Back to Journals » Orthopedic Research and Reviews » Volume 17
Trifocal Ilizarov Bone Transport for a 21-cm Tibial Defect in a Chronic Smoker with Longstanding Osteomyelitis: A Complex Limb Salvage Case
Authors Hayat U, Abdulaziz AA ![]() , Alghamdi FA
, Alghamdi FA ![]() , Alnofeay KA
, Alnofeay KA ![]() , Ashry HG, Labban AA
, Ashry HG, Labban AA
Received 22 June 2025
Accepted for publication 24 November 2025
Published 8 December 2025 Volume 2025:17 Pages 583—592
DOI https://doi.org/10.2147/ORR.S547786
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Clark Hung
Umar Hayat,1 Abdulaziz A Abdulaziz,2 Faisal A Alghamdi,3 Khalid Ahmad Alnofeay,1 Hassan Ghazi Ashry,1 Atif Ahmed Labban1
1Orthopedic Department, King Faisal Hospital, Makkah, Saudi Arabia; 2Orthopedic Department, King Faisal Medical Complex Taif, Taif, Saudi Arabia; 3College of Medicine, Umm Al-Qura University, Makkah, Saudi Arabia
Correspondence: Faisal A Alghamdi, College of Medicine, Umm Al-Qura University, Makkah, Saudi Arabia, Email [email protected]
Abstract: This case study presents the successful management of a 21-cm tibial defect in a 38-year-old man smoker with longstanding osteomyelitis using trifocal Ilizarov bone transport. Despite the complexities posed by chronic infection and extensive bone loss, a meticulously planned staged reconstructive protocol involving aggressive debridement, targeted antimicrobial therapy, and advanced bone transport techniques culminated in remarkable limb salvage and functional recovery. Integration of low-intensity pulsed ultrasound (LIPUS) further optimized bone healing in this intricate scenario. This case report addresses these gaps by detailing a successful trifocal Ilizarov strategy augmented with LIPUS in a chronic smoker with an exceptionally large tibial defect.
Keywords: ilizarov, reconstruction, bone regeneration, bone loss tibial defect
Introduction
Chronic osteomyelitis of the tibia remains one of the most formidable complications following both intra- and extramedullary fixation of leg fractures. Its incidence can be as high as 22.4% in certain series, particularly in the context of open fractures, contaminated wounds, and inadequate initial stabilization or soft tissue management.1–3 Once established, chronic osteomyelitis presents a complex therapeutic dilemma, often requiring a multidisciplinary approach involving aggressive debridement, targeted antimicrobial therapy, and definitive skeletal reconstruction.
Among the modifiable risk factors, smoking has been consistently identified as a significant contributor to the pathogenesis and persistence of chronic osteomyelitis. Beyond its systemic effects, smoking impairs local vascularity, suppresses osteoblastic activity, and adversely affects both primary bone healing and regenerate formation in distraction osteogenesis.4
The management of large segmental tibial defects resulting from infection-related debridement poses an additional challenge. Various reconstructive options exist, including the Masquelet induced membrane technique, vascularized or non-vascularized autologous bone grafting, and bone transport using distraction osteogenesis.5–7 However, in Cierny–Mader type IV chronic osteomyelitis—with extensive segmental bone loss and compromised host status—traditional methods such as sequestrectomy, antibiotic therapy, and repeated internal fixation often yield suboptimal outcomes and high failure rates.8–10
In this context, the Ilizarov method of bone transport has emerged as the gold standard for limb salvage in cases of extensive diaphyseal bone loss, particularly when accompanied by active infection and soft tissue compromise. First described by Professor Gavril Ilizarov, the technique allows for simultaneous infection control, segmental bone regeneration, and correction of deformity without the need for massive bone grafting.11–14
Existing literature suggests that bifocal Ilizarov bone transport is effective, but it is associated with long external-fixation times and regenerate problems; trifocal transport may shorten treatment but remains under-reported and controversial.15 There is also limited evidence regarding the use of low-intensity pulsed ultrasound (LIPUS) during distraction osteogenesis, especially in smokers.16
This report presents a rare and particularly challenging case of chronic post-traumatic osteomyelitis in a 38-year-old male with a 22-year history of infection, heavy smoking, and a resultant 21-cm tibial defect. The successful management of this case using staged debridement and trifocal Ilizarov bone transport augmented by LIPUS offers insight into the application of advanced limb reconstruction strategies in high-risk, multiply operated patients.
Case Presentation
A 38-year-old man, previously healthy but a chronic smoker, presented to our tertiary limb reconstruction clinic with a long-standing, draining sinus over the anterior aspect of his right leg (Figure 1). His clinical history was striking: 22 years prior, he had sustained a high-energy road traffic accident resulting in a Gustilo-Anderson grade IIIB open fracture of the right tibial shaft. At the time, the injury was managed with a monolateral external fixator and coverage using a split-thickness skin graft. Despite undergoing six separate procedures over several years—addressing both bony stabilization and soft tissue reconstruction—he had never fully recovered. Since the initial injury, he had lived with intermittent purulent discharge and the occasional extrusion of bone fragments through the sinus. His leg had become not just a source of pain but a visible reminder of trauma, infection, and limitation.
 |
Figure 1 Clinical picture of the leg on the first visit of the patient showing sequestrum protruding through the sinus. |
At presentation, the patient reported escalating pain, foul-smelling discharge, and a large bone fragment visibly protruding through the sinus tract. He described significant functional limitations and expressed emotional fatigue from years of living with a non-healing wound. (Figure 2) Radiographs and computed tomography revealed dense cortical sclerosis, periosteal hyperplasia, and a large sequestrum involving the mid-diaphysis of the tibia. Laboratory investigations were consistent with chronic osteomyelitis.
 |
Figure 2 X-ray of the right leg on the day of admission showing sequestra and sclerosis of the middle segment of the tibia. |
After extensive counseling, including discussions around the relative benefits of amputation versus limb salvage, the patient expressed a strong preference to retain his limb. A two-stage reconstructive strategy was planned. The first stage focused on eradicating infection. Under general anesthesia, approximately 21 cm of infected mid-tibial diaphysis was excised (Figure 3), followed by the application of an Ilizarov circular external fixator (Figure 4). Antibiotic-loaded polymethyl methacrylate (PMMA) cement was inserted to maintain space and deliver local antimicrobial therapy (Figure 5). Multiple intraoperative samples were obtained for microbiological and histopathological analysis. Postoperatively, he was treated with six weeks of culture-directed intravenous antibiotics. Wound culture and sensitivity showed Proteus Mirabilis ESBL sensitive to bactrim started on meropenem while admitted then discharged on bactrim for six weeks till labs return to normal range as adviced by infectious disease department.
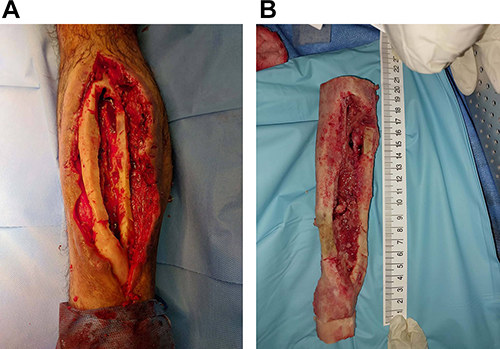 |
Figure 3 (A) Per-op clinical picture of the wound after the second debridement, showing extensive sclerosis with no bleeding bone. (B) Length of tibia excised after radical debridement till bleeding bone. |
 |
Figure 4 Clinical picture of the leg with the Ilizarov frame in place. |
 |
Figure 5 Immediate post-op x-ray showing remaining tibia, fibular osteotomy, and bone cement in situ. |
The second stage of reconstruction began six weeks later. After confirming local infection control, the cement spacer was removed and a proximal tibial corticotomy was performed (Figure 6). Bone transport was initiated 10 days postoperatively at a rate of 1 mm/day. However, after three months, regenerate formation at the proximal site was suboptimal. In response, a second corticotomy was performed distally (Figure 7), converting the strategy to trifocal bone transport to reduce total time in the frame and improve regenerate quality.
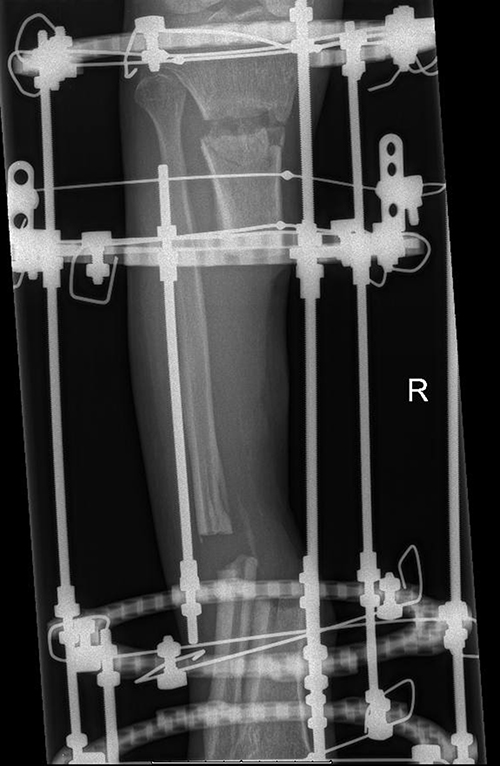 |
Figure 6 X-ray taken during follow-up showing bone transport at proximal. |
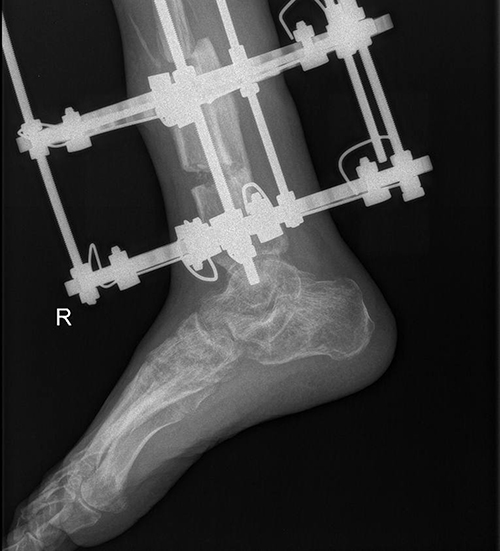 |
Figure 7 Distal osteotomy sites in progress. |
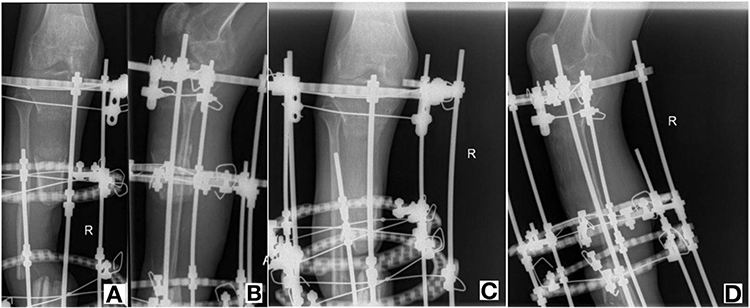 |
Figure 8 (A and B) Radiographs obtained in April 2024 demonstrating delayed regenerate maturation 6 months after fixator application. (C and D) Radiographs obtained in August 2024, four months after initiation of LIPUS, showing improved regenerate quality. |
During the distraction phase, the patient required two additional surgeries: one for exchange of infected wires and another for realignment and frame adjustment. Despite these challenges, he remained compliant and motivated. Supportive measures were introduced to optimize osteogenesis. Nutritional counseling, oral supplements, and an individualized physiotherapy regimen were initiated. The patient successfully stopped smoking six months after frame application. The accordion technique—alternating compression and distraction—was employed twice to stimulate regeneration at the proximal site. In addition, two courses of low-intensity pulsed ultrasound (LIPUS) were administered, both of which resulted in qualitative improvement in callus density and morphology on radiographs (Figure 8).
Given the magnitude of the defect and delayed regenerate formation, a residual limb shortening of 4 cm was accepted. Ultimately, 17 cm of new bone was successfully transported and consolidated. At the 18-month follow-up, radiographs confirmed union at the docking site and mature regenerate formation (Figure 9). The external fixator was dynamized prior to removal to promote load-sharing.
 |
Figure 9 X-ray after removal of the frame showing (A) completely united bone (B) mechanical alignment maintained. |
At the final assessment (Figure 10), three months after removal of ilizarov fixator the patient had achieved a full range of motion at the knee with only mild ankle stiffness. Functional outcomes were satisfactory: the Knee Society Score was 95/100, and the functional score was 60/100. According to the ASAMI criteria, both bone and functional results were graded as “good.” The bone healing index was calculated at 1.1 cm/month, consistent with literature benchmarks for trifocal transport in complex tibial defects.17
 |
Figure 10 Clinical picture of the patient 2 months after the removal of the frame. |
Discussion
The primary objective in this case was to restore equal limb length to regain optimal function. Several reconstructive options were considered to address the extensive tibial bone defect. Autologous bone grafting, while biologically favorable, is limited in cases of large defects due to the need for multiple donor sites, which introduces significant morbidity and donor site complications.18
Free vascularized fibular grafts from the contralateral limb are a suitable option for large defects but are best reserved for cases where the donor limb is not under high functional demand, which was not applicable in our patient. Allograft reconstruction presents its own challenges, including complex preparation, preservation requirements, and risk of immunologic rejection or infection.18,19 Furthermore, the presence of soft tissue involvement and the extent of the defect precluded these traditional approaches, as adequate soft tissue coverage must be established first—an inherently time-consuming step. While amputation offers rapid functional rehabilitation and can be a viable option in selected cases, the irreversible loss of the limb makes it an unfavorable first-line solution for most patients.
After a comprehensive evaluation, multilevel bone transport was selected as the most suitable reconstructive approach. This technique is particularly advantageous in managing extensive bone loss, as it reduces total treatment time and addresses segmental defects effectively. For instance, Lerner in his research has successfully employed bifocal transport to bridge a 22 cm tibial gap.20 Similarly, Alkenani in his study demonstrated successful unifocal transport in a large defect (14.5 cm) without the need for an intramedullary nail, achieving full bone regeneration.21 However, it is important to note that multilevel transport requires a complex external fixator system and may be associated with delayed regenerate consolidation.22
To optimize healing in our case, low-intensity pulsed ultrasound (LIPUS) was integrated into the management protocol. In a retrospective cohort study by Song et al involving 30 patients, LIPUS significantly improved consolidation, particularly in the anterior and medial cortices (p < 0.001 and p = 0.002, respectively). It was associated with denser, more uniform callus formation, potentially translating into stronger bone regeneration.23
In our case, a trifocal lengthening strategy combined with LIPUS allowed for full restoration of a 17 cm tibial defect. The adjunctive use of LIPUS was especially valuable given the complicating factors of chronic osteomyelitis and a history of smoking, both of which negatively impact bone healing. This approach achieved successful limb salvage. Equalization of limb length and restoration of function.
Conclusion
This case emphasizes the feasibility of trifocal Ilizarov reconstruction for large 21 cm tibial bone defect complicated by Osteomyelitis and smoking. The integration of LIPUS may augment regenerate maturation in compromised bone, representing a potential adjunct to modern distraction osteogenesis protocols.
Ethical Approval
Institutional approval was not required for publishing the case details according to our institution’s policies.
Informed Consent for Publication
Written informed consent was obtained from the patient’s for publication of this case report and accompanying images.
Acknowledgments
We extend our sincere gratitude to the patient for their cooperation and willingness to share their medical journey, and to Dr. Nahla H Hariri for her invaluable assistance in the publication of this case study. Thank you to all involved for their contributions to the successful outcome of this study.
Author Contributions
All authors contributed to the data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval or the version to be published, and agree to be accountable for all aspects of the work.
Funding
This case report did not receive any specific grants from funding agencies in the public, commercial, or nonprofit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lazzarini L, Mader JT, Calhoun JH. Osteomyelitis in long bones. J Bone Joint Surg Ame. 2004;86(10):2305–2318.
2. Calhoun JH, Manring MM, Shirtliff M. Osteomyelitis of the long bones. Semina Plastic Surg. 2009;23(2):59–72. doi:10.1055/s-0029-1214158
3. Kremers HM, Nwojo ME, Ransom JE, Wood-Wentz CM, Melton LJ III, Huddleston PM III. Trends in the epidemiology of osteomyelitis: a population-based study, 1969 to 2009. J Bone Joint Surg Ame. 2015;97(10):837–845.
4. Huang X, Li Q, Chen J, Liu T, Zhao Y, Teng Y. Clinical features of chronic tibial osteomyelitis: a single-center retrospective study of 282 cases in Xinjiang, China. BMC Musculoskeletal Disord. 2024;25(1). doi:10.1186/s12891-024-07928-7
5. Uzel AP, Lemonne F, Casoli V. Tibial segmental bone defect reconstruction by Ilizarov type bone transport in an induced membrane. Orthop Traumatol Surg Res. 2010;96:194–198.
6. Pipitone PS, Rehman S. Management of traumatic bone loss in the lower extremity. Orthoped Clin North Ame. 2014;45(4):469–482. doi:10.1016/j.ocl.2014.06.008
7. Meselhy MA, Singer MS, Halawa AM, Hosny GA, Adawy AH, Essawy OM. Gradual fibular transfer by Ilizarov external fixator in post-traumatic and post-infection large tibial bone defects. Arch Orthopaedic Trauma Surg. 2018;138(5):653–660. doi:10.1007/s00402-018-2895-z
8. Henke PK, Blackburn SA, Wainess RW, et al. Osteomyelitis of the foot and toe in adults is a surgical disease: conservative management worsens lower extremity salvage. Ann Surg. 2005;241(6):885–894. doi:10.1097/01.sla.0000164172.28918.3f
9. Heitzmann LG, Battisti R, Rodrigues AF, et al. Postoperative chronic osteomyelitis in the long bones - current knowledge and management of the problem. Revista Brasileira de Ortopedia. 2019;54(6):627–635. doi:10.1016/j.rbo.2017.12.013
10. Morris R, Hossain M, Evans A, et al. Induced membrane technique for treating tibial defects gives mixed results. Bone Joint J. 2017;99-B(5):680–685. doi:10.1302/0301-620X.99B5.BJJ-2016-0694.R2
11. Plakseychuk A, Plakseychuk Y, Gruen GS, Ziran BH. Treatment of osteomyelitis with Ilizarov frame. Operat Techniq Orthopaed. 2002;12(4):273–281. doi:10.1053/otor.2002.36312
12. McNally M, Ferguson J, Kugan R, Stubbs D. Ilizarov treatment protocols in the management of infected nonunion of the tibia. J of Orthop Trauma. 2017;31(5):S47–S54. doi:10.1097/BOT.0000000000000987
13. Schwartsman V, Martin SN, Ronquist RA, Schwartsman R. Tibial fractures: the Ilizarov alternative. Clin Orthopaedics Related Res. 1992;278:207–215. doi:10.1097/00003086-199205000-00033
14. Chaddha M, Gulati D, Singh AP, Maini L. Management of massive posttraumatic bone defects in the lower limb with the Ilizarov technique. Acta Orthopaedica Belgica. 2010;76:811–820.
15. Xu YQ, Fan XY, He XQ, Wen HJ. Reconstruction of massive tibial bone and soft tissue defects by trifocal bone transport combined with soft tissue distraction: experience from 31 cases. BMC Musculoskeletal Disorders. 2021;22(1):34. doi:10.1186/s12891-020-03894-y
16. Simpson AH, Keenan G, Nayagam S, Atkins RM, Marsh D, Clement ND. Low-intensity pulsed ultrasound does not influence bone healing by distraction osteogenesis: a multicentre double-blind randomised control trial. Bone Joint J. 2017;99-B(4):494–502. doi:10.1302/0301-620X.99B4.BJJ-2016-0559.R1
17. Li R, Zhu G, Chen C, Chen Y, Ren G. Bone transport for treatment of traumatic composite tibial bone and soft tissue defects: any specific needs besides the Ilizarov technique? Biomed Res Int. 2020;2020(1):2716547. doi:10.1155/2020/2716547
18. Abdel-Aal AM. Ilizarov bone transport for massive tibial bone defects. Orthopedics. 2006;29(1):70–74.
19. World Health Organization. Global status report on road safety 2009. 2009. Available from: http://www.who.int/violenceinjuryprevention/roadsafetystatus/2009/en/.
20. Lerner A, Fodor L, Stein H, Soudry M, Peled IJ, Ullmann Y. Extreme bone lengthening using distraction osteogenesis after trauma: a case report. J of Orthop Trauma. 2005;19(6):420–424. doi:10.1097/01.bot.0000177388.05060.a4
21. Alkenani NS, Alosfoor MA, Al-Araifi AK, Alnuaim HA. Ilizarov bone transport after massive tibial trauma: case report. Inter J Surg Case Rep. 2016;28:101–106. doi:10.1016/j.ijscr.2016.08.040
22. Mauffrey C, Barlow BT, Smith W. Management of segmental bone defects. J Ame Acad Orthopaed Surge. 2015;23(3):143–153. doi:10.5435/JAAOS-D-14-00018
23. Song MH, Kim TJ, Kang SH, Song HR. Low-intensity pulsed ultrasound enhances callus consolidation in distraction osteogenesis of the tibia by the technique of lengthening over the nail procedure. BMC Musculoskeletal Disord. 2019;20(1):1–8. doi:10.1186/s12891-019-2490-7
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.