to perform, cost-effective, and suitable for repeated monitoring in IBD management. Limitations remain, such as insufficient sensitivity for detecting R. torques, which requires further optimization. Nevertheless, detection of these fecal markers serves as a complementary approach to conventional biomarkers, aiding in the diagnosis and management of IBD. As a direction for further research, 2D-PCR method holds potential adaptation for broader microbial panels, and multicenter clinical validation is required to validate its clinical significance.
Abbreviations
IBD, Inflammatory bowel disease; UC, ulcerative colitis; CD, Crohn’s disease; CDI, C. difficile infection; PCR, polymerase chain reaction; 2D-PCR, Two-dimensional PCR; Tm, melting temperature; NCBI, National Center for Biotechnology Information; AUC, Area under the ROC curve; CRP, C-reactive protein, ESR, erythrocyte sedimentation rate; FC, fecal calprotectin; FOBT, fecal occult blood test; CI, confidence interval; PPV, positive predictive value; NPV, negative predictive value.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
This study was conducted in full compliance with the ethical standards of the institutional and national research committees, as well as the principles outlined in the Declaration of Helsinki and other applicable guidelines. Ethical approval was granted by the Ethics Committee of Longhua Hospital, Shanghai University of Traditional Chinese Medicine (Approval No. 2022LCSY099). Prior to participation, written informed consent was obtained from all individuals involved in the study. Strict measures were implemented throughout the research to ensure confidentiality and protect participant data in accordance with ethical and legal requirements.
Acknowledgments
We thank International Science Editing for editing this paper. The study adhered to the RECORD guidelines.
Author Contributions
Yueying Li: Formal analysis; Investigation; Methodology; Writing-original draft. Hui Guo: Data curation, Validation; Visualization; Writing-original draft. Weiwei Liu: Conceptualization, Funding acquisition; Project administration; Resources; Supervision; Writing-review and editing. All authors took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the National Natural Science Foundation of China (Grant No. 82472361), the grant of Shanghai Municipal Health Leading Talent Plan of Shanghai Municipal Health Commission (Grant No. 2022LJ021), the grant of Scientific and Technological Innovation Action Plan-Medical Innovation Special Research Project from Shanghai Municipal Commission of Science and Technology (Grant No. 22Y11902900, 23Y11908000).
Disclosure
The authors declare that they have no competing interests.
References
1. Hracs L, Windsor JW, Gorospe J, et al. Global evolution of inflammatory bowel disease across epidemiologic stages. Nature. 2025;642(8067):458–14. doi:10.1038/s41586-025-08940-0
2. Kaplan GG, Windsor JW. The four epidemiological stages in the global evolution of inflammatory bowel disease. Nat Rev Gastroenterol Hepatol. 2021;18(1):56–66. doi:10.1038/s41575-020-00360-x
3. Xu L, He B, Sun Y, et al. Incidence of Inflammatory Bowel Disease in Urban China: a Nationwide Population-based Study. Clin Gastroenterol Hepatol. 2023;21(13):3379–86.e29. doi:10.1016/j.cgh.2023.08.013
4. Plevris N, Lees CW. Disease Monitoring in Inflammatory Bowel Disease: evolving Principles and Possibilities. Gastroenterology. 2022;162(5):1456–75.e1. doi:10.1053/j.gastro.2022.01.024
5. Buisson A, Gonzalez F, Poullenot F, et al. Comparative Acceptability and Perceived Clinical Utility of Monitoring Tools: a Nationwide Survey of Patients with Inflammatory Bowel Disease. Inflammatory Bowel Dis. 2017;23(8):1425–1433. doi:10.1097/MIB.0000000000001140
6. Jiang P, Zheng C, Xiang Y, et al. The involvement of TH17 cells in the pathogenesis of IBD. Cytokine Growth Factor Rev. 2023;69:28–42. doi:10.1016/j.cytogfr.2022.07.005
7. Lu Q, Yang MF, Liang YJ, et al. Immunology of Inflammatory Bowel Disease: molecular Mechanisms and Therapeutics. J Inflamm Res. 2022;15:1825–1844. doi:10.2147/JIR.S353038
8. Wan J, Zhou J, Wang Z, et al. Epidemiology, pathogenesis, diagnosis, and treatment of inflammatory bowel disease: insights from the past two years. Chinese Med J. 2025;138(7):763–776. doi:10.1097/CM9.0000000000003542
9. Haneishi Y, Furuya Y, Hasegawa M, Picarelli A, Rossi M, Miyamoto J. Inflammatory Bowel Diseases and Gut Microbiota. Int J Mol Sci. 2023;25(1):24. doi:10.3390/ijms25010024
10. Hu Y, Chen Z, Xu C, Kan S, Chen D. Disturbances of the Gut Microbiota and Microbiota-Derived Metabolites in Inflammatory Bowel Disease. Nutrients. 2022;15(1):14. doi:10.3390/nu15010014
11. Vich Vila A, Zhang J, Liu M, Faber KN, Weersma RK. Untargeted faecal metabolomics for the discovery of biomarkers and treatment targets for inflammatory bowel diseases. Gut. 2024;73(11):1909–1920. doi:10.1136/gutjnl-2023-329969
12. Dai D, Zhu J, Sun C, et al. GMrepo v2: a curated human gut microbiome database with special focus on disease markers and cross-dataset comparison. Nucleic Acids Res. 2022;50:D777–d84.
13. Vich Vila A, Hu S, Andreu-Sánchez S, et al. Faecal metabolome and its determinants in inflammatory bowel disease. Gut. 2023;72(8):1472–1485. doi:10.1136/gutjnl-2022-328048
14. Hong J, Fu T, Liu W, et al. An Update on the Role and Potential Molecules in Relation to Ruminococcus gnavus in Inflammatory Bowel Disease, Obesity and Diabetes Mellitus. Diabetes Metabolic Syndrome Obesity. 2024;17:1235–1248. doi:10.2147/DMSO.S456173
15. Rocha I, Torrinhas R, Fonseca D, et al. Pro-Inflammatory Diet Is Correlated with High Veillonella rogosae, Gut Inflammation and Clinical Relapse of Inflammatory Bowel Disease. Nutrients. 2023;16(1):15. doi:10.3390/nu16010015
16. Scanu M, Toto F, Petito V, et al. An integrative multi-omic analysis defines gut microbiota, mycobiota, and metabolic fingerprints in ulcerative colitis patients. Front Cell Infect Microbiol. 2024;14:1366192. doi:10.3389/fcimb.2024.1366192
17. Shoaei P, Shojaei H, Jalali M, et al. Clostridium difficile isolated from faecal samples in patients with ulcerative colitis. BMC Infect Dis. 2019;19(1):361. doi:10.1186/s12879-019-3965-8
18. Dong D, Su T, Chen W, et al. Clostridioides difficile aggravates dextran sulfate solution (DSS)-induced colitis by shaping the gut microbiota and promoting neutrophil recruitment. Gut Microbes. 2023;15(1):2192478. doi:10.1080/19490976.2023.2192478
19. Cook L, Wong MQ, Rees WD, et al. Dysregulated Immunity to Clostridioides difficile in IBD Patients Without a History of Recognized Infection. Inflammatory Bowel Dis. 2024;30(5):820–828. doi:10.1093/ibd/izad238
20. Tang M, Wang C, Xia Y, Tang J, Wang J, Shen L. Clostridioides difficile infection in inflammatory bowel disease: a clinical review. Exp Rev Anti-Infective Ther. 2024;22(5):297–306. doi:10.1080/14787210.2024.2347955
21. Gonzales-Luna AJ, Skinner AM, Alonso CD, et al. Redefining Clostridioides difficile infection antibiotic response and clinical outcomes. Lancet Infect Dis. 2023;23(7):e259–e65. doi:10.1016/S1473-3099(23)00047-6
22. Wu X, Li Y, Shang Y, et al. Application of two-dimensional polymerase chain reaction to detect four types of microorganisms in feces for assisted diagnosis of IBD. Int J Clin Chem. 2024;555:117802. doi:10.1016/j.cca.2024.117802
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.