Back to Journals » International Journal of Women's Health » Volume 15
Treating Vestibular Migraine When Pregnant and Postpartum: Progress, Challenges and Innovations
Authors Teelucksingh S, Murali Govind R, Dobson R ![]() , Nelson-Piercy C, Ovadia C
, Nelson-Piercy C, Ovadia C ![]()
Received 9 October 2022
Accepted for publication 18 January 2023
Published 16 February 2023 Volume 2023:15 Pages 321—338
DOI https://doi.org/10.2147/IJWH.S371491
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Siara Teelucksingh,1,* Renuka Murali Govind,1,* Ruth Dobson,2,3 Catherine Nelson-Piercy,1,4 Caroline Ovadia4,5
1Department of Obstetric Medicine, Guy’s and St. Thomas’ NHS Foundation Trust, London, UK; 2Preventive Neurology Unit, Queen Mary University of London, London, UK; 3Department of Neurology, Royal London Hospital, London, UK; 4Department of Women and Children’s Health, King’s College London, London, UK; 5Department of Obstetrics and Gynaecology, Guy’s and St Thomas’ NHS Foundation Trust, London, UK
*These authors contributed equally to this work
Correspondence: Caroline Ovadia, Department of Women and Children’s Health, King’s College London, 10th Floor North Wing, St. Thomas’ Hospital, London, SE1 7EH, UK, Email [email protected]
Abstract: Vestibular migraine is a leading cause of vertigo in pregnancy and, although not a distinct migraine subtype, is an episodic syndrome associated with migraine. Vestibular migraine is associated with diverse symptoms such as vertigo, aura, allodynia, osmophobia, nausea, vomiting and tinnitus, many of which may be exacerbated by, masked or even dismissed in pregnancy. Vestibular migraine is likely an underdiagnosed and undertreated condition in pregnancy. The aetiology of vestibular migraine remains incompletely understood, although various theories have been proposed, including genetic predisposition, neurochemical dysregulation and pro-inflammatory mechanisms, all of which are derived from the pathophysiology of classical migraine. Physiologic changes to the endocrine, haematologic and vascular systems in pregnancy may affect pathophysiological processes in vestibular migraine, and can alter the course of symptoms experienced in pregnancy. These changes also predispose to secondary headache disorders, which may have similar presentations. There has been considerable progress in therapeutic advances in vestibular migraine prophylaxis and treatment outside of pregnancy. There is currently no significant evidence base for acute treatment or prophylaxis for pregnant patients, with treatment recommendations extrapolated from studies on classical migraine, and offered on a benefit versus risk basis. Challenges commonly encountered include difficulty establishing a diagnosis, in addition to recognising and treating neuropsychiatric and gestational co-morbidities. Anxiety, depression, hypertensive disorders and cardiovascular disease are closely associated with migraine, and important contributors to morbidity and mortality during pregnancy. Identifying and treating vestibular migraine during pregnancy offers a unique opportunity to impact future patient health through screening and early treatment of associated co-morbidities. There have been innovations in classical migraine therapy that may confer benefit in vestibular migraine in pregnancy, with emphasis on lifestyle modification, effective prophylaxis, abortive therapies, cognitive behaviour therapy and management of vestibular migraine-related comorbidities.
Keywords: vestibular, migraine, dizziness, vertigo, pregnancy
Introduction
Migraine is the most common neurological disorder in pregnancy and is an inherited tendency to have headaches with sensory disturbance that may manifest in complex and atypical ways. Whilst studies of classical migraine are abundant, we aim to focus on the progress, challenges and innovations encountered in the treatment of vestibular migraine in pregnancy and postpartum. We hope to improve awareness of vestibular migraine as a possible diagnosis in pregnant women presenting with dizziness, highlighting the challenges in making a diagnosis, and offer suggestions for differentiating vestibular migraine from alternative etiologies. This review also highlights commonly overlooked co-morbidities, and discusses existing evidence-based treatment options for vestibular migraine in pregnancy and postpartum. Finally, we consider emerging therapies and potential areas for future innovation and research.
Migraine affects 959 million people worldwide and is among the leading causes of days of work lost due to sickness.1 The highest prevalence of migraine occurs in females of childbearing age, estimated at 25%.1,2 Vestibular migraine is the most common cause of recurrent spontaneous vertigo, affecting up to 1% of the general population and 10% of the migraineurs; and has a female preponderance of 3:1.3
Physiologic changes to the endocrine, haematologic and vascular systems in pregnancy may affect pathophysiological processes in migraine and can predispose to the first presentation or an altered clinical course in people with a history of migraine.4 Diagnosing migraine during pregnancy can be challenging due to the variability in clinical presentation within individuals along with the increased risk of secondary headache disorders.
Vestibular migraine may present in the absence of a headache,5 and atypical presentations may pose diagnostic uncertainty. It is therefore likely to be underdiagnosed, undertreated and for co-morbidities to go unrecognised.
Vestibular migraine is associated with debilitating symptoms, particularly vertigo, nausea, vomiting, osmophobia and allodynia. These symptoms overlap with those typical of early pregnancy, and may mimic or be masked by nausea and vomiting of pregnancy. In this context, migraine symptoms may be triggered or exacerbated by dehydration and impaired nutrition. There has been significant progress in conceptualising the pathophysiology of vestibular migraine. This has helped to identify reversible causes, which are considered triggers, and to inform evidence-based effective treatment strategies.
Pre-pregnancy counselling (PPC) should be offered to women with a diagnosis of migraine.1 This is of benefit to highlight the natural history of migraine, and how symptoms may develop or change during the course of pregnancy. This is also an opportunity to review pharmacologic therapies, particularly anticonvulsants with known teratogenic effects, to counsel about the impact of nausea and vomiting in pregnancy and migraine exacerbation, risk of secondary headache disorders and other gestational syndromes such as preeclampsia, as well as to discuss lactation plans and future contraceptive options. Similarly, optimisation of pre-pregnancy health, for example, use of prenatal folic acid and completion of relevant vaccination courses, are of benefit in PPC.
Pharmacologic agents are often prescribed or endorsed on a benefit-risk basis. Patients should be counselled as such; they can be reassured about the safety of most first-line abortive and preventive medications. Innovations, such as calcitonin gene-related peptide blocking monoclonal antibodies, are not routinely recommended in pregnancy but may be selected after detailed counselling on the available data and with shared decision-making with the patient.1
Studies have demonstrated that migraine confers a predisposition to secondary headache disorders in pregnant patients, such as cerebral venous sinus thrombosis, preeclampsia and cerebrovascular disease, including transient ischaemic attacks and ischaemic stroke.6 It is therefore important that syndromes such as vestibular migraine are promptly diagnosed and healthcare workers remain vigilant to exclude secondary headache disorders when patients present with non-reassuring symptoms during an acute attack.7,8
There is an association between migraine and neuropsychiatric disorders, such as anxiety and depression. Functional neurological disorders may coexist with vestibular migraine.9 An atypical cluster of presenting symptoms and the concomitant occurrence of psychosomatic symptoms can lead to vestibular migraine being misdiagnosed as a functional neurological disorder. Patients with vestibular migraine, particularly those with chronic symptoms (>15 days/month), are prone to a deterioration in their quality of life and mental health, for which cognitive behaviour therapy may play an important role.3
In treating vestibular migraine, like in classical migraine, there is a disconnect between published literature and established clinical practice, where commonly used treatments often have a limited evidence base. It is often the case that treatment is individualised and offered on a benefit-risk basis.
Progress
The association between migraine and vertigo was first described in 1873,10,11 whilst the term “vestibular migraine” was first used by Dieterich and Brandt in 1999.12 Vestibular migraine had only been recognised as a distinct entity, and given a well-defined consensus diagnosis by The International Headache Society and the International Bárány Society for Neuro-otology in 2012.13
Vestibular migraine is diagnosed using four criteria as defined by the Third Headache Classification Committee.14 These are: a present of past history of migraine, at least five episodes of moderate or severe vestibular symptoms lasting between 5 minutes and 72 hours, and at least half of the episodes associated with at least one of three migrainous features (headache, photophobia, and/or phonophobia and visual aura). Typical migrainous headaches are characeterised by at least two of unilateral headache, pulsating quality, moderate or severe intensity, and aggravation by routine physical activity. Despite the misnomer, vestibular migraine is not strictly classified as a migraine subtype, but instead as an episodic syndrome that may be associated with migraine. Patients with vestibular migraine have a past or current history of migraine; a past history can precede the onset of vertigo by a mean duration of 8 years.15 It is important to note that, unlike classical migraine, headache may not be present in every attack.
Internal vertigo refers to a false sense of self-motion, while external vertigo refers to a false sense that the surroundings are spinning or flowing. Some patients may describe dizziness, characterised by a sensation of disturbed spatial orientation, with nausea triggered by head movement. Triggers include positional change, visual stimulus or head movement.14
Core symptoms of a vestibular migraine rarely last for more than 72 hours. Ten percent of the patients may experience symptoms for seconds, 30% for minutes, 30% for hours, and 30% may experience attacks over several days.16
Other migrainous features that are not listed in the diagnostic criteria, but may be encountered in patients with vestibular migraine, are osmophobia, neuropsychiatric symptoms such as emotional lability, autonomic symptoms, such as dry mouth and diarrhoea, nonspecific sensory changes, blurred vision, motion sickness susceptibility and Alice in Wonderland syndrome (AIWS) dysperceptions.17,18 Auditory disturbances, such as tinnitus, muffled hearing and ear fullness that typically occur in both ears, have also been reported in up to 60% of the patients.19
Pathophysiology
The pathophysiology of migraines is incompletely understood.20 Current understanding of the pathophysiology of vestibular migraine is based on hypotheses on the pathophysiology of classical migraine (Figure 1).
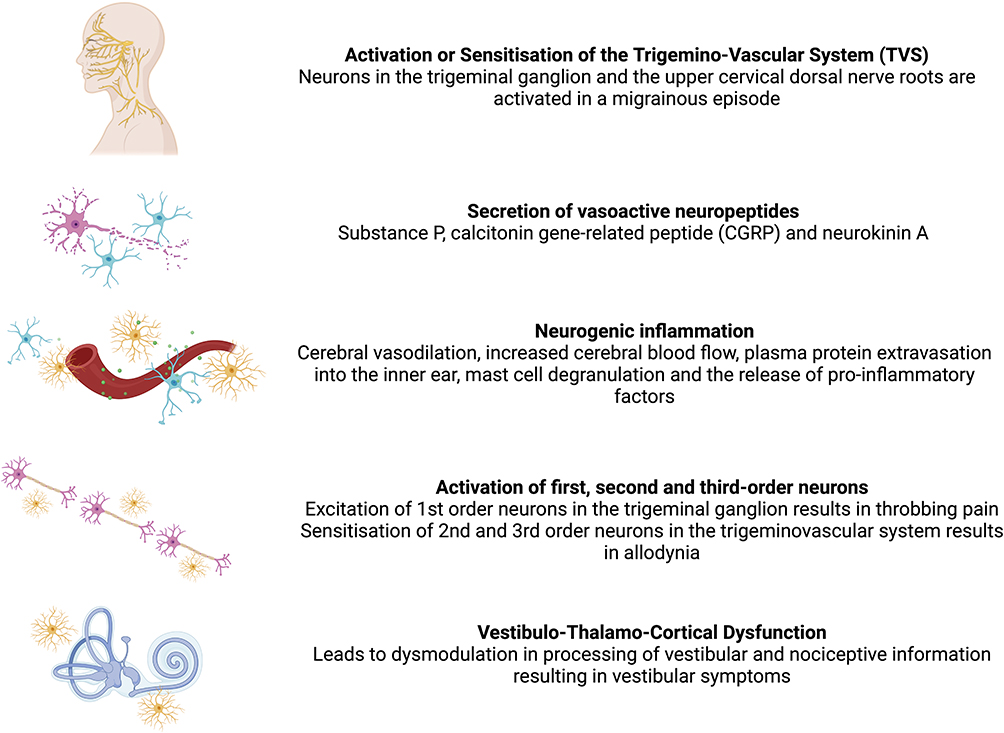 |
Figure 1 Neuropathological features of vestibular migraine. Created with BioRender.com. |
Genetic, epigenetic and environmental factors are thought to play a role in the pathophysiology of vestibular migraine. Familial vestibular migraine inheritance typically occurs with an autosomal dominant pattern, though no specific genes have yet been identified in their pathogenesis.21
It is believed that the trigemino-vascular system (TVS), which comprises neurons originating from the trigeminal ganglion and upper cervical dorsal nerve roots, is the anatomical location implicated in a migraine attack.20 Activation or sensitisation of the TVS results in the secretion of vasoactive neuropeptides, including substance P, calcitonin gene-related peptide, and neurokinin A. These neuropeptides in turn cause neurogenic inflammation, characterised by cerebral vasodilation, increased cerebral blood flow, plasma protein extravasation into the inner ear, mast cell degranulation and the release of pro-inflammatory factors. This results in increased excitability of first-order neurons in the trigeminal ganglion, causing throbbing pain. These mediators also sensitise second-order and third-order trigemino-vascular neurons (central sensitisation), causing allodynia.22
Cortical spreading depression (CSD) is another pathophysiological mechanism implicated in headache, visual, motor and auditory symptoms experienced during a migraine episode. CSD refers to the sequential spread of neuronal and glial depolarisation across the cerebral cortex, resulting in the activation of trigeminal nerve afferents and altered blood–brain permeability. This process results in inflammatory changes in the meninges, generating the headache experienced in a migraine attack.22
Vestibulo-thalamo-cortical dysfunction, which results in altered processing of vestibular and nociceptive information, is thought to be responsible for vestibular symptoms in a vestibular migraine.22
The natural history of migraine in pregnancy and the puerperium is influenced by physiologic changes to the endocrine system. Oestrogen levels rise during pregnancy and fall precipitously in the puerperium (Figure 2).7
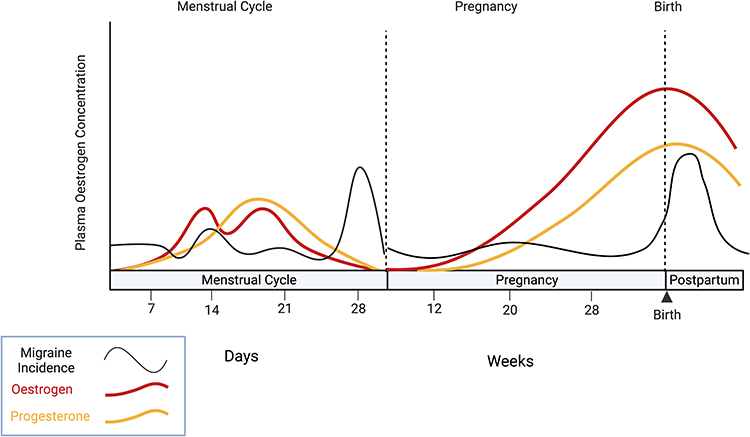 |
Figure 2 Oestrogen concentration and its effect on migraine incidence in the menstrual cycle, pregnancy and postpartum. Created with BioRender.com. Notes: Adapted from Handb Clin Neurol, 172, van Casteren DS, van den Brink AM, Terwindt GM. Migraine and other headache disorders in pregnancy. 187–199, copyright 2020, with permission from Elsevier.25 |
Patients with a previous history of migraine, particularly menstrual migraine, often report improvement during pregnancy due to loss of cyclical fluctuation of oestrogen levels. Whilst the number of patients with complete migraine remission in the first trimester is low (10.6%), improvement during the first trimester is seen in nearly half of cases (46.8%), and 85% report improvement in the second and third trimesters. Migraine with aura is less likely to improve or remit compared with migraine without aura.23
In clinical practice, migraine tends to recur toward the end of pregnancy and early postpartum period, likely influenced by sleep deprivation, stress and hormonal fluctuations.24
Management
There has been significant progress in the evidence available to treat vestibular migraine, most of which is in the form of retrospective case series and observational studies. Current treatment practices are extrapolated from existing guidelines on prophylactic and abortive treatment for classical migraine as there are currently no specific guidelines for the treatment of vestibular migraine in pregnancy.
Many abortive and preventive therapies used in classical migraine are safe in pregnancy and the puerperium. However, the effectiveness of classical migraine treatment for vestibular migraine remains inadequately investigated. Safety data for the use of novel treatments that have proven effective for difficult to treat symptoms of classical migraine outside of pregnancy, such as calcitonin gene-related peptide (CGRP) receptor antagonists and neuromodulation and neurostimulation devices, are lacking.7
Treatment goals for vestibular migraine include reducing the frequency at which attacks occur, reducing the severity of symptoms and duration of an attack and identification and treatment of co-morbidities. Management of vestibular migraine in pregnancy and the puerperium requires a multi-pronged approach, including trigger avoidance, lifestyle modification and pharmacotherapy, abortive treatment targeted at abating symptoms of vertigo, headache, nausea and vomiting, and safe and effective prophylaxis.
Safety data and a summary of evidence on the efficacy of treatment of vestibular migraine in pregnancy and the puerperium are presented in Tables 1 and 2.
 |
Table 1 Summary of Abortive Therapy for Vestibular Migraine and Safety in Pregnancy and Breastfeeding |
 |
Table 2 Summary of Prophylactic Treatment for Vestibular Migraine and Safety in Pregnancy and Breastfeeding |
Abortive Treatment
Simple Analgesia
Analgesic options such as paracetamol throughout pregnancy and non-steroidal anti-inflammatory drugs (NSAIDs) up to 30–32 weeks of gestation, can be used to treat the headache component of vestibular migraine.26 NSAIDs are the preferred first-line agent for use wherever possible, ideally a soluble version due to possible concomitant gastroparesis. Use of paracetamol greater than two to three times a week predisposes to medication overuse headache (MOH). Opioids should be avoided in migraine due to a high risk of MOH.
Antiemetic Therapy
Adjunctive treatment for nausea during an episode of vertigo in pregnancy includes the use of antihistamines, such as prochlorperazine, promethazine and cyclizine. Metoclopramide is safe and effective for nausea during pregnancy. Promethazine and prochlorperazine may be preferred for use during a vestibular migraine episode because their antidopaminergic action may also target migrainous activity within the trigeminocervical complex, though this theory is controversial.27,28
Selective Serotonin Receptor Agonists (Triptans)
Triptans are selective serotonin (5-HT1B and 5-HT1D) receptor agonists and have well-established efficacy in treating migraine in the early stages of an attack. Their mechanisms of action are multifactorial and include a combination of vasoconstrictive properties, inhibition of the abnormal activation of peripheral nociceptors, inhibition of plasma protein extravasation and reduced release of vasoactive peptides, such as substance P and CGRP.29
Triptans confer benefit when taken within 2 hours of the onset of a migraine episode. Retrospective cohort studies have demonstrated success in aborting both headache and vestibular symptoms in vestibular migraine. Of the triptans, sumatriptan has the most pregnancy safety data to support its use.30 Triptans should be avoided in severe hypertension due to a predisposition to adverse vascular events, though vasoconstriction appears to be limited to extracerebral arterial vasculature.31
Given a well-documented overlay between migraine and anxiety and depressive disorders, it is not uncommon for triptans to be prescribed to patients receiving serotonin reuptake inhibitors (SSRIs) and serotonin and norepinephrine reuptake inhibitors (SNRIs).32 Though controversial and with a lack of supporting data, caution with the use of triptans in conjunction with other serotonergic drugs should be taken, due to the theoretical risk of serotonin syndrome when used in combination.33
First-Line Prophylaxis
Lifestyle Modification
Patients should be counselled on general lifestyle measures that can contribute to migraine control. Sleep hygiene, regular exercise, relaxation techniques and avoidance of triggers are recommended as first-line interventions. Meal regularity and adequate hydration are paramount. In a retrospective chart review, caffeine cessation led to a reduction in self-reported symptoms of vestibular migraine in 14% of the patients.53 In another prospective study on 28 patients, lifestyle measures alone led to a reduction in participants’ perceived dizziness handicap and headache disability. Of note, restful sleep was particularly helpful in reducing symptoms of both dizziness and headache, with 39% of participants reporting a significant reduction in dizziness handicap and 18% of patients reporting improvement in headache disability.54 Vestibular rehabilitation plays an important role in the management of chronic and episodic vestibular disorders, but its role in vestibular migraine is yet to be established.
Aspirin
Aspirin is prescribed as first-line prophylaxis in pregnant patients with classical migraine. Although this practice is not currently included in international guidelines for migraine treatment, its use is endorsed by the United Kingdom Teratology Information Service (UKTIS). There are no specific data for aspirin prophylaxis in vestibular migraine. The use of low-dose aspirin, however, is safe during pregnancy and the puerperium and it is used widely internationally to reduce the risk of preeclampsia.26
Beta-Adrenergic Receptor Blockers
Beta-blockers can effectively prevent classical migraines at low doses, and propranolol, metoprolol and timolol are licensed for this use. The use of propranolol and metoprolol has been explored for use in patients with vestibular migraine; existing evidence suggests that propranolol is effective as prophylaxis. Both drugs are safe during pregnancy and breastfeeding. First-trimester exposure to beta-blockers is not associated with increased congenital malformation, and there is no association of propranolol or metoprolol with intrauterine growth restriction.55
The use of propranolol in vestibular migraine has been studied in prospective and retrospective open-label trials and demonstrated reduction in vertigo severity scores (VSS) at doses starting at 40 mg daily orally, titrated to a maximum dose of 160 mg. The use of propranolol 80 mg administered once daily resulted in vestibular symptom improvement in 73% of the patients.41 In contrast, the prophylactic treatment of vestibular migraine with metoprolol (PROVEMIG) in a randomised controlled trial failed to demonstrate a difference in vestibular episodes between metoprolol and placebo.43
Tricyclic Antidepressants
Amitriptyline is given orally and up-titrated to a maximum dose of 75 mg once a day for classical migraine. Data for its use in prophylaxis in vestibular migraine are lacking. Data from a small retrospective cohort study comprising 12 patients showed overall clinical improvement in headache and vestibular symptoms in 77% of the patients prescribed 25 mg of amitriptyline and in 100% of the patients prescribed 50 mg of amitriptyline.44 Experience in clinical practice, however, differs significantly, as the use of amitriptyline is often limited by side effects.
Amitriptyline is safe in pregnancy. However, there have been recent reports that its use is associated with a slightly increased risk of gestational diabetes mellitus (GDM), though whether this is a causal link is unclear. Amitriptyline is also safe during breastfeeding; while small amounts pass into breast milk, it is not expected to cause any adverse effects in the baby.26
Second-Line Prophylaxis
Calcium Channel Blockers
Cinnarizine is a well-tolerated L-type calcium channel blocker, which has early onset effects on migraine prophylaxis. Its mechanism of action is due to direct inhibition of vestibular hair cell stimulation and antihistamine effect. In a retrospective, single-centre, open-label trial, cinnarizine use over 3 months was found to be safe and effective in reducing both headache and vertigo in vestibular migraine.49 However, safety data in pregnancy are lacking, and therefore it is not currently recommended.
In two large open-label trials in patients with migraine without aura, flunarizine was found more effective than propranolol in treating headache; and treating vertigo compared with betahistine.47,48 However, these trials did not specifically include patients with vestibular migraine. One randomised controlled trial found that flunarizine was more effective than betahistine and vestibular exercises for management of vestibular migraine; demonstrating reduction in vertiginous episodes, reduction in severity of vertigo but with no impact on the frequency or severity of the headache.47 Weight gain and somnolence are the most significant side effects of flunarizine. Safety data in pregnancy are also lacking and thus flunarizine is also not currently recommended.
Acetazolamide
Acetazolamide is not typically used in the treatment of classical migraine. It has, however, been used successfully in the treatment of vertigo and ataxia experienced by patients with Episodic Ataxia 2 (EA2), effectively attenuating or preventing attacks in half to three-quarters of patients.56 Acetazolamide has been used in pregnant patients with Idiopathic Intracranial Hypertension (IIH) with adequate safety data, particularly after the first trimester of pregnancy.56,57 Acetazolamide as prophylactic treatment for vestibular migraine administered in divided doses to a maximum dose of 500mg daily has been studied in a retrospective study of 50 patients.46 Acetazolamide has reportedly been effective in reducing the frequency of vertigo attacks over a 3-month period from 3.9 to 1.4, frequency of headache attacks from 4.3 to 2.9 and Vertigo Activity Scores VAS from 5.6 to 2.3. However, side effects reported were significant, with 6 patients dropping out of the study due to intolerable side effects and 87% of the patients reporting an adverse effect. The most commonly reported side effects were paraesthesia and altered taste.46 The use of acetazolamide could be explored as a second-line agent, with careful review for tolerability, in patients whose vestibular symptoms are refractory to other agents.
Third-Line Prophylaxis
Greater Occipital Nerve Block
Greater occipital nerve (GON) block (local anaesthetic ± corticosteroid injection) is increasingly becoming a method of migraine prophylaxis for patients with chronic or refractory migraine.58 It has been successfully used for classical migraine prophylaxis in pregnancy, and there is no theoretical reason why it would be harmful. Patients can be reassured that systemic absorption of locally infiltrated pharmacotherapy is very low; therefore, the theoretical impact on the fetus is minimal. It has a very rapid onset of action in relieving headache and avoids side effects typically associated with chronic medication use. It may provide an alternative treatment option with increasing availability, although specific evidence upon its effects on vestibular symptoms is lacking.
Botox
Botox (Botulinum toxin type A injection, Onabotulinumtoxin A) may be recommended in cases of vestibular migraine refractory to standard therapy on a benefit versus risk basis.
A retrospective study on the use of botox on 80 patients with vestibular migraine between 2014 and 2019 showed an improvement in scores of the Migraine Disability Assessment Scale (MIDAS), Dizziness Handicap Inventory (DHI) and Visual Analogue Scales (VAS) that was statistically significant, suggesting an improvement in symptoms of both headache and vertigo. Limited data from case reports and retrospective analyses suggest that there is no increase in the risk of congenital anomalies compared to background risk.59
Limiting factors for its use include the lack of safety data during breastfeeding and the variable access to specialist headache services.
Alternative Treatments
Acupuncture has been widely used with reported benefit in migraine, vertigo and mood disorders and is generally considered safe in pregnancy.60 Patients may require up to 10 sessions over 5–8 weeks to see benefit.
Coenzyme Q10 supplementation has been successfully used for migraine prophylaxis outside of pregnancy, and included in trials to prevent preeclampsia.1,61 Benefit in vestibular migraine prophylaxis remains unknown.
Although riboflavin is a constituent of many over-the-counter pregnancy multivitamins, the current guidance advises against its use as high doses up to 400 mg are required for effective migraine prophylaxis and safety data in pregnancy are lacking.62,63
There are no safety data to support the use of feverfew and butterbur extract and thus it is not recommended in the treatment of vestibular migraine in pregnancy.1,64
Drugs That are Currently Not Recommended for Treatment of Vestibular Migraine in Pregnancy and Postpartum
High-Dose Aspirin
Aspirin at analgesic doses (>100 mg) is not recommended for the management of headache or migraine in pregnancy.1 Studies on aspirin at doses ≥300 mg per day in the third trimester have reported an association with neonatal bleeding complications, premature closure of the ductus arteriosus and persistent pulmonary hypertension of the newborn.65
Opioids
Opioids are not recommended for chronic headache syndromes, due to low efficacy and contribution to MOH.1,66
Ergotamine Derivatives
Although not in common current clinical use, ergotamine derivatives (ergots) are contraindicated in pregnancy due to an association with neural tube defects, and their vasoconstrictive properties pose an increased risk of miscarriage due to uterine contraction.67
Angiotensin-Converting Enzyme (ACE) Inhibitors and Angiotensin Receptor Blockers (ARBs)
Although the ACE inhibitor, lisinopril, and the angiotensin-II receptor antagonist, candesartan, have been used for migraine prophylaxis, neither are recommended in pregnancy and both are contraindicated in the second and third trimesters due to teratogenicity.1 Alternative management options should be recommended for women who conceive while taking these medications at the point of a positive pregnancy test.
Anticonvulsants
Anti-epileptic drugs have been successfully used as prophylaxis for classical migraine outside pregnancy. Drugs such as valproate and lamotrigine have the added benefit of use as mood stabilisers.68 The use of lamotrigine, sodium valproate and topiramate have been studied for use in vestibular migraine prophylaxis. However, topiramate and sodium valproate are teratogenic and thus relatively contraindicated for use as vestibular migraine prophylaxis in pregnancy. Effective contraception is required for women of childbearing age when taking sodium valproate, in particular.
While lamotrigine is used in pregnancy for epilepsy treatment, it is not typically recommended for use in the prevention of classical migraine in pregnancy. Recommendations for use in pregnancy advise using it if the benefits outweigh the risks, and the use of alternative agents is preferable. Lamotrigine has not been associated with an increased risk of miscarriage, stillbirth, premature delivery or small for gestational age infants and studies on lamotrigine as a cause for neurodevelopmental delay in the infant are also generally reassuring.6 Its use in pregnancy should be accompanied by 5 mg of folic acid supplementation throughout gestation.
Challenges
Differential Diagnosis and Secondary Headache Disorders
There is significant overlap in the clinical symptoms of vestibular migraine and other paroxysmal vestibular disorders. Migraine can also coexist with these conditions, further adding to the challenge of diagnosing vestibular migraine with confidence. The key differential diagnoses and the similarities and differences in their clinical features have been summarised in Table 3.69
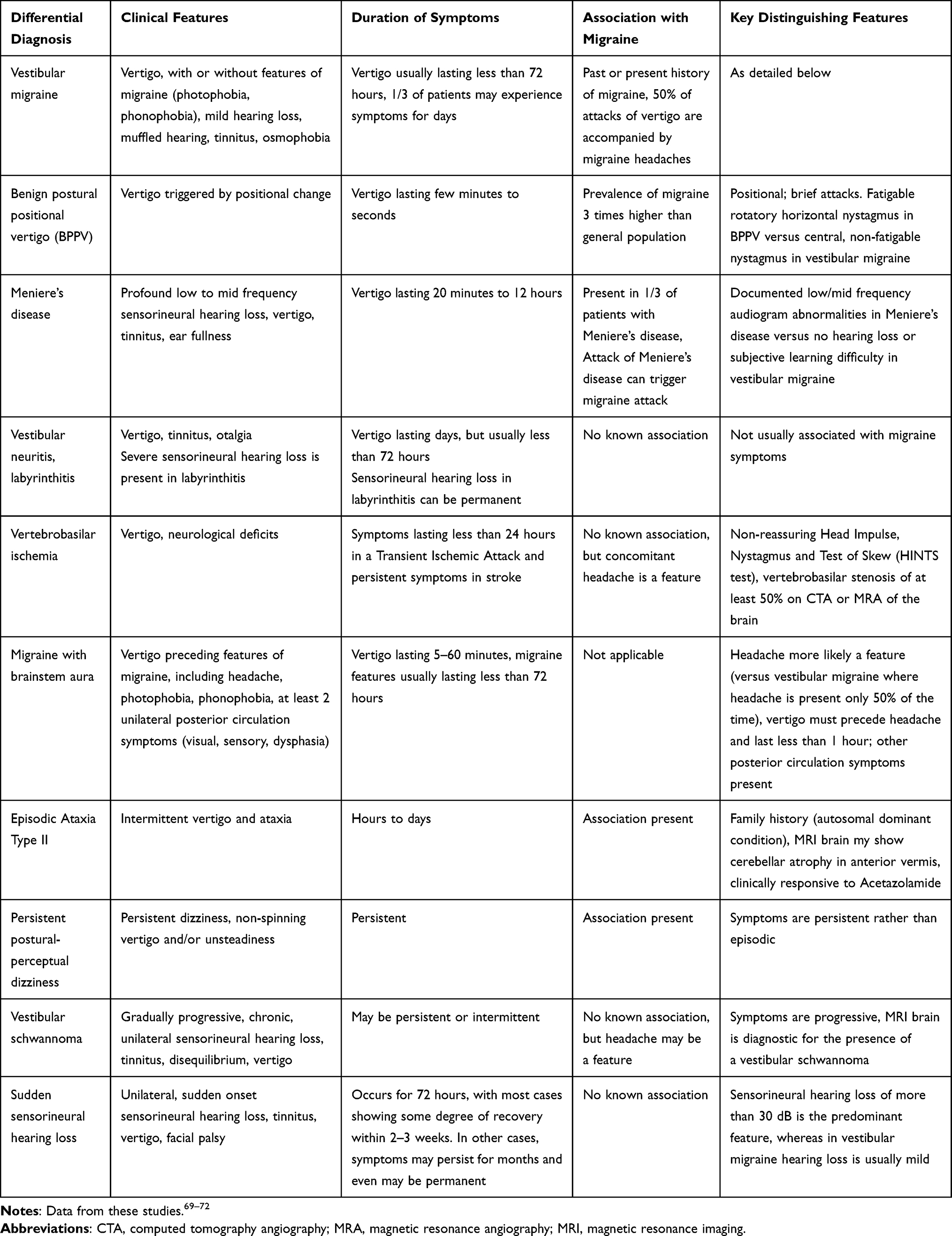 |
Table 3 Differential Diagnosis of Vertigo in Pregnancy and Postpartum |
The dizziness and headache experienced by vestibular migraineurs can mimic physiological symptoms of pregnancy, which may be dismissed by healthcare practitioners and lead to patients hesitating to seek help for their symptoms.
The predisposition to secondary headache disorders in pregnancy poses further diagnostic challenges. Pregnancy is associated with an increased risk of thrombosis and vascular events whilst migraine (with aura) is associated with cerebrovascular events. Physiologic changes to the endocrine, haematological and vascular systems increase the risk of cerebral venous sinus thrombosis, preeclampsia and cerebrovascular events, including transient ischaemic attacks and ischaemic stroke. Though pregnancy itself is not a cause of IIH, weight gain in the context of a pregnancy is a confounding factor.73 Symptoms typical of IIH may mimic vestibular migraine, and vice versa, as they may both present with headache, visual disturbances and tinnitus. Fundoscopic examination for papilloedema may help delineate the two diagnoses. A high index of suspicion must be maintained to carefully exclude secondary headache disorders and neurovascular events.
There is a wide variation in phenotypes of vestibular migraine. Current diagnostic criteria do not accommodate for the possible spectrum of disease, thereby excluding patients who may potentially have a non-classic presentation and who may benefit from treatment.74 One such example of phenotypic variance is in the duration of symptoms16; many patients with vestibular migraine report chronic symptoms lasting for more than 15 days a month.
Chronic Migraine and Medication Overuse Headache
Medication overuse headache (MOH) is common in migraineurs and can be avoided by restriction of analgesic use to a maximum of 2 days per week.66 The goal of abortive treatment is to terminate a migraine at onset; however, frequent use of abortive treatment increases the risk of transforming from episodic to chronic migraine. In this case, the mainstay of treatment is then to break the biofeedback loop by means of trigger avoidance, avoidance of abortive therapy use and establishing effective prophylaxis.74
Chronic vestibular migraine has a dramatic impact on quality of life, despite the common absence of the headache that characterises many other forms of migraine. Delays in diagnosis and not having access to potentially helpful treatment options can further impact on these patients’ physical and emotional well-being. Mothers and Babies: Reducing Risk through Audits and Confidential Enquiries across the UK (MBRRACE-UK) 2021 highlighted that psychiatric disorders are among the top 5 most common causes of maternal mortality in the United Kingdom.75
Investigating Vestibular Migraine and Radiation Use in Pregnancy
Vestibular migraine is a clinical diagnosis. A focused history, combined with a thorough neurological examination, is key to making the diagnosis, with an emphasis on excluding important differential diagnoses, especially secondary headache disorders.
Neuroimaging may be used to exclude the sinister differential diagnoses discussed above, and may also be employed at first presentation to exclude a central cause for vertigo.
Magnetic resonance imaging (MRI) is the preferred imaging modality for headache and vertigo during pregnancy. There is no radiation risk, but gadolinium contrast should be avoided during pregnancy due to an association with fetal developmental abnormalities, fetal inflammatory conditions, and spontaneous miscarriage. For venous imaging, magnetic resonance venography (MRV) without gadolinium should be requested. Under exceptional circumstances, gadolinium may be used where the benefit outweighs the risk.76
Computed tomography (CT) potentially exposes the fetus to ionising radiation, which is associated with congenital malformations, fetal mutagenesis, growth restriction and childhood malignancy, particularly if the fetus is exposed in early gestation.77,78 However, women should be reassured that the estimated fetal radiation dose from a CT scan of the head with fetal shielding is very low; the cumulative fetal exposure being 0.05 rad, which is far less than the accepted maximum cumulative fetal dose of 5 rad during pregnancy.79 In an emergency situation, CT head may be more appropriate than MRI due to rapidity of access and to limit the time to diagnosis. Iodinated contrast is avoided when possible as it can suppress fetal thyroid function.
During the puerperium, there are no specific limitations for neuroimaging and the use of both iodinated contrast and gadolinium are considered safe during lactation. Less than 1% of the maternal dose of contrast media is excreted into breast milk and less than 0.01% is absorbed by the fetus. Women should be counselled as such and breastfeeding does not need to be interrupted following gadolinium exposure.80
Other investigations of relevance include an audiogram to quantify hearing loss to exclude a diagnosis of Meniere’s disease.
Neurophysiological testing such as posturography, caloric testing, vestibular evoked myogenic potentials (VEMPs), cervical and ocular VEMPs, subjective visual vertical (SVV) and assessment of auditory brainstem response (ABR) have been used in different studies. None of these tests yield specific results in patients with vestibular migraine.13
Contraception
Progesterone-only hormonal contraceptive agents are generally preferred including the progesterone-only pill, intrauterine contraceptive device or contraceptive implant. Combined (oestrogen-containing) hormonal contraceptive use may increase the risk of thromboembolic and/or vascular events and should be avoided in patients with migraine with aura. Caution should be used for those without aura and additional risk factors for thrombosis.81
Managing Expectations
Realistic goals of management should be discussed with patients on an individual basis. Reduction in frequency, severity and duration of vestibular migraine episodes, and improvement of quality of life, are reasonable targets. It is often not feasible to achieve complete remission or cure of migraine.
Innovations
Cognitive Behaviour Therapy
Given the significant overlay of neuropsychiatric syndromes with vestibular migraine, and with many patients experiencing chronic symptoms, behavioural interventions, for example relaxation techniques such as mindfulness or meditation or cognitive behavioural therapy, are often found to be useful and effective adjuncts to standard therapy.82,83
Emerging Therapies
Magnesium
The most substantial evidence for magnesium effectiveness has been demonstrated in patients with migraine with aura. Magnesium is an intracellular cation that has been associated with both the function of serotonin and regulation of vascular tone. Magnesium is thought to prevent CSD, which produces the visual and sensory changes in the common forms of aura. Other mechanisms of magnesium action include improved platelet function and decreased release or blocking of neuroinflammatory vasoactive peptides including Substance P and glutamate. Magnesium may also prevent the vasoconstriction caused by the neurotransmitter serotonin. Magnesium in the treatment of preeclampsia, gestational leg cramps, and maternal treatment for fetal neuroprotection provides good evidence of safety.84 Prophylactic treatment of migraine by means of oral magnesium oxide/citrate at a dose of 400–600 mg daily is a safe, cost-efficient strategy and well-tolerated option. The most common adverse effect is diarrhoea; prolonged high doses given intravenously have been reported to cause fetal bone demineralisation and should be avoided.
Calcitonin Gene-Related Peptide Blocking Monoclonal Antibodies
The novel calcitonin gene-related peptide (CGRP) blocking monoclonal antibodies (MAbs) – erenumab, fremanezumab, galcanezumab – have been approved for migraine prevention but were not tested in pregnancy; available safety data are currently limited to case series. Whilst MAbs are known to cross the placenta, they have been safely used in other conditions with no adverse safety signals. CGRP plays a role in vascular regulation, and low levels were found in women with preeclampsia; it is currently unknown whether this is causative or an effect of the disease. CGRP-blocking MAbs are not routinely used in pregnancy, but may be endorsed on a risk/benefit basis after counselling the patient about the existing limited data. CGRP-blocking MAbs have a half-life of 1 month.85
Cyproheptadine
Cyproheptadine is an antihistamine with properties of serotonin antagonism and calcium channel blockade. Its use has not been rigorously studied, but it is widely used in the prevention of childhood migraine, with observational data suggesting that it is an efficacious and safe option.86 Side effects include weight gain and an increased appetite, which may make it an unpopular option during pregnancy. Cyproheptadine has not been demonstrated to be teratogenic, though there is a lack of controlled studies in pregnancy. Its use during breastfeeding is not recommended as there are a lack of safety data. Its use as an adjunctive agent could be potentially explored in select cases of vestibular migraine where other treatment options are deemed unsuitable, if safety data become more robust and adverse effects can be better quantified.
Neuromodulation Devices
The evidence for neuromodulation devices, such as nVNS gammaCore, for the treatment of cluster headaches or migraine in pregnancy is limited to case reports, although no adverse effects have been reported.87 There is no reason to suspect it would be unsafe; however, its use in the context of vestibular migraine has not been established.
Conclusion
Vestibular migraine is a leading cause of episodic vertigo, affecting up to 1% of the general population, and is an important cause of vertigo in pregnancy. Physiologic changes to the endocrine, haematologic and vascular systems in pregnancy may affect pathophysiological processes in migraine and can predispose to the first presentation or an altered clinical course in people with a history of migraine. Vestibular migraine is a clinical diagnosis and atypical presentations may pose a diagnostic challenge.
There has been considerable progress in recognition of vestibular migraine as a distinct diagnosis and an entity that may complicate the pregnancy course. There has been notable development of an evidence base to guide prescribing effective pharmacologic therapy in pregnancy and the postpartum period, and many standard migraine treatments can be safely used.
However, despite established diagnostic criteria, there is currently no robust evidence-based approach for acute treatment or prophylaxis of vestibular migraine, with treatment recommendations generally extrapolated from studies on classical migraine.1 Management of vestibular migraine can prove challenging in pregnancy and the puerperium due to a combination of factors including the predisposition to secondary headache disorders, associated gestational and neuropsychiatric comorbidities, and special considerations surrounding lactation and contraception.
Future research into the treatment of vestibular migraine in pregnancy, including establishing the safety of novel treatment options, is needed. Agents such as Botox and CGRP receptor antagonists have shown encouraging results in studies involving non-pregnant patients with classical and vestibular migraine. Though retrospective studies have been reassuring, there remain unaddressed concerns that need to be explored before they can be recommended for use in pregnancy.
Future work holds potential for phenotyping vestibular migraine and offering personalised management strategies on an individual biopsychosocial basis.88
Disclosure
Dr Ruth Dobson reports grants from MS Society, NMSS, BMA Foundation, Horne Family Charitable Trust and MRC; grants, personal fees, and non-financial support from Biogen; grants, personal fees from Merck; personal fees, non-financial support from Janssen, Novartis and Roche, outside the submitted work. Professor Catherine Nelson-Piercy reports personal fees from Sanofi, UCB and Alexion Pharma, outside the submitted work. Dr Caroline Ovadia reports personal fees from Mirum Pharmaceuticals, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Afridi SK. Current concepts in migraine and their relevance to pregnancy. Obstet Med. 2018;11:154–159. doi:10.1177/1753495X18769170
2. Sawle GV, Ramsay MM. The neurology of pregnancy. J Neurol Neurosurg Psychiatry. 1998;64:711–725. doi:10.1136/jnnp.64.6.717
3. Shen Y, Qi X, Wan T. The treatment of vestibular migraine: a narrative review. Ann Indian Acad Neurol. 2020;23:602–607. doi:10.4103/aian.AIAN_591_19
4. Goadsby PJ, Goldberg J, Silberstein SD. Migraine in pregnancy. BMJ. 2008;336:1502–1504. doi:10.1136/bmj.39559.675891.AD
5. Headache Classification Committee. Vestibular migraine. The International Classification of Headache Disorders.
6. Negro A, Delaruelle Z, Ivanova TA, et al. Headache and pregnancy: a systematic review. J Headache Pain. 2017;18:106. doi:10.1186/s10194-017-0816-0
7. Parikh SK, Delbono MV, Silberstein SD. Managing migraine in pregnancy and breastfeeding. Prog Brain Res. 2020;255:275–309.
8. Bushnell CD, Jamison M, James AH. Migraines during pregnancy linked to stroke and vascular diseases: US population based case-control study. BMJ. 2009;338:b664. doi:10.1136/bmj.b664
9. Altamura C, Corbelli I, de Tommaso M, et al. Pathophysiological bases of comorbidity in migraine. Front Hum Neurosci. 2021;15:640574. doi:10.3389/fnhum.2021.640574
10. Cal R, Bahmad F. Migraine associated with auditory-vestibular dysfunction. Braz J Otorhinolaryngol. 2008;74:606–612. doi:10.1016/S1808-8694(15)30611-X
11. Liveing E. On megrim, sick-headache, and some allied disorders. Ind Med Gaz. 1873;8:305–306.
12. Dieterich M, Brandt T. Episodic vertigo related to migraine (90 cases): vestibular migraine. J Neurol. 1999;246:883–892. doi:10.1007/s004150050478
13. Dieterich M, Obermann M, Celebisoy N. Vestibular migraine: the most frequent entity of episodic vertigo. J Neurol. 2016;263(Suppl 1):S82–9. doi:10.1007/s00415-015-7905-2
14. Third Headache Classification Committee. The International Classification of Headache Disorders.
15. Thakar A, Anjaneyulu C, Deka RC. Vertigo syndromes and mechanisms in migraine. J Laryngol Otol. 2001;115:782–787. doi:10.1258/0022215011909251
16. Lempert T, Olesen J, Furman J, et al. Vestibular migraine: diagnostic criteria. J Vestib Res. 2012;22:167–172. doi:10.3233/VES-2012-0453
17. Abouzari M, Cheung D, Pham T, et al. The relationship between vestibular migraine and motion sickness susceptibility. Otol Neurotol. 2020;41:1116–1121. doi:10.1097/MAO.0000000000002705
18. Mastria G, Mancini V, Viganò A, et al. Alice in Wonderland Syndrome: a clinical and pathophysiological review. Biomed Res Int. 2016;2016:8243145. doi:10.1155/2016/8243145
19. Shi S, Wang D, Ren T, et al. Auditory manifestations of vestibular migraine. Front Neurol. 2022;13:944001. doi:10.3389/fneur.2022.944001
20. Furman JM, Marcus DA, Balaban CD. Vestibular migraine: clinical aspects and pathophysiology. Lancet Neurol. 2013;12:706–715. doi:10.1016/S1474-4422(13)70107-8
21. Kim JS, Yue Q, Jen JC, et al. Familial migraine with vertigo: no mutations found in CACNA1A. Am J Med Genet. 1998;79:148–151. doi:10.1002/(SICI)1096-8628(19980901)79:2<148::AID-AJMG11>3.0.CO;2-J
22. Espinosa-Sanchez JM, Lopez-Escamez JA. New insights into pathophysiology of vestibular migraine. Front Neurol. 2015;6:12. doi:10.3389/fneur.2015.00012
23. Onorato K, Dougherty C, Ailani J. Migraine during pregnancy. Pract Neurol. 2019;19:72–75. doi:10.1136/practneurol-2018-002016
24. Tang B, Yu X, Jiang W, et al. Clinical significance of serum sex hormones in postmenopausal women with vestibular migraine: potential role of estradiol. J Int Med Res. 2021;49:3000605211016379. doi:10.1177/03000605211016379
25. van Casteren DS, van den Brink AM, Terwindt GM. Migraine and other headache disorders in pregnancy. Handb Clin Neurol. 2020;172:187–199.
26. Ovadia C. Prescribing for pregnancy: managing chronic headache and migraine. Drug Ther Bull. 2021;59:152–156. doi:10.1136/dtb.2021.000031
27. Fejzo MS, Trovik J, Grooten IJ, et al. Nausea and vomiting of pregnancy and hyperemesis gravidarum. Nat Rev Dis Primers. 2019;5:62. doi:10.1038/s41572-019-0110-3
28. Gelfand AA, Goadsby PJ. A neurologist’s guide to acute migraine therapy in the emergency room. Neurohospitalist. 2012;2:51–59. doi:10.1177/1941874412439583
29. Nicolas S, Nicolas D. Triptans. Available from. Treasure Island (FL): StatPearls Publishing;2022. https://www.ncbi.nlm.nih.gov/books/NBK554507/.
30. Ephross SA, Sinclair SM. Final results from the 16-year sumatriptan, naratriptan, and treximet pregnancy registry. Headache. 2014;54:1158–1172. doi:10.1111/head.12375
31. Benemei S, Cortese F, Labastida-Ramírez A, et al. Triptans and CGRP blockade – impact on the cranial vasculature. J Headache Pain. 2017;18:103. doi:10.1186/s10194-017-0811-5
32. Evans RW. The FDA alert on serotonin syndrome with combined use of SSRIs or SNRIs and triptans: an analysis of the 29 case reports. Med Gen Med. 2007;9:48.
33. Foong AL, Grindrod KA, Patel T, et al. Demystifying serotonin syndrome (or serotonin toxicity). Can Fam Physician. 2018;64:720–727.
34. Derry S, Moore RA. Paracetamol (Acetaminophen) with or without an antiemetic for acute migraine headaches in adults. Cochrane Database Sys Rev. 2013;4:CD008040.
35. Derry S, Rabbie R, Moore RA. Diclofenac with or without an antiemetic for acute migraine headaches in adults. Cochrane Database Sys Rev. 2013;4:CD008783.
36. Rabbie R, Derry S, Moore RA. Ibuprofen with or without an antiemetic for acute migraine headaches in adults. Cochrane Database Sys Rev. 2013;4:CD008039.
37. Law S, Derry S, Moore RA. Naproxen with or without an antiemetic for acute migraine headaches in adults. Cochrane Database Sys Rev. 2013;10:CD009455.
38. Derry CJ, Derry S, Moore RA. Sumatriptan (all routes of administration) for acute migraine attacks in adults - overview of Cochrane reviews. Cochrane Database Sys Rev. 2014;5:CD009108.
39. Lauritsen CG, Marmura MJ. Current treatment options: vestibular migraine. Curr Treat Options Neurol. 2017;19:38. doi:10.1007/s11940-017-0476-z
40. Goncalves Morganti LO, Cavalcante Salmito M, Duarte JA, et al. Vestibular migraine: clinical and epidemiological aspects. Braz J Otorhinolaryngol. 2016;82:397–402. doi:10.1016/j.bjorl.2015.06.003
41. Van Ombergen A, Van Rompaey V, Van de Heyning P, et al. Vestibular migraine in an otolaryngology clinic: prevalence, associated symptoms, and prophylactic medication effectiveness. Otol Neurotol. 2015;36:133–138. doi:10.1097/MAO.0000000000000596
42. Çelik O, Tanyeri Toker G, Eskiizmir G, et al. The effectiveness of medical prophylactic treatment on vestibular migraine and its effect on the quality of life. J Int Adv Otol. 2020;16:28–33. doi:10.5152/iao.2019.6522
43. Bayer O. Results and lessons learnt from a randomised controlled trial: prophylactic treatment of vestibular migraine with metoprolol (PROVEMIG). Trials. 2019;20:813. doi:10.1186/s13063-019-3903-5
44. Cavalcante Salmito M, Duarte JA, Goncalves Morganti LO, et al. Prophylactic treatment of vestibular migraine. Braz J Otorhinolaryngol. 2017;83:404–410. doi:10.1016/j.bjorl.2016.04.022
45. Bisdorff AR. Treatment of migraine related vertigo with lamotrigine an observational study. Bull Soc Sci Med Grand Duche Luxemb. 2004;2:103–108.
46. Celebisoy N, Gokcay F, Karahan C, et al. Acetazolamide in vestibular migraine prophylaxis: a retrospective study. Eur Arch Otorhinolaryngol. 2016;273:2947–2951. doi:10.1007/s00405-015-3874-4
47. Lepcha A, Amalanathan S, Augustine AM, et al. Flunarizine in the prophylaxis of migrainous vertigo: a randomised controlled trial. Eur Arch Otorhinolaryngol. 2014;271:2931–2936. doi:10.1007/s00405-013-2786-4
48. Liu F, Ma T, Che X, et al. The efficacy of venlafaxine, flunarizine, and valproic acid in the prophylaxis of vestibular migraine. Front Neurol. 2017;8:524. doi:10.3389/fneur.2017.00524
49. Taghdiri F, Togha M, Razeghi Jahromi S, et al. Cinnarizine for the prophylaxis of migraine associated vertigo: a retrospective study. Springerplus. 2014;3:231. doi:10.1186/2193-1801-3-231
50. Gode S, Celebisoy N, Kirazli T, et al. Clinical assessment of topiramate therapy in patients with migrainous vertigo. Headache. 2010;50:77–84. doi:10.1111/j.1526-4610.2009.01496.x
51. Carmona S, Settecase N. Use of topiramate (topamax) in a subgroup of migraine-vertigo patients with auditory symptoms. Ann N Y Acad Sci. 2005;1039:517–520. doi:10.1196/annals.1325.057
52. Salviz M, Yuce T, Acar H, et al. Propranolol and venlafaxine for vestibular migraine prophylaxis: a randomized controlled trial. Laryngoscope. 2016;126:169–174. doi:10.1002/lary.25445
53. Nowaczewska M, Wiciński M, Kaźmierczak W. The ambiguous role of caffeine in migraine headache: from trigger to treatment. Nutrients. 2020;12:2259. doi:10.3390/nu12082259
54. Roberts RA, Watford KE, Picou EM, et al. Effects of lifestyle modification on vestibular migraine. Otol Neurotol. 2021;42:e1537–e1543. doi:10.1097/MAO.0000000000003297
55. Duan L, Ng A, Chen W, et al. Beta-blocker subtypes and risk of low birth weight in newborns. J Clin Hypertens. 2018;20:1603–1609. doi:10.1111/jch.13397
56. Falardeau J, Lobb B, Golden S, et al. The use of Acetazolamide during pregnancy in intracranial hypertension patients. J Neuroophthalmol. 2012;33:9–12. doi:10.1097/WNO.0b013e3182594001
57. Chih A, Patel B. Idiopathic intracranial hypertension in pregnancy. Fed Pract. 2015;32:36–40.
58. Chowdhury D, Mundra A. Role of greater occipital nerve block for preventive treatment of chronic migraine: a critical review. Cephalalgia Reports. 2020;3:1–20. doi:10.1177/2515816320964401
59. Sürmeli R, Habeşoğlu TE. A new treatment option for vestibular migraine: onabotulinum toxin type A. Istanbul Med J. 2020;21:177–181. doi:10.4274/imj.galenos.2020.93753
60. Hu T, Zhang A, Jiang B, et al. Is acupuncture effective and safe for prophylaxis of vestibular migraine? A protocol for systematic review and meta analysis. Medicine. 2020;99:e23533. doi:10.1097/MD.0000000000023533
61. Sazali S, Badrin S, Norhayati MN, et al. Coenzyme Q10 supplementation for prophylaxis in adult patients with migraine-a meta-analysis. BMJ Open. 2021;11:e039358. doi:10.1136/bmjopen-2020-039358
62. Boehnke C, Reuter U, Flach U, et al. High-dose riboflavin treatment is efficacious in migraine prophylaxis: an open study in a tertiary care centre. Eur J Neurol. 2004;11:475–477. doi:10.1111/j.1468-1331.2004.00813.x
63. National Institute for Health and Care Excellence. Scenario: migraine in adults; 2022. Available from: https://cks.nice.org.uk/topics/migraine/management/adults/.
64. Din L, Lui F. Butterbur. Available from. Treasure Island (FL): StatPearls Publishing;2022. https://www.ncbi.nlm.nih.gov/books/NBK537160/.
65. UK Teratology Information Service. Use of aspirin and aspirin overdose in pregnancy. 2019. Available from: https://www.medicinesinpregnancy.org/bumps/monographs/USE-OF-ASPIRIN-AND-ASPIRIN-OVERDOSE-IN-PREGNANCY/.
66. Vandenbussche N, Laterza D, Lisicki M, et al. Medication-overuse headache: a widely recognized entity amidst ongoing debate. J Headache Pain. 2018;19:50. doi:10.1186/s10194-018-0875-x
67. Bánhidy F, Acs N, Puhó E, et al. Ergotamine treatment during pregnancy and a higher rate of low birth weight and preterm birth. Br J Clin Pharmacol. 2007;64:510–516. doi:10.1111/j.1365-2125.2007.02901.x
68. Bialer M. Why are antiepileptic drugs used for nonepileptic conditions? Epilepsia. 2012;53:26–33. doi:10.1111/j.1528-1167.2012.03712.x
69. Beh SC. Vestibular migraine: how to sort it out and what to do about it. J Neuroophthalmol. 2019;39:208–219. doi:10.1097/WNO.0000000000000791
70. Frosolini A, Marioni G, Gallo C, de Filippis C, Lovato A. Audio-vestibular disorders and pregnancy: a systematic review. Am J Otolaryngol. 2021;42:103136. doi:10.1016/j.amjoto.2021.103136
71. Foley RW, Shirazi S, Maweni RM, et al. Signs and symptoms of acoustic neuroma at initial presentation: an exploratory analysis. Cureus. 2017;9:e1846. doi:10.7759/cureus.1846
72. Kuhn M, Heman-Ackah SE, Shaikh JA, Roehm PC. Sudden sensorineural hearing loss: a review of diagnosis, treatment, and prognosis. Trends Amplif. 2011;15:91–105. doi:10.1177/1084713811408349
73. Thaller M, Wakerley BR, Abbott S, et al. Managing idiopathic intracranial hypertension in pregnancy: practical advice. Pract Neurol. 2022;22:295–300. doi:10.1136/practneurol-2021-003152
74. Luzeiro I, Luís L, Gonçalves F, et al. Vestibular migraine: clinical challenges and opportunities for multidisciplinarity. Behav Neurol;2016:6179805. doi:10.1155/2016/6179805
75. Knight M, Bunch K, Tuffnell D, et al., Eds. on Behalf of MBRRACE-UK. Saving Lives, Improving Mothers’ Care - Lessons Learned to Inform Maternity Care from the UK and Ireland Confidential Enquiries into Maternal Deaths and Morbidity 2017-19. Oxford: National Perinatal Epidemiology Unit, University of Oxford; 2021.
76. Mallampalli MP, Rizk HG, Kheradmand A, et al. Care gaps and recommendations in vestibular migraine: an expert panel summit. Front Neurol. 2022;12:812678. doi:10.3389/fneur.2021.812678
77. Kumar R, De Jesus O. Radiation Effects on the Fetus. Treasure Island (FL): StatPearls Publishing; 2022.
78. Singh N, McLean K. Five things to know about intravascular contrast media for imaging in breastfeeding women. CMAJ. 2012;184:E775. doi:10.1503/cmaj.112148
79. Toppenberg KS, Hill DA, Miller DP. Safety of radiographic imaging during pregnancy. Am Fam Physician. 1999;59:1813–1820.
80. Sundgren PC, Leander P. Is administration of gadolinium-based contrast media to pregnant women and small children justified? J Magn Reson Imaging. 2011;34:750–757. doi:10.1002/jmri.22413
81. Calhoun AH, Batur P. Combined hormonal contraceptives and migraine: an update on the evidence. Cleve Clin J Med. 2017;84:631–638. doi:10.3949/ccjm.84a.16033
82. Weatherall MW. The diagnosis and treatment of chronic migraine. Ther Adv Chronic Dis. 2015;6:115–123. doi:10.1177/2040622315579627
83. Bae JY, Sung HK, Kwon NY, et al. Cognitive behavioral therapy for migraine headache: a systematic review and meta-analysis. Medicina. 2021;58:44. doi:10.3390/medicina58010044
84. von Luckner A, Riederer F. Magnesium in migraine prophylaxis - is there an evidence-based rationale? A systematic review. Headache. 2018;58:199–209. doi:10.1111/head.13217
85. Hoskin JL, Fife TD. New anti-CGRP medications in the treatment of vestibular migraine. Front Neurol. 2022;12:799002. doi:10.3389/fneur.2021.799002
86. Peroutka SJ, Allen GS. The calcium antagonist properties of cyproheptadine: implications for antimigraine action. Neurology. 1984;34:304–309. doi:10.1212/WNL.34.3.304
87. Moisset X, Pereira B. Neuromodulation techniques for acute and preventive migraine treatment: a systematic review and meta-analysis of randomised controlled trials. J Headache Pain. 2020;21:142. doi:10.1186/s10194-020-01204-4
88. Rosignoli C, Ornello R, Onofri A, et al. Applying a biopsychosocial model to migraine: rationale and clinical implications. J Headache Pain. 2022;23:100. doi:10.1186/s10194-022-01471-3
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.