Back to Journals » Therapeutics and Clinical Risk Management » Volume 22
Transnasal Humidified Rapid-Insufflation Ventilatory Exchange versus Oropharyngeal Airway-Assisted Face-Mask Ventilation for Gastric Insufflation During Induction of General Anesthesia in Patients at High Risk for Obstructive Sleep Apnea
Authors Jia Z, Xu Y, Zhang C ![]() , Jiang H, Han Y, Yuan X, Wang H, Xie K
, Jiang H, Han Y, Yuan X, Wang H, Xie K
Received 12 March 2026
Accepted for publication 10 June 2026
Published 26 June 2026 Volume 2026:22 608591
DOI https://doi.org/10.2147/TCRM.S608591
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor De Yun Wang
Zhe Jia,1,2,* Yangfei Xu,3,* Can Zhang,4 Huifang Jiang,1,2 Yingying Han,4 Xiaohong Yuan,1,2 Hongwei Wang,5 Kangjie Xie1,2,6
1Department of Anesthesiology, Zhejiang Cancer Hospital, Hangzhou, Zhejiang, People’s Republic of China; 2Hangzhou Institute of Medicine (HIM), Chinese Academy of Sciences, Hangzhou, Zhejiang, People’s Republic of China; 3The Second School of Clinical Medicine, Zhejiang Chinese Medical University, Hangzhou, Zhejiang, People’s Republic of China; 4Graduate School, Wenzhou Medical University, Wenzhou, Zhejiang, People’s Republic of China; 5Department of Anesthesiology, Tongde Hospital of Zhejiang Province, Hangzhou, Zhejiang, People’s Republic of China; 6Department of Anesthesiology, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Kangjie Xie, Department of Anesthesiology, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, People’s Republic of China, Email [email protected] Hongwei Wang, Department of Anesthesiology, Tongde Hospital of Zhejiang Province, Hangzhou, Zhejiang, People’s Republic of China, Email [email protected]
Purpose: Obstructive sleep apnea (OSA) is an independent risk factor for gastric insufflation during the induction of general anesthesia. We aimed to compare the impact of oropharyngeal airway-assisted face-mask ventilation and transnasal humidified rapid-insufflation ventilatory exchange (THRIVE) on gastric insufflation in patients with high-risk OSA.
Patients and Methods: Patients at high risk for OSA scheduled for elective major abdominal surgery under general anesthesia were randomized 1:1 to either Group T (THRIVE throughout induction) or Group M (face-mask preoxygenation followed by oropharyngeal airway-assisted pressure-controlled ventilation). Gastric antrum ultrasonography was performed at baseline (T1), after preoxygenation (T2), and post-intubation (T4) to assess changes of antral cross-sectional area (CSAa). Arterial blood gases were analyzed at T1, T2, after induction during ventilation/apnea (T3), and T4. Adverse events and patient comfort were recorded. The primary outcome was the incidence of gastric insufflation at T4. Secondary outcomes included CSAa percentage change, oxygenation and arterial blood gas variables, adverse events, and patient comfort.
Results: Of 100 randomized patients, 94 completed the study (47 per group). Group T demonstrated a significantly lower incidence of gastric insufflation post-intubation compared to Group M (23.4% vs 44.7%; P = 0.030) and a smaller median percentage increase in antral cross-sectional area (7.62% vs 13.24%; P = 0.070). THRIVE provided superior preoxygenation (higher PaO2 at T2, P < 0.001). During apnea (T3–T4), Group T maintained adequate oxygenation (SpO2 > 92%) without mechanical ventilation but developed mild hypercapnia, which was expected to improve following continued mechanical ventilation after intubation. Adverse event rates were non-significant (P = 1.000). Patient comfort scores were significantly higher in Group T (P < 0.001).
Conclusion: In patients at high risk for OSA, THRIVE reduces the incidence of gastric insufflation during induction compared with oropharyngeal airway-assisted face-mask ventilation. THRIVE improves preoxygenation and patient comfort. Oxygenation was maintained during apnea, with a transient increase in PaCO2 observed after intubation.
Keywords: transnasal humidified rapid-insufflation ventilatory exchange, oropharyngeal airway, gastric insufflation, general anesthesia, obstructive sleep apnea
Introduction
It is reported that pulmonary aspiration of gastric contents, which can result from gastric reflux, remains a significant cause of morbidity and mortality during general anesthesia.1 Contributing factors include elevated intragastric pressure, lower esophageal sphincter dysfunction, delayed gastric emptying, and ineffective ventilation techniques. During induction, the loss of consciousness, relaxation of airway muscles, and suppression of pharyngeal reflexes elevate the risk of aspiration, particularly when gastric insufflation occurs.2 Such distension can impair surgical visibility during abdominal procedures, complicate the surgical field, and increase the risk of perioperative injury. Therefore, preventing gastric insufflation is crucial for patient safety and surgical efficacy.
The high prevalence of obstructive sleep apnea (OSA), especially among surgical populations, makes preoperative identification of at-risk patients a necessary foundation for implementing safety measures.3 Although polysomnography is the gold standard for diagnosing OSA, it is not suitable for routine preoperative use due to time and resource constraints. For patients with a STOP-Bang score of ≥3, the likelihood of having OSA is high.4 In addition, overweight and obesity are closely associated with upper airway collapsibility and increased perioperative airway-related complications; therefore, patients with a body mass index (BMI) ≥25 kg/m2 and a STOP-Bang score ≥3 were considered a population at high risk for OSA in the present study. Previous research has shown that OSA is an independent risk factor for gastric insufflation during anesthesia induction.5 Therefore, patients at high risk for OSA may be particularly vulnerable to gastric insufflation and hypoxemia during induction. Patients with OSA pose unique challenges during induction due to reduced oxygen reserves and an increased risk of hypoxemia, with a higher risk for difficult mask ventilation and airway management, underscoring the need for effective preoxygenation.6,7
Current strategies, such as pressure-controlled face ventilation (PCFV) and modified rapid sequence induction, aim to balance adequate ventilation with minimizing gastric insufflation. PCFV delivers positive pressure to inflate the lungs but concurrently risks forcing gas into the esophagus, leading to gastric insufflation. One study has shown that an inspiratory pressure of 15 cm H2O allowed for reduced occurrence of gastric insufflation with proper lung ventilation during induction of anesthesia.8 However, these methods remain suboptimal. Although an oropharyngeal airway helps to establish a patent airway by preventing the tongue from covering the epiglottis,9 it may also reduce upper airway resistance and decrease the inspiratory pressure required for effective mask ventilation, thereby potentially lowering the risk of gas entering the esophagus and stomach. However, its effect on gastric insufflation in patients at high risk for OSA remains unclear. In contrast, transnasal humidified rapid insufflation ventilatory exchange (THRIVE) is based on apneic oxygenation. It delivers a continuous flow of humidified oxygen via the nasal cannula, facilitating oxygen uptake and carbon dioxide clearance through diffusion and convection, respectively, without generating significant positive pressure in the pharynx. THRIVE has shown promise as an apneic oxygenation technique,10,11 yet its impact on gastric insufflation risk in patients at high risk for OSA has not been thoroughly evaluated.
To date, no previous study has directly compared THRIVE with oropharyngeal airway-assisted face-mask ventilation in patients at high risk for OSA during anesthetic induction. Therefore, we designed this study to compare THRIVE with oropharyngeal airway-assisted face-mask ventilation in patients at high risk for OSA during anesthetic induction, focusing on the incidence of gastric insufflation, oxygenation efficacy, and patient comfort. In addition, we aimed to evaluate whether THRIVE could serve as an effective airway-management strategy while reducing gastric insufflation during induction in this high-risk population.
Materials and Methods
Study Design and Ethics
This study was conducted in accordance with the principles of the Declaration of Helsinki and approved by the Medical Ethics Committee of Zhejiang Cancer Hospital on March 26, 2024 (Approval No. IRB-2024-284 (IIT)), and written informed consent was obtained from all subjects participating in the trial. The trial was registered before patient enrollment in the Chinese Clinical Trial Registry (ChiCTR2400083976). This study was reported in line with the Consolidated Standards of Reporting Trials (CONSORT) guidelines.12
Patient Recruitment
Patient recruitment took place from May 2024 to December 2024. Written informed consent was obtained from all eligible participants before surgery. This prospective study included adults aged 18 to 80 years with a STOP-Bang score of ≥3 and a body mass index (BMI) of ≥25 kg∙m−2, undergoing elective major abdominal surgery with general anesthesia and endotracheal intubation (ASA I–III). Exclusion criteria included craniofacial or nasopharyngeal abnormalities, gastrointestinal instrumentation, inadequate gastric sonographic imaging, ASA classification >III, active respiratory conditions (eg, obstructive lung disease, recent bronchospasm within three months, or acute airway infection within one week), pregnancy, and lactation.
Randomization and Allocation
A total of 116 patients at high risk for OSA were initially enrolled in the study. Of these, 12 did not meet the inclusion criteria, and 4 declined to participate, yielding 100 patients for randomization. Participants were sequentially numbered and randomized using a computer-generated sequence into two groups: oropharyngeal airway-assisted face-mask ventilation (Group M, n=50) and THRIVE (Group T, n=50). Allocation concealment was maintained with sealed opaque envelopes managed by an independent study coordinator. Treatment allocation was established by opening a sealed opaque envelope after informed consent had been given and once the patient was in the operating theater preoperative area. All gastric ultrasonography procedures were performed by a single experienced anesthesiologist, while a blinded evaluator independently analyzed the gastric antrum images. Although patients and the attending anesthesiologist were aware of group assignments because of the visible differences between the ventilation modalities, the ultrasound examiner and image assessor were not involved in group allocation or intraoperative management. Efforts were made to minimize awareness of the assigned intervention during ultrasonographic assessment to reduce potential assessment bias.
Gastric Insufflation and Antral Cross-Sectional Area Measurement
Gastric ultrasound, an imaging modality that has recently emerged for assessing gastric volume and detecting gastric insufflation, demonstrates high sensitivity and specificity. Real-time ultrasonographic examination of the gastric antrum during mask ventilation allows for the straightforward visualization of gastric air entry. The presence of air is indicated by characteristic sonographic artifacts, such as an acoustic shadow or a comet-tail artifact.13 The standardized scanning technique for the gastric antrum involves a sagittal view obtained slightly to the right of the anterior midline, inferior to the xiphoid process. The gastric antrum was located between the left lobe of the liver and the pancreas at the level of the abdominal aorta.14 The patient is positioned supine, and a standard low-frequency (2–5 MHz) convex array abdominal probe is used, with the probe marker oriented cranially. In the fasted state before anesthesia induction, ultrasonography of the gastric antrum typically reveals a’bull’s-eye’sign. Following mask ventilation, a significant increase in the antral cross-sectional area may be observed, and the presence of acoustic shadowing or the characteristic “comet-tail” sign indicates gastric insufflation (Figure 1). The degree of gastric insufflation can be quantified by comparing the antral cross-sectional area (CSAa) measured via ultrasound before and after ventilation.15 For optimal data accuracy, the antral cross-sectional area (CSAa) should be measured during gastric systole. The CSAa is calculated using the formula: CSAa=(AP×CC×π)/4, where AP and CC represent the anteroposterior and craniocaudal diameters of the antrum, respectively.16 Therefore, this study utilized gastric ultrasound to monitor for gastric insufflation and to quantify associated changes in the CSAa during the induction of general anesthesia in patients at high risk for OSA.
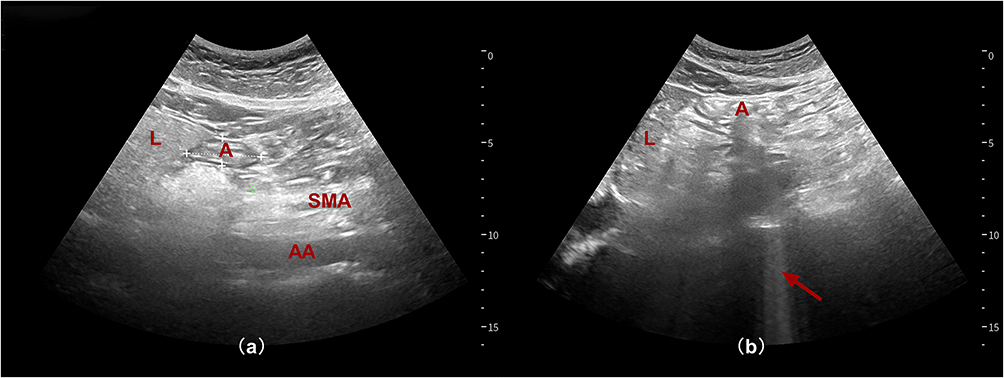 |
Figure 1 Ultrasonographic diagnosis of gastric insufflation. (a) No gastric insufflation. (b) Gastric insufflation. The red arrow indicates the comet tail. Abbreviations: A, gastric antrum; L, liver; SMA, superior mesenteric artery; AA, abdominal aorta. |
Intervention
Preoperative Evaluation
One day before surgery, each participant received a comprehensive preoperative evaluation that included a review of medical history, demographic information (such as sex and age) along with detailed anthropometric measurements (including height, weight, body mass index, and neck circumference), airway anatomical assessments (thyromental distance, interincisal distance, and Mallampati score), risk stratification using ASA Classification and STOP-Bang Score, functional evaluations of cardiopulmonary and respiratory status, and baseline laboratory tests. Written informed consent was obtained from every patient and their family after a full explanation of the study protocol.
Preoperative Preparation
On the day of surgery, patients fasted for 8 h and abstained from clear liquids for at least 2 h. No pre-anesthetic medication was administered. Upon arrival in the operating room, baseline vital signs—non-invasive blood pressure, heart rate, and peripheral oxygen saturation—were recorded (T1). A radial arterial catheter was then inserted for continuous invasive arterial blood pressure monitoring and arterial blood gas sampling. A trained anesthesiologist, blinded to group assignment, obtained ultrasound images of the gastric antrum to assess image quality and exclude residual gastric contents (Supplemental Figure S1). During gastric systole, three consecutive images of the CSAa were acquired at 5s intervals and stored. Blinding was attempted by draping the ventilation equipment to minimize visualization of the ventilation modality during ultrasonography; however, complete concealment of group allocation could not be guaranteed because of the visible differences between the THRIVE and face-mask ventilation setups.
Anesthesia Induction and Ventilation
Anesthesia induction was administered by a separate anesthesiologist. Both groups received preoxygenation for 3 min. Patients in the oropharyngeal airway-assisted face-mask ventilation group were preoxygenated via a tightly sealed mask (100% O2, 10 L∙min−1) (Supplemental Figure S2). In contrast, patients in the THRIVE group received high-flow, heated, and humidified oxygen (100% O2, 30 L∙min−1, 37°C) via nasal cannula without mask ventilation (OptiflowTM, Fisher and Paykel Healthcare Limited, Auckland, New Zealand) (Supplemental Figure S3). After 3 min of preoxygenation (T2), gastric antral ultrasonography was repeated, CSAa images were obtained, and arterial blood gas analysis was performed simultaneously. Anesthesia was then induced using propofol (1.5–2 mg∙kg−1), sufentanil (0.4 μg∙kg−1), and rocuronium (0.9 mg∙kg−1), dosed according to ideal body weight. Upon confirmation of unconsciousness, procedures differed between groups. In the oropharyngeal airway-assisted face-mask ventilation group, an oropharyngeal airway was inserted (size: 9 cm for women, 10 cm for men), the head was tilted back, and a tight-fitting mask was secured using a two-handed jaw thrust technique. Ventilation was provided via the anesthesia machine in pressure-controlled ventilation (PCV) mode with settings: inspiratory pressure 15 cm H2O, I: E ratio 1: 2, respiratory rate 12 breaths min−1, PEEP 0 cm H2O, 100% O2, and flow rate 10 L∙min−1. The THRIVE group continued to receive high-flow, heated, and humidified oxygen (100% O2, 37°C) via nasal cannula, with the flow rate adjusted to 60 L∙min−1. The head was tilted back, and a two-handed jaw lift was performed to maintain airway patency while keeping the mouth closed. After 3 min of ventilation (T3), arterial blood gas analysis was performed, followed immediately by tracheal intubation. If SpO2 fell below 92% for more than 10s after induction, two-person mask ventilation was initiated. Immediately after tracheal intubation (T4), gastric antral ultrasonography was repeated, CSAa images were obtained, and arterial blood gas analysis was performed simultaneously. Mask ventilation and oropharyngeal airway placement were performed by an anesthetist with >5 years of clinical experience. An anesthesiologist with expertise in gastric ultrasound assessed for the presence of comet-tail signs and measured the gastric antral area. The results were averaged from three CSAa images.
Data Collection
The primary outcome was the incidence of gastric insufflation at T4, as determined by the presence of a comet-tail sign on gastric ultrasonography. Gastric insufflation detected at T2 was considered baseline insufflation before induction-related ventilation or apneic oxygenation and was analyzed separately. Arterial blood gas and oxygenation-related variables (including SpO2, pH, PaO2, and PaCO2) were recorded at time points T1, T2, T3, and T4. Adverse events—including epistaxis, pharyngeal discomfort, barotrauma, regurgitation/aspiration, and postoperative nausea/vomiting within 24 hours—were systematically documented. Patient comfort before loss of consciousness was quantified using a standardized six-point smiley-face scale (Supplemental Figure S4).17
Sample Size Calculation
The sample size was calculated for this trial was calculated using PASS 15.0 software (NCSS, LLC, Kaysville, UT, USA), based on data from previous studies and relevant literature.5 Gastric insufflation was reported in 13% (4/30) of patients in the THRIVE group,5 and our pilot study showed that 40% (12/30) of patients in the oropharyngeal airway-assisted face-mask ventilation group experienced gastric insufflation. To achieve 80% power with a significance level of 0.05 for detecting between-group differences, a minimum of 41 patients per group was required. Considering potential dropouts, the final sample size was set at 50 patients per group.
Statistical Analysis
Statistical analysis was conducted using SPSS 26.0 (IBM Corp). Continuous variables with normal distribution were expressed as mean ± standard deviation, while non-normally distributed data were reported as median (interquartile range). Between-group comparisons employed independent samples t-test for parametric data and Mann–Whitney U-test for non-parametric distributions. Categorical variables were presented as frequencies (percentages), analyzed using χ2-test or Fisher’s exact test as appropriate. The 95% confidence interval for the absolute risk reduction of the primary outcome was calculated using the Newcombe method for two independent proportions. For longitudinal analysis of CSAa, repeated-measures ANOVA with Greenhouse-Geisser correction addressed violations of sphericity (Mauchly’s test P < 0.05). All hypothesis testing was two-tailed, with α = 0.05 considered statistically significant. Data visualization was generated using GraphPad Prism 10.0 (GraphPad Software).
Results
This prospective study enrolled 116 patients at high risk for OSA between May and December 2024. After excluding 12 patients who did not meet the inclusion criteria and 4 who declined to participate, 100 participants were randomized equally to either Group M or Group T. 3 participants per group were subsequently excluded due to indiscernible gastric antral ultrasound images during pre-trial assessment. Ultimately, 47 participants in each group completed protocolized anesthesia induction and ventilation procedures with full assessment compliance. Participant progression is detailed in the CONSORT diagram (Figure 2), with baseline demographic and clinical characteristics presented in Table 1.
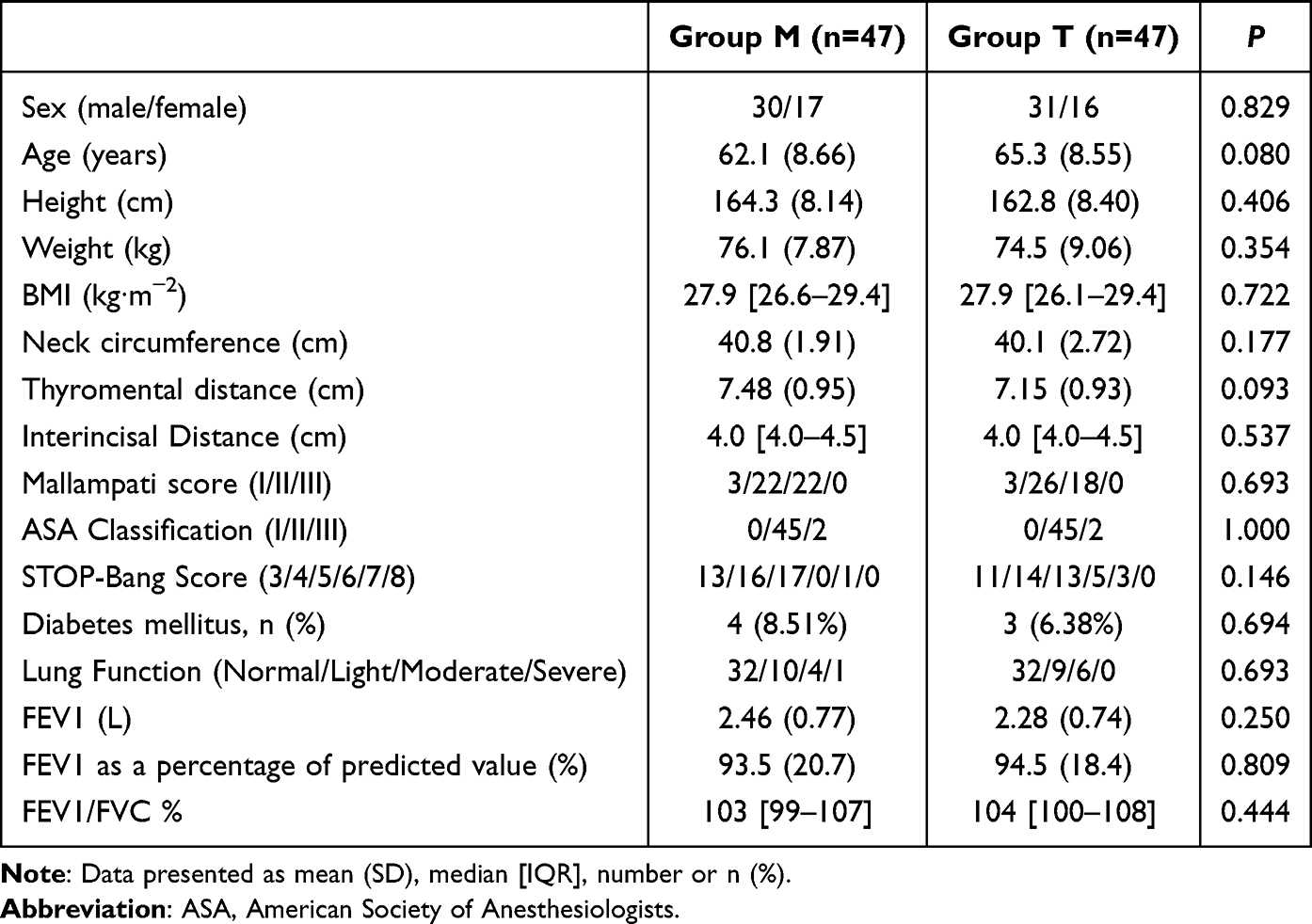 |
Table 1 Baseline Patient Characteristics |
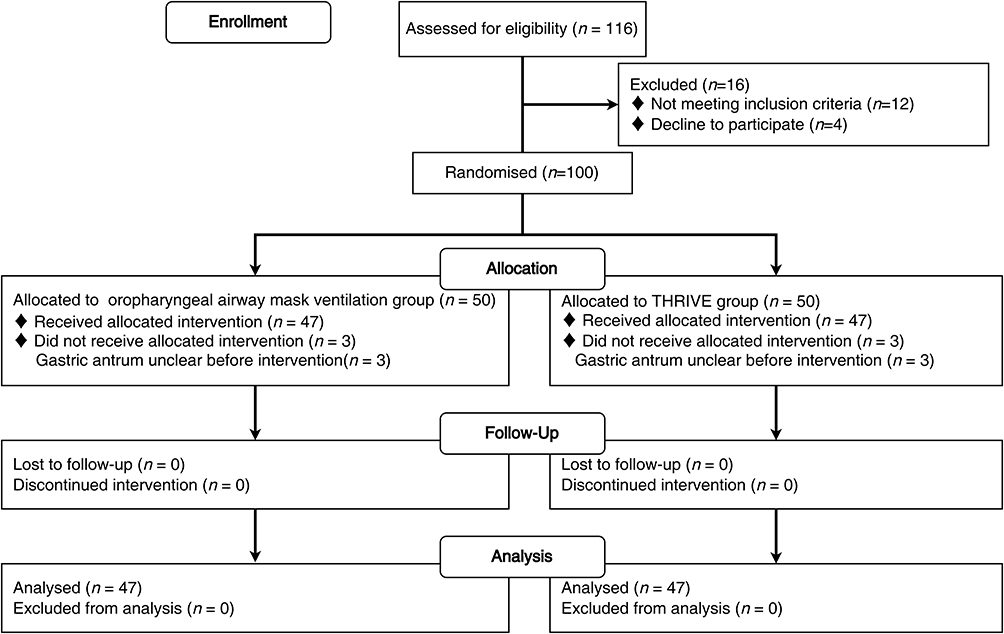 |
Figure 2 CONSORT Flow Diagram. |
The Incidence of Gastric Insufflation
This study evaluated gastric insufflation incidence through ultrasonographic detection of comet-tail signs in the gastric antrum under different ventilation modalities (Table 2). At the T2 timepoint (3 min preoxygenation pre-induction), gastric insufflation rates were comparable between groups, occurring in 10.6% (5/47) of patients in Group M and 14.9% (7/47) of patients in Group T (P = 0.536). The primary outcome was the incidence of gastric insufflation at T4 (immediately after tracheal intubation). At T4, Group T demonstrated a significantly lower incidence of gastric insufflation compared with Group M (23.4% [11/47] vs 44.7% [21/47]), corresponding to an absolute risk reduction of 21.3% (95% CI, 2.1% to 38.4%). Chi-square analysis demonstrated a statistically significant intergroup difference (χ2 = 4.738, P = 0.030).
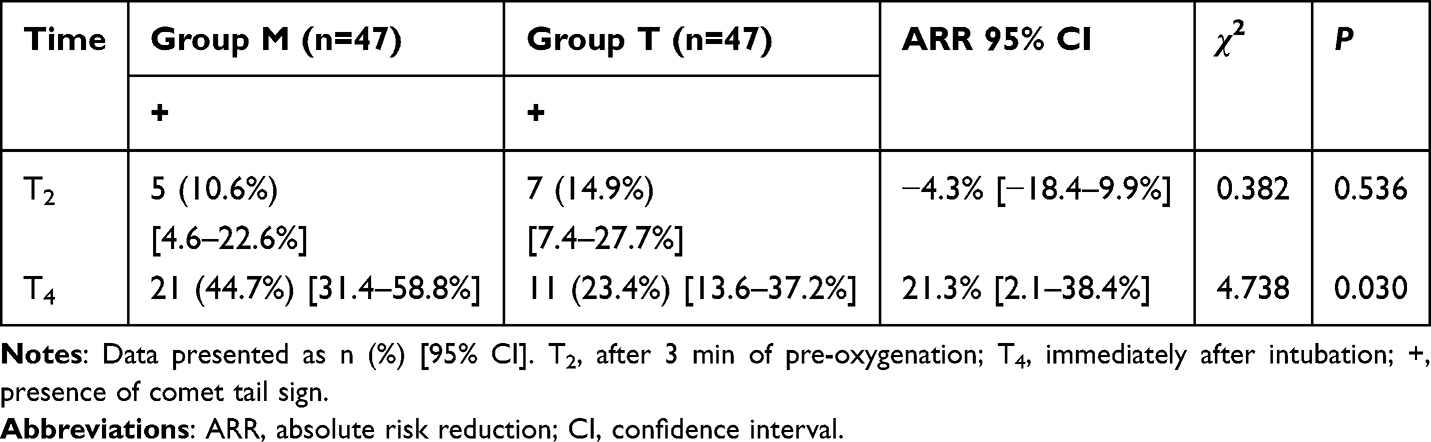 |
Table 2 The Incidence of Comet Tail Sign |
The Cross-Sectional Area of the Gastric Antrum
Repeated-measures ANOVA with Greenhouse–Geisser adjustment for violations of sphericity showed no between-group differences in CSAa at T1, T2, or T4 (all P > 0.05), indicating comparable antral size across these time points. A significant group-by-time interaction was detected (P < 0.001), demonstrating that ventilation mode influenced CSAa trajectories. Specifically, the median percentage increase in CSAa from T1 to T4 was higher in the mask ventilation group (Group M: 13.24%, IQR 3.64–33.48%) than in the THRIVE group (Group T: 7.62%, IQR 2.55–18.55%; P = 0.070), although the difference in CSAa did not reach statistical significance. These findings, summarized in Supplemental Table 1, suggest that THRIVE is associated with less gastric insufflation and reduced intragastric gas accumulation compared with mask ventilation.
SpO2 and Arterial Blood Gas pH, PaO2, PaCO2
Normality testing confirmed the non-normal distribution of SpO2 data; all other parameters exhibited normal distribution. Between-group comparisons utilized independent samples t-tests for normally distributed variables and non-parametric tests for SpO2. Supplemental Table 2 presents the values for SpO2, pH, PaO2, and PaCO2 at each time point. Trends for pH, PaO2, and PaCO2 are illustrated in Figure 3.
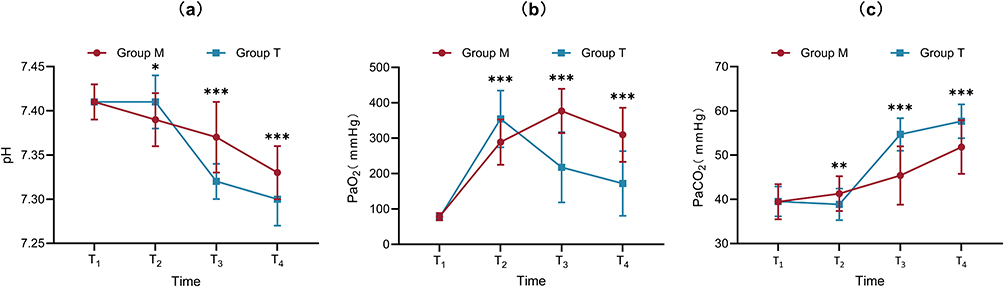 |
Figure 3 Arterial blood gas variables including (a) pH, (b) PaO2, (c) PaCO2 at before pre-oxygenation (T1), after 3 min of pre-oxygenation (T2), after 3 min of ventilation following induction of unconsciousness by anesthesia (T3), and immediately after intubation (T4). *P < 0.05, **P < 0.01, ***P < 0.001. Abbreviations: pH, potential of hydrogen; PaO2, Partial pressure of oxygen in arterial blood; PaCO2, Partial pressure of carbon dioxide in arterial blood. |
At baseline (T1), no significant intergroup differences were observed for SpO2, pH, PaO2, or PaCO2 (P > 0.05 for all). Following 3 min of preoxygenation (T2), SpO2 reached 100% in both groups (P = 0.559). However, significant intergroup differences emerged for arterial blood gases at T2 (P < 0.05). Specifically, PaO2 was significantly higher in Group T (354.47 ± 79.90 mmHg) compared with Group M (288.83 ± 63.89 mmHg; P < 0.001). Conversely, PaCO2 was significantly lower in Group T (38.85 ± 3.56 mmHg) than in Group M (41.28 ± 3.92 mmHg; P = 0.002), although values in both groups remained within the normal physiological range.
Significant intergroup differences persisted for pH, PaO2, and PaCO2 at T3 and T4 (P < 0.001 for all comparisons). At T3, PaO2 was significantly lower in Group T (217.74 ± 99.23 mmHg) compared with Group M (376.87 ± 62.65 mmHg; P < 0.001). This difference remained significant at T4, with lower PaO2 in Group T (172.06 ± 91.33 mmHg) versus Group M (309.64 ± 76.31 mmHg; P < 0.001), likely reflecting the absence of mechanical ventilation in Group T during these time points. Despite these differences, oxygenation levels remained clinically acceptable. Concurrently, PaCO2 was significantly higher in Group T at both T3 (54.67 ± 3.68 mmHg vs 45.38 ± 6.61 mmHg in Group M; P < 0.001) and T4 (57.64 ± 3.83 mmHg vs 51.83 ± 6.09 mmHg in Group M; P < 0.001), accompanied by corresponding reductions in pH. However, all measured parameters remained within clinically acceptable ranges and were expected to improve following continued mechanical ventilation after tracheal intubation. No significant intergroup differences in SpO2 were observed during intubation, and SpO2 was greater than 92%.
General Adverse Reaction
The following adverse events were systematically monitored within 24 hours post-procedure: epistaxis, nasopharyngeal discomfort, pneumatic pressure injury, regurgitation/aspiration, and nausea/vomiting. Statistical analysis revealed no significant difference in the incidence of these events between Group M and Group T (P = 1.000) (Supplemental Table 3). No instances of epistaxis, pneumatic pressure injury, or regurgitation/aspiration were observed in either group. Nasopharyngeal discomfort occurred in two patients in Group M and one patient in Group T; symptoms were mild in all cases. Postoperative nausea and vomiting (PONV) within the first 24 hours occurred in five patients in each group and were successfully managed with symptomatic treatment. It should be noted that the absence of rare adverse events in this sample size does not allow conclusions regarding equivalence of safety between the two interventions. PONV may also be influenced by multiple perioperative factors, including anesthetic management and individual susceptibility.
Comfort
Patient comfort during preoxygenation and induction of anesthesia was evaluated using a six-point smiley face scale, where a score of 0 indicated no discomfort. Statistical analysis revealed that patients in Group T experienced significantly greater comfort compared to those in Group M (P < 0.001) (Figure 4 and Supplemental Table 4). These results suggest that the ventilation method utilized in Group T provided a more comfortable experience during the preoxygenation and induction phases.
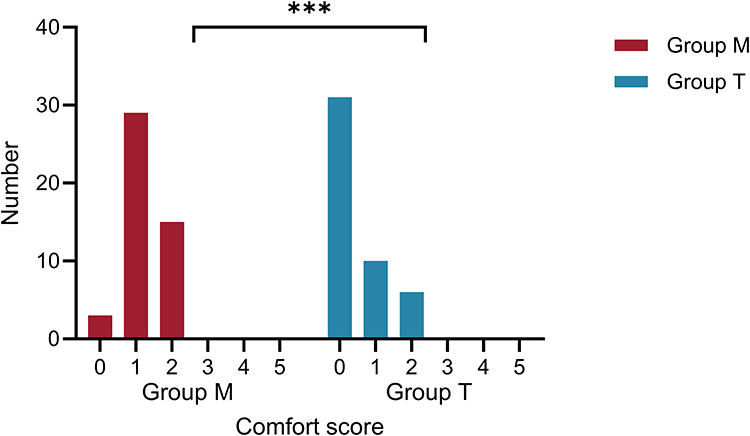 |
Figure 4 Comparison of comfort scores between Group M and Group T. Group comparison, ***P < 0.001. |
Discussion
THRIVE significantly reduced the incidence of gastric insufflation during general anesthesia induction in patients at high risk for OSA. This effect is likely attributable to its sustained low airway pressure (<10 cm H2O), which remains below the typical lower esophageal sphincter pressure in awake adults (16 cm H2O), thereby reducing gas ingress associated with the pressure fluctuations inherent in conventional mask ventilation.18 These findings are consistent with previous reports on pressure-controlled ventilation (10–15 cm H2O),8,15,19–21 and extend the demonstrated utility of THRIVE to high-risk OSA populations. However, THRIVE did not completely prevent gastric insufflation, which was still observed in 23.4% of cases. This highlights a fundamental physiological limit: any gas flow into the upper airway risks an inherent risk of gastric insufflation in susceptible individuals. Therefore, THRIVE should be viewed as a risk-reduction strategy rather than a definitive solution, and appropriate monitoring for this complication remains necessary. It is important to note that this study did not demonstrate a direct reduction in pulmonary aspiration, a rare clinical event. While the comet-tail sign is a valuable surrogate safety endpoint, future research with the statistical power to track clinical aspiration events is needed to confirm whether reducing this marker translates into improved patient-centered outcomes.
Although THRIVE significantly reduced the incidence of comet-tail signs indicative of gastric insufflation and showed a possible trend toward reduced gastric distension, the between-group difference in CSAa change did not reach statistical significance. This discrepancy may reflect the higher sensitivity of comet-tail artifacts for detecting small amounts of intragastric air, whereas measurable changes in gastric antral area may require a greater volume of gastric distension. In addition, interindividual variability in gastric compliance and the limited sample size may have reduced the ability to detect statistically significant CSAa differences. This observation is consistent with documented gastric insufflation occurring at pressures of 10–25 cmH2O in non-paralyzed patients,22 a risk that THRIVE may mitigate through its stable, low-pressure delivery. In OSA patients, characterized by inherent pharyngeal collapsibility and posterior tongue displacement,23,24 an oropharyngeal airway relieves supraglottic obstruction but may alter upper airway geometry and airflow distribution in a way that is not fully understood. During positive-pressure ventilation, airflow may be redistributed within the upper airway, and any potential effect on pressure transmission to the hypopharyngeal region remains speculative. The independent contribution of the oropharyngeal airway to gastric insufflation therefore remains hypothetical, as this study lacked a mask-ventilation-only control group for direct comparison. This requires validation in future controlled studies.
THRIVE offers several established advantages: it improves preoxygenation, prolongs safe apnea time, and, as shown here, reduces gastric insufflation. These benefits are attributed to the maintenance of positive airway pressure and the washout of upper airway dead space, mechanisms that have been previously demonstrated in general populations.5,25,26 Blood gas analysis confirmed THRIVE provided superior preoxygenation, with significantly higher PaO2 than the facemask group. However, during the apneic period, the THRIVE group exhibited a marked downward trend in PaO2, indicating a progressive decline in oxygen reserve. But safe SpO2 levels were maintained in both groups throughout the procedure. These findings support the potential role of THRIVE as a strategy for maintaining oxygenation while reducing the risk of gastric insufflation during anesthetic induction, consistent with emergency difficult airway protocols and previous findings.25–28 In the context of an anticipated or encountered difficult airway, where intubation may be prolonged, the decision to use THRIVE necessitates a careful risk-benefit analysis: the potential benefit of a higher initial PaO2 must be balanced against the risk of a more rapid depletion of oxygen reserves during a potentially challenging apnea. It is noteworthy that mild hypercapnia was observed in the THRIVE group at the early post-intubation time point, and further changes after initiation of mechanical ventilation were not assessed in this study. This finding is a recognized physiological consequence of apneic oxygenation, as THRIVE primarily facilitates oxygen delivery and carbon dioxide clearance through diffusion and convection, which is less efficient than active alveolar ventilation. In most patients, In most patients, this transient increase in PaCO2 is expected to improve following the initiation of effective mechanical ventilation after intubation.; however, in patients with comorbidities, even transient hypercapnia may be detrimental. Therefore, we propose that THRIVE should be used with caution, if at all, in patients with conditions that may be exacerbated by hypercapnia, such as known intracranial hypertension or severe pulmonary arterial hypertension.
Within Enhanced Recovery After Surgery (ERAS) frameworks, THRIVE may offer potential perioperative benefits. Enhanced patient comfort (P < 0.05) may contribute to reduced induction-related stress responses, while the reduction in gastric insufflation may have implications for perioperative complication reduction. These findings are consistent with previous research.17 However, postoperative recovery outcomes and surgical field visibility were not directly assessed in this study. Therefore, the potential role of THRIVE in improving ERAS-related outcomes warrants further investigation.
This study has several limitations that should be acknowledged. First, patients were screened for high risk of obstructive sleep apnea (OSA) using the STOP-Bang score (≥3)29,30 rather than confirmed by the diagnostic gold standard, polysomnography (PSG), due to practical and logistical constraints, which may introduce potential misclassification bias and limit accurate assessment of OSA severity. Second, the incidence of gastric insufflation was evaluated using ultrasound-based measurement of gastric antral cross-sectional area, which represents a surrogate endpoint rather than the clinically definitive outcome of pulmonary aspiration, and therefore cannot fully reflect true aspiration risk; moreover, measurements were performed only at predefined time points, which may not capture dynamic peri-induction changes. Third, the sample size was relatively limited, potentially reducing statistical power for detecting rare adverse events; although the observed incidence of gastric insufflation in the THRIVE group was higher than initially assumed during sample size estimation, suggesting that the true effect size may have been smaller than expected a priori, the study remained sufficiently powered to detect statistically significant between-group differences in the primary outcome but was not specifically powered for safety endpoints. Finally, the single-center design may limit generalizability, and patient-reported comfort scores may be influenced by subjective psychological factors, introducing potential reporting bias. Future multicenter studies incorporating PSG-confirmed OSA populations, clinically relevant aspiration outcomes, and predefined safety powering are warranted to further strengthen the evidence base.
Conclusion
In patients at high risk for OSA undergoing elective abdominal surgery, THRIVE reduced ultrasound-detected gastric insufflation during induction compared with oropharyngeal airway-assisted pressure-controlled mask ventilation, while improving preoxygenation and comfort. THRIVE maintained oxygenation during apnea, with a transient increase in PaCO2 observed after intubation, warranting caution in patients vulnerable to hypercapnia. No significant differences in adverse event rates were observed between groups. Overall, THRIVE may be a useful option for preoxygenation and ventilation in this patient population.
Abbreviations
OSAS, Obstructive Sleep Apnea Syndrome; THRIVE, Transnasal Humidified Rapid-insufflation Ventilatory Exchange; BMI, Body Mass Index; ASA, American Society of Anesthesiologists; CSAa, Cross-sectional area of the antrum; PCV, Pressure Control Ventilation; PCFV, Pressure Controlled Face Ventilation; PEEP, Positive End-Expiratory Pressure; pH, potential of hydrogen; PaO2, Partial pressure of oxygen in arterial blood; PaCO2, Partial pressure of carbon dioxide in arterial blood; SpO2, Peripheral Capillary Oxygen Saturation; FEV1, Forced Expiratory Volume in one second; FVC, Forced Vital Capacity; ERAS, Enhanced Recovery After Surgery; PSG, Polysomnography.
Data Sharing Statement
All data generated or analyzed during this study are included in the article. Further inquiries about the datasets can be directed to the corresponding author (Kangjie Xie) on reasonable request.
Acknowledgments
We sincerely thank all members of the research group for their valuable help and support during the study.
Funding
This study was supported by the Zhejiang Province Traditional Chinese Medicine Science and Technology Project (2023ZL302) and the Zhejiang Province Medical and Health Research Project (2025KY728).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sakai T, Planinsic RM, Quinlan JJ, Handley LJ, Kim T-Y, Hilmi IA. The incidence and outcome of perioperative pulmonary aspiration in a university hospital: a 4-year retrospective analysis. Anesth Analg. 2006;103:941–12. doi:10.1213/01.ane.0000237296.57941.e7
2. Ng A, Smith G. Gastroesophageal reflux and aspiration of gastric contents in anesthetic practice. Anesth Analg. 2001;93:494–513. doi:10.1213/00000539-200108000-00050
3. Benjafield AV, Ayas NT, Eastwood PR, et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: a literature-based analysis. Lancet Respir Med. 2019;7:687–698. doi:10.1016/S2213-2600(19)30198-5
4. Chung F, Abdullah HR, Liao P. STOP-Bang questionnaire: a practical approach to screen for obstructive sleep apnea. Chest. 2016;149:631–638. doi:10.1378/chest.15-0903
5. Zhou X, Huang X, Zhou Z, et al. Effect of transnasal humidified rapid-insufflation ventilatory exchange on gastric insufflation during anaesthesia induction: a randomised controlled trial and multivariate analysis. Eur J Anaesth. 2023;40:521–528. doi:10.1097/EJA.0000000000001846
6. Sato S, Hasegawa M, Okuyama M, et al. Mask ventilation during induction of general anesthesia: influences of obstructive sleep apnea. Anesthesiology. 2017;126:28–38. doi:10.1097/ALN.0000000000001407
7. Cozowicz C, Memtsoudis SG. Perioperative management of the patient with obstructive sleep apnea: a narrative review. Anesth Analg. 2021;132:1231. doi:10.1213/ANE.0000000000005444
8. Bouvet L, Albert M-L, Augris C, et al. Real-time detection of gastric insufflation related to facemask pressure-controlled ventilation using ultrasonography of the antrum and epigastric auscultation in nonparalyzed patients: a prospective, randomized, double-blind study. Anesthesiology. 2014;120:326–334. doi:10.1097/ALN.0000000000000094
9. Kim SH, Kim JE, Kim YH, et al. An assessment of oropharyngeal airway position using a fibreoptic bronchoscope. Anaesthesia. 2014;69:53–57. doi:10.1111/anae.12502
10. Spence EA, Rajaleelan W, Wong J, Chung F, Wong DT. The effectiveness of high-flow nasal oxygen during the intraoperative period: a systematic review and meta-analysis. Anesth Analg. 2020;131:1102–1110. doi:10.1213/ANE.0000000000005073
11. Wong DT, Dallaire A, Singh KP, et al. High-flow nasal oxygen improves safe apnea time in morbidly obese patients undergoing general anesthesia: a randomized controlled trial. Anesth Analg. 2019;129:1130–1136. doi:10.1213/ANE.0000000000003966
12. Schulz KF, Altman DG, Moher D, et al. CONSORT 2010 Statement: updated guidelines for reporting parallel group randomised trials. BMJ. 2010;340:c332–c332. doi:10.1136/bmj.c332
13. Tan Y, Wang X, Yang H, et al. Ultrasonographic assessment of preoperative gastric volume in patients with dyspepsia: a prospective observational study. BMC Anesthesiol. 2022;22:21. doi:10.1186/s12871-021-01559-4
14. Perlas A, Xiao MZ, Tomlinson G, et al. Baseline gastric volume of fasting diabetic patients is not higher than that of non-diabetics. A cross-sectional non-inferiority study. Anesthesiology. 2024;140:648–656. doi:10.1097/ALN.0000000000004815
15. Gamal M, Mostafa M, Farrag Y, et al. Evaluation of adequacy of ventilation and gastric insufflation at three levels of inspiratory pressure for facemask ventilation during induction of anaesthesia: a randomised controlled trial. Anaesth Crit Care Pain Med. 2022;41:101132. doi:10.1016/j.accpm.2022.101132
16. Van de Putte P, Perlas A. Ultrasound assessment of gastric content and volume. Br J Anaesth. 2014;113:12–22. doi:10.1093/bja/aeu151
17. Merry AF, van Waart H, Allen SJ, et al. Ease and comfort of pre-oxygenation with high-flow nasal oxygen cannulae vs. facemask: a randomised controlled trial. Anaesthesia. 2022;77:1346–1355. doi:10.1111/anae.15853
18. Von Goedecke A, Voelckel WG, Wenzel V, et al. Mechanical versus manual ventilation via a face mask during the induction of anesthesia: a prospective, randomized, crossover study. Anesth Analg. 2004;98:260–263. doi:10.1213/01.ANE.0000096190.36875.67
19. Ding Y, Huang T, Ge Y, Gao J, Zhang Y. Effect of trans-nasal humidified rapid insufflation ventilatory exchange on reflux and microaspiration in patients undergoing laparoscopic cholecystectomy during induction of general anesthesia: a randomized controlled trial. Front Med. 2023;10:1212646. doi:10.3389/fmed.2023.1212646
20. Calairadjane J, Rudingwa P, Panneerselvam S, Kuberan A, Velraj J. Assessment of incidence of gastric insufflation using ultrasound in anaesthetised and paralysed patients receiving transnasal humidified rapid insufflation ventilatory exchange: a pre and postintervention study. Eur J Anaesth. 2023;40:529–531. doi:10.1097/EJA.0000000000001851
21. Crístian De Carvalho C, Iliff HA, Santos Neto JM, et al. Effectiveness of preoxygenation strategies: a systematic review and network meta-analysis. Br J Anaesth. 2024;133:152–163. doi:10.1016/j.bja.2024.02.028
22. Cajander P, Edmark L, Ahlstrand R, Magnuson A, De Leon A. Effect of positive end-expiratory pressure on gastric insufflation during induction of anaesthesia when using pressure-controlled ventilation via a face mask: a randomised controlled trial. Eur J Anaesth. 2019;36:625–632. doi:10.1097/EJA.0000000000001016
23. Eriksson LI, Sundman E, Olsson R, et al. Functional Assessment of the Pharynx at Rest and during Swallowing in Partially Paralyzed Humans. Anesthesiology. 1997;87:1035–1043. doi:10.1097/00000542-199711000-00005
24. Chou HC, Wu TL. Large hypopharyngeal tongue: a shared anatomic abnormality for difficult mask ventilation, difficult intubation, and obstructive sleep apnea? Anesthesiology. 2001;94:936–937. doi:10.1097/00000542-200105000-00043
25. Lei G, Wu L, Xi C, Xiao Y, Wang G. Transnasal humidified rapid insufflation ventilatory exchange augments oxygenation in children with juvenile onset recurrent respiratory papillomatosis during surgery: a prospective randomized crossover controlled trial. Anesth Analg. 2023;137:578–586. doi:10.1213/ANE.0000000000006521
26. Lodenius Å, Piehl J, Östlund A, Ullman J, Jonsson Fagerlund M. Transnasal humidified rapid-insufflation ventilatory exchange (THRIVE) vs. facemask breathing pre-oxygenation for rapid sequence induction in adults: a prospective randomised non-blinded clinical trial. Anaesthesia. 2018;73:564–571. doi:10.1111/anae.14215
27. Mir F, Patel A, Iqbal R, Cecconi M, Nouraei SA. A randomised controlled trial comparing transnasal humidified rapid insufflation ventilatory exchange (THRIVE) pre-oxygenation with facemask pre-oxygenation in patients undergoing rapid sequence induction of anaesthesia. Anaesthesia. 2017;72:439–443. doi:10.1111/anae.13799
28. Zheng D, Yao Y, Luo C, et al. Effectiveness of trans-nasal humidified rapid insufflation ventilatory exchange compared with standard facemask oxygenation for pre- and apneic oxygenation during anesthesia induction: a meta-analysis based on randomized controlled trials. PLoS One. 2024;19:e0302626. doi:10.1371/journal.pone.0302626
29. Nagappa M, Patra J, Wong J, et al. Association of STOP-Bang questionnaire as a screening tool for sleep apnea and postoperative complications: a systematic review and bayesian meta-analysis of prospective and retrospective cohort studies. Anesth Analg. 2017;125:1301–1308. doi:10.1213/ANE.0000000000002344
30. Cho T, Yan E, Chung F. The STOP-Bang questionnaire: a narrative review on its utilization in different populations and settings. Sleep Med Rev. 2024;78:102007. doi:10.1016/j.smrv.2024.102007
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.