")
Back to Journals » Clinical Ophthalmology » Volume 17
Twenty-Year Follow-Up of Cataract Surgery in Car-Drivers: Associations Between Subjective Visual Difficulties and Objective Visual Function
Authors Mönestam EI
Received 6 June 2023
Accepted for publication 21 August 2023
Published 29 August 2023 Volume 2023:17 Pages 2553—2561
DOI https://doi.org/10.2147/OPTH.S424536
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Eva I Mönestam
Department of Clinical Sciences/Ophthalmology, Faculty of Medicine, Umeå University, Umeå, S-901 85, Sweden
Correspondence: Eva I Mönestam, Department of Clinical Sciences/Ophthalmology, Faculty of Medicine, Umeå University, Umeå, S-901 85, Sweden, Tel +46702544508, Email [email protected]; [email protected]
Background/Aims: Driving especially at night is a visually demanding task. Long-time outcome of cataract surgery in drivers is important to study, as many patients live for decades after surgery. The purpose of this study is to longitudinally investigate visual function in active car drivers, 20 years after cataract surgery.
Methods: From a population-based, prospective, cohort of cataract surgery patients, initiated in 1997– 98, 114 of the 133 surviving patients were included. Preoperatively, postoperatively 5, 10, 15 and 20 years after surgery, the patients answered a visual function questionnaire including driving status and difficulty. Habitual visual acuity, best corrected visual acuity (BCVA), and low contrast acuity (LCVA) 10% and 2.5% were measured.
Results: The driving difficulties in daylight were almost absent after surgery and did not change over 20 years. Nighttime driving was more difficult and declined longitudinally after surgery, p=0.013, but were at 20 years still less than before cataract surgery. Patients with better BCVA experienced less difficulties driving in darkness, p=0.005. Self-reported problems with glare were significantly associated with BCVA of the better-seeing eye, LCVA 10% and LCVA 2.5% (p=0.046, p=0.033, and 0.024 respectively). Self-reported difficulties with seeing in low-contrast conditions were also significantly associated with BCVA, p=0.004.
Conclusion: Twenty years after cataract surgery, most active drivers have no or minor visual functional problems during driving in daytime. Difficulties in nighttime driving are more common and increase significantly over time. Twenty years after surgery, all current drivers had still better subjective ability to drive, compared with before surgery.
Plain Language Summary: Driving, especially at dusk and darkness, is challenging for most people, especially for drivers with cataract. Cataract surgery is known to improve overall driving performance, but few studies have reported data on long-time visual outcome in drivers. This study repeatedly examined the visual acuity and self-perceived visual difficulties in 51 current drivers from before and after cataract surgery, and at 5, 10, 15 and 20 years after surgery.
The study shows no or minor visual difficulties in daytime driving. Difficulties in nighttime driving are more pronounced and increase significantly over 20 years.
In conclusion, most active drivers still have excellent visual results 20 years after cataract surgery.
Active drivers with visual functional problems caused by cataract should be prioritized for surgery.
Keywords: cataract surgery, long-term outcome, car-drivers
Introduction
Driving is a highly challenging task, especially when driving in dusk and darkness.1,2 Typical symptoms of age-related cataract are reduced vision, disability glare, and impaired visual function in low-contrast conditions.3 Cataract surgery significantly improves several aspects of visual function in most patients, and this improvement is sustained several years after surgery, at least in eyes without comorbidity.4
Older people represent a large and increasing part of the driving public and tend to continue driving an automobile through late life.5 By 2030, one-quarter of the driving individuals are estimated to be 65 years or older.6 For elderly people, driving is an important means of travelling.7 Especially in rural areas, driving may in fact be the only alternative for transportation. As a result of cataract surgery being the most common surgical procedure worldwide,8 driving is performed by an increasing number of elderly people who had cataract surgery in one or both eyes.
Little is known about the associations between subjective visual difficulties and objective visual function in relation to car-driving, especially when long-time cataract surgery outcome is analyzed.
The purpose of the present paper was to assess driving status, self-reported driving difficulties and visual acuity (VA), 20 years after cataract surgery. The aim was also to longitudinally analyze data from preoperatively to 20 years after surgery in this subgroup of cataract surgery patients. To the best of our knowledge, no study has presented prospective, longitudinal data on cataract surgery outcomes in drivers as long as 20 years after surgery.
Materials and Methods
Participants
Data for the current analysis are derived from a prospective, longitudinal, population-based cohort study on cataract surgery outcome. All patients who had cataract surgery between June 1, 1997 and May 31, 1998, at Norrlands University Hospital in Umeå, Sweden, were prospectively registered. All cataract surgeries in the cataract population were at the time performed at the university clinic, as there were no other public and private operating eye clinics in the area. As a result of the Swedish health care policy, patients did seldom crosscounty borders. Therefore, the number of residents who had surgery in other districts was negligible. The admitting area of the hospital is a semi-rural area of northern Sweden with few buses and limited access to transportation other than by private car. Detailed study methods of this cohort, inclusion and exclusion criteria, and 5-, 10-, 15- and 20-year results have previously been published.9,10 In brief, 810 patients who had cataract surgery during a 1-years period 1997–98 were included at baseline, 133 patients of these (16%) were still alive 20 years after surgery. If the patients underwent cataract surgery on both their eyes under the study period, data from the first eye only were used.
Nineteen of 133 patients (14%) did not participate in the follow-up; 9 of 133 (7%) suffered from dementia, and 10 (7%) could not be located or were unable to participate. At the 20-year follow-up, 114 of 133 survivors (84%) participated, and 100 of 114 patients (88%) also underwent a clinical eye examination in a standardized manner.
The study followed the tenets of the Declaration of Helsinki and informed consent was obtained from all participants at the beginning of each examination. The Ethics Committee of Umeå University approved the study. As a result from the wording of the informed consent from each patient at each examination, it was not possible to share the data.
Examinations Pre- and Postoperatively, 5, 10, 15, and 20 Years After Surgery
A few weeks before surgery, the habitual or presenting VA was measured monocularly, and best corrected visual acuity (BCVA) was recorded after subjective refraction in both eyes. VA and low contrast visual acuity (LCVA) 10% and 2.5% were measured using the logarithm of the minimum angle of resolution (logMAR) ETDRS charts at a distance of 4 meters. The anterior and posterior part of the eyes were examined using biomicroscopy. Approximately 4–8 weeks postoperatively the VA tests and the eye examinations were repeated. Each postoperative follow-up examination was performed in the same manner as at baseline.
The Questionnaire
Driving habits and driving difficulty were self-reported using the VF-14 (Visual Function) questionnaire with a few additional questions known to be important for driving. The VF-14 is a widely used patent-reported outcome instrument, developed in the US, to assess activity limitations in 14 vision-specific activities performed in everyday life.11 Of the 14 vision-dependent activities addressed in the VF-14 index, 2 are directly related to driving. The specific questions analysed in this study are shown in Figure 1. The VF-14 questionnaire has been found appropriate for use also in Europe.12 The questions were answered a few weeks before surgery, 3–4 months postoperatively, and 5, 10, 15, and 20 years after surgery.
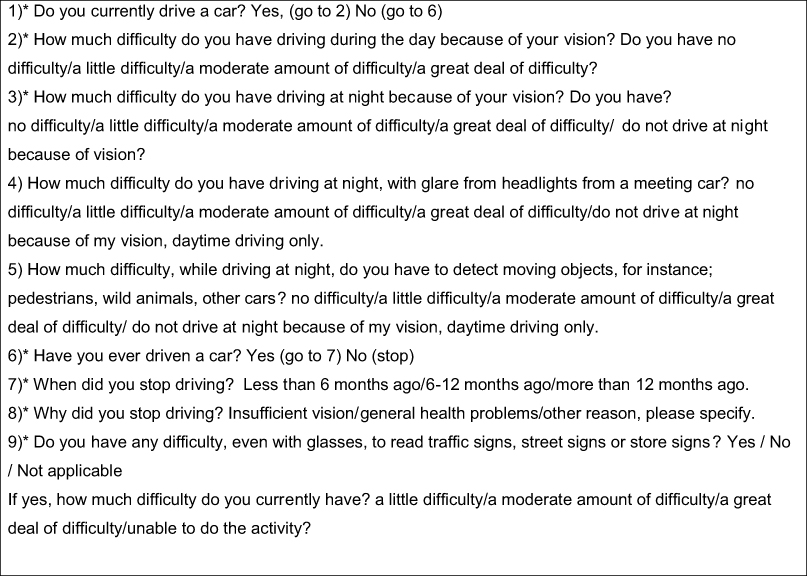 |
Figure 1 The driving-related questions analysed in the study. Questions from the Visual Function-14 questionnaire are shown with a star (*). Questions 4 and 5 are the additional driving-related questions. |
Visual Requirements for Driving
The present VA requirements for unrestricted driving in Sweden are similar to the VA standards for driving legally with a European Union license. A group I license is required for light traffic that includes personal cars. A binocular acuity, with corrective lenses, if necessary, of logMAR 0.5 (20/40) or better is required.13
Statistical Methods
Descriptive statistics for the vision variables were calculated, to examine the distributions. Independent sample t-tests were used to compare age-differences, BCVA and habitual VA for the better eye between current and former drivers.
The age-difference between current drivers, former drivers and those who never had a driving license was measured with ANOVA (analysis of variance) and post hoc Bonferroni test. ANOVA was used to control for age when analysing differences in BCVA between drivers, former drivers, and those without license.
Univariate ANOVAs were also used to assess the associations between the degree of self-reported difficulties driving at night, difficulties with glare and problems with low-contrast conditions during driving at night, and BCVA and LCVA 10% and LCVA 2.5%. The better-eye BCVA and LCVA 10% and LCVA 2.5% values were used for each patient.
Yate’s corrected chi-square tests or Fisher’s exact tests were used to assess differences in categorical variables, when appropriate. Repeated measures analysis was used to analyse the longitudinal change in nighttime driving, self-reported glare, and self-reported visual problems in low-contrast conditions.
SPSS (Statistical Package for the Social Sciences for MS Windows, software 27.0, SPSS Inc., Chicago, IL) was used for all data analyses. All tests were two-sided, and P-values <0.05 were considered statistically significant.
Results
Study Participants, Descriptive Data and Visual Acuity, 20 Years After Surgery
The study includes 114 of 133 living patients (86%), who had cataract surgery 20 years previously. Fifty-one patients of 114 (45%) reported being current drivers, 42 of 114 (37%) were former drives and 21 of 114 (18%) had never had a driving license. Table 1 shows the demographics.
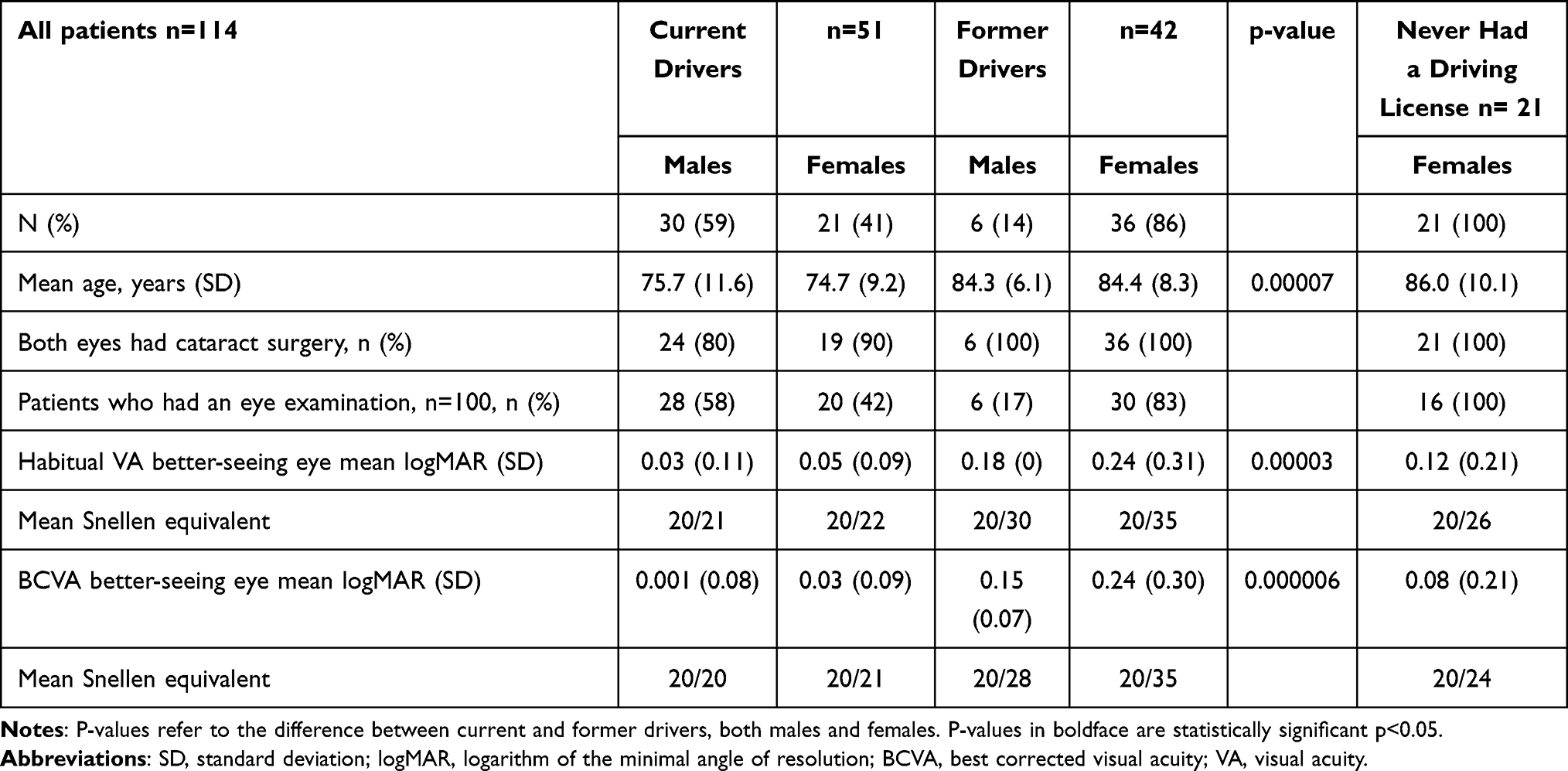 |
Table 1 Demographics and Visual Acuity of the Better-Seeing Eye by Driving Status |
The current drivers were significantly younger (p=0.00007), and significantly more often males than females compared with the former drivers, (30 of 51 (59%) vs 6 of 42 (17%)), respectively, p=0.00001, Table 1. The current drivers had a significantly better habitual VA and BCVA in their better-seeing eyes compared with the former drivers, p=0.00003 and p=0.000006, respectively, Table 1. However, after BCVA was adjusted for age, this difference was no longer significant (p=0.14).
Of the 114 patients, 105 (92%) had undergone cataract surgery in both eyes at the 20-year follow-up. Those who only had one eye operated at 20 years still had no significant cataract in the fellow eye. Of the 114 patients, 107 (91%) had an Alcon MA60BM IOL implanted, 1 IOL was unknown and 6 were Pharmacia 722A or 757 C.
There was no significant difference in YAG-frequency in any eye between the current and former drivers, 27 of 51 (53%) and 19 of 36 (53%), respectively, p=0.99.
Daytime Driving
The majority of current drivers, 50 of 51 (98%) reported no difficulty in daytime driving after 20 years. Only one of the current drivers stated minor problems with distance perception.
Figure 2 shows the longitudinal change over 20 years, in self-reported difficulties with daytime driving, in the 51 patients who remained driving 20 years after surgery. Cataract surgery has a significant impact on the mean perceived difficulties in daytime driving, which were moderate before surgery, reached a very low level postoperatively without any tendency to decline over 20 years postoperatively, Figure 2.
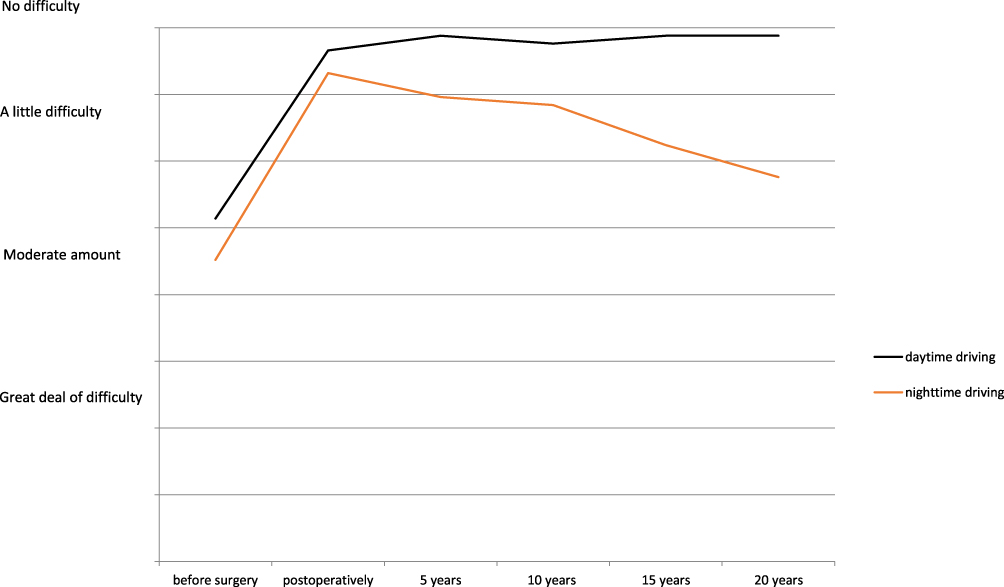 |
Figure 2 Longitudinal change in self-reported difficulties with daytime and nighttime driving, from before cataract surgery to 20 years after surgery, respectively. Mean score, 51 drivers. |
Nighttime Driving
Figure 2 also shows the longitudinal change over 20 years in mean score of self-reported difficulties driving at night. There is a significant longitudinal decline from a few months postoperatively to 20 years after surgery, p=0.013. There was no significant difference between males and females, p=0.41. The self-reported difficulties with nighttime driving at 20 years after surgery, were however still less than before cataract surgery.
Glare and Low Contrast Vision
Twenty years after cataract surgery, 7 of 51 active drivers (14%) never drove at night, only during daytime. Of 44 current nighttime drivers, 20 (45%) reported they had no difficulties with glare from meeting cars headlights, 22 (50%) had minor difficulties and 2 (5%) had a moderate amount of difficulty.
At 20 years after cataract surgery, 30 drivers of 44 (68%) did not experience any difficulties in seeing for instance, pedestrians, animals, or other cars, in low contrast conditions during nighttime driving, and 14 (32%) stated minor difficulties.
There was an increasing tendency to report difficulties with glare and low contrast vision at nighttime driving from 5 to 20 years after surgery, and these trends were however not significant, p=0.53 and p=0.86, respectively, Figure 3.
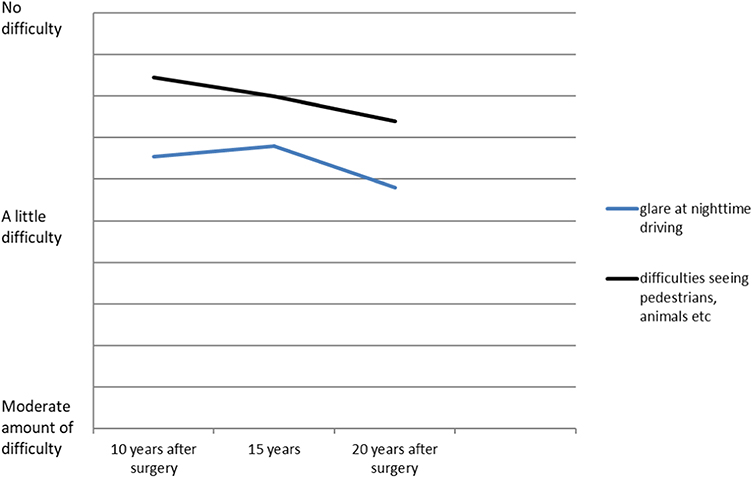 |
Figure 3 Longitudinal change in self-reported difficulties with glare and detection of low-contrast objects when driving at night, from 5 to 20 years after surgery. Mean score, 44 current nighttime drivers. |
Self-Reported Visual Difficulties with Driving in Relation to BCVA, and Low-Contrast Acuity, 20 Years After Surgery
There was a statistically significant association with self-reported difficulties driving at night and BCVA in the better-seeing eye, p=0.005. Patients with better BCVA reported less difficulties. The corresponding p-values for LCVA 10% and LCVA 2.5% did not reach statistical significance, p= 0.097 and p=0.25, respectively.
Self-reported problems with glare were significantly associated with BCVA of the better-eye, LCVA 10% and LCVA 2.5% (p=0.046, p=0.033, and p=0.024, respectively).
Self-reported difficulties with seeing pedestrians, etc, in low-contrast conditions were also significantly associated with BCVA (p=0.004) but not with LCVA 10% and LCVA 2.5% (p=0.14 and p=0.16, respectively).
Non-Drivers and Reasons Being a Former Driver
All non-drivers who never had a driving license were females, and were significantly older than the current drivers, p=0.0001, Table 1. The current drivers had a better habitual VA and BCVA compared with patients without driving license, but this difference was not significant, p=0.58.
A patient might have several reasons for stop driving, Figure 4. The most common reason was “feeling too old/other medical problems” (n=23/42; 55%) followed by “no need for a car” (n=16/42; 38%). Only 10 patents of 42 (24%) reported vision problems as a reason; of these, 7 patients stated visual impairment as the only reason for having stopped driving (7/42; 17%). Five of them did not fulfil the visual requirements for driving and the cause was for all these patients age-related macular degeneration. Two patients had a BCVA above the visual requirements for driving, but impairment of the visual fields caused by glaucoma and stroke, respectively.
 |
Figure 4 The most common reasons being a former driver. |
Fulfilment of the Visual Requirements for Driving
Twenty years after cataract surgery two current drivers (2/51; 4%) did not fulfil the visual requirements for car driving with their habitual glasses. They had only one and two letters loss to fulfil the requirements, respectively, ie, the habitual VA was 20/44 (logMAR 0.34) and 20/42 (logMAR 0.32), in their better seeing eyes. After refraction and new glasses their VA improved to 20/28 (logMAR 0.14) and 20/32 (logMAR 0.2), respectively, ie, well above the requirements of Sweden (logMAR 0.3 (20/40) or better binocularly).
Discussion
Driving requires effective coordination of visual, motor and cognitive skills.14 Older adults face a number of challenges associated with natural aging.15 Vision problems such as inability to spot objects in darkness, rain or being dazzled by oncoming headlights may be experienced by people with clinically healthy eyes.1 Even with normal BCVA, almost all self-reported and clinical measures of visual function decline with ageing, including for instance glare recovery time, and LCVA with and without glare. An important reason for this is increased intraocular light scattering.14 There is consistent evidence that cataract negatively affects driving, and that cataract surgery improves overall driving performance and reduces crash risk.16–18 In the present study, 20 years after cataract surgery, the majority of active drivers have good vision and no self-reported driving difficulty during daytime.
It is well known that especially nighttime driving is difficult for older individuals. Visual skills are pushed to their limit at night by decreased illumination, by disability glare and scattered light from oncoming headlights.14 The present study found a significant, longitudinal decline, over 20 years after cataract surgery, in self-assessed ability to drive at night, p=0.013. However, at 20 years after surgery, the self-reported difficulties with nighttime driving were less than before cataract surgery. This shows an excellent long-term effectiveness of cataract surgery, in improving visual function in this demanding activity.
Previous research has shown inconsistent results regarding the associations of BCVA as well as LCVA, and self-reported difficulties in nighttime driving, glare disability, etc.3,16 The present study found that patients with better BCVA in the better-seeing eye reported significantly less difficulties while driving at night, p= 0.005. This is in agreement with several previous studies.19,20
On the other hand, it has been reported that the measure most strongly associated with driving difficulty was contrast sensitivity.20–22 In the present study, the corresponding associations for LCVA 10% and LCVA 2.5% did not reach statistical significance, probably as a result of small sample sizes.
Twenty years after surgery, self-reported problems with glare were significantly associated with BCVA of the better seeing eye, LCVA 10% as well as LCVA 2.5%. Difficulties seeing pedestrians. etc. in low-contrast conditions were also significantly associated with BCVA. Glare sensitivity has been associated with self-reported driving difficulties,23 and predict self-restriction in driving behavior.20,24
There was an increasing tendency to report difficulties with glare and low contrast vision at nighttime driving from 5 to 20 years after surgery, these trends were however not significant, p=0.53 and p=0.86, respectively, Figure 3.
The former drivers were significantly older and more often women than the current drivers, which is consistent with previous research.19 A self-imposed, self-regulation of driving is common among elderly people, especially in women.7 This might be a result of women being inherently more cautious and thus restrict themselves more often than men.25 The present study shows as expected, that drivers were significantly younger and had better vision than non-drivers, according to previous research.2,25
Driving cessation is a process in which many older drivers gradually limit driving before giving it up entirely. In an effort to improve safety, older drivers with failing visual function may place restrictions on their driving by reducing their mileage and avoiding high-risk driving situations, such as driving in darkness and bad weather or lightning conditions.20,25 Self-regulation of driving is a positive coping strategy that enables individuals to reduce driving risk.26 The progressive reduction and cessation of driving in older drivers is not only a result of worse visual function but is at least partly related to other health problems, Figure 4.20,27 Involuntary driving cessation has however a negative impact on mobility and quality of life and associated mental health implications.26 Many urban and rural areas have poor to absent transportation infrastructure with small alternatives to car-driving, if they are present at all.
Most current drivers in the present study had at least 20/40 habitual vision in their better-seeing eye, 20 years after cataract surgery. With optimal correction, all active drivers fulfilled the visual requirements for driving in Sweden.
Strengths of the study are the high participation rate and the longitudinal design. The prospective, longitudinal design of the study reduced the risk for bias and confounding. Patients were followed and regularly examined in the same manner from before surgery to 20 years after surgery. The present study was undertaken in a sparsely populated, mostly rural area of northern Sweden, in which the public transport options were limited, causing a considerable need for car-driving in the elderly population.
There are several limitations of the study. Driving information was self-reported. As in many other population-based studies, selective participation may have biased the results, although it is likely to be small because the participation rate was high. The study was also limited by the relatively low number of drivers remaining, 20 years after cataract surgery, which is inevitable as the mean age for cataract surgery in most western countries is approximately 75 years. Information bias is defined as those who knew they had worse vision, were more likely to self-report driving difficulties and modifications because they felt it was the more socially desirable answer. This bias was minimized because the participants filled out the questionnaire before they had their vision examined.
LCVA 10% and LCVA 2.5% were used to examine low-contrast visual function. Most previous research use contrast sensitivity. As these measures examine similar visual functions, ie, vision in low-contrast conditions, it is believed that it is possible to compare findings using LCVA with previous research using contrast sensitivity.
Funding
Grants from the Västerbottens County Council Research Fund, Umeå, Sweden; the Swedish Government (“Agreement concerning Research and Education of Doctors” ALF), Ögonfonden, Gothenburg, Sweden; and Capio Medocular, Stockholm, Sweden, are acknowledged. The sponsor or funding organization had no role in the design or conduct of this research.
Disclosure
The author has no financial disclosures and no possible conflicts of interest to report.
References
1. Owsley C. Vision and aging. Annu Rev Vis Sci. 2016;2(10):255–271. doi:10.1146/annurev-vision-111815-114550
2. Rubin GS, Ng ESW, Bandeen-Roche K, Jeyl PM, Freeman EE, West SK. A prospective, population-based study of the role of visual impairment in motor vehicle crashes among older drivers: the SEE Study. Invest Ophthalmol Vis Sci. 2007;48(4):1483–1491. doi:10.1167/iovs.06-0474
3. Owsley C, Stalvey BT, Wells J, Sloane ME, McGwin G. Visual risk factors for crash involvement in older drivers with cataract. Arch Ophthalmol. 2001;119(6):881–887. doi:10.1001/archopht.119.6.881
4. Mönestam E. Long-term outcome of cataract surgery: 20-year results from a population-based prospective study. J Cataract Refract Surg. 2019;45(12):1732–1737. doi:10.1016/j.jcrs.2019.07.026
5. Foley DJ, Heimovitz HK, Guralnik JM, Brock DB. Driving life expectancy of persons aged 70 years and older in the United States. Am J Public Health. 2002;92(8):1284–1289. doi:10.2105/AJPH.92.8.1284
6. Lyman S, Ferguson SA, Braver ER, Williams AF. Older driver involvements in police reported crashes and fatal crashes: trends and projections. Inj Prev. 2002;8(2):116–120. doi:10.1136/ip.8.2.116
7. Sengupta S, van Landingham SW, Solomon SD, Do DV, Friedman DS, Ramulu PY. Driving habits in older patients with central vision loss. Ophthalmology. 2014;121(3):727–732. doi:10.1016/j.ophtha.2013.09.042
8. Kahawita SK, Goggin M. Cataract surgery audit at an Australian urban teaching hospital. Clin Exp Ophthalmol. 2015;43(6):514–522. doi:10.1111/ceo.12496
9. Mönestam E, Lundqvist B, Wachtmeister L. Visual function and car driving: longitudinal results 5 years after cataract surgery in a population. Br J Ophthalmol. 2005;89(4):459–463. doi:10.1136/bjo.2004.051151
10. Mönestam E, Lundqvist B. Extended long-term outcomes of cataract surgery. Acta Ophthalmol. 2012;90(7):651–656. doi:10.1111/j.1755-3768.2011.02138.x
11. Steinberg EP, Tielsch JM, Schein OD, et al. The VF-14. An index for functional impairment in patients with cataract. Arch Ophthalmol. 1994;112(5):630–638. doi:10.1001/archopht.1994.01090170074026
12. Alonso J, Espallargues M, Andersen TF, et al. International applicability of the VF-14; an index of visual function in patients with cataracts. Ophthalmol. 1997;104(5):799–807. doi:10.1016/S0161-6420(97)30230-9
13. Bro T, Lindblom B. Strain out a gnat and swallow a camel? – Vision and driving in the Nordic countries. Acta Ophthalmol. 2018;96(6):623–630. doi:10.1111/aos.13741
14. Mainster MA, Timberlake GT. Why HID headlights bother older drivers. Br J Ophthalmol. 2003;87(1):113–117. doi:10.1136/bjo.87.1.113
15. Lombardi DA, Horrey WJ, Courtney TK. Age-related differences in fatal intersection crashes in the United States. Accid Anal Prev. 2017;99(1):20–29. doi:10.1016/j.aap.2016.10.030
16. Agramunt S, Meuleners LB, Fraser ML, Morlet N, Chow KC, Ng JQ. Bilateral cataract, crash risk, driving performance, and self-regulation practices among older drivers. J Cataract Refract Surg. 2016;42(5):788–794. doi:10.1016/j.jcrs.2016.02.023
17. Wood JM, Carberry TP. Bilateral cataract surgery and driving performance. Br J Ophthalmol. 2006;90(7):1277–1280. doi:10.1136/bjo.2006.096057
18. Meuleners LB, Hendrie D, Lee AH, Ng JQ, Morlet N. The effectiveness of cataract surgery in reducing motor vehicle crashes: a whole population study using linked data. Ophthalmic Epidemiol. 2012;19(1):23–28. doi:10.3109/09286586.2011.628776
19. Patnaik JL, Pecen PE, Hanson K, et al. Driving and visual acuity in patients with age-related macular degeneration. Ophthalmol Retina. 2019;3(4):336–342. doi:10.1016/j.oret.2018.11.004
20. Keay L, Munoz B, Turano KA, et al. Visual and cognitive deficits predict stopping or restricted driving: the Salisbury Eye Evaluation Driving Study (SEEDS). Invest Ophthalmol Vis Sci. 2009;50(1):107–113. doi:10.1167/iovs.08-2367
21. Swain TA, McGwin G Jr, Wood JM, Antin JF, Owsley C. Naturalistic driving techniques and association of visual risk factors with at-fault crashes and near crashes by older drivers with vision impairment. JAMA Ophthalmol. 2021;139(6):639–645. doi:10.1001/jamaophthalmol.2021.0862
22. Fraser ML, Meuleners LB, Lee AH, Ng JQ, Morlet N. Which visual measures affect change in driving difficulty after first eye cataract surgery? Accid Anal Prev. 2013;58(9):10–14. doi:10.1016/j.aap.2013.04.015
23. Rubin GS, Bandeen-Roche K, Huang GH, et al. The association of multiple visual impairments with self-reported visual disability: SEE project. Inv Ophthalmol Vis Sci. 2001;42(1):64–72.
24. Freeman EE, Munoz B, Turano KA, West SK. Measures of visual function and time to driving cessation in older adults. Optom Vis Sci. 2005;82(8):765–773. doi:10.1097/01.opx.0000175008.88427.05
25. Freeman EE, Munoz B, Turano KA, West SK. Measures of visual function and their association with driving modification in older adults. Invest Ophthalmol Vis Sci. 2006;47(2):514–520. doi:10.1167/iovs.05-0934
26. Gwyther H, Holland C. The effect of age, gender and attitudes on self-regulation in driving. Accid Anal Prev. 2012;45(3):19–28. doi:10.1016/j.aap.2011.11.022
27. Freund B, Szinovacz M. Effects of cognition on driving involvement among the oldest old: variations by gender and alternative transportation options. Gerontologist. 2002;42(5):621–633. doi:10.1093/geront/42.5.621
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.