Back to Journals » Clinical Interventions in Aging » Volume 10
Treatment of primary osteoporosis in men
Received 12 June 2014
Accepted for publication 18 September 2014
Published 30 December 2014 Volume 2015:10 Pages 105—115
DOI https://doi.org/10.2147/CIA.S44057
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Richard Walker
Andrea Giusti,1 Gerolamo Bianchi2
1Bone Clinic, Department of Gerontology and Musculoskeletal Sciences, Galliera Hospital, 2Department of Rheumatology, La Colletta Hospital, ASL3, Arenzano, Genoa, Italy
Abstract: With the aging of the population worldwide, osteoporosis and osteoporotic fractures are becoming a serious health care issue in the Western world. Although less frequent than in women, osteoporosis in men is a relatively common problem. Hip and vertebral fractures are particularly relevant, being associated with significant mortality and disability. Since bone loss and fragility fractures in men have been recognized as serious medical conditions, several randomized controlled trials (RCTs) have been undertaken in males with osteoporosis to investigate the anti-fracture efficacy of the pharmacological agents commonly used to treat postmenopausal osteoporosis. Overall, treatments for osteoporosis in men are less defined than in women, mainly due to the fact that there are fewer RCTs performed in male populations, to the relatively smaller sample sizes, and to the lack of long-term extension studies. However, the key question is whether men are expected to respond differently to osteoporosis therapies than women. The pharmacological properties of bisphosphonates, teriparatide, denosumab, and strontium ranelate make such differentiation unlikely, and available clinical data support their efficacy in men with primary osteoporosis as well as in women. In a series of well-designed RCTs, alendronate, risedronate, zoledronic acid, and teriparatide were demonstrated to reduce the risk of new vertebral fractures in men presenting with primary osteoporosis (including osteoporosis associated with low testosterone levels) and to improve the bone mineral density (BMD). In preliminary studies, ibandronate, denosumab, and strontium ranelate also showed their beneficial effects on surrogate outcomes (BMD and markers of bone turnover) in men with osteoporosis. Although direct evidence about their non-vertebral anti-fracture efficacy are lacking, the effects of bisphosphonates, denosumab, teriparatide, and strontium ranelate on surrogate outcomes (BMD and markers of bone turnover) were similar to those reported in pivotal RCTs undertaken in postmenopausal women, in which vertebral and non-vertebral anti-fracture efficacy have been clearly demonstrated. In conclusion, sufficient data exist to support the use of these pharmacological agents in men with primary osteoporosis. Further RCTs are warranted to establish their long-term efficacy and safety.
Keywords: bisphosphonates, teriparatide, denosumab, strontium ranelate
Introduction
Osteoporosis is defined as an asymptomatic bone disease characterized by low bone mineral density (BMD) and deterioration of microarchitecture of the skeleton, leading to an increased fracture risk.1
Osteoporosis-related fractures are classically recognized as a significant health care issue in women, but are now increasingly viewed as an important health care problem in men as well.2 Although fewer men sustain osteoporotic fractures than women during aging, it has been estimated that one in eight men over the age of 50 years old will sustain an osteoporotic fracture during their lifetime, and that 20%–30% of hip fractures occur in men.2,3
Studies of male osteoporosis have increased the awareness of the problem and have improved our understanding of the pathogenesis of osteoporosis and fragility fractures in men. In this context, a number of small randomized controlled trials (RCTs), undertaken in men with primary and secondary osteoporosis, have helped to position available pharmacological treatments in the therapy of male osteoporosis.3,4
In contrast to the wealth of data about the efficacy of pharmacological agents in the management of postmenopausal osteoporosis, information regarding their efficacy in male osteoporosis is relatively limited. Most of the RCTs undertaken in men did not present enough statistical power to address drug effects on fracture risk (particularly non-vertebral fractures), mainly due to the small samples of the populations included. Therefore, in most RCTs, the primary endpoints were the change in the BMD and markers of bone turnover. Nevertheless, the effects of bisphosphonates, denosumab, teriparatide, and strontium ranelate on surrogate outcomes, such as BMD and markers of bone turnover, were similar to those reported in pivotal RCTs undertaken in postmenopausal women, for which vertebral and non-vertebral anti-fracture efficacy have been clearly demonstrated, suggesting that these agents should be effective in men as well as in women.2–5
This review provides an overview of available treatment options for the management of primary osteoporosis in men, including hypogonadism-associated osteoporosis.
Age-related bone loss and causes of osteoporosis in men
Unlike women, men do not have a menopause. As such, they do not present with a midlife loss of sex steroid production and do not experience accelerated bone loss and fracture risk increase, unless they develop hypogonadism or are prescribed androgen deprivation therapy for prostate cancer.2,3 In men, bone loss proceeds slowly, starting at middle age.
With aging, men experience a lower endocortical resorption and a greater periosteal expansion compared to women.2 The periosteal apposition may even counteract the cortical thinning produced by endocortical resorption, producing a lower net bone loss compared to women and, most important, an absolute increase in bone size. The increased bone size, together with a lower intracortical porosity, produces higher bone strength and lower bone fragility in men compared to women.
The trabecular bone loss in aging males is mainly produced by a trabecular thinning due to reduced bone formation, rather than by trabecular perforation and loss of connectivity (characteristic of high bone turnover states).2 Indeed, the trabecular thinning observed in males does not cause the same loss of strength of the vertebral body produced by the loss of connectivity induced by the menopause in women. This further explains sex differences in bone fragility during aging.
Traditionally, it was believed that the decrease in bioavailable or free testosterone level was the main cause of age-related bone loss in men.2 However, both cross-sectional and longitudinal evidence indicates that levels of bioavailable estradiol rather than testosterone are strongly correlated with the BMD and fracture risk.2,3 The function of testosterone in aging men is less clear, being potentially involved in the maintenance of muscle strength and balance.2,3 The primary cause of the declining of sex steroid levels in men is an age-associated increase in sex hormone-binding globulin (SHBG) value, that, in turn, limits the biological available sex steroids and produces a decline in bioavailable testosterone and estrogen levels (respectively, by 64% and 47% during the male lifespan).2,3
Several different conditions may produce osteoporosis and fragility fractures in men (Table 1).2,3 In most cases, an osteoporotic fracture is the consequence of the coexistence of several conditions (medications and/or specific diseases) and risk factors related to lifestyle (eg, cigarette smoking, alcohol abuse, sedentary lifestyle). An important proportion of osteoporotic males, however, have idiopathic disease. Particularly in young men, idiopathic osteoporosis may present quite dramatically. Although its pathogenesis remains uncertain, genetic factors appear to play a key role in the pathogenesis of idiopathic osteoporosis.
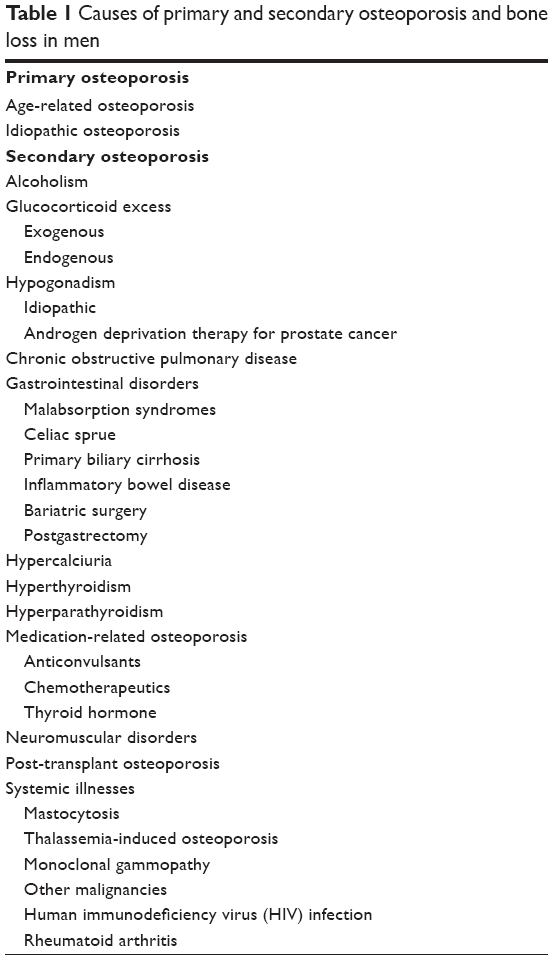 | Table 1 Causes of primary and secondary osteoporosis and bone loss in men |
The most frequent secondary causes of osteoporosis in men are alcohol abuse, glucocorticoid excess, and hypogonadism (both idiopathic and related to androgen deprivation therapy for prostate cancer). Secondary causes of osteoporosis may be superimposed on an underlying age-related bone loss or idiopathic osteoporosis, producing dramatic clinical presentations.
Management of male osteoporosis: general measures
Once a complete diagnostic work-up has defined the nature (primary or secondary) of osteoporosis, identified underlying causes and potentially modifiable risk factors for fragility fractures, and assessed the absolute risk of fracture (using a validated tool such as FRAX),6,7 the management of men presenting with osteoporosis should consist of the implementation of general measures and the prescription of a specific pharmacological agent.
General measures for fracture prevention in men are similar to those in women: excellent nutrition, appropriate calcium intake (between 1,000 mg and 1,500 mg per day), physical exercise, and avoidance of detrimental lifestyle factors (eg, smoking, excessive alcohol consumption). Vitamin D supplementation should always be considered in order that an adequate vitamin D level (25-hydroxy vitamin D >30 ng/mL) is attained and maintained, due to its implication for bone health and falls prevention.8 In patients at risk of falls, intervention to prevent falls and to improve muscle mass and strength should be implemented. Finally, patients presenting with osteoporosis and a high fracture risk should be instructed to lift objects using proper techniques and to avoid lifting objects that are too heavy, due to the potential risk of vertebral fractures.
In patients presenting with a secondary condition potentially associated with increased bone fragility and fracture risk (eg, primary hyperparathyroidism, hypogonadism), this should, if possible, be treated and/or removed. Men presenting with hypogonadism should receive testosterone, on the basis of current hypogonadism treatment guidelines, associated with a classical osteoporosis medication.5,9 Indeed, although testosterone has been demonstrated to prevent bone loss and to improve bone mass in hypogonadal men,2,3,5 there is still little evidence about long-term treatment and no data about its anti-fracture efficacy.
Management of male osteoporosis: pharmacological agents
Bisphosphonates, strontium ranelate, teriparatide, and denosumab have been tested versus placebo or an active agent in a number of RCTs undertaken in men presenting with primary (idiopathic and age-related) or hypogonadism-associated osteoporosis. The general characteristics and the main results of these RCTs are depicted in Tables 2 and 3.
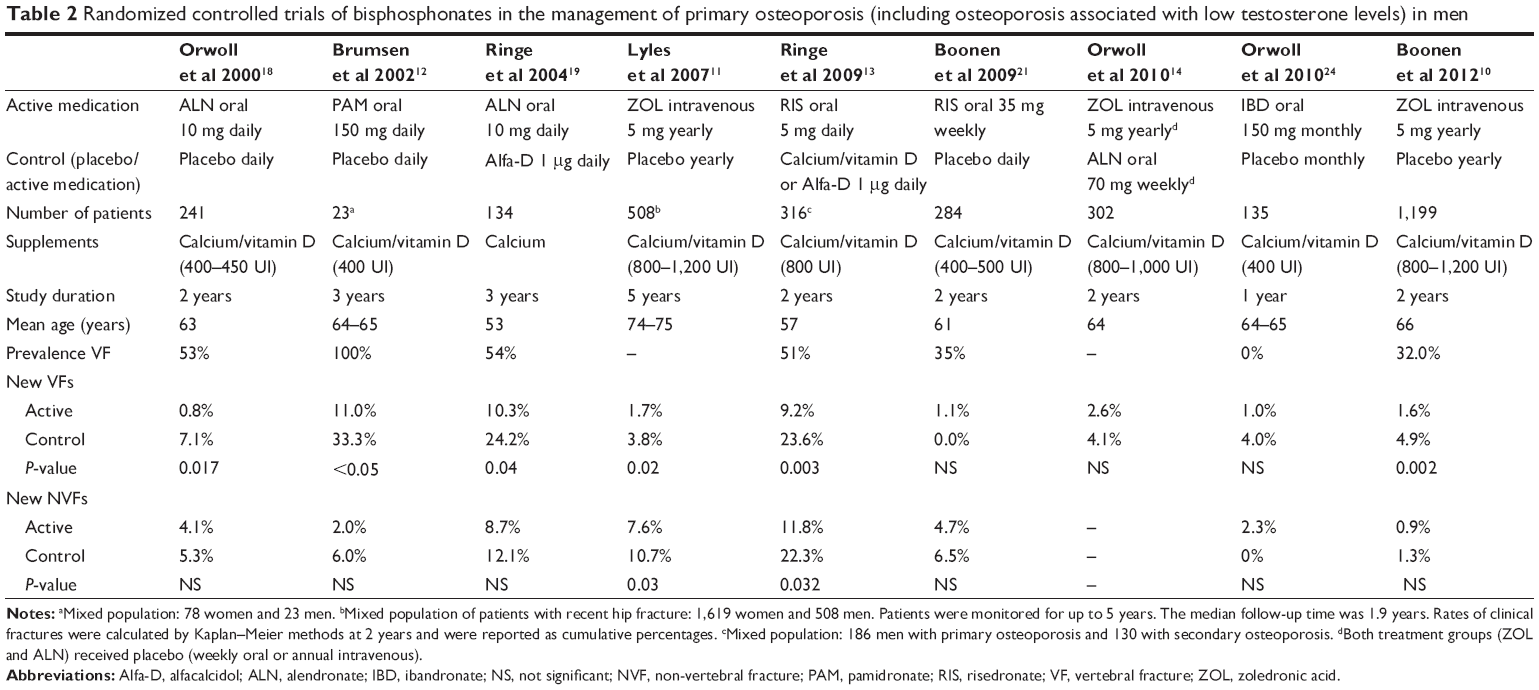 | Table 2 Randomized controlled trials of bisphosphonates in the management of primary osteoporosis (including osteoporosis associated with low testosterone levels) in men |
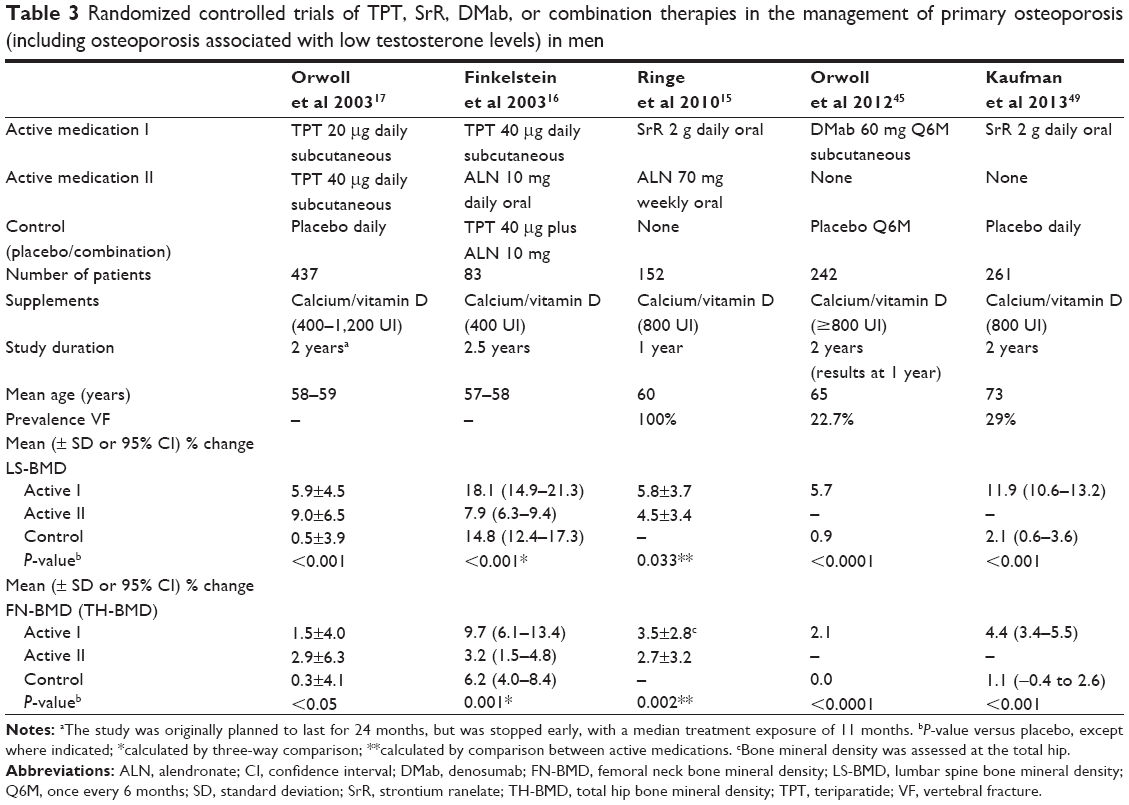 | Table 3 Randomized controlled trials of TPT, SrR, DMab, or combination therapies in the management of primary osteoporosis (including osteoporosis associated with low testosterone levels) in men |
Studies included relatively small numbers of patients. Only one of them (with zoledronic acid) was designed to assess anti-fracture efficacy,10 and none of them assessed the long-term effect of treatment (eg, due to absence of extension studies). Two RCTs included men and women,11,12 and another study was conducted in a mixed population that also included men presenting with secondary osteoporosis.13 Two “head-to-head” RCTs compared two active medications (zoledronic acid versus alendronate, strontium ranelate versus alendronate);14,15 another trial tested two active medications (alendronate and teriparatide) and their combination;16 and one study assessed two different doses of teriparatide.17
Bisphosphonates
Alendronate
Oral alendronate has been tested against placebo or alfacalcidol in two RCTs undertaken in men with primary or hypogonadism-associated osteoporosis (Table 2).18,19 In both studies, alendronate produced significantly higher increases of the BMD at the lumbar spine, femoral neck, and total hip, compared to placebo or alfacalcidol, after 2 or 3 years of treatment (Figure 1). The BMD response to alendronate was independent of age, smoking status, baseline free testosterone, and estradiol concentrations.18
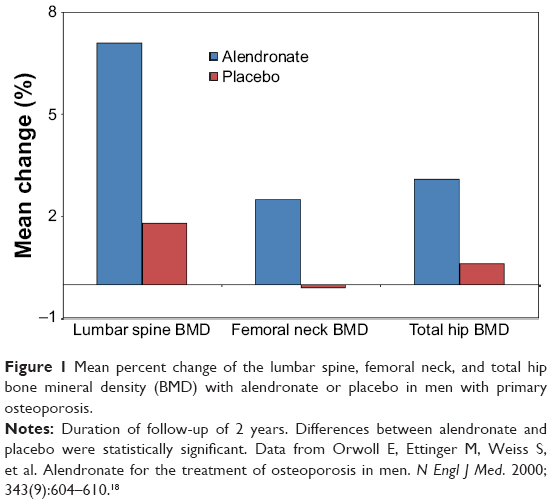 | Figure 1 Mean percent change of the lumbar spine, femoral neck, and total hip bone mineral density (BMD) with alendronate or placebo in men with primary osteoporosis. |
Orwoll et al18 randomized 241 men to receive oral alendronate 10 mg or placebo daily for 2 years. Although the trial was not powered for a fracture outcome, alendronate treatment was associated with a significant reduction of the risk of new morphometric vertebral fracture (odds ratio [OR] =0.10, 95% confidence interval [CI]: 0.00–0.88). Alendronate also decreased the risk of new non-vertebral fracture by 22.6%, but this decrease was not statistically significant.
Ringe et al19 evaluated the efficacy of oral alendronate 10 mg versus alfacalcidol 1 μg daily in a 3-year open-label RCT of 134 men. Alendronate-treated patients experienced a significantly lower incidence of new vertebral fracture compared to placebo-treated subjects (OR =0.36, 95% CI: 0.14–0.94). A nonsignificant lower incidence of new non-vertebral fracture with alendronate was also reported.
In a systematic review of RCTs of alendronate in men, Sawka et al20 pooled the results of these trials, incorporating prior information of anti-fracture efficacy in women. They estimated the ORs for incident fractures in men treated with alendronate: OR (95% CI) for vertebral fractures was 0.44 (0.23–0.83) and OR (95% CI) for non-vertebral fractures was 0.60 (0.29–1.44).
Risedronate
In a 2-year, open-label RCT (Table 2), Ringe et al13 randomized 316 men with primary (59%) or secondary osteoporosis to receive oral risedronate 5 mg daily (with calcium 1,000 mg and cholecalciferol 800 IU daily) or calcium and either cholecalciferol or alfacalcidol alone daily (alfacalcidol 1 μg daily in patients with prevalent vertebral fractures). Risedronate treatment significantly reduced the risk of new vertebral (61%) and non-vertebral fractures (45%) over 2 years of treatment, and significantly increased the BMD at the lumbar spine, femoral neck, and total hip (Figure 2). The authors did not report a separate analysis of the incidence of fractures in men presenting with primary versus secondary osteoporosis.
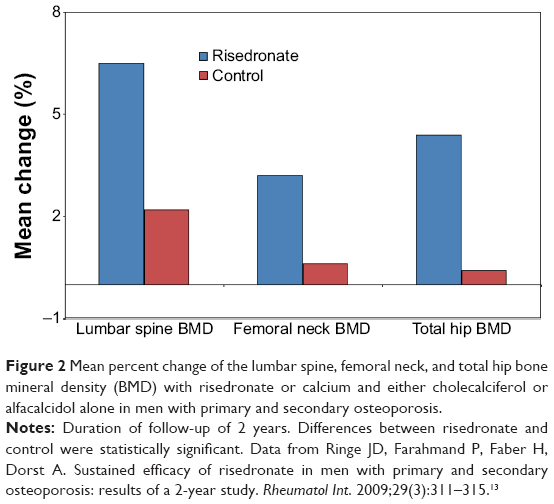 | Figure 2 Mean percent change of the lumbar spine, femoral neck, and total hip bone mineral density (BMD) with risedronate or calcium and either cholecalciferol or alfacalcidol alone in men with primary and secondary osteoporosis. |
The beneficial effect on the BMD of oral risedronate 35 mg once weekly versus placebo was evaluated in a 2-year, double-blind, placebo-controlled study including 284 men with primary osteoporosis (Table 2).21 Risedronate was demonstrated to produce a significantly greater increase of the BMD at the lumbar spine and hip compared to placebo. Very few fractures occurred during the study, and there were no significant differences between the risedronate and placebo groups.
Zoledronic acid
Three RCTs investigated the beneficial effects of intravenous zoledronic acid 5 mg once yearly versus placebo or alendronate (Table 2).10,11,14,22,23 In a large, randomized, placebo-controlled trial, Lyles et al examined the efficacy of zoledronic acid in men (n=508) and women (n=1,619) presenting with hip fracture.11,22 Approximately 22% of the men had secondary osteoporosis. Zoledronic acid showed a 35% (hazard ratio [HR] =0.65, 95% CI: 0.50–0.84) reduced risk of new clinical fractures in the overall population compared with placebo, being effective in decreasing the risk of new clinical vertebral (HR =0.54, 95% CI: 0.32–0.92) and non-vertebral fractures (HR =0.73, 95% CI: 0.55–0.98). No significant treatment-by-sex interaction was observed. A recent analysis undertaken to further evaluate the beneficial effect of zoledronic acid in the subgroup of 508 men demonstrated that the increases of the BMD in men were of a similar magnitude to those observed in women in the same study.22 Very few clinical fractures were observed in men, with no statistically significant differences between zoledronic acid and placebo.
A recent, fracture-endpoint RCT investigated the efficacy of zoledronic acid versus placebo in 1,199 men presenting with primary or hypogonadism-associated osteoporosis.10 A significantly lower proportion of men in the zoledronic acid group experienced one or more new morphometric vertebral fractures over 24 months as compared with men in the placebo group, with a relative risk reduction of 67%. Similar results were observed for moderate-to-severe and worsening morphometric vertebral fractures, while no significant difference was observed between groups in the incidence of new clinical fractures. Zoledronic acid also significantly increased the BMD at the lumbar spine, total hip, and femoral neck over 24 months, as compared to placebo (Figure 3). Total testosterone level did not affect the anti-fracture efficacy of zoledronic acid or its beneficial effects on the BMD.
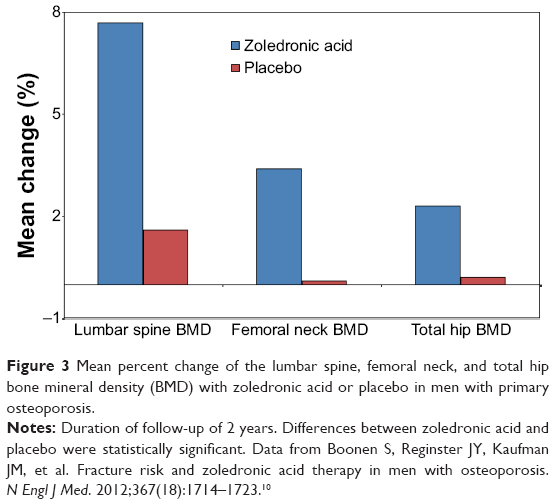 | Figure 3 Mean percent change of the lumbar spine, femoral neck, and total hip bone mineral density (BMD) with zoledronic acid or placebo in men with primary osteoporosis. |
In line with these findings, a 2-year head-to-head RCT comparing once-yearly zoledronic acid with once-weekly alendronate in men with primary or hypogonadism-associated osteoporosis demonstrated the noninferiority of zoledronic acid compared to alendronate in improving the BMD at the lumbar spine, femoral neck, and total hip.14
Other bisphosphonates
In a 3-year RCT of men (n=23) and women (n=78) with primary osteoporosis treated with oral pamidronate 150 mg daily or placebo, pamidronate decreased the incidence of new vertebral fractures by 67%, with a similar response in men and women.12 Lumbar spine BMD increased significantly in pamidronate-treated patients, with a significantly greater increase compared to placebo. BMD response to pamidronate was similar in men and women (absolute increase: 0.047 g/cm2 in women, 0.040 g/cm2 in men), although the mean percent change in women (10.13%±1.67%) was greater compared to men (5.98%±1.49%) due to the lower baseline BMD of the women.
Orwoll et al investigated the safety and efficacy of 150 mg monthly oral ibandronate versus placebo in a small, 1-year RCT of men with primary or hypogonadism-associated osteoporosis.24 After 1 year, ibandronate-treated men demonstrated a significantly greater increase of the lumbar spine, total hip, and femoral neck BMD compared to placebo-treated patients. The lumbar spine BMD response to ibandronate was independent of age, baseline body mass index, baseline total hip BMD, and ethnicity.
Bisphosphonates in men with primary osteoporosis: summary
In summary, findings from RCTs with alendronate, risedronate, and zoledronic acid demonstrated their efficacy in reducing the risk of new vertebral fractures in men with primary and hypogonadism-associated osteoporosis.25 Evidence for a significant effect on non-vertebral fractures is still insufficient, mainly due to the small numbers of patients included in clinical trials.
Oral and intravenous bisphosphonates (alendronate, risedronate, pamidronate, ibandronate, and zoledronic acid), given daily or intermittently, were also shown to significantly reduce markers of bone turnover (data not shown) and to increase the BMD compared to baseline and to placebo. These results were similar to those observed in pivotal RCTs undertaken in women with postmenopausal osteoporosis.26–34
Overall, bisphosphonates were well tolerated, producing only expected (on the basis of previous studies) and self-limiting specific adverse effects including upper gastrointestinal toxicity associated with oral use, and symptoms related to an acute phase reaction (diffuse musculoskeletal pain and fever) after the first exposure to intravenous zoledronic acid. No cases of osteonecrosis of the jaw or atypical femur fracture were described, and no new relevant safety issues were reported.
Teriparatide
Teriparatide treatment for the management of primary osteoporosis in men has been evaluated in two well-designed RCTs as monotherapy or combination therapy.17,35–37
Orwoll et al randomized 437 men with primary osteoporosis to receive teriparatide 20 μg, teriparatide 40 μg, or placebo injection daily (Table 3). The trial was originally designed to last 2 years, but it was stopped after a median duration of 11 months.17 A follow-up safety study provided the opportunity to follow the patients up to 30 months after teriparatide discontinuation and to obtain radiographs at 18 months.36 During the “core” study, indices of bone formation increased early in the course of therapy with teriparatide, followed by increases of markers of osteoclastic activity. Markers of bone turnover were stable or declined slightly in the placebo group. Daily treatment with teriparatide at both doses increased, dose-dependently, lumbar spine and femoral neck BMD (Table 2). BMD changes were significantly greater in the teriparatide groups compared to the placebo group, beginning at 3 months. The BMD response to treatment was independent of baseline free testosterone, age, body mass index, baseline lumbar spine BMD, smoking, and alcohol intake. The time course and the magnitude of the changes of BMD in men treated with teriparatide were comparable with those observed in women.38 From the original treatment trial baseline17 to the 18-month visit of the follow-up study,36 there was a lower incidence of new moderate or severe vertebral fractures in the combined teriparatide groups compared to the placebo group (relative risk reduction =83%; new vertebral fracture: placebo 11.7% versus combined teriparatide 5.7%, P=0.07; new moderate or severe vertebral fractures: placebo 6.8% versus combined teriparatide 1.1%, P=0.01).
Finkelstein et al randomized 83 men to receive alendronate (10 mg oral daily), teriparatide (40 μg subcutaneous daily), or the combination therapy for 30 months (with teriparatide therapy starting at month 6).16 After 30 months (Table 2), the BMD at the lumbar spine and femoral neck increased significantly more in the teriparatide group compared to the other two groups (alendronate alone or combination). Considering also the changes of the markers of bone turnover, the authors concluded that alendronate treatment impaired the ability of teriparatide to increase the BMD, due to an attenuation of the teriparatide-induced stimulation of bone formation. In a prospective cohort substudy incorporating these data about teriparatide monotherapy in men (Finkelstein et al16) and similar data from an identical protocol performed in postmenopausal women, Leder et al37 compared BMD response to teriparatide administration (months 0–30) and discontinuation (months 30–42) between males and females. During the teriparatide treatment, the magnitude of the BMD increases (lumbar spine, total hip, femoral neck) did not differ between men and women. The mean female–male difference (95% CI) in the change in BMD was 0.3 (−6.0, 6.6) at the lumbar spine, 0.1 (−4.9, 5.0) at the femoral neck, and 0.4 (−4.5, 5.2) at the total hip. Interestingly, during the 12 months of follow-up after teriparatide discontinuation, BMD response to discontinuation was different between the sexes. Lumbar spine BMD decreased by 7.1%±3.8% in women and by 4.1%±3.5% in men (P=0.036). Total hip and femoral neck BMD also decreased significantly in women (3.8%±3.9% and 3.1%±4.3%, respectively), but remained stable in men. Overall, these results confirmed the comparable efficacy of teriparatide treatment in men and women, but suggested a different trend in BMD response to discontinuation.
Teriparatide in men with primary osteoporosis: summary
Taken together, studies of teriparatide in males with primary or hypogonadal osteoporosis provide evidence that teriparatide is effective in the management of osteoporosis in men as well as in women.35 Although data about vertebral fracture risk reduction should be interpreted with caution due to the nature of the studies (post-treatment follow-up), the small sample size (279 men out of the 437 from the original sample), and other confounders, they strongly indicate that teriparatide is effective in reducing the risk of new vertebral fractures in men presenting with primary osteoporosis.36
Teriparatide was well tolerated, producing only expected and self-limiting specific adverse effects, including transient post-dose increase of serum calcium and 24-hour urinary calcium excretion, nausea, and headache. The overall safety and tolerability of teriparatide in men and women have also been highlighted by a decade of experience that has not revealed relevant safety issues.39
Denosumab
The anti-fracture efficacy of the antiresorptive denosumab, a monoclonal antibody that binds and neutralizes the activity of RANKL (a key osteoclast cytokine), has been clearly established in RCTs performed in postmenopausal women and men receiving androgen-deprivation therapy for nonmetastatic prostate cancer.40–43
The efficacy and safety of denosumab in men with low BMD (primary or hypogonadism-associated) have been investigated in a 2-year RCT performed in 242 patients (ADAMO study). Preliminary results from the first year of the study have been recently published (Table 3).44 Denosumab increased lumbar spine BMD by 5.7% at 12 months compared with an increase of 0.9% in the placebo group (P<0.0001). Denosumab treatment also significantly increased the BMD at the total hip and femoral neck compared to placebo (total hip: denosumab 2.4% versus placebo 0.3%, P<0.0001; femoral neck: denosumab 2.1% versus placebo, P<0.0001). The BMD response to denosumab was independent of baseline testosterone level, lumbar spine BMD, 10-year risk of major osteoporotic fractures, age, race, previous osteoporotic fractures, and baseline serum beta-C-terminal telopeptide of type I collagen (CTX). Treatment with denosumab produced a significant (versus baseline and placebo) decrease of serum CTX. Overall, the incidence of adverse events was similar between treatment groups, and no relevant safety issue with denosumab was reported (eg, hypocalcemia, osteonecrosis of the jaw, complications of fracture healing, atypical femoral fractures).
BMD gains in the ADAMO study were comparable to those reported in the RCT undertaken in postmenopausal women, in which vertebral, hip, and non-vertebral anti-fracture efficacy was demonstrated.40 Furthermore, the significant reduction in serum CTX with denosumab observed early after initiating treatment and the sustained reduction of bone turnover up to 12 months were consistent with what has been observed in postmenopausal women with osteoporosis.40
In conclusion, although the ADAMO study was not designed to assess the anti-fracture efficacy of denosumab, the similarity of effects on surrogate markers (BMD and markers of bone turnover) in males and females with osteoporosis suggests that denosumab may be effective in reducing fracture risk in men with primary or hypogonadism-associated osteoporosis as well as in men with prostate cancer receiving androgen-deprivation therapy and postmenopausal women.40–43
Strontium ranelate
The mechanism of action of strontium ranelate is not fully understood. Preclinical studies indicated that strontium ranelate induces opposite effects on bone, suggesting that it may have a dual action of inhibiting bone resorption and stimulating bone formation.45–47 However, in a recent study performing transiliac bone biopsies in subjects treated with strontium ranelate and alendronate, strontium ranelate failed to demonstrate a significant anabolic action on bone remodeling.45
Two RCTs have investigated the effects of oral strontium ranelate 2 g daily compared to placebo or alendronate (70 mg weekly) in men with established primary osteoporosis (Table 3).15,48
Kaufman et al randomized 261 males with primary osteoporosis to receive strontium ranelate or placebo for 2 years.48 Randomization was unbalanced (2:1) in favor of strontium ranelate. After 12 and 24 months, the mean percent change of the BMD at the lumbar spine, total hip, and femoral neck was significantly greater in the treatment group compared to the placebo group. At 24 months, the average percent increase (95% CI) at the lumbar spine was 11.9% (10.6–13.2) in the strontium ranelate group and 2.1% (0.6–3.6) in the placebo group (P<0.001). Total hip and femoral neck BMD improved, respectively, by 3.7% (2.7–4.8) and 4.4% (3.4–5.5) after 2 years of treatment with strontium ranelate, but remained stable in patients who received placebo (P<0.001). These changes in BMD were comparable in magnitude to those observed previously in pivotal RCTs undertaken postmenopausal women.49,50 Strontium ranelate therapy also produced a significant improvement in quality of life and pain compared to placebo. Notably, the trial was not powered for a fracture outcome and new radiographic vertebral fractures were recorded as adverse events. New radiographic vertebral fractures occurred in 5.8% of men receiving strontium ranelate and 7.8% of men receiving placebo, with no significant difference between the two groups.
The incidence of the most common adverse events was similar in the two groups. However, the safety analyses revealed an imbalance in the occurrence of coronary artery disorders (angina pectoris and coronary artery disease) between strontium ranelate and placebo groups, with a significant higher incidence of adverse events in the strontium ranelate group (strontium ranelate 8.7% versus placebo 4.6%).
In an open-label, 12-month, BMD-endpoint RCT, men with primary osteoporosis were randomized to receive strontium ranelate or alendronate (70 mg weekly).15 In this small trial, including only 152 subjects, Ringe et al found that mean percent increases in the lumbar spine and total hip BMD were greater with strontium ranelate compared to alendronate. Although differences between groups were significant, extreme caution should be used in the interpretation of these results, since it is well established that the increment in BMD with strontium ranelate is largely dependent on a treatment-induced artifact.51 Indeed, long-term treatment with strontium ranelate produces an exchange with calcium in the bone mineral.47 After 3 years’ therapy, bone tissue contains around one strontium atom for every 100 calcium atoms. Due to the higher atomic number of strontium (Z =38) compared with that of calcium (Z =20), when BMD is measured by bone densitometry, strontium attenuates X-ray more strongly than calcium, causing an overestimation of the BMD.47
In conclusion, even if these RCTs were not designed to assess the anti-fracture efficacy of strontium ranelate, the similarity of effects on BMD in males and females with osteoporosis suggests that strontium ranelate may be effective in reducing fracture risk in men with primary osteoporosis as well as in postmenopausal women.
Although data from pivotal RCTs initially suggested a good profile of tolerability, a recent review of safety data from the Pharmacovigilance Risk Assessment Committee (PRAC), integrating safety information from RCTs undertaken in osteoporotic females, males, and patients with osteoarthritis, raised some issues about the cardiovascular safety of strontium ranelate.52 In light of two articles recently published that did not support such results,53,54 further research is strongly warranted to clarify the overall safety and tolerability of strontium ranelate.
Conclusion
Fragility fractures in men are a remarkable health care issue worldwide, being associated with significant disability, mortality, and reduction of quality of life.55
There is less evidence supporting the anti-fracture efficacy of available pharmacological agents in men than in women. However, the similarity between sexes regarding effects on BMD and the available data on fracture endpoints support the view that the efficacy of bisphosphonates, denosumab, teriparatide, and strontium ranelate does not differ between men and women.55,56
The choice of the pharmacological agent to be used to reduce fracture risk in men should be based on the clinical characteristics of the patient, potential interactions with underlying medical conditions or other treatments, the severity of osteoporosis and the degree of fracture risk, the costs of the treatment, and the patient’s preferences.56 Although it is not possible to establish specific recommendations on the basis of available evidence, three relevant key points should be considered when prescribing an anti-fracture therapy: the baseline fracture risk of the patient, the cost of the pharmacological agent, and its efficacy in reducing fracture risk. In this context, for example, in clinical practice, teriparatide should be, when possible, the first choice in patients presenting with severe osteoporosis and prevalent fragility fractures, followed by an antiresorptive agent (eg, denosumab or bisphosphonate), while an antiresorptive pharmacological agent should be considered as the first choice in subjects with less severe osteoporosis.
Disclosure
NIH Consensus Development Panel on Osteoporosis Prevention, Diagnosis, and Therapy. Osteoporosis prevention, diagnosis, and therapy. JAMA. 2001;285(6):785–795. | ||
Khosla S, Amin S, Orwoll E. Osteoporosis in men. Endocr Rev. 2008;29(4):441–464. | ||
Drake MT, Khosla S. Male osteoporosis. Endocrinol Metab Clin North Am. 2012;41(3):629–641. | ||
Giusti A, Papapoulos SE. Treatment of male osteoporosis with bisphosphonates. In: Orwoll E, Bilezikian J, Vanderschueren D, editors. Osteoporosis in Men: The Effects of Gender on Skeletal Health.Waltham, MA: Academic Press; 2009:667–679. | ||
Kaufman JM, Reginster JY, Boonen S, et al. Treatment of osteoporosis in men. Bone. 2013;53(1):134–144. | ||
Kanis JA, Oden A, Johnell O, et al. The use of clinical risk factors enhances the performance of BMD in the prediction of hip and osteoporotic fractures in men and women. Osteoporos Int. 2007;18(8):1033–1046. | ||
Kanis JA, Oden A, Johansson H, Borgström F, Ström O, McCloskey E. FRAX and its applications to clinical practice. Bone. 2009;44(5):734–743. | ||
Adami S, Romagnoli E, Carnevale V, et al; Italian Society for Osteoporosis, Mineral Metabolism and Bone Diseases (SIOMMMS). [Guidelines on prevention and treatment of vitamin D deficiency. Italian Society for Osteoporosis, Mineral Metabolism and Bone Diseases (SIOMMMS)]. Reumatismo. 2011;63(3):129–147. Italian. | ||
Orwoll ES. Osteoporosis in men. In: Rosen C, editor. Primer on the Metabolic Bone Diseases and Disorders of Mineral Metabolism. Washington DC: American Society for Bone and Mineral Research; 2013:508–513. | ||
Boonen S, Reginster JY, Kaufman JM, et al. Fracture risk and zoledronic acid therapy in men with osteoporosis. N Engl J Med. 2012;367(18):1714–1723. | ||
Lyles KW, Colón-Emeric CS, Magaziner JS, et al; HORIZON Recurrent Fracture Trial. Zoledronic acid and clinical fractures and mortality after hip fracture. N Engl J Med. 2007;357(18):1799–1809. | ||
Brumsen C, Papapoulos SE, Lips P, et al. Daily oral pamidronate in women and men with osteoporosis: a 3-year randomized placebo-controlled clinical trial with a 2-year open extension. J Bone Miner Res. 2002;17(6):1057–1064. | ||
Ringe JD, Farahmand P, Faber H, Dorst A. Sustained efficacy of risedronate in men with primary and secondary osteoporosis: results of a 2-year study. Rheumatol Int. 2009;29(3):311–315. | ||
Orwoll ES, Miller PD, Adachi JD, et al. Efficacy and safety of a once-yearly i.v. infusion of zoledronic acid 5 mg versus a once-weekly 70-mg oral alendronate in the treatment of male osteoporosis: a randomized, multicenter, double-blind, active-controlled study. J Bone Miner Res. 2010;25(10):2239–2250. | ||
Ringe JD, Dorst A, Farahmand P. Efficacy of strontium ranelate on bone mineral density in men with osteoporosis. Arzneimittelforschung. 2010;60(5):267–272. | ||
Finkelstein JS, Hayes A, Hunzelman JL, Wyland JJ, Lee H, Neer RM. The effects of parathyroid hormone, alendronate, or both in men with osteoporosis. N Engl J Med. 2003;349(13):1216–1226. | ||
Orwoll ES, Scheele WH, Paul S, et al. The effect of teriparatide [human parathyroid hormone (1–34)] therapy on bone density in men with osteoporosis. J Bone Miner Res. 2003;18(1):9–17. | ||
Orwoll E, Ettinger M, Weiss S, et al. Alendronate for the treatment of osteoporosis in men. N Engl J Med. 2000;343(9):604–610. | ||
Ringe JD, Dorst A, Faber H, Ibach K. Alendronate treatment of established primary osteoporosis in men:3-year results of a prospective, comparative, two-arm study. Rheumatol Int. 2004;24(2):110–113. | ||
Sawka AM, Papaioannou A, Adachi JD, Gafni A, Hanley DA, Thabane L. Does alendronate reduce the risk of fracture in men? A meta-analysis incorporating prior knowledge of anti-fracture efficacy in women. BMC Musculoskelet Disord. 2005;6:39. | ||
Boonen S, Orwoll ES, Wenderoth D, Stoner KJ, Eusebio R, Delmas PD. Once-weekly risedronate in men with osteoporosis: results of a 2-year, placebo-controlled, double-blind, multicenter study. J Bone Miner Res. 2009;24(4):719–725. | ||
Boonen S, Orwoll E, Magaziner J, et al; HORIZON Recurrent Fracture Trial. Once-yearly zoledronic acid in older men compared with women with recent hip fracture. J Am Geriatr Soc. 2011;59(11):2084–2090. | ||
Ruza I, Mirfakhraee S, Orwoll E, Gruntmanis U. Clinical experience with intravenous zoledronic acid in the treatment of male osteoporosis: evidence and opinions. Ther Adv Musculoskelet Dis. 2013;5(4):182–198. | ||
Orwoll ES, Binkley NC, Lewiecki EM, Gruntmanis U, Fries MA, Dasic G. Efficacy and safety of monthly ibandronate in men with low bone density. Bone. 2010;46(4):970–976. | ||
Sim IeW, Ebeling PR. Treatment of osteoporosis in men with bisphosphonates: rationale and latest evidence. Ther Adv Musculoskelet Dis. 2013;5(5):259–267. | ||
Black DM, Cummings SR, Karpf DB, et al. Randomised trial of effect of alendronate on risk of fracture in women with existing vertebral fractures. Fracture Intervention Trial Research Group. Lancet. 1996;348(9041):1535–1541. | ||
Cummings SR, Black DM, Thompson DE, et al. Effect of alendronate on risk of fracture in women with low bone density but without vertebral fractures: results from the Fracture Intervention Trial. JAMA. 1998;280(24):2077–2082. | ||
Liberman UA, Weiss SR, Bröll J, et al. Effect of oral alendronate on bone mineral density and the incidence of fractures in postmenopausal osteoporosis. The Alendronate Phase III Osteoporosis Treatment Study Group. N Engl J Med. 1995;333(22):1437–1443. | ||
Pols HA, Felsenberg D, Hanley, DA et al. Multinational, placebo-controlled, randomized trial of the effects of alendronate on bone density and fracture risk in postmenopausal women with low bone mass: results of the FOSIT study. Fosamax International Trial Study Group. Osteoporos Int. 1999;9(5):461–468 . | ||
Harris ST, Watts NB, Genant HK, et al. Effects of risedronate treatment on vertebral and nonvertebral fractures in women with postmenopausal osteoporosis: a randomized controlled trial. Vertebral Efficacy With Risedronate Therapy (VERT) Study Group. JAMA. 1999;282(14):1344–1352. | ||
McClung MR, Geusens P, Miller PD, et al; Hip Intervention Program Study Group. Effect of risedronate on the risk of hip fracture in elderly women. Hip Intervention Program Study Group. N Engl J Med. 2001;344(5):333–340. | ||
Reginster JY, Minne HW, Sorensen OH, et al. Randomized trial of the effects of risedronate on vertebral fractures in women with established postmenopausal osteoporosis. Vertebral Efficacy with Risedronate Therapy (VERT) Study Group. Osteoporos Int. 2000;11(1):83–91. | ||
Chesnut III CH, Skag A, Christiansen C, et al; Oral Ibandronate Osteoporosis Vertebral Fracture Trial in North America and Europe (BONE). Effects of oral ibandronate administered daily or intermittently on fracture risk in postmenopausal osteoporosis. J Bone Miner Res. 2004;19(8):1241–1249. | ||
Black DM, Delmas PD, Eastell R, et al; HORIZON Pivotal Fracture Trial. Once-yearly zoledronic acid for treatment of postmenopausal osteoporosis. N Engl J Med. 2007;356(18):1809–1822. | ||
Cusano NE, Costa AG, Silva BC, Bilezikian JP. Therapy of osteoporosis in men with teriparatide. J Osteoporos. 2011;2011:463675. | ||
Kaufman JM, Orwoll E, Goemaere S, et al. Teriparatide effects on vertebral fractures and bone mineral density in men with osteoporosis: treatment and discontinuation of therapy. Osteoporos Int. 2005;16(5):510–516. | ||
Leder BZ, Neer RM, Wyland JJ, Lee HW, Burnett-Bowie SM, Finkelstein JS. Effects of teriparatide treatment and discontinuation in postmenopausal women and eugonadal men with osteoporosis. J Clin Endocrinol Metab. 2009;94(8):2915–2921. | ||
Neer RM, Arnaud CD, Zanchetta JR, et al. Effect of parathyroid hormone (1–34) on fractures and bone mineral density in postmenopausal women with osteoporosis. N Engl J Med. 2001;344(19):1434–1441. | ||
Cipriani C, Irani D, Bilezikian JP. Safety of osteoanabolic therapy: a decade of experience. J Bone Miner Res. 2012;27(12):2419–2428. | ||
Cummings SR, San Martin J, McClung MR, et al; FREEDOM Trial. Denosumab for prevention of fractures in postmenopausal women with osteoporosis. N Engl J Med. 2009;361(8):756–765. | ||
Papapoulos S, Chapurlat R, Libanati C, et al. Five years of denosumab exposure in women with postmenopausal osteoporosis: results from the first two years of the FREEDOM extension. J Bone Miner Res. 2012;27(3):694–701. | ||
Bone HG, Chapurlat R, Brandi ML, et al. The effect of three or six years of denosumab exposure in women with postmenopausal osteoporosis: results from the FREEDOM extension. J Clin Endocrinol Metab. 2013;98(11):4483–4492. | ||
Smith MR, Egerdie B, Hernàndez Toriz N, et al; Denosumab HALT Prostate Cancer Study Group. Denosumab in men receiving androgen-deprivation therapy for prostate cancer. N Engl J Med. 2009;361(8):745–755. | ||
Orwoll E, Teglbjærg CS, Langdahl BL, et al. A randomized, placebo-controlled study of the effects of denosumab for the treatment of men with low bone mineral density. J Clin Endocrinol Metab. 2012;97(9):3161–3169. | ||
Chavassieux P, Meunier PJ, Roux JP, Portero-Muzy N, Pierre M, Chapurlat R. Bone histomorphometry of transiliac paired bone biopsies after 6 or 12 months of treatment with oral strontium ranelate in 387 osteoporotic women: randomized comparison to alendronate. J Bone Miner Res. 2014;29(3):618–628. | ||
Blake GM, Fogelman I. Bone: strontium ranelate does not have an anabolic effect on bone. Nat Rev Endocrinol. 2013;9(12):696–697. | ||
Fogelman I, Blake GM. Strontium ranelate for the treatment of osteoporosis. BMJ. 2005;330(7505):1400–1401. | ||
Kaufman JM, Audran M, Bianchi G, et al. Efficacy and safety of strontium ranelate in the treatment of osteoporosis in men. J Clin Endocrinol Metab. 2013;98(2):592–601. | ||
Reginster JY, Seeman E, De Vernejoul MC, et al. Strontium ranelate reduces the risk of nonvertebral fractures in postmenopausal women with osteoporosis: Treatment of Peripheral Osteoporosis (TROPOS) study. J Clin Endocrinol Metab. 2005;90(5):2816–2822. | ||
Meunier PJ, Roux C, Seeman E, et al. The effects of strontium ranelate on the risk of vertebral fracture in women with postmenopausal osteoporosis. N Engl J Med. 2004;350(5):459–468. | ||
Blake GM, Fogelman I. The correction of BMD measurements for bone strontium content. J Clin Densitom. 2007;10(3):259–265. | ||
Protelos and Osseor [webpage on the Internet]. London: European Medicines Agency Available from: http://www.ema.europa.eu/ema/index.jsp?curl=pages/medicines/human/referrals/Protelos_and_Osseor/human_referral_prac_000025.jsp&mid=WC0b01ac05805c516f. Accessed June 8, 2014. | ||
Cooper C, Fox KM, Borer JS. Ischaemic cardiac events and use of strontium ranelate in postmenopausal osteoporosis: a nested case-control study in the CPRD. Osteoporos Int. 2014;25(2):737–745. | ||
Svanström H, Pasternak B, Hviid A. Use of strontium ranelate and risk of acute coronary syndrome: cohort study. Ann Rheum Dis. 2014;73(6):1037–1043. | ||
Kanis JA, Bianchi G, Bilezikian JP, et al. Towards a diagnostic and therapeutic consensus in male osteoporosis. Osteoporos Int. 2011;22(11):2789–2798. | ||
Giusti A, Bianchi G. Male osteoporosis. Reumatismo. 2014;66(2):136–143. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.