")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Trichoscopic Features of Syphilitic Alopecia and Alopecia Areata: A Comparative Study
Authors Tejapira K , Sakpuwadol N , Pomsoong C , Ratanapokasatit Y , Suchonwanit P
Received 2 June 2023
Accepted for publication 11 August 2023
Published 17 August 2023 Volume 2023:16 Pages 2259—2269
DOI https://doi.org/10.2147/CCID.S424054
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Kasama Tejapira, Nawara Sakpuwadol, Cherrin Pomsoong, Yanisa Ratanapokasatit, Poonkiat Suchonwanit
Division of Dermatology, Department of Medicine, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand
Correspondence: Poonkiat Suchonwanit, Division of Dermatology, Department of Medicine, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, 270 Rama VI Road, Ratchathewi, Bangkok, 10400, Thailand, Tel +66-2-2011141, Fax +66-2-201-1211 ext 4, Email [email protected]
Background: Syphilitic alopecia (SA) and alopecia areata (AA) are two distinct conditions that frequently present diagnostic difficulties, especially when differentiating between them due to their similar clinical presentations. Trichoscopy may help in differential diagnosis, but a comparison between trichoscopic features of SA and AA is yet to be researched.
Objective: To compare trichoscopic features between SA and AA and determine their discriminative values.
Methods: Electronic medical records and trichoscopic images of patients diagnosed with SA or AA between January 2000 and February 2022 were retrieved. Trichoscopic features were statistically compared, and their discriminative values were demonstrated as sensitivity, specificity, predictive value, likelihood ratio, and area under the receiver operating characteristic curve (AUC).
Results: A total of 69 patients were included: 23 SA and 46 AA cases were matched with a 1:2 ratio. Black dots, broken hairs, pigtail hairs, exclamation mark hairs, tapered hairs, angulated hairs, and non-pigmented regrowing hairs were significantly more prevalent in AA than in SA (all P< 0.05), whereas erythematous background was more prevalent in SA than in AA patients (P=0.008). Among the aforementioned trichoscopic features, exclamation mark hairs and non-pigmented regrowing hairs had a high positive likelihood ratio for AA (16.17 and 8.34, respectively); however, only exclamation mark hairs revealed high AUC (AUC=0.816).
Conclusion: Despite the presence of several similar trichoscopic features between SA and AA, trichoscopy can aid in distinguishing between the two diseases. Exclamation mark hairs are the only trichoscopic feature that can be used to differentiate patients with clinically suspicious SA from those with AA.
Keywords: alopecia areata, alopecia syphilitica, dermoscopy, exclamation mark hairs, syphilis, trichoscopy
Introduction
Non-scarring alopecia is one of the chief presenting complaints among dermatology patients. Among this group of disorders, syphilitic alopecia (SA) and alopecia areata (AA) are two distinct conditions that often pose a challenge in differential diagnosis, since both can show similar clinical presentations that usually require a histopathological examination to achieve a definitive diagnosis.1–3
SA is a relatively rare non-scarring alopecia disorder, occurring in approximately 2.9–22.2% of patients with secondary syphilis.4–6 It is considered a great imitator due to its various presentations that mimic other hair disorders, such as AA and trichotillomania. SA comprises three distinct hair loss patterns, including moth-eaten, diffuse, and mixed alopecia, and can affect eyebrows and eyelashes.7 It can be classified based on mucocutaneous involvement into symptomatic SA (alopecia with syphilitic skin lesions) and essential SA (hair loss without other cutaneous features).5 Proper antibiotic treatment for syphilis is effective in achieving significant hair regrowth.
AA is an immune-mediated non-scarring alopecia with 1.7–2.1% lifetime prevalence.8–10 Despite its prevalence, the causes and mechanisms of AA are not yet fully understood. AA manifests in various clinical types, including a well-circumscribed patch or patches, reticular, diffuse, ophiasis, complete scalp hair loss (alopecia totalis), and total body hair loss (alopecia universalis).11,12 AA highly impacts patients’ quality of life owing to its unpredictable treatment response and clinical course.13,14
Cutaneous manifestations of secondary syphilis are helpful in differentiating SA from AA; however, its absence in essential SA complicates the diagnosis.15 Trichoscopy, a non-invasive diagnostic tool widely used in evaluating hair and scalp disorders, has shown promising results in the accurate diagnosis of both conditions.16 It has been reported to significantly reduce scalp biopsy rate, an invasive diagnostic procedure, and increase the diagnostic yield of SA by 40%.17 However, most trichoscopic features reported in SA are non-specific, and several findings overlap with those found in AA, such as tapered hairs, pigtail hairs, and zigzag hairs.18 Currently, data regarding the comparison of trichoscopic characteristics between two conditions are limited. Therefore, this study aims to compare trichoscopic features between SA and AA and determine their discriminative ability.
Materials and Methods
Study Design and Ethical Consideration
This cross-sectional, analytic, retrospective study was employed in a university-based hospital (Ramathibodi Hospital, Bangkok, Thailand). The Institutional Review Board for Ethics in Human Research approved this study following the principles of the Declaration of Helsinki (MURA2022/521). The need for informed consent was waived, and data were analyzed anonymously.
Study Participants
Patients diagnosed with SA or AA attending hair clinic between January 2000 and February 2022 were included and classified into SA and AA groups for analysis. A minimum follow-up period of 6 months for each participant was required. SA diagnosis was made based on the following: (i) being diagnosed with syphilis according to criteria of Center for Disease Control;19,20 (ii) hair loss within 6 months after disease onset; (iii) significant hair regrowth within 6 months after antibiotic therapy; and (iv) histopathological features consistent with SA. For the AA group, biopsy-confirmed cases with age and hair loss pattern matched with SA patients were included in SA:AA ratio of 1:2 for comparison. Patients with clinical and investigational findings inconsistent with SA or AA, other concomitant hair and scalp disorders, and incomplete medical records were excluded.
Data Collection and Assessment
We retrospectively reviewed the medical records of all included participants. Data were extracted from the hospital’s electronic database. Baseline demographics, including age, sex, clinical characteristics, and duration of disease, were collected. Hair loss patterns of SA and AA were categorized into patch-type (localized non-scarring alopecic patch), reticular (multiple coalesced patches), diffuse (uniform hair loss over the entire scalp), and mixed ones (combination of patch-type and diffuse alopecia). Trichoscopic images of SA and AA were thoroughly reviewed by a hair specialist. Trichoscopic features were reported as the following: (i) hair shaft abnormalities (ie, upright regrowing hairs, hypopigmented hair shafts, broken hairs, pigtail hairs, exclamation mark hairs, tapered hairs, angulated/zigzag hairs, and non-pigmented regrowing hairs); (ii) follicular opening abnormalities (ie, yellow dots, black dots, and empty follicles); and (iii) scalp abnormalities (ie, erythematous background, telangiectasia, perifollicular scales, and interfollicular scales).
Statistical Analysis
Statistical analysis was performed using SPSS Statistics version 18 (SPSS Inc., Chicago, IL, USA). Continuous variables were expressed as mean ± standard deviation (SD) or median (interquartile range, IQR). Categorical variables were expressed as proportions. Differences of variables between SA and AA were determined using chi-square, Fisher’s exact test, Mann–Whitney U-test, or independent samples t-test, as appropriate. P<0.05 was considered statistically significant. The diagnostic ability of each trichoscopic sign in differentiating SA from AA was demonstrated as sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and likelihood ratio (LR) with corresponding 95% confidence intervals (CI). For the construction of receiver operating characteristics (ROC) curves, the relationship between the sensitivity and specificity of each trichoscopic feature was plotted, and the area under the ROC curve (AUC) was obtained to provide its discriminative ability.
Results
Demographics and Clinical Characteristics
Baseline demographics are summarized in Table 1. Twenty-three patients with SA and 46 patients with AA met the inclusion criteria. The mean ages at disease onset in AA and SA patients were 30.9 ± 9.1 and 27.6 ± 8.8 years, respectively (P=0.155). The median duration of disease was 1 (1–3) month in patients with SA, comparable to those with AA (2 [1–6] months; P=0.42). Male predominance was demonstrated in both group with 86.9% in SA and 76.1% in AA (P=0.29). The reticular type was the most common hair loss pattern (AA=18 [39.1%] vs SA=9 [39.1%]), followed by patch-type (AA=12 [26.1%] vs SA=6 [26.1%]), diffuse (AA=8 [17.4%] vs SA=4 [17.4%]), and mixed pattern (AA=8 [17.4%] vs SA=4 [17.4%]). No statistically significant differences in baseline characteristics between the two groups were observed.
 |
Table 1 Comparison of Baseline Characteristics Between Syphilitic Alopecia and Alopecia Areata |
Comparison of Trichoscopic Features
The trichoscopic signs observed in each group are summarized in Table 2. Regarding signs of hair shaft abnormalities, broken hairs (AA=60.9% vs SA=17.4%; P<0.001), pigtail hairs (AA=30.4% vs SA=8.7%; P=0.043), exclamation mark hairs (AA=67.4% vs SA=0%; P<0.001), tapered hairs (AA=60.9% vs SA=21.7%; P=0.002), angulated hairs (AA=26.1% vs SA=4.3%; P=0.029), and non-pigmented regrowing hairs (AA=34.8% vs SA=0%; P=0.004) were significantly more prevalent in AA than SA. Whereas upright regrowing hairs (AA=65.2% vs SA=60.9%; P=0.72) and hypopigmented hair shafts (AA=17.4% vs SA=26.1%; P=0.39) were both observed in SA and AA without statistically significant difference.
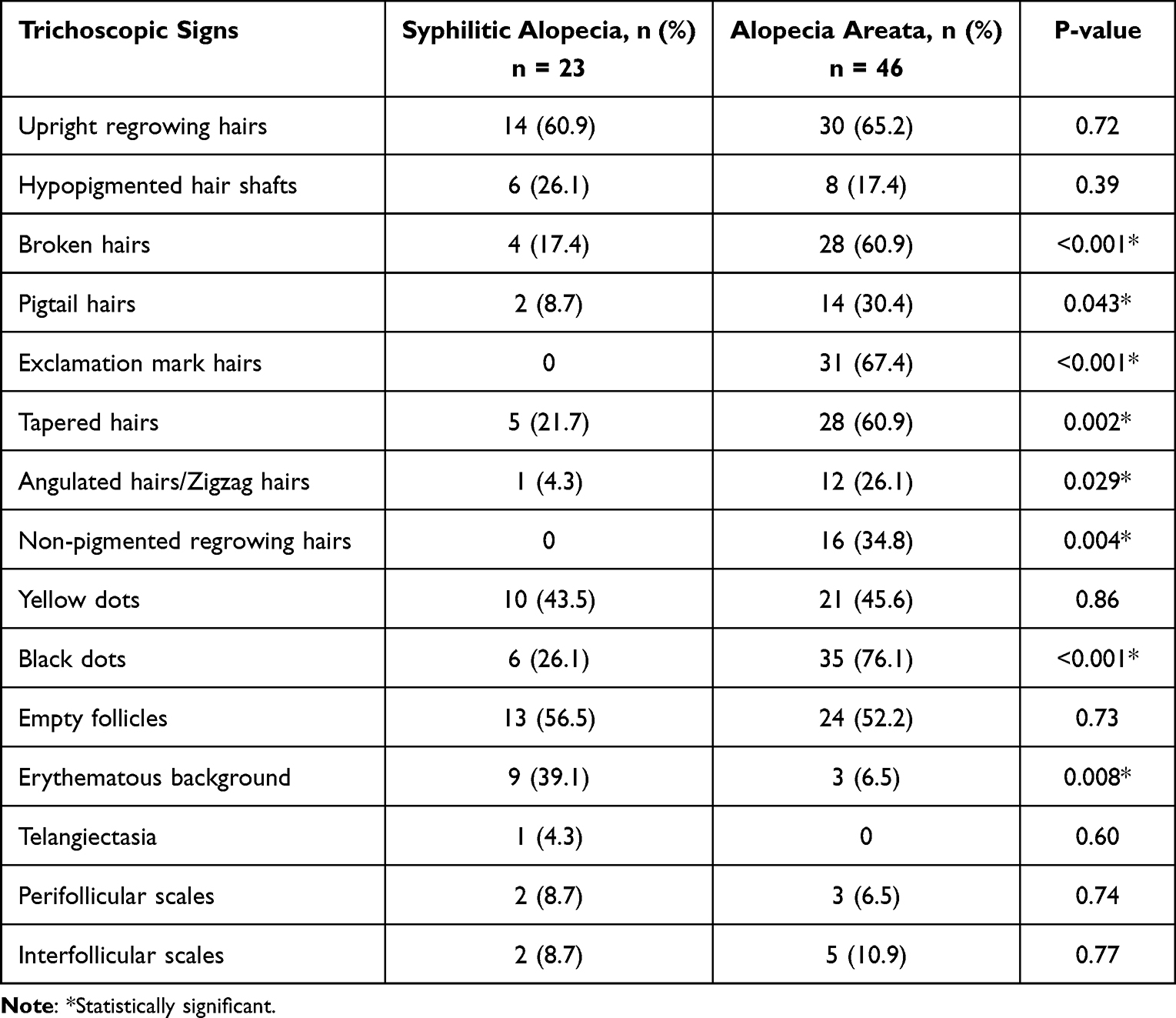 |
Table 2 Comparison of Trichoscopic Features Between Syphilitic Alopecia and Alopecia Areata |
In terms of follicular opening abnormalities, a significantly higher percentage of AA patients exhibit black dots compared to SA (AA=76.1% vs SA=26.1%; P<0.001), while the percentages of yellow dots (AA=45.6% vs SA=43.5%; P=0.86) and empty follicle (AA=52.2% vs SA=56.5%; P=0.73) observed in SA and AA groups were not different.
According to scalp abnormalities, the erythematous background was more prevalent in SA than in AA patients (AA=6.5% vs SA=39.1%; P=0.008), while the prevalence of telangiectasia (AA=0% vs SA=4.3%; P=0.6), perifollicular scales (AA=6.5% vs SA=8.7%; P=0.74), and interfollicular scales (AA=10.9% vs SA=8.7%; P=0.77) between groups was not different. Figures 1 and 2 demonstrate examples of trichoscopic features of SA and AA, respectively.
 |
Figure 1 Trichoscopic features of syphilitic alopecia (original magnification x20): (A) empty follicles (yellow circles) and erythematous background; (B) hypopigmented hair shafts (blue arrows) and erythematous background; (C) perifollicular scales, interfollicular scales, and erythematous background (green circle); (D) tapered hairs (red arrows), black dots (red star), and yellow dots (red circle). |
 |
Figure 2 Trichoscopic features of alopecia areata (original magnification x20): (A) exclamation mark hair (yellow arrow), angulated/zigzag hairs (yellow star), and hypopigmented hair shafts; (B) exclamation mark hair (blue arrow) and telangiectasia (blue circles); (C) angulated/zigzag hairs (green arrow) and black dots (green circles); (D) exclamation mark hairs, tapered hairs (red star), and non-pigmented regrowing hairs (red arrows). |
Discriminative Ability of Trichoscopy
Sensitivity, specificity, PPV, NPV, LR, and AUC for all trichoscopic features of SA and AA are demonstrated in Table 3 and Table 4, respectively. Exclamation mark hairs, angulated hairs, and non-pigmented regrowing hairs had considerably high specificity (exclamation mark hairs=95.83%, angulated hairs=95.65%, and non-pigmented regrowing hairs=95.83) and PPV (exclamation mark hairs=96.88%, angulated hairs=92.31%, and non-pigmented regrowing hairs=94.12%) for AA. Additionally, exclamation mark hairs and non-pigmented regrowing hairs also had a high positive LR for AA (exclamation mark hairs=16.17 and non-pigmented regrowing hairs=8.34); nevertheless, only exclamation mark hairs revealed high AUC (AUC=0.816). In contrast, features of scalp abnormalities showed significantly high specificity to SA (erythematous background=93.48%, telangiectasia=97.87%, perifollicular scales=93.48%, and interfollicular scales=89.13%). However, their PPV, NPV, LR, and AUC were inconsiderable. Other trichoscopic signs with comparable prevalence, namely upright regrowing hairs, hypopigmented hair shafts, yellow dots, empty follicles, telangiectasia, perifollicular scales, and interfollicular scales, had insignificant AUC values for both SA and AA.
 |
Table 3 Diagnostic Performance of Trichoscopy Toward Syphilitic Alopecia |
 |
Table 4 Diagnostic Performance of Trichoscopy Toward Alopecia Areata |
Discussion
SA and AA can manifest overlapping clinical and trichoscopic presentations, leading to diagnostic challenges. Our study indicates that despite the presence of several similar trichoscopic features between SA and AA, trichoscopy can provide additional diagnostic information that aids in differentiating between them. Exclamation mark hairs and non-pigmented regrowing hairs revealed significant positive LR, reporting their diagnostic values to specify AA patients correctly. Moreover, exclamation mark hairs showed considerable AUC value, being the best discriminative sign to differentiate AA from SA.
Diagnosis of SA is usually made upon clinical suspicion and serological test. Trichoscopic examination is increasingly used in diagnosing hair disorders, including SA, which was reported to have up to 40% increased rate of SA diagnosis.17 The present study reported trichoscopic features that were prevalently observed in SA, including upright regrowing hairs (60.9%), empty follicles (56.5%), yellow dots (43.5%), and erythematous background (39.1%). In comparison, black dots (76.1%), exclamation mark hairs (67.4%), upright regrowing hairs (65.2%), tapered hairs (60.9%), broken hairs (60.9%), empty follicles (52.2%), and yellow dots (45.6%) were frequently exhibited in AA. Results were consistent with those of previous studies that reported short regrowing hairs and black dots as the most prevalent trichoscopic signs for SA and AA, respectively.5,18,21–23 Moreover, our findings support that trichoscopic signs of SA are nonspecific and overlap with those of AA.18,23 Exclamation mark hairs, angulated hairs/zigzag hairs, and non-pigmented regrowing hairs provided high specificity and PPV of more than 90% towards AA. However, only exclamation mark hairs showed high AUC, which favored the diagnosis of AA over SA.
Our study is the first to compare the prevalence of each trichoscopic finding between SA and AA. Features representing hair shaft abnormalities, including broken hairs, pigtail hairs, exclamation mark hairs, tapered hairs, angulated hairs, non-pigmented regrowing hairs, and black dots, were significantly higher in AA compared to those in SA, whereas erythematous background, a feature of scalp abnormalities, was found to be significantly higher in SA than in AA. These findings indicate that AA mainly affects hair follicles, while the scalp is an additional area affected by SA other than hair follicles, corresponding to histopathological features of peribulbar infiltration in AA and inflammatory cells infiltration of the epidermis and dermis in SA.1,18
Treponema pallidum is found in the perivascular and peribulbar regions and sometimes penetrates the follicular matrix.24–29 Consequently, an immune reaction against treponemal antigens attacks hair follicles at the peribulbar region17,18,24–26,30–32 and may contribute to weakening affected hair shafts. Immune response against Treponema pallidum also causes small vessel vasculitis, which leads to subsequent loss of terminal hairs and arrest of the hair cycle.17,33 The aforementioned process may contribute to hair shaft abnormalities in SA that mimic clinical features of AA since both diseases share a pathogenic mechanism of inflammation at the bulb of hair follicles.26,34
Black dots, exclamation mark hairs, broken hairs, and angulated/zigzag hairs are considered a spectrum of clinical presentations arising from weakened hair shafts.35–38 Consequently, higher percentages of those signs observed in AA than in SA could be attributed to differences in intensity and duration of inflammatory reaction on hair follicles, with SA providing a lower degree of hair follicle disruption than AA. Notably, black dots and broken hairs were non-discriminative signs between SA and AA since they may occur following any mechanical trauma.38
Upright regrowing hairs, pigtail hairs, and non-pigmented regrowing hairs are trichoscopic features depicting hair regrowth.37 The prevalence of pigtail hairs in SA was significantly lower than in AA, though the feature was non-discriminative, while upright regrowing hairs, representing healthy regrowth hairs, appeared non-different. Our results were compatible with a previously reported incidence of pigtail hairs of 4–61%37 in AA and 4.9%18 in SA and an incidence of upright regrowing hairs of up to 96% in SA37 and 78% in AA.18 Since pigtail hairs represent rapid terminal hair regrowth with incomplete hair follicle recovery,39 these results may indicate a higher degree of follicular disruption in AA than in SA. Non-pigmented regrowing hairs refer to hair regrowth without follicular melanogenesis, and this characteristic is commonly found in AA. Our study confirmed this observation by exclusively reporting this sign in the AA group with high specificity. However, the diagnostic value of non-pigmented regrowing hairs for AA is limited in patients with grey hairs.
Trichoscopic features of scalp abnormalities in SA, including telangiectasia, perifollicular, and interfollicular scales, were presented almost as frequently in AA, except for significantly higher in the erythematous background, consistent with that reported in the previous literature.18,23 Erythematous background exhibited in SA was coherent with a higher degree of inflammation at the interfollicular area in SA compared to that in AA.40,41
The strength of our study is based on the fact that all included participants were biopsy-confirmed and analyzed based on matched cases. However, it was limited by its retrospective design and a relatively small number of cases. Our study was conducted at a single tertiary referral center in a homogeneous population, which may limit its generalizability. Future prospective, multicenter studies with a larger number of cases would be warranted to confirm our findings and better determine the discriminative ability of trichoscopy in differentiating SA and AA.
Conclusion
Our study is the first to compare trichoscopic features between SA and AA and evaluate their discriminative values in differentiating two diseases, emphasizing the diagnostic process of SA and AA using trichoscopy. A differential diagnosis between SA and AA should be considered in patients presenting with non-scarring alopecia. Although scalp biopsy provides a high diagnostic yield, trichoscopy remains an important investigative technique since it is a non-invasive, inexpensive, and less time-consuming method of distinguishing between SA and AA. The presence of hair shaft abnormalities favors clinical suspicion of AA; however, it is not definitively diagnostic, except for those who exhibit exclamation mark hairs, which reveal high discriminative ability for AA.
Data Sharing Statement
The data sets used to support the findings of this study are available from the corresponding author upon request.
Ethics Approval and Consent to Participate
This cross-sectional, analytic, retrospective study was employed in a university-based hospital (Ramathibodi Hospital, Bangkok, Thailand). The Institutional Review Board for Ethics in Human Research approved this study following the principles of the Declaration of Helsinki (MURA2022/521). The need for informed consent was waived, and data were analyzed anonymously.
Funding
No sources of funding were used to prepare this manuscript.
Disclosure
The authors declare that this manuscript was prepared in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Suchonwanit P, Kositkuljorn C, Pomsoong C. alopecia areata: an autoimmune disease of multiple players. Immunotargets Ther. 2021;10:299–312. doi:10.2147/ITT.S266409
2. Chanprapaph K, Mahasaksiri T, Kositkuljorn C, Leerunyakul K, Suchonwanit P. Prevalence and risk factors associated with the occurrence of autoimmune diseases in patients with alopecia areata. J Inflamm Res. 2021;14:4881–4891. doi:10.2147/JIR.S331579
3. Suchonwanit P, Kositkuljorn C, Mahasaksiri T, Leerunyakul K. A comparison of the efficacy and tolerability of three corticosteroid treatment regimens in patients with alopecia areata. J Dermatolog Treat. 2022;33(2):756–761. doi:10.1080/09546634.2020.1773384
4. Vafaie J, Weinberg JM, Smith B, Mizuguchi RS. Alopecia in association with sexually transmitted disease: a review. Cutis. 2005;76(6):361–366.
5. Tognetti L, Cinotti E, Perrot JL, Campoli M, Rubegni P. Syphilitic alopecia: uncommon trichoscopic findings. Dermatol Pract Concept. 2017;7(3):55–59. doi:10.5826/dpc.0703a12
6. Bi MY, Cohen PR, Robinson FW, Gray JM. Alopecia syphilitica-report of a patient with secondary syphilis presenting as moth-eaten alopecia and a review of its common mimickers. Dermatol Online J. 2009;15(10):6. doi:10.5070/D3390280M2
7. Pareek SS. Unusual location of syphilitic alopecia: a case report. Sex Transm Dis. 1982;9(1):43–44. doi:10.1097/00007435-198201000-00010
8. Safavi K. Prevalence of alopecia areata in the first national health and nutrition examination survey. Arch Dermatol. 1992;128(5):702. doi:10.1001/archderm.1992.01680150136027
9. Mirzoyev SA, Schrum AG, Davis MDP, Torgerson RR. Lifetime incidence risk of alopecia areata estimated at 2.1% by Rochester Epidemiology Project, 1990-2009. J Invest Dermatol. 2014;134(4):1141–1142. doi:10.1038/jid.2013.464
10. Chanprapaph K, Pomsoong C, Kositkuljorn C, Suchonwanit P. Intramuscular corticosteroid therapy in the treatment of alopecia areata: a time-to-event analysis. Drug Des Devel Ther. 2022;16:107–116. doi:10.2147/DDDT.S342179
11. Alkhalifah A. Alopecia areata update. Dermatol Clin. 2013;31(1):93–108. doi:10.1016/j.det.2012.08.010
12. Mahasaksiri T, Kositkuljorn C, Anuntrangsee T, Suchonwanit P. Application of topical immunotherapy in the treatment of alopecia areata: a review and update. Drug Des Devel Ther. 2021;15:1285–1298. doi:10.2147/DDDT.S297858
13. Rattananukrom T, Suchonwanit P. Are drug treatment strategies really effective against alopecia areata? Expert Opin Pharmacother. 2021;22(3):257–260. doi:10.1080/14656566.2020.1854728
14. Thadanipon K, Suchonwanit P. Measuring patient quality of life following treatment for Alopecia. Patient Prefer Adherence. 2021;15:1601–1610. doi:10.2147/PPA.S282399
15. Suchonwanit P, McMichael AJ. Alopecia in association with malignancy: a review. Am J Clin Dermatol. 2018;19(6):853–865. doi:10.1007/s40257-018-0378-1
16. Suchonwanit P, Iamsumang W, Leerunyakul K. Topical finasteride for the treatment of male androgenetic alopecia and female pattern hair loss: a review of the current literature. J Dermatolog Treat. 2022;33(2):643–648. doi:10.1080/09546634.2020.1782324
17. Piraccini BM, Broccoli A, Starace M, et al. Hair and scalp manifestations in secondary syphilis: epidemiology, clinical features and trichoscopy. Dermatology. 2015;231(2):171–176. doi:10.1159/000431314
18. Pomsoong C, Sukanjanapong S, Ratanapokasatit Y, Suchonwanit P. Epidemiological, clinical, and trichoscopic features of syphilitic alopecia: a retrospective analysis and systematic review. Front Med. 2022;9:890206. doi:10.3389/fmed.2022.890206
19. Hazra A, Collison MW, Davis AM. CDC sexually transmitted infections treatment guidelines, 2021. JAMA. 2022;327(9):870–871. doi:10.1001/jama.2022.1246
20. Workowski KA, Bolan GA. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep. 2015;64(Rr–03):1–137.
21. Doche I, Hordinsky MK, Valente NYS, Romiti R, Tosti A. Syphilitic alopecia: case reports and trichoscopic findings. Skin Appendage Disord. 2017;3(4):222–224. doi:10.1159/000477415
22. Vaccaro M, Macca L, Custurone P, Guarneri F. When hair loss is not just a cosmetic problem: moth-eaten alopecia in secondary syphilis. J Cosmet Dermatol. 2022;21(2):853–854. doi:10.1111/jocd.14105
23. Sun HY, Wong XL, Chen MKY, Sebaratnam DF. Trichoscopy of syphilitic alopecia: a systematic review. Sex Transm Infect. 2022;98(7):539–540. doi:10.1136/sextrans-2021-055302
24. Hernández-Bel P, Unamuno B, Sánchez-Carazo JL, Febrer I, Alegre V. Syphilitic alopecia: a report of 5 cases and a review of the literature. Actas Dermosifiliogr. 2013;104(6):512–517. doi:10.1016/j.ad.2012.02.009
25. Jordaan HF, Louw M. The moth-eaten alopecia of secondary syphilis. A histopathological study of 12 patients. Am J Dermatopathol. 1995;17(2):158–162. doi:10.1097/00000372-199504000-00008
26. Nam-Cha SH, Guhl G, Fernández-Peña P, Fraga J. Alopecia syphilitica with detection of Treponema pallidum in the hair follicle. J Cutan Pathol. 2007;34(Suppl 1):37–40. doi:10.1111/j.1600-0560.2006.00726.x
27. Lin YY, Tseng YS, Zhu W. Case of syphilis with alopecia and folliculitis as manifestations. Indian J Dermatol Venereol Leprol. 2021;87(1):125–256. doi:10.4103/ijdvl.IJDVL_336_18
28. Chanprapaph K, Sutharaphan T, Suchonwanit P. Scalp biophysical characteristics in males with androgenetic alopecia: a comparative study with healthy controls. Clin Interv Aging. 2021;16:781–787. doi:10.2147/CIA.S310178
29. Suchonwanit P, Triyangkulsri K, Ploydaeng M, Leerunyakul K. Assessing biophysical and physiological profiles of scalp seborrheic dermatitis in the Thai population. Biomed Res Int. 2019;2019:5128376. doi:10.1155/2019/5128376
30. Ciupińska M, Skibińska J, Sikora M, Blicharz L, Kotowska M, Rudnicka L. Nonscarring alopecia and hypopigmented lesions may be unusual signs of secondary syphilis. Skin Appendage Disord. 2021;7(3):203–205. doi:10.1159/000511577
31. Rattanakaemakorn P, Suchonwanit P. Scalp pruritus: review of the pathogenesis, diagnosis, and management. Biomed Res Int. 2019;2019:1268430. doi:10.1155/2019/1268430
32. Suchonwanit P, Leerunyakul K, Kositkuljorn C. Diagnostic and prognostic values of cutaneous manifestations in COVID-19. Dermatol Ther. 2020;33(4):e13650. doi:10.1111/dth.13650
33. Rebora A, Guarrera M. Teloptosis and kenogen: two new concepts in human trichology. Arch Dermatol. 2004;140(5):619–620. doi:10.1001/archderm.140.5.619
34. Bansal A, Relhan V, Garg VK, Saran RK. A cross-sectional study of the histopathology and immunology of alopecia areata: unearthing the role of the Janus kinase-signal transducer and activator of transcription pathway. Indian J Dermatol Venereol Leprol. 2019;85(5):455–461. doi:10.4103/ijdvl.IJDVL_738_17
35. Adya K, Inamadar A, Palit A, Shivanna R, Deshmukh N. Light microscopy of the hair: a simple tool to “untangle” hair disorders. Int J Trichology. 2011;3(1):46–56. doi:10.4103/0974-7753.82124
36. Rudnicka L, Olszewska M, Rakowska A, Slowinska M. Trichoscopy update 2011. J Dermatol Case Rep. 2011;5(4):82–88. doi:10.3315/jdcr.2011.1083
37. Waśkiel A, Rakowska A, Sikora M, Olszewska M, Rudnicka L. Trichoscopy of alopecia areata: an update. J Dermatol. 2018;45(6):692–700. doi:10.1111/1346-8138.14283
38. Khunkhet S, Vachiramon V, Suchonwanit P. Trichoscopic clues for diagnosis of alopecia areata and trichotillomania in Asians. Int J Dermatol. 2017;56(2):161–165. doi:10.1111/ijd.13453
39. Rudnicka L, Olszewska M, Rakowska A. Atlas of Trichoscopy: Dermoscopy in Hair and Scalp Disease. Springer Science & Business Media; 2012.
40. Alessandrini A, Starace M, Bruni F, et al. Alopecia areata incognita and diffuse alopecia areata: clinical, trichoscopic, histopathological, and therapeutic features of a 5-year study. Dermatol Pract Concept. 2019;9(4):272–277. doi:10.5826/dpc.0904a05
41. Hoang MP, High WA, Molberg KH. Secondary syphilis: a histologic and immunohistochemical evaluation. J Cutan Pathol. 2004;31(9):595–599. doi:10.1111/j.0303-6987.2004.00236.x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.