Back to Journals » Journal of Pain Research » Volume 19
Trigeminal Nerve Blocks for Medically Intractable Painful Trigeminal Neuropathy
Received 4 November 2025
Accepted for publication 14 March 2026
Published 23 March 2026 Volume 2026:19 574753
DOI https://doi.org/10.2147/JPR.S574753
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor King Hei Stanley Lam
You-Chia Chen,1,2 Hsinlin Thomas Cheng2
1Department of Neurology, Cathay General Hospital, Taipei, Taiwan, Republic of China; 2Department of Neurology, Mass General Brigham, Harvard Medical School, Boston, MA, USA
Correspondence: Hsinlin Thomas Cheng, Department of Neurology, Mass General Brigham, Harvard Medical School, WACC835, 15 Parkman Street, Boston, MA, 02114, USA, Tel +1 617 726 0240, Fax +1 617 726-6991, Email [email protected]
Introduction: Painful trigeminal neuropathy (PTN) is a debilitating condition with persistent facial pain after a trigeminal nerve injury. It could be refractory to medication treatments and causes significant physical discomfort and psychological stress that significantly affects quality of life. This study aims to demonstrate the efficacy of trigeminal nerve blocks (TNB) for patients with PTN and to identify the parameters that affect treatment outcomes.
Methods: In this retrospective chart review, we examined the medical records of 90 PTN patients who received trigeminal nerve blocks at Mass General Hospital (MGH) between March 2023 and March 2025. The trigeminal nerve blocks were performed using a variety of combinations of local anesthetics, from 2% lidocaine, 2% lidocaine plus 0.5% ropivacaine, to 4% lidocaine with 0.75% Bupivacaine. Triamcinolone was co-administered if no contraindication, including uncontrolled diabetes, hypertension, active infections, or psychological illness, existed.
Results: The mean age was 50.6 years, and 71.1% of the participants were female. Seventy-three patients (81.1%) achieved ≥ 50% pain reduction. The duration of relief was: ≥ 6 weeks in 45 patients (50.0%), ≥ 8 weeks in 33 patients (36.7%), and ≥ 12 weeks in 21 patients (23.3%). Among the 33 patients with ≥ 8 weeks of relief, the effective regimens were: 2% lidocaine + triamcinolone (n=4, 12.1%), 2% lidocaine + 0.5% ropivacaine + triamcinolone (n=10, 30.3%), and 4% lidocaine + 0.75% bupivacaine + triamcinolone (n=13, 39.4%). The poor prognostic factors for treatment effects lasting shorter than 8 weeks include depression, involvement of the maxillary nerve (V2), and symptoms of facial numbness.
Conclusion: The current study suggests that TNB with local anesthetics and steroids may be associated with better outcomes in patients with painful trigeminal neuropathy, based on this retrospective analysis.
Keywords: facial pain, local anesthetics, triamcinolone, nerve injury, trigeminal neuropathy
Introduction
Painful trigeminal neuropathy (PTN) is a chronic, debilitating neuropathic facial pain associated with a condition indicative of neural damage. The pain is frequently described as excruciating, squeezing, burning, or pins-and-needles, with or without intermittent sharp pain over one or more territories of the trigeminal nerve branches. Unlike trigeminal neuralgia, with paroxysmal pain with a silent period between attacks, the symptoms of PTN are continuous or nearly continuous, with less frequent paroxysmal stabbing pain.1,2 In contrast to trigeminal neuralgia, which is frequently associated with vascular contacts on the cisternal trigeminal roots, PTN is primarily caused by peripheral injuries to the trigeminal nerve.3 Unfortunately, many patients with PTN are misdiagnosed as having trigeminal neuralgia and receive unsuccessful medication and unnecessary surgical treatments.
The common causes of PTN includes direct nerve injuries from dental procedures (such as endodontic therapies, dental implants, local anesthesia injections, or tooth extraction), mechanical facial trauma, nasosinus surgeries, cosmetic or orthognathic surgeries, nerve inflammation from the contiguous tissues infection (such as paranasal sinusitis, pulpitis, or temporomandibular arthritis), viral infection [herpes zoster, coronavirus 2019 (COVID-19)], autoimmune diseases, tumor, or idiopathic neuropathy from unclear etiology.2,4
The pharmacotherapeutic treatment for PTN is similar to treating other types of neuropathic pain, postherpetic neuralgia, or trigeminal neuralgia.1,5,6 First-line choices included tricyclic antidepressants, serotonin-norepinephrine reuptake inhibitors, and gabapentinoids. Secondary choices included anti-epileptic drugs such as carbamazepine, oxcarbazepine, topiramate, and lamotrigine.1,6 However, many PTN cases are refractory to medication treatments.
Evidence of trigeminal nerve blocks (TNB) targeting trigeminal nerve branches has been accumulating for the treatment of trigeminal neuralgia,7,8 headache,9,10 and orofacial pain.11 These procedures provide rapid relief of facial pain in parallel with medication and surgical management. The application of local anesthetic around the nerve blocks sodium channels on peripheral nerves, inhibiting the transmission of nociceptive action potentials and the release of neurotransmitters. Local anesthetics and steroids also have multiple anti-inflammatory mechanisms that reduce the production of inflammatory cytokines and block inflammatory cell aggregation.12 Despite these mechanistic benefits, the efficacy of TNB specifically for PTN remains uncertain. Anatomical variations can contribute to mechanical irritation, compression susceptibility, and differential spread of injectate along the proximal trajectory of the trigeminal nerve, potentially affecting outcomes.13 There are clearly questions that need to be answered to improve the current management of PTN.14
This study aims to assess the efficacy of TNB in patients with PTN and to identify clinical parameters that affect its outcome, using retrospective chart reviews from patients treated at the Mass General Facial Pain Clinic. Our results demonstrate that TNB, combined with short- and long-acting local anesthetics and triamcinolone, is an effective treatment for PTN. In addition, we determined the clinical parameters that affect the outcome of the procedures.
Materials and Methods
Ethics Statement
The study was performed following the standards of the Declaration of Helsinki. The study was approved by the Ethics Committee of Mass General Hospital, Boston, Massachusetts (Protocol No. 2024P002719). A waiver of patient consent/authorization was approved for this retrospective study.
Institutional Review Board granted a waiver of consent/authorization due to the difficulty in locating individuals who may have moved, and limited research resources for locating individuals and sending letters and consent forms, and the impact on the scientific validity of the study if only data of individuals from whom we were able to obtain informed consent were used. Participants’ privacy was protected. All data were anonymized or maintained with confidentiality in the study.
Data Collection
We reviewed the medical records of patients who underwent TNB for PTN between March 2023 and March 2025 using ICD-10 code G50.8. We collected detailed medical history, including the onset of symptoms, pain distribution, symptom characteristics, clinically evident neuropathic symptoms (hyperalgesia, allodynia, hypoesthesia, hypoalgesia) within the context of trigeminal nerve dysfunction, comorbidities, and findings on physical and neurological exams. The PTN was determined based on whether the symptomatology met the diagnostic criteria of the International Classification of Headache 3rd edition (ICHD-3).2 At least three months of two medication regimens, including TCA, gabapentinoids, SNRI, and/or anti-convulsants, were tried before the patients were treated with TNB. Medication use remains unchanged during TNB treatments.
Clinical Parameters
Patient demographics, including age, sex, body mass index (BMI), and comorbidities such as migraine, temporomandibular joint disease (TMD), diabetes, prediabetes, ipsilateral trigeminal nerve root vascular contact, autoimmune disease, small fiber neuropathy, associated history of head and neck cancer, depression, anxiety, other psychiatric problems, substance used history such as smoking, alcohol, and cannabis, and associated trigeminal traumatic history such as dental procedures, head and neck surgeries, or facial trauma were collected. The causes of PTN were also identified, including dental procedures, facial trauma, postherpetic neuralgia, post-COVID-19, associated nasosinus infections, neoplasms, or idiopathic neuropathies. A Numerical Rating Scale (NRS) from 0 to 10 was used before the procedures and within 10 minutes after the procedure was documented in the medical records.
Inclusion/Exclusion Criteria
The inclusion criteria of these patients included: 1) A confirmed diagnosis of trigeminal neuropathy (ICD10 code G50.8); 2) Age is at least 18 years old; 3) symptoms have lasted for at least 3 months or more with failures of at least two medications. 4) receiving TNB at least once; 5) No medication change after the TNB and during the follow-up periods, and 6) follow-up at least 12 weeks after the procedure for evaluation of treatment response.
The exclusion criteria included 1) age less than 18 years; 2) the diagnosis of trigeminal neuralgia, atypical facial pain, or others that do not meet the diagnosis criteria of PTN in ICHD-3. 3) symptoms less than three months; 4) receiving other trigeminal nerve procedures such as gasserian nerve blocks, sphenopalatine nerve blocks, or rhizotomy; 5) no follow-up at least 12 weeks after the procedure; 6) Medication change after TNB and during a follow-up period. 7) Facial deformities.
Procedure Protocols
Patients signed an informed consent form that outlined the indications, risks, benefits, procedural details, potential complications, and aftercare information before receiving TNB. Trigeminal branches, including the auriculotemporal, supraorbital, supratrochlear, infratrochlear, infraorbital, mental, the external nasal branches of the anterior ethmoidal nerves, zygomaticofacial, and zygomaticotemporal nerves, were treated when local neuropathic symptoms or tenderness on palpation were present.(Figure 1)
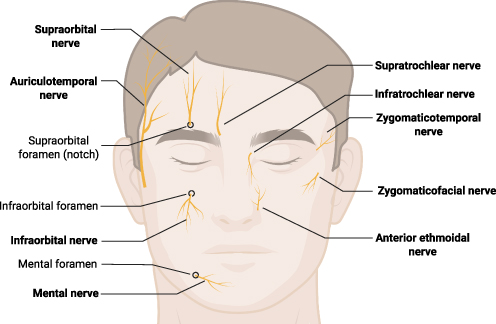 |
Figure 1 Trigeminal nerve blocks for painful trigeminal neuropathy. Trigeminal branches, including the auriculotemporal, supraorbital, supratrochlear, infratrochlear, infraorbital, mental, the external nasal branches of the anterior ethmoidal nerves, zygomaticofacial, and zygomaticotemporal nerves, were treated when local neuropathic symptoms or tenderness on palpation were present. NB: nerve blocks. The figure was created by the authors using BioRender software (www.biorender.com) without the use of artificial intelligence. |
The skin was cleaned with 70% Isopropyl alcohol three times before the procedure. The TNB regimen includes local anesthetics with triamcinolone (1:10 dilution, 40 mg/mL triamcinolone acetonide injectable suspension USP, Amneal Pharmaceuticals LLC, Bridgewater, New Jersey, USA). The local anesthetics used include 2% lidocaine (Short-acting, Auromedics Pharma LLC. Windsor, New Jersey, USA), 4% lidocaine (short-acting, Hospira, Inc, Lake Forrest, Illinois, USA), 0.5% Ropivacaine (long-acting, Somerset, Therapeutics, LLC, Hollywood, Florida, USA), 0.75% Bupivacaine (long- acting Eugua US LLC, E Windsor, New Jersey, USA). Triamcinolone was co-administered unless contraindicated by uncontrolled diabetes, hypertension, active infections, or psychological illness.
Most patients who failed short-acting local anesthetics progressed to regimens combining short- and long-acting agents. The techniques used for the injections were detailed by Pascal et al.15 Briefly, a 15-mm-long, 27-G needle on a 5-mL syringe was inserted perpendicularly to the skin lateral to the foramen corresponding to each trigeminal branch identified by palpation (Figure 1). The needles were inserted until just before bone contact, without entering the canal, to avoid direct nerve injury. Total amounts of 0.5 mL of solution were injected into each of the trigeminal nerve branches. Either unilateral or bilateral injections were performed according to symptomatology. All patients undergoing trigeminal nerve block procedures were scheduled for follow-up within 3 months of the procedures. For each follow-up evaluation, the NRS pain score after treatment and the duration of the treatment effect were documented. Patients received repetitive treatments if the results were satisfactory.
Outcome Analysis
The primary outcome of this study is the proportion of patients with 50% or greater pain relief lasting 8 weeks or longer (satisfactory pain reduction) after the procedures. The correlations between demographic characteristics, comorbidities, symptom characteristics, substance use status, and injection regimens with the outcome of satisfactory pain relief were analyzed statistically.
Statistical Analysis
The qualitative and ordinal variables are presented as frequencies and percentages, respectively. Quantitative continuous variables are represented by means and standard deviations (SD). We used Student’s t-test or a median test for hypothesis testing of quantitative, continuous variables. For the categorical variables, we demonstrated the frequencies and percentages. We used the two-tailed Pearson Chi-Square test or Fisher’s exact test to assess significant differences between outcome groups. Missing BMI data were handled using complete-case analysis. A p-value less than 0.05 indicated a significant difference. Statistical analysis was performed with IBM SPSS Statistics (version 28.0.0.0 (190), IBM Corp., Armonk, NY, USA).
Results
Duration of >50% Pain Reduction After Trigeminal Nerve Blocks
A total of 90 patients fulfilled the inclusion criteria during the chart review. Seventy-three patients (81.1%) achieved a satisfactory pain relief (50% or greater reduction in pain intensity) among all patients. (Table 1) The mean duration of satisfactory pain relief was 5.8 weeks after the procedures. Twenty-one (23.3%) patients achieved 12 weeks or more of > 50% pain reduction following the procedures, while 33 (36.7%) patients had > 8 weeks of relief; 45 (50.0%) patients had > 6 weeks; 63 (70.0%) had at least 2 weeks of 50% pain relief. Ten (11.1%) patients received less than 2 weeks of satisfactory pain relief. Seventeen patients (18.9%) failed to achieve pain reduction greater than 50% after the procedures (Table 1). Adverse events were local injection site pain (5.2%), and ecchymosis (2.1%).
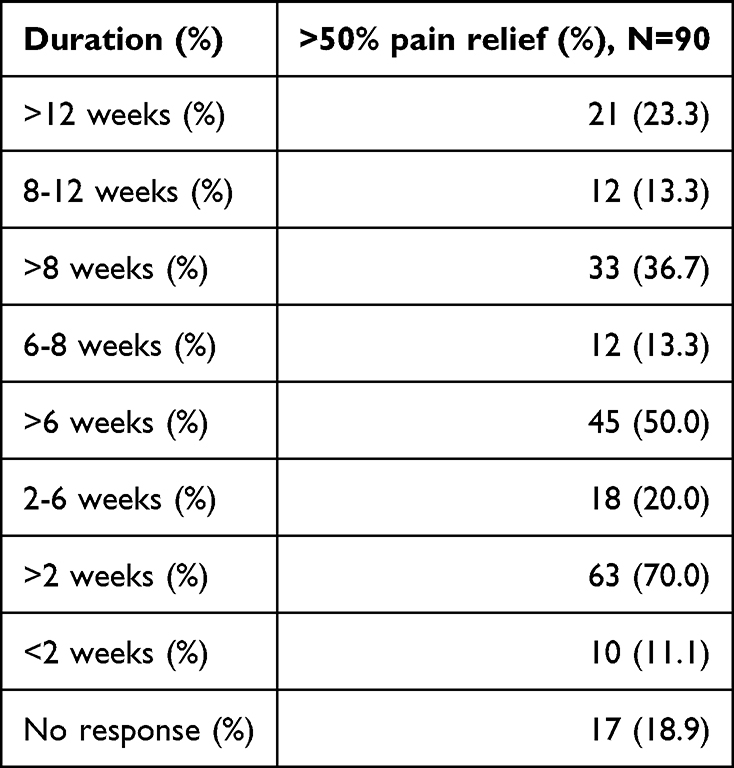 |
Table 1 Duration of >50% Pain Relief Following Trigeminal Nerve Blocks |
Treatment Outcomes Using Different Regimens
The 33 patients who achieved satisfactory pain reduction at 8 weeks. Among them, 27 (81.8%) had triamcinolone. The mean duration of pain relief was 5.9 weeks for patients who received triamcinolone. In contrast, only 6 (18.2%) patients who received local anesthetics without triamcinolone achieved similar efficacy following the procedure (Table 2). Only 4 (12.1%) patients had a satisfactory outcome using 2% lidocaine + triamcinolone. Ten patients (30.3%) had satisfactory relief from 2% lidocaine + 0.5% ropivacaine + triamcinolone. Thirteen patients (39.4%) achieved a satisfactory result after receiving 4% lidocaine+0.75% bupivacaine+triamcinolone (Table 2). In addition, eight patients who received other regimens achieved satisfactory pain relief, including 2 (6.1%) patients who received 2% lidocaine only, 1 (3.0%) patient received 0.75% bupivacaine with triamcinolone, 3 (9.1%) patients who received 0.75% bupivacaine only, one (3%) patient received 2% lidocaine + 0.5% Ropivacaine, and one (3%) patient received 4% lidocaine+0.5% Ropivacaine+triamcinolone.
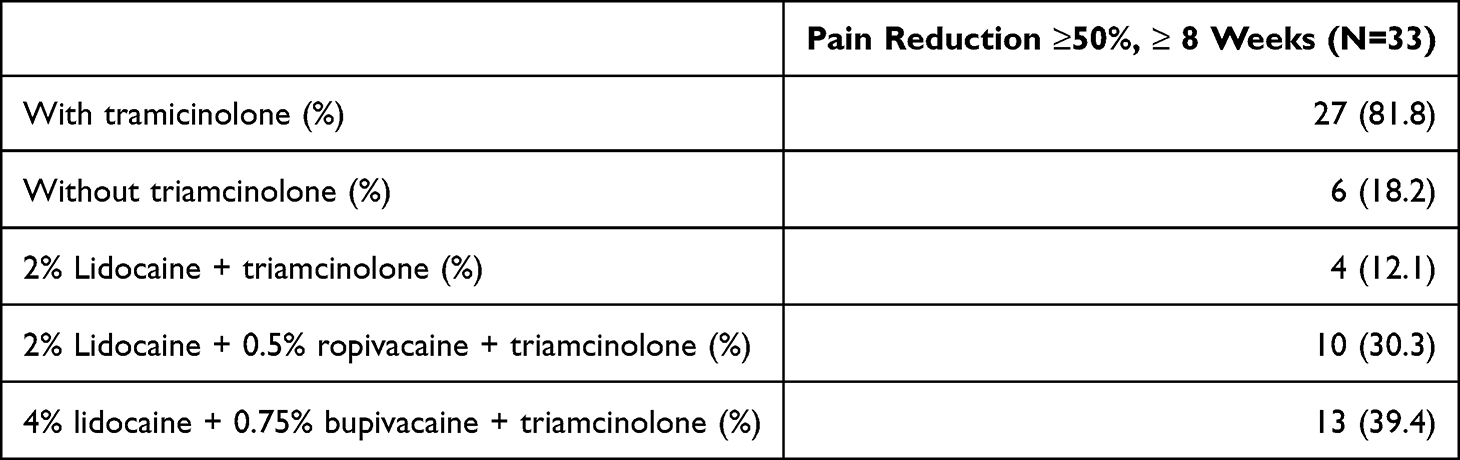 |
Table 2 Regimens Used for Achieving >50% Pain Relief at 8 Weeks |
Patient Demographic Characteristics and Satisfactory Pain Relief
The mean age was 50.6 years, with a female dominance (71.1%). The mean BMI was 27.1 kg/m2. (Table 3). There is no significant correlation between parameters, including age, sex, and BMI > 30, and achieving satisfactory pain relief at 8 weeks or at other time points (data not shown).
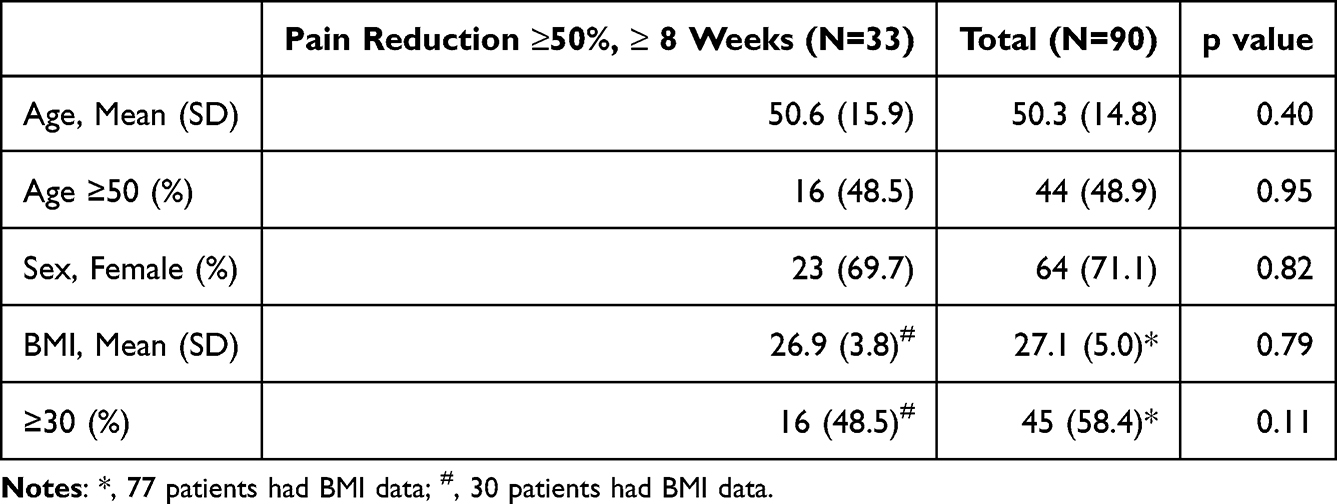 |
Table 3 Patient Demographic Information |
Pain Etiology and Outcome Analysis
Among different causes of PTN, trauma-related was the most common cause (63.3%), followed by idiopathic (17.8%), infectious (13.3%), neoplastic (4.4%), and stroke (1.1%). (Table 2). Sixty-seven percent of traumatic, 18.2% of infectious, 15.2% of idiopathic patients had satisfactory pain relief, but none of the neoplastic and stroke patients had satisfactory pain relief. There was no significant difference in PTN etiologies in achieving successful treatment responses at 8 weeks after the procedures (Table 4).
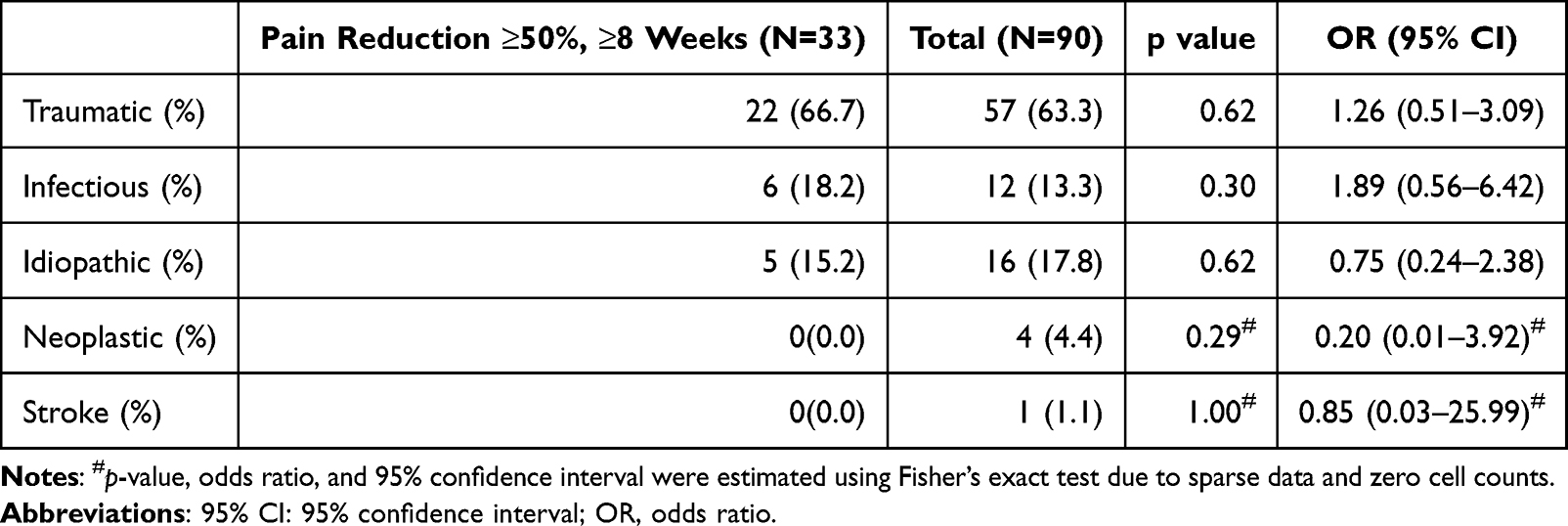 |
Table 4 The Correlation Between the PTN Etiology and >50% Pain Relief at 8 Weeks |
The Correlation of Comorbidities and Satisfactory Pain Relief
The history of common facial pain comorbidities was recorded and analysed in relation to the efficacy of the procedures. Overall, 94.4% of patients had at least six months history of facial pain before first injection, 16.7% with history of surgeries for trigeminal neuralgia (microvascular decompressions, radiosurgeries, or rhizotomies), 34.4% with history of previous dental procedures, 24.4% with history of head and neck surgeries, 15.6% with history of facial traum15, 37.8% with migraine, 38.9% with temporomandicular joint disorder (TMD), 38.9% with depression, 43.3% with anxiety, 16.7% with history of COVID-19 infection. The only related historical factor that correlates with satisfactory pain relief at 8 weeks is depression. Patients who had a depression diagnosis are less likely to achieve satisfactory pain relief at 8 weeks after the procedures (p=0.03, Table 5).
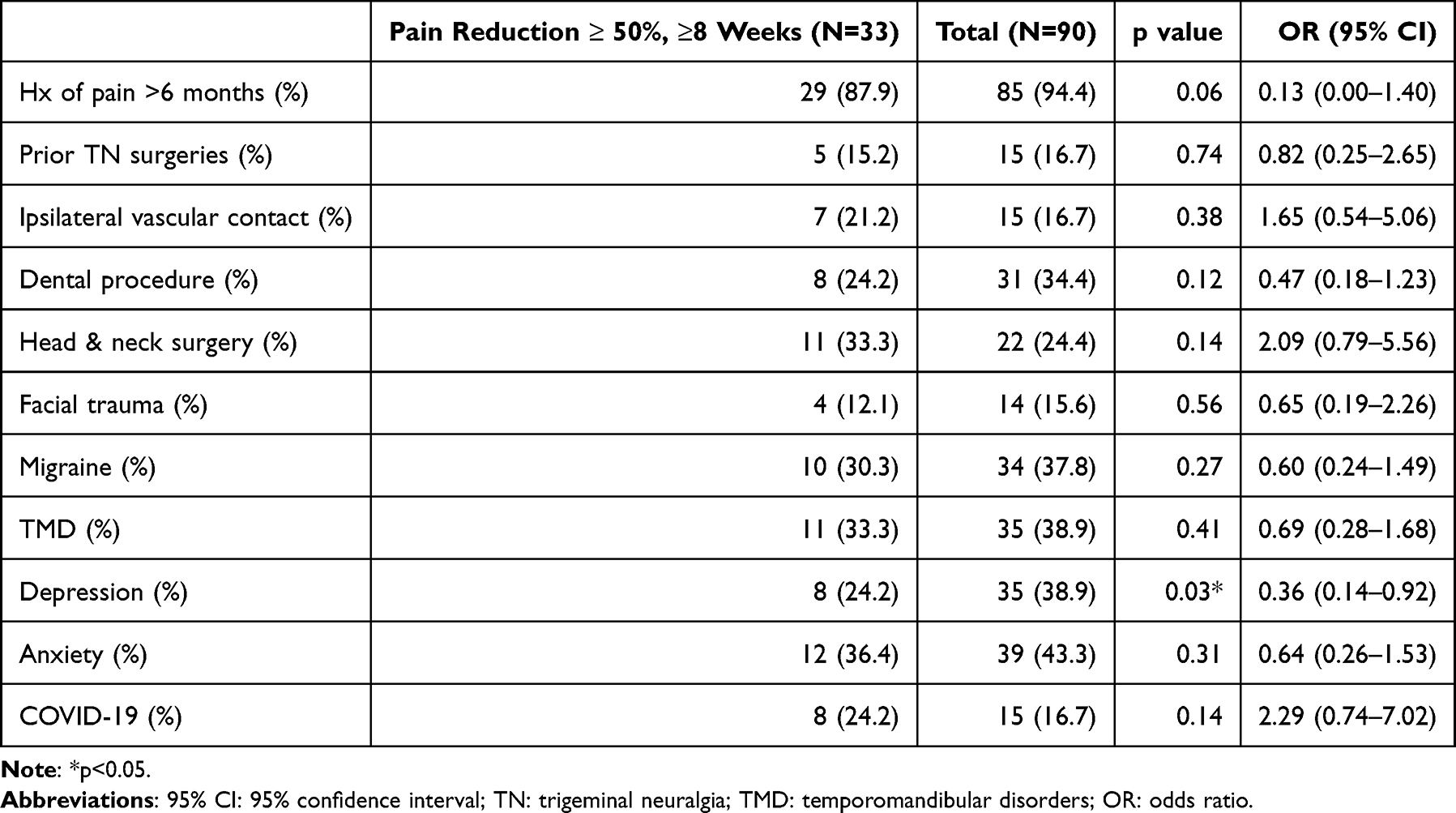 |
Table 5 The Correlation Between Comorbidities and >50% Pain Relief at 8 Weeks |
The Correlation of Clinical Symptomatology and Satisfactory Pain Relief
The correlation between symptomatic characteristics and satisfactory outcome is demonstrated in Table 6. Preprocedural pain intensity, bilateral V1/V3 distributions, constant pain, and allodynia did not predict better or worse pain relief. In contrast, patients were significantly less likely to achieve satisfactory pain relief (>8 weeks) with V2 involvement (p=0.03) and with facial numbness (p=0.02) (Table 6).
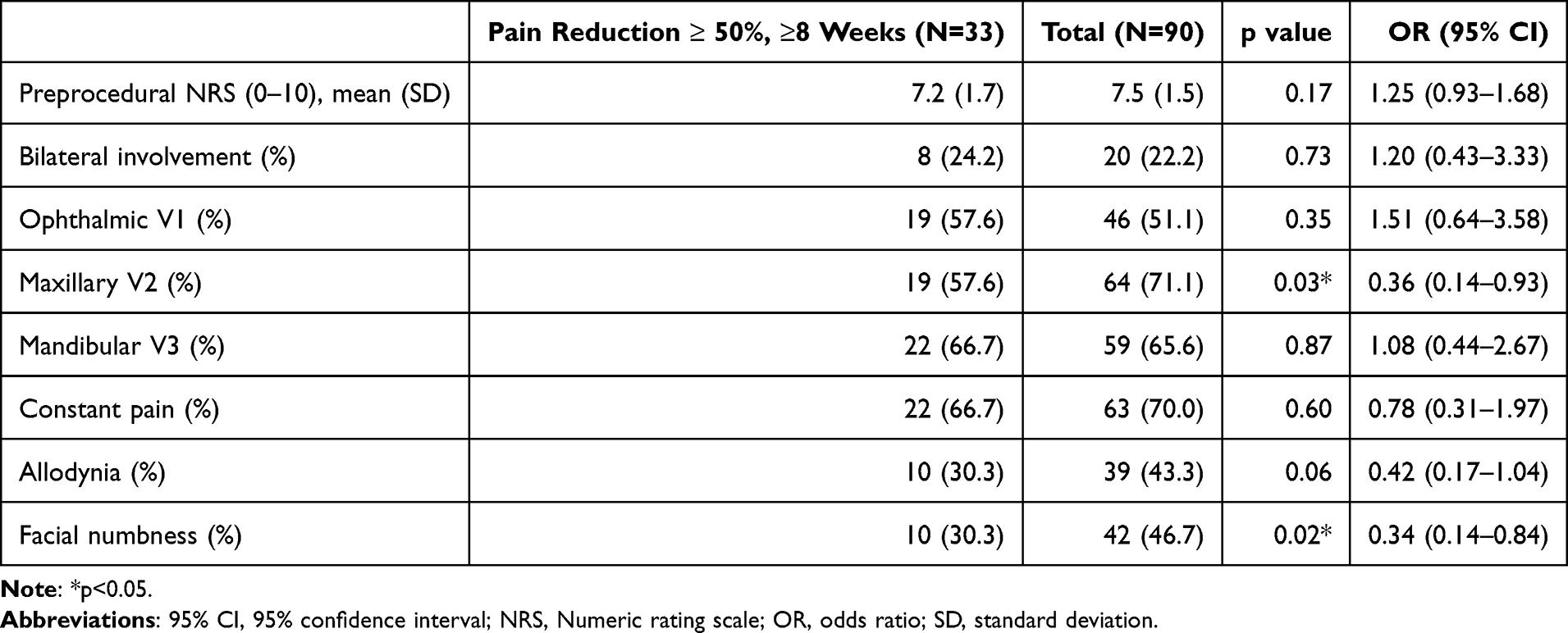 |
Table 6 The Correlation Between the Characteristics of Pain Symptoms and >50% Pain Relief at 8 Weeks |
Discussion
The current study explored the use of TNB for PTN with different local anesthetics, combining short-acting (lidocaine) and long-acting (ropivacaine, bupivacaine) regimens. This strategy has proven to be effective. Among all PTN patients undergoing peripheral nerve block procedures, most (81.1%) achieved at least 50% pain reduction, regardless of procedure duration. 50% of patients achieved >50% pain reduction within 6 weeks, and 36.7% achieved >50% relief that lasted for more than 8 weeks. The efficacy of our study was comparable to published studies in similar scenarios. Among them, Lee et al reported a retrospective descriptive study using TNB to treat chronic orbital pain. They showed that 84.2% of patients achieved partial or complete symptom improvement.14 In addition, Balta et al performed TNB with 2% lidocaine and 10 mg triamcinolone in 72 patients with trigeminal neuralgia and reported a 79.2% pain reduction rate at 1 month in a retrospective study.7 In contrast, the better pain reduction rate and duration in our study may be due to the use of higher concentrations of lidocaine (2~4%) combined with longer-acting local anesthetics (ropivacaine and bupivacaine). However, our data may be biased toward patients who did not require medication changes and who followed up after treatment to document the procedures’ efficacy. This selection bias is due to the medication change, an additional confounding variable that affects the procedure outcome analysis, and the limitations of a retrospective study in excluding patients who did not follow up.
Steroid use on local nerve blocks has been controversial. Although our data did not aim to study the efficacy of steroid use, the results demonstrate that steroid use is associated with longer pain relief (81.8% with steroid vs 18.2% without steroid achieving >50% reduction after 8 weeks), with relief persisting for a mean of 5.9 weeks. These data are consistent with numerous reports in the literature describing the positive effects of steroids on pain relief, nerve block, and nerve regeneration.16 However, future studies that use placebo-controlled groups are necessary for determining the positive effects of steroid use in TNB.
Many patients (39.4%) needed regimens containing 4% lidocaine and 0.75% bupivacaine, or 2% lidocaine and 0.5% ropivacaine (30.3%) to achieve satisfactory pain relief at 8 weeks. In contrast, only 12.1% of patients responded to 2% lidocaine and triamcinolone. The current results suggest that combining a short-acting (lidocaine) and a longer-acting (ropivacaine or bupivacaine) local anesthetic is an effective strategy for TNB to achieve >50% pain reduction > 8 weeks after the procedures. In contrast, Cuvillon et al reported that mixtures of long-acting local anesthetics with lidocaine had a faster onset but a shorter duration of anesthesia.17 In our study, TNB-induced pain relief lasted much longer than local anesthesia. The multimodal analgesic, a mixture of a short-acting local anesthetic (lidocaine) and a long-acting local anesthetic (bupivacaine or ropivacaine), provides prolonged analgesia, consistent with the report by Hemmi et al.18
The mean age of PTN patients in our study was 50.3 years, with a female predominance of 71.1%, which is comparable to previous literature on posttraumatic trigeminal neuropathy reporting a mean age of around 50 years and a female proportion ranging from 66–72%.19,20 In contrast, a RCT study of PHN patients reported an older average age of 60.1 years and a lower female proportion of 55.7%.21 This discrepancy may be attributed to the higher prevalence of herpes zoster infection in the elderly, whereas posttraumatic trigeminal neuropathy is more common in the younger population. In our study, more than half (63.3%) of patients were trauma-related, while infection-related cases, such as PHN, were only about 13.3%.
In our study, we found a significantly reduced TNB efficacy in patients with maxillary nerve (V2) involvement and persistent numbness in the trigeminal territories. In support of our data, Van der Cruyssen et al analyzed the prognostic factors of 384 posttraumatic trigeminal neuropathy patients with neurosensory disturbance (NSDs).19 They found that patients with thermal hyperesthesia had higher odds of persistent NSDs. In addition, higher odds of moderate-to-severe pain intensity in patients with maxillary nerve involvement, which may account for the shorter duration of the treatment effect and more severe pain intensity, consistent with our current results.
The current result demonstrates that depression is a significant factor that is associated with failure to reach > 50% pain reduction at 8 weeks after TNB. Other studies with pain procedures support this finding. For example, Kim et al reported the depression has negative impact on absolute score of (1) numeric rating scale for back pain, (2) numeric rating scale for leg pain, (3) disease-specific physical disability—Oswestry Disability Index, and (4) preference-based health status—EuroQol-5D for patients who had epidural steroid injections for degenerative joint pain in the spine.22
We recognized that many factors can affect TNB treatment outcomes, such as facial morphometric differences, which can influence injection trajectory, tissue penetration depth, diffusion of anesthetic agents, and the ease of accessing specific peripheral branches during nerve block procedures.23 In the current study, we did not include any records of patients with significant facial deformities.
Because of the limitation of a retrospective chart review, the current study cannot compare treatment efficacies across different regimen combinations. Instead, only the most effective regimen for each patient was recorded. Future comparison studies are needed to evaluate the efficacy across different regimens further.
Conclusions
The current study demonstrated preliminary positive results that TNB with combinations of short-acting and long-acting local anesthetics plus a steroid may be an effective therapy for treating patients with medically refractory chronic painful trigeminal neuropathy. Future studies using a randomized, placebo-controlled approach are required to elucidate the effects of peripheral trigeminal nerve blocks and the optimal injection regimens.
Data Sharing Statement
https://doi.org/10.7910/DVN/OZWKS3, Harvard Dataverse, V1.
Acknowledgments
The authors thank Dr. Jen-Tse Chen of the Cathay General Hospital and the Mass General Brigham Neuroscience Institute for their support of the project. HTC is supported by NIH 1R21DE031410.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors have no competing interests in this work.
References
1. Benoliel R, Kahn J, Eliav E. Peripheral painful traumatic trigeminal neuropathies. Oral Dis. 2012;18(4):317–9. doi:10.1111/j.1601-0825.2011.01883.x
2. Olesen J. Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia. 2018;38(1):1–211.
3. Wilcox SL, Gustin SM, Eykman EN, et al. Trigeminal nerve anatomy in neuropathic and non-neuropathic orofacial pain patients. J Pain. 2013;14(8):865–872. doi:10.1016/j.jpain.2013.02.014
4. Garcia-Blanco M, Gualtieri AF, Lovaglio-Rivas AC, Ruffini JM, Puia SA. Trigeminal nerve injuries. Four years’ experience at a single Argentine referral center and a literature review. Acta Odontol Latinoam. 2021;34(3):263–270. doi:10.54589/aol.34/3/263
5. Finnerup NB, Attal N, Haroutounian S, et al. Pharmacotherapy for neuropathic pain in adults: a systematic review and meta-analysis. Lancet Neurol. 2015;14(2):162–173. doi:10.1016/S1474-4422(14)70251-0
6. Niemeyer CS, Harlander-Locke M, Bubak AN, Rzasa-Lynn R, Birlea M. Trigeminal postherpetic neuralgia: from pathophysiology to treatment. Curr Pain Headache Rep. 2024;28(4):295–306. doi:10.1007/s11916-023-01209-z
7. Balta S, Köknel Talu G. Clinical effectiveness of peripheral nerve blocks with lidocaine and corticosteroid in patients with trigeminal neuralgia. Agri. 2021;33(4):237–242. doi:10.14744/agri.2021.26032
8. Di Stani F, Ojango C, Dugoni D, et al. Combination of pharmacotherapy and lidocaine analgesic block of the peripheral trigeminal branches for trigeminal neuralgia: a pilot study. Arq Neuropsiquiatr. 2015;73(8):660–664. doi:10.1590/0004-282X20150077
9. Blumenfeld A, Ashkenazi A, Napchan U, et al. Expert consensus recommendations for the performance of peripheral nerve blocks for headaches--a narrative review. Headache. 2013;53(3):437–446. doi:10.1111/head.12053
10. Hascalovici JR, Robbins MS. Peripheral nerve blocks for the treatment of headache in older adults: a retrospective study. Headache. 2017;57(1):80–86. doi:10.1111/head.12992
11. Renton T, Beke A. A narrative review of therapeutic peripheral nerve blocks for chronic orofacial pain conditions. J Oral Facial Pain Headache. 2022;36(1):49–58. doi:10.11607/ofph.3017
12. Martin F, Martinez V, Mazoit JX, et al. Antiinflammatory effect of peripheral nerve blocks after knee surgery: clinical and biologic evaluation. Anesthesiology. 2008;109(3):484–490. doi:10.1097/ALN.0b013e318182c2a1
13. Ogut E, Armagan K, Barut C. Reappraisal of the types of trigeminal porus and importance in surgical applications. Surg Radiol Anat. 2021;43(7):1169–1178. doi:10.1007/s00276-020-02651-z
14. Lee G, Pham CM, Kardon RH, Shriver EM. Peripheral trigeminal nerve blocks for chronic orbital pain: clinical features and outcomes. Ophthalmic Plast Reconstr Surg. 2022;38(4):369–376. doi:10.1097/IOP.0000000000002120
15. Pascal J, Charier D, Perret D, Navez M, Auboyer C, Molliex S. Peripheral blocks of trigeminal nerve for facial soft-tissue surgery: learning from failures. Eur J Anaesthesiol. 2005;22(6):480–482. doi:10.1017/S0265021505260817
16. Couch B, Hayward D, Baum G, et al. A systematic review of steroid use in peripheral nerve pathologies and treatment. Front Neurol. 2024;15:1434429. doi:10.3389/fneur.2024.1434429
17. Cuvillon P, Nouvellon E, Ripart J, et al. A comparison of the pharmacodynamics and pharmacokinetics of bupivacaine, ropivacaine (with epinephrine) and their equal volume mixtures with lidocaine used for femoral and sciatic nerve blocks: a double-blind randomized study. Anesth Analg. 2009;108(2):641–649. doi:10.1213/ane.0b013e31819237f8
18. Hemmi T, Sasahara N, Yusa K, Ishikawa S, Kobayashi T, Iino M. Analgesic effect of a lidocaine-ropivacaine mixture for extraction of impacted mandibular third molars: a randomized controlled trial. Clin Oral Investig. 2023;27(10):5969–5975. doi:10.1007/s00784-023-05210-z
19. Van der Cruyssen F, Peeters F, De Laat A, Jacobs R, Politis C, Renton T. Prognostic factors, symptom evolution, and quality of life of posttraumatic trigeminal neuropathy. Pain. 2022;163(4):e557–e571. doi:10.1097/j.pain.0000000000002408
20. Melek LN, Smith JG, Karamat A, Renton T. Comparison of the neuropathic pain symptoms and psychosocial impacts of trigeminal neuralgia and painful posttraumatic trigeminal neuropathy. J Oral Facial Pain Headache. 2019;33(1):77–88. doi:10.11607/ofph.2157
21. Makharita MY, Amr YM, El-Bayoumy Y. Effect of early stellate ganglion blockade for facial pain from acute herpes zoster and incidence of postherpetic neuralgia. Pain Physician. 2012;15(6):467–474.
22. Kim EJ, Chotai S, Stonko DP, et al. Patient-reported outcomes after lumbar epidural steroid injection for degenerative spine disease in depressed versus non-depressed patients. Spine J. 2017;17(4):511–517. doi:10.1016/j.spinee.2016.10.017
23. Alheet G, Barut C, Ogut E. Quantitative analysis of surgical landmarks of the face in fixed cadaveric heads: clinical and anatomical implications. Surg Radiol Anat. 2024;46(11):1811–1823. doi:10.1007/s00276-024-03474-y
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.