Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 15
Triple Therapy with Budesonide/Glycopyrrolate/Formoterol Fumarate Improves Inspiratory Capacity in Patients with Asthma-Chronic Obstructive Pulmonary Disease Overlap
Authors Ishiura Y ![]() , Fujimura M, Ohkura N
, Fujimura M, Ohkura N ![]() , Hara J
, Hara J ![]() , Kasahara K, Ishii N, Sawai Y, Shimizu T, Tamaki T
, Kasahara K, Ishii N, Sawai Y, Shimizu T, Tamaki T ![]() , Nomura S
, Nomura S ![]()
Received 14 September 2019
Accepted for publication 9 January 2020
Published 5 February 2020 Volume 2020:15 Pages 269—277
DOI https://doi.org/10.2147/COPD.S231004
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Richard Russell
Yoshihisa Ishiura,1,2 Masaki Fujimura,3 Noriyuki Ohkura,4 Johsuke Hara,4 Kazuo Kasahara,4 Nobuyasu Ishii,1 Yusuke Sawai,1 Toshiki Shimizu,1 Takeshi Tamaki,1 Shosaku Nomura1
1First Department of Internal Medicine, Kansai Medical University, Moriguchi, Osaka, Japan; 2Respiratory Medicine, Toyama City Hospital, Toyama, Japan; 3Respiratory Medicine, National Hospital Organization Nanao Hospital, Nanao, Japan; 4Respiratory Medicine, Kanazawa University Hospital, Kanazawa, Japan
Correspondence: Yoshihisa Ishiura
First Department of Internal Medicine, Kansai Medical University, Kansai Medical University Medical Center, 10-15 Fumizono-Cho, Moriguchi, Osaka 570-8507, Japan
Tel +81-6-6992-1001
Fax +81-6-6993-9837
Email [email protected]
Purpose: Asthma-chronic obstructive pulmonary disease overlap (ACO), characterized by airway limitation, is an important condition with high incidence and mortality. Although some guidelines recommend triple therapy with inhaled corticosteroids/long-acting muscarinic antagonists/long-acting β2 agonists, this treatment approach is based on the extrapolation of data from studies of asthma or chronic obstructive pulmonary disease (COPD) alone.
Methods: A 12-week, randomized, open-label cross-over pilot study was conducted in 19 patients with ACO to investigate the effect of triple therapy with glycopyrrolate (GLY) 50 μg/day on budesonide/formoterol fumarate (BUD/FORM) 640/18 μg/day. The study period included a 4-week wash-out, 4-week run-in, and 4-week treatment period. Respiratory function tests, fractional exhaled nitric oxide (FeNO), a COPD assessment test (CAT) and an asthma control questionnaire (ACQ) were carried out 0, 4, and 8 weeks after randomization.
Results: A total of 19 patients with stable ACO (19 males and no females) with a mean age of 70.7 ± 7.6 years (± standard deviation, SD; range 55– 83 years) participated in this study. All patients were ex-smokers with a smoking history of 63.1 ± 41.1 pack-years (± SD). Mean values for inspiratory capacity (IC), an index of hyperinflation of the lung that causes exertional dyspnea and reduced exercise, were 1.93 L (± 0.47 L) after the run-in, 1.85 L (± 0.51 L) after the BUD/FORM dual therapy period and 2.11 L (± 0.58 L) after the BUD/GLY/FORM triple therapy period. IC values after the BUD/GLY/FORM triple therapy were significantly higher than those after the run-in (p < 0.02). FeNO values, ACQ, and CAT scores were not significantly different among the run-in, wash-out, and triple-therapy periods.
Conclusion: The present pilot study showed that triple therapy with BUD/GLY/FORM results in an improvement in lung function parameters including IC, indicating the potential value of triple therapy as standard treatment for ACO.
Keywords: asthma-COPD overlap, budesonide, glycopyrrolate, formoterol fumarate, triple therapy
Plain Language Summary
Asthma-chronic obstructive pulmonary disease overlap (ACO) is important because patients with ACO have significantly worse outcomes compared with asthma or chronic obstructive pulmonary disease (COPD) alone. Triple therapy with inhaled corticosteroids/long-acting muscarinic antagonists/long-acting β2 agonists is recommend based on the extrapolation of data from studies of asthma or chronic obstructive pulmonary disease (COPD) alone, but therapeutic studies for ACO have never been conducted before. This study was conducted in patients with ACO to investigate the effect of triple therapy with glycopyrrolate (GLY) on budesonide/formoterol fumarate (BUD/FORM). Spirometry parameters including inspiratory capacity (IC), an index of hyperinflation of the lung that causes exertional dyspnea and reduced exercise, after triple therapy with BUD/GLY/FORM were significantly improved compared with the values obtained after the wash-out and run-in periods. The present pilot study showed that triple therapy with BUD/GLY/FORM results in an improvement in lung function parameters, so we can conclude that this triple therapy has the potential value as standard treatment for ACO.
Introduction
Chronic obstructive pulmonary disease (COPD), characterized by persistent and progressive airway limitation, remains a major public health problem because of its association with increased morbidity and mortality, and corresponding economic and social burden.1–3 According to the World Health Organization (WHO), an estimated 64 million people had COPD globally and more than 3 million people died of COPD, which corresponding to 5% of all deaths worldwide.4 Recently, there has been increasing interest in recognizing the phenotype within COPD, given that it a heterogeneous condition, comprising various clinical and pathophysiological components with differing responses to therapeutic interventions.5 Several phenotypes of COPD have been proposed, among which the most recognized is asthma-COPD overlap (ACO). ACO is a phenotype of COPD, characterized by a persistent airflow limitation associated with several characteristics of asthma and COPD.6–10 ACO also has become a recent focus of interest,6–10 because patients with ACO have worse health-related quality of life, more rapid disease progression,11 frequent and abrupt respiratory exacerbation,12 increased co-morbidities, and greater health-care utilization, leading to a greater socioeconomic burden than for patients with asthma or COPD alone.9,10,13,14 Previous studies showed that 53–55% of COPD patients present with an asthma-predominant phenotype.5,15 In the UPLIFT trial, nearly 66% of COPD patients improved their respiratory functions by more than 15% after receiving bronchodilator therapy.16 These studies demonstrate the high prevalence of ACO. More importantly, previous studies have demonstrated that ACO is a stronger effector of low quality of life than asthma or COPD alone.17,18 Other studies also reported that patients with ACO had more severe and frequent COPD exacerbation in the preceding year, resulting in death during follow-up (odds ratio of 3.55).12,17,18 Patients with ACO therefore utilize a large proportion of available medical resources, with a two to six times higher economic burden than that of asthma or COPD alone.13,19,20 However, few therapeutic studies for ACO have been conducted to date10 because patients with COPD are typically excluded from clinical trials for asthma, and patients with asthma have also been excluded from clinical trials for COPD.
Triple therapy with inhaled corticosteroids (ICS), long-acting muscarinic antagonists (LAMA) and long-acting β2 agonists (LABA) has become increasingly popular in clinical practice as an effective and convenient treatment for obstructive airway diseases,21,22 given the continuous need to improve symptoms and reduce the risk of exacerbation and hospitalization in this patients population.23–25 Some guidelines also recommend triple therapy with ICS/LAMA/LABA to improve lung function and respiratory symptoms and to reduce respiratory exacerbation.8,26,27 Unfortunately, this treatment approach is based on the extrapolation of data derived from studies of patients with asthma or COPD alone, as few therapeutic studies for ACO have previously been conducted.10 Moreover, previous reports have not considered inspiratory capacity (IC), an index of hyperinflation of the lung that causes exertional dyspnea and reduced exercise in chronic obstructive airway diseases.28–30 We therefore conducted the present study to compare the efficacy of ICS/LAMA/LABA triple therapy with that of ICS/LABA dual therapy in terms of hyperinflation of the lung to confirm the clinical benefit of triple therapy for ACO.
Materials and Methods
This was a 12-week, randomized, open-label cross-over pilot study to evaluate the effect of once-daily single inhalation of glycopyrrolate (GLY) 50 µg/day administered via the BreezhalerTM dry powder inhaler as add-on to budesonide/formoterol fumarate (BUD/FORM) 640/18 µg/day (160/4.5 µg two inhalations twice daily) via the TurbuhalerTM dry powder inhaler. Randomization was carried out using a sealed envelope method and patients with ACO were allocated into two groups as shown in Figure 1. This study is registered as university hospital medical information network (UMIN) 000026651 and was conducted between March 2017 and Aug 2017.
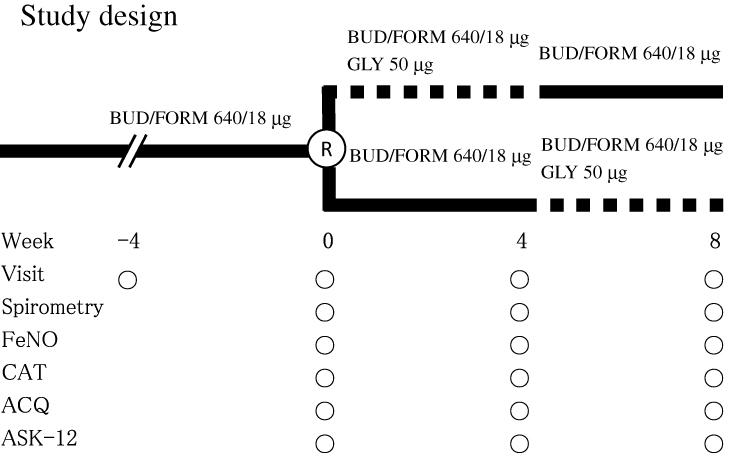 |
Figure 1 Design for the randomized, open-label cross-over study. Solid line, dual therapy with budesonide/formoterol fumarate (BUD/FORM); dotted line, triple therapy with glycopyrrolate (GLY) plus BUD/FORM. Abbreviations: ACQ, questionnaire; ASK-12, adherence status with knowledge-12; CAT, chronic obstructive pulmonary disease assessment test; FeNO, fractional exhaled nitric oxide; R, randomization. |
Subjects
Outpatients with ACO, diagnosed with ACO in accordance with previous studies,5–7,14,19 were enrolled in this study if they satisfied the following inclusion criteria: episodic respiratory symptoms and increased airflow variability (asthma: airway hyperresponsiveness [AHR] or bronchodilator response [BDR]) as well as incompletely reversible airway obstruction (COPD: post-bronchodilator forced expiratory volume in 1 s [FEV1]/forced vital capacity [FVC] <70%, and post-bronchodilator FEV1 <80% of predicted values). AHR was defined as a 20% decrease in FEV1 from baseline after inhalation of <8 mg/mL methacholine. BDR was defined as an increase in post-bronchodilator FEV1 200 mL and 12% compared with pre-bronchodilator FEV1. All patients were permitted to take bronchodilatory gents such as oral theophylline, leukotriene receptor antagonists, and mucolytic agents, as shown in Table 1.
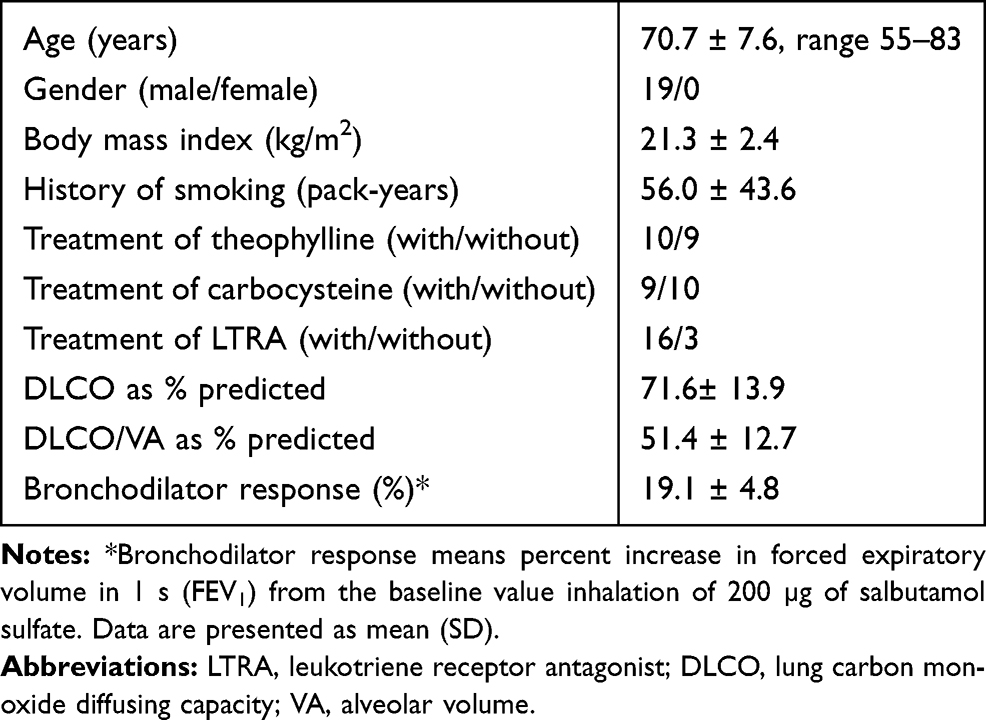 |
Table 1 Patient Characteristics |
Exclusion criteria included oral steroid therapy for at least 8 weeks prior to participation. Patients also excluded when their symptoms were moderate to severe and unstable.
A total of 19 patients with stable ACO (19 males and no females) with a mean age of 70.7 ± 7.6 years (± standard deviation, SD; range 55–83 years) participated in this pilot study. All patients were outpatients of Toyama City Hospital and ex-smokers with a smoking history of 63.1 ± 41.1 pack-years (± SD).
Study Protocol
The medication for patients with ACO was discontinued at 9.00 p.m. 2 days before starting the study to allow a washout period of at least 24 h before the measurement of respiratory functions at 10.00 a.m. on each test day. Each patient attended four visits, separated by 4 weeks, at the same time each day. Patients received BUD/FORM 640/18 µg/day for at least 4 weeks before randomization, as shown in Figure 1. Subsequently, patients were randomized into two groups and underwent treatment with GLY 50 µg/day plus BUD/FORM 640/18 µg/day, or with BUD/FORM 640/18 µg/day alone. Respiratory function was measured at 0, 4, and 8 weeks after randomization and included IC, vital capacity (VC), FVC, FEV1, FEV1/FVC, peak expiratory flow (PEF), forced expiratory flow at 25–75% (FEF25–75%), maximum expiratory flow rate at 50% forced vital capacity (MEF50), and maximum expiratory flow rate at 25% forced vital capacity (MEF25). Measurement of other parameters was also carried out at each visit and included fractional exhaled nitric oxide (FeNO), COPD assessment test (CAT) score, asthma control questionnaire (ACQ) score, adherence status with knowledge-12 (ASK-12) score, electrocardiogram, and blood examinations including peripheral blood eosinophils and immunoglobulin E (IgE).
Measurements
Respiratory functions were measured using a dry wedge spirometer (Chestac 8900TM, Chest Co., Ltd., Tokyo, Japan) to assess the bronchodilatory effect for small airway obstruction of the treatment regimens as previously reported.31–33 The FeNO level, a surrogate eosinophilic airway inflammatory marker, was measured using a commercially available device (NIOX MINOTM, Aerocrine, Stockholm, Sweden) prior to any forced expiratory maneuvers.34 To assess and quantify the effect of COPD symptoms on patient health status, patients were asked to complete a CAT, a simple questionnaire that represents a reliable and valid tool to examine the impact of COPD symptoms over time.35 The CAT comprised eight items scored from 0 to 5 to give a maximum total score of 40. CAT scores of 1–10, 11–20, 21–30, and 31–40, respectively, represent mild, moderate, severe, and very severe health status impairment.35 To evaluate asthma control status during the previous 4 weeks, patients were asked to complete an ACQ5, an easy five-question test that evaluates their asthma symptoms.36 Each question was scored from 0 to 6, giving a total score in the range of 0–30, with high scores corresponding to a high level of symptoms and therefore poor asthma control. To detect and address patient-specific barriers to medication adherence, allocated patients were asked to complete an ASK-12, a 12-item questionnaire consisting of three domains related to medication adherence: inconvenience/forgetfulness, treatment beliefs, and behavior. Responses for each item were scored from 1 to 5. Scores could range from 12 to 60, with higher scores representing greater barriers to adherence.37 All adverse events reported during the study period.
Data Analysis
Data are shown as the mean ± SD. One-way analysis of variance was used for analyzing differences between the run-in period, the BUD/FORM dual therapy period and the BUD/GLY/FORM triple therapy period in respiratory functions, FOT parameters, FeNO levels, CAT scores, ACQ scores, heart rates measured by electrocardiogram, and blood examinations including IgE. Values for IC, FEV1, and FEF25–75% were also compared pairwise between each of the run-in period, the BUD/FORM dual therapy period, and the BUD/GLY/FORM triple therapy period using paired t-tests. Values of p-value < 0.05 were considered statistically significant. All analyses were performed using StatView 4.5J software (Abacus Concepts, Berkeley, CA, USA).
Results
Respiratory function obtained by spirometry is shown in Table 2. Several parameters were significantly higher after BUD/GLY/FORM triple therapy compared with corresponding values after the run-in or BUD/FORM dual therapy periods. Changes in IC after the run-in and each treatment period are shown in Figure 2. Mean values for IC were 1.93 L (± 0.47 L) after the run-in, 1.85 L (± 0.51 L) after the BUD/FORM dual therapy period and 2.11 L (± 0.58 L) after the BUD/GLY/FORM triple therapy period. IC values after the BUD/GLY/FORM triple therapy were significantly higher than those after the run-in (p < 0.02). Changes in FEV1 after the run-in and each treatment period are shown in Figure 3. Mean values for FEV1 were 1.42 L (± 0.51 L) after the run-in, 1.41 L (± 0.48) after the BUD/FORM dual therapy period, and 1.52 L (± 0.44 L) after the BUD/GLY/FORM triple therapy period. FEV1 values after the BUD/GLY/FORM triple therapy were significantly higher than those after the run-in (p < 0.01). Changes in FEF25–75% after the run-in and each treatment period, as shown in Figure 4, were significantly higher after the BUD/GLY/FORM triple therapy period than after the run-in and the BUD/FORM dual therapy period. Mean values for FEF25–75% were 0.56 L/s (± 0.26 L/s) after the run-in, 0.51 L/s (± 0.23 L/s) after the BUD/FORM dual therapy period and 0.63 L/s (± 0.28 L/s) after the BUD/GLY/FORM triple therapy period. FEF25–75% values after the BUD/GLY/FORM triple therapy period were significantly higher than those after the run-in (p < 0.01). FeNO level, CAT score, ACT score, ASK-12 score, blood examinations (eosinophils and IgE), serum examinations for liver/renal functions and electrocardiograms were not significantly different among the run-in, BUD/FORM dual therapy period and BUD/GLY/FORM triple therapy period, as shown in Table 2. None of the patients enrolled in this study complained of cardiovascular or gastroenterological symptoms after the administration of BUD/FORM or BUD/GLY/FORM. We also observed no exacerbations and side effects in each group during study period.
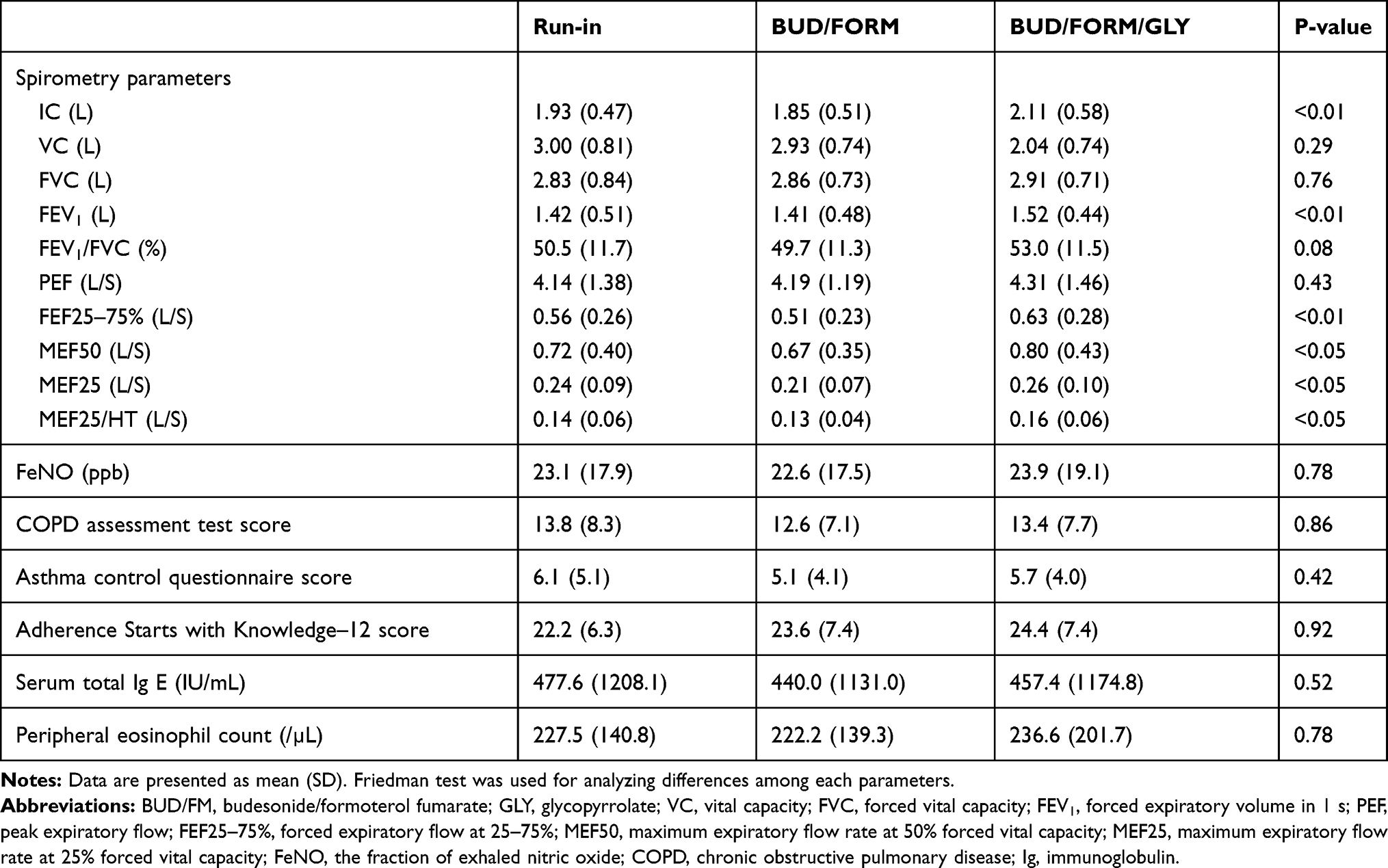 |
Table 2 Spirometry Parameters, FeNO, CAT, ACT, and Blood Examination Parameters After Each Treatment |
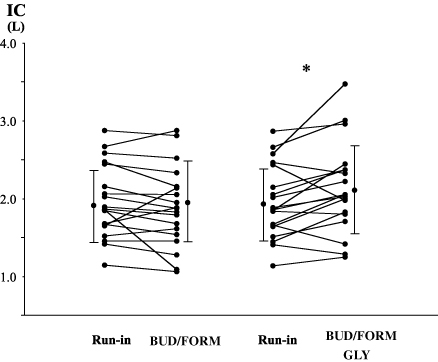 |
Figure 2 Individual data for inspiratory capacity (IC), before each treatment with BUD/FORM dual therapy and after BUD/GLY/FORM triple therapy, in patients with asthma–chronic obstructive pulmonary disease (ACO). Each panel shows the parameter changes for all patients and the mean ± SD. *p < 0.02 between treatments, determined by paired t-test. |
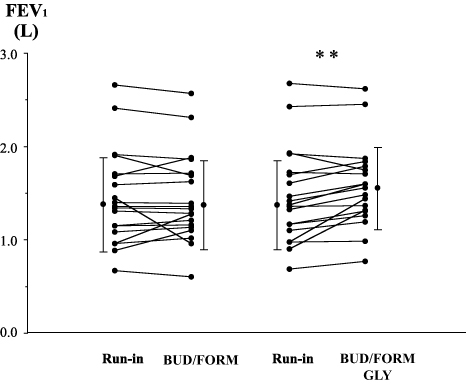 |
Figure 3 Individual data for forced expiratory volume in 1 s (FEV1), before each treatment and after dual therapy with BUD/FORM and triple therapy with BUD/GLY/FORM, in patients with ACO. Each panel shows the parameter changes for all patients and the mean ± SD. **p < 0.01 between treatments, determined by paired t-test. |
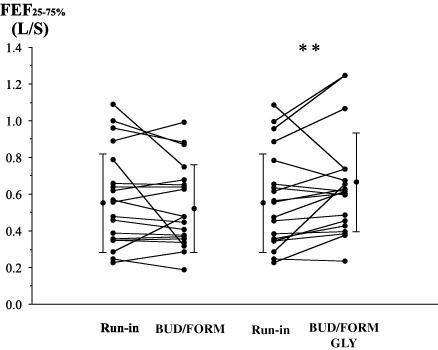 |
Figure 4 Individual data for forced expiratory flow at 25–75% (FEF25–75%), before each treatment and after dual therapy with BUD/FORM and triple therapy with BUD/GLY/FORM, in patients with ACO. Each panel shows the parameter changes for all patients and the mean ± SD. **p < 0.01 between treatments, determined by paired t-test. |
Discussion
Our results showed that 4-week treatment with BUD/GLY/FORM triple therapy improved lung function including FEV1 and IC, an index of hyperinflation of the lung, compared with BUD/FORM dual therapy. These findings indicate the potential of triple therapy with BUD/GLY/FORM to become standard treatment for ACO.
Triple therapy with ICS/LAMA/LABA has been a focus of interest because a recent real-world survey revealed that 29.6% of patients with ACO were prescribed triple therapy as a more aggressive therapy for disease associated with more symptoms and greater physician-perceived risk of exacerbation.22 Triple therapy with distinct and complementary mechanisms of action can offer improved efficacy in the treatment of COPD and asthma, which may in turn help to relieve the burden of these diseases on lung function, symptoms, daily activities, and risk of exacerbation.23–25 Triple therapy is therefore increasingly considered a useful and convenient option in patients with obstructive airway diseases.23–25 Some guidelines for ACO also recommend triple therapy to improve lung function and respiratory symptoms and to reduce respiratory exacerbation.4,12,27 This treatment approach, however, is based on data derived from studies of patients with COPD or asthma alone, as randomized clinical trials have not been conducted in patients with ACO prior to the publication of these guidelines. We previously reported the usefulness of dual therapy with ICS/LABA as a maintenance therapy for ACO,9 and subsequently conducted a study to investigate the effect of triple therapy with ICS/LAMA/LABA.10 We have also demonstrated the advantage of triple therapy in patients with ACO but did not focus on the IC, an index of inspiratory restraint resulting from hyperinflation of the lung.28,29 Hyperinflation of the lung is an important finding that causes exertional dyspnea and reduced exercise in patients with COPD.30 Decreased of lung hyperinflation has been shown to correlate with improvement in dyspnea after treatment38 and dynamic hyperinflation, such as the IC, are more closely related to exercise tolerance than FEV1.29 Tantucci and colleagues showed that IC is a powerful independent predictor of mortality from respiratory causes in patients with COPD and also represents a significant risk factor for morbidity in these patients, at least in terms of exacerbation-related hospitalization.28 Therefore, we conducted the present study and clearly showed that 4-week BUD/GLY/FORM triple therapy improved IC in patients with ACO. This result indicates the potential of triple therapy with BUD/GLY/FORM to become a standard treatment in patients with ACO.
GLY, a once-daily LAMA used as add-on therapy in this study, has been approved for the maintenance of COPD symptoms and improves both lung function and health status through inhibition of acetylcholine-mediated bronchoconstriction by binding to M3 receptors.39 Recently, accumulating evidences showed the benefits of LAMAS for the maintenance of asthma control.40 Blais et al showed the bronchoprotective effect of GLY in asthmatic patients.41 Virchow and their colleagues also showed the beneficial effect of GLY on ICS/LABA in uncontrolled asthma.42 The BUD administered in this study is an ICS retained in airway tissue for longer than other inhaled steroids, resulting in significant prolongation of the anti-inflammatory effect.43,44 Moreover, FORM is a LABA with a rapid onset of action and a duration of effect of at least 12 hrs.45 Recently, Ferguson and colleagues have shown the efficacy of triple therapy of BUD/GLY/FORM in patients with COPD.46 Other studies have also shown that triple therapy with ICS/LAMA/LABA including tiotropium, another LAMA, improves lung function and decreases asthma exacerbation.25,47 These findings provide a strong rationale for the use of BUD/GLY/FORM in patients with ACO, as an entity of overlapping asthma and COPD, to maximize clinical benefits and lung function, thereby preventing disease exacerbation.
This study had several limitations. First, although we observed statistically significant improvements in respiratory functions, these results alone cannot elucidate the etiology of the clinically beneficial effect. A potent bronchodilatory effect may be the main factor to which the results of our study are attributable since the value of FeNO did not change after the triple therapy period. However, a recent study showed the anti-inflammatory effect of LAMA.48 We therefore suggest that an examination of airway mediators may help to define this mechanism. Further studies are thus required to investigate the mechanisms of the bronchodilatory effects of triple therapy with BUD/GLY/FORM. Second, a specific, formal definition of ACO has yet to be established.7,15,19 Although multiple definitions have been proposed based on a specific inflammatory pattern,26 these definitions are not specific for asthma and COPD. For example, airway eosinophilic inflammation has been identified in only 48% of patients with asthma and 34% of those with COPD.7 We conducted the present study based on physiological lung function criteria described in previous studies.6,7,10,15,19,33 In contrast, concordance with the proportion of ACO patients in several different studies indicates the validity of the physiological lung function criteria.5,7,14,19 Further studies are required to establish better diagnostic criteria for ACO. Third, ASK-12 tended to be higher with triple treatment, but there was no statistical difference. We consider that additional inhalation instruction after GLY administration might be related to the elevation of ASK total score. Finally, pulmonary physiology outcome measures confirmed the bronchodilatory effects of triple therapy with effect of LAMAs, but CAT scores and ACQ scores did not show benefits with respect to health-care outcomes despite the improvement in IC. The number of enrolled patients in our study may have been insufficient to detect difference in symptom scores, because this study was conducted as a pilot study without power calculation. A larger study may therefore be required to clarify the benefits of ICS/LAMA/LABA triple therapy with respect to health-care outcomes.
Conclusions
In conclusion, 4-week treatment of ACO patients with BUD/GLY/FORM triple therapy resulted in a significant improvement from baseline in lung function, including IC, compared with BUD/FORM dual therapy, and with a comparable safety profile. These findings support the potential for triple therapy with BUD/GLY/FORM to become a standard treatment for ACO. Further studies are required to confirm the beneficial effect of other ICS/LAMA/LABA combination and, more interestingly, to define the precise etiology of the clinical efficacy of these combinations.
Abbreviations
ACO, asthma-COPD overlap; ACQ, asthma control questionnaire; AHR, airway hyperresponsiveness; ASK-12, scores adherence status with knowledge-12; BDR, bronchodilator response; BUD, budesonide; CAT, COPD assessment test; COPD, chronic obstructive pulmonary disease; FEF25–75%, forced expiratory flow at 25–75%; FeNO, fractional exhaled nitric oxide; FEV1, forced expiratory volume in 1 s; FORM, formoterol fumarate; FVC, forced vital capacity; GLY, glycopyrrolate; IC, inspiratory capacity; ICS, inhaled corticosteroid; IgE, immunoglobulin E; LABA, long-acting β2 agonist; LAMA, long-acting muscarinic antagonist; MEF25, maximum expiratory flow rate at 25% forced vital capacity; MEF50, maximum expiratory flow rate at 50% forced vital capacity; PEF, peak expiratory flow; SD, standard deviation; UMIN, university hospital medical information network; VC, vital capacity; WHO, World Health Organization.
Ethics Approval and Informed Consent
The study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Ethics Committee of Toyama City Hospital (approval no. UMIN000026651). Written informed consent was obtained from all patients prior to participation.
Data Sharing Statement
The clinical study data used to support the findings of this study are available from the corresponding author upon request.
Acknowledgment
We thank Clare Cox, PhD, from Edanz Group for editing a draft of this manuscript.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Lopez AD, Shibuya K, Rao C, et al. Chronic obstructive pulmonary disease: current burden and future projections. Eur Respir J. 2006;27:397–412. doi:10.1183/09031936.06.00025805
2. Pauwels RA, Buist AS, Calverley PM, Jenkins CR, Hurd SS; GOLD Scientific Committee. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) workshop summary. Am J Respir Crit Care Med. 2001;163:1256–1276. doi:10.1164/ajrccm.163.5.2101039
3. Mathers CD, Loncar D. Projection of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006;3:e442. doi:10.1371/journal.pmed.0030442
4. WHO. Chronic Obstructive Pulmonary Disease Phenotypes (COPD). Burden of COPD. WHO; 2019. Available from: https://www.who.int/respiratory/copd/burden/en/.
5. Marsh SE, Travers J, Weatherall M, et al. Proportional classification of COPD phenotypes. Thorax. 2008;63:761–767. doi:10.1136/thx.2007.089193
6. Gibson PG, Simpson JL. The overlap syndrome of asthma and COPD: what are its features and how important is it? Thorax. 2009;64:728–735. doi:10.1136/thx.2008.108027
7. Fu JJ, Gibson PG, Simpson JL, McDonald VM. Longitudinal changes in clinical outcomes in older patients with asthma, COPD and asthma-COPD overlap syndrome. Respiration. 2014;87:63–74. doi:10.1159/000352053
8. Global Initiative for Asthma [webpage on the Internet]. 2018 GINA Report, Global Strategy for Asthma Management and Prevention. GINA; 2018. Available from: https://ginasthma.org.
9. Ishiura Y, Fujimura M, Shiba Y, Ohkura N, Hara J, Kasahara K. A comparison of the efficacy of once-daily fluticasone furoate/vilanterole with twice-daily fluticasone propionate/salmeterol in asthma-COPD overlap syndrome. Pulm Pharmacol Ther. 2015;35:28–33. doi:10.1016/j.pupt.2015.10.005
10. Ishiura Y, Fujimura M, Ohkura N, et al. Effect of triple therapy in patients with asthma-COPD overlap. Int J Clin Pharmacol Ther. 2019;57(8):384–392. doi:10.5414/CP203382
11. Lange P, Parner J, Vestbo J, Schnohr P, Jensen G. A 15-year follow-up study of ventilatory function in adults with asthma. N Engl J Med. 1998;339:1194–1200. doi:10.1056/NEJM199810223391703
12. Hardin M, Silverman EK, Barr RG, et al. The clinical features of the overlap between COPD and asthma. Respir Res. 2011;12:127. doi:10.1186/1465-9921-12-127
13. Shaya FT, Dongyi D, Akazawa MO, et al. Burden of concomitant asthma and COPD in a medicaid population. Chest. 2008;134(1):14–19. doi:10.1378/chest.07-2317
14. Soriano JB, Visick GT, Muellerova H, Payvandi N, Hansell AL. Patterns of comorbidities in newly diagnosed COPD and asthma in primary care. Chest. 2005;128:2099–2107. doi:10.1378/chest.128.4.2099
15. Fu JJ, McDonald VM, Gibson PG, Simpson JL. Systemic inflammation in older adults with asthma-COPD overlap syndrome. Allergy Asthma Immunol Res. 2014;6:316–324. doi:10.4168/aair.2014.6.4.316
16. Tashkin DP, Celli B, Senn S, et al.; UPLIFT Study Investigators. Bronchodilator responsiveness in patients with COPD. Eur Respir J. 2008;31:742–750. doi:10.1183/09031936.00129607
17. Diaz-Guzman E, Khosravi M, Mannino DM. Asthma, chronic obstructive pulmonary disease, and mortality in the U.S. population. COPD. 2011;8(6):400–407. doi:10.3109/15412555.2011.611200
18. Kauppi P, Kupiainen H, Lindqvist A, et al. Overlap syndrome of asthma and COPD predicts low quality of life. J Asthma. 2011;48(3):279–285. doi:10.3109/02770903.2011.555576
19. McDonald VM, Higgins I, Gibson PG. Managing older peoples with coexistent asthma and chronic obstructive lung disease; diagnostic and therapeutic challenge. Drugs Aging. 2013;30:1–17. doi:10.1007/s40266-012-0042-z
20. Zeki AA, Schivo M, Chan A, Albertson TE, Louie S. The asthma-COPD overlap syndrome: a common clinical problem in the elderly. J Allergy (Cairo). 2011;861926. doi:10.1155/2011/861926
21. Vanfleteren L, Fabbri LM, Papi A, Petruzzelli S, Celli B. Triple therapy (ICS/LABA/LAMA) in COPD: time for a reappraisal. Int J COPD. 2018;13:3971–3981. doi:10.2147/COPD.S185975
22. Ding B, Small M. Treatment trends in patients with asthma-COPD overlap syndrome in a COPD cohort: findings from a real world survey. Int J COPD. 2017;12:1753–1763. doi:10.2147/COPD.S136314
23. Ismaila AS, Birk R, Shah D, et al. Once-daily triple therapy in patients with advanced COPD: healthcare resource utilization data and associated costs from the FULFIL trial. Adv Ther. 2017;34(9):2163–2172. doi:10.1007/s12325-017-0604-x
24. Lipson DA, Barnhart F, Brealey N, et al. Once-daily single-inhaler triple versus dual therapy in patients with COPD. N Engl J Med. 2018;378(18):1671–1680. doi:10.1056/NEJMoa1713901
25. Peters SP. Tiotropium bromide triple combination therapy improves lung function and decreases asthma exacerbations. Evid Based Med. 2013;18(5):179. doi:10.1136/eb-2012-101100
26. Miravitlles M, Soler-Cataluña JJ, Calle M, et al. Spanish guideline for COPD (GesEPOC). Update 2014. Arch Bronconeumol. 2014;50(Suppl 1):1–16. doi:10.1016/S0300-2896(14)70070-5
27. Japanese Respiratory Society[The JRS Guidelines for the Management of ACO 2018]. Medical Review. Tokyo; 2018. in Japanese.
28. Tantucci C, Donati P, Nicosia F, et al. Inspiratory capacity predicts mortality in patients with chronic obstructive pulmonary disease. Respir Med. 2008;102(4):613–619. doi:10.1016/j.rmed.2007.11.004
29. Diaz O, Villafranca C, Ghezzo H, et al. Role of inspiratory capacity on exercise tolerance in COPD patients with and without tidal expiratory flow limitation at rest. Eur Respir J. 2000;16(2):269–275. doi:10.1034/j.1399-3003.2000.16b14.x
30. O’Donnell DE, Revill SM, Webb KA. Dynamic hyperinflation and exercise intolerance in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2001;164(5):770–777. doi:10.1164/ajrccm.164.5.2012122
31. Ishiura Y, Fujimura M, Yamamoto H, Ishiguro T, Ohkura N, Myou S. COX-2 inhibition attenuates cough reflex sensitivity to inhaled capsaicin in patients with asthma. J Investig Allergol Clin Immunol. 2009;19:370–374.
32. Ishiura Y, Fujimura M, Yamamoto H, Ohkura N, Myou S. Role of COX-2 in cough reflex sensitivity to inhaled capsaicin in patients with sinobronchial syndrome. Cough. 2010;6:7. doi:10.1186/1745-9974-6-7
33. Ishiura Y, Fujimura M, Shiba Y, et al. A comparison of the efficacy of once-daily fluticasone furoate/vilanterole with twice-daily fluticasone propionate/salmeterol in elderly asthmatics. Drug Res (Stuttg). 2018;68(1):38–44. doi:10.1055/s-0043-118536
34. Alving K, Janson C, Nordvall L. Performance of a new hand-held device for exhaled nitric oxide measurement in adults and children. Respir Res. 2006;7:67. doi:10.1186/1465-9921-7-67
35. Mackay AJ, Donaldson GC, Patel AR, Jones PW, Hurst JR, Wedzicha JA. Usefulness of the chronic obstructive pulmonary disease assessment test to evaluate severity of COPD exacerbations. Am J Respir Crit Care Med. 2012;185:1218–1224. doi:10.1164/rccm.201110-1843OC
36. Werner CU, Linde K, Schäffner J, Storr C, Schneider A. Weekly self-measurement of FEV1 and PEF and its impact on ACQ (asthma control questionnaire)-scores: 12-week observational study with 76 patients. NPJ Prim Care Respir Med. 2017;27(1):64. doi:10.1038/s41533-017-0064-4
37. Matza LS, Park J, Coyne KS, Skinner EP, Malley KG, Wolever RQ. Derivation and validation of the ASK-12 adherence barrier survey. Ann Pharmacother. 2009;43(10):1621–1630. doi:10.1345/aph.1M174
38. Belman MJ, Botnick WC, Shin JW. Inhaled bronchodilators reduce dynamic hyperinflation during exercise in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1996;153(3):967–975. doi:10.1164/ajrccm.153.3.8630581
39. D’Urzo A, Kerwin E, Overend T, D’Andrea P, Chen H, Goyal P. Once daily glycopyrronium for the treatment of COPD: pooled analysis of the GLOW1 and GLOW2 studies. Curr Med Res Opin. 2014;30(3):493–508. doi:10.1185/03007995.2013.858618
40. Price D, Fromer L, Kaplan A, van der Molen T, Román-Rodríguez M. Is there a rationale and role for long-acting anticholinergic bronchodilators in asthma? NPJ Prim Care Respir Med. 2014;24(1):14023. doi:10.1038/npjpcrm.2014.23
41. Blais CM, Davis BE, Cockcroft DW. The effect of glycopyrronium and indacaterol, as monotherapy and in combination, on the methacholine dose-response curve of mild asthmatics: a randomized three-way crossover study. Respir Res. 2017;18(1):146. doi:10.1186/s12931-017-0628-4
42. Virchow JC, Kuna P, Paggiaro P, et al. Single inhaler extrafine triple therapy in uncontrolled asthma (TRIMARAN and TRIGGER): two double-blind, parallel-group, randomised, controlled Phase 3 trials. Lancet. 2019;394(10210):1737–1749. doi:10.1016/S0140-6736(19)32215-9
43. Mapel DW, Roberts MH. Management of asthma and chronic obstructive pulmonary disease with combination inhaled corticosteroids and long-acting β-agonists: a review of comparative effectiveness research. Drugs. 2014;74(7):737–755. doi:10.1007/s40265-014-0214-8
44. Hozawa S, Terada M, Haruta Y, Hozawa M. Comparison of early effects of budesonide/formoterol maintenance and reliever therapy with fluticasone furoate/vilanterol for asthma patients requiring step-up from inhaled corticosteroid monotherapy. Pulm Pharmacol Ther. 2016;37:15–23. doi:10.1016/j.pupt.2016.01.005
45. Price D, Dutchman D, Mawson A, Bodalia B, Duggan S, Todd P. FLOW (formoterol in the management of mild asthma–formoterol Turbuhaler with budesonide Turbuhaler) research group. Early asthma control and maintenance with formoterol following reduction of inhaled corticosteroid dose. Thorax. 2002;57(9):791–798. doi:10.1136/thorax.57.9.791
46. Ferguson GT, Rabe KF, Martinez FJ, et al. Triple therapy with budesonide/glycopyrrolate/formoterol fumarate with co-suspension delivery technology versus dual therapies in chronic obstructive pulmonary disease (KRONOS): a double-blind, parallel-group, multicentre, phase 3 randomised controlled trial. Lancet Respir Med. 2018;6(10):747–758. doi:10.1016/S2213-2600(18)30327-8
47. Barnes PJ. Triple inhalers for obstructive airways disease: will they be useful? Expert Rev Respir Med. 2011;5(3):297–300. doi:10.1586/ers.11.26
48. Benfante A, Braido F, Scichilone N. The anti-inflammatory properties of tiotropium. Lancet Respir Med. 2018;6(8):e37. doi:10.1016/S2213-2600(18)30190-5
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.