Back to Journals » Journal of Healthcare Leadership » Volume 18
Translation, Cultural Adaptation and Validation: Exploring the Transferability of a Health Management Competency Model to the Norwegian Healthcare
Authors Leikvoll Oskarsson IM, Ødegård A, Hoås Rødal J, Liang Z ![]()
Received 5 October 2025
Accepted for publication 31 January 2026
Published 17 February 2026 Volume 2026:18 572228
DOI https://doi.org/10.2147/JHL.S572228
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Pavani Rangachari
Ingrid Marie Leikvoll Oskarsson,1 Atle Ødegård,2,3 Jorunn Hoås Rødal,1 Zhanming Liang4
1Faculty of Business Administration and Social Sciences, Molde University College, Molde, Norway; 2Faculty of Health Sciences and Social Care, Molde University College, Molde, Norway; 3Faculty of Social Science and History, Volda University College, Volda, Norway; 4College of Business, Law and Governance, James Cook University, Townsville, Queensland, Australia
Correspondence: Ingrid Marie Leikvoll Oskarsson, Faculty of Business Administration and Social Sciences, Molde University College, Molde, NO-6402, Norway, Email [email protected]
Purpose: The healthcare sector faces complex challenges that demand a highly competent management workforce. Although considerable efforts have been made to develop management competency frameworks that provide lists of core competencies for health managers, few frameworks have undergone rigorous validity and reliability testing. The present study aimed to translate and culturally adapt the Management Competency Assessment Partnership (MCAP) tool for use in the Norwegian healthcare context and to evaluate its psychometric properties.
Methods: An eleven-step translation and cultural adaptation procedure was developed in accordance with established guidelines. A pilot study was conducted using the adapted MCAP tool with 53 healthcare managers in Norway. The resulting test scores were analyzed using inter-item correlations and exploratory factor analysis to assess the construct validity and reliability.
Results: The comprehensive translation and cross-cultural adaptation procedure contributed to the Norwegian version retained strong fidelity to the original tool. Preliminary findings demonstrated acceptable reliability and supported the construct validity of the MCAP tool test scores within the Norwegian healthcare context.
Conclusion: A rigorous translation and cross-cultural adaptation process is essential to preserve conceptual integrity when implementing assessment instruments across contexts. The preliminary findings of this study adds to previous cross-contextual validation studies using the MCAP tool, further supporting its utility as a representative framework for assessing health management competencies.
Keywords: translation, cultural adaptation, competencies, healthcare, management, leadership
Introduction
Healthcare managers (HCM) play a pivotal role in ensuring that healthcare services are delivered efficiently, cost-effectively, and at a high level of quality.1 Contemporary healthcare organizations are undergoing continuous transformation2,3 and face a broad range of persistent and emerging challenges that managers at all levels must address. These include chronic workforce shortages,2,4 skills gaps arising from rapid medical and technological advances,5 a growing need for interprofessional collaboration,6,7 rising costs and resource constraints,8 an increasing prevalence of chronic and complex conditions,2,9 expanding service demands from both frail older adults and younger populations, and persistent tension between clinical autonomy and organizational performance imperatives.10
Healthcare organizations are often conceptualized as complex adaptive systems, characterized by diverse structures, extensive cross-sectoral linkages, and a coexistence of centralized governance with substantial professional autonomy.10 This complexity, coupled with the challenges described above, renders healthcare organizations particularly demanding to manage.11,12 Accordingly, it has been argued that healthcare managers must possess sophisticated and adaptable competencies to navigate and address these demands.10
Health management competency (HMC) is generally defined as the integration of knowledge, skills and attitudes needed to fulfill managerial responsibilities, as demonstrated through managerial practice.13 Competency-based approaches can support recruitment and selection, inform targeted education and professional development initiatives, and strengthen long-term organizational sustainability.14 Consequently, healthcare organizations and researchers have invested considerable effort in producing competency frameworks to guide management development.15 However, while the importance of competent HCMs is widely recognized, empirical evidence specifying core competencies and adequate levels of performance remains limited.1
A range of models have been developed to assess health management competencies across managerial levels, sectors, organizations, or professional groups. General frameworks include the National Center for Healthcare Leadership competency model in the United States (CDC-US) and the UK National Health Services Medical Leadership Competency Framework (MLCF), both of which have been applied beyond their countries of origin.16,17 More specialized frameworks target specific managerial groups, such as first-line nurse managers,18 nurse managers in primary care19,20 and hospital settings,21 physician managers at senior level,19,22 or across multiple managerial levels.23 Still, relatively few instruments have been rigorously tested across contexts to establish psychometric properties such as validity and reliability,15 and the reporting of translation, cross-cultural adaptation and evaluation of psychometric properties of a health management competency assessment tool remains absent.
Without such evaluation, the usefulness of competency frameworks as assessment tools for identifying competency strengths and gaps among health managers remains uncertain. Recent reviews highlight the Management Competency Assessment Partnership (MCAP) as the only health management competency assessment instrument with robust cross-contextual evaluation to date.14,15 In their systematic review, Kakemam et al found that competencies and behavioral indicators reported across studies were largely consistent with those embedded in MCAP, and recommended the MCAP Tool – originally developed24 and subsequently tested in the Australian healthcare system1,25 – as a candidate framework for assessing health management competencies across settings.14
The MCAP Tool is the result of over a decade of systematic research and development.24–26 It comprises six core competencies operationalized through 82 behavioral items, providing a structured and empirically grounded framework for assessing health management competency. The tool has been tested and verified in diverse healthcare contexts, including Australia,13,26 Iran,15,27 Tanzania,28 India,29 China,30,31 and Nepal,32 and has also been explored in other sector such as veterinary care.33 Collectively, these studies suggest cross-contextual robustness, while also underscoring the importance of local cultural adaptation and psychometric evaluation prior to implementation in new settings.
Adopting and adapting a rigorously tested instrument such as MCAP can be advantageous. Identifying and operationalizing core competencies is resource-intensive, requiring substantial time, funding, and expertise.34,35 Translation, cultural adaptation, and psychometric testing of an established tool may conserve resources while enabling comparative research and shared learning across contexts.34,36 When a construct has been theoretically defined and empirically tested with reliability and validity assessments, adopting and adapting an established instrument is often preferable to developing a new model from scratch.37 This study therefore aims to contribute to the literature by providing a description of translation and cross-cultural adaption of the MCAP instrument and conduct preliminary assessments of its psychometric properties.
Study Aim
The aim of this study was to translate and cross-culturally adapt the MCAP health management competency tool for use among healthcare managers in Norway, and to conduct a preliminary evaluation of its measurement properties in this context. Specifically, the objectives were (1) Translate the MCAP questionnaire into Norwegian and culturally adapt it while preserving conceptual equivalence; (2) Assess the relevance and interpretability of the MCAP’s six core competencies and behavioral indicators for Norwegian healthcare managers; and (3) explore preliminary evidence related to construct validity and internal consistency in the Norwegian context, including identifying potential items or domains that may require contextual refinement prior to broader application.
The Norwegian Healthcare Context
Norway’s healthcare system differs from the Australia context in which MCAP was originally developed and most extensively tested. Norway provides universal coverage through a predominantly publicly owned, tax-funded system with relatively limited private provision. Services are organized across municipal primary care and publicly governed specialist services (hospitals). Because management roles, governance arrangements, and professional autonomy can vary across health system designs, the MCAP Tool requires translation, cultural adaptation, and psychometric evaluation before it can be applied full scale as a competency assessment instrument in Norway. Few validated tools exist for assessing management competencies in Scandinavian healthcare systems.
Materials and Methods
Study Design and Sample
This cross-sectional study followed established guidelines for translation and cross-cultural adaptation38 and adhered to the Consensus-based Standards for the Selection of Health Measurement Instruments (COSMIN) criteria.39 The study proceeded in two stages.
First, a translating and cross-culturally adapting process for the MCAP Tool was developed. Second, the Norwegian version of the MCAP questionnaire was pilot tested among Norwegian healthcare managers to explore preliminary psychometric properties, including aspects of validity, reliability, and factor structure, as well as to identify items requiring refinements prior to a large-scale validation.
The MCAP Tool used in this study consists of 6 core competencies (C) with 80 associated behavioral items (Appendix 1). Each item is assessed using two Likert scales: a five-point importance scale, and a seven-point MCAP competency assessment descriptive scale.1,25 Detailed descriptions of these scales are also provided in Appendix 1.
This study used a snowball sampling strategy to increase the response ratio, with the rationale that receiving the survey from one’s own manager would increase the possibility that the lower-level managers would response to the online survey. To recruit participants for the pilot, primary and specialist healthcare services within one Norwegian county were invited to participate in an online survey. This county was selected because of its contextual similarities in healthcare services and practical accessibility for recruitment, follow-up interviews, and continued adaptation of the MCAP Tool. Participants were recruited between August and November 2023. An invitation was sent by Email to directors of municipal healthcare services (n = 26) and hospital clinics (n = 6) in the selected county. Directors who did not respond were subsequently contacted by phone by the lead researcher.
The clinic managers at five hospital clinics and directors of municipal health care in sixteen municipalities agreed to participate. Data collection took place from November 2023 to February 2024. Directors and clinic managers who agreed to participate received detailed study information and a link to the online MCAP questionnaire, which they distributed to healthcare managers within their departments. Implied consent was obtained on the first page of the questionnaire.
Translation and Cultural Adaptation
Because rigorous translation and cultural adaptation are necessary for maintaining conceptual integrity and ensuring high-quality measurement,40 this study designed a process guided by established recommendations.38,41 Although no single “gold standard” exists,40 the procedure, that was initiated in August 2022, followed a three phase, 11-step process (Figure 1).
 |
Figure 1 Process of translating, culturally adapting and conducting preliminary testing of the Management Competencies Assessment Partnership (MCAP) from the Australian to the Norwegian context and language. |
Phase 1: Preparation, Forward Translation, and Back-Translation
The MCAP originator was contacted to request permission and establish collaboration for translation, cultural adaptation, and testing. Several meetings were held to clarify concepts and ensure fidelity to the original framework. The 80-item MCAP questionnaire was then translated as follows:
Forward translation was performed independently by an experienced translator (T1) fluent in English and familiar with HR and management terminology but not with the competency framework, and the lead researcher (T2), who was familiar with MCAP and healthcare management. Then the two translators compared their version and agreed on a single reconciled draft. A third professional translator (T3), unaware of the tool’s content, carried out a conceptual back-translation, instructed to focus on meaning rather than the literal equivalence.38
Phase 2: Comparison, Revision and Harmonization
The back-translated version was reviewed jointly by the MCAP originator and the lead researcher. Conceptual discrepancies were identified and resolved through iterative revisions and consultations with the translators. Although the initial back-translation was more literal than conceptual, repeated cycles of review ensured that conceptual equivalence and intended meaning were maintained.
Phase 3: Cognitive Debriefing and Finalization
To assess face and content validity, four healthcare managers from the target population and one professional completed the translated questionnaire and provided detailed feedback.37 Participants received both an electronic and a Word copy to facilitate annotation. After 8–14 days, in-depth interviews, lasting 60–120 minutes, were conducted to evaluate clarity and comprehensibility of the language; cultural relevance and scope of the content; and accuracy of items in reflecting the competencies of Norwegian healthcare managers.
A senior colleague with extensive experience in survey and health services research, but independent of the project, joined the final review to ensure methodological rigor. Based on feedback, wording was refined to improve fluency and accessibility, and all changes were re-translated into English with detailed justifications for approval by the MCAP originator. Several rounds of communication ensured agreement on the final Norwegian version.
The finalized questionnaire was imported into an electronic survey platform, proofread by a health services research group, and then distributed for pilot testing in the study population.
Pilot Testing for Validation Assessment
Procedure and Data Analysis
Participants completed the Norwegian version of the MCAP online survey. The dataset was first exported to Microsoft Excel for data cleaning (eg, checking for missing or erroneous values) and then imported into IBM SPSS Statistics (v. 29.0) for analysis. The aim was to examine whether the data collected followed the theoretically expected pattern,42 thereby providing preliminary evidence of the construct validity of the MCAP model in the Norwegian context.
Factor analysis is well-suited technique to exploring the underlying structure of multivariate data.43 In validating scores from measurement models, confirmatory factor analysis (CFA) is particularly recommended.37 Factor analysis groups variables based on shared variance derived from the correlation matrix, with items expected to load strongly on the latent factor they represent.44 However, the appropriateness of factor analysis depends on factors such as sample size and inter-item relationships,43,44 and statistical validity is a prerequisite for construct validity.45 The pilot sample (n = 53) was considered insufficient for a full CFA of the complete MCAP instrument with stable parameter estimation and adequate power. Accordingly, consistent with a pilot validation phase, the analytic objective was to generate preliminary evidence about internal structure and reliability, identify potentially problematic items, and inform refinement and future testing in a larger, adequately powered sample.46
There is little guidance in the literature regarding appropriate sample size for pilot studies,47 varying from approximately 10 participants47 to 10% of the final study size48 or between 10 and 40 participants.47 Thabane et al suggest that the sampling should be based on the same inclusion and exclusion criteria as the full-scale study, and states that “a pilot study should be large enough to provide useful information about the aspects that are being assessed for feasibility”.46 With regard to factor analysis, there are a wide range of recommendations regarding sample size. Cattell49 recommends a N:p ratio of between 3 and 6 respondents per variable measured, while Everitt50 states that the N:p ratio should be no lower than 10:1, which is supported by more recent other authors.44,51 In this study, the sample size is considered too small to proceed a full scale CFA, and an alternative procedure adequate to meet the objectives of this study was therefore followed.
Previous research indicates that inter-item correlation matrices can provide comparable insights into dimensionality, such as, for example, a principal component analysis or factor analysis.52 Item-level analysis further supports identification of items that do not align well with their intended domain. Splitting the scale is another strategy to improve items-to-respond ratio, or the sample size, N, to the number of variables being analyzed, r. Analyzing each of the six competency subscales separately, allows researchers to examine whether correlations within a domain are stronger than those between domains, which provides evidence for internal validity.53 This step also facilitates the detection of items that may require revision or removal.37
Given these considerations, analyses were selected to align with the study aims and the constraints of a small sample. Inter-item and item-total correlations (using Pearson’s r) were used to evaluate within-domain coherence and to flag items that did not align well with their intended competency domain. Exploratory factor analysis (EFA) was then used as a complementary approach to explore the dimensionality of each domain and assess whether item clustering was broadly consistent with the intended domain structure. To optimize the N:p ratio and support interpretable domain-level assessment, the MCAP instrument was divided into six subscales. The N:p ratio did not meet the recommended 10:1 ratio but improved the ratio ranging from 5,88:1 (C6) to 3,12:1 (C2 and C4) and was considered sufficient for the purpose of this pilot study as the aim of the current study was not to provide evidence of statistical generalization. Inter-item correlations were calculated within each subscale to assess internal structure and coherence, and to summarize within-domain consistency. Values were interpreted with reference to recommendations for relatively narrow constructs,53 higher average correlations indicating stronger within-domain consistency.54 EFA was then conducted on each subscale, and findings were interpreted alongside the inter-item correlations for theoretical assessment.
Cronbach’s Alpha was calculated for each subscale to evaluate internal consistency,55 with a α ≥ 0.80 set as the benchmark for acceptable reliability.56 This coefficient assumes that all items within a subscale measure the same underlying construct.57 Item-total correlations and inter-item correlations were further examined to evaluate the strength and direction of associations both within and across subscales. Following Clark and Watson,53 an average inter-item correlation of > 0.50 was considered desirable, reflecting the MCAP’s conceptualization as a narrow construct. Corrected item-total correlations, inter-item correlation patterns, and “alpha if item deleted” statistics were examined to identify items that weakened domain coherence (eg, very low corrected item-total correlations, negative/near-zero inter-item correlations, or material increases in alpha when deleted). Where items were provisionally flagged for moderation (move or remove), alpha was recalculated after removal or addition of items to quantify the impact on subscale reliability. Any modifications were treated as preliminary and interpreted alongside conceptual relevance, with the primary intent of guiding refinement before larger-scale validation.
Missing data were examined at the item response level before analysis. For correlation analyses, pairwise deletion was applied to retain available information for each item pair. For EFA and Cronbach’s alpha, listwise deletion was applied within each domain (ie, complete cases per subscale) to ensure a consistent covariance matrix for estimation. Effective sample sizes for domain-specific analyses were recorded and considered in interpretation.
Ethical Considerations
The study was reviewed by the Norwegian Agency for Shared Services in Education and Research and deemed compliant with national ethical guidelines (reference number 384281).
Approval to conduct research in specialist healthcare was included in the application to the Norwegian Data Access Committee (reference number 2023/5353).
Results
A total of 53 healthcare managers from three management levels from specialized (N=20) and primary healthcare (N=33) completed the survey. Overall, the response patterns were plausible and consistent with the study’s aims, and the results are supported by a rigorous translation and adaptation process and an analytic strategy appropriate for pilot-scale psychometric exploration. However, because n = 53 limits statistical power and stable estimation for confirmatory analysis such as full-scale CFA, the findings should be interpreted as preliminary, exploratory evidence intended to inform refinement and guide future validation in larger samples.
Over 90% of respondents rated all competencies as “important” or “very important”. Consequently, subsequent analysis used the seven-point Likert scale measuring respondent’s competency levels, which demonstrated greater response variability and analytical value.
Translation and Cultural Adaptation Process
The translation and cultural adaptation process was completed as planned, with no major deviations from the predefined protocol. Informants participating in the harmonization and preliminary testing confirmed that the Norwegian MCAP Tool was both understandable and relevant to Norwegian healthcare management, indicating face and content validity. Feedback primarily concerned cumbersome wording, which was addressed through iterative revisions in collaboration with fellow researchers and the MCAP originator. The main procedural challenge arose from the blinded back-translation step, which ultimately was judged to be more obstructive than beneficial for ensuring conceptual equivalence. Despite this, the final Norwegian version of MCAP thus retained conceptual fidelity to the original instrument while achieving linguistic and cultural appropriateness.
Pilot Testing
Sampling Adequacy and Factorability
To assess the suitability of the data for factor analysis, Kaiser-Meyer-Olkin (KMO) statistics and Bartlett’s test of Sphericity were conducted for each of the six subscales (Table 1). KMO values were high across subscales, and Bartlett’s tests were statistically significant, indicating that correlation matrices were factorable and supporting the use of domain-specific exploratory analyses.
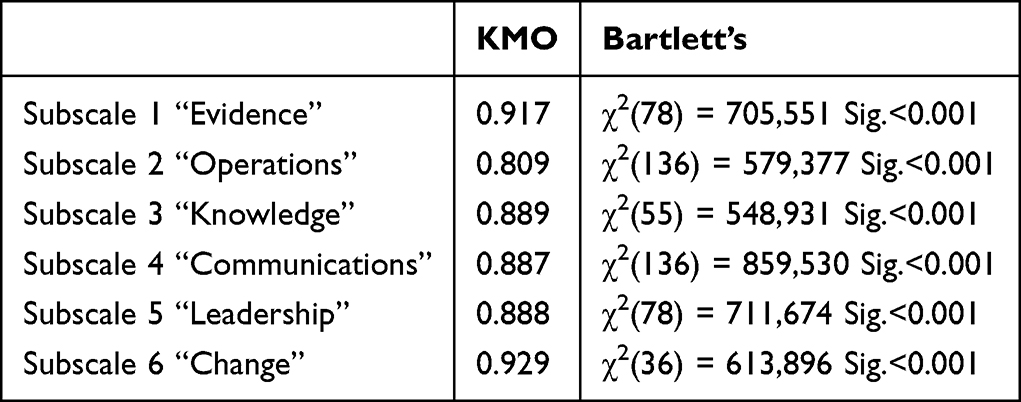 |
Table 1 Kaiser-Meyer-Olkin and Bartlett’s Test of Sphericity Results within Subscale |
Inter-Item Correlations
Each subscale was labeled subscale one through six (C1-C6). Prior to item-scale analyses, two items from Subscale 2 (C2.1 and C2.2) were excluded due to high rates of missing responses (16 and 10 cases, respectively), which reduced their interpretability in this pilot dataset. Across the remaining 78 items (3080 pairwise correlations), 96.14% were statistically significant at p <0.01 level, 2.73% at p <0.05, and 1.14% were non-significant. All within-domain correlations were statistically significant at p <0.01 level. Item-total correlation scores demonstrated stronger within-subscale than between-subscale correlations, with one exception. Subscale 2 (C2) showed a slightly higher, but non-significant, correlation with Subscale 6 (C6). Item-total correlations within and between subscales are presented in Table 2. Complete correlation matrixes are provided in Appendix II.
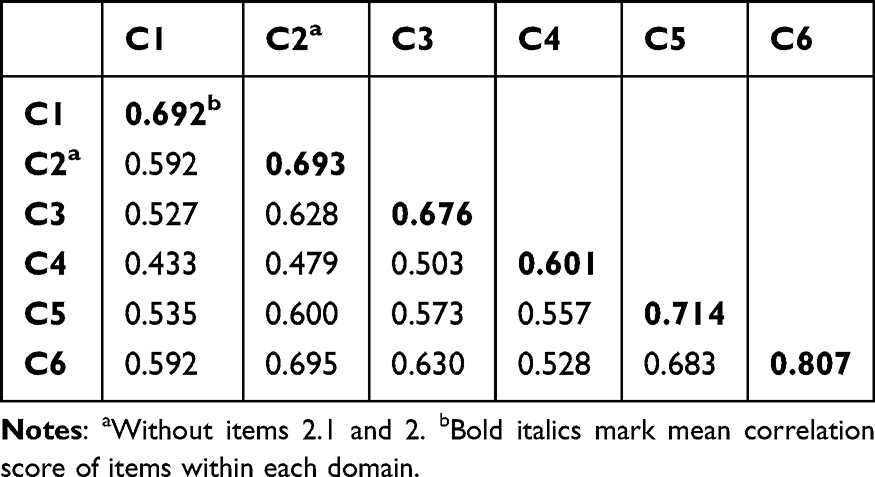 |
Table 2 Item-Total Correlation Scores for Each Subscale Internal and Between Domains |
All six subscales met the predefined criterion of an average inter-item correlation >0.50,53 indicating strong within-domain coherence in this pilot sample. Given the small sample size, these correlation-based findings are interpreted as exploratory indicators of internal structure.
Items Flagged for Theoretical Review
A closer inspection of inter-item correlations indicated that some items correlated more strongly with items outside their assigned subscale (Table 3). These items were flagged for theoretical review to assess whether cross-correlations reflected conceptual overlap, translation nuances, or potential domain misalignment.
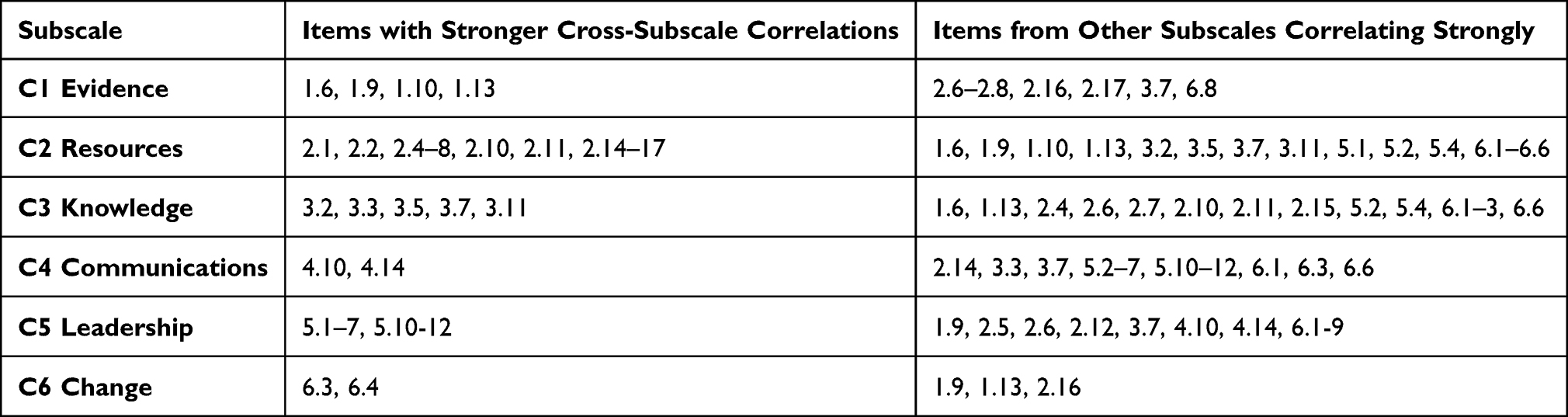 |
Table 3 Items Identified for Theoretical Evaluation Based on Inter-Item Correlations |
Overall, cross-subscale correlations were most frequent for items in C2 (Resources) and tended to overlap with C6 (Change) and, to a lesser extent, C4 (Communications), suggesting expected conceptual adjacency between operational management, performance improvement/change, and feedback/relationship practices.
Subscale-Specific Analysis
Because of the pilot sample size (n = 53) limits full-model confirmatory testing, as previously mentioned, EFA were conducted within each subscale and interpreted alongside correlation patterns to evaluate whether results were broadly consistent with the intended domain structure and to identify items needing refinement.
Subscale 1 – Evidence-Informed Decision Making (C1)
Seven cross-correlating items were reviewed; none warranted reassignment. However, item C1.13 (“Commit to ongoing personal and professional development”) showed strong cross-loadings and reflected a general personal attribute rather than a discrete competency. It was therefore excluded from further analysis.
Subscale 2 – Operations, Administration and Resource Management (C2)
Thirteen items showed strong correlations with other subscales. After theoretical evaluation, three items were reassigned. C2.14 (“Recognize and develop the performance of others by providing timely and appropriate feedback”) was reassigned to C4 (Communication). C2.15 (“Contribute to continuous improvement of organizational processes, including quality and safety”) and C2.16 (“Use performance measures and industry benchmarks to inform continuous performance improvement”) were reassigned to C6 (Change).
Factor analysis of subscale 2 initially yielded a four-factor solution; after removing C2.1, C2.2, C2.14, C2.15 and C2.16, the model stabilized to a one-factor solution with improved conceptual fit, and a new composite variable was computed.
Subscale 3: Demonstrated Knowledge of the Healthcare Environment and the Organization (C3)
Despite some strong cross-correlations, only item C3.7 (“Apply quality indices and benchmarks to identify opportunities, set performance standards, and improve quality”) was removed for disrupting the correlation matrix due to cross-loadings. A revised composite variable was computed.
Subscale 4: Interpersonal Communication Qualities and Relationship Management (C4)
Initially, C4 produced a two-factor solution. Incorporating C2.14, reassigned from C2, simplified the structure to a one-factor model with strong internal consistency. A new composite variable was computed.
Subscale 5: Leading People and Organization (C5)
C5 exhibited high internal consistency with mean inter-item correlation of .714. Despite some cross-subscale correlations, no items required reassignment or removal.
Subscale 6: Enabling and Managing Change (C6)
C6 showed the strongest internal consistency with a mean inter-item correlation of .807. Two items reassigned from C2 (C2.15 and C2.16) fit conceptually and statistically, and their inclusion did not alter the factor structure. The final composite variable included these items.
Summary of Pilot Refinements and Interpretation
Across subscale analysis, C1.13, C2.1, C2.2 and C3.7 were excluded from further analyses, while C2.14 was reassigned to C4, C2.15 and C2.16 were reassigned to C6. In this pilot dataset, these adjustments improved domain coherence and interpretability and supported more stable, predominantly unidimensional solutions within several subscales. Results of factor analyses (including scree plots and variance explained) are provided in Appendix III.
Discussion
Translation and Cultural Adaptation to Maintain Conceptual and Contextual Integrity
The present study examined the applicability, translation, and cultural adaptation of the MCAP health management competency tool within the Norwegian healthcare context. A rigorous, guideline-informed procedure was followed.38,41 Although time-consuming, systematic approaches are essential for ensuring translation quality and safeguarding the conceptual integrity of the source instrument.40 However, given the pilot sample size (n = 53) and the exploratory analytic approach applied in the psychometric assessment, the findings should be interpreted as preliminary evidence intended to guide refinement and inform larger-scale confirmatory validation studies.
To situate the translation approach within current practice, a Medline search (2010–2024) on translation and cultural adaptation of questionnaires was undertaken as a rapid scan of commonly used methodological approaches. Of 249 records, 40 papers from 2022 to 2024 were reviewed to examine contemporary approaches. Among 37 studies citing formal guidelines, 10 followed Beaton et al;58 others applied frameworks by Wild et al,38 Sousa and Rojjanasrirat,59 Brislin,60,61 WHO (1998),62 Guillemin et al,63 Yasir,64 or combinations thereof. Across these approaches, there are clear commonalities, including the use of two or more independent translators, forward and back-translation, and the synthesis of the different versions. While the present study developed a procedure based on Wild et al, this rapid scan did not indicate severe limitations in the overall approach used here. This scan was intended to contextualize the selected procedure rather than function as a systematic review.
The present findings also illustrate both the value and the limitations of established procedures for translation and cultural adaptation of measurement instruments. A structured approach supported conceptual fidelity and transparency, but it also exposed inherent tensions in how recommended steps function in practice. A literal back-translation, while recommended in many guidelines, proved too rigid in this study, yielding overly literal Norwegian phrasing and semantic shifts that risked obscuring the intended managerial concepts.34 This experience reinforces critiques that formal guidelines, although widely endorsed, cannot by themselves guarantee conceptual equivalence when constructs are contextually embedded and language-specific meanings diverge.40,58
By contrast, an iterative process involving the MCAP originator and subject-matter experts allowed meaning to be negotiated, resulting in a final version that balanced semantic accuracy with contextual resonance. This suggests that translation quality depends not only on adherence to formal steps, but also on collaborative interpretation, and one might suggest that it is the thoroughness and rigorous effort that provide quality rather than formal steps. At the same time, reliance on expert judgement may reduce replicability and introduce subjective bias. Cross-cultural validation therefore requires a dual emphasis: preserving theoretical constructs while allowing flexible, context-sensitive decisions when literal translation is counterproductive.
Decisions not to add or remove items further highlight this tension. Retaining the original structure safeguarded the MCAP Tool’s theoretical coherence and comparability across countries, supporting international benchmarking and shared learning. However, conservative retention may also limit the ability to capture uniquely Norwegian expressions of leadership and management practice, including emphasis on egalitarian decision-making and co-production. The trade-off between cross-context comparability and local specificity remains a recurring challenge in global health workforce assessment.
Rather than adding or removing content at the translation stage, cultural adaptation emphasized linguistic refinement to ensure clarity and functional equivalence. For example, the item “Seek appropriate evidence from multiple organizational sources to guide the identification of solutions” was simplified to “Locate and apply knowledge within own organization to reach good solutions”, reflecting both the Norwegian use of the term evidence and the preference to shorter formulations. Similarly, distinctions in English between management, leadership, administration and governance, are not mirrored in Norwegian where the terms leader/leadership covers the broader set of managerial responsibilities. Hence, English distinctions between manager/management and leader/leadership were addressed through functional equivalence using the Norwegian terms of leader/leadership,65 which also created minor awkwardness when leadership appears as a core management competency. Further, expressions such as “drive organizational change” were reformulated to align with Norwegian norms of shared leadership while preserving the intended meaning. Cognitive interviews with representatives of the target population, combined with expert review by researchers familiar with Norwegian healthcare, suggested that the translated items were generally clear, contextually appropriate, and theoretically coherent.37 Together, these procedures provide support for the adapted instrument’s conceptual and contextual integrity.
Relevance and Construct Validity: Theoretical Robustness Amid Contextual Differences
Despite structural and cultural differences between Norwegian and Australian health systems, the MCAP framework showed substantial contextual resonance in this pilot sample. Exploratory factor analyses conducted within domains largely reproduced the original six-domain structure, suggesting that MCAP’s core competency areas may be meaningful across national contexts. However, because the analyses were exploratory and the sample-size limits full-model confirmatory testing, these findings should be interpreted as initial support rather than definitive evidence of the Norwegian tool’s structure.
Nonetheless, some domain-specific refinements were necessary for this sample. In summary, items C1.13, C2.1, C2.2 and C3.7 were excluded, while C2.14 was reassigned to C4, C2.15 and C2.16 were reassigned to C6. These modifications are best viewed as provisional refinements derived from pilot-scale evidence and theoretical review, to be re-evaluated in subsequent confirmatory studies. Subscale 2 (C2: “Resources”) required the most extensive modification. Items related to detailed workforce administration and balancing organizational and staff needs were frequently marked as not relevant by the participants, consistent with Norwegian managerial role distributions where such tasks may be located at other administrative levels. Moreover, items related to performance improvement and feedback aligned more closely with C4 (Communication) and C6 (Change) in this sample which may reflect Norwegian expectations of participatory leadership and continuous improvement as embedded in collaborative change processes. These findings suggest that while MCAP may capture universal managerial competencies, its behavioral indicators can still reflect the institutional arrangements and management philosophies of the system in which it originated.
The observed cross-loadings across domains also invite theoretical reflection. Some may reflect genuine overlaps in managerial practice, where competencies such as communication, leadership, and change management are interdependent rather than discrete. This raises the question of whether striving for strict one-domain purity might oversimplify the complex, integrative nature of healthcare management. Alternatively, cross-loadings could be partly statistical, influenced by a moderate sample size and ceiling effects from consistently high importance ratings. Larger studies using more diverse samples could clarify whether these overlaps are conceptual or methodological.
Overall, the MCAP framework was largely upheld in this Norwegian pilot. Considering the substantial contextual differences between the Australian and Norwegian healthcare systems, the findings provide preliminary support for the transferability of MCAP and initial evidence consistent with construct validity of the adapted MCAP tool in Norway, while also identifying specific indicators that may benefit from contextual refinement.
Psychometric Properties and Construct Validity of MCAP
The Norwegian MCAP version demonstrated promising psychometric patterns in this pilot sample. KMO values exceeded .80 and Bartlett’s tests were statistically significant (p < 0.001), supporting the factorability of the domain correlation matrices and the appropriateness of exploratory analyses. Cronbach’s alpha values above .90 indicated high internal consistency, although very high alpha values may also reflect redundancy and should be interpreted alongside item-level patterns.53
The observed alignment between empirical patterns and the theoretical structure provides initial support for construct validity, understood as the accumulation of evidence that instrument scores reflect intended theoretical constructs,66,67 pending confirmatory testing in larger samples. Content and face validity were reinforced through cognitive interviews, pre-testing, and expert review, suggesting that Norwegian managers found the items comprehensible and relevant. Taken together, these results suggest that MCAP can likely be applied in Norway without major structural changes, while allowing for targeted refinement of specific behavioral indicators prior to broader implementation and confirmatory testing.
Broader Implications and Conceptual Considerations
The findings underscore both the potential and the limits of a global competency framework. A key advantage is the opportunity for international benchmarking and shared professional development, enabling health systems to compare management competencies on a common basis. At the same time, the necessity to reassign or remove certain items reveals that even well-evaluated and tested global tools remain influenced by local governance models, managerial role distributions, and linguistic norms.
If validated in larger Norwegian samples, a competency assessment tool such as MCAP could support several applied functions. First, it could inform needs-based management development by identifying domain-specific strengths and gaps among managers across municipal and specialist services, thereby enabling more targeted training initiatives. Second, competency profiles could complement recruitment, onboarding, and succession planning by clarifying expectations for management roles and providing a structured basis for feedback and professional development conversations. Finally, aggregated competency data could support organizations and policymakers monitor system-wide capability needs (eg, change management, quality improvement, communication) and align management development investments with strategic priorities in Norwegian healthcare.
Norway illustrates the broader conceptual challenge of applying standardized tools across different systems. Norwegian services are highly decentralized within a publicly funded and predominantly publicly owned system and emphasize municipal autonomy and collaborative governance. These features may shape behavioral expressions of leadership and management differently than those presupposed in the Australian model. As Beaton et al caution,58 striving for equivalence solely at the level of content can obscure that the same task may be approached differently in a new cultural context. Sociocultural characteristics, such as collective decision-making, high professional autonomy, and consensus-oriented leadership, may shape how management competencies are understood and enacted. For example, competencies related to “driving organizational change” or “exercising authority” might be interpreted less as top-down directives and more as facilitation of shared processes and interprofessional dialogue. If such nuances are ignored, the use of competency frameworks risks promoting formal compliance without fostering the substantive professional development they are intended to support. Recognizing and integrating these conceptual specificities is therefore essential to ensure that competency assessments like MCAP are not only psychometrically sound but also meaningful, actionable, and culturally responsive.
Beyond the Norwegian context, this study contributes methodologically to international competency model validation by demonstrating a transparent approach to translation, cognitive debriefing, and domain-focused pilot psychometric testing when sample sizes are insufficient for full-model confirmatory analyses. The results should therefore be interpreted primarily as evidence of methodological transferability showing how models such as MCAP can be systematically adapted and scrutinized in a new health system, rather than as outcome generalization. Larger Nordic studies, including confirmatory analyses and assessments of measurement invariance, are needed to evaluate structural stability and cross-country comparability.
Methodological Considerations
Interpretations of these results should consider several limitations. The pilot sample was relatively small and drawn from a single county, which limits generalizability and restricts statistical power for confirmatory analyses. Small samples may also inflate reliability estimates and contribute to instability in factor solutions. While high internal consistency supports coherence of the domains, very high alpha coefficients can also signal item redundancy.53 Complementary measures such as McDonald’s omega or item response theory analyses could provide a more nuanced picture of reliability and item discrimination.58 Cross-loadings and ceiling effects may partly reflect sample size constraints and homogeneity. Finally, the Medline scan of translation practices was not a systematic review and was used only to contextualize procedural choices, not to provide comprehensive methodological synthesis. Future studies across larger and more diverse Norwegian regions, and ideally across other Nordic countries, could test the stability of these preliminary findings and explore whether the observed cross-domain relationships reflect conceptual reality or sample-specific artifacts.
Conclusion
In summary, this study translated and cross-culturally adapted the MCAP tool for Norwegian healthcare managers and provides preliminary evidence relevant to its conceptual relevance and measurement performance in this context. Cognitive debriefing and expert review supported linguistic clarity and contextual fit, and pilot analyses indicated strong internal coherence within the competency domains, while also identifying a small number of items that required reassignment or exclusion to improve interpretability in this sample. These findings should be interpreted as exploratory, offering initial support consistent with construct validity and cross-context applicability rather than conclusive evidence of transferability.
Next research steps should include the Norwegian MCAP version in a larger and more diverse national sample using confirmatory approaches – and where feasible – assessment of measurement invariance across settings and managerial levels, as well as evaluating stability over time through longitudinal or test–retest designs. If supported on future validation studies, the Norwegian MCAP tool could provide a practical foundation for management education and workforce development by helping organizations and training programs identify competency needs, tailor leadership development, and support structured feedback and professional growth, while enabling comparison and shared learning across healthcare systems.
Abbreviations
MCAP, Management Competency Assessment Partnership; HCM, healthcare managers; HMC, health management competency; COSMIN, Consensus-based Standards for the Selection of Health Measurement Instruments; HR, human relation; CFA, confirmatory factor analysis; EFA, exploratory factor analysis; KMO, Kayser-Meyer-Olkin; C1 … 6, competency domain; C1.1 … C6.13, competency items; WHO, World Health Organization.
Data Sharing Statement
The dataset used in the study is available from the corresponding author: Ingrid Marie Leikvoll Oskarsson, upon reasonable request.
Acknowledgments
The authors would like to express their sincere gratitude to all researchers and professionals who contributed to this study. Special thanks to Professor Emeritus Petter Laake at the University of Oslo and Associate Professor Astrid Hoås Morin at the Norwegian University of Science and Technology for their competent and invaluable statistical advice on correlation and factor analysis. We also thank Professor Turid Aarseth at Molde University College for her meticulous proofreading and excellent advice during the finalization of the translated questionnaire. Our appreciation extends to the Health and Welfare research group at Molde University College for their thorough proofreading and constructive comments on the translated questionnaire. Finally, we are deeply grateful to all participants who generously invested their time and effort in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Howard PF, Liang Z, Leggat S, Karimi L. Validation of a management competency assessment tool for health service managers. J Health Organ Manag. 2018;32(1):113–14. doi:10.1108/JHOM-08-2017-0223
2. Figueroa CA, Harrison R, Chauhan A, Meyer L. Priorities and challenges for health leadership and workforce management globally: a rapid review. BMC Health Serv Res. 2019;19(1):239. doi:10.1186/s12913-019-4080-7
3. Florencio LC, Rivera RR, Prado-Inzerillo M. Shaping the new nurse leader generation: strategies for effective leadership development in the postpandemic era. Nurse Leader. 2024;22(4):388–392. doi:10.1016/j.mnl.2024.04.011
4. Fitzsimmons J, Loughery P, Fitzpatrick EV. Charting the course: evolving leadership competencies to navigate health care transformation. Nurse Leader. 2024;22(6):681–687. doi:10.1016/j.mnl.2024.08.004
5. Brommeyer M, Whittaker M, Mackay M, Ng F, Liang Z. Building health service management workforce capacity in the era of health informatics and digital health – a scoping review. Int J Med Inform. 2023;169:104909. doi:10.1016/j.ijmedinf.2022.104909
6. Slater CE, Keefe B, Jacobs K. Impact of the interprofessional leadership in healthcare certificate on health professionals’ collaboration and leadership abilities. J Interprof Educ Pract. 2023;32:100658. doi:10.1016/j.xjep.2023.100658
7. Tataw DB, Stokes EW. Leadership in interProfessional healthcare practice (IPHP): readiness, roles, and compentencies for healthcare managers and human resource professionals. J Interprof Educ Pract. 2023;32:100635. doi:10.1016/j.xjep.2023.100635
8. Ayeleke RO, Dunham A, North N, Wallis K. The concept of leadership in the health care sector. Leadership. 2018;83. doi:10.5772/intechopen.76133
9. Heinen M, van Oostveen C, Peters J, Vermeulen H, Huis A. An integrative review of leadership competencies and attributes in advanced nursing practice. J Adv Nurs. 2019;75(11):2378–2392. doi:10.1111/jan.14092
10. Vainieri M, Ferrè F, Giacomelli G, Nuti S. Explaining performance in health care: how and when top management competencies make the difference. Health Care Manag Rev. 2019;44(4):306–317. doi:10.1097/HMR.0000000000000164
11. Ghiasipour M, Mosadeghrad AM, Arab M, Jaafaripooyan E. Leadership challenges in health care organizations: the case of Iranian hospitals. Med J Islam Repub Iran. 2017;31(1):96. doi:10.14196/mjiri.31.96
12. Jaafaripooyan E, Mosadeghrad A, Ghiasipour M, Shaqura I. A leadership model for Iranian health-care organizations. Leadership Health Serv. 2020;33(4):461–475. doi:10.1108/LHS-05-2020-0022
13. Liang Z, Howard PF. Competencies required by senior health executives in New South Wales, 1990–1999. Aust Health Rev. 2010;34(1):52–58. doi:10.1071/AH09571
14. Kakemam E, Liang Z, Janati A, Arab-Zozani M, Mohaghegh B, Gholizadeh M. Leadership and management competencies for hospital managers: a systematic review and best-fit framework synthesis. J Healthcare Leadership. 2020;12:59–68. doi:10.2147/JHL.S265825
15. Kakemam E, Liang Z. Guidance for management competency identification and development in the health context: a systematic scoping review. BMC Health Serv Res. 2023;23(1):421. doi:10.1186/s12913-023-09404-9
16. Dikic M, Nikolic D, Todorovic J, et al. Alignment of perceived competencies and perceived job tasks among primary care managers. Healthcare. 2020;8(1):9. doi:10.3390/healthcare8010009
17. Gulati S, Weir C. Cultural competence in healthcare leadership education and development. Societies. 2022;12(2):39. doi:10.3390/soc12020039
18. Gunawan J, Aungsuroch Y, Fisher ML, Marzilli C, Hastuti E, Hastuti E. Refining core competencies of first-line nurse managers in the hospital context: a qualitative study. Int J Nurs Sci. 2023;10(4):492–502. doi:10.1016/j.ijnss.2023.08.001
19. Maulina F, Hasanbasri M, Scheele F, Busari JO. Seeking consensus on physician leadership development in rural and remote Indonesian primary care settings: a Delphi study. Leadersh Health Serv. 2025;38(1):101–135. doi:10.1108/LHS-03-2024-0027
20. de Oliveira IB, Peres AM, Almeida Bastos R, Casey M, Timmins F. Managerial competencies engaged in innovative actions in primary health care: a qualitative study of Brazilian nurses. J Nurs Manag. 2023;2023(1):8746398. doi:10.1155/2023/8746398
21. Gunawan J, Aungsuroch Y, Fisher ML, McDaniel AM, Marzilli C. Managerial competence of first-line nurse managers in public hospitals in Indonesia. J Multidisciplinary Healthc. 2020;13:1017–1025. doi:10.2147/JMDH.S269150
22. Gulati K, Madhukar V, Verma V, Singh AR, Gupta SK, Sarkar C. Medical leadership competencies: a comparative study of physicians in public and private sector hospitals in India. Int J Health Plann Manag. 2019;34(1):e947–e963. doi:10.1002/hpm.2709
23. Liou Y, Lin P, Chang Y, Liaw J. Perceived importance of competencies by nurse managers at all levels: a cross‐sectional study. J Nurs Manag. 2022;30(3):633–642. doi:10.1111/jonm.13545
24. Liang Z, Howard PF, Koh LC, Leggat S. Competency requirements for middle and senior managers in community health services. Australian J Prim Health. 2013;19(3):256–263. doi:10.1071/PY12041
25. Liang Z, Blackstock FC, Howard PF, et al. An evidence-based approach to understanding the competency development needs of the health service management workforce in Australia. BMC Health Serv Res. 2018;18(1):976. doi:10.1186/s12913-018-3760-z
26. Liang Z, Blackstock F, Howard P, et al. A health management competency framework for Australia. Aust Health Rev. 2020;44(6):958–964. doi:10.1071/AH19006
27. Liang Z, Kakemam E. Identifying competency development needs of hospital managers in Iran: a national survey. BMC Med Educ. 2025;25(1):122. doi:10.1186/s12909-025-06721-x
28. Kingu U, Ismail I, Kibusi S. Managerial competency of primary healthcare facility managers in the selected district councils in Tanzania. Manag Econ Res J. 2023;5(1):45–65. doi:10.48100/merj.2023.277
29. Sandhu MV, Liang Z. Competency assessment of project managers of a national NGO in India. J Health Manag. 2021;23(3):558–574. doi:10.1177/09720634211035248
30. Feng Z, Zhang H, Liang Z. The role of competent leaders in nursing staff empowerment: a cross-sectional study. J Healthcare Leadership. 2025;17:327–341. doi:10.2147/JHL.S527992
31. Liang Z, Howard P, Wang J, Xu M. A call for leadership and management competency development for directors of medical services—evidence from the Chinese public hospital system. Int J Environ Res Public Health. 2020;17(18):6913. doi:10.3390/ijerph17186913
32. Pokhrel P, Jones A, Crowe M, Kaphle H, Liang Z. Assessment of management competency among senior hospital managers in Nepalese public hospitals: a cross-sectional study. Asia Pacific J Health Manag. 2025;20(3). doi:10.24083/apjhm.v20i3.4889
33. Liang Z, Hompas T. Building management capability for clinical veterinary organisations—An Australian pilot study. Veterinary Record Open. 2025;12(1):e70007. doi:10.1002/vro2.70007
34. Epstein J, Santo RM, Guillemin F. A review of guidelines for cross-cultural adaptation of questionnaires could not bring out a consensus. J Clin Epidemiol. 2015;68(4):435–441. doi:10.1016/j.jclinepi.2014.11.021
35. Mokhtarinia HR, Hosseini A, Maleki-Ghahfarokhi A, Gabel CP, Zohrabi M. Cross-cultural adaptation, validity, and reliability of the Persian version of the spine functional index. Health Qual Life Outcomes. 2018;16(1):95. doi:10.1186/s12955-018-0928-5
36. Mokhtarinia HR, Hosseini ZSJ, Shokouhyan SM, Gabel CP. Translation, cultural adaptation and assessment of psychometrics properties of the extended version of the nordic musculoskeletal questionnaire (NMQ-E) in Persian language speaking people. BMC Musculoskelet Disord. 2024;25(1):89. doi:10.1186/s12891-024-07192-9
37. Lambert LS, Newman DA. Construct development and validation in three practical steps: recommendations for reviewers, editors, and authors. Organizational Res Methods. 2023;26(4):574–607. doi:10.1177/10944281221115374
38. Wild D, Grove A, Martin M, et al. Principles of good practice for the translation and cultural adaptation process for patient-reported outcomes (PRO) measures: report of the ISPOR task force for translation and cultural adaptation. Value Health. 2005;8(2):94–104. doi:10.1111/j.1524-4733.2005.04054.x
39. Mokkink LB, Terwee CB, Patrick DL, et al. The COSMIN checklist for assessing the methodological quality of studies on measurement properties of health status measurement instruments: an international Delphi study. Qual Life Res. 2010;19(4):539–549. doi:10.1007/s11136-010-9606-8
40. Acquadro C, Conway K, Hareendran A, Aaronson N; European Regulatory Issues and Quality of Life Assessment (ERIQA) Group. Literature review of methods to translate health-related quality of life questionnaires for use in multinational clinical trials. Value Health. 2008;11(3):509–521. doi:10.1111/j.1524-4733.2007.00292.x
41. Ljoså T, Jacobsen H, Granan L, Reme S. ReKS modifiserte oversettelsesmetode for spørreskjema. Frem-og-tilbake oversettelse med kulturell tilpasning og lingvistisk validering Oslo: regional Kompetansetjeneste for smerte (ReKS), Avdeling for smertebehandling, Oslo universitetssykehus (OUS). 2013.
42. Matsunaga M. How to factor-analyze your data right: do’s, don’ts, and how-to’s. Int j psychol res. 2010;3(1):97–110. doi:10.21500/20112084.854
43. Pett MA, Lackey NR, Sullivan JJ. Making Sense of Factor Analysis: The Use of Factor Analysis for Instrument Development in Health Care Research. SAGE; 2003.
44. Shrestha N. Factor analysis as a tool for survey analysis. Am J Applied Math Statistics. 2021;9(1):4–11. doi:10.12691/ajams-9-1-2
45. Lund T, Kleven TA, Kvernbekk T, Christophersen KA. Innføring i Forskningsmetodologi. Oslo: Unipub; 2002.
46. Thabane L, Ma J, Chu R, et al. A tutorial on pilot studies: the what, why and how. BMC Med Res Method. 2010;10(1):1. doi:10.1186/1471-2288-10-1
47. Hertzog MA. Considerations in determining sample size for pilot studies. Res Nurs Health. 2008;31(2):180–191. doi:10.1002/nur.20247
48. Lackey NR, Wingate AL. The pilot study: one key to research success. Kansas Nurse. 1986;61(11):6–7.
49. Cattell R. The Scientific Use of Factor Analysis in Behavioral and Life Sciences. Springer Science & Business Media; 2012. doi:10.1007/978-1-4684-2262-7
50. Everitt BS. Multivariate analysis: the need for data, and other problems. Br J Psychiatry. 1975;126(3):237–240. doi:10.1192/bjp.126.3.237
51. Pituch KA, Stevens JP. Applied Multivariate Statistics for the Social Sciences: Analyses with SAS and IBM’s SPSS. Routledge; 2015.
52. Yusuf B, Sulaiman B. Comparing local item dependency from inter-item correlation matrix and principal component analysis from factor analysis for dimensionality of multidimensional dataset. Int J Scientific Res Pub. 2020;10(7):254–264. doi:10.29322/IJSRP.10.07.2020.p10332
53. Clark LA, Watson D. Constructing validity: basic issues in objective scale development. American Psychological Association; 2016:203. doi:10.1037/14805-012.
54. Raykov T, Marcoulides GA. Introduction to Psychometric Theory.
55. Cronbach LJ. Coefficient alpha and the internal structure of tests. Psychometrika. 1951;16(3):297–334. doi:10.1007/BF02310555
56. Nunnally JC. An overview of psychological measurement. In: Wolman BB editor. Clinical Diagnosis of Mental Disorders. Springer; 1978:97–146. doi:10.1007/978-1-4684-2490-4_4
57. Peters GJY. The alpha and the omega of scale reliability and validity: why and how to abandon Cronbachâ€TM s alpha and the route towards more comprehensive assessment of scale quality. European Health Psychol. 2014;16(2):56–69.
58. Beaton DE, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine. 2000;25(24):3186–3191. doi:10.1097/00007632-200012150-00014
59. Sousa VD, Rojjanasrirat W. Translation, adaptation and validation of instruments or scales for use in cross-cultural health care research: a clear and user-friendly guideline. J Eval Clin Pract. 2011;17(2):268–274. doi:10.1111/j.1365-2753.2010.01434.x
60. Brislin RW. The wording and translation of research instruments. In: Field Methods in Cross-Cultural Research. Cross-Cultural Research and Methodology Series. Vol. 8. Sage Publications, Inc; 1986:137–164.
61. Jones PS, Lee JW, Phillips LR, Zhang XE, Jaceldo KB. An adaptation of Brislin’s translation model for cross-cultural research. Nursing Res. 2001;50(5):300. doi:10.1097/00006199-200109000-00008
62. The Whoqol Group. The world health organization quality of life assessment (WHOQOL): development and general psychometric properties1. Soc Sci Med. 1998;46(12):1569–1585. doi:10.1016/S0277-9536(98)00009-4
63. Guillemin F, Bombardier C, Beaton D. Cross-cultural adaptation of health-related quality of life measures: literature review and proposed guidelines. J Clin Epidemiol. 1993;46(12):1417–1432. doi:10.1016/0895-4356(93)90142-N
64. Yasir AS. Cross cultural adaptation & psychometric validation of instruments: step-wise. Int J Psychiat. 2016;1(1):4.
65. Herd AM, Adams-Pope BL, Bowers A, Sims B. Finding what works: leadership competencies for the changing healthcare environment. J Leadership Educ. 2016;15(4):217–233. doi:10.12806/V15/I4/C2
66. Messick S. Validity of psychological assessment: validation of inferences from persons’ responses and performances as scientific inquiry into score meaning. Am Psychologist. 1995;50(9):741–749. doi:10.1037/0003-066X.50.9.741
67. Messick S. Validity of test interpretation and use. ETS Res Report Series. 1990;1990(1):1487–1495. doi:10.1002/j.2333-8504.1990.tb01343.x
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Preventing and Mitigating Inter-Professional Conflict Among Healthcare Professionals in Nigeria
Adigwe OP, Mohammed ENA, Onavbavba G
Journal of Healthcare Leadership 2023, 15:1-9
Published Date: 6 January 2023
Spanish Translation and Cultural Adaptations of Physical Therapy Parent Educational Materials for Use in Neonatal Intensive Care
McCarty DB, Sierra-Arevalo L, Caldwell Ashur AC, White JT, Villa Torres L
Patient Preference and Adherence 2024, 18:93-100
Published Date: 12 January 2024
Exploring the Peer Leadership Network of Rehabilitation Healthcare Professionals Following Leader Development Training
Becker ES
Journal of Healthcare Leadership 2024, 16:39-52
Published Date: 25 January 2024
Change in Organizational Structure Influences Perceived Leadership in a Dutch Radiotherapy Center
Swart RR, Jacobs MJ, Van Merode F, Boersma LJ
Journal of Healthcare Leadership 2025, 17:297-314
Published Date: 5 July 2025
Healthcare Leadership in Resource-Limited Settings: Reimagining Public Hospital Governance in Somalia
Ali AS, Ahmed MM
Journal of Healthcare Leadership 2026, 18:608330
Published Date: 11 May 2026