Back to Journals » Open Access Emergency Medicine » Volume 14
Traumatic Injuries Following Mechanical versus Manual Chest Compression
Authors Saleem S, Sonkin R, Sagy I, Strugo R, Jaffe E, Drescher M, Shiber S
Received 23 May 2022
Accepted for publication 13 September 2022
Published 4 October 2022 Volume 2022:14 Pages 557—562
DOI https://doi.org/10.2147/OAEM.S374785
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Safwat Saleem,1 Roman Sonkin,2 Iftach Sagy,3,4 Refael Strugo,2 Eli Jaffe,2 Michael Drescher,1,5 Shachaf Shiber1,5
1Emergency Department, Rabin Medical Center – Beilinson Hospital, Petach-Tikva, Israel; 2Magen David Adom (Israel National Emergency Medical Service), Ramat Gan, Israel; 3Rheumatology Unit, Soroka Hospital, Be’er Sheva, Beer Sheva, Israel; 4Faculty of Medicine, University of the Negev, Be’er Sheva, Israel; 5Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel
Correspondence: Shachaf Shiber, Department of Emergency Medicine, Rabin Medical Center – Beilinson Hospital, 39 Jabotinski St, Petach Tikva, 4941492, Israel, Tel +972-54-4699750, Email [email protected]
Objective: Survival after out-of-hospital cardiac arrest (OHCA) depends on multiple factors, mostly quality of chest compressions. Studies comparing manual compression with a mechanical active compression-depression device (ACD) have yielded controversial results in terms of outcomes and injury. The aim of the present study was to determine whether out-of-hospital ACD cardiopulmonary resuscitation (CPR) use is associated with more skeletal fractures and/or internal injuries than manual compression, with similar duration of cardiopulmonary resuscitation (CPR) between the groups.
Methods: The cohort included all patients diagnosed with out-of-hospital cardiac arrest (OHCA) at a tertiary medical center between January 2018 and June 2019 who achieved return of spontaneous circulation (ROSC). The primary outcome measure was the incidence of skeletal fractures and/or internal injuries in the two groups. Secondary outcome measures were clinical factors contributing to skeletal fracture/internal injuries and to achievement of ROSC during CPR.
Results: Of 107 patients enrolled, 45 (42%) were resuscitated with manual chest compression and 62 (58%) with a piston-based ACD device (LUCAS). The duration of chest compression was 46.0 minutes vs. 48.5 minutes, respectively (p=0.82). There were no differences in rates of ROSC (53.2% vs.50.8%, p=0.84), cardiac etiology of OHCA (48.9% vs.43.5%, p=0.3), major complications (ribs/sternum fracture, pneumothorax, hemothorax, lung parenchymal damage, major bleeding), or any complication (20.5% vs.12.1%, p=0.28). On multivariate logistic regression analysis, factors with the highest predictive value for ROSC were cardiac etiology (OR 1.94;CI 2.00– 12.94) and female sex (OR 1.94;CI 2.00– 12.94). Type of arrhythmia had no significant effect. Use of the LUCAS was not associated with ROSC (OR 0.73;CI 0.34– 2.1).
Conclusion: This is the first study to compare mechanical and manual out-of-hospital chest compression of similar duration to ROSC. The LUCAS did not show added benefit in terms of ROSC rate, and its use did not lead to a higher risk of traumatic injury. ACD devices may be more useful in cases of delayed ambulance response times, or events in remote locations.
Keywords: cardiopulmonary resuscitation, CPR, fractures, active compression-decompression device, ACD
Introduction
Survival after out-of-hospital cardiac arrest (OHCA) depends on multiple factors. One of the most important is the quality and timing of basic life support, consisting mainly of chest compressions and early defibrillation1–4. To ease the difficulty of effective manual compression in the prehospital/patient transport setting,5 researchers developed the active compression-decompression (ACD) device which allows for recoil of the chest and self-compressions during cardiopulmonary resuscitation (CPR) and lessens caregiver fatigue.6 Luo et al7 found that compared to manual chest compression, ACD device-assisted compression was associated with higher rates of return of spontaneous cardiac rhythm (ROSC) and survival after 24 hours, but not more hospital discharges or improvement in neurological status.
ACD devices can be categorized into auto-pulse load-distributing band (LDB) devices and mechanical piston devices (MPD) depending on the mechanism that delivers compressions. LDB devices have been found to improve coronary perfusion during CPR.8 Studies of the Lund University Cardiopulmonary Assist System (LUCAS), a type of MPD with a vacuum head, reported improved perfusion to cerebral neurological systems and coronary arteries, achieving high PCO2 values compared to standard manual compression.9–11 The LUCAS is also amenable for use during coronary catheterization12,13 and during Extracorporeal cardiopulmonary resuscitation (ECPR), a rescue strategy for nonresponders to CPR in cardiac arrest.13
With the expanded distribution of ACD devices, investigations of their relative efficacy and safety in patients with OHCA have increased. Hallstrom and colleagues14 found no significant difference between the LDB device and manual compression in the percentage of patients who achieved ROSC; indeed, both survival rate and neurological outcomes were lower in the LDB group. However, an important limitation of this study was that the device was programmed to a rate of 80 compressions per minute whereas manual compressions are performed, according to the guidelines at a rate of 100–120 per minute.14 Smekal et al15 compared the LUCAS to manual chest compression and reported an increase in the number of rib and bone fractures in the LUCAS group. Additional injuries were examined, but the results were equivocal. By contrast, Kralj and colleagues16 found no difference in the injury rate of resuscitated patients between the LUCAS and manual compression. None of the studies conducted so far stratified outcomes of spontaneous pulse recurrence, hospitalization survival, and 30-day hospitalization survival by duration of CPR.
The aim of the present study was to determine if the use of ACD devices during CPR is associated with more skeletal fractures and/or internal injuries than manual compression, with similar duration of cardiopulmonary resuscitation (CPR) between the groups.
Methods
Setting and Design
A retrospective study was conducted between January 2018 and June 2019. Data were collected from the electronic database of Magen David Adom (MDA), the Israel National Emergency Medical Service, and Rabin Medical Center, a tertiary hospital in central Israel.
MDA operates according to the American emergency medical services model, using mobile intensive care units manned by paramedics and regular ambulances manned by medics. All mobile intensive care units have been equipped with the LUCAS (Physio‐Control Inc., Lund, Sweden), a piston-type ACD device, since January 2014.
Study Population
The cohort consisted of patients diagnosed with OHCA at Rabin Medical Center during the study period who achieved ROSC prior to transport to the hospital. Only patients who underwent chest x-ray and point-of-care ultrasound on emergency department admission were included to ensure that the information on skeletal fractures and/or internal injuries was complete. Patients were divided into two groups by method of CPR: manual or mechanical (LUCAS) chest compression. The groups were pre-matched for CPR time.
Data Collection
Demographic, clinical, treatment, and outcome data of the patients were retrospectively collected by review of the healthcare databases of MDA and Rabin Medical Center.
Study Outcomes
The primary outcome measure was the incidence of skeletal fractures and/or internal injuries in patients resuscitated with the LUCAS device. Secondary outcomes were clinical factors contributing to the occurrence of skeletal fractures and/or internal injuries during CPR (for example, patient age and sex, duration of CPR) and predicting ROSC [for example, patient age and sex, type of CPR used (manual, LUCAS), type of arrhythmia, etiology of cardiac arrest (cardiac, other)]. The skeletal and internal injuries investigated were rib fractures, flail chest, sternum fracture, pneumothorax, major bleeding, hemothorax, and lung parenchymal damage.
Statistical Analysis
Data are expressed as mean and standard deviation (SD), median and interquartile range (IQR) or number and percentage. T-test, chi-square test, and nonparametric tests were used as appropriate to compare clinical characteristics between groups. Due to the small number of complications, regression analysis of between-group differences for this factor was not performed. A multivariate logistic regression model was applied to identify factors predicting ROSC. Data were generated with SPSS, version 25.0. A p value of <0.05 was considered significant.
Results
A total of 107 patients enrolled in the study. Their epidemiological, clinical, and radiological manifestations are listed in Table 1. CPR was performed with manual chest compressions in 45 patients (42%) and with the LUCAS in 62 patients (58%). The corresponding durations of chest compression to ROSC were 46.0 and 48.5 minutes, with no significant difference between the groups (p=0.82).
 |
Table 1 Characteristics of Patients with OHCA |
ROSC was achieved in 25 patients (53.2%) with manual chest compression and in 31 patients (50.8%) using the LUCAS; the difference was not statistically significant (p=0.82). OHCA was due to a cardiac etiology in the majority of patients in both groups (n=22, 48.9% and n=27, 43.5%, respectively; p=0.3). There were no significant between-group differences in the rates of major complications (ribs/sternum fracture, pneumothorax, hemothorax, lung parenchymal damage, major bleeding) or of any complication (Table 1) (20.5% vs 12.1%, respectively, p=0.28).
There were no fatal complications due to CPR in both groups.
On multivariate logistic regression analysis, factors with the strongest predictive values for ROSC were cardiac etiology (OR 1.94; CI 2.00–12.94) and female sex (OR 1.94; CI 2.00–12.94), followed by young age (OR 1.01, 95% CI 0.99–1.04). Use of the LUCAS was not associated with achievement of ROSC (OR 0.73; CI 0.34–2.1) (Table 2).
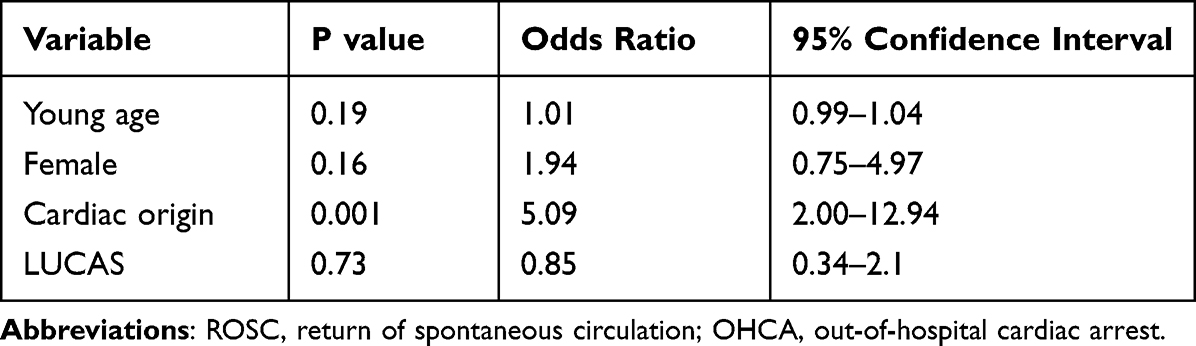 |
Table 2 Logistic Regression Predicting ROSC in Patients with OHCA |
Discussion
This is the first study, to our knowledge, to examine traumatic manifestations of prehospital chest compression with the LUCAS compared to manual compression, both applied for a similar duration. The results show that the LUCAS was not associated with a higher rate of traumatic complications. At the same time, it did not have any advantage in terms of achieving ROSC over manual compression, in agreement with earlier studies.17,18
The PARAMEDIC study from the UK by Gates et al17 was based on data from clusters of ambulance service vehicles that were randomly assigned to administer CPR with the LUCAS-2 or manual chest compression. Intention-to-treat analysis showed that 30-day survival was 6.3% (104/1652) in the LUCAS-2 group and 6.8% (193/2819) in the manual compression group (OR 0.86, 95% CI 0.64–1.15). No serious adverse events were noted. Similarly, in a prospective registry study of 278 patients, Karasek et al18 found no significant difference in the rate of ROSC between the those who underwent CPR with the LUCAS (44/144, 30.6%) and those who did not (69/278, 24.8%) (p=0.35). Use of the LUCAS was associated with a significantly higher rate of conversion from non-shockable to shockable rhythm (20.7% vs 10.10%; p=0.04) and a significantly lower rate of 30-day survival (5.07% vs 16.31%, p=0.044).
Milling et al19 retrospectively compared the outcomes of 84 patients who underwent both manual and mechanical chest compression with 353 patients treated with manual chest compression only. On unadjusted analysis, mechanical chest compression as an adjunct was associated with a higher risk of injuries than manual chest compression (p <0.001, OR 3.10). However, the difference lost significance when the analysis was adjusted (with statistical technique) for duration of CPR.
In a 2021 meta-analysis examining the effectiveness of mechanical chest compression devices,20 15 studies (n=18,474) were analyzed: 6 randomized controlled trials, 2 cluster randomized controlled trials, 5 retrospective case-control studies, and 2 phased prospective cohort studies. The pooled estimate summary effect did not indicate a significant difference in achieving ROSC between mechanical and manual compression (Mantel-Haenszel OR 1.16, 95% CI 0.97–1.39; p=0.11, I2=0.83).
We also found that achieving ROSC was related to female sex, cardiac etiology of OHCA. These observations are supported by previous literature.21–23 Navab et al21 sought to identify major factors contributing to ROSC in the prehospital setting. A total of 3214 patients were included. The overall rate of success of ROSC was 8.3%, and of hospital death, 4.1%. Factors negatively associated with ROSC outcomes were older age, longer ambulance response time, longer CPR duration, and history of cardiac disease. Factors positively associated with ROSC were being witnessed, bystander CPR, and initial shockable rhythm. In another study of 1150 patients in whom CPR was attempted,22 ROSC was achieved in 250 (27.8%). The rate of ROSC was significantly higher when CPR was initiated by bystanders (p <0.001). The likelihood of achieving ROSC was higher in patients with VF/VT cardiac rhythm than with asystole (OR 2.68, 95% CI 1.86–3.85; p < 0.001), and higher (by 1.78-fold) when the event occurred in a public place (p <0.001).
A recent study of 8115 patients (32.4% female) used logistic regression to examine the effect of sex and the interaction of sex and age on ROSC and survival to hospital discharge.23 Female patients had a lower proportion of bystander-witnessed cardiac arrests and initial shockable rhythms. In concordance with our study, the likelihood of ROSC was higher in female than male patients (OR 1.29, 95% CI 1.15–1.42, p <0.001). The ROSC advantage was significant in female patients with non-shockable rhythms (OR 1.48, 95% CI 1.24–1.78, p < 0.001) and female patients of premenopausal age. However, there was no significant difference in survival to hospital discharge between females and males overall or by sex-age groups. Both younger females and younger males had a higher survival rate to hospital discharge than older females and males.
Strengths and Limitations
This study was limited by its retrospective design and the reliance on data from the patients’ medical records. It is possible that there were some errors, though it is unlikely that they would have occurred more often in a particular group.
Our main advantage of our study is that there is no statistically significant difference in length of CPR between the groups. Past studies had difficulty understanding if there are more traumatic injuries from mechanical CPR. Naturally, using LUCAS device happens in a longer CPR. In our study, we matched the time of CPR between the groups and we could assess exactly that LUCAS device is not contributing to more traumatic complication than manual compressions.
Another important advantage of our study was the availability of a digital patient record system that includes data from emergency medicine services as well as the main hospitals serving the community. We also applied strict inclusion criteria, and excluded patients without imaging studies documenting the presence (or absence) of post-CPR traumatic injuries.
Conclusion
This study showed that the use of a mechanical compression-decompression device (LUCAS) in patients with prehospital cardiac arrest was not associated with improved rates of ROSC compared to manual compression. It also does not pose an elevated risk of traumatic injuries. Mechanical CRP devices may be useful when ambulance response times are delayed or too few or untrained response teams are available, or in remote events occurring a long distance from a hospital.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Statement
The Rabin Hospital Ethics Committee approved this study, and that all data accessed complied with relevant data protection and privacy regulations – IRB – RMC – 20-477.
We confirm that the guidelines outlined in the Declaration of Helsinki were followed.
Funding
No funding was received for this study.
Disclosure
The authors report no conflict of interest.
References
1. Steen S, Liao Q, Pierre L, Paskevicius A, Sjöberg T. The critical importance of minimal delay between chest compressions and subsequent defibrillation: a haemodynamic explanation. Resuscitation. 2003;58(3):
2. Sato Y, Weil MH, Sun S, et al. Adverse effects of interrupting precordial compression during cardiopulmonary CPR. Crit Care Med. 1997;25(5):
3. Paradis NA, Martin GB, Rivers EP, et al. Coronary perfusion pressure and the return of spontaneous circulation in human cardiopulmonary CPR. JAMA. 1990;263(8):1106. doi:10.1001/jama.1990.03440080084029
4. Eftestøl T, Sunde K, Andreas Steen P. Effects of interrupting precordial compressions on the calculated probability of defibrillation success during out-of-hospital cardiac arrest. Circulation. 2002;105(19):
5. Olasveengen TM, Wik L, Steen PA. Quality of cardiopulmonary CPR before and during transport in out-of-hospital cardiac arrest. Resuscitation. 2008;76(2):
6. Yuksen C, Prachanukool T, Aramvanitch K, Thongwichit N, Sawanyawisuth K, Sittichanbuncha Y. Is a mechanical-assist device better than manual chest compression? A randomized controlled trial. Open Access Emerg Med. 2017;9:
7. Luo X, Zhang H, Chen G, Ding W, Huang L. Active compression-decompression cardiopulmonary CPR (CPR) versus standard CPR for cardiac arrest patients: a meta-analysis. World J Emerg Med. 2013;4(4):
8. Wik L, Kiil S. Use of an automatic mechanical chest compression device (LUCAS) as a bridge to establishing cardiopulmonary bypass for a patient with hypothermic cardiac arrest. Resuscitation. 2005;66(3):
9. Steen S, Liao Q, Pierre L, Paskevicius A, Sjöberg T. Evaluation of LUCAS, a new device for automatic mechanical compression and active decompression CPR. Resuscitation. 2002;55(3):
10. Rubertsson S, Karlsten R. Increased cortical cerebral blood flow with LUCAS; a new device for mechanical chest compressions compared to standard external compressions during experimental cardiopulmonary CPR. Resuscitation. 2005;65(3):
11. Axelsson C, Karlsson T, Axelsson AB, Herlitz J. Mechanical active compression-decompression cardiopulmonary CPR (ACD-CPR) versus manual CPR according to pressure of end tidal carbon dioxide (PETCO2) during CPR in out-of-hospital cardiac arrest (OHCA). Resuscitation. 2009;80(10):
12. Wagner H, Terkelsen CJ, Friberg H, et al. Cardiac arrest in the catheterisation laboratory: a 5-year experience of using mechanical chest compressions to facilitate PCI during prolonged CPR efforts. Resuscitation. 2010;81(4):
13. Marinacci LX, Mihatov N, D’Alessandro DA, et al. Extracorporeal cardiopulmonary resuscitation (ECPR) survival: a quaternary center analysis. J Card Surg. 2021;36:2300–2307. doi:10.1111/jocs.15550
14. Hallstrom A, Rea TD, Sayre MR, et al. Manual chest compression vs use of an automated chest compression device during resuscitation following out-of-hospital cardiac arrest: a randomized trial. JAMA. 2006;295(22):
15. Smekal D, Lindgren E, Sandler H, Johansson J, Rubertsson S. CPR-related injuries after manual or mechanical chest compressions with the LUCAS™ device: a multicentre study of victims after unsuccessful resuscitation. Resuscitation. 2014;85(12):
16. Kralj E, Podbregar M, Kejžar N, Balažic J. Frequency and number of resuscitation related rib and sternum fractures are higher than generally considered. Resuscitation. 2015;93:
17. Gates S, Lall R, Quinn T, et al. Prehospital randomised assessment of a mechanical compression device in out-of-hospital cardiac arrest (PARAMEDIC): a pragmatic, cluster randomised trial and economic evaluation. Health Technol Assess. 2017;21(11):
18. Karasek J, Ostadal P, Klein F, et al. LUCAS II device for cardiopulmonary resuscitation in a nonselective out-of-hospital cardiac arrest population leads to worse 30-day survival rate than manual chest compressions. J Emerg Med. 2020;59(5):
19. Milling L, Astrup BS, Mikkelsen S. Prehospital cardiopulmonary resuscitation with manual or mechanical chest compression: a study of compression-induced injuries. Acta Anaesthesiol Scand. 2019;63(6):
20. Sheraton M, Columbus J, Surani S, Chopra R, Kashyap R. Effectiveness of mechanical chest compression devices over manual cardiopulmonary CPR: a systematic review with meta-analysis and trial sequential analysis. West J Emerg Med. 2021;22(4):810–819. doi:10.5811/westjem.2021.3.50932
21. Navab E, Esmaeili M, Poorkhorshidi N, Salimi R, Khazaei A, Moghimbeigi A. Predictors of out of hospital cardiac arrest outcomes in pre-hospital settings; a retrospective cross-sectional study. Arch Acad Emerg Med. 2019;7(1):36.
22. Czapla M, Zielińska M, Kubica-Cielińska A, Diakowska D, Quinn T, Karniej P. Factors associated with return of spontaneous circulation after out-of-hospital cardiac arrest in Poland: a one-year retrospective study. BMC Cardiovasc Disord. 2020;20(1):288. doi:10.1186/s12872-020-01571-5
23. Awad E, Humphries K, Grunau B, Besserer F, Christenson J. The effect of sex and age on return of spontaneous circulation and survival to hospital discharge in patients with out of hospital cardiac arrest: a retrospective analysis of a Canadian population. Resusc Plus. 2021;5:100084. doi:10.1016/j.resplu.2021.100084
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.