")
Back to Journals » Clinical Ophthalmology » Volume 16
Trends and Clinical Characteristics of Pediatric Patients Presenting to an Ophthalmology Emergency Department with an Initial Diagnosis of Optic Nerve Head Elevation
Authors Cavuoto KM, Markatia Z, Patel A, Osigian CJ
Received 12 March 2022
Accepted for publication 27 April 2022
Published 18 May 2022 Volume 2022:16 Pages 1525—1528
DOI https://doi.org/10.2147/OPTH.S366154
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Kara M Cavuoto, Zahra Markatia, Annika Patel, Carla J Osigian
Department of Ophthalmology, Bascom Palmer Eye Institute, University of Miami Miller School of Medicine, Miami, FL, USA
Correspondence: Kara M Cavuoto, Department of Ophthalmology, Bascom Palmer Eye Institute, University of Miami Miller School of Medicine, 900 NW 17th Street, Miami, FL, USA, 33136, Tel +1 305-326-6324, Fax +1 305-547-3675, Email [email protected]
Objective: Optic nerve head elevation may be the only clinical sign of a vision- and/or life-threatening condition, particularly in children who are asymptomatic or fail to report symptoms. The purpose of this study is to identify epidemiologic trends, clinical characteristics, and diagnostic outcomes of pediatric patients presenting to an ophthalmology emergency department (ED) with suspected optic nerve head elevation.
Methods: This retrospective study identified pediatric patients (≤ 18 years) presenting to an ophthalmology ED over a five- year period with suspected optic nerve head elevation to describe demographic trends, clinical characteristics, and diagnostic outcomes.
Results: Of the 213 patients, the majority were female (73.2%) and tended to be older than males (14.3 vs 11.2 years, p< 0.001). The most common diagnoses were papilledema (52.6%), pseudopapilledema (31.5%), and optic nerve drusen (8.0%). When symptoms were present, most (73.7%) patients presented with headache (67.5%) or visual disturbance (54.8%). Of 144 neuroimaging studies obtained, 80 (55.6%) had positive findings and these were significantly associated with symptoms at presentation (p=0.017) and age (p=0.034), but not sex (p=0.791). Asymptomatic females and children > 12 years old were more likely to have an abnormal MRI than males and children ≤ 12 (OR=1.56 and 1.22, respectively).
Conclusion: Patient demographics such as age and sex in conjunction with concurrent symptoms are important factors in determining the urgency of neuroimaging in children with suspected optic nerve head elevation.
Keywords: ophthalmology, pediatric, emergency department, optic nerve head elevation
Introduction
Optic nerve head elevation may be due to a variety of etiologies, including benign causes such as anatomic variants or high hyperopic refractive error. However, optic nerve head elevation may also be a sign of vision- or life-threatening conditions such as elevated intracranial pressure (ICP), idiopathic intracranial hypertension (IIH) or intracranial tumors.1–4 Although headache, nausea and/or visual disturbances can be present, children may be asymptomatic or fail to report symptoms5,6 and thus symptoms cannot be relied upon to conclusively determine the etiology. Given the potential vision- and life-threatening conditions that can cause optic nerve head elevation, this study aims to identify the demographic trends, clinical characteristics, and diagnostic outcomes of this finding in children presenting to an ophthalmology emergency department (ED).
Methods
This retrospective chart review was approved by the Institutional Review Board, adhered to the tenets of the Declaration of Helsinki, and complied with the Health Insurance Portability and Accountability Act. The medical records of all patients ≤18 years old who presented directly to an ophthalmology specific ED and were diagnosed by an ophthalmologist with optic nerve head elevation on dilated fundus examination between January 1, 2016, and October 31, 2020, were reviewed. Demographic data collected included age at time of visit, sex, chief complaint, clinical diagnosis at time of visit (by ICD-9 or ICD-10 code), referral status, and imaging results. Positive findings on imaging were defined as perioptic nerve sheath distension, optic nerve tortuosity, globe flattening, empty sella, demyelinating lesions and/or intracranial mass.
Statistical analysis was performed using SPSS. Both a Bayesian one-way ANOVA and a pairwise comparison of diagnoses were performed to study the relationship between age and diagnosis. Independent samples t-tests were used to compare age, sex, MRI outcomes and diagnoses. Odds ratios were used to compare the relationship between symptoms, sex, age and MRI findings.
Results
A total of 213 (73.2% female) patients were included. The average age at presentation was 13.5 + 3.6 years old (range 1.0 to 18.0 years old). Male patients tended to be younger than female patients (11.2 vs 14.3 years, p<0.001).
The most common diagnosis among patients presenting with suspected optic nerve head elevation was papilledema (52.6%, n=112), followed by pseudopapilledema (31.5%, n=67), optic nerve drusen (8.0%, n=17), optic neuritis (7.0%, n=15), and optic neuropathy (0.9%, n=2). The diagnoses by sex are detailed in Table 1.
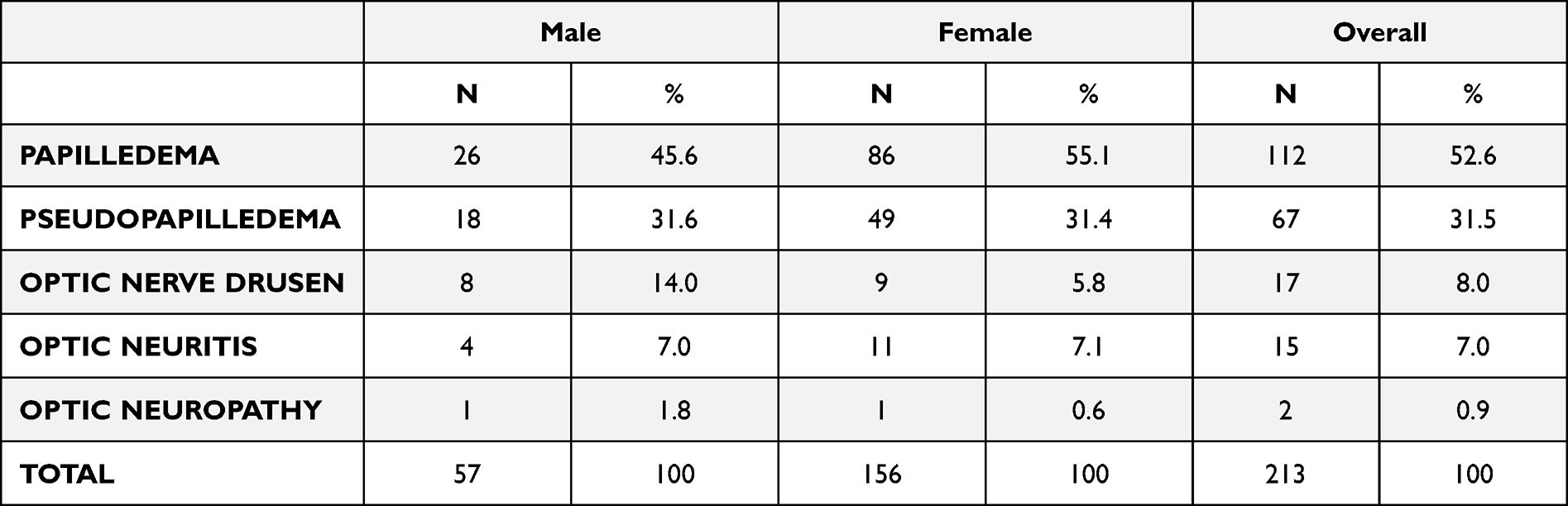 |
Table 1 Clinical Diagnoses in Pediatric Patients with Suspected Optic Nerve Head Elevation |
The mean age of patients diagnosed with papilledema was 13.9 ± 3.6 years old (n=112, range 1.0 to 18.0 years old). Overall, 86 (76.8%) were female with a mean age that was significantly older than males (14.6 vs 11.5 years, p=0.001). The second most common diagnosis was pseudopapilledema (31.5%, n=67). The mean age for these patients was slightly younger than patients with true papilledema at 13.1 ± 3.7 years old (range 4.0 to 18.0 years old). Similar to patients with papilledema, females with pseudopapilledema were significantly older than males (14.3 vs 9.7 years, p<0.001).
Of the population studied, 73.7% (n=157) of patients with suspected optic nerve head elevation presented with neurologic symptoms, of whom 52 (33.1%) reported two symptoms and 19 (12.1%) reported three or more symptoms. Symptomatic patients most commonly complained of headache (67.5%, n=106) and visual disturbances (54.8%, n=86), followed by pulsatile tinnitus (7.6%, n=12), vomiting (4.5%, n=7), and nausea (3.8%, n=6). The frequencies of reported neurologic symptoms overall and by sex can be found in Table 2.
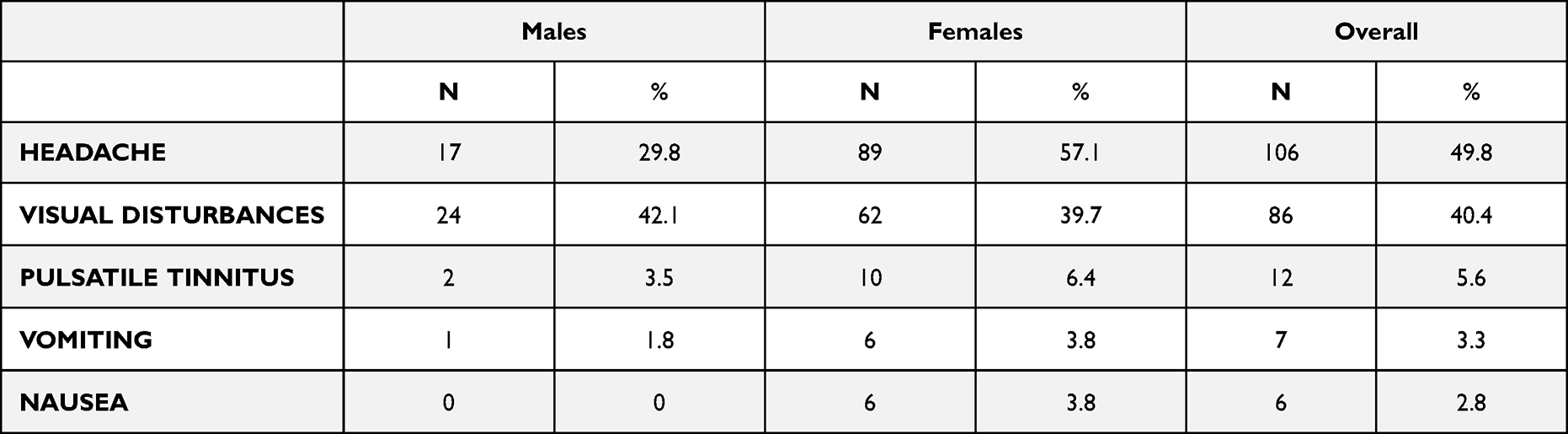 |
Table 2 Most Common Neurologic Symptoms by Sex in Pediatric Patients Presenting to the Emergency Department Diagnosed with Suspected Optic Nerve Head Elevation |
Of the 213 patients in the study, 67.6% underwent neuroimaging. Of the 144 neuroimaging studies, 80 (55.6%) had positive findings, the majority of which were consistent with findings of increased intracranial pressure causing papilledema (n=63, 78.8%). Of these, 59 (93.7%) supported a diagnosis of IIH and 4 (6.3%) demonstrated an intracranial mass, which included pilocytic astrocytoma (n=2), astrocytic hamartoma (n=1), and sphenoid mass (n=1). All patients with papilledema and positive MRI findings were symptomatic at presentation. Overall, positive MRI findings were significantly more common in symptomatic patients compared to asymptomatic patients (49.3%, n=71 vs 6.3%, n=9, p=0.017). Patients with positive findings on MRI were significantly older than patients with normal findings (14.6 vs 13.4 years old, p=0.034). Out of 56 asymptomatic patients, 23 (41.1%) were diagnosed with true papilledema. Although overall asymptomatic patients were approximately three times more likely to have a normal MRI than symptomatic patients (odds ratio [OR]=3.02), asymptomatic females and children >12 years old were more likely to have an abnormal MRI than males and children ≤12 years old (OR=1.56 and 1.22, respectively).
Discussion
Our study found that approximately half of children presenting with an initial diagnosis of optic nerve head elevation in the emergency department were diagnosed with papilledema, with a higher percentage of females than males (76.8% vs 23.2%). Additionally, our data demonstrated that the mean age of females was significantly older than males. These data align with prior studies that found that most patients with papilledema were females in early adolescence.4,7 However the sex and age trends were similar in children with both papilledema and pseudopapilledema, highlighting that age and sex alone cannot distinguish between these diagnoses.
One of the most concerning etiologies of optic nerve head elevation is an intracranial tumor. A study by Nuijts et al examining the ophthalmological findings in children presenting with primary brain tumors found that papilledema was present in nearly half (44.1%) of patients.8 In our study, tumors represented only 1.9% of our overall population and 6.3% of the patients with papilledema; conversely, all 4 patients with intracranial tumors presented with papilledema. Our overall prevalence was also lower than the 15.8% of children with papilledema who were diagnosed with tumors in a study by Hyde et. al.9 These differences may be due to the different inclusion criteria, age limits, type of centers (ophthalmology ED versus pediatric ophthalmology clinic) and geographic locations.
Nearly three-quarters of patients presented with symptoms. When symptoms were reported, headache was most commonly reported followed by visual disturbances, consistent with prior studies.4,5,7 However, 56 children in our study were asymptomatic at presentation. Despite the lack of symptoms, 41% of asymptomatic patients were diagnosed with papilledema. Although to a lesser degree, Yamamoto et al also found that 22 patients (13.3%) in their study did not present with symptoms such as headache but were found to have papilledema on examination.7 Furthermore, our study found asymptomatic females and children older than 12 years had a higher risk of positive findings on neuroimaging when compared to males and children under 12 years. This may suggest a lower threshold for neuroimaging should be emphasized in patients in certain demographic groups despite the lack of symptoms. This is important to note, as prior literature suggests that asymptomatic patients with typical IIH demographics may not need urgent neuroimaging.4
The limitations of this study include the retrospective nature of the methodology and the identification of patients by the ICD-9 or ICD-10 diagnosis in the electronic medical records. Also, the decision to perform neuroimaging in the ED was at the discretion of the physician evaluating the patient. Additionally, some patients may have obtained neuroimaging and followed up at an outside facility or with an outside provider. Finally, the data includes patients at one institution, which may not represent other patient populations, geographic locations or ophthalmologic points of care.
In conclusion, half of the children with optic nerve head elevation were diagnosed with papilledema. Symptoms such as headache or visual disturbances may help determine which patients should undergo urgent neuroimaging, however asymptomatic patients may still have papilledema. Therefore clinicians should weigh age at presentation, sex, and associated symptoms as well as the clinical index of suspicion to determine the urgency of neuroimaging in children with suspected optic nerve head elevation.
Abbreviations
ED, emergency department; ON, optic nerve; ICP, intracranial pressure; IIH, idiopathic intracranial hypertension.
Ethics Approval and Consent to Participate
This cross-sectional study was approved by the Institutional Review Board at the University of Miami, complied with the Health Insurance Portability and Accountability Act, and adhered to the tenets of the Declaration of Helsinki.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
KC, ZM, AP, and CO report no conflicts of interest in this work.
References
1. Freund P, Margolin E. Pseudopapilledema. StatPearls; 2021.
2. Lyons CJ, Wiwatwongwana A. The optic nerve and visual pathways. Handb Clin Neurol. 2013;113:1515–1525.
3. Chen JJ, Bhatti MT. Papilledema. Int Ophthalmol Clin. 2019;59(3):3–22. doi:10.1097/IIO.0000000000000274
4. Crum OM, Kilgore KP, Sharma R, et al. Etiology of Papilledema in Patients in the Eye Clinic Setting. JAMA Netw Open. 2020;3(6):e206625. doi:10.1001/jamanetworkopen.2020.6625
5. Maheswaran M, Dheera MS, Kumar M, Kowsalya A. Pediatric Papilledema at a Tertiary Care Ophthalmological Center. Indian Pediatr. 2020;57(10):966–967. doi:10.1007/s13312-020-2006-4
6. Heidary G. Pediatric Papilledema: review and a Clinical Care Algorithm. Int Ophthalmol Clin. 2018;58(4):1–9. doi:10.1097/IIO.0000000000000242
7. Yamamoto E, Farber D, Rothner D, Moodley M. Assessment of Pediatric Pseudotumor Cerebri Clinical Characteristics and Outcomes. J Child Neurol. 2021;36(5):341–349. doi:10.1177/0883073820972231
8. Nuijts MA, Stegeman I, Porro GL, et al. Ophthalmological Evaluation in Children Presenting With a Primary Brain Tumor. J Neuroophthalmol. 2021;1:548. doi:10.1097/WNO.0000000000001421
9. Hyde RA, Mocan MC, Sheth U, Kaufman L. Evaluation of the underlying causes of papilledema in children. Can J Ophthalmol. 2019;54(6):653–658. doi:10.1016/j.jcjo.2019.02.007
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.