Back to Journals » International Medical Case Reports Journal » Volume 18
Treating Multiline Treatment Failure in Advanced Colon Cancer Based on Evolutionary Theory: A Case Report
Authors Wu X, Xian Q ![]() , Ling R, Zhu W
, Ling R, Zhu W
Received 22 August 2025
Accepted for publication 15 November 2025
Published 4 December 2025 Volume 2025:18 Pages 1533—1538
DOI https://doi.org/10.2147/IMCRJ.S560068
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Thomas E Hutson
Xinyu Wu, Qingying Xian, Rui Ling, Wenyu Zhu
Department of Oncology, The Second People’s Hospital of Changzhou, The Third Affiliated Hospital of Nanjing Medical University, Changzhou, Jiangsu, People’s Republic of China
Correspondence: Wenyu Zhu, The Third Affiliated Hospital of Nanjing Medical University, Ge Hu 68 Hao, Wujin Qu, Changzhou, Jiangsu, 213000, People’s Republic of China, Email [email protected]
Purpose: Currently, there is no standard regimen for third-line therapy in advanced colon cancer. Intratumoral heterogeneity and tumor evolution have been substantiated in multiple cancer types, paving the way for exploratory research into new treatment strategies for pulmonary metastases from colorectal cancer.
Patients and Methods: In this report, we present a case of advanced colon cancer with lung metastasis. After multiple lines of therapy (including FOLFOX, FOLFIRI combined with targeted therapy) failed, the patient received a lung cancer–derived regimen to colorectal pulmonary metastases through an evolutionary perspective.
Results: After two cycles, the patient achieved partial response (PR), and after eight cycles, the disease was stable (SD), with a good quality of life.
Conclusion: The application of a lung cancer–derived regimen to colorectal pulmonary metastases through an evolutionary perspective may offer a new therapeutic direction for patients who have exhausted standard options.
Keywords: multiple lung metastasis, colorectal cancer, chemotherapy, evolution
Introduction
Colorectal cancer (CRC) is the third most common malignancy globally and ranks second in China, with the 5-year survival rate for metastatic disease remaining around 10–14%.1–3 While molecularly targeted therapies have improved outcomes in advanced CRC, standardized regimens for third-line treatment and beyond are still lacking.4
Therapeutic resistance arises from tumor evolution governed by clonal selection.5 Cytotoxic chemotherapy and targeted agents create a selective pressure that favors treatment-resistant subclones. These subclones, whether pre-existing or newly evolved, then proliferate and outcompete others, leading to eventual treatment failure.6 This evolutionary trajectory often results in a tumor genetically and phenotypically distinct from the primary lesion, particularly in a distant metastatic site like the lung. Growing evidence suggests that the metastatic microenvironment plays a decisive role in this process of clonal selection and adaptation. For instance, tumor-associated Schwann cells and fibroblasts have been shown to drive cancer progression and treatment resistance by remodeling the local tumor microenvironment (TME).7,8 Thus, this evidence supports the evolutionary concept that interactions between the TME and tumor cells critically shape therapeutic responses.
Here, we report a case of advanced CRC with lung metastases where conventional therapies failed. Guided by this evolutionary perspective, a primary lung cancer regimen was applied, resulting in significant tumor shrinkage and clinical benefit.
Case Description
In April 2013, a 66-year-old male was newly diagnosed with an adenocarcinoma located in the sigmoid colon. The pathologic finding after the radical resection of the sigmoid colon cancer revealed a stage IIB adenocarcinoma pT4N0M0 with a KRAS mutation. Microsatellite instability (MSI) testing revealed microsatellite instability (MSS) type. From May to October 2013, the patient completed 12 cycles of FOLFOX4 adjuvant chemotherapy, with good tolerance and no severe adverse reaction. He was followed up for 8 years after surgery, and regular reexaminations showed no signs of recurrence or metastasis. In May 2021, a computed tomography (CT) scan at our hospital showed multiple metastases in the left lung and bilateral adrenal glands. A biopsy of the left lung was performed, and the pathology showed adenocarcinoma. Next-generation sequencing (NGS) revealed a KRAS mutation, and PD-L1 testing was positive (TPS 1%, CPS 5%). The tumor mutational burden (TMB) was low (3.99muts/Mb). After multidisciplinary team (MDT) evaluation, he was diagnosed with metastatic colorectal cancer (mCRC).
Considering the histologic results, first-line chemotherapy with mFOLFOX6 and bevacizumab (BV) was initiated In June 2021. After 12 cycles of chemotherapy had been administered, radiological assessment revealed stable disease (SD) according to Response Evaluation Criteria in Solid Tumors (RECIST), version 1.1.9 Therefore, the patient continued to receive maintenance treatment with bevacizumab plus capecitabine for 5 cycles. In July 2022, the patient displayed an elevated carcinoembryonic antigen (CEA) level of 110ng/mL in the serum and enlargement of left pulmonal lesions in radiologic imaging, indicating progressive disease (PD). Subsequently, the patient received of second-line treatment with bevacizumab plus FOLFIRI for 9 cycles, during which treatment response was evaluated as SD. On January 2023, a follow-up CT scan demonstrated that the lesion in the anterior segment of the upper lobe of the left lung had increased in size compared to before. According to RECIST 1.1, it was evaluated as PD. The patient then underwent radiofrequency ablation (RFA) of the lung lesion. After the operation, the patient received third-line therapy with regorafenib plus penpulimab, which the best response was assessed as partial response (PR). While, after 6 cycles of regorafenib plus penpulimab, pulmonal progression was observed in August 2023. Subsequently, the patient began fourth-line treatment with fruquintinib plus penpulimab for 2 cycles. Due to hand-foot skin rash with pain 2 weeks after taking fruquintinib, the patient received penpulimab monotherapy for 1 cycle. However, after only 3 cycles of fourth-line treatment regimen disease progressed. All applied treatment sequences are precisely illustrated in Figure 1.
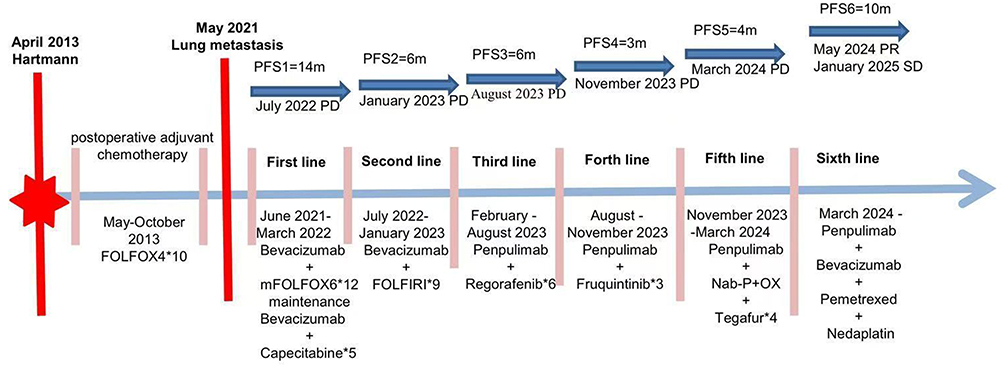 |
Figure 1 Clinical course and therapeutic approaches starting in April 2013 after primary diagnosis. |
Given that the patient’s response to standard first-line to current therapy was mediocre, it was considered that the patient had developed systemic resistance to colorectal cancer treatment. Thus, in November 2023, the therapy regimen was changed to lung metastasis-oriented approach, using a chemotherapy and immunotherapy regimen of albumin-bound paclitaxel (Nab-P), oxaliplatin (OX), tegafur, and penpulimab. After 2 cycles, the response was evaluated as SD with tumor lesions shrinkage. Considering the shrinkage in lung lesions with this treatment, it was deemed effective for lung metastases, although the response was evaluated as PD after 4 cycles (Figure 2A).
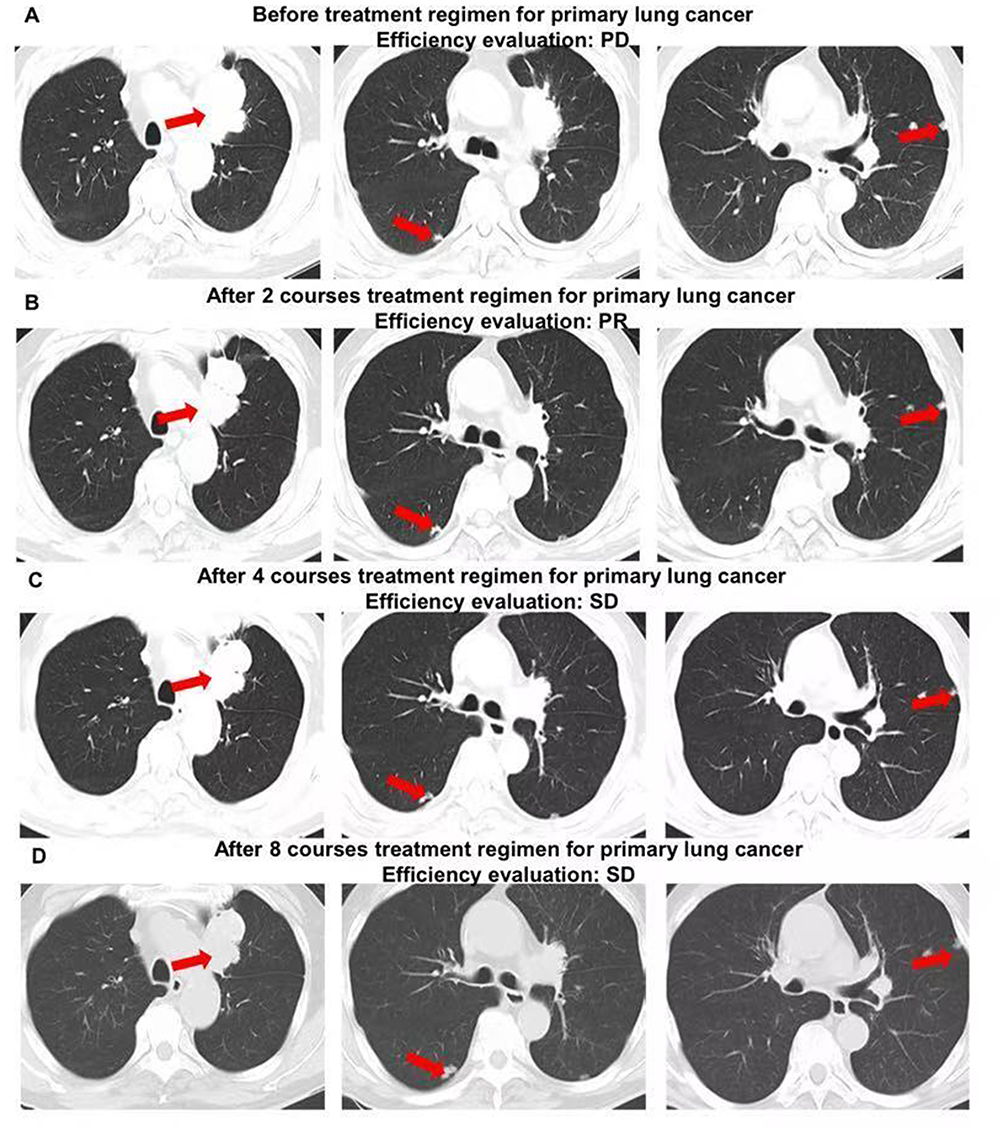 |
Figure 2 Consecutive CT findings from the start of sixth-line chemotherapy to the end of 8 courses. (A) CT image after 4 cycles of the fifth-line regimen show disease progression in the lung lesions (red arrows indicate representative lesions). (B) CT image after 2 cycles of the sixth-line regimen show partial response with significant shrinkage of the lung lesions. (C) CT image after 4 cycles of the sixth-line regimen show stable disease following initial shrinkage. (D) CT image after 8 cycles of the sixth-line regimen show stable disease. |
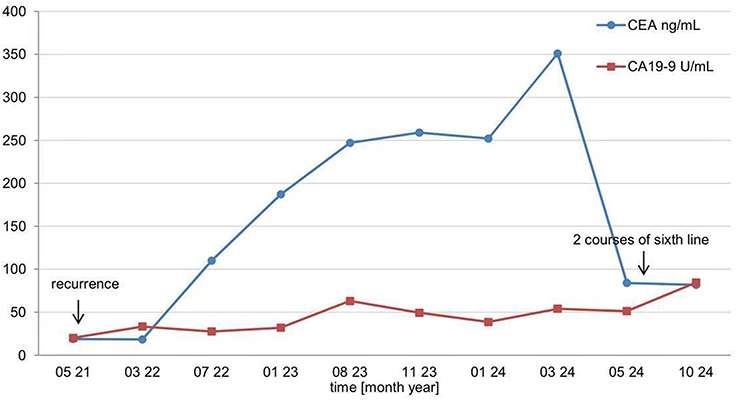 |
Figure 3 Changes in tumor markers (CEA and CA19-9). |
In March 2024, treatment was adjusted to a regimen including bevacizumab, pemetrexed, nedaplatin plus penpulimab. After 2 cycles, the response was assessed as PR (Figure 2B). During the third and fourth cycles of treatment, the patient experienced grade IV myelosuppression, intestinal infection, and severe anemia as adverse effects. After symptomatic treatment with PEG-CSF and blood transfusion, the patient improved. To date, the patient has completed 8 cycles of this regimen with a current best response of PR (Figure 2C and D). The CEA significantly decreased from 351ng/mL to 84ng/mL. Although carbohydrate antigen 19–9 (CA19-9) was above the normal range before the beginning of this treatment, it slightly decreased after two cycles of treatment (Figure 3). The patient maintains a good quality of life with an Eastern Cooperative Oncology Group (ECOG) performance status (PS) score of 1. Continuation of this treatment plan is currently recommended.
Discussion
As a leading cause of cancer mortality, colorectal cancer (CRC) frequently metastasizes, with pulmonary metastases occurring in 10–20% of cases and conferring a poor median survival of 17.7 months.10–12 While standard first- and second-line therapies exist, treatment-refractory metastatic CRC (mCRC) presents a major challenge.13 Although later-line options have expanded to include immunotherapy and targeted agents,14–16 with regimens such as regorafenib (REGONIVO study) showing promise,17 there is a notable lack of proven effective options specifically for patients with lung metastases after standard lines fail.
The patient’s disease free survival period of up to 8 years after surgery suggests that the initial radical treatment effectively eliminated the dominant clone, but failed to eradicate the dormant minimal residual disease (MRD). The study has shown that residual tumor stem cells or slowly proliferating cells surviving chemotherapy can enter a dormant state through the acquisition of mutations and epigenetic modifications, thereby evading the killing of traditional cytotoxic drugs.18 Over time, when the body’s immune surveillance weakens or the microenvironment undergoes pro-inflammatory changes, disseminated dormant tumor cells “re-awake”, resume proliferation, gradually acquire metastasis-promoting traits (such as EMT activation) in the lung tissue microenvironment, and eventually form visible metastatic lesions on imaging.19 This dynamic evolution not only leads to the failure of conventional treatments but also highlights the urgent need for dynamic monitoring methods and intervention strategies targeting tumor dormancy mechanisms. A study constructing a model of dormant tumor metastasis found that the stimulator of interferon genes (STING) pathway was less active in dormant tumor cells, preventing the recruitment of NK cells and T cells, and allowing tumor cells to survive through immune escape.20 Systemic treatment of mice with STING agonists can eliminate dormant metastasis, providing a therapeutically actionable strategy for the preventing disease relapse.
In this case, the observed sensitivity of lung metastases to a regimen used for primary lung cancer aligns with the emerging concept of managing cancer based on evolutionary dynamics and the metastatic site’s biology, rather than solely on the primary origin. This approach is conceptually supported by the “seed and soil” hypothesis. Furthermore, emerging experimental evidence shows that evolutionarily-informed therapeutic strategies can overcome lineage-defined resistance by directly targeting the adaptive immunosuppressive traits tumors develop in specific organ microenvironments.21 The primary and metastatic lesions undergo distinct epigenetic modifications and local microenvironmental regulations, leading to differences in drug responses despite the same genetic mutations.22 A research using bioprinted breast tumor microenvironment (TME) models showed differing sensitivities to chemotherapy in distinct parts, highlighting environmentally mediated drug resistance.23 In Stephen Paget’s “seed and soil” theory, the interaction between the tumor and its TME is mentioned, which can promote tumor growth, affect its progression, and even influence treatment response.24 In glioblastoma grafted mouse tumors, it was found that differential exposure of tumor cells to blood-borne and angiocrine factors results in diverse metabolic microenvironments, making tumor cells around blood vessels have mammalian target of rapamycin signaling pathway (mTOR) dependent anabolic capabilities and stronger proliferative abilities, which is more conducive to tumor invasion and metastasis.25 In fact, a large number of influencing factors directly regulate the traits of immune cells and stromal cells. As tumor cells evolve, the interaction between TME and cancer cells also changes, which is often a key factor leading to treatment resistance.26–28
The evolutionary analysis of this case is limited by the lack of multi-time-point molecular lineage tracing data. It is crucial to emphasize that while the metastatic microenvironment is the most plausible explanation for the differential treatment response observed, this remains a hypothetical inference in this case, as we lack direct molecular proof from the metastatic site. The single-cell sequencing technology developed in recent years can reveal comprehensive clonal evolutionary trees, while spatial transcriptomics can resolve the spatiotemporal influence of the microenvironment on clonal selection.29,30 The clinical application of these technologies in the future will significantly enhance the precision of tumor evolutionary dynamics analysis and provide better decision making guidance for later-line treatment.
Conclusion
In recent years, Intratumoral heterogeneity and tumor evolution have been substantiated in multiple cancer types. Tumor cells at different stages are exposed to dynamic and changing biological selection pressures, driving genetic diversity to evolve over time. Moreover, even if local and distant metastatic tumor cells originate from the same source, they will develop genetic differences due to different local microenvironments. In hence, treatment strategies targeting the biological characteristics of specific metastatic lesions may offer a new therapeutic direction for colorectal cancer patients with pulmonary metastases. Future clinical trials, such as basket trials based on metastatic organ site rather than primary tumor origin, are warranted to validate this concept. Furthermore, integrating dynamic monitoring of metastatic microenvironment and an evolutionary perspective into clinical decision-making could pave the way for more effective, personalized strategies in advanced colorectal cancer therapy.
Ethics Statement
No formal ethical clearance was required for the publication of this case. No institutional approval was required for the publication of this case. Informed consent for publication of this case report and any accompanying images was obtained from the patient.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zheng R, Zhang S, Zeng H, et al. Cancer incidence and mortality in China, 2016. J Natl Cancer Cent. 2022;2(1):1–9. doi:10.1016/j.jncc.2022.02.002
2. American cancer society. Survival rates for colorectal cancer. 2025. Available from: https://www.cancer.org/cancer/colon-rectal-cancer/detection-diagnosis-staging/survival-rates.html.
3. Zeng H, Chen W, Zheng R, et al. Changing cancer survival in China during 2003-15: a pooled analysis of 17 population-based cancer registries. Lancet Glob Health. 2018;6(5):e555–e567. doi:10.1016/s2214-109x(18)30127-x
4. Yoshino T, Cervantes A, Bando H, et al. Pan-Asian adapted ESMO clinical practice guidelines for the diagnosis, treatment and follow-up of patients with metastatic colorectal cancer. ESMO Open. 2023;8(3):101558. doi:10.1016/j.esmoop.2023.101558
5. Laplane L, Maley CC. The evolutionary theory of cancer: challenges and potential solutions. Nat Rev Cancer. 2024;24(10):718–733. doi:10.1038/s41568-024-00734-2
6. Tarabichi M, Martincorena I, Gerstung M, et al. Neutral tumor evolution? Nat Genet. 2018;50(12):1630–1633. doi:10.1038/s41588-018-0258-x
7. Ebrahim NAA, Soliman SMA, Othman MO, et al. Molecular mechanisms and clinical significance of perineural invasion in malignancies: the pivotal role of tumor-associated Schwann cells in cancer progression and metastasis. Med Oncol. 2025;42(5):171. doi:10.1007/s12032-025-02729-x
8. Ebrahim NAA, Soliman SMA. Advanced biomaterials and biomedical devices for studying tumor-associated fibroblasts: current trends, innovations, and future prospects. Biomed Mater Devices. 2026;4(1):287–301. doi:10.1007/s44174-025-00287-4
9. Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumors: revised RECIST guideline (version 1.1). EurJ Cancer. 2009;45(2):228–247. doi:10.1016/j.ejca.2008.10.026
10. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–263. doi:10.3322/caac.21834
11. Marks KM, West NP, Morris E, et al. Clinicopathological, genomic and immunological factors in colorectal cancer prognosis. Br J Surg. 2018;105(2):e99–e109. doi:10.1002/bjs.10756
12. Cavallaro P, Bordeianou L, Stafford C, et al. Impact of single-organ metastasis to the liver or lung and genetic mutation status on prognosis in stage IV colorectal cancer. Clin Colorectal Cancer. 2020;19(1):e8–e17. doi:10.1016/j.clcc.2019.12.001
13. Benson AB, Venook AP, Adam M, et al. Colon cancer, version 3.2024, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2024;22(2 D):e240029. doi:10.6004/jnccn.2024.0029
14. Grothey A, Van Cutsem E, Sobrero A, et al. Regorafenib monotherapy for previously treated metastatic colorectal cancer (CORRECT): an international, multicentre, randomised, placebo-controlled, Phase 3 trial. Lancet. 2013;381(9863):303–312. doi:10.1016/s0140-6736(12)61900-x
15. Mayer RJ, Van Cutsem E, Falcone A, et al. Randomized trial of Tas-102 for refractory metastatic colorectal cancer. N Engl J Med. 2015;372(20):1909–1919. doi:10.1056/nejmoa1414325
16. Dasari A, Lonardi S, Garcia-Carbonero R, et al. Fruquintinib versus placebo in patients with refractory metastatic colorectal cancer (FRESCO-2): an international, multicentre, randomised, double-blind, phase 3 study. Lancet. 2023;402(10395):41–53. doi:10.1016/s0140-6736(23)00772-9
17. Fukuoka S, Hara H, Takahashi N, et al. Regorafenib plus nivolumab in patients with advanced gastric or colorectal cancer: an open-label, dose-escalation, and dose-expansion phase Ib trial (REGONIVO, EPOC1603). J Clin Oncol. 2020;38(18):2053–2061. doi:10.1200/jco.19.03296
18. Tamamouna V, Pavlou E, Neophytou CM, et al. Regulation of metastatic tumor dormancy and emerging opportunities for therapeutic intervention. Int J Mol Sci. 2022;23(22):13931. doi:10.3390/ijms232213931
19. Gomatou G, Syrigos N, Vathiotis IA, et al. Tumor dormancy: implications for invasion and metastasis. Int J Mol Sci. 2021;22(9):4862. doi:10.3390/ijms22094862
20. Hu J, Sánchez-Rivera FJ, Wang Z, et al. STING inhibits the reactivation of dormant metastasis in lung adenocarcinoma. Nature. 2023;616(7958):806–813. doi:10.1038/s41586-023-05880-5
21. Luo Z, Jiang M, Cheng N, et al. Remodeling the hepatic immune microenvironment and demolishing T cell traps to enhance immunotherapy efficacy in liver metastasis. J Control Release. 2024;373:890–904. doi:10.1016/j.jconrel.2024.07.057
22. Gerstberger S, Jiang Q, Ganesh K. Metastasis. Cell. 2023;186(8):1564–1579. doi:10.1016/j.cell.2023.03.003
23. Yuan T, Fu X, Hu R, et al. Bioprinted, spatially defined breast tumor microenvironment models of intratumoral heterogeneity and drug resistance. Trends Biotechnol. 2024;42(11):1523–1550. doi:10.1016/j.tibtech.2024.06.007
24. Nguyen B, Fong C, Luthra A, et al. Genomic characterization of metastatic patterns from prospective clinical sequencing of 25,000 patients. Cell. 2022;185(3):563–575.e11. doi:10.1016/j.cell.2022.01.003
25. Kumar S, Sharife H, Kreisel T, et al. Intra-tumoral metabolic zonation and resultant phenotypic diversification are dictated by blood vessel proximity. Cell Metab. 2019;30(1):201–211.e6. doi:10.1016/j.cmet.2019.04.003
26. Polyak K, Haviv I, Campbell IG. Co-evolution of tumor cells and their microenvironment. Trends Genet. 2009;25(1):30–38. doi:10.1016/j.tig.2008.10.012
27. Hirata E, Sahai E. Tumor microenvironment and differential responses to therapy. Cold Spring Harb Perspect Med. 2017;7(7):a026781. doi:10.1101/cshperspect.a026781
28. Binnewies M, Roberts EW, Kersten K, et al. Understanding the tumor immune microenvironment (TIME) for effective therapy. Nat Med. 2018;24(5):541–550. doi:10.1038/s41591-018-0014-x
29. Morita K, Wang F, Jahn K, et al. Clonal evolution of acute myeloid leukemia revealed by high-throughput single-cell genomics. Nat Commun. 2020;11(1):5996. doi:10.1038/s41467-020-19119-8
30. Denisenko E, de Kock L, Tan A, et al. Spatial transcriptomics reveals discrete tumour microenvironments and autocrine loops within ovarian cancer subclones. Nat Commun. 2024;15(1):2860. doi:10.1038/s41467-024-47271-y
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Symptom Network Analysis in Patients Undergoing Chemotherapy for Colorectal Cancer: A Cross-Sectional Study
Xie R, Gu XX, Wang Y
Cancer Management and Research 2025, 17:3073-3085
Published Date: 7 December 2025