Back to Journals » Infection and Drug Resistance » Volume 13
Trend and Characteristics of Acinetobacter baumannii Infections in Patients Attending Universal College of Medical Sciences, Bhairahawa, Western Nepal: A Longitudinal Study of 2018
Authors Raut S ![]() , Rijal KR
, Rijal KR ![]() , Khatiwada S
, Khatiwada S ![]() , Karna S
, Karna S ![]() , Khanal R, Adhikari J, Adhikari B
, Khanal R, Adhikari J, Adhikari B ![]()
Received 16 April 2020
Accepted for publication 17 May 2020
Published 8 June 2020 Volume 2020:13 Pages 1631—1641
DOI https://doi.org/10.2147/IDR.S257851
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Shristi Raut,1 Komal Raj Rijal,2 Sulochana Khatiwada,1 Subash Karna,1 Rita Khanal,1 Janak Adhikari,3 Bipin Adhikari4
1Department of Microbiology, Universal College of Medical Sciences, Bhairahawa, Nepal; 2Central Department of Microbiology, Tribhuvan University, Kirtipur, Kathmandu, Nepal; 3B.P. Koirala Institute of Health Sciences, Dharan, Nepal; 4Centre for Tropical Medicine and Global Health, Nuffield Department of Medicine, University of Oxford, Oxford, UK
Correspondence: Shristi Raut Email [email protected]
Background: Acinetobacter baumannii is one of the major organisms causing nosocomial infections and is intrinsically resistant to multiple classes of antibiotics. The main objective of this study was to investigate the trend and characteristics of A. baumannii infections including its resistance pattern among patients attending Universal College of Medical Sciences, Teaching Hospital (UCMSTH) in Western Nepal, between January and December 2018.
Patients and Methods: A total of 4862 clinical samples received at the microbiology laboratory of UCMSTH over a period of a year were analyzed. Following bacterial culture on the samples, culture-positive isolates were tested for antibiotic susceptibility using a modified Kirby–Bauer method. The demographic profile of the patient, information about samples, and the antibiotic profile of the A. baumannii isolated from different samples were recorded and analyzed.
Results: A total of 1180 (24.2%; 1180/4862) organisms were isolated from the total samples. Acinetobacter baumannii (12.4%; 147/1180) was the third most common organism. Prevalence of A. baumannii was found to be high in late summer/early winter (July: 15.9%; 18/113 and December: 18.8%; 13/69). The majority 71.4% (n=105) of A. baumannii isolates were multidrug resistant (MDR). None of the isolate was pan-drug resistant. Colistin, polymyxin B, and tigecycline were 100% sensitive to A. baumannii. MDR bacteria were significantly associated with the gender of the patients [female: 51.4% (54/105) versus male: 48.6% (51/105); p=0.05], clinical specimens [swab: 40% (42/105) sputum: 21.9% (23/105) and urine: 10.5% (11/105); p=0.02] and different wards of the hospital [surgery: 30.5% (32/105); ICU: 21.9% (23/105) and medicine: 19.0% (20/105); p< 0.03].
Conclusion: The high burden of MDR Acinetobacter isolates in clinical specimens shows an alarming presence of antimicrobial resistance. Two-thirds of the specimens showed MDR and were associated with demographic and clinical characteristics of the patients. In the management of infectious diseases at UCMSTH, there should be a high suspicion of Acinetobacter infection, and isolation and treatment should be carried out based on an antibiotic susceptibility test.
Keywords: Acinetobacter baumannii, culture, antibiotic profile, multidrug resistance
Introduction
The burden of antimicrobial resistance (AMR) in developing countries is disproportionately higher and is attributed to the high prevalence of infectious diseases, poor hygiene, and fragile health systems.1 A major challenge in developing countries is due to a high proportion of hospital-acquired infections that continue to affect the treatment outcomes and development of AMR.2 More than 10 million deaths are projected to be caused by AMR by 2050 if the current situations of AMR continue uncontrolled.3
ESKAPE bacterial pathogens, i.e. Enterococcus faecium, Staphylococcus aureus, Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa, and Enterobacteriaceae are the most important bacterial pathogens with a high propensity to develop AMR.4 Of these bacterial pathogens, A. baumannii is one of the most challenging bacterial pathogens because of its unique antibiotic resistance characteristics.5 The genus Acinetobacter includes non-lactose-fermenting, catalase-positive, non-motile, non-fastidious, oxidase-negative, and aerobic Gram-negative coccobacilli. A. baumannii is clinically very significant because it is involved with nosocomial infections and is intrinsically resistant to wider classes of antimicrobials with a high propensity to developing resistance. The unique ability of Acinetobacter to survive desiccation renders its viability in inanimate objects for months and thus facilitates its spread in the hospital. Multidrug-resistant Acinetobacter spp. has been associated with prolonged hospital admissions, morbidity, and deaths.6,7
More than 20 Acinetobacter species have been reported to date. One of the commonest Acinetobacter species in clinical settings is A. baumannii,8,9 which causes a variety of infections including respiratory tract infection, bacteremia, meningitis, and wound infection. Virulence factors of these organisms causing such infections include outer membrane porins, capsule, lipopolysaccharides, phospholipase D, iron acquisition systems, and regulatory proteins.10 Multidrug-resistant A. baumannii is recognized to cause life-threatening infections with limited therapeutic options. It is also developing resistance to the remaining drugs used to treat these infections, such as the carbapenem group of antibiotics. In recent years, the numbers of reported carbapenem-resistant Acinetobacter spp. are increasing, which has further narrowed the treatment options. There are only a few drugs such as colistin, polymyxin B, and tigecycline currently effective for multidrug-resistant Acinetobacter spp.11
In recent years, increasing numbers of multidrug-resistant infections by Acinetobacter species have been reported from tertiary hospitals of Nepal.12–14 Rapid growth of MDR Acinetobacter infections, particularly contributing to nosocomial infections, with limited and expensive drugs available for treatment in economically underprivileged countries, are major challenges.15 Despite its high prevalence, poor clinical suspicion and high empiric treatment without diagnosis even in tertiary care centers in Nepal are significant clinical challenges ultimately contributing to AMR.16 Few previous studies have explored the prevalence of Acinetobacter infections in hospitalized patients.12–14 Reported prevalence ranged from 12.5% to 71.3% in Nepal Medical College, Teaching Hospital;17 12.7% in Norvic Hospital;13 35.9% in B&B Hospital,14 and 49.6% in Tribhuvan University Teaching Hospital.18 These studies were concentrated in Kathmandu and none in our knowledge investigated the longitudinal data for a year. The main objective of this study was to investigate the monthly trend and prevalence of MDR A. baumannii including its antimicrobial susceptibility patterns in various clinical samples received in the Microbiology Laboratory of UCMSTH, Bhairahawa, Nepal.
Patients and Methods
Study Design, Setting, and Sample
A longitudinal, hospital-based study was conducted at Universal College of Medical Sciences, and the study population comprised patients aged between 0 and 95 years who attended the hospital for treatment.
A total of 4862 different clinical specimens were collected following a standard protocol for pediatric (below 15 years of age) and adult patients between January and December 2018. Informed consent and assent (from parents) in case of children were received for the study.
A total of 1180 organisms isolated were included in the study. Samples included urine (n=434), wound swabs (n=303), pus (n=215), blood (n=117), sputum (n=82), endotracheal tip (n=9), fluid (n=13), and others (n=4) and were analyzed using various microbiological methods.19
Sample Collection
Urine samples from children who were not able to use the toilet on their own were collected using an adhesive, sealed, sterile collection bag assisted by their parents and a lab assistant. Children who could use the toilet on their own were asked to collect the mid-stream urine in a sterile, dry, leak-proof container assisted by their parents as and when needed. Genitalia was cleaned using an alcohol swab before and after the collection of samples to reduce contamination.
Pus from infected wounds was aspirated using a syringe by trained medical personnel. For non-oozing wounds, a cotton swab was rolled over the surface of the wound for a minimum of five times. Swabs from each patient were tested for culture and Gram staining.
Around 2 mL of blood was collected in sterile culture bottles containing BHI (Brain Heart Infusion) broth. Similarly, specimens were also collected from endotracheal and catheter tips. After labeling the collected samples, they were transferred to a laboratory for further processing maintaining a cold chain maintenance.20
Laboratory Examinations
Culture
Methodologies outlined in standard microbiological guidelines were utilized to process the samples.19,21
Urine Sample
A sterile-calibrated loop was used to inoculate urine samples on MacConkey agar (MA) and blood agar (BA), and they were incubated at 37°C for 24 h. Colony count ≥105 colony forming units (CFU)/mL of urine was considered positive based on the Kass, Marple, and Sanford criteria.21
Blood Sample
Brain heart infusion (BHI) broth was used for incubation (at 37̊C for 7 days) of blood samples. Samples showing turbidity were sub-cultured in MacConkey and blood agar at 37̊C for 24–48 h.
Pus, Wound Swab
MA and BA plates were used for the inoculation of specimens and were incubated at 37̊C overnight.
Other Specimens
At first, the specimens from endotracheal and catheter tips were incubated on BHI broth at 37̊C for 24 h and were later sub-cultured on MA and BA plates.
Identification of Bacterial Isolates and Acinetobacter baumanii
Preliminary identification of bacterial isolates was based on the colony morphology and Gram staining reaction. Thus, the identified isolates underwent biochemical tests (indole, methyl red, Voges Prausker, citrate, triple sugar iron agar, oxidative/fermentative, urease test, coagulase test, catalase, and oxidase test for confirmation).19,21 Acinetobacter baumannii was confirmed by various phenotypic tests that included: Gram-negative coccobacilli, catalase positive, oxidase negative, non-fastidious, non-fermentative (oxidative), gas negative, H2S negative, hemolysis negative, growth at 44°C, nitrate reduction negative, urease negative, indole negative, methyl red positive, Voges-Proskauer negative, citrate positive, and utilization 10% lactose positive.22
Antibiotic Susceptibility Test (AST)
All the isolates of A. baumannii were investigated for AST against ampicillin (10 μg), amikacin (30 μg), amoxiclav (30/10 μg), cefepime (30 μg), cefotaxime (30 μg), ceftriaxone (30 μg), cefoperazone-sulbactam (75/30 μg), doxycycline (30 μg), levofloxacin (5 μg), gentamicin (10 μg), imipenem (10 μg), piperacillin/tazobactam (100/10 μg), polymyxin B (300 units), tobramycin (10 μg), tetracycline (30 μg), and tigecycline (15 μg) (Hi-Media India Pvt. Ltd) following the Kirby–Bauer method on Mueller–Hinton agar. A suspension of the test organism was prepared in peptone water and matched to 0.5 McFarland standard for AST. With the help of a sterile cotton swab, lawn culture of the suspension was made on a Mueller–Hinton agar plate. Antibiotic discs were placed on MHA maintaining a 25 mm distance between two discs and were incubated at 37֯C for 24 h. After 24 h, the zone of inhibition was measured for each antibiotic, and results were interpreted as sensitive, intermediate, and resistant on the basis of CLSI guidelines, 2018.23 Isolates not susceptible to ≥3 antibiotic classes were categorized as multidrug resistant.24 MDR was defined as the development of resistance to at least one agent in three or more of the following five antimicrobial groups: 1) cephalosporins (ceftazidime or cefepime), 2) carbapenems (imipenem or meropenem), 3) ampicillin-sulbactam, 4) fluoroquinolones (ciprofloxacin or levofloxacin), and 5) aminoglycosides (gentamicin, tobramycin, amikacin, netilmicin).24
Quality Control
All media and reagents used in this study were tested and verified for sterility and performance. For AST, the quality was assured using the control strains of E. coli ATCC 25922 and S. aureus ATCC 25923.
Data Management and Statistical Analysis
At first, all raw data were entered into a Microsoft Excel spreadsheet from the laboratory’s microbiological register. All data were compared and cross-checked for consistency against the register to remove the aberrant and outlying data. Cleaned Excel spreadsheet data were then exported into SPSS 21 version IBM SPSS Statistics for Windows, Armonk, NY: IBM Corp. Figures 1 and 2 were made in Microsoft Excel. Descriptive and inferential analyses were conducted. A chi-squared test was used to measure the association between the variables.
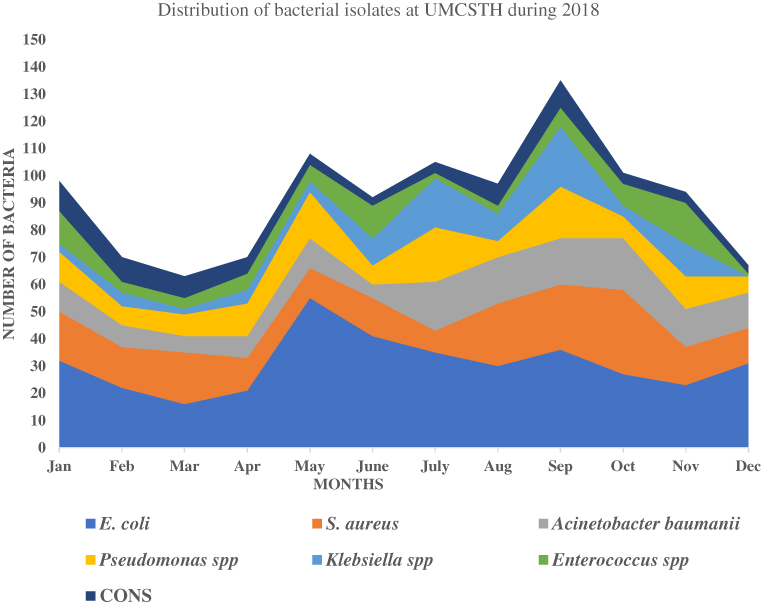 |
Figure 1 Distribution of top seven bacterial genera at UMCSTH during 2018. |
 |
Figure 2 Month wise trend of Acinetobacter baumannii among total bacterial isolates at UMCS. |
Result
Bacterial Isolates
A total of 4862 samples were received in the microbiology laboratory of UCMSTH in 2018 for culture and sensitivity. From 4862 samples, 1180 (24.2%; 1180/4862) organisms were isolated. The most common organisms isolated were E. coli (369/1180; 31.2%) followed by S. aureus (202/1180; 17.1%). A. baumannii (147/1180; 12.4%) was the third most common organism isolated from a variety of samples. The highest number of A. baumannii isolates (33.3%; 49/147) was recovered from swab cultures, followed by sputum cultures (21.1%; 31/147) (Table 1).
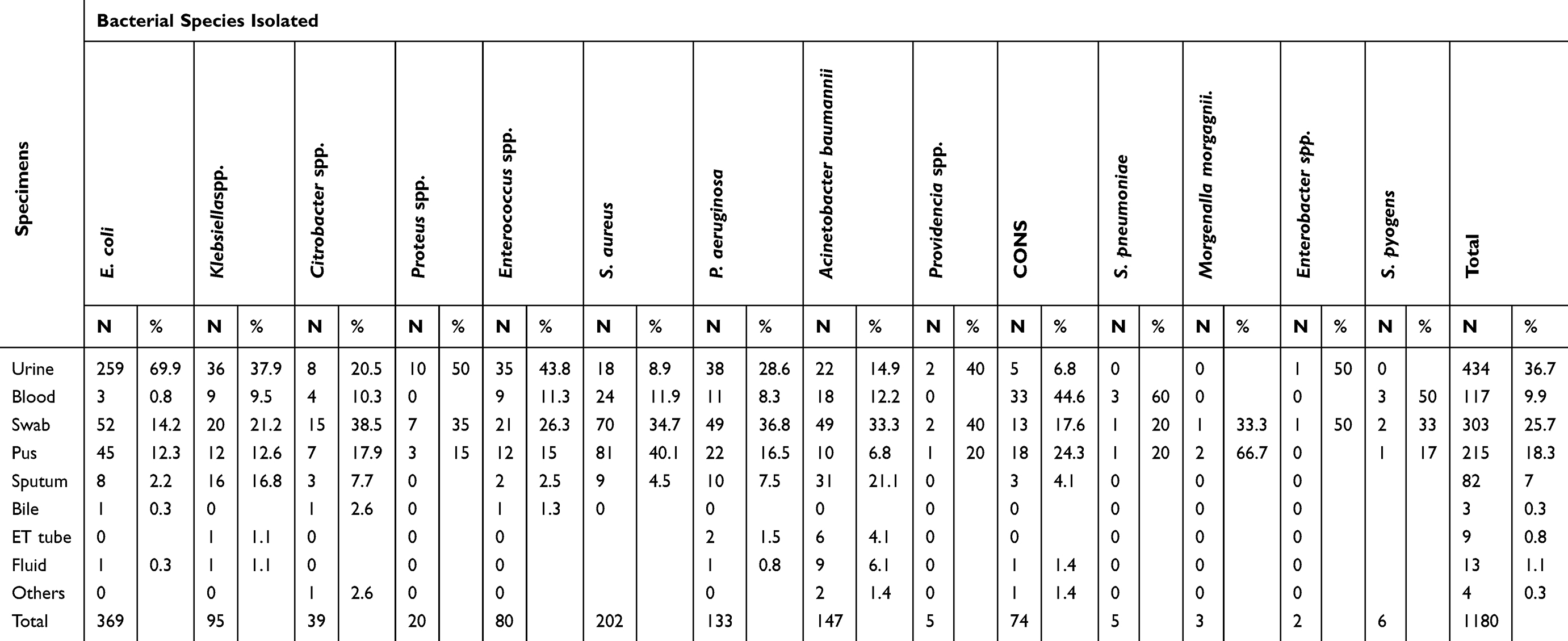 |
Table 1 Distribution of Bacterial Isolates in Different Clinical Specimens (n=1180) |
Month-Wise Distribution of Acinetobacter baumanii at UCMS During 2018
E. coli (n=369) was the most predominant organism isolated, followed by S. aureus (n=202), whereas Providencia spp. (n=5), Morganella spp. (n=3) and Enterobacter spp. (n= 2) were the least isolated bacterial pathogens in UCMS during 2018 (Figure 1). The highest numbers of bacterial pathogens were isolated in September (11.9%; 140/1180) followed by May (9.9%; 117/1180) and July (9.5%; 113/1180) (Table 2). However, the highest burden of A. baumannii was found in December (18.8%; 13/69) followed by August (16.8%; 17/101). The lowest burden of A. baumannii was seen in the months of March (7.5%; 6/80) and June (5.2%; 11/117) (Figure 2).
 |
Table 2 Month Wise Distribution of Bacterial Pathogens at UCMS in 2018 (n=1180) |
Antibiotic Susceptibility Patterns
Out of 147 A. baumannii isolates, 71.42% (n=105) were MDR. None of the isolate was pan-drug resistant. Colistin, polymyxin B, and tigecycline are the reserve drugs for the treatment of MDR A. baumannii as it is 100% sensitive to these drugs. Other than these antibiotics, the carbapenem group of drugs such as meropenem and imipenem are the drugs of choice to treat life-threatening infections by A. baumannii (Table 3).
 |
Table 3 Antibiotic Susceptibility of MDR Acinetobacter baumannii Isolates (n=147) |
Distribution of MDR A. baumannii Cases in Relation to Gender and Age of the Patients
A significant association was observed between gender of the patients (female: 51.4%; 54/105 versus male: 48.6%; 51/105; p=0.05) and MDR bacteria (Table 4). More than half of the patients (53.3%; 56/105) in the age group 16–45 years had an infection by A. baumannii, of which 70% (56/80) were MDR. No association was found between the age and development of MDR (p>0.05) (Table 4).
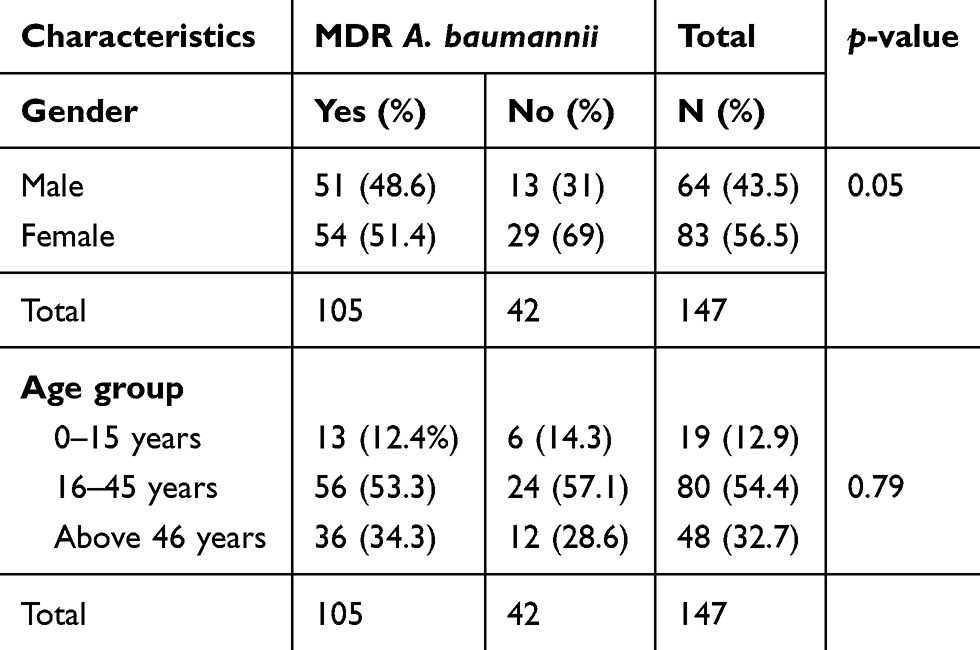 |
Table 4 MDR Acinetobacter baumannii Cases According to Gender and Age of Patient |
MDR Acinetobacter baumannii in Different Clinical Specimens and Wards of Hospital
One-third of the isolates of A. baumannii (32.7%; 48/147) were isolated from swab specimens; the next highest source was sputum (21.8%; 32/147). Of 48 isolates, 87.5% (42/48) were MDR A. baumannii. There was a significant association between the clinical specimens and isolation of MDR A. baumannii (p<0.05) (Table 5).
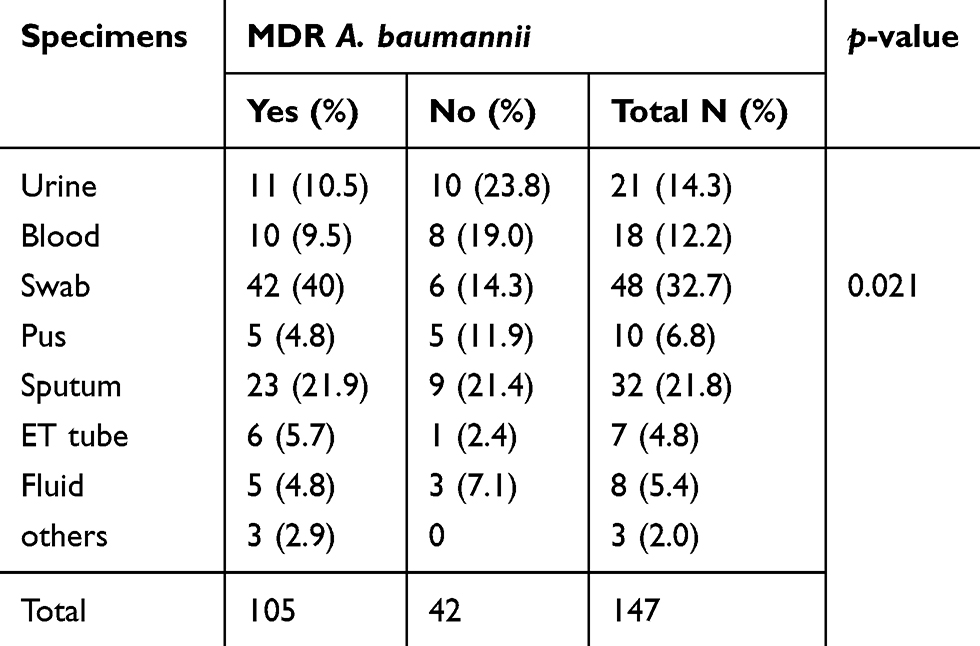 |
Table 5 Sample Wise Distribution of MDR Acinetobacter baumannii |
Out of 147 isolates, 26.5% (39/147) were isolated from the surgery ward followed by the medicine ward (21.1%; 31/147). Out of 39 isolates, 82% (32/39) were MDR A. baumannii in the surgery ward, whereas 64.5% (20/31) were MDR in the medicine ward. There was a significant association between the isolation of bacteria in different wards of the hospital and MDR A. baumannii (p<0.03) (Table 6).
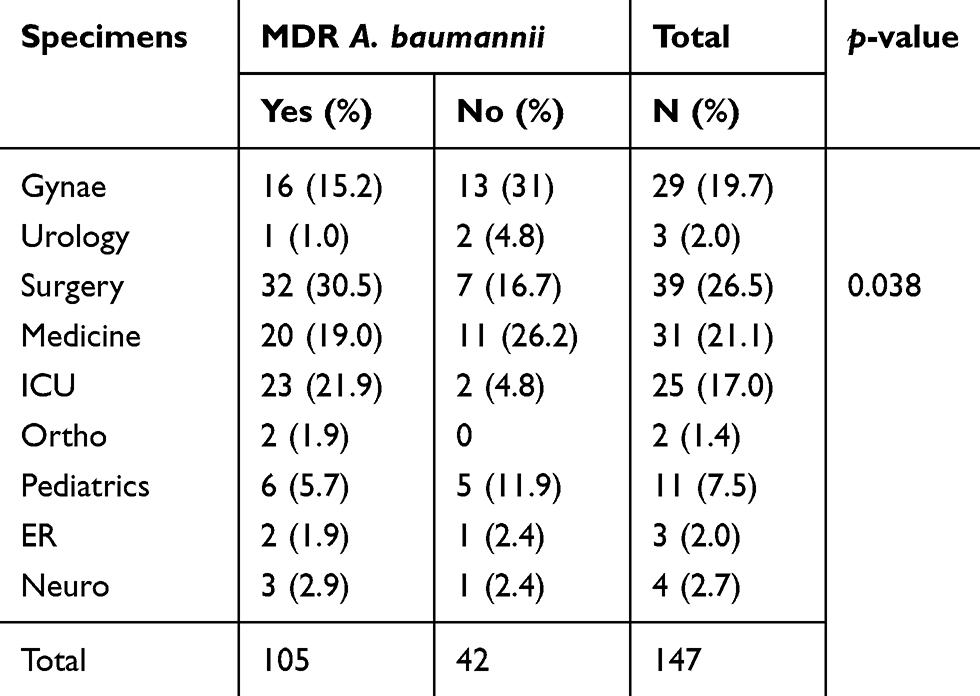 |
Table 6 Ward Wise Distribution of MDR Acinetobacter baumannii |
Discussion
Overall Findings
One-fourth of the clinical samples received in the microbiology laboratory of UMCSTH showed bacterial growth during 2018. In this study, the most common bacteria from clinical specimens were E. coli followed by S. aureus, A. baumannii, Pseudomonas spp. and Klebsiella spp. The prevalence of these organisms was similar to a recent study conducted at a tertiary care hospital in Kathmandu where Acinetobacterspecies were the third most common organism after E. coli and Klebsiella species.13 Two-thirds of the specimens showed MDR, and they were associated with female gender, surgery & medicine ward, and specimens from swab & sputum. Our findings agree with the past studies conducted in various settings of Nepal.25–27 Patterns of bacterial genera identified in this study were similar to a study conducted in India28 and Iran.29 The most common infections in the hospital were urinary tract infections, bacteremia, and surgical wounds. The presence and predominance of particular pathogens in this study may have been affected by the types of patients, their illnesses, device utilization rates, and the empirical antibiotic usage patterns.30
In our study, the prevalence of Acinetobacter infections was 12.5% among all the clinical specimens received during 2018. The findings in this study are consistent with past studies reported from Nepal.13,17 Acinetobacter spp. were the third most common organisms isolated from the samples in our study and were common during late summer and early winter months, a phenomenon commonly referred to as seasonality,31 resonating with previous longitudinal studies.32 Nonetheless, the seasonality was variable between settings and studies and the mechanisms mediating seasonality remain unclear.33
Acinetobacter spp. can remain as a dormant pathogen as it is widely prevalent in the environment and has substantial capacity to colonize. A. baumannii constituted almost half (41.8%) of all the nosocomial infections in India34 and has been shown to infect almost all the human organs. In this study, the highest number of Acinetobacter baumanii was isolated from swab culture (33.3%), followed by sputum (21.1%) and urine culture (14.9%) respectively. This difference in the sample might be due to size, sources, types of sample, antibiotic usages, and infection control practice in the hospital, which can affect the isolation rate of bacteria from different clinical specimens.17,35,36
MDR Acinetobacter baumannii
In our study, the prevalence of MDR A. baumannii was 71.4% among various clinical specimens. These findings agree with the past similar studies conducted in Kathmandu,17 India,37 and Lebanon.38 Misuse of broad-spectrum antibiotics including carbapenem has been attributed as one of the major factors for the global rise in MDR A. baumannii.35 The availability of antimicrobials over the counter (OTC) in Nepal is a major challenge and continues to add to the development of antimicrobial resistance.1,39 An Iranian study found an increase of MDR A. baumannii from 50% to 94% in the period between 2001 and 2011.40
More than 90% of Acinetobacter baumannii was found to be resistant to antibiotics: ampicillin, ciprofloxacin, ceftriaxone, cefotaxime, cefoperazone, cefepime, and amoxiclav. Similar patterns of resistance were reported from a tertiary teaching hospital in Kathmandu.41 We found a high resistance of Acinetobacter not only in the β-lactam antibiotics but also among fluoroquinolones: ciprofloxacin (87%). The findings are consistent with previous studies reported from India42 and Italy.43
Fluoroquinolones are extensively used as broad-spectrum antibiotics for the treatment of wide varieties of bacterial diseases and are a significant contributor to the rapid increase in resistance over the years.42 Furthermore, a high rate of resistance to fluoroquinolones is due to the presence of R-plasmids bacterium, which acts as a reservoir of multidrug resistance.44 Carbapenems were used for the treatment of Acinetobacter infections in the late 1990s.45 However, globally, the rapid pace of development of resistant strains prompted scientists and clinicians to change the treatment regimens of Acinetobacter infections. In the current study, 34% of Acinetobacter were resistant to imipenem and 20% were resistant to meropenem. These findings are concordant with reports from Delhi, India,46 Nepal,41 and Banglore, India.47
Imipenem-resistant Acinetobacter spp. in nosocomial infections, particularly in an intensive care unit (ICU), has been reported to be endemic in a tertiary care hospital in India.37 A combination of reserved drugs such as colistin, polymyxin B, and tigecycline is the only remaining treatment option to treat carbapenem-resistant cases.11 As Acinetobacter baumannii can easily survive in hospital settings, it has a high potential to spread among inpatients in ICU.11
In our study, three reserved drugs that included colistin, polymyxin B, and tigecycline were 100% effective on Acinetobacter spp. However, in a few studies, tigecycline was also reported to be ineffective on Acinetobacter spp.48,49 Colistin was widely used to treat MDR strains, because of its proven activity.50,51 Various studies have shown a 57–77% cure rate of colistin in severely ill patients infected by Acinetobacter species.52
Implications for Clinical Management of Acinetobacter Infections in a Tertiary Hospital
Acinetobacter species are known to cause nosocomial infections and are mostly multidrug resistant. In this study, Acinetobacter species were the third most common organism isolated. In addition, the high survival advantage of Acinetobacter spp. in a hospital environment with efficient transmissibility among the patients renders it as one of the dangerous pathogens with limited treatment options. Thus, clinicians working in infectious diseases should have a high suspicion for Acinetobacter infections, reduce the empiric management with broad-spectrum antibiotics, and follow the antibiotic sensitivity for appropriate treatment. In particular, the demographic and clinical characteristics of patients with MDR Acinetobacter spp. can provide clues for the management of these infections. The high risk of MDR infections among females and patients admitted to major wards such as surgery, ICU, and medicine, including specific samples such as swab, sputum, and urine are only precursors for clinicians to pay particular attention in making clinical suspicion, diagnosis, and management based on antibiotic susceptibility tests. As Acinetobacter infections can persist for a prolonged period on animate and inanimate objects, tertiary hospitals should consider sustainable management of these infections by maintaining hospital hygiene, strict decontamination and aseptic measures, and coordination and collaboration between various departments.
Strengths and Limitations
This is the first study conducted to explore the prevalence of Acinetobacter infections in a tertiary clinical setting; a provincial level hospital located in a busy and bustling city in Western Nepal and attracting patients from in and outside the province. The findings generated from this study will provide a useful reference for regional infection epidemiology in addition to informing clinicians managing Acinetobacter infections in the hospital. The findings in this study are limited by the phenotypic detection of AMR and MDR strains of Acinetobacter species. Future studies should confirm the identification of Acinetobacter baumannii genetically via amplification of the blaOXA-51 gene, since phenotypic identifications are usually not enough.53 In this study, we used E. coli and S. aureus as controls because the control strain of Acinetobacter species was not available in our facility. As a result, the study might have incurred biases in reporting the susceptibility of the antibiotics. Future studies can explore the genotypic identification and characterization of pathogenic strains, along with phylogenetic analysis. Accurate identification of clinically important species of Acinetobacter using the molecular method was beyond the scope of the study.
Conclusion
A. baumannii is a notable bacterium for causing severe, mostly hospital-acquired, infections. Two-thirds of the specimens showed MDR, associated with specific demographic of the patients who were admitted at in-patient settings that included surgery, ICU, and medicine wards and among the particular specimens such as swab, sputum, and urine. The findings of this study should generate a discussion and seminar among the clinical practitioners of UCMSTH in order to inform the clinical practice that includes clinical suspicion, diagnostic recommendations, and subsequent management. UCMSTH and the hospitals in the region can tailor their infectious disease management protocol and pharmacovigilance for proper isolation, diagnostics, and treatment.
Data Sharing Statement
All data pertaining to this study are presented within the manuscript.
Ethics Approval and Consent to Participate
Ethical approval for the study was obtained from the institutional review committee of the Universal College of Medical Sciences (Registration number: UCMS/IRC/203/2018). A written informed consent was obtained from each patient before collection of the sample.
Acknowledgments
We are grateful to the staff and faculty members of the Universal College of Medical Sciences, Bhairahawa for their support and coordination to accomplish the study. We express our gratitude to all the patients providing samples for the study.
Author Contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
The logistic support for the study was received from the Departmental fund of Universal College of Medical Sciences, Bhairahawa.
Disclosure
All the authors declared that they have no competing interests.
References
1. Pokharel S, Raut S, Adhikari B. Tackling antimicrobial resistance in low-income and middle-income countries. BMJ Glob Health. 2019;4(6):e002104. doi:10.1136/bmjgh-2019-002104
2. Ayukekbong JA, Ntemgwa M, Atabe AN. The threat of antimicrobial resistance in developing countries: causes and control strategies. Antimicrob Resist Infect Control. 2017;6(1):47. doi:10.1186/s13756-017-0208-x
3. O’Neill J. Antimicrobial resistance: tackling a crisis for the health and wealth of nations. Rev Antimicrob Resist. 2014;20:1–16.
4. Boucher HW, Talbot G, Bradley J. Bad bugs, no drugs: no ESKAPE! An update from the infectious diseases society of America. Clin Infect Dis. 2009;48(1):1–12. doi:10.1086/595011
5. Gonzalez-Villoria AM, Valverde-Garduno V. Antibiotic-resistant Acinetobacter baumannii increasing success remains a challenge as a nosocomial pathogen. J Pathog. 2016;2016:7318075. doi:10.1155/2016/7318075
6. Neidell MJ, Cohen B, Furuya Y, et al. Costs of healthcare- and community-associated infections with antimicrobial-resistant versus antimicrobial-susceptible organisms. Clin Infect Dis. 2012;55(6):807–815. doi:10.1093/cid/cis552
7. Lautenbach E, Synnestvedt M, Weiner MG, et al. Epidemiology and impact of imipenem resistance in Acinetobacter baumannii. Infect Control Hosp Epidemiol. 2009;30(12):1186–1192. doi:10.1086/648450
8. Peleg AY, Seifert H, Paterson DL. Acinetobacter baumannii: emergence of a successful pathogen. Clin Microbiol Rev. 2008;21:538–582.
9. Abbott I, Cerqueira GM, Bhuiyan S, Peleg AY. Carbapenem resistance in Acinetobacter baumannii: laboratory challenges, mechanistic insights and therapeutic strategies. Expert Rev Anti Infect Ther. 2013;11(4):395–409. doi:10.1586/eri.13.21
10. Pendse R, Gupta S, Yu D, Sarkar S. HIV/AIDS in the South-East Asia region: progress and challenges. J Virus Erad. 2016;2(Suppl 4):1–6.
11. Doi Y, Murray GL, Peleg AY. Acinetobacter baumannii: evolution of antimicrobial resistance-treatment options. Semin Respir Crit Care Med. 2015;36(1):85–98. doi:10.1055/s-0034-1398388
12. Shrestha S, Tada T, Shrestha B, et al. Emergence of aminoglycoside resistance due to arma methylase in multi-drug resistant Acinetobacter baumannii isolates in a university hospital in Nepal. J Nepal Health Res Counc. 2016;14(33):72–76.
13. Khanal BR, Wagle S, Tiwari BR. Biofilm formation and colistin susceptibility of clinical isolates of Acinetobacter species in a tertiary care hospital of Nepal. National J Lab Med. 2019;8(1):12–15.
14. Koirala A, Agrahari G, Dahal N, Ghimire P, Rijal KR. ESBL and MBL mediated resistance in clinical isolates of nonfermentating Gram negative bacilli (NFGNB) in Nepal. J Microb Antimicrob Agents. 2017;3(1):18–24.
15. Almasaudi SB. Acinetobacter spp. as nosocomial pathogens: epidemiology and resistance features. Saudi J Biol Sci. 2018;25(3):586–596. doi:10.1016/j.sjbs.2016.02.009
16. Acharya KP, Wilson RT. Antimicrobial Resistance in Nepal. Front Med. 2019;6:105. doi:10.3389/fmed.2019.00105
17. Amatya R, Acharya D. Prevalence of tigecycline resistant multidrug resistant Acinetobacter Calcoaceticus- Acinetobacter baumanii complex from a tertiary care hospital in Nepal. Nepal Med Coll J. 2015;17(1–2):83–86.
18. Shrestha S, Tada T, Miyoshi-Akiyama T, et al. Molecular epidemiology of multidrug-resistant Acinetobacter baumannii isolates in a university hospital in Nepal reveals the emergence of a novel epidemic clonal lineage. Int J Antimicrob Agents. 2015;46(5):526–531. doi:10.1016/j.ijantimicag.2015.07.012
19. American Society for Microbiology. Manual of Clinical Microbiology. 11th ed. ASM Press, 2015.
20. Kayastha K, Dhungel B, Karki S, et al. Extended-spectrum -lactamase-producing Escherichia coli and Klebsiella species in pediatric patients visiting international friendship children’s hospital, Kathmandu, Nepal. Infect Dis (Auckl). 2020;13:1–7. doi:10.1177/1178633720909798
21. Forbes BA, Daniel SF, Weissfelt SA. Bailey and Scott;s Diagnostic Microbiology. Mosby Publication; 2007.
22. Malini A, Deepa E, Gokul B, Prasad S. Nonfermenting gram-negative bacilli infections in a tertiary care hospital in Kolar, Karnataka. J Lab Physicians. 2009;1(02):62–66. doi:10.4103/0974-2727.59701
23. Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Susceptibility Testing. M100S. Accessed on; January 20 2018.
24. Magiorakos AP, Srinivasan A, Carey RB, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18(3):268–281. doi:10.1111/j.1469-0691.2011.03570.x
25. Guragin N, Pradhan A, Dhungel B, Banjara MR, Rijal KR, Ghimire P. Extended spectrum B-lactamase producing Gram negative bacterial isolates from urine of patients visiting everest hospital, Kathmandu, Nepal. TUJM. 2019;6(1):26–31.
26. Shrestha LB, Bhattarai NR, Khanal B. Comparative evaluation of methods for the detection of biofilm formation in coagulase-negative staphylococci and correlation with antibiogram. Infect Drug Resist. 2018;11:607–613. doi:10.2147/IDR.S159764
27. Dumaru R, Baral R, Shrestha LB. Study of biofilm formation and antibiotic resistance pattern of Gram-negative Bacilli among the clinical isolates at BPKIHS, Dharan. BMC Res Notes. 2019;12(1):38. doi:10.1186/s13104-019-4084-8
28. Trojan R, Razdan L, Singh N. Antibiotic susceptibility patterns of bacterial isolates from pus samples in a tertiary care hospital of Punjab, India. Int J Microbiol. 2016;2016:9302692. doi:10.1155/2016/9302692
29. Mohammadi-Mehr M, Feizabadi M. Antimicrobial resistance pattern of Gram-negative bacilli isolated from patients at ICUs of Army hospitals in Iran. Iran J Microbiol. 2011;3(1):26–30.
30. Hassanzadeh P, Motamedifar M, Hadi N. Prevalent bacterial infections in intensive care units of Shiraz University of medical sciences teaching hospitals, Shiraz, Iran. Jpn J Infect Dis. 2009;62(4):249–253.
31. Richet H. Seasonality in Gram-negative and healthcare-associated infections. Clin Microb Infect. 2012;18(10):934–940. doi:10.1111/j.1469-0691.2012.03954.x
32. McDonald LC, Banerjee SN, Jarvis WR. Seasonal variation of Acinetobacter infections: 1987–1996. Nosocomial Infections Surveillance System. Clin Infect Dis. 1999;29(5):1133–1137. doi:10.1086/313441
33. Burnham JP, Feldman MF, Calix JJ. Seasonal changes in the prevalence of antibiotic-susceptible Acinetobacter calcoaceticus-baumannii complex isolates result in increased multidrug resistance rates during winter months. Open Forum Infect Dis. 2019;6(6):245. doi:10.1093/ofid/ofz245
34. Prashanth K, Badrinath S. Nosocomial infections due to Acinetobacter species: clinical findings, risk and prognostic factors. Indian J Med Microbiol. 2006;24(1):39–44. doi:10.4103/0255-0857.19893
35. Van TD, Dinh QD, Vu PD, et al. Antibiotic susceptibility and molecular epidemiology of Acinetobacter calcoaceticus-baumannii complex strains isolated from a referral hospital in northern Vietnam. J Glob Antimicrob Resist. 2014;2(4):318–321. doi:10.1016/j.jgar.2014.05.003
36. Shrestha M, Khanal B. Acinetobacter Species: phenotypic characterization and antimicrobial resistance. J Nobel Med Coll. 2013;2(1):43–48. doi:10.3126/jonmc.v2i1.7675
37. Banerjee T, Mishra A, Das A, Sharma S, Barman H, Yadav G. High prevalence and endemicity of multidrug resistant Acinetobacter spp. In intensive care unit of a tertiary care hospital, Varanasi, India. J Pathog. 2018;2018:9129083. doi:10.1155/2018/9129083
38. Kanafani ZA, Zahreddine N, Tayyar R, et al. Multi-drug resistant Acinetobacter species: a seven-year experience from a tertiary care center in Lebanon. Antimicrob Resist Infect Control. 2018;7(1):9. doi:10.1186/s13756-017-0297-6
39. Raut S, Adhikari B. Ceftazidime-avibactam in ceftazidime-resistant infections. Lancet Infect Dis. 2016;16(9):997. doi:10.1016/S1473-3099(16)30194-3
40. Moradi J, Hashemi FB, Bahador A. Antibiotic resistance of Acinetobacter baumannii in Iran: a systemic review of the published literature. Osong Public Health Res Perspect. 2015;6(2):79–86. doi:10.1016/j.phrp.2014.12.006
41. Mishra SK, Rijal BP, Pokhrel BM. Emerging threat of multidrug resistant bugs–Acinetobacter calcoaceticus baumannii complex and methicillin resistant Staphylococcus aureus. BMC Res Notes. 2013;6(1):98. doi:10.1186/1756-0500-6-98
42. Joshi SG, Litake GM, Ghole VS, Niphadkar KB. Fluoroquinolone resistance from a transferable plasmid in Acinetobacter calcoaceticus. Indian J Pathol Microbiol. 2004;47(4):593–594.
43. Mezzatesta ML, Trovato G, Gona F, et al. In vitro activity of tigecycline and comparators against carbapenem-susceptible and resistant Acinetobacter baumannii clinical isolates in Italy. Ann Clin Microbiol Antimicrob. 2008;7(1):4. doi:10.1186/1476-0711-7-4
44. Bergogne-Berezin E, Towner KJ. Acinetobacter spp. as nosocomial pathogens: microbiological, clinical, and epidemiological features. Clin Microbiol Rev. 1996;9(2):148–165. doi:10.1128/CMR.9.2.148
45. Go ES, Urban C, Burns J, et al. Clinical and molecular epidemiology of Acinetobacter infections sensitive only to polymyxin B and sulbactam. Lancet. 1994;344(8933):1329–1332. doi:10.1016/S0140-6736(94)90694-7
46. Gupta EMS, Sood S, Dhawan B, Das BK, Kapil A. Emerging resistance to carbapenems in a tertiary care hospital in north India. Ind J Med Res. 2006;124:95–98.
47. Sinha M, Srinivasa H. Mechanisms of resistance to carbapenems in meropenem- resistant Acinetobacter isolates from clinical samples. Ind J Med Microb. 2007;25(2):121–125. doi:10.4103/0255-0857.32717
48. Peleg AY, Potoski BA, Rea R, et al. Acinetobacter baumannii bloodstream infection while receiving tigecycline: a cautionary report. J Antimicrob Chemother. 2007;59(1):128–131. doi:10.1093/jac/dkl441
49. Navon-Venezia S, Leavitt A, Carmeli Y. High tigecycline resistance in multidrug-resistant Acinetobacter baumannii. J Antimicrob Chemother. 2007;59(4):772–774. doi:10.1093/jac/dkm018
50. Vakili B, Fazeli H, Shoaei P, et al. Detection of colistin sensitivity in clinical isolates of Acinetobacter baumannii in Iran. J Res Med Sci. 2014;19(Suppl 1):S67–S70.
51. Montefour K, Frieden J, Hurst S, et al. Acinetobacter baumannii: an emerging multidrug-resistant pathogen in critical care. Crit Care Nurse. 2008;28(1):15–25. doi:10.4037/ccn2008.28.1.15
52. Maragakis LL, Perl TM. Antimicrobial resistance: Acinetobacter baumannii: epidemiology, antimicrobial resistance, and treatment options. Clin Infect Dis. 2008;46(8):1254–1263. doi:10.1086/529198
53. Turton JF, Woodford N, Glover J, Yarde S, Kaufmann ME, Pitt TL. Identification of Acinetobacter baumannii by detection of the blaOXA-51-like carbapenemase gene intrinsic to this species. J Clin Microbiol. 2006;44(8):2974–2976. doi:10.1128/JCM.01021-06
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.