Back to Journals » Patient Preference and Adherence » Volume 19
Treatment Inertia Among Elderly Patients with Chronic Heart Failure: A Qualitative Study
Authors Jiao M, Wang W, Chen C ![]() , Zhang X
, Zhang X ![]() , Zhao X
, Zhao X ![]()
Received 10 September 2025
Accepted for publication 28 November 2025
Published 9 December 2025 Volume 2025:19 Pages 3973—3984
DOI https://doi.org/10.2147/PPA.S560907
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Emma Veale
Mengfan Jiao,1,2,* Wei Wang,1,* Chunxu Chen,1 Xiaoman Zhang,1 Xiaojing Zhao1
1Department of Cardiology, Shandong Provincial Hospital Affiliated to Shandong First Medical University, Jinan, 250021, People’s Republic of China; 2Department of Nursing, Shandong First Medical University and Shandong Academy of Medical Sciences, Taian, 271099, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaojing Zhao, Email [email protected]
Background: Treatment inertia in chronic heart failure (CHF) commonly refers to the failure to initiate or intensify evidence-based therapy in a timely manner and refers to delays, avoidance, or inadequate engagement by patients in evidence-based therapy. While the clinician or healthcare system level have been extensively studied, patient-level inertia among elderly adults remain under-investigated due to limited health literacy patient-related factors, particularly in China where healthcare access, insurance policies, and literacy levels differ significantly. Understanding the behavioral and contextual determinants of this phenomenon is crucial for improving disease management among aging populations.
Purpose: Guided by the COM-B (capability–opportunity–motivation–behavior) framework, this qualitative study explored patient-level treatment inertia and its influencing factors among elderly Chinese patients with CHF, aiming to inform culturally tailored interventions.
Methods: A descriptive phenomenological design was adopted. Semi-structured interviews were conducted with 14 hospitalized CHF patients aged ≥ 60 years from May to July 2024 in a tertiary hospital in Shandong Province. Data were analyzed using Colaizzi’s seven-step method, following COREQ criteria for qualitative research reporting.
Results: Three themes emerged: (1) deficient capability (insufficient symptom perception and low health literacy); (2) weakened motivation (multiple pressures, distrust in medical technology, limited engagement incentives); (3) constrained opportunity (insufficient family support and limited medical resources).
Conclusion: Patient-level treatment inertia among elderly CHF patients arises from the interaction of cognitive, motivational, and systemic constraints. Enhancing health literacy, improving psychosocial motivation, and establishing family and community-based support systems may mitigate inertia and improve patient outcomes.
Keywords: heart failure, treatment inertia, influencing factors, COM-B model, qualitative research
Introduction
Chronic heart failure (CHF), a chronic condition resulting from prolonged cardiac overload or myocardial injury, usually leads to compromise in the heart’s pumping function.1 Heart failure is a major global health concern, with an estimated 64 million people worldwide. It is projected that the prevalence of HF will increase due to the ageing of the population.2 In China, the prevalence reached approximately 1.3% in 2019, translating to nearly 13 million affected individuals.3 Despite significant advances in pharmacological and device-based therapy, treatment adherence and disease management remain suboptimal, particularly among elderly patients, resulting in repeated hospitalizations and disease progression. In addition, the unique structure of China’s healthcare and medical insurance systems further affects patients’ treatment behaviors.
Treatment inertia, which refers to the failure to promptly initiate or intensify treatment based on evidence-based clinical guidelines, is very likely to results in the inability to achieve or maintain treatment goals and disease control.4 In this study, we focus on patient-level treatment inertia, defined as the failure or delay of patients to initiate, maintain, or escalate therapy according to medical advice, due to capability, opportunity, or motivational barriers. Such inertia reflects not only individual capability and motivation but also the accessibility and structure of healthcare systems.
Compared to middle-aged and young patients with CHF, older adults are particularly prone to treatment inertia due to limited health literacy, misconceptions about symptoms, and reduced motivation for self-management.5 However, this attitude poses obstacles to the timely and adequate management of their condition. While the European Society of Cardiology (ESC, 2023) and the American Heart Association (AHA, 2022) emphasize patient empowerment and shared decision-making as key strategies for overcoming inertia in heart failure management.6,7 However, such recommendations face challenges in China’s partially insurance.
In China’s healthcare system, patients choose to participate in employee medical insurance or resident medical insurance based on their job nature, with the reimbursement rates differing by about 20%. Although emergency and outpatient treatments can receive partial reimbursement, many chronic disease medications still require out-of-pocket payments.8 Reimbursement rates also drop when patients seek cross-regional care. Meanwhile, urban-rural resource gaps and variable primary-care capability can delay timely escalation.9 Collectively, these structural features interact with low literacy and aging-related vulnerabilities to reinforce patient-level inertia.
Existing studies have mainly explored physicians’ clinical inertia, whereas patients’ psychosocial barriers to treatment are under-researched.10 Therefore, this study adopted a descriptive phenomenological approach within the COM-B framework to explore treatment inertia among elderly CHF patients in China’s healthcare context. The findings aim to provide evidence-based insights for improving treatment outcomes in this population.
Materials and Methods
Study Design
A descriptive phenomenological qualitative study was conducted from May to July 2024 in a tertiary hospital in Shandong Province, China. Semi-structured interviews were used to elicit in-depth narratives on treatment-related behaviors.
Participants and Sampling
The study employed a purposive sampling method to select CHF patients hospitalized in a tertiary hospital in from May to July 2024 as the research participants. Inclusion criteria for patients: (1) Hospitalized patients aged ≥60 years old; (2) Diagnosed with chronic heart failure; (3) NYHA classification of II to IV, with stable condition; (4) Clear consciousness and ability to express clearly; (5) Voluntarily participated in the study and consented to interviews and recordings. Exclusion criteria: (1) Concurrent malignancy or other severe physical illnesses; (2) Presence of consciousness disturbance, unconsciousness, or major mental illnesses.
A total of 20 patients were approached, with 14 agreeing to participate, 6 declined (3 due to fatigue, 2 disinterest, 1 family refusal). Sample size was determined by data saturation, which was achieved after 12 interviews, with two additional interviews conducted to confirm no new themes emerged.
Theoretical Framework
The COM-B (capability, opportunity, motivation, behavior) theoretical model was used as theoretical guidance to guide data collection and analysis. It explains that people need capability, opportunity and motivation to engage in behavior.11 The advantage of this model lies in its ability to explore the factors that contribute to patients’ treatment inertia and provide scientific advice for their rehabilitation treatment. Based on the COM-B model, this study analyzed the determinants of treatment inertia from the perspective of patients.
Data Collection
Semi-structured, face-to-face interviews were conducted in quiet hospital meeting rooms. An interview outline was developed for medical staff and patients based on COM-B models. After the interview outline is drawn up, researchers familiar with the subject are invited to revise it. After the pre-experiment, the interview outline was modified again to form the final interview outline (Table 1). Prior to the interview, the demographic data of the participants were collected, the interviewer introduced the purpose and content of the interview to the participants so as to, gain their trust and consent, and eventually obtain a signed informed consent. The interviewer recorded the entire interview, with each interview lasting within a duration of 20–40 minutes which was adjusted according to the participants’ emotions and actual situation. After the interviews, the two researchers transcribed the interviews verbatim into text within 24 hours. The interview content was returned to the participants to ensure its authenticity and the interviews were concluded when no new information emerged, indicating data saturation. To protect the patients’ privacy, participants were referred to by codes A1-A14 instead of their names.
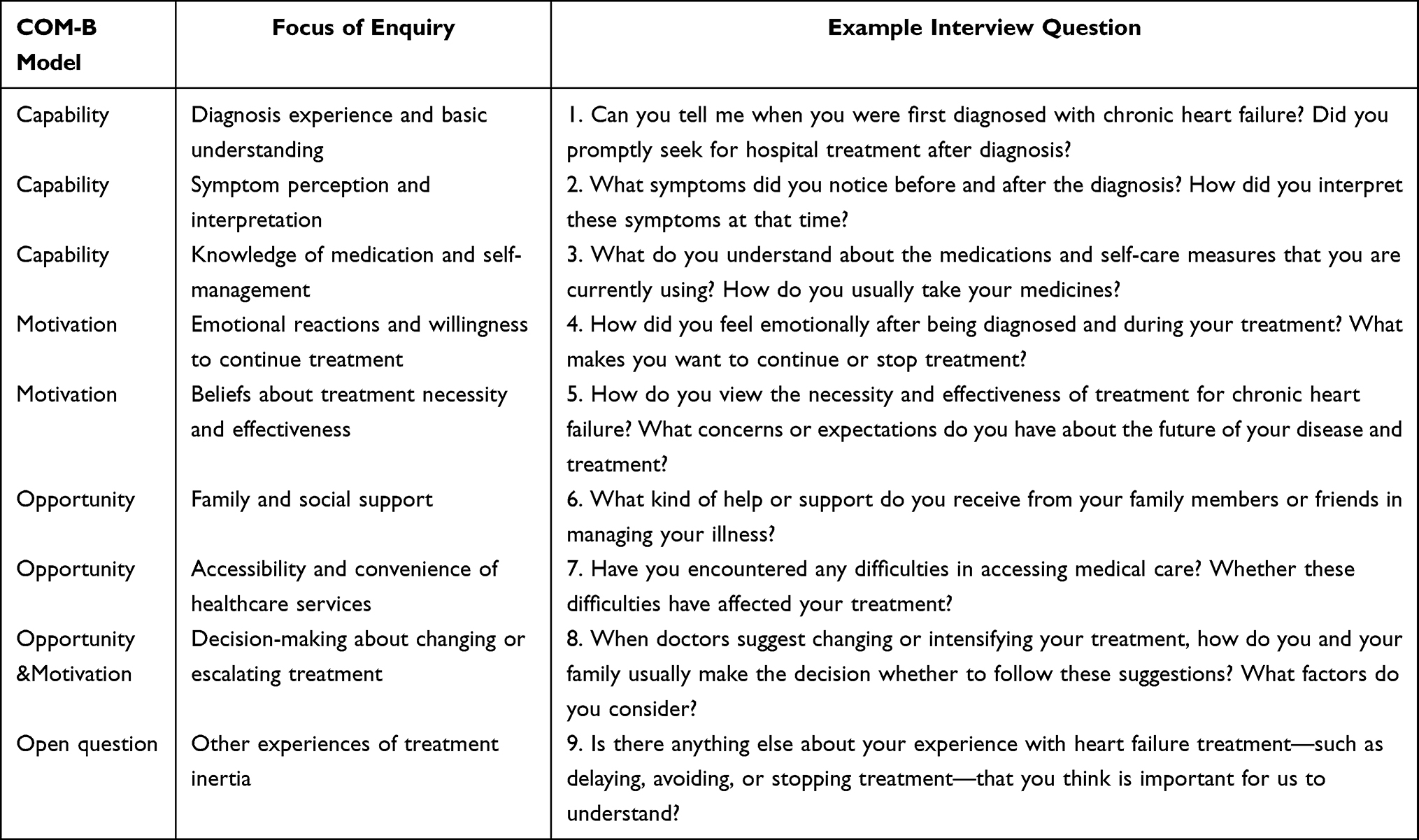 |
Table 1 The Interview Guide for Participants |
Data Analysis
Within 24 hours after the interview, the audio recordings were transcribed into textual form. If there were any disagreements with the contents of the transcripts among the researchers, the researcher would confirm with the participants to clarify their opinions. To ensure credibility, dependability, and confirmability, the study adhered to the COREQ guidelines.12
NVivo 15 software was used to manage the qualitative data. Colaizzi’s method was adopted for data analysis: (1) meticulously and repeatedly combing through the interview data; (2) analyzing and extracting significant content that emerged from the data; (3) refining and coding the recurring content; (4) categorizing and summarizing the coded content; (5) conducting a detailed analysis of the coded content to distill themes; (6) organizing the analyzed interview data to derive meaningful conclusions; (7) verifying the derived themes with the participants to ensure the accuracy of the results.
Ethics
Ethical approval was obtained from the Ethics Committee of Shandong Provincial Hospital Affiliated to Shandong First Medical University (Approval No. 2022-269). The research strictly adhered to the Declaration of Helsinki. The informed consent form was endorsed by each included participant after they were all informed about the study and volunteered to participate. To protect the patients’ privacy, participants were referred to by codes A1-A14 instead of their names. Participants were informed that they could withdraw from the study at any time or refuse to answer any questions.
Results
A total of 14 CHF patients were interviewed in this study, including 8 males and 6 females, aged 60 to 77 years, with an average age of (67.0 ± 4.96) years. Most participants reported delaying treatment or passive treatment behaviors. The number of comorbidities was (4.1±1.9), and the average number of tablets taken by patients was (8.1±2.8) types. The demographic characteristics are shown in Table 2. The dosage of the main drugs and the number of people who used the drugs are shown in Table 3.
 |
Table 2 Patient Characteristics (n=14) |
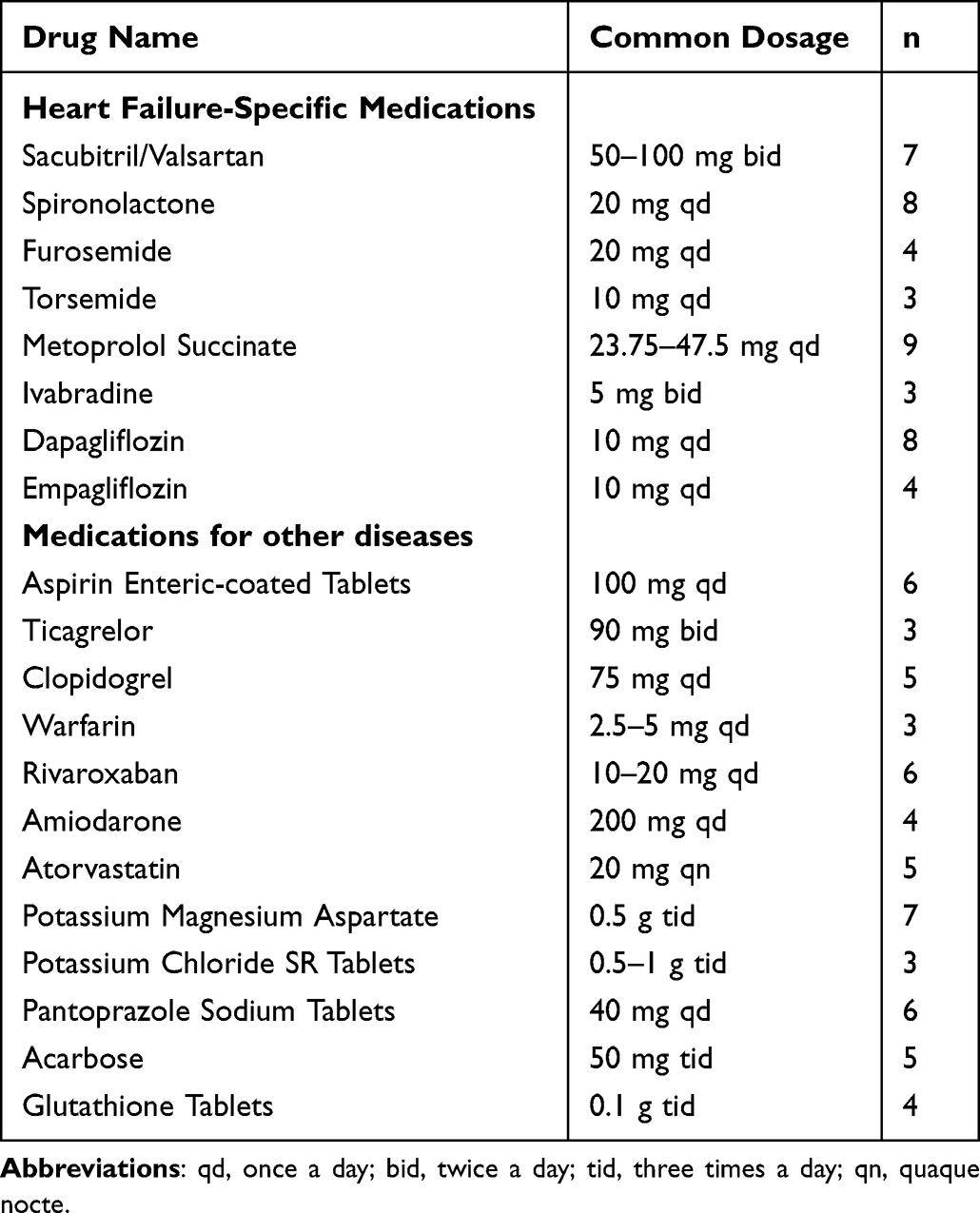 |
Table 3 Main Medication Profile of the Patient |
Thematic analysis of the interviews revealed three major themes and seven sub-themes, including deficient capability, weakened motivation and constrained opportunity. These themes correspond to the three core components of the COM-B model—Capability, Motivation and Opportunity. Additionally, interview data were also given to illustrate these main themes emerging during the analysis (Table 4).
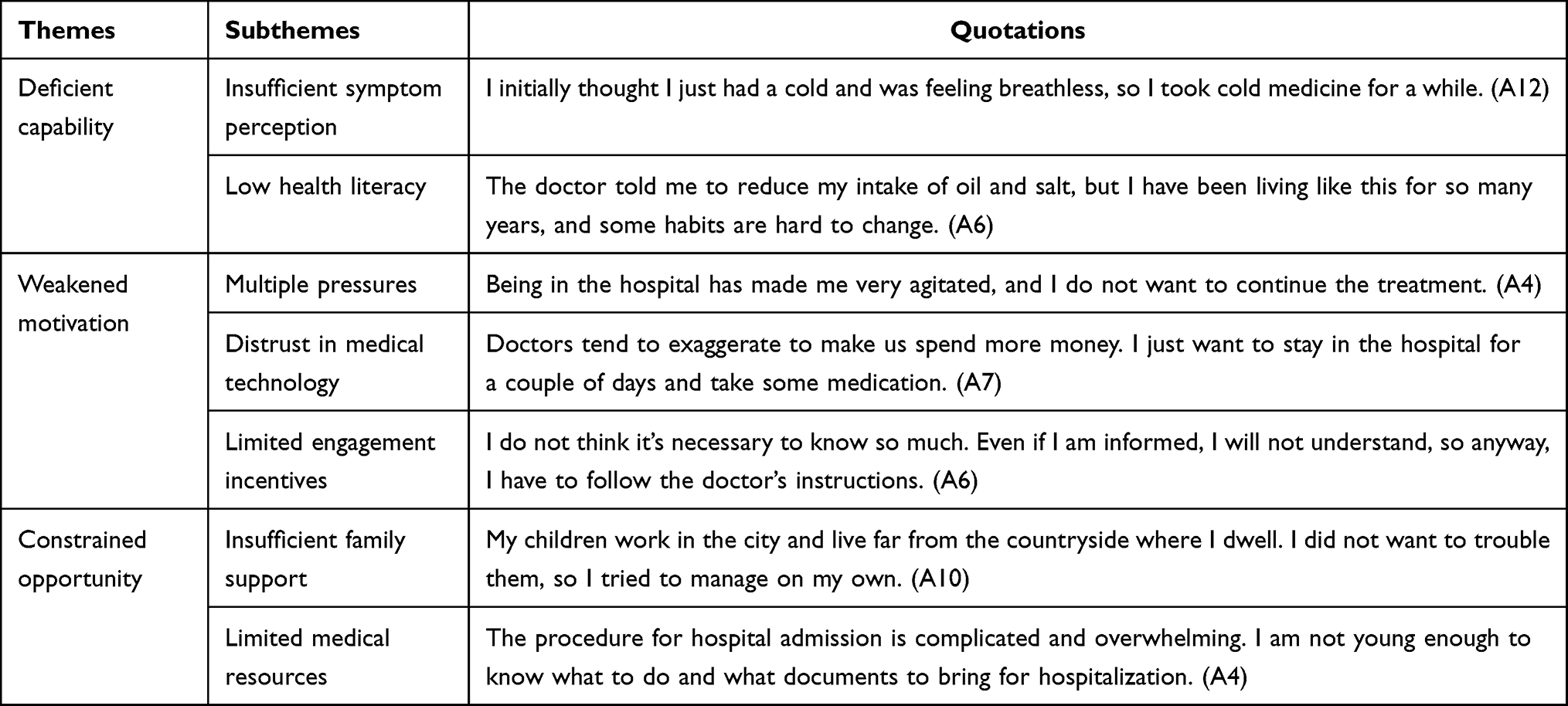 |
Table 4 Themes, Subthemes and Quotations |
Theme 1: Deficient Capability
Insufficient Symptom Perception
With the progression of the disease, it is common that patients with CHF often experience a series of symptoms such as chest tightness, fatigue, and edema. However, most elderly cases lack the ability to perceive these symptoms accurately, making it difficult for them to appropriately monitor the symptoms and severity of their condition. Many patients, although exhibited obvious heart failure symptoms before hospitalization, mistook them for other illnesses due to their inability to discern, thereby delaying treatment and exacerbating their condition.
One said:
I suddenly couldn’t catch my breath, and my heart was racing. I thought it was due to my blood sugar, so I kept taking my diabetes medication till the symptoms were eased. But when I felt unwell again, the medication didn’t work anymore, so I came to the hospital. [A1]
Another one said:
I initially thought I just had a cold and was feeling breathless, so I took cold medicine for a while, but it didn’t improve anything. When I couldn’t bear it anymore, I came to the hospital for a check-up. [A12]
At first, I couldn’t catch my breath, and even slight movements made me gasp for air. I thought I was just tired, so I rested for a while, but I still felt chest tightness and shortness of breath. I didn’t consider it to be related to heart disease at all. [A14]
Some patients, who experience sudden symptoms such as chest pain, are unaware that the symptoms represent heart failure and therefore are unaware of their higher risk of worsening.
Low Health Literacy
The majority of elderly patients exhibit low levels of health literacy due to a lack of knowledge about their condition, consequently leading to poor self-management and compliance. Meanwhile, elderly patients with heart failure often have multiple comorbidities and take various medications, which can be confusing for older adults. As a result, some elderly patients do not follow medical advice and take medications based on their own judgment, leading to uncontrolled conditions. According to the patients who were re-admitted into the hospital, most of them reported that they failed to strictly follow medical advice, in addition to neglecting the importance of self-management practices such as medication adherence and diet.
Just as a participant stated:
I was careless and didn’t think it was as serious as the doctor said, so I relaxed my medication regimen. A few days later, I felt terrible and had to come back to the hospital. It’s a lesson learned. [A2]
Some patients who have improved their symptoms through treatment believe they are in good or healthy condition and therefore do not follow their doctor’s advice.
One participant described:
The doctor prescribed me a quarter of the pill, how could I remember it, and the pill was not easy to break, so I took half or a whole pill. [A13]
Furthermore, some patients indicated that they were unable to alter their existing lifestyle habits and therefore could not engage in rigorous self-management. These behaviors were considered to be the primary reasons for the patients’ exacerbation of symptoms and subsequent re-hospitalization. For instance:
The doctor told me to reduce my intake of oil and salt, but I’ve been living like this for so many years, and some habits are hard to change. I didn’t think it was necessary to be so strict with my diet. [A6]
Theme 2: Weakened Motivation
Patients Face Multiple Pressures
Heart failure, being a chronic condition requiring long-term treatment with recurrent episodes, imposes significant economic pressures and psychological burdens on most elderly patients.
Some patients delay initiating or escalating treatment owing to concerns about the high costs of hospitalization, ultimately ending up with inadequate and untimely treatment. For example:
I am a farmer who needs to work the land. Being trapped in the hospital means I can’t work, and I am losing my earnings. At the same time, the hospital bills are enormous. [A5]
A patient shared:
When I arrived at the county hospital, the doctor diagnosed me with heart complications and recommended hospitalization for better care. However, the exorbitant costs kept me from getting treatment, which eventually worsened my condition and forced me into hospitalization. Although the medical insurance covered half the expenses, it was still far from enough for us. I couldn’t afford the long-term hospitalization costs. [A9]
Additionally, some patients express that their emotions are negatively impacted by the disease, thus resulting in a passive attitude towards treatment.
And the patient said:
I’ve been hospitalized for so long, and I’ve been in critical condition several times. I even don’t know if it is possible for me to recover. Being in the hospital has made me very agitated, and I don’t want to continue the treatment. [A4]
Distrust in Medical Technology
Most elderly heart failure patients have limited knowledge about disease management and cognitive limitations regarding treatment options and medical technologies. This leads some to believe hospitalization can not cure their condition, resulting in treatment denial or delays due to lack of confidence.
One patient described:
I’ve been suffering from this illness for years, and it’s never been cured. I’m hospitalized every day, and I’ve been on life-threatening status several times. I keep wondering if hospitalization is useless at all. I don’t want to be treated, but there’s nothing I can do. [A5]
Additionally, many patients remain skeptical about advanced treatment plans, viewing them as potentially risky and unwilling to undergo such procedures.
One said:
I think my current treatment plan is quite good. With injections and medications, there’s no need to try new treatments, which, I reckon, might not be safe enough. [A3]
And Another pointed out:
I’m reluctant to upgrade my treatment. The current treatment is sufficient. Besides, the reason I’m so ill is that the doctor who treated me initially was incompetent and failed to diagnose my heart failure. So I don’t think the upgrade treatment will work for me. [A11]
Limited Engagement Incentives
Active participation and cooperation from patients are crucial for the rehabilitation of CHF patients. However, most elderly patients perceive heart failure as an incurable disease, lacking confidence in treatment and believing that it is solely the doctors’ responsibility. For example:
I had heard that this disease could not be cured before. After I was diagnosed, I felt that the sky had collapsed. How could I get such a disease? At first, I thought I would not treat it, anyway, it could not be cured. [A7]
It’s not my business to keep a watchful eye on the treatment, it’s the doctor’s responsibility. As patients, we just follow their instructions. I know this illness can’t be cured, so I just let nature take its course. [A14]
Consequently, they demonstrate limited enthusiasm and involvement in the treatment process. A patient said:
I don’t think it’s necessary to know so much. Even if I’m informed, I won’t understand, so anyway, I have to follow the doctor’s instructions. [A6]
Theme 3: Constrained Opportunity
Insufficient Family Support
Family support can be a powerful strength against patients’ treatment inertia. Since elderly patients often experience anxiety and fear, therefore necessitating emotional care from their families after illness onset, adequate family support can enhance patients’ confidence and motivation in their treatment for CHF.
However, when family support is insufficient, Elderly patients often delay seeking medical care due to transportation difficulties or unfamiliarity with registration procedures, patients may exhibit delayed or inactive treatment behaviors. For example:
My children work in the city and live far from the countryside where I dwell. I didn’t want to trouble them, so I tried to manage on my own. [A10]
I’ve been feeling unwell for a long time, but I was afraid of burdening my children. I didn’t know how to arrange hospitalization, so I kept putting it off. Only when I couldn’t bear it anymore, I told them, and they brought me to the hospital for examination. That’s when we found out it was heart failure. [A12]
Limited Medical Resources
It is known that medical resources are crucial for patients’ treatment, and providing sufficient resources can enhance patients’ confidence on treatment. Elderly patients, due to mobility limitations and cognitive decline, tend to have higher demands for medical resources. However, the inadequacy of these resources often leads to patients losing patience and motivation for treatment.
When the hospital’s elderly service system is not perfect and can not effectively help elderly patients to deal with hospitalization, these patients will have inertia and delay seeking medical treatment.
One participant stated:
The procedure for hospital admission is complicated and overwhelming. I am not young enough to know what to do and what documents to bring for hospitalization, and I have to queue up early in the morning to wait for registration, fearing there will be no vacant hospital bed available. [A4]
At the same time, some departments are short of beds, so patients cannot be hospitalized in time. For instance:
Before I came here, I was informed that this hospital was always short of beds. When I arrived, I had to wait for two days. I am not a local, so I waited downstairs every day before admission. If it wasn’t for the fear of delaying treatment, I wouldn’t have wanted to be hospitalized here. [A9]
I came for treatment two months ago and was prescribed medication for heart failure, but there were no beds available. I’ve been waiting for two months. It’s difficult to get admitted for treatment. [A11]
Discussion
This study applied the COM-B framework to explore behavioral and contextual determinants of patient-level treatment inertia among elderly Chinese patients with CHF. The analysis highlights how deficits in capability, limited opportunity, and weakened motivation mutually reinforce behavioral inertia, leading to suboptimal disease management and poor prognosis. Compared with international findings, the unique structure of China’s healthcare system-partial medical insurance coverage, regional disparities in access, and the pivotal role of family care giving-adds additional layers to the behavioral mechanisms underlying treatment inertia.
Capability: Strengthening Health Literacy and Self-Management Skills
Studies have shown that most of the CHF patients are still ignorant about their disease, with older patients exhibiting lower treatment motivation and health literacy. This, in turn, predisposes elderly patients to treatment inertia, thus negatively impacting treatment outcomes and increasing the risk of rehospitalization as well as disease progression.
Consistent with findings from the European Heart Failure Association and BMC Nursing, inadequate disease knowledge strongly predicts medication omission and delayed medical contact.13,14 In our study, misinterpretation of breathlessness or fatigue as “a cold” led to treatment delays averaging several days. CHF is a progressive disease that, if not appropriately treated and managed, can lead to gradual worsening of symptoms. According to the COM-B model, capability encompasses both physical and psychological capacity to engage in a behavior. Enhancing patient capability thus requires systematic education strategies that match cognitive and literacy levels of elderly populations.
In China, health education for CHF is often fragmented and concentrated in hospitals, resulting in limited continuity after discharge. To address this, a tiered health education model should be implemented. Hospitals could standardize educational materials, while community nurses deliver continuous, simplified reinforcement using pictorial or video tools suitable for low-literacy groups.15 Mobile health platforms, such as WeChat Mini Programs or Healthy China App, could be leveraged for remote follow-up and self-monitoring. At the same time, the scope of discharge monitoring is expanded. Establishing “Heart Failure Self-Management Clinics” within community health centers would further enhance patients’ capability through routine assessment, personalized coaching, and feedback on self-care behaviors.
Motivation: Addressing Psychological Burden and Building Trust
Elderly CHF patients universally face multiple treatment-related stresses, which not only induce treatment inertia but also negatively retard physical recovery through associated negative emotions.16,17 Many interviewees in this study expressed having experienced multiple pressures, which, coupled with negative emotions, fostered a sense of treatment inertia and hindered timely and adequate treatment.18 Meanwhile, some patients distrust or resist disease treatment due to insufficient understanding of medical technology or experience of misdiagnosis. Severe psychological stress often causes avoidance behaviors, thereby decreasing patients’ treatment adherence and self-management capabilities, ultimately resulting in delayed or inadequate treatment and adverse health outcomes.19,20
According to the COM-B model, motivation reflects both reflective (beliefs, intentions) and automatic (emotional) processes that drive behavior. Motivation determines whether knowledge is transformed into sustained behavior. In this study, emotional exhaustion, financial stress, and distrust in medical technology weakened patients’ willingness to maintain treatment adherence. Consistent with previous research, fatalistic attitudes and low self-efficacy are common psychological barriers among elderly Chinese patients with chronic diseases.
To enhance motivation, psychological and cultural factors must be addressed in tandem with economic concerns. Firstly, nursing-led psychological counseling combined with peer support can mitigate depression, anxiety, and hopelessness. Research has demonstrated that timely and effective psychological guidance can help patients shift their mindset, improve treatment adherence and thereby reduce mortality and disease recurrence rates.21,22 Secondly, shared decision-making (SDM) should be integrated into the clinical workflow. Although SDM is recommended by the ESC and AHA, its adaptation to China requires simplified communication formats-visualized treatment options, cost explanations, and family-inclusive discussions to rebuild patient trust. Thirdly, to reduce the perceived financial burden, policy-level adjustments such as expanding outpatient drug reimbursement for CHF medications and implementing “chronic disease management packages” within community insurance programs could enhance treatment continuity and perceived value.
Moreover, building trust requires transparent communication and continuity of care. Healthcare professionals should provide personalized psychological support to elderly patients by deepening the understanding on their needs and feelings, as well as offering care and reassurance, thereby reducing psychological distance and improving adherence motivation.
Opportunity: Creating Supportive Family and System Environments
Opportunity factors in the COM-B model encompass environmental and social enablers of behavior. In China, elderly patients’ treatment adherence is heavily shaped by family structure, medical accessibility, and administrative convenience. In this study, many elderly participants lacked family care giving and experienced logistical barriers such as hospital overcrowding, long registration queues and transportation difficulties. These systemic constraints reflect the structural nature of treatment inertia.
Strengthening opportunity thus requires multi-level action. At the micro level, family- inclusive education should empower relatives with basic care giving skills, symptom monitoring knowledge and emotional support techniques. It is worth noting that the benefits of social support on elderly patients cannot be overlooked. Higher levels of social support correlate with better self-care, reduced negative emotions, as well as increased treatment motivation and participation among patients. As the primary living environment, care support system for patients, and family emotional support are all indispensable for boosting treatment confidence among elderly CHF patients.23 Family members can act as behavioral reinforcers within the COM-B model, maintaining patients’ daily adherence behaviors, thereby being able to achieve the goal to improve family support and alleviate patients’ depressive emotions.
At the meso level, hospitals should implement age-friendly service pathways-simplifying admission and reimbursement procedures, offering volunteer navigation and tele-registration systems, and prioritizing high-risk CHF patients for rapid access. Establishing multidisciplinary heart-failure teams that integrate nursing, psychology, pharmacy, and nutrition professionals can also ensure coordinated support.24
At the macro level, strengthening motivation also requires reducing the systemic and financial uncertainties faced by elderly patients. In China, fragmented information systems across regions often prevent seamless sharing of medical records, leading to repeated examinations, higher out-of-pocket costs, and reduced confidence in the care process.25 To address this, establishing a nationally integrated health-information platform that enables real-time data sharing across provinces would allow full transparency of patients’ diagnostic and treatment histories.26 Such interoperability would support mutual recognition of diagnostic tests, improve care continuity, and substantially reduce unnecessary repeat testing, thereby alleviating financial burden, especially for patients with limited income. By lowering avoidable costs and improving efficiency, a nationwide information-sharing system can enhance patients’ perceived value of treatment and strengthen their motivation to seek timely and continuous care.
Strengthening Primary Healthcare and Health System Coordination
In recent years, although the level of diagnosis and treatment of heart failure in China has improved, there still exists a situation of inadequate diagnosis and treatment, as well as improper treatment in clinical practice.27 Improving the quality of heart failure management in China requires not only strengthening the application of clinical guidelines but also enhancing the service capacity and interpretive ability of primary healthcare institutions. In many regions, poor primary care infrastructure means patients cannot be treated effectively locally, especially the elderly and have to travel across the country for treatment. However, the functional decline, limited mobility and transportation difficulties of elderly patients often make them give up cross-regional medical treatment, which eventually leads to treatment delay and treatment inertia. To mitigate this, training programs should prioritize improving primary healthcare providers’ understanding and implementation of guideline-based therapy, thereby enhancing the quality of primary care services. Simultaneously, a vertical management system should be established between tertiary hospitals and community healthcare institutions to ensure effective collaboration, thereby reducing the need for patients to seek treatment in distant locations.
Under the current China medical insurance system, the reimbursement rate for local medical treatment is relatively high (70–80%), but the reimbursement rate for cross-regional treatment drops to about 50%. This policy unintentionally discourages patients, particularly those on limited incomes, from seeking timely advanced care, reinforcing treatment inertia through economic pressure.28 Policymakers should therefore increase outpatient and chronic disease reimbursement for resident insurance, and gradually narrow the reimbursement gap between resident and employee medical insurance.29 Furthermore, enhancing hospital to hospital collaboration, such as through regular tele-consultations and remote multidisciplinary case discussions led by tertiary centers, would reduce unnecessary interregional transfers, lower patients’ out-of-pocket costs, and prevent delayed treatment due to financial or logistical constraints.30 These reforms would not only improve equity and timeliness of access but also protect vulnerable elderly patients from financial hardship and promote early, continuous management of chronic heart failure.31
Limitations
This study was conducted in a single province with a small sample, potentially limiting transferability. And as with most qualitative studies, potential recall bias exists in patient reports. Finally, while data saturation was achieved, a larger sample might have revealed additional insights. Future multi-center and mixed-method studies are recommended to validate these findings and quantify treatment inertia.
Conclusion
Applying the COM-B framework illuminated how cognitive limitations, motivational deficits, and systemic barriers jointly sustain treatment inertia among elderly CHF patients.
Enhancing patient capability through tailored education, addressing emotional stressors, strengthening family support, and ensuring equitable healthcare access are critical to improving adherence and outcomes. Integrating these findings into national CHF management programs may reduce rehospitalization and mortality. Future efforts should focus on developing and implementing targeted strategies to address the specific barriers identified in this study, particularly within China’s unique healthcare context.
Data Sharing Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request. The data are not publicly available due to privacy or ethical restrictions.
Ethics Approval
This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Shandong Provincial Hospital Affiliated to Shandong First Medical University (Approval No. 2022-269).
Consent for Publication
All participants signed informed consent, including permission to publish anonymous responses and direct quotes.
Acknowledgments
The authors thank all patients for their participation in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Shandong Province Medical and Health Science and Technology Project (Grant ID: 202303010274).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Working Group on Heart Failure, National Center for Cardiovascular Quality Improvement (NCCQI). 2020 Clinical performance and quality measures for heart failure in China. Chin Circ J. 2021;36(3):221–238. doi:10.3969/j.issn.1000-3614.2021.03.002
2. Shahim B, Kapelios CJ, Savarese G, et al. Global public health burden of heart failure: an updated review. Card Fail Rev. 2023;9:e11. doi:10.3969/j.issn.1000-3614.2021.03.002
3. Hao G, Wang X, Chen Z, et al. Prevalence of heart failure and left ventricular dysfunction in China: the China Hypertension Survey, 2012–2015. Eur J Heart Fail. 2019;21(11):1329–1337. doi:10.1002/ejhf.1629
4. Sherrod CF, Farr SL, Sauer AJ. Overcoming treatment inertia for patients with heart failure: how do we build systems that move us from rest to motion? Eur Heart J. 2023;44(22):1970–1972. doi:10.1093/eurheartj/ehad169
5. Lan Y, Yi M, Wang X, et al. Application of rehabilitation nursing care based on fear-avoidance model of pain in older patients with chronic heart failure. J Nurs Sci. 2024;39(11):96–100. doi:10.3870/j.issn.1001-4152.2024.11.096
6. Heidenreich PA, Bozkurt B, Aguilar D, et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022;145(18):e895–e1032. doi:10.1161/CIR.0000000000001062
7. Baudry G, Girerd N, Cikes M, et al. Knowledge and application of ESC/HFA guidelines in the management of advanced heart failure. Eur J Heart Fail. 2025;27(6):1126–1135. doi:10.1002/ejhf.3530
8. Shen M, He W, Yeoh E-K, et al. The association between an increased reimbursement cap for chronic disease coverage and healthcare utilization in China: an interrupted time series study. Health Policy Plann. 2020;35(8):1029–1038. doi:10.1093/heapol/czaa087
9. Pu X, Wang Y, Zhang W, et al. Can basic medical insurance reduce elderly family income inequality in China? Front Public Health. 2022;10:838733. doi:10.3389/fpubh.2022.838733
10. Verhestraeten C, Heggermont WA, Maris M. Clinical inertia in the treatment of heart failure: a major issue to tackle. Heart Fail Rev. 2021;26(6):1359–1370. doi:10.1007/s10741-020-09979-z
11. Liu MR, Ren P, Liang FC, Jiang XR. Overview of the COM-B modeland its current application status. Chin Gen Pract Nurs. 2022;20(1):44–48. doi:10.12104/j.issn.1674-4748.2022.01.011
12. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
13. Sedlar N, Lainscak M, Farkas J. Self-care perception and behaviour in patients with heart failure: a qualitative and quantitative study. ESC Heart Fail. 2021;8(3):2079–2088. doi:10.1002/ehf2.13287
14. Kleman C, Turrise S, Winslow H, et al. Individual and systems-related factors associated with heart failure self-care: a systematic review. BMC Nurs. 2024;23(1):110. doi:10.1186/s12912-023-01689-9
15. Longhini J, Gauthier K, Konradsen H, et al. The effectiveness of nursing interventions to improve self-care for patients with heart failure at home: a systematic review and meta-analysis. BMC Nurs. 2025;24(1):286. doi:10.1186/s12912-025-02867-7
16. Xi X, Shen L, Ding X. Impact of psychosomatic comprehensive nursing care on negative emotion and cardiac function in postoperative acute myocardial infarction patients complicated with left heart failure treated by PCI. PJCCPVD. 2019;27(4):107–110. doi:10.3969/j.issn.1008-5971.2019.04.019
17. Zhao HX, Yuan Y, Chen CY. Effects of mindfulness-bdsed stress reduction training on negative emotions in elderly patients with chronic heart failure. Chin J Mod Nurs. 2018;24(19):2315–2318. doi:10.3760/cma.j.issn.1674-2907.2018.19.020
18. Veskovic J, Cvetkovic M, Tahirovic E, et al. Depression, anxiety, and quality of life as predictors of rehospitalization in patients with chronic heart failure. BMC Cardiovasc Disord. 2023;23(1):525. doi:10.1186/s12872-023-03500-8
19. Sbolli M, Fiuzat M, Cani D, et al. Depression and heart failure: the lonely comorbidity. Eur J Heart Fail. 2020;22(11):2007–2017. doi:10.1002/ejhf.1865
20. Ma M, Peng F, Jiang X, et al. Research progress on treatment burden of patients with chronic heart failure. Chin Nurs Res. 2023;37(10):1760–1764. doi:10.12102/j.issn.1009-6493.2023.10.013
21. Qiu AP, Wang JY, Liu SJ. Effect of psychological nursing intervention on mood, cardiac function, and quality of life in elderly patients with chronic heart failure. Hainan Med J. 2020;31(13):1766–1768. doi:10.3969/j.issn.1003-6350.2020.13.037
22. Gao J, Han M, Cao H, et al. Effect of early psychological nursing on bad mood and sleep in elderly patients with chronic heart failure. J Int Psychiatry. 2022;49(6):1131–1133, 1136. doi:10.13479/j.cnki.jip.2022.06.012
23. Wang YQ, Zhang HC, Sun XH, et al. Research progress on family care in patients with chronic heart failure from the perspective of family system theory. Chin J Nurs. 2023;58(13):1659–1664. doi:10.3761/j.issn.0254-1769.2023.13.020
24. Zhang S-Y. Chinese guidelines for the diagnosis and treatment of heart failure 2024. J Geriatric Cardiol. 2025;22(3):277–331. doi:10.26599/1671-5411.2025.03.002
25. Li Y, Lu C, Liu Y. Medical insurance information systems in China: mixed methods study. JMIR Med Inform. 2020;8(9):e18780. doi:10.2196/18780
26. Zeng M, Cheng H, Zhang W. The digital amplifier in medical insurance: how Chinese provincial pooling policy optimizes chronic disease management. Healthcare. 2025;13(20):2643. doi:10.3390/healthcare13202643
27. Zhang J, Zhang YH, Huang J, et al. National heart failure guideline 2023 (Simplified Version). Chin Circ J. 2023;38(12):1207–1238. doi:10.3969/j.issn.1000-3614.2023.12.001
28. Ma M, Tian W, Kang J, et al. Does the medical insurance system play a real role in reducing catastrophic economic burden in elderly patients with cardiovascular disease in China? Implication for accurately targeting vulnerable characteristics. Glob Health. 2021;17(1):36. doi:10.1186/s12992-021-00683-7
29. Du W, Liu P, Xu W. Effects of decreasing the out-of-pocket expenses for outpatient care on health-seeking behaviors, health outcomes and medical expenses of people with diabetes: evidence from China. Int J Equity Health. 2022;21(1):162. doi:10.1186/s12939-022-01775-5
30. Silva-Cardoso J, Juanatey JRG, Comin-Colet J, et al. The future of telemedicine in the management of heart failure patients. Card Fail Rev. 2021;7:e11. doi:10.15420/cfr.2020.32
31. Liu S, Li J, Wan D-Y, et al. Effectiveness of eHealth Self-management interventions in patients with heart failure: systematic review and meta-analysis. J Med Internet Res. 2022;24(9):e38697. doi:10.2196/38697
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Resilience in Informal Caregivers of Patients with Heart Failure in China: Exploring Influencing Factors and Identifying the Paths
Peng Y, Xu Y, Yue L, Chen F, Wang J, Sun G
Psychology Research and Behavior Management 2023, 16:1097-1107
Published Date: 6 April 2023
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025
Real-Life Experiences of Self-Capacity Management in Patients with Chronic Heart Failure: A Qualitative Study
Wang A, Zhang N, Li M, Mao Q, Ma A, Wang G, Li M, Li Q
Patient Preference and Adherence 2025, 19:1747-1762
Published Date: 17 June 2025
Factors Influencing Adherence to Dietary Interventions Among Patients with Gestational Diabetes Mellitus in China: A Qualitative Study Based on the COM-B Model
Jia CL, Wang LJ, Li LH, Lu YJ, Yang Y
Journal of Multidisciplinary Healthcare 2025, 18:4653-4663
Published Date: 5 August 2025