Back to Journals » Biologics: Targets and Therapy » Volume 12
Two decades with omalizumab: what we still have to learn
Authors Incorvaia C ![]() , Mauro M, Makri E, Leo G, Ridolo E
, Mauro M, Makri E, Leo G, Ridolo E
Received 19 July 2018
Accepted for publication 22 September 2018
Published 26 October 2018 Volume 2018:12 Pages 135—142
DOI https://doi.org/10.2147/BTT.S180846
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Doris Benbrook
Cristoforo Incorvaia,1 Marina Mauro,2 Elena Makri,1 Gualtiero Leo,3 Erminia Ridolo4
1Cardiac/Pulmonary Rehabilitation, ASST Pini/CTO, Milan, Italy; 2Allergy Department, Sant’Anna Hospital, Como, Italy; 3Pediatric Allergy and Respiratory Pathophysiology Unit, Department of Pediatrics, Vittore Buzzi Children’s Hospital, Milan, Italy; 4Department of Medicine and Surgery, University of Parma, Parma, Italy
Abstract: From its availability for clinical use nearly two decades ago for severe asthma, omalizumab has gained strong evidence of efficacy and safety in the treatment of severe asthma not controlled by standard-of-care therapy. It has been acknowledged by Global Initiative on Asthma guidelines as add-on therapy against severe uncontrolled asthma. Thanks to controlled trials supporting its efficacy, omalizumab has also been licensed for the treatment of chronic spontaneous urticaria. The optimal duration of treatment in either disease has not been established. Despite its high price, omalizumab appears to be cost-effective in severe uncontrolled asthma as well as in chronic urticaria. The literature suggests a wide range of applications for omalizumab in various disorders regardless of allergic or non-allergic pathophysiology.
Keywords: anti-IgE antibody, omalizumab, severe asthma, chronic spontaneous urticaria, efficacy, safety, cost-effectiveness
Major steps in omalizumab development
The rational basis for treating immunoglobulin (Ig)E-mediated allergy with anti-IgE antibodies has been envisioned for a long time. However, use of murine anti-IgE in vivo was precluded for a long time by anaphylactic reactions to heterologous antibodies. Nevertheless, murine anti-IgE was used commonly for in vitro studies to investigate allergic pathophysiology by blockade of mediator release by basophils and mast cells.
Eventually, a recombinant anti-IgE humanized monoclonal antibody-E25, known today as “omalizumab”, fulfilled all the requirements for clinical use thanks to its peculiar composition: it contains 95% of a human IgG1 antibody, whereas the specific antibody-binding site of murine origin comprises <5% of the total molecule.1 Clinical trials have shown the efficacy of omalizumab against IgE-mediated allergic diseases,2 particularly against allergic asthma.3 Omalizumab seems to be able to result in a decrease of mediator release, thus reducing allergic inflammation, through inhibition of IgE binding to the high-affinity IgE receptor (FcεRI) on the surface of mast cells and basophils.3
Several trials have confirmed the therapeutic role of omalizumab. Omalizumab is acknowledged in Global Initiative for Asthma guidelines with the indication for severe uncontrolled asthma at 150 mg every 4 weeks to 375 mg every 2 weeks, with individual dosing dependent on body weight and level of total IgE up to 700 IU/mL.4 In 2006, a Cochrane meta-analysis (14 randomized trials involving 3,143 patients) by Walker et al5 showed a significant decrease in levels of free IgE compared with placebo. It also revealed significant differences in favor of omalizumab with regard to the number of patients able to reduce use of inhaled corticosteroids by >50% and the number of patients who could stop daily intake of inhaled corticosteroids.5
The evidence provided by Walker et al5 was strengthened by additional meta-analyses. An updated Cochrane meta-analysis in 2014 looking at 25 trials on adults and children showed that omalizumab reduced the prevalence of asthma exacerbations and hospitalizations as adjunctive therapy to inhaled corticosteroids and was significantly more effective than placebo in achieving a decrease in use or withdrawal of inhaled corticosteroids. Other studies have shown the capacity of omalizumab to spare the use of oral corticosteroids in patients with severe, persistent asthma.6–9 Also, the prevalence of serious adverse events was shown to be significantly lower with omalizumab than with placebo by Normansell et al.10
With regard to anaphylactic reactions, the Executive Committees of the American Academy of Allergy, Asthma & Immunology as well as the American College of Allergy, Asthma and Immunology formed the Omalizumab Joint Task Force with the aim to review the incidence of anaphylaxis to omalizumab. In 39,510 patients receiving omalizumab, an anaphylaxis-reporting rate of 0.09% of patients was estimated.11
Other types of adverse events, such as thrombocytopenia, parasitosis (giardiasis), and dyspnea were reported by Yalcin et al, who suggested monitoring patients with severe asthma for ≥3 hours after omalizumab injection.12 No such reactions were described in patients treated for urticaria but, due to the much more recent approval of omalizumab for such indications, longer observation is needed to draw conclusions.
In the Cochrane meta-analysis by Normansell et al, the authors mentioned that the sparing effect of omalizumab on the use of systemic corticosteroids and potential threshold level of baseline serum IgE for optimal efficacy merited further investigation.10
In another meta-analysis, Lai et al analyzed the controlled trials carried out for ≥52 weeks involving an overall population of 2,749 patients. The ability of omalizumab to achieve complete withdrawal of inhaled corticosteroids was demonstrated, along with significant improvements in quality of life (QoL) as well as good safety and tolerability.13
It is now acknowledged that real-life studies expand the information on a given medical treatment because they include patients seen in everyday clinical practice (who are frequently not admitted to controlled trials because of the rigid selection criteria). Alhossan et al undertook a meta-analysis on 25 studies that evaluated the effectiveness of omalizumab in real-life conditions, including the heterogeneity of patients and clinicians, and sites of treatment. The effectiveness indicators were: lung function; symptom control; corticosteroid use; prevalence of exacerbations and hospitalizations at 4, 6, 12, and 24 months; and QoL. Asthma treatment with omalizumab was associated with many patients receiving a good-to-excellent response to treatment according to all indicators. Alhossan et al concluded that the results in real life “mirror and extend the efficacy data from randomized controlled trials (RCTs)”.14
Despite the important outcomes mentioned earlier, factors that can affect application of omalizumab for asthma should be considered. The results obtained in diseases other than asthma allow us to imagine further applications of omalizumab. Omalizumab efficacy has been reported for several IgE-mediated (allergic rhinitis, food allergy, allergic bronchopulmonary aspergillosis, anaphylaxis, atopic dermatitis) and non-IgE-mediated (urticaria, nasal polyposis, idiopathic angioedema, mastocytosis) disorders,15 but several others are emerging, as described in the following section.
Issues to be investigated in omalizumab treatment
Optimal duration of treatment in patients with asthma
Clinical data
The first study investigating the optimal duration of omalizumab treatment for asthma was published by Nopp et al in 2010. Eighteen patients with severe allergic asthma were followed up for 3 years after 6-year treatment with omalizumab. At the end of follow-up after treatment withdrawal, 12 patients had improved or unchanged asthma compared with those having ongoing omalizumab treatment.16 Xolair Persistency of Response after Long-term Therapy (XPORT) was a double-blind, placebo-controlled trial for patients with moderate-to-severe persistent asthma receiving long-term omalizumab treatment randomized to two arms: continuing omalizumab at the same dose vs withdrawal to placebo. Patients were followed up for 1 year, with exacerbation of severe asthma as the primary outcome. Also, Asthma Control Questionnaire and Asthma Control Test (ACT) scores were used to assess symptom control. The number of patients without asthma exacerbations was significantly higher in the omalizumab group (67%) than in the placebo group (47.7%). Moreover, patients continuing with omalizumab therapy had significantly better asthma control (as defined by lower scores in the Asthma Control Questionnaire and ACT).17
In the Omalizumab Dose Reduction (OMADORE) study, the follow-up duration was extended to 30 months. In a group of patients with severe asthma receiving omalizumab for at least 12–18 months, provided they had reached the lowest tolerated dose and had spirometric values equal or better than that at study entry, the omalizumab dose was halved, and in the case of clinical stability after 6 months, halved for a second time. In 34.3% of patients, it was possible to withdraw omalizumab treatment.18
In a real-life study involving 49 asthmatic patients who agreed to stop omalizumab treatment after 6 years, 12 patients relapsed in the first year after discontinuation and seven within 13–48 months. Global results suggested that the effects of 6 years of omalizumab treatment could be maintained in 60% of patients for ≥4 years.19
Biomarkers that could be used as criteria for withdrawal of omalizumab treatment
The first biomarker proposed for withdrawal of omalizumab treatment was identified by Nopp et al due to a significant downregulation of basophil allergen sensitivity (CD-sens).16 In a recent study, the same authors used CD-sens as an index to measure the efficacy of omalizumab treatment in 32 patients during 16–32 weeks. CD-sens turned negative in nine patients but remained positive in 15 cases. In the latter group of patients, the omalizumab dose was increased, and resulted in negative CD-sens for an additional three patients. Based on these findings, Nopp et al suggested that CD-sens could be used as a measure of the direct effect of omalizumab therapy to monitor IgE-mediated allergic asthma,20 but this hypothesis needs to be tested in prospective studies on larger groups of patients.
Another reliable biomarker for discontinuation of omalizumab treatment could be generation of cluster of differentiation (CD)4+ Foxp3+ regulatory T cells. These cells seem to be related to the development of tolerance to the causative allergen orientating the immune response involved in asthma pathogenesis.21,22 Other candidate biomarkers to monitor treatment response and possible use as cessation criteria based on the development of a negative test have been proposed. In particular, two biomarkers clearly related to asthma severity have been proposed: blood levels of eosinophils and fractional exhaled nitric oxide.23 In a prospective real-world study of 801 patients with asthma receiving omalizumab, 622 completed the study. Treatment was successful (as assessed by a reduced prevalence of exacerbation and hospitalizations, as well as improved ACT scores), but a significant correlation with biomarker status was not detected.24 The potential importance of allowing more precise monitoring of omalizumab efficacy and use as a criterion for ceasing omalizumab therapy means that further studies are needed.
Outcome of omalizumab treatment in other allergic and non-allergic disorders
As mentioned earlier, the clinical efficacy of omalizumab in other diseases has been reported.25 Reports on a spectrum of IgE-mediated reactions (in which efficacy is expected) will not be discussed here. Instead, efficacy against conditions not definitely related to IgE-mediated mechanisms or allergic disorders will be discussed. The former consists of exercise-induced anaphylaxis26 and oral allergy syndrome.27 With regard to the latter, Table 1 shows the additional disorders reported as “responsive” to omalizumab in recent years. Most articles are case reports or case series that require confirmation. The only controlled trial was carried out on chronic sinusitis,28 and was based on previous positive findings obtained in nasal polyposis, for which a systematic review is available.40 The authors showed that monoclonal antibodies (not only omalizumab but also reslizumab and mepolizumab were evaluated) improved several outcomes, including opacification (as assessed by computed tomography), nasal airflow, olfaction, and QoL, along with changes in type-2 helper T-cell (Th2)-associated biomarkers and good safety and tolerability.28
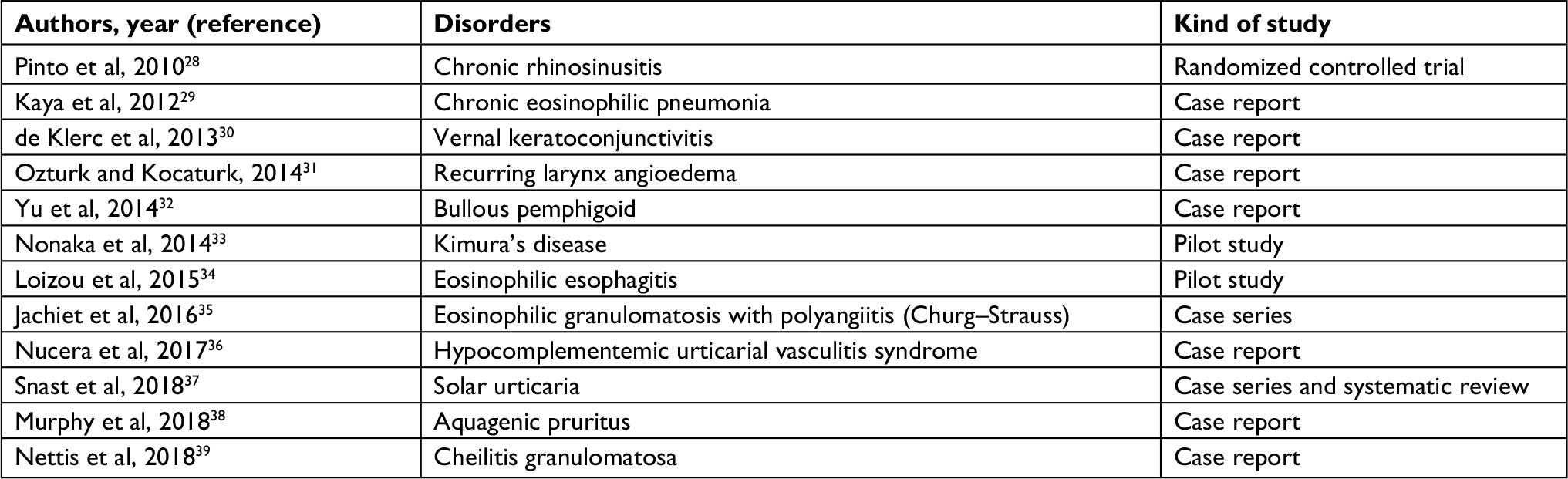 | Table 1 Non-IgE-mediated disorders recently reported as responsive to omalizumab |
Among new reports there are further variants of urticaria which, in addition to those known already, make this type of skin disease the most frequently associated with omalizumab efficacy.
Chronic urticaria
Chronic idiopathic urticaria is more commonly termed “chronic spontaneous urticaria” (CSU). Omalizumab treatment has been shown to be efficacious and safe, initially from a randomized, placebo-controlled trial that compared doses of 75, 300, and 600 mg, with the latter two doses being significantly effective.41 Kaplan et al analyzed the efficacy obtained with omalizumab doses of 75, 150, and 300 mg in three RCTs. The response was dose-dependent, the highest being achieved with 300 mg.42 Further trials confirmed such outcomes and showed that after a 12-week course of omalizumab treatment, urticaria remained well controlled for the subsequent 24 weeks.43
RCT evidence resulted in approval by the US Food and Drug Administration and European Medicine Agency to license omalizumab treatment in patients aged ≥12 years with CSU who remain symptomatic despite the use of H1 antihistamine agents. Omalizumab efficacy was endorsed recently in a prospective Phase IV study in 136 CSU patients receiving 300 mg of omalizumab every 4 weeks for 12 weeks.43 However, just as for asthma, the optimal duration of treatment is not known.44 Using a 12-week schedule, the prevalence of relapse of urticaria following treatment discontinuation was high.45 Ferrer et al undertook a re-analysis of the data from the ASTERIA trial using a high baseline urticaria activity score and early response to treatment to estimate the probability of rapid relapse of urticaria.46 Just like for asthma, biomarkers possibly associated with treatment response were investigated.
Due to the importance of D-dimer (a degradation product of fibrin) as a marker of disease activity in CSU,47 some studies have assessed its role in predicting the response to omalizumab treatment. Cugno et al recently reviewed available data and concluded that the baseline levels of D-dimer were higher in treatment-responsive patients.48 Interestingly, even though CSU is not an IgE-mediated disease, the total IgE level was found to be predictive of response to omalizumab treatment. In fact, non-responders to omalizumab had significantly lower IgE levels (17.9 IU/mL, range 17.0–55.0 IU/mL) compared with partial responders (82.0 IU/mL, range 46.2–126.5 IU/mL) (P=0.008) and complete responders (73.7 IU/mL, range 19.45–153.8 IU/mL) (P=0.032).49
Another quite common subgroup of urticaria is chronic inducible urticaria (CIU), which is elicited by several physical triggers, such as cold, heat, and delayed pressure.50 Maurer et al carried out a systematic review of the available literature (43 studies [trials, case series, and case reports]) on the effect of omalizumab treatment upon CIU. The highest evidence of efficacy was found for symptomatic dermographism as well as cold and/or solar urticaria, with rapid onset of action in most cases and complete/partial symptom relief in many patients, along with good safety and tolerability in adults and children.51 However, omalizumab is not approved for use in CIU or for all other variants of urticaria except CSU, so it may only be used off-label.52 Regardless of the level of evidence for the different subgroups of urticaria, the mechanism of action of omalizumab is not known. Table 2 highlights the putative mechanisms of action suggested so far, none of which have been demonstrated definitely to work.
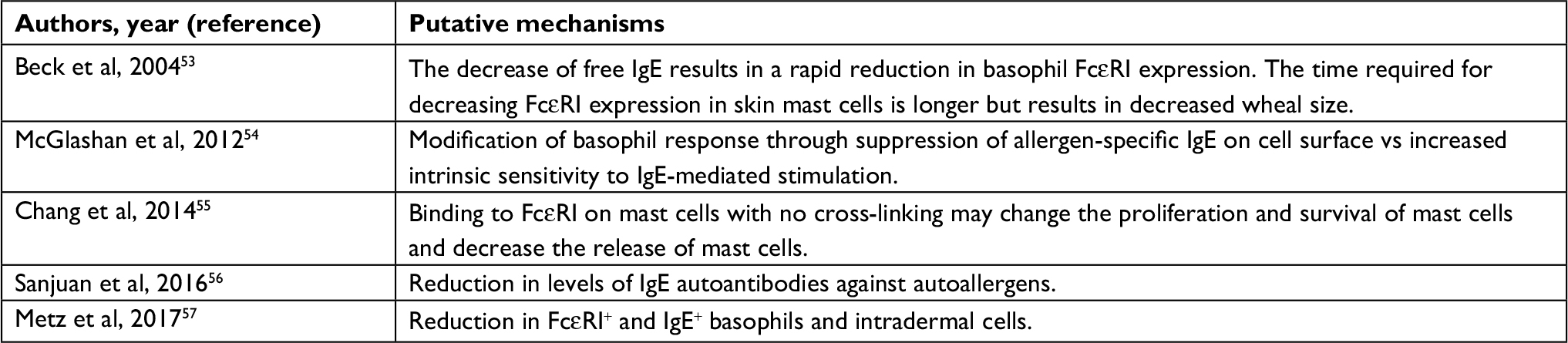 | Table 2 Putative mechanisms of omalizumab in urticaria |
Omalizumab and allergen immunotherapy (AIT)
Even though omalizumab may be beneficial in people with non-allergic asthma and a high level of total IgE,58,59 allergic asthma remains the major target. A pivotal treatment of respiratory allergy (including rhinitis and asthma) is AIT, which is the only etiological treatment.60
The safety of AIT has been a critical issue previously due to anaphylactic (and sometimes fatal) reactions due to subcutaneous administration. After identification of the major risk factors (and particularly the high risk associated with uncontrolled asthma when the allergen extract is injected), the prevalence of severe reactions is very low.61 However, in patients who develop such reactions, switching to other routes of administration (especially the safer sublingual route) or withdrawal of AIT could prevent further reactions.62 This strategy denies the patient treatment that could modify the natural history of allergy.
A significant role for omalizumab has been shown in patients carrying a high risk of systemic reactions to AIT. In children with severe allergic asthma (considered to be at the highest risk), omalizumab pretreatment and subcutaneous AIT led to good safety and tolerability.63 Casale et al reported a fivefold decrease in anaphylaxis risk associated with a rush schedule of subcutaneous AIT in 159 patients with allergic rhinitis caused by ragweed pollen.64 An identical outcome was achieved in 248 patients with allergic asthma randomized to treatment with omalizumab or placebo. Omalizumab-treated patients had significantly fewer systemic allergic reactions (P=0.017) to AIT than placebo-treated patients, and in 87.3% of omalizumab-treated patients, the target maintenance immunotherapy dose was reached compared with 72.1% of placebo-treated patients (P=0.004).65 In patients undergoing immunotherapy with venom from Hymenoptera species, treatment discontinuation exposes the patient to potentially fatal reactions to further stings.66
Most studies have reported the ability of omalizumab to allow treatment tolerance in patients with repeated systemic reactions,67 and in the few unsuccessful cases, it is likely that insufficient doses of omalizumab were used. A recent report showed that increasing the omalizumab dose up to 450 mg may achieve protection from systemic reactions in patients unresponsive to standard doses.68
With regard to the mechanism of action, in oral immunotherapy for food allergy (which, although not accepted in guidelines, has been used by some authors for desensitization to food allergy), one study demonstrated that supplementing treatment with omalizumab resulted in specific desensitization to the administered food, with an initial omalizumab-dependent depletion of allergen-reactive T cells and subsequent increase in allergen-specific T-regulatory cells that induced the reversal of Th2 cell-like activity.69 It is unlikely that this mechanism of action is limited to food-allergy immunotherapy supplemented with omalizumab, and may also work in other forms of immunotherapy in combination with omalizumab.
Cost-effectiveness of omalizumab
The cost-effectiveness of a medical treatment is related to the growth in gross domestic product. Normansell et al stated that “given the high cost of the drug, identification of biomarkers predictive of response is of major importance for future research”.10 In fact, the economic studies available when that meta-analysis was carried out gave contrasting results. Indeed, a study by Brown et al based on indices of health economics, such as the incremental cost-effectiveness ratio (ICER) and quality-adjusted life years (QALYs), concluded that omalizumab as add-on therapy in patients with severe persistent allergic asthma was cost-effective.70 In the same period, a different conclusion was drawn by Sullivan and Turk, who summarized the effectiveness of omalizumab in clinical trials in patients with uncontrolled severe persistent allergic asthma despite high-dose inhaled corticosteroids plus long-acting beta-agonists. They concluded that “the cost-effectiveness of omalizumab compares well with other biologic treatments for chronic illness”.71
In 2012, the Evidence Review Group from the UK National Institute of Health and Clinical Excellence stated that “the potential small gain in QALYs associated with omalizumab was not sufficient to compensate for the high treatment cost even under the most favorable scenario analyses.”72
More homogeneous outcomes were observed in subsequent studies. Norman et al undertook a systematic review involving eleven trials and 13 observational studies. The ICER for adults and adolescents was £83,822 per QALY gained, whereas the ICER for children was £78,009 per QALY gained. The major indicators of cost-effectiveness were asthma-related mortality risk, improvement in health-related QoL, and the frequent adverse effects related to use of oral corticosteroids (which are usually reduced if omalizumab is added to treatment).73
In the most recent systematic review involving 20 studies of cost-effectiveness analysis (19 of which were on omalizumab) from 2000–2018, ten studies concluded that omalizumab was cost-effective, five that omalizumab was cost-effective only in severe uncontrolled asthma, and four that it was not cost-effective.74 The comparators used to define cost-effectiveness are of critical importance. In fact, if asthma-related death is used as a parameter, the results may be considerably different in developed countries with a national health system, whereas if severe exacerbations are used as comparators, the conclusions are dissimilar.
Real-life studies have reported on the cost-effectiveness of omalizumab compared with standard-of-care (SOC) therapy in patients with severe persistent asthma.75,76 In two studies from the US, the cost-effectiveness of add-on omalizumab was compared with tiotropium and bronchial thermoplasty, respectively. In the first study, Zafari et al found that tiotropium was cost-effective compared with omalizumab and SOC therapy in patients with uncontrolled allergic asthma at a willingness-to-pay of US$50,000/QALY.77 However, the bronchodilator tiotropium is added if standard treatment cannot control asthma, but is useful as “on-top therapy” and not as an alternative to omalizumab.4 A second study by Zafari et al found that QALYs were 3.08 for SOC therapy, 3.24 for thermoplasty, and 3.26 for omalizumab. They suggested that there was a >60% chance that bronchial thermoplasty could become cost-effective compared with SOC therapy and omalizumab at a willingness to pay of US$100,000/QALY in moderate-to-severe allergic asthma, though the need for further research was underlined.78
The cost-effectiveness of omalizumab has also been evaluated for CSU, but the results must be analyzed separately from asthma data due to the marked differences between the two diseases. In particular, the cost for health systems is very much lower for urticaria than for severe asthma. In a study by Tatar et al, a Markov model with a 10-year horizon was used to approximate the costs associated with omalizumab (300 mg/every 4 weeks) and SOC therapy for 24 weeks (as mentioned in the license for the drug) in patients with CSU unresponsive to H1 antihistamines. Data from two Phase III studies were used, and concluded the possible cost-effectiveness of omalizumab.79 In a study by Kanters et al using a Markov model on patients with CSU, omalizumab was found to be more cost-effective than cyclosporine, with an incremental QALYs of 11.3. The ICER for omalizumab was €4.510 per QALY gained. When compared with SOC therapy, the incremental QALYs for omalizumab were 9.2 and the ICER was €17.502/QALY gained, thereby suggesting the cost-effectiveness of omalizumab compared with cyclosporine and SOC therapy.80 The same research team from the Erasmus University of Rotterdam undertook another Markov model-based study including in the outcome measures the productivity losses obtained from a burden-of-illness study in Dutch patients. The ICER of omalizumab vs SOC therapy was €17 502 per QALY gained, and productivity costs had important roles in the ICER value. The results of that study were used to establish omalizumab as third-line therapy in guidelines for CSU treatment in The Netherlands.81 A similar outcome was confirmed in a study conducted in the UK which showed that “with a deterministic ICER of £3,183 in the base case, omalizumab was associated with increased costs and benefits relative to SOC”. Further, in that study, the productivity index was one of the main indicators but, even considering early discontinuation in non-responders, the impact on results was not significant.82
Conclusion
After nearly two decades of use, there is robust evidence that omalizumab is efficacious and safe for the treatment of severe asthma not controlled by SOC treatment and in CSU. The optimal duration of treatment is not known in either disease. However, evidence from studies such as XPORT17 and OMADORE18 has shown that indefinite treatment is not always needed. Despite its high price, the cost-effectiveness of omalizumab has been demonstrated in severe asthma and CSU (which is associated with medical expenditure much lower than that for asthma). The literature suggests a wide range of applications of omalizumab in various disorders regardless of allergic or non-allergic pathophysiology. Potential use of omalizumab against chronic rhinosinusitis, vernal keratoconjunctivitis, eosinophilic esophagitis, and Churg–Strauss syndrome merits investigation through controlled trials.
Disclosure
The authors report no conflicts of interest in this work.
References
Presta LG, Lahr SJ, Shields RL, et al. Humanization of an antibody directed against IgE. J Immunol. 1993;151(5):2623–2632. | ||
Jardieu PM, Fick RB. IgE inhibition as a therapy for allergic disease. Int Arch Allergy Immunol. 1999;118(2–4):112–115. | ||
Milgrom H, Fick RB, Su JQ, Jq S. Treatment of allergic asthma with monoclonal anti-IgE antibody. rhuMAb-E25 Study Group. N Engl J Med. 1999;341(26):1966–1973. | ||
Global Initiative for Asthma Report, Global strategy for Asthma Management and Prevention. Available from: https://ginasthma.org/2018-gina-report-global-strategy-for-asthma-management-and-prevention/. Accessed May 13, 2018. | ||
Walker S, Monteil M, Phelan K, Lasserson TJ, Walters EH. Anti-IgE for chronic asthma in adults and children. Cochrane Database Syst Rev. 2006;19(2):CD003559. | ||
Siergiejko Z, Świebocka E, Smith N, et al. Oral corticosteroid sparing with omalizumab in severe allergic (IgE-mediated) asthma patients. Curr Med Res Opin. 2011;27(11):2223–2228. | ||
Domingo C, Moreno A, José Amengual M, Montón C, Suárez D, Pomares X. Omalizumab in the management of oral corticosteroid-dependent IGE-mediated asthma patients. Curr Med Res Opin. 2011;27(1):45–53. | ||
Barnes N, Menzies-Gow A, Mansur AH, et al. Effectiveness of omalizumab in severe allergic asthma: a retrospective UK real-world study. J Asthma. 2013;50(5):529–536. | ||
Braunstahl GJ, Chen CW, Maykut R, Georgiou P, Peachey G, Bruce J. The eXpeRience registry: the “real-world” effectiveness of omalizumab in allergic asthma. Respir Med. 2013;107(8):1141–1151. | ||
Normansell R, Walker S, Milan SJ, Walters EH, Nair P. Omalizumab for asthma in adults and children. Cochrane Database Syst Rev. 2014;1:CD003559. | ||
Cox L, Platts-Mills TA, Finegold I, et al; American Academy of Allergy, Asthma & Immunology; American College of Allergy, Asthma and Immunology. American Academy of Allergy, Asthma & Immunology/American College of Allergy, Asthma and Immunology Joint Task Force Report on omalizumab-associated anaphylaxis. J Allergy Clin Immunol. 2007;120(6):1373–1377. | ||
Yalcin AD, Bisgin A, Cetinkaya R, Yildirim M, Gorczynski RM. Clinical course and side effects of anti-IgE monoclonal antibody in patients with severe persistent asthma. Clin Lab. 2013;59(1–2):7–17. | ||
Lai T, Wang S, Xu Z. Long-term efficacy and safety of omalizumab in patients with persistent uncontrolled allergic asthma: a systematic review and meta-analysis. Sci Rep. 2015;3(5):8191. | ||
Alhossan A, Lee CS, MacDonald K, Abraham I. “Real-life” Effectiveness Studies of Omalizumab in Adult Patients with Severe Allergic Asthma: Meta-analysis. J Allergy Clin Immunol Pract. 2017;5(5):1362–1370.e2. | ||
Incorvaia C, Mauro M, Riario-Sforza GG, Frati F, Tarantini F, Caserini M. Current and future applications of the anti-IgE antibody omalizumab. Biologics. 2008;2(1):67–73. | ||
Nopp A, Johansson SG, Adédoyin J, Ankerst J, Palmqvist M, Oman H. After 6 years with Xolair; a 3-year withdrawal follow-up. Allergy. 2010;65(1):56–60. | ||
Ledford D, Busse W, Trzaskoma B, et al. A randomized multicenter study evaluating Xolair persistence of response after long-term therapy. J Allergy Clin Immunol. 2017;140(1):162–169.e2. | ||
Domingo C, Pomares X, Navarro A, et al. A step-down protocol for treatment in oral corticosteroid dependent allergic asthma patients. Br J Clin Pharmacol. 2018;84(2):339–348. | ||
Vennera MDC, Sabadell C, Picado C; Spanish Omalizumab Registry. Duration of the efficacy of omalizumab after treatment discontinuation in “real life” severe asthma. Thorax. 2018;73(8):782–784. | ||
Johansson SGO, Lilja G, Hallberg J, Nopp A. A clinical follow-up of omalizumab in routine treatment of allergic asthma monitored by CD-sens. Immun Inflamm Dis. 2018;6(3):382–391. | ||
Amat F, Tallon P, Foray AP, et al. Control of asthma by omalizumab: the role of CD4+ Foxp3+ regulatory T cells. Clin Exp Allergy. 2016;46(12):1614–1616. | ||
Palomares O, Yaman G, Azkur AK, Akkoc T, Akdis M, Akdis CA. Role of Treg in immune regulation of allergic diseases. Eur J Immunol. 2010;40(5):1232–1240. | ||
Tabatabaian F, Ledford DK. Omalizumab for severe asthma: toward personalized treatment based on biomarker profile and clinical history. J Asthma Allergy. 2018;11:53–61. | ||
Casale TB, Luskin AT, Busse W, et al. Omalizumab Effectiveness by Biomarker Status in Patients with Asthma: Evidence From PROSPERO, A Prospective Real-World Study. J Allergy Clin Immunol Pract. Epub 2018 May 22. | ||
Stokes J. Anti-IgE Treatment for disorders other than asthma. Front Med (Lausanne). 2017;21(4):152. | ||
Peterson MR, Coop CA. Long-term omalizumab use in the treatment of exercise-induced anaphylaxis. Allergy Rhinol (Providence). 2017;8(3):170–172. | ||
Asero R. Disappearance of severe oral allergy syndrome following omalizumab treatment. Eur Ann Allergy Clin Immunol. 2017;49(3):143–144. | ||
Pinto JM, Mehta N, DiTineo M, Wang J, Baroody FM, Naclerio RM. A randomized, double-blind, placebo-controlled trial of anti-IgE for chronic rhinosinusitis. Rhinology. 2010;48(3):318–324. | ||
Kaya H, Gümüş S, Uçar E, et al. Omalizumab as a steroid-sparing agent in chronic eosinophilic pneumonia. Chest. 2012;142(2):513–516. | ||
de Klerk TA, Sharma V, Arkwright PD, Biswas S. Severe vernal keratoconjunctivitis successfully treated with subcutaneous omalizumab. J AAPOS. 2013;17(3):305–306. | ||
Ozturk AB, Kocaturk E. Omalizumab in recurring larynx angioedema: a case report. Asia Pac Allergy. 2014;4(2):129–130. | ||
Yu KK, Crew AB, Messingham KA, Fairley JA, Woodley DT. Omalizumab therapy for bullous pemphigoid. J Am Acad Dermatol. 2014;71(3):468–474. | ||
Nonaka M, Sakitani E, Yoshihara T. Anti-IgE therapy to Kimura’s disease: a pilot study. Auris Nasus Larynx. 2014;41(4):384–388. | ||
Loizou D, Enav B, Komlodi-Pasztor E, et al. A pilot study of omalizumab in eosinophilic esophagitis. PLoS One. 2015;10(3):e0113483. | ||
Jachiet M, Samson M, Cottin V, et al. Anti-IgE Monoclonal Antibody (Omalizumab) in Refractory and Relapsing Eosinophilic Granulomatosis With Polyangiitis (Churg-Strauss): Data on Seventeen Patients. Arthritis Rheumatol. 2016;68(9):2274–2282. | ||
Nucera E, Basta F, Buonomo A, et al. A Case of hypocomplementemic urticarial vasculitis syndrome successfully treated with omalizumab. J Investig Allergol Clin Immunol. 2017;27(6):382–384. | ||
Snast I, Kremer N, Lapidoth M, et al. Omalizumab for the Treatment of Solar Urticaria: Case Series and Systematic Review of the Literature. J Allergy Clin Immunol Pract. 2018;6(4):1198–1204.e3. | ||
Murphy B, Duffin M, Tolland J. Aquagenic pruritus successfully treated with omalizumab. Clin Exp Dermatol. 2018;43(7):858–859. | ||
Nettis E, Di Leo E, Bisaccia M, Marasco C, Foti C, Vacca A. A favorable response to omalizumab in a patient with cheilitis granulomatosa. J Allergy Clin Immunol Pract. 2018;6(4):1425–1426. | ||
Tsetsos N, Goudakos JK, Daskalakis D, Konstantinidis I, Markou K. Monoclonal antibodies for the treatment of chronic rhinosinusitis with nasal polyposis: a systematic review. Rhinology. 2018;56(1):11–21. | ||
Saini S, Rosen KE, Hsieh HJ, et al. A randomized, placebo-controlled, dose-ranging study of single-dose omalizumab in patients with H1-antihistamine-refractory chronic idiopathic urticaria. J Allergy Clin Immunol. 2011;128(3):567–573.e1. | ||
Kaplan A, Ferrer M, Bernstein JA, et al. Timing and duration of omalizumab response in patients with chronic idiopathic/spontaneous urticaria. J Allergy Clin Immunol. 2016;137(2):474–481. | ||
Bérard F, Ferrier Le Bouëdec MC, Bouillet L, et al. Omalizumab in patients with chronic spontaneous urticaria nonresponsive to H1-antihistamine treatment: results of the phase IV open-label SUNRISE study. Br J Dermatol. Epub 2018 Jun 21. | ||
Asero R, Canonica GW, Cristaudo A, et al. Critical appraisal of the unmet needs in the treatment of chronic spontaneous urticaria with omalizumab: an Italian perspective. Curr Opin Allergy Clin Immunol. 2017;17(6):453–459. | ||
Türk M, Yılmaz İ, Bahçecioğlu SN. Treatment and retreatment with omalizumab in chronic spontaneous urticaria: Real life experience with twenty-five patients. Allergol Int. 2018;67(1):85–89. | ||
Ferrer M, Giménez-Arnau A, Saldana D, et al. Predicting chronic spontaneous urticaria symptom return after omalizumab treatment discontinuation: exploratory analysis. J Allergy Clin Immunol Pract. 2018;6(4):1191–1197.e5. | ||
Kolkhir P, André F, Church MK, Maurer M, Metz M. Potential blood biomarkers in chronic spontaneous urticaria. Clin Exp Allergy. 2017;47(1):19–36. | ||
Cugno M, Genovese G, Ferrucci S, Casazza G, Asero R, Marzano AV. IgE and D-dimer baseline levels are higher in responders than nonresponders to omalizumab in chronic spontaneous urticaria. Br J Dermatol. 2018;179(3):776–777. | ||
Ertas R, Ozyurt K, Atasoy M, Hawro T, Maurer M. The clinical response to omalizumab in chronic spontaneous urticaria patients is linked to and predicted by IgE levels and their change. Allergy. 2018;73(3):705–712. | ||
Sánchez J, Amaya E, Acevedo A, Celis A, Caraballo D, Cardona R. Prevalence of Inducible Urticaria in Patients with Chronic Spontaneous Urticaria: Associated Risk Factors. J Allergy Clin Immunol Pract. 2017;5(2):464–470. | ||
Maurer M, Metz M, Brehler R, et al. Omalizumab treatment in patients with chronic inducible urticaria: A systematic review of published evidence. J Allergy Clin Immunol. 2018;141(2):638–649. | ||
El-Qutob D. Off-Label Uses of Omalizumab. Clin Rev Allergy Immunol. 2016;50(1):84–96. | ||
Beck LA, Marcotte GV, MacGlashan D, Togias A, Saini S. Omalizumab-induced reductions in mast cell Fce psilon RI expression and function. J Allergy Clin Immunol. 2004;114(3):527–530. | ||
MacGlashan DW, Savage JH, Wood RA, Saini SS. Suppression of the basophil response to allergen during treatment with omalizumab is dependent on 2 competing factors. J Allergy Clin Immunol. 2012;130(5):1130–1135.e5. | ||
Chang TW, Chen C, Lin CJ, Metz M, Church MK, Maurer M. The potential pharmacologic mechanisms of omalizumab in patients with chronic spontaneous urticaria. J Allergy Clin Immunol. 2015;135(2):337–342. | ||
Sanjuan MA, Sagar D, Kolbeck R. Role of IgE in autoimmunity. J Allergy Clin Immunol. 2016;137(6):1651–1661. | ||
Metz M, Staubach P, Bauer A, et al. Clinical efficacy of omalizumab in chronic spontaneous urticaria is associated with a reduction of FcεRI-positive cells in the skin. Theranostics. 2017;7(5):1266–1276. | ||
Garcia G, Magnan A, Chiron R, et al. A proof-of-concept, randomized, controlled trial of omalizumab in patients with severe, difficult-to-control, nonatopic asthma. Chest. 2013;144(2):411–419. | ||
Domingo C, Pomares X, Angril N, Rudi N, Amengual MJ, Mirapeix RM. Effectiveness of omalizumab in non-allergic severe asthma. J Biol Regul Homeost Agents. 2013;27(1):45–53. | ||
Bousquet J, Lockey R, Malling HJ. Allergen immunotherapy: therapeutic vaccines for allergic diseases. A WHO position paper. J Allergy Clin Immunol. 1998;102(4 Pt 1):558–562. | ||
James C, Bernstein DI. Allergen immunotherapy: an updated review of safety. Curr Opin Allergy Clin Immunol. 2017;17(1):55–59. | ||
Normansell R, Kew KM, Bridgman AL. Sublingual immunotherapy for asthma. Cochrane Database Syst Rev. 2015;8:CD011293. | ||
Lambert N, Guiddir T, Amat F, Just J. Pre-treatment by omalizumab allows allergen immunotherapy in children and young adults with severe allergic asthma. Pediatr Allergy Immunol. 2014;25(8):829–832. | ||
Casale TB, Busse WW, Kline JN, et al; Immune Tolerance Network Group. Omalizumab pretreatment decreases acute reactions after rush immunotherapy for ragweed-induced seasonal allergic rhinitis. J Allergy Clin Immunol. 2006;117(1):134–140. | ||
Massanari M, Nelson H, Casale T, et al. Effect of pretreatment with omalizumab on the tolerability of specific immunotherapy in allergic asthma. J Allergy Clin Immunol. 2010;125(2):383–389. | ||
Dantzer JA, Wood RA. The use of omalizumab in allergen immunotherapy. Clin Exp Allergy. 2018;48(3):232–240. | ||
Incorvaia C, Mauro M, Gritti BL, Makri E, Ridolo E. Venom immunotherapy in patients with allergic reactions to insect stings. Expert Rev Clin Immunol. 2018;14(1):53–59. | ||
Boni E, Incorvaia C, Mauro M. Dose-dependence of protection from systemic reactions to venom immunotherapy by omalizumab. Clin Mol Allergy. 2016;14:14. | ||
Abdel-Gadir A, Schneider L, Casini A, et al. Oral immunotherapy with omalizumab reverses the Th2 cell-like programme of regulatory T cells and restores their function. Clin Exp Allergy. 2018;48(7):825–836. | ||
Brown R, Turk F, Dale P, Bousquet J. Cost-effectiveness of omalizumab in patients with severe persistent allergic asthma. Allergy. 2007;62(2):149–153. | ||
Sullivan SD, Turk F. An evaluation of the cost-effectiveness of omalizumab for the treatment of severe allergic asthma. Allergy. 2008;63(6):670–684. | ||
Burch J, Griffin S, McKenna C, et al. Omalizumab for the treatment of severe persistent allergic asthma in children aged 6-11 years: a NICE single technology appraisal. Pharmacoeconomics. 2012;30(11):991–1004. | ||
Norman G, Faria R, Paton F, et al. Omalizumab for the treatment of severe persistent allergic asthma: a systematic review and economic evaluation. Health Technol Assess. 2013;17(52):1–342. | ||
McQueen RB, Sheehan DN, Whittington MD, van Boven JFM, Campbell JD. Cost-Effectiveness of Biological Asthma treatments: a systematic review and recommendations for future economic evaluations. Pharmacoeconomics. 2018;31(1):96–108. | ||
Vennera Mdel C, Valero A, Uría E, Forné C, Picado C. Cost-effectiveness analysis of omalizumab for the treatment of severe persistent asthma in real clinical practice in Spain. Clin Drug Investig. 2016;36(7):567–578. | ||
Suzuki C, Lopes da Silva N, Kumar P, Pathak P, Ong SH. Cost-effectiveness of omalizumab add-on to standard-of-care therapy in patients with uncontrolled severe allergic asthma in a Brazilian healthcare setting. J Med Econ. 2017;20(8):832–839. | ||
Zafari Z, Sadatsafavi M, Mark FitzGerald J; Canadian Respiratory Research Network. Canadian Respiratory Research Network. Cost-effectiveness of tiotropium versus omalizumab for uncontrolled allergic asthma in US. Cost Eff Resour Alloc. 2018;30:16–3. | ||
Zafari Z, Sadatsafavi M, Marra CA, Chen W, FitzGerald JM. Cost-Effectiveness of bronchial thermoplasty, omalizumab, and standard therapy for moderate-to-severe allergic asthma. PLoS One. 2016;11(1):e0146003. | ||
Tatar M, Sezen S, Senturk A, Balp MM, Saylan M, Keskinaslan A. Cost-effectiveness of omalizumab in chronic idiopathic urticarial refractory to H1-antihistamines in Turkey. Value Health. 2014;17(7):A604. | ||
Kanters TA, Gertsen K, Hakkaart L. Cost-effectiveness of omalizumab ìn chronic spontaneous urticaria In The Netherlands. Value Health. 2015;18(7):A423. | ||
Kanters TA, Thio HB, Hakkaart L. Cost-effectiveness of omalizumab for the treatment of chronic spontaneous urticaria. Br J Dermatol. 2018;179(3):702–708. | ||
Graham J, McBride D, Stull D, et al. Cost utility of omalizumab compared with standard of care for the treatment of chronic spontaneous urticaria. Pharmacoeconomics. 2016;34(8):815–827. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.