Back to Journals » Research and Reports in Urology » Volume 15
Treating and Managing Urinary Incontinence: Evolving and Potential Multicomponent Medical and Lifestyle Interventions
Authors Mohamed-Ahmed R, Taithongchai A, da Silva AS, Robinson D, Cardozo L
Received 16 March 2023
Accepted for publication 10 June 2023
Published 17 June 2023 Volume 2023:15 Pages 193—203
DOI https://doi.org/10.2147/RRU.S387205
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Panagiotis J Vlachostergios
Rayan Mohamed-Ahmed, Annika Taithongchai, Ana Sofia da Silva, Dudley Robinson, Linda Cardozo
Department of Urogynaecology, King’s College Hospital, London, UK
Correspondence: Rayan Mohamed-Ahmed, Email [email protected]
Abstract: Incontinence is defined by either ICS 2002 or IUGA/ICS 2010 as the involuntary loss of urine and includes urgency urinary incontinence (UUI), stress urinary incontinence (SUI) or mixed urinary incontinence (MUI). It has a high worldwide prevalence with an associated impact on quality of life. Despite existing management options for the management of urinary incontinence, patients continue to be troubled by symptoms or side effects of existing treatment. There is therefore a requirement for ongoing research into treatment options for the management of UUI and SUI, that are more effective and tolerable to patients. Advances in treatment of UUI include a more selective beta 3 agonist, Vibegron, which has less impact on cardiac function than Mirabegron. Hormonal treatment, including Ospemifene and Prasterone, may improve GSM and in turn symptoms of UUI. There are advances in the types of neuromodulators available, including those that are rechargeable at home and are MRI safe. Laser has shown promising initial results. There is developing interest in the microbiome, and how this may impact future treatment modalities. Advances in treatment of SUI include the use of mobile health applications to support delivery of pelvic floor muscle training. Litoxetine, a selective serotonin reuptake inhibitor, has shown promising results at phase III trials. Functional magnetic stimulation is being developed to improve contractility of pelvic floor muscles. We also discuss interventions that improve tissue elasticity and regeneration, such as platelet rich plasma, autologous stem cell transplantation, laser therapy and radiofrequency treatment, which show short term benefits.
Keywords: overactive bladder, stress urinary incontinence, laser treatment
Introduction
Incontinence is defined by either ICS 2002 or IUGA/ICS 2010 as the involuntary loss of urine and includes urgency urinary incontinence (UUI), stress urinary incontinence (SUI) or mixed urinary incontinence (MUI).1
The management of these symptoms can often be frustrating for both the patient and clinician, as there is no “perfect” treatment for any form of incontinence. Therefore, there continues to be a drive to find the most effective, least invasive treatment with minimal adverse effects or contraindications.
The purpose of this review is to summarise the existing and new conservative and medical interventions that are being implemented or investigated in the management of urinary incontinence.
Urgency Urinary Incontinence
Overactive bladder (OAB) is characterised by symptoms of urinary urgency, with or without urgency urinary incontinence (UUI) usually with frequency and/or nocturia, in the absence of proven infection or other pathology.1 This condition has an estimated prevalence of 12–15%, although this is likely to be an underestimation, and is expected to affect 400 million people worldwide.2,3 The condition has a significant adverse impact on quality of life, with approximately one third of patients reporting that it makes them feel depressed.4 Symptoms of OAB can affect work and social life, activities of daily living and relationships with families and partners.2
Conservative Measures
Current conservative advice regarding reducing OAB symptoms includes weight loss, decreasing fluid intake, particularly caffeinated and carbonated drinks, and bladder retraining.5,6 Those who suffer from troublesome nocturia should be advised to stop drinking two to three hours before going to sleep, as well as decreasing their caffeine intake throughout the day.6,7
There has been increasing interest in the effects of specific dietary modifications. Everaert et al performed post hoc analysis on prospective observational data they had obtained from patients with nocturnal polyuria, often present in OAB.8 They analysed the volume, osmolality and levels of creatine, urea and sodium in urine collected over 24 hours. Patients in the nocturnal polyuria group had higher levels of night-time urinary urea/sodium excretion and estimated dietary protein intake. They suggested there could therefore be a role for decreasing evening dietary protein intake to reduce nocturia.
A Mediterranean diet, which is high in olive oil and vegetables but low in red meat, has known anti-inflammatory benefits with reductions in metabolic complications and has been postulated to also have benefits on bladder function. A recent prospective cohort study conducted by Bozkurt et al assessed association between OAB symptom severity, using the OAB V8 questionnaire, and eating a Mediterranean diet.9 They recruited 326 patients without medical or metabolic syndrome comorbidities who completed the surveys. Statistical analysis showed a significant negative correlation between eating a Mediterranean diet and OAB symptoms.
Medication
Anticholinergics
First line pharmacological treatment for OAB involves the use of anticholinergic medications, such as solifenacin, tolterodine, trospium chloride, fesoterodine, darifenacin and oxybutynin.10 Anticholinergic medications work by preventing the activation of muscarinic receptors on the detrusor muscle by acetylcholine.11 However, common side effects include dry mouth, blurred vision and constipation, which can contribute to patient discontinuation of the treatment, in addition to concerns over anticholinergic burden in older patients due to associated risk of cognitive impairment or dementia.12,13 A recent meta-analysis on the persistence with use of anticholinergics reports a rate of only 21.8% at 12 months, secondary to side effects and ineffectiveness.14 There are no new recent advances in the development of anticholinergic medications.
Beta 3 Agonists
An alternative to anticholinergic medication is the beta 3 adrenergic receptor agonist Mirabegron.10 Mirabegron works by smooth muscle relaxation of the detrusor muscle during the filling phase, thereby improving OAB symptoms.15 Its use has been licensed for the management of OAB in the United Kingdom since 2013.16 A recent systematic review and meta-analysis (n=46,666 patients) of 50 mg Mirabegron used once daily for OAB shows it to be efficacious in treatment of OAB when compared to placebo and as effective as using the first line anticholinergics, with placebo level side effects.17 A large retrospective cohort study of 21,996 patients in the UK with OAB showed that the median duration from initiation of treatment to discontinuation was significantly longer in patients using Mirabegron, when compared to those using antimuscarinics.18
In addition to its effect on beta-3 receptors, Mirabegron has also been shown to act on the beta 1 adrenergic receptors in cardiac smooth muscle which can increase contractility in the right atrium.19 This leads to limitation in its use in patients suffering from long QT syndrome or severe uncontrolled hypertension, with a theoretical increased risk in tachycardia, although recent studies have not proven this.17
A newer more highly selective beta 3 adrenergic receptor agonist called Vibegron has recently shown promising results in phase III trials. It has less effect on beta 1 and beta 2 adrenergic receptors making it less likely to affect cardiac smooth muscle.20,21 A phase III, randomised, double-blinded placebo-controlled study with 1232 patients suffering from OAB showed a statistically significant improvement in urinary urgency and UUI with Vibegron 50 mg or 100 mg once daily when compared to treatment with placebo over a 12-week period.20 The EMPOWUR study, an international phase III randomised, double-blinded, placebo and active controlled study, recruited 1518 patients to receive treatment with either Vibegron 75 mg once daily, Tolterodine extended release 4 mg once daily or a placebo.22 Over a 12-week period, Vibegron led to a significant reduction in episodes of UUI with a discontinuation rate similar to placebo (1.7% vs 1.1%) and a more tolerable side effect profile when compared to Tolterodine.22 A sub-population analysis of the >65 group showed the once daily 75 mg Vibegron to be well tolerated, efficacious and have rapid onset compared to placebo.23 A systematic review including nine papers indirectly compared the efficacy of Vibegron 75 mg once daily, Mirabegron 25 mg once daily, Mirabegron 50 mg once daily and Tolterodine extended release 4 mg one daily.24 The results showed a significant improvement in total volume of urine voided as well as total episodes of incontinence at 52 weeks of treatment with Vibegron when compared to Mirabegron 50 mg.24
Phosphodiesterase Type 5 Inhibitors
Phosphodiesterase type 5 inhibitors (PDEF5) are widely used in the treatment of erectile dysfunction. In vivo studies have demonstrated that PDEF5 is involved in mediating bladder smooth muscle relaxation.25 Therefore, effects of Tadalafil were investigated in patients with OAB in a randomised, double-blind, placebo-controlled trial (n=96). The results reported significant reductions in OAB symptoms (measured by Indevus Urgency Severity Score and OAB symptoms scores) compared with baseline and placebo, with no reported adverse events.26 These findings are yet to be replicated however in larger studies.
Hormonal Treatment
Genitourinary symptoms of the menopause (GSM), which include but are not limited to vaginal dryness, irritation, dysuria, incontinence, and recurrent urinary tract infections, can affect 27–84% of postmenopausal women.27 The increased incidence of lower urinary tract symptoms (LUTS) in postmenopausal women is partly secondary to oestrogen deficiency causing atrophy of the urogenital epithelium.28 Vaginal oestrogens are therefore commonly used in the management of GSM. A meta-analysis of 11 studies showed a significant reduction in urinary frequency, urgency and UUI in postmenopausal women treated with them.29
Some women are not suitable for topical oestrogens, such as those with a history of breast cancer being treated with aromatase inhibitors.30 Therefore there has been interest in Ospemifene, a selective oestrogen receptor modulator (SERM), as an alternative for treating GSM in this cohort of patients.31 A retrospective cohort study of 46 postmenopausal women with OAB symptoms, who received Ospemifene 60 mg daily for 12 weeks, showed a significant reduction in frequency, urgency and UUI symptoms with an overall improvement in vaginal health index (VHI).32 A further prospective cohort study of 25 patients with detrusor overactivity (DO) who were treated with Ospemifene 60 mg daily for 12 weeks published similar findings with regards to improvement in OAB symptoms.33 Published studies all have small patient numbers and so before establishing the use of Ospemifene in clinical practice, further randomised controlled studies with larger numbers with longer follow up will need to be conducted.
Dehydroepiandrosterone (DHEA) is a sex steroid mainly produced in the adrenal cortex, which can be metabolised to androstenedione and then to oestrodiol. A pilot study of 32 postmenopausal women suffering from OAB and GSM received 6.5 mg prasterone (a DHEA) intravaginally for three months showed a reduction in symptoms of urgency, UUI and an improvement in quality of life.34 Similar to Ospemifene, there is a need for further research into the use of DHEAs in treatment of OAB in postmenopausal women.
OnabotulinumtoxinA
Botulinum toxin is known to act on neuromuscular junctions where it inhibits presynaptic release of acetylcholine, thereby preventing muscular contraction.35
OnabotulinumtoxinA (BOTOX®) is the only licensed form of botulinum toxin for use in patients in the United Kingdom with OAB who have not responded to medical treatment and are willing to learn clean intermittent self-catheterisation (CISC).10 Initial treatment is usually with 100 units of BOTOX diluted in 10 ml of saline, injected intravesically under cystoscopic guidance using either local or general anaesthetic.36 A single-centre, double-blinded, randomised controlled trial of 34 patients demonstrated significant reduction in urgency and UUI as well as an increase in maximum cystometric capacity for patients receiving 200 units of intravesical BOTOX.37 There is no evidence of superiority in trigone sparing vs trigone involving injections.38 Side effects include recurrent UTIs in 25% of patients and voiding dysfunction, with one in ten patients requiring clean intermittent self-catheterisation.39–41
Although there are newer forms of botulinum toxin available, such as AbobotulinumtoxinA, a recent review has shown there is sparse evidence regarding their use.42 Further research in the form of RCTs would be required to demonstrate efficacy, safety and superiority before being used routinely in clinical practice.
Nerve Stimulation
Percutaneous Tibial Nerve Stimulation
Percutaneous Tibial Nerve Stimulation (PTNS) is a licensed treatment for patients with refractory OAB who decline invasive treatment such as SNS.10 A thin electrode is placed at the ankle and electronic stimulation is given for 30 minutes weekly for twelve weeks, with top ups occurring as needed thereafter.10 Although the exact mechanism of action is unknown, the treatment is thought to work by neuromodulation of the sacral nerve plexus.43
The SUmiT Study enrolled 220 patients with OAB and randomised them to a sham or PTNS group. The results reported 54.5% of patients in the PTNS group vs 20.9% in the sham group had improvement (marked or moderate) of their symptoms. There were no significant adverse events.44 Follow up was extended to three years in 50 patients from the PTNS arm of the SUmiT group; 29 patients completed this. The results demonstrated 77% of patients had maintained a marked or moderate improvement in their OAB symptoms, with a significant reduction in episodes of urgency incontinence, mean daytime voids and mean night-time voids when compared to baseline.45
A randomised controlled multi-centre study of 100 patients has shown a statistically significant subjective improvement in symptoms for patients with OAB when using PTNS compared to tolterodine, although interestingly no difference in urinary frequency, severity of urgency or episodes of UUI.46
BlueWind™ is a PTNS device manufactured by BlueWind Medical which involves implantation of the stimulator; this can be performed under local anaesthetic. Patients then undergo stimulation at home by wearing a wireless device over the stimulator.47 It is MRI safe and relieves the burden on patients needing to attend hospital weekly for 12 weeks for their PTNS sessions. Data from the pilot study of 15 patients (13 female, two male) demonstrated a significant reduction in episodes of urinary urgency and urge incontinence at three months when compared to baseline.48 One patient required explantation of the device due to presumed infection. A three year follow up study of 20 patients using BlueWind™ showed a 73% improvement in quality of life scores.49 The product is still under development and is not yet available outside clinical trials.
Sacral Nerve Stimulation
In patients who do not respond to or decline treatment with intravesical BOTOX injections, use of sacral nerve stimulation (SNS) can be considered.10 This involves implanting an electrode into the S3–S4 sacral foramen enabling for stimulation of the somatic afferent inhibition of bladder sensations thus normalising the micturition reflex. Licensed devices for SNS include InterStim™, which requires replacement after battery expiration (on average after five to seven years) and the Axonics Therapy devices.50,51 This includes the AxonicsF15™ with a battery life of 10–20 years, or the newer AxonicsR15™, which is a smaller device that patients can recharge at home and is compatible with MRI scanners.51
A three-year multicentre prospective cohort study recruited 340 patients with OAB and implanted InterStim™ devices in 272 of them. The results showed a significant reduction in episodes of urinary frequency and urgency incontinence compared to baseline with improvements in quality of life scores based on the International Consultation on Incontinence Questionnaire of OAB quality of life (ICIQ OABqol).52 A single-centre retrospective cohort study with a median follow up time of four years showed resolution of OAB symptoms in 60% of patients who underwent SNS with InterStim™.53
A prospective multicentre study of 129 patients assessing the efficacy of the newer rechargeable AxonicsR15™ device reported a 94% patient satisfaction at two years.54 93% of patients had a greater than or equal to 50% reduction in urgency urinary incontinence episodes with a significant reduction in ICIQ-OABqol scores.54 Device related adverse events occurred in 16% of patients, the majority of which (9%) were reported as an uncomfortable change in stimulation requiring reprogramming.54
Peroneal Nerve Stimulation
Peroneal electric Transcutaneous NeuroModulation (Peroneal eTNM®) is a device manufactured to provide superficial stimulation of the peroneal nerve, which is thought to influence the afferent pathways involved in bladder function.55
A prospective multicentre RCT allocated 51 patients to daily Peroneal eTNM® use and 25 to solifenacin 5 mg daily.56 There was a higher rate of adverse side effects in the solifenacin group when compared to the neuromodulation group (48% vs 12%). The rates of response when comparing urgency and UI episodes were similar in both treatment groups. A 12 month follow up on the neuromodulation cohort showed 48% of patients with persisting therapeutic effect.57 Larger studies are required to prove superiority of peroneal nerve stimulation when compared to other forms of neuromodulation.
Laser
Laser treatment was introduced into gynaecology practice in the 1970s and was initially used for the treatment of cervical lesions.58 More recently, use of lasers has been undertaken for GSM, lower urinary tract dysfunction and vaginal aesthetics.59 The two main types of laser include non-ablative photothermal erbium:YAG (Er:YAG) and microablative fractional CO2 laser. These are thought to remodel connective tissue of the vagina, increase collagen and improve elasticity.60
A prospective study of 150 patients assigned to either treatment of OAB with Er:YAG laser (10 minute sessions using Fotona monthly for three months), Mirabegron 25 mg once daily or Fesoterodine 4 mg once daily, showed a significant reduction in OAB symptoms across all three groups.61 Patients in the Er:YAG group had a statistically significant improvement in vaginal health scores when compared to the medical treatment groups. There were no adverse events in the Er:YAG laser group, but there were adverse side effects associated with pharmacological treatment.
A prospective observational study of 30 women receiving monthly vaginal CO2 therapy for three months demonstrated a significant improvement in urgency episodes and urgency incontinence.62 This was also associated with an improvement in vaginal health index scores.
There may be a role for laser treatment in postmenopausal women with OAB, although more definitive studies are needed to differentiate the effect from placebo effect.
Microbiome
There have been significant recent advances in understanding the human microbiome and the effect that this plays on immunity, disease development/progression and treatment options.63 Recent research on the gut, vaginal and urinary microbiome has shown a dysbiosis and decreased diversity of the microbiome in patients with OAB symptoms.64–67 Further work is ongoing to understand these differences and may stimulate advances in treatment or allow us to predict which patients may respond to pre-existing treatment options.
Stress Urinary Incontinence
The International Continence Society (ICS) defines SUI as “the complaint of any involuntary loss of urine on effort or physical exertion (eg sporting activities) or on sneezing or coughing” and it has an estimated prevalence of 10–39% worldwide.1 Treatment options for SUI include initial conservative measure, including supervised pelvic floor muscle training (PFMT), vaginal support pessaries and then surgical interventions.
Conservative Measures
The mainstay of first line treatment for SUI are lifestyle modifications, including weight loss when applicable, and supervised PFMT.10
With the increase in accessibility to smartphones and electronic devices, mobile health (mHealth) applications have allowed improvement in patient access to disease information and management.68 The use of these have been investigated in the management of women with SUI. A randomised controlled trial of 123 women with SUI allocated 61 patients to a control group and 62 to an intervention group.69 The intervention group were enrolled in a PFMT programme, delivered via a mHealth application. At three months follow up, there was a significant reduction in both International Consultation of Incontinence Questionnaire: Urinary Incontinence – Short Form (ICIQ-UI SF) and ICIQ Lower Urinary Incontinence Symptoms Quality of Life (ICIQ-LUTS qol) scores in the App group when compared to the control group.
A systematic review of six papers assessing the use of mHealth applications in delivering PFMT to patients with SUI showed that they caused a decrease in symptoms and an improvement in quality of life.70
With an increase in waiting times to access healthcare services, mHealth applications are an accessible way for patients to initiate their own treatment for SUI, without adverse effects, however this type of management may only be suitable for the technology literate population.
Selective Noradrenaline Reuptake Inhibitors/Selective Serotonin Reuptake Inhibitors
Duloxetine, a noradrenaline reuptake inhibitor, has been shown to increase contraction of the urethral sphincter during filling and thereby improving symptoms of stress or mixed urinary incontinence.71
A double-blind, multicentre, randomised controlled study assigned 1378 patients with predominant SUI to 40 mg duloxetine twice daily and 1380 patients to placebo.72 At six weeks, there was a significant reduction in incontinence episodes for those in the treatment group with a sustained improvement to symptoms at long term (72 week) follow up.
Litoxetine, a selective serotonin reuptake inhibitor and a mixed serotonin agonist-antagonist, has shown efficacy in increasing bladder capacity and urethral sphincter activity in rodents.73 Two double-blind, multicentre, randomised controlled trials investigated the use of litoxetine in treating men and women with MUI.73 The first group (RCT1) consisted of 198 women, of which 48 were assigned to Litoxetine 40 mg twice daily, 52 in the Litoxetine 20 mg twice daily group, 48 to the Litoxetine 10 mg twice daily group and 50 to placebo twice daily. The second group (RCT2) consisted of 82 men and women, of whom 53 were assigned to the Litoxetine 30 mg twice daily group and 29 to placebo. Significance in reduction of incontinence episodes was only demonstrated in post-hoc analysis of more severe incontinence subgroups, in patients taking Litoxetine 30 mg BD or more. There was one serious adverse event reported (somnolence) and milder adverse events, reported in 83 participants, included headache, nausea, vomiting, diarrhoea and rash. Further phase III data are required prior to the use of Litoxetine in clinical practice.
Functional Magnetic Stimulation
Functional Magnetic Stimulation (FMS) is a treatment during which electrical activity is administered to a patient sitting on a chair, which leads to neuromodulation of the sacral plexus and in turn causes pelvic muscle contraction due to nerve depolarisation.74 Contraindications to use of FMS include, but are not limited to, cardiac arrhythmias, cardiac pacemakers, venous thromboembolism and neurological disorders.75
A prospective study of one hundred patients (60 with SUI and 40 with OAB) received FMS treatment using an FMS Tesla Care® chair.76 The treatment programme involved twice weekly twenty-minute sessions for eight weeks. 47% and 50% of patients in the SUI and OAB groups respectively reported themselves as cured at two month follow up. No serious adverse events were reported.
An RCT of 111 women allocated 40 patients to a PFMT group, 37 to a PFMT with FMS and 34 to a control group.75 Patient reported outcome measures at follow up showed a significant improvement in incontinence severity using the King’s Health Questionnaire (KHQ) and the Revised Urinary Incontinence Scale (RUIS) in the two treatment groups when compared to the controls. Of note, there was no significant difference in improvement to symptoms between the two treatment groups. There was no long term follow up. Further randomised controlled trials will therefore need to be conducted on FMS to exclude placebo effect.
Autologous Stem Cell Transplantation
The role of stem cell transplantation in the management of SUI has been researched since 2004.77 The literature demonstrates that implantation of stem cell tissue on the external urethral sphincter can lead to its strengthening, thereby decreasing leakage with raised intra-abdominal pressures.78 The stem cells used for these purposes can be derived from muscles (muscle-derived stem cells, MDSCs) or adipose tissue (adipose tissue-derived stem cells, ADSCs).
A pilot study of five patients who underwent cystoscopic-guided transurethral injections of ADSCs combined with collagen showed all patients reported subjective improvement at 12 months.79 Three out of five patients had a negative cough test with a full bladder at 12 months. There were no serious adverse events reported. A further small prospective study of ten patients who underwent transurethral and transvaginal implantation of ADSCs, demonstrated a significant reduction in the ICIQ-UI SF score at 6 and 24 weeks.80
A prospective study of 12 patients who underwent intrasphincteric MDSC injections, derived from the deltoid muscle, reported that three out of twelve were dry at 12 month follow up, with the remaining nine patients reporting a significant improvement to their symptoms.81 There were no serious adverse events related to the procedure and two reports of urinary tract infections, treated with antibiotics. Similar rates of improvement were demonstrated in a prospective study of 80 patients, without serious adverse events.82
Further larger randomised controlled trials should be conducted on stem cell transplantation in women with SUI, before its use can be recommended.
Laser
In a randomised controlled trial of 114 patients, 57 were recruited to the Er:YAG laser treatment for SUI and 57 to the sham treatment group.83 At three months, 21.4% of patients in the laser group reported being “dry” compared to 3.6% in the sham treatment group; the chance of cure was higher in patients diagnosed with mild SUI as baseline. The treatment was well tolerated, with a low risk profile including self-limiting vaginal discharge and vaginal dryness in the laser group.
A prospective study of 150 patients allocated 50 patients to treatment of SUI with a tension free vaginal tape (TVT), 50 to transobturator tape (TOT) and 50 to Er:YAG laser treatment.84 There were similar rates in improvement of symptoms at 12 month follow up when compared to baseline across all three treatment groups.
A prospective, double-blinded randomised controlled trial using CO2 laser allocated 63 patients to the treatment group and 69 to sham treatment.85 At three month follow up, there was a significant reduction in one hour pad weight in the treatment group when compared to the sham group. This was also associated with significant improvements in ICIQ UI scores. These results however were not maintained and at six months, one hour pad test weights and ICIQ UI scores were similar across both groups.
Radiofrequency Treatment
Transcutaneous temperature-controlled radiofrequency (TTCRF) treatment has been investigated for use in the treatment of SUI due to its ability to restore elasticity in vulvovaginal tissue.86
A prospective double-blind randomised controlled trial allocated ten patients to treatment with TTCRF and ten to a placebo group.87 The treatment regimen included use of ThermiVa®, a vaginal TTCRF device, for three to five minutes in the labia majora/minor and the vaginal canal. At 12 week follow up, there were no significant adverse events and a significant reduction in ICIQ UI scores as well as an improvement in overall vaginal health.
A prospective, double-blind randomised controlled trial allocated 42 patients to CO2 laser, 57 to TTCRF and 50 to sham treatment.88 In the per protocol group analysis, at 12 month follow up, there was subjective cure in 84.2%, 76.3% and 39.5% of patients in the laser, TTCRF and sham treatment groups respectively (p=0.01). Objective cure, defined as a negative stress and pad test plus absence of leaking in a 7 day voiding diary, was 50.0%, 55.2% and 18.4% amongst the laser, TTCRF and sham groups respectively (p=0.03). Rates of subjective and objective cure between the two treatment groups were similar. No significant adverse events were reported.
Platelet Rich Plasma
Platelet rich plasma (PRP) is obtained by centrifugation of autologous blood which is then re-injected into the patient to support release of growth factors and therefore tissue regeneration.89 Recent use of PRP has been adopted by many specialties, including orthopaedics, plastic surgery, ophthalmology, dermatology and cosmetics and therefore has been investigated in the treatment of SUI.90
A prospective study of 26 women with intrinsic sphincter deficiency (ISD) who underwent four PRP injections for urodynamic stress incontinence (USI), showed that 80% of patients reported improvement of symptoms with 46% reporting being “dry” at three month follow up.91 There were no reported adverse effects.
A further prospective study of 20 patients who underwent two PRP injections also reported significant reduction in urinary leakage using the one hour pad test, with 80% of patients reporting an improvement in their SUI symptoms at six months.92
Conclusion
There are promising new treatments emerging for conservative and medical management of urinary incontinence, as illustrated in Figures 1 and 2.
 |
Figure 1 Existing and evolving management options for UUI. |
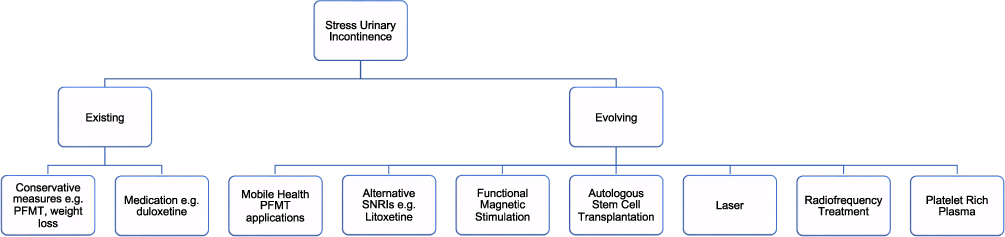 |
Figure 2 Existing and evolving management options of SUI. |
BlueWind™ combines patient convenience with treatment efficacy of nerve stimulation. In addition, Vibegron may be the answer for patients who cannot tolerate anticholinergics but have contraindications for the use of Mirabegron. Further studies assessing long term follow up and outcomes are necessary to provide an evidence base before changing guidelines and practice.
The new emerging treatments for SUI remain in pilot experimental phases with few likely to be in routine clinical practice in the near future. All require significantly larger studies with long term outcome data before universal adoption.
Disclosure
Mr Dudley Robinson reports personal fees from Astellas and Ixaltis, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Abrams P, Cardozo L, Wagg A, Wein A. Incontinence 6th Ed; 2017.
2. Milsom I, Abrams P, Cardozo L, Roberts RG, Thüroff J, Wein AJ. How widespread are the symptoms of an overactive bladder and how are they managed? A population-based prevalence study. BJU Int. 2001;87(9):760–766. doi:10.1046/j.1464-410x.2001.02228.x
3. Irwin DE, Kopp ZS, Agatep B, Milsom I, Abrams P. Worldwide prevalence estimates of lower urinary tract symptoms, overactive bladder, urinary incontinence and bladder outlet obstruction. BJU Int. 2011;108(7):1132–1138.
4. Irwin DE, Milsom I, Kopp Z, Abrams P, Cardozo L. Impact of overactive bladder symptoms on employment, social interactions and emotional well-being in six European countries. BJU Int. 2006;97(1):96–100.
5. Swithinbank L, Hashim H, Abrams P. The effect of fluid intake on urinary symptoms in women. J Urol. 2005;174(1):187–189.
6. Hashim H, Abrams P. How should patients with an overactive bladder manipulate their fluid intake? BJU Int. 2008;102(1):62–66.
7. Cornu JN, Abrams P, Chapple CR, et al. A contemporary assessment of nocturia: definition, epidemiology, pathophysiology, and management--a systematic review and meta-analysis. Eur Urol. 2012;62(5):877–890.
8. Alwis US, Delanghe J, Dossche L, et al. Could evening dietary protein intake play a role in nocturnal polyuria? J Clin Med. 2020;9(8):1.
9. Bozkurt YE, Temeltaş G, Müezzinoğlu T, Üçer O. Mediterranean diet and overactive bladder. Int Neurourol J. 2022;26(2):129–134.
10. Urinary incontinence and pelvic organ prolapse in women: management. NICE NG123; 2019.
11. Andersson K-E. Antimuscarinics for treatment of overactive bladder. Lancet Neurol. 2004;3(1):46–53. doi:10.1016/S1474-4422(03)00622-7
12. Yeowell G, Smith P, Nazir J, Hakimi Z, Siddiqui E, Fatoye F. Real-world persistence and adherence to oral antimuscarinics and mirabegron in patients with overactive bladder (OAB): a systematic literature review. BMJ Open. 2018;8(11):e021889. doi:10.1136/bmjopen-2018-021889
13. Kouladjian O’Donnell L, Gnjidic D, Nahas R, Bell JS, Hilmer SN. Anticholinergic burden: considerations for older adults. J Pharm Pract Res. 2017;47(1):67–77. doi:10.1002/jppr.1303
14. Song YS, Lee HY, Park JJ, Kim JH. Persistence and adherence of anticholinergics and beta-3 agonist for the treatment of overactive bladder: systematic review and meta-analysis, and network meta-analysis. J Urol. 2021;205(6):1595–1604. doi:10.1097/JU.0000000000001440
15. Igawa Y, Yamazaki Y, Takeda H, et al. Functional and molecular biological evidence for a possible β 3 -adrenoceptor in the human detrusor muscle. Br J Pharmacol. 1999;126(3):819–825. doi:10.1038/sj.bjp.0702358
16. NICE. Mirabegron for treating symptoms of overactive bladder. Technology appraisal guidance [TA290]; 2013.
17. Kelleher C, Hakimi Z, Zur R, et al. Efficacy and Tolerability of Mirabegron Compared with Antimuscarinic Monotherapy or Combination Therapies for Overactive Bladder: a Systematic Review and Network Meta-analysis. Eur Urol. 2018;74(3):324–333. doi:10.1016/j.eururo.2018.03.020
18. Chapple CR, Nazir J, Hakimi Z, et al. Persistence and adherence with mirabegron versus antimuscarinic agents in patients with overactive bladder: a retrospective observational study in UK clinical practice. Eur Urol. 2017;72(3):389–399. doi:10.1016/j.eururo.2017.01.037
19. Mo W, Michel MC, Lee XW, Kaumann AJ, Molenaar P. The β 3 -adrenoceptor agonist mirabegron increases human atrial force through β 1 -adrenoceptors: an indirect mechanism? Br J Pharmacol. 2017;174(16):2706–2715. doi:10.1111/bph.13897
20. Yoshida M, Takeda M, Gotoh M, Nagai S, Kurose T. Vibegron, a novel potent and selective β3-adrenoreceptor agonist, for the treatment of patients with overactive bladder: a randomized, double-blind, placebo-controlled phase 3 study. Eur Urol. 2018;73(5):783–790. doi:10.1016/j.eururo.2017.12.022
21. Brucker BM, King J, Mudd PN Jr, McHale K. Selectivity and maximum response of vibegron and mirabegron for β3-adrenergic receptors. Curr Ther Res Clin Exp. 2022;96:100674. doi:10.1016/j.curtheres.2022.100674
22. Staskin D, Frankel J, Varano S, Shortino D, Jankowich R, Mudd PN Jr. International phase III, randomized, double-blind, placebo and active controlled study to evaluate the safety and efficacy of vibegron in patients with symptoms of overactive bladder: EMPOWUR. J Urol. 2020;204(2):316–324. doi:10.1097/JU.0000000000000807
23. Varano S, Staskin D, Frankel J, Shortino D, Jankowich R, Mudd PN Jr. Efficacy and safety of once-daily vibegron for treatment of overactive bladder in patients aged ≥65 and ≥75 years: subpopulation analysis from the EMPOWUR randomized, international, phase III study. Drugs Aging. 2021;38(2):137–146. doi:10.1007/s40266-020-00829-z
24. Kennelly MJ, Rhodes T, Girman CJ, Thomas E, Shortino D, Mudd PN Jr. Efficacy of vibegron and mirabegron for overactive bladder: a systematic literature review and indirect treatment comparison. Adv Ther. 2021;38(11):5452–5464.
25. Uckert S, Oelke M. Phosphodiesterase (PDE) inhibitors in the treatment of lower urinary tract dysfunction. Br J Clin Pharmacol. 2011;72(2):197–204.
26. Chen H, Wang F, Yu Z, et al. Efficacy of daily low-dose tadalafil for treating overactive bladder: results of a randomized, double-blind, placebo-controlled trial. Urology. 2017;100:59–64.
27. Statement NP. The 2020 genitourinary syndrome of menopause position statement of The North American Menopause Society; 2020.
28. Robinson D, Cardozo L. Estrogens and the lower urinary tract. Neurourol Urodyn. 2011;30(5):754–757.
29. Cardozo L, Lose G, McClish D, Versi E. A systematic review of the effects of estrogens for symptoms suggestive of overactive bladder. Acta Obstet Gynecol Scand. 2004;83(10):892–897.
30. Cold S, Cold F, Jensen MB, Cronin-Fenton D, Christiansen P, Ejlertsen B. Systemic or vaginal hormone therapy after early breast cancer: a Danish observational cohort study. J Natl Cancer Inst. 2022;114(10):1347–1354.
31. Goldstein SR, Bachmann GA, Koninckx PR, Lin VH, Portman DJ, Ylikorkala O. Ospemifene 12-month safety and efficacy in postmenopausal women with vulvar and vaginal atrophy. Climacteric. 2014;17(2):173–182.
32. Schiavi MC, Zullo MA, Faiano P, et al. Retrospective analysis in 46 women with vulvovaginal atrophy treated with ospemifene for 12 weeks: improvement in overactive bladder symptoms. Gynecol Endocrinol. 2017;33(12):942–945.
33. Novara L, Sgro LG, Mancarella M, Capece R, Canale E, Biglia N. Potential effectiveness of ospemifene on detrusor overactivity in patients with vaginal atrophy. Maturitas. 2020;138:58–61.
34. Matarazzo MG, Sarpietro G, Fiorito D, et al. Intravaginal 6.5 mg prasterone administration in postmenopausal women with overactive bladder syndrome: a pilot study. Eur J Obstet Gynecol Reprod Biol. 2021;263:67–71.
35. Burgen AS, Dickens F, Zatman LJ. The action of botulinum toxin on the neuro-muscular junction. J Physiol. 1949;109(1–2):10–24.
36. Fontaine C, Papworth E, Pascoe J, Hashim H. Update on the management of overactive bladder. Ther Adv Urol. 2021;13:17562872211039034.
37. Sahai A, Khan MS, Dasgupta P. Efficacy of botulinum toxin-A for treating idiopathic detrusor overactivity: results from a single center, randomized, double-blind, placebo controlled trial. J Urol. 2007;177(6):2231–2236.
38. El-Hefnawy AS, Elbaset MA, Taha DE, et al. Trigonal-sparing versus trigonal-involved Botox injection for treatment of idiopathic overactive bladder: a randomized clinical trial. Low Urin Tract Symptoms. 2021;13(1):22–30.
39. Araklitis G, Cardozo L. Safety issues associated with using medication to treat overactive bladder. Expert Opin Drug Saf. 2017;16(11):1273–1280.
40. Dmochowski R, Chapple C, Nitti VW, et al. Efficacy and safety of onabotulinumtoxinA for idiopathic overactive bladder: a double-blind, placebo controlled, randomized, dose ranging trial. J Urol. 2010;184(6):2416–2422.
41. Herschorn S, Kohan A, Aliotta P, et al. The efficacy and safety of OnabotulinumtoxinA or solifenacin compared with placebo in solifenacin naïve patients with refractory overactive bladder: results from a multicenter, randomized, double-blind phase 3b trial. J Urol. 2017;198(1):167–175.
42. Flint R, Rantell A, Cardozo L. AbobotulinumtoxinA for the treatment of overactive bladder. Expert Opin Biol Ther. 2018;18(10):1005–1013.
43. Bhide AA, Tailor V, Fernando R, Khullar V, Digesu GA. Posterior tibial nerve stimulation for overactive bladder-techniques and efficacy. Int Urogynecol J. 2020;31(5):865–870.
44. Peters KM, Carrico DJ, Perez-Marrero RA, et al. Randomized trial of percutaneous tibial nerve stimulation versus Sham efficacy in the treatment of overactive bladder syndrome: results from the SUmiT trial. J Urol. 2010;183(4):1438–1443.
45. Peters KM, Carrico DJ, Wooldridge LS, Miller CJ, MacDiarmid SA. Percutaneous tibial nerve stimulation for the long-term treatment of overactive bladder: 3-year results of the STEP study. J Urol. 2013;189(6):2194–2201.
46. Peters KM, Macdiarmid SA, Wooldridge LS, et al. Randomized trial of percutaneous tibial nerve stimulation versus extended-release tolterodine: results from the overactive bladder innovative therapy trial. J Urol. 2009;182(3):1055–1061.
47. Medical B. BlueWind RENOVA iStim™ for the treatment of Overactive Bladder (OAB); 2022. Available from: https://bluewindmedical.com/bluewind-renova/.
48. van Breda HMK, Martens FMJ, Tromp J, Heesakkers J. A new implanted posterior tibial nerve stimulator for the treatment of overactive bladder syndrome: 3-month results of a novel therapy at a single center. J Urol. 2017;198(1):205–210.
49. Dorsthorst MJT, Digesu GA, Tailor V, et al. 3-year followup of a new implantable tibial nerve stimulator for the treatment of overactive bladder syndrome. J Urol. 2020;204(3):545–550.
50. Medtronics. InterStimTM II neurostimulator for bladder control and bowel control; 2022. Available from: https://www.medtronic.com/uk-en/healthcare-professionals/products/urology/sacral-neuromodulation-systems/interstim-ii.html.
51. Axonics. Experience choice without compromise; 2022. Available from: https://www.axonics.com/hcp/axonics-system/system-overview.
52. Siegel S, Noblett K, Mangel J, et al. Three-year follow-up results of a prospective, multicenter study in overactive bladder subjects treated with sacral neuromodulation. Urology. 2016;94:57–63.
53. Gandhi S, Gajewski JB, Koziarz A, Almutairi S, Ali A, Cox A. Long-term outcomes of sacral neuromodulation for lower urinary tract dysfunction: a 23-year experience. Neurourol Urodyn. 2021;40(1):461–469.
54. Pezzella A, McCrery R, Lane F, et al. Two-year outcomes of the ARTISAN-SNM study for the treatment of urinary urgency incontinence using the Axonics rechargeable sacral neuromodulation system. Neurourol Urodyn. 2021;40(2):714–721.
55. Krhut J, Peter L, Rejchrt M, Slovak M, Skugarevska B, Zvara P. Peroneal electric transcutaneous NeuroModulation (eTNM(®)): a novel method for the treatment of the overactive bladder. J Healthc Eng. 2021;2021:4016346.
56. Krhut J, Rejchrt M, Slovak M, et al. Prospective, randomized, multicenter trial of peroneal electrical transcutaneous neuromodulation vs solifenacin in treatment-naïve patients with overactive bladder. J Urol. 2023;209(4):734–741.
57. Rejchrt M, Krhut J, Gärtner M, Blok BFM, Zvara P. Effect duration of the initial course of peroneal electrical Transcutaneous NeuroModulation in patients with overactive bladder. World J Urol. 2023;2023:1.
58. Holmquist ND, Bellina JH, Danos ML. Vaginal and cervical cytologic changes following laser treatment. Acta Cytol. 1976;20(4):290–294.
59. Robinson D, Flint R, Veit-Rubin N, Araklitis G, Cardozo L. Is there enough evidence to justify the use of laser and other thermal therapies in female lower urinary tract dysfunction? Report from the ICI-RS 2019. Neurourol Urodyn. 2020;39(Suppl 3):S140–s7.
60. Salvatore S, Leone Roberti Maggiore U, Athanasiou S, et al. Histological study on the effects of microablative fractional CO2 laser on atrophic vaginal tissue: an ex vivo study. Menopause. 2015;22(8):845–849.
61. Okui N. Efficacy and safety of non-ablative vaginal erbium:YAG laser treatment as a novel surgical treatment for overactive bladder syndrome: comparison with anticholinergics and β3-adrenoceptor agonists. World J Urol. 2019;37(11):2459–2466.
62. Perino A, Cucinella G, Gugliotta G, et al. Is vaginal fractional CO2 laser treatment effective in improving overactive bladder symptoms in post-menopausal patients Preliminary results? Eur Rev Med Pharmacol Sci. 2016;20(12):2491–2497.
63. Bosco N, Noti M. The aging gut microbiome and its impact on host immunity. Genes Immun. 2021;22(5–6):289–303.
64. Sze C, Pressler M, Lee JR, Chughtai B. The gut, vaginal, and urine microbiome in overactive bladder: a systematic review. Int Urogynecol J. 2022;33(5):1157–1164.
65. Pearce MM, Hilt EE, Rosenfeld AB, et al. The female urinary microbiome: a comparison of women with and without urgency urinary incontinence. mBio. 2014;5(4):e01283–14.
66. Li K, Chen C, Zeng J, et al. Interplay between bladder microbiota and overactive bladder symptom severity: a cross-sectional study. BMC Urol. 2022;22(1):39.
67. Okamoto T, Hatakeyama S, Imai A, et al. Altered gut microbiome associated with overactive bladder and daily urinary urgency. World J Urol. 2021;39(3):847–853.
68. Hamine S, Gerth-Guyette E, Faulx D, Green BB, Ginsburg AS. Impact of mHealth chronic disease management on treatment adherence and patient outcomes: a systematic review. J Med Internet Res. 2015;17(2):e52.
69. Asklund I, Nyström E, Sjöström M, Umefjord G, Stenlund H, Samuelsson E. Mobile app for treatment of stress urinary incontinence: a randomized controlled trial. Neurourol Urodyn. 2017;36(5):1369–1376.
70. Hou Y, Feng S, Tong B, Lu S, Jin Y. Effect of pelvic floor muscle training using mobile health applications for stress urinary incontinence in women: a systematic review. BMC Womens Health. 2022;22(1):400.
71. Cardozo L, Drutz HP, Baygani SK, Bump RC. Pharmacological treatment of women awaiting surgery for stress urinary incontinence. Obstet Gynecol. 2004;104(3):511–519.
72. Cardozo L, Lange R, Voss S, et al. Short- and long-term efficacy and safety of duloxetine in women with predominant stress urinary incontinence. Curr Med Res Opin. 2010;26(2):253–261.
73. Dmochowski RR, Haab F, Robinson D. A randomized, placebo-controlled clinical development program exploring the use of litoxetine for treating urinary incontinence. Neurourol Urodyn. 2021;40(6):1515–1523.
74. Galloway NT, El-Galley RE, Sand PK, Appell RA, Russell HW, Carlan SJ. Extracorporeal magnetic innervation therapy for stress urinary incontinence. Urology. 1999;53(6):1108–1111.
75. Weber-Rajek M, Strączyńska A, Strojek K, et al. Assessment of the Effectiveness of Pelvic Floor Muscle Training (PFMT) and Extracorporeal Magnetic Innervation (ExMI) in treatment of stress urinary incontinence in women: a randomized controlled trial. Biomed Res Int. 2020;2020:1019872.
76. Braga A, Castronovo F, Caccia G, et al. Efficacy of 3 tesla functional magnetic stimulation for the treatment of female urinary incontinence. J Clin Med. 2022;11(10):1.
77. Chermansky CJ, Tarin T, Kwon DD, et al. Intraurethral muscle-derived cell injections increase leak point pressure in a rat model of intrinsic sphincter deficiency. Urology. 2004;63(4):780–785.
78. Hart ML, Izeta A, Herrera-Imbroda B, Amend B, Brinchmann JE. Cell Therapy for Stress Urinary Incontinence. Tissue Eng Part B Rev. 2015;21(4):365–376.
79. Kuismanen K, Sartoneva R, Haimi S, et al. Autologous adipose stem cells in treatment of female stress urinary incontinence: results of a pilot study. Stem Cells Transl Med. 2014;3(8):936–941.
80. Arjmand B, Safavi M, Heidari R, et al. Concomitant transurethral and transvaginal-periurethral injection of autologous adipose derived stem cells for treatment of female stress urinary incontinence: a phase one clinical trial. Acta Med Iran. 2017;55(6):368–374.
81. Sèbe P, Doucet C, Cornu JN, et al. Intrasphincteric injections of autologous muscular cells in women with refractory stress urinary incontinence: a prospective study. Int Urogynecol J. 2011;22(2):183–189.
82. Peters KM, Dmochowski RR, Carr LK, et al. Autologous muscle derived cells for treatment of stress urinary incontinence in women. J Urol. 2014;192(2):469–476.
83. Blaganje M, Šćepanović D, Žgur L, Verdenik I, Pajk F, Lukanović A. Non-ablative Er:YAG laser therapy effect on stress urinary incontinence related to quality of life and sexual function: a randomized controlled trial. Eur J Obstet Gynecol Reprod Biol. 2018;224:153–158.
84. Okui N. Comparison between erbium-doped yttrium aluminum garnet laser therapy and sling procedures in the treatment of stress and mixed urinary incontinence. World J Urol. 2019;37(5):885–889.
85. Lauterbach R, Aharoni S, Justman N, Farago N, Gruenwald I, Lowenstein L. The efficacy and safety of a single maintenance laser treatment for stress urinary incontinence: a double-blinded randomized controlled trial. Int Urogynecol J. 2022;33(12):3499–3504.
86. Millheiser LS, Pauls RN, Herbst SJ, Chen BH. Radiofrequency treatment of vaginal laxity after vaginal delivery: nonsurgical vaginal tightening. J Sex Med. 2010;7(9):3088–3095.
87. Leibaschoff G, Izasa PG, Cardona JL, Miklos JR, Moore RD. Transcutaneous Temperature Controlled Radiofrequency (TTCRF) for the treatment of menopausal vaginal/genitourinary symptoms. Surg Technol Int. 2016;29:149–159.
88. Seki AS, Bianchi-Ferraro A, Fonseca ESM, Sartori MGF, Girão M, Jarmy-Di Bella ZIK. CO(2) Laser and radiofrequency compared to a sham control group in treatment of stress urinary incontinence (LARF study arm 3). A randomized controlled trial. Int Urogynecol J. 2022;33(12):3535–3542.
89. Paget LDA, Reurink G, de Vos RJ, et al. Effect of platelet-rich plasma injections vs placebo on ankle symptoms and function in patients with ankle osteoarthritis: a randomized clinical trial. JAMA. 2021;326(16):1595–1605.
90. Andia I, Rubio-Azpeitia E, Martin JI, Abate M. Current concepts and translational uses of platelet rich plasma biotechnology; 2015.
91. Chiang CH, Kuo HC. The efficacy and mid-term durability of urethral sphincter injections of platelet-rich plasma in treatment of female stress urinary incontinence. Front Pharmacol. 2022;13:847520.
92. Athanasiou S, Kalantzis C, Zacharakis D, Kathopoulis N, Pontikaki A, Grigoriadis T. The use of platelet-rich plasma as a novel nonsurgical treatment of the female stress urinary incontinence: a prospective pilot study. Female Pelvic Med Reconstr Surg. 2021;27(11):e668–e72.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.