Back to Journals » International Journal of Women's Health » Volume 17
Translation and Validation of the Edinburgh Postnatal Depression Scale for Eritrea: A Screening Tool for Postpartum Depression in Primary Health Care Facilities
Authors Gebregziabher NK ![]() , Netsereab TB
, Netsereab TB ![]() , Alazar FA, Fessaha YG, Sium AH, Ghebrehiwet NK
, Alazar FA, Fessaha YG, Sium AH, Ghebrehiwet NK
Received 2 September 2024
Accepted for publication 24 January 2025
Published 6 February 2025 Volume 2025:17 Pages 299—310
DOI https://doi.org/10.2147/IJWH.S487258
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Nahom Kiros Gebregziabher,1,2 Tesfit Brhane Netsereab,1,3 Feven Andebrhan Alazar,4 Yerusalem Gebremeskel Fessaha,4 Aman Hadish Sium,4 Nardos Kidane Ghebrehiwet4
1Department of Community Medicine, Orotta College of Medicine and Health Sciences, Asmara, Eritrea; 2Department of Epidemiology & Biostatistics, School of Public Health, Tianjin Medical University, Tianjin, People’s Republic of China; 3Department of Epidemiology and Health Statistics, Xiangya School of Public Health, Central South University, Changsha, Hunan, People’s Republic of China; 4Ministry of Health, Asmara, Eritrea
Correspondence: Nahom Kiros Gebregziabher, Department of Community Medicine, Orotta College of Medicine and Health Sciences, Asmara, Eritrea, Email [email protected]
Introduction: Postpartum depression (PPD) is a mood disorder characterized by symptoms such as changes in sleep and eating patterns, fatigue, sadness, crying, anxiety, and guilt. The Edinburgh Postnatal Depression Scale (EPDS) was developed to be used as a self-report questionnaire for English-speaking populations to screen for postnatal depression. This study aims to translate, validate, and adapt the EPDS into Eritrean settings.
Methods: This study employed a cross-sectional study design to evaluate the performance of the EPDS as a screening tool by using a sample of 380 mothers from four primary healthcare facilities. The standard Diagnostic and Statistical Manual of Mental Disorders was used as a criterion to assess depression in postpartum women.
Results: Postpartum depression was identified in 28 (7.4%) of the mothers based on the standard Diagnostic and Statistical Manual of Mental Disorders. The translated Tigrinya version EPDS has good internal consistency with Cronbach’s alpha of 0.712. The exploratory factor analysis identified three factors, confirming the EPDS’s multidimensionality. The area under the receiver operating characteristic curve was 0.87, and optimal sensitivity and specificity combination was found at 10/11 score cut-off points, 85.7% and 88%, respectively.
Conclusion: The Eritrean version of EPDS has proven to be a valid and reliable instrument for the identification of postpartum depression in clinical settings.
Plain Language Summary: Postpartum depression (PPD) is a significant concern affecting new mothers worldwide. Recognizing the need for practical screening tools tailored to specific cultural contexts, researchers set out to adapt and validate the Edinburgh Postnatal Depression Scale (EPDS).
Why was the study done?
Researchers aimed to adapt and validate the EPDS for Eritrea to provide a reliable tool for detecting PPD in mothers who recently gave birth. This is crucial as PPD is a severe condition affecting maternal and family well-being, and existing tools were not tailored for the Eritrean cultural context.
What did the researchers do and find?
The EPDS was translated into a local language and tested among new mothers in Asmara, Eritrea. Following the translation, they tested the scale’s reliability and validity by administering it to a group of new mothers in primary healthcare settings in Asmara, Eritrea. The findings were promising; the translated EPDS retained its reliability and validity, effectively identifying mothers experiencing symptoms of postpartum depression. This validation suggests the adapted EPDS is a robust tool for screening PPD in the Eritrean context.
What do these results mean?
The successful validation of the EPDS for Eritrean mothers is a significant advancement for maternal health care in Eritrea. Healthcare providers can now use this culturally and linguistically appropriate tool to screen for postpartum depression, leading to early detection and intervention. Improving screening can significantly enhance new mothers’ mental health and overall well-being, supporting healthier families and communities.
Keywords: EPDS, postpartum depression, Eritrea, validation, mental health, Tigrinya
Introduction
It is estimated that one in four individuals will experience some form of mental or behavioral disorder in their lifetime. Globally, approximately 10% of pregnant women and 13% of postpartum women experience mental disorders, primarily depression. In developing countries, these rates are higher, with 15.6% of women affected during pregnancy and 19.8% after childbirth.1 Postpartum depression (PPD), a mood disorder characterized by symptoms such as changes in sleep and eating patterns, fatigue, sadness, crying, anxiety, and guilt, is classified by the Diagnostic and Statistical Manual of Mental Disorders (DSM) as a type of depressive episode occurring within one year of childbirth.2 Although the exact cause of PPD remains unclear, factors such as hormonal changes, genetics, birth-related trauma, and socio-demographic variables are believed to play a role.3–5
Accurately measuring the burden of pregnancy-related and postpartum morbidity is essential for addressing maternal health issues and achieving the health objectives outlined in the Sustainable Development Goals. The prevalence of postpartum depression varies widely across countries.6,7 This variation is mainly due to differences in health-seeking behaviors, cultural interpretations of symptoms, and socio-economic and other context-specific factors.8,9 Despite its prevalence, postpartum depression is often unrecognized,10 posing significant challenges to efforts aimed at reducing maternal morbidity and mortality.
In Eritrea, contrary to the expected high prevalence of common mental disorders, reported incidence and prevalence are notably low at 14.5%.11 This discrepancy may be due to underreporting and under/misdiagnosis, stemming from a shortage of mental health facilities and adequately trained health professionals,11–13 particularly in primary healthcare facilities. This makes the probability of underdiagnosing cases of postpartum depression higher since the majority of pregnant mothers get maternal health services from such facilities. Hence, it is crucial to use easily administered screening tools like the Edinburgh Postnatal Depression Scale (EPDS) for early detection and treatment of mental disorders at community-level health facilities. This will facilitate the implementation of an integrated primary health care approach for mental health services, as it is cost-effective and helps to reduce the stigma associated with mental illness.
Developed in 1987 by Cox, Holden, and Sagovsky, the 10-item EPDS is a self-report questionnaire designed to screen for postnatal depression.14 The EPDS has shown high reliability and specificity in identifying depressive symptoms in postpartum women.15–17 Although initially created for English-speaking populations, the EPDS has been translated into several languages and validated in numerous cultural contexts, with each version recommending unique cut-off scores. It is essential to fine-tune the tool to local contexts as it was found to have some sociocultural factors related to its application.18,19 The variability in cut-off points highlights the need to adapt the original English version to local contexts before use. Therefore, it is recommended to establish the semantic, technical, diagnostic, and conceptual equivalence of the EPDS in screening before adopting the tool for clinical practice or research.20 According to a systematic review assessing perinatal depression in African settings, with the EPDS being the most studied scale, the limited evidence base hinders robust conclusions and effective mental health programming.21 The EPDS has yet to be translated or validated in Eritrea. This study aims to fill that gap by translating, validating, and adapting the EPDS for an Eritrean setting.
Methods
Study Design and Setting
This cross-sectional study aimed to evaluate the performance of the EPDS as a screening tool. The study was conducted in four selected health facilities across four subzones of the Maekel Region in Eritrea from January to April 2018. These facilities were categorized into two groups—rural and urban settings. Tsaeda-Christian Health Center and Seregeka Health Center represented the rural health facilities, while Semenawi Asmara Health Center and Freselam Health Station represented the urban ones. These primary healthcare facilities were chosen because they are typically the first point of contact for postpartum women, who visit for their child’s first vaccinations by six weeks postpartum. The diverse socio-economic catchment population ensured a representative sample.
Study Population, Sample Size, and Sampling Technique
The target population included recently delivered mothers within 2 to 14 weeks postpartum. Mothers visiting the selected health facilities during the data collection period and confirmed to be free from known medical and mental illnesses were randomly selected for the study.
The sample size was determined using the single population proportion formula, with a 95% Confidence Interval (CI) and a margin of error set at 5%. Assuming a 50% prevalence rate, the initial sample size was 384, adjusted to 375 using a correction factor for the actual population size (17,369). Including a 5% allowance for non-response, the final sample size was 393. This sample was proportionally allocated to the health facilities based on the number of mothers attending for child immunization. A simple random sampling technique was used to select participants by using the list of mothers in the immunization register as a sampling frame.
Data Collection Instruments
Data was collected using a structured, closed-ended questionnaire that included socio-demographic and maternity-related information. The EPDS and the DSM-5 criteria for Major Depressive Disorder (MDD) were used to assess postpartum depression.
EPDS and DSM-5 Major Depressive Disorder Diagnostic Criteria
The EPDS is a 10-item self-reporting scale assessing various depressive symptoms, with each item scored from 0 to 3, yielding a total score range of 0 to 30.14 Items cover anhedonia, self-blame, anxiety, fear, coping ability, sleep difficulties, sadness, tearfulness, and self-harm ideas.
The DSM-52, developed by the American Psychiatric Association and WHO, includes criteria for diagnosing MDD. Diagnosis requires five or more symptoms within two weeks, significantly impacting social, occupational, or other areas of functioning, excluding symptoms attributable to other medical conditions. This gold standard tool was used to validate the EPDS in this study.
Translation and Cultural Adaptation of EPDS
The EPDS was translated into Tigrinya by bilingual experts. A back translation was performed, and semantic equivalence was ensured. The Tigrinya version was administered to 20 mothers to assess its understandability, with adjustments made based on their feedback. Data from the pilot study was not included in the final analysis.
Data Collection Procedure
Participants were recruited from the Expanded Program of Immunization (EPI) clinics and interviewed privately in the selected health facilities. Socio-demographic and maternity-related data were collected, followed by a nurse administration of the Tigrinya EPDS. Finally, blinded psychiatric nurses used the DSM-5 MDD to interview mothers for postpartum depression.
Data Analysis
Data were analyzed using SPSS version 23. Descriptive statistics like frequencies and proportions were used to describe the sample characteristics. After checking for the normality of the data, mean and standard deviation or median and interquartile range were used to summarize continuous variables, and a nonparametric independent t-test (Mann–Whitney U-test) was used to compare mean EPDS scores between depressed and non-depressed groups. The internal consistency or reliability of the scale was assessed using Cronbach’s alpha. Content, face, and construct validity were evaluated, including exploratory factor analysis for structural validity. Criterion validity was determined by correlating EPDS and DSM-5 scores. Qualified professionals in psychiatry and psychology assessed the content validity of the translated EPDS to ensure it adequately reflected postpartum depression. Language experts assessed the instrument’s language and semantic validity, and the floor and ceiling effects were determined post-data collection. Face validity was investigated during questionnaire administration, which examines the tool’s meaning, intention, and acceptability to mothers. The structural construct validity of the Tigrinya-EPDS was assessed using exploratory factor analysis (EFA) with principal component analysis and Varimax rotation. Following the Kaiser-Guttman criterion, this analysis identified the dimensional structure and the number of factors to be retained based on the screen test and rotated eigenvalues greater than 1.0. Sampling adequacy was tested using the Kaiser-Meyer-Olkin (KMO) measure, and the patterned relationship of the items was confirmed with Bartlett’s test of sphericity. Criterion validity was established by calculating the correlation between EPDS scores and DSM-5 MDD criteria using Pearson’s correlation coefficient. The sensitivity and specificity of the EPDS were calculated, with ROC analysis determining its screening accuracy.
Results
Sample Characteristics
A total of 380 mothers responded to the Tigrinya version EPDS and the DSM-5 MDD diagnostic interviews, resulting in a response rate of 96.7%. The mean age of the mothers was 27.78 years (SD ±5.26), and the range was from 16 to 43 years. Table 1 presents the demographic and maternity-related characteristics of the study participants. The majority of women were aged 25–34 (60.8%), married (90.8%), and had secondary education (76.1%). Most were housewives (77.9%) and identified as Orthodox Christians (68.4%). The perceived wealth class was predominantly middle class (66.6%). In terms of maternity history, a significant portion had 2–4 pregnancies (57.4%) and delivered at term (91.8%) in health facilities (95.0%) via normal vaginal delivery (83.9%). Postpartum, the highest proportion of women were interviewed between 2 and 4 weeks (41.3%) after childbirth (Table 1).
 |
Table 1 Characteristics of the Sample |
Based on the DSM-5 criteria for Major Depressive Disorder (MDD), respondents were classified as either depressed or not depressed, with 28 mothers (7.4%) exhibiting depressive symptoms. The median EPDS score was 6.26 (SD ±4.4, CI: 5.82–6.71), with scores ranging from 0 to 21. For depressed mothers, the median EPDS score was 14 (IQR 4), while for non-depressed mothers, it was 5 (IQR 7). A Mann–Whitney U-test revealed a statistically significant difference in median EPDS scores between the two groups (U = 1246.5, z = −6.59, p < 0.0001).
Psychometric Properties of the Eritrean EPDS
Reliability
The translated Tigrinya version of the EPDS demonstrated good internal consistency, with a Cronbach’s alpha of 0.712.
Face and Content Validity
The translated EPDS was well received by the mothers, who found it an easily understood and quickly administrable interview tool. The questions were clear and relevant, with participants grasping the intention of the screening tool, thus indicating good face validity. Content validity was assessed by experts in clinical psychology and psychiatry, confirming that the EPDS adequately covered significant depression-specific symptoms. Additionally, the study showed no floor or ceiling effects, as only 7% of respondents scored the lowest possible score and none scored the highest, further supporting good content validity.
Factor Structure (Exploratory Factor Analysis)
Before conducting Exploratory Factor Analysis (EFA), the suitability of the dataset was confirmed. A Determinant score of 0.201 indicated the absence of multicollinearity, well above the threshold of 0.00001. Bartlett’s Test of Sphericity (χ2 = 601.471, df = 45, p < 0.001) confirmed the patterned relationships necessary for EFA. Sample size adequacy was supported by a KMO measure of 0.769 and the diagonal element of the Anti-Correlation matrix at 0.626, confirming the dataset’s suitability for EFA.
The orthogonally rotated values of the EFA revealed three meaningful factors. These factors were extracted using rotated eigenvalues greater than 1 and the scree plot (see Figure 1). While the elbow criterion suggests that the slope of the eigenvalues levels off after the second factor, the Kaiser criterion supports retaining the third factor as its eigenvalue is greater than 1. Given that the third factor still explains meaningful variance and may provide valuable insights aligned with the context and theoretical framework of the data, its inclusion ensures a more comprehensive representation of the underlying constructs. The first factor (F1) included items 6 (inability to cope), 7 (difficulty sleeping), 8 (sadness), 9 (crying), and 10 (thoughts of self-harm), and was named “Depression” due to the specific symptoms of depressive disorders. The second factor (F2) included items 3 (self-blame), 4 (anxiety), and 5 (panic) and was named “Anxiety.” The third factor (F3) consisted of items 1 and 2, which assessed the ability to experience pleasure and was named ‘Anhedonia.’ These factors explained 53.67% of the covariance among the variables. The model had only 3 (6%) nonredundant residuals with absolute values greater than 0.05, indicating a good fit. The factor loadings in the rotated factor matrix were reasonably desirable, with only two complex variables (items 5 and 7).
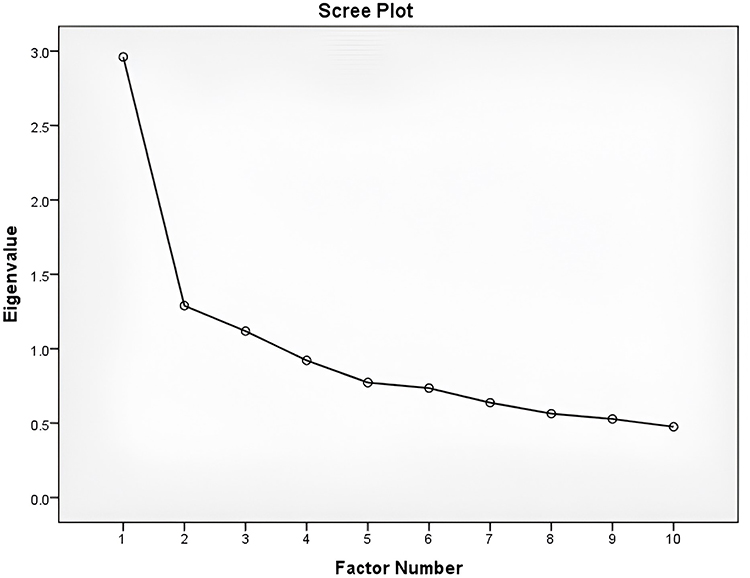 |
Figure 1 Scree plot. |
Criterion Validity
The criterion validity of the Eritrean EPDS, when evaluated against the “gold standard” DSM-5 MDD criteria, demonstrated satisfactory accuracy with a Pearson’s r of 0.497 (p < 0.001). The area under the Receiver Operating Characteristic (ROC) curve further illustrated the tool’s accuracy, which was plotted using the range of EPDS scores and the DSM-5 MDD categories (depressed and not-depressed) as the state variable. The area under the curve (AUC) was found to be 0.87 (Std. Error = 0.048, Asymp. Sig. < 0.001; CI: 0.77–0.96), indicating excellent performance in detecting postpartum depression (see Figure 2).
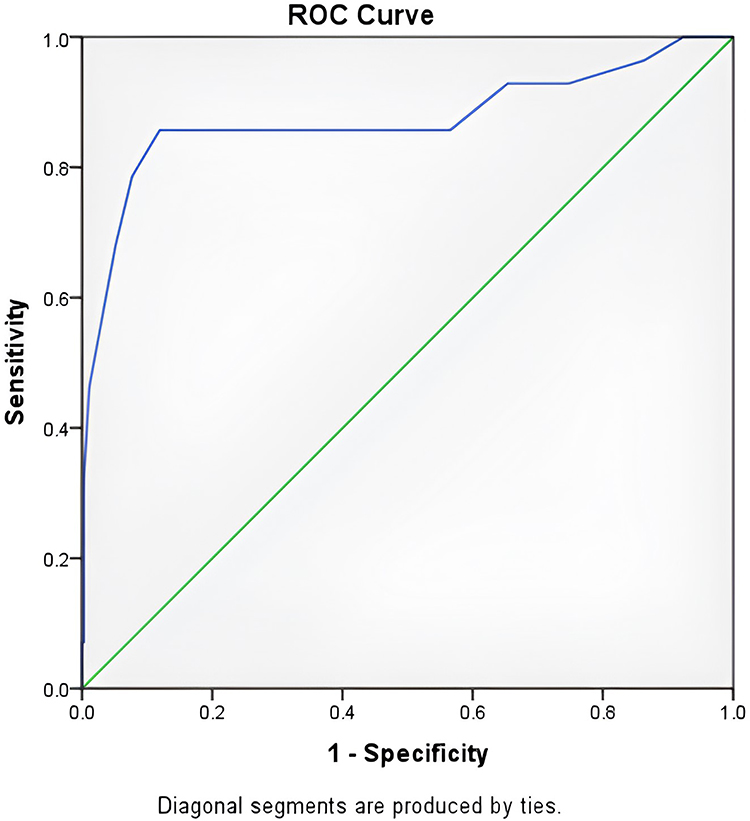 |
Figure 2 Receiver Operating Characteristics curve for the performance of EPDS (total score) against DSM-5. |
Sensitivity and Specificity
Table 2 displays the range of cut-off scores for positive EPDS screening. The optimal combination of sensitivity and specificity was identified at a score of 10/11. Using this cut-off point (11), the sensitivity was 85.7%, specificity was 88%, positive predictive value (PPV) was 36.3%, and negative predictive value (NPV) was 98.7%, as calculated from Table 3. Applying this cut-off point, 66 (17.4%) of our study participants were identified as having postpartum depression.
 |
Table 2 Sensitivity and Specificity of Eritrean EPDS |
 |
Table 3 Two-by-Two Table for the EPDS, Cut-off Score 11 |
Discussion
The primary aim of this study was to translate the Edinburgh Postnatal Depression Scale (EPDS) into Tigrinya, an Eritrean local language, and to validate it as a screening tool for postpartum depression among mothers in primary healthcare facilities. The sample characteristics indicate a diverse mix of socio-economic, demographic, and maternity-related properties, ensuring a suitable sample for a validation study. Several validation studies have used different criteria as the gold standard to validate EPDS for various reasons. In our study, we used the DSM-5 criteria for major depressive symptoms since it is the diagnostic criterion used to diagnose psychiatric conditions in the study setting.
The EPDS’s validity against DSM-5 MDD was satisfactory, as evidenced by Pearson’s correlation coefficient. The area under the ROC curve of 0.87 is excellent, indicating the overall diagnostic ability of the translated scale, with the value indicating greater classification accuracy.22 However, the current study’s finding was lower than a report in a Danish study where the AUC of EPDS against DSM-5 was found to be 0.96.23 Similar findings were reported from studies conducted in Nepal (0.98)24 and Uganda (0.84–0.97).25 A lower AUC (0.78) for postpartum was also reported in a study conducted in Portugal.26 The difference in the reported AUC across studies could be related to differences in patient characteristics and depression symptoms spectrum.27
The appropriate cut-off point for this setting was determined to be 10/11 (≥11), with a sensitivity of 85.7%, specificity of 88%, PPV of 36.3%, and NPV of 98.7%. This cutoff point was higher than that reported by a study from Ethiopia, where the optimal cutoff point was 6/7.28 A similar study conducted in Sudan recommended a slightly higher cutoff point of ≥12.29 In India, research suggests using a cut-off score of 9/10 to be used as screening depression in antenatal women.30 In line with the current study, in a Kenyan validation study, a cut-off score of ≥11 is recommended to identify postpartum depression among Kamba-speaking postnatal women, which has a sensitivity of 81.0% and a specificity of 82.6%.31 The different cutoff points recommended in different settings mainly reflect the cultural differences of the study area and the gold standard used to validate the scale since the other studies employed the International Classification of Disease (ICD-10) or Patient Health Questionnaire (PHQ-9). However, as indicated in a systematic review by Brooke Levis et al,16 a cut-off value of 11 or higher optimized sensitivity and specificity, while a cut-off value of 13 or higher, although less sensitive, provided greater specificity. As recommended,32,33 we need to pay due attention to item 10 when evaluating EPDS screening results. It was found that the prevalence of suicidal ideation was 16 times higher in women with postpartum depression than those without.34 Hence, further assessment of women who answered anything other than “no” to item 10, regardless of the total score, would be beneficial.
The internal consistency of the Eritrean EPDS, assessed by Cronbach’s alpha (0.71), was satisfactory and aligned with other validation studies.35 However, lower36 and higher37–39 alpha values have been reported elsewhere, likely due to differences in translation methodologies, which are crucial for ensuring precision and validity. In addition, factors like differences in the cultural and linguistic contexts of the populations being studied, variations in sample sizes, and the demographic characteristics of participants, such as age, socioeconomic status, and educational background, might contribute to the difference.
Ensuring the content validity of a translated scale is crucial for accurate and culturally relevant assessment of postpartum depression, leading to reliable screening and effective clinical interventions.40 In addition, high content validity allows for valid cross-cultural comparisons, supports clinical decision-making, and enhances the integrity of research findings. The content validity of the translated EPDS is considered excellent and facilitated by experts in psychology, psychiatry, and language. Mothers who participated in this study understood and answered the questions without difficulty, although item 2 required additional explanation. Therefore, the instrument’s scale was proven consistent, and its contents were valid in assessing postpartum depression.
While Cox et al suggested a unidimensional structure for the EPDS,14 this study identified a multidimensional structure consistent with several other studies.41,42 The factor analysis revealed three factors with high loadings categorized as depression, anxiety, and anhedonia. This finding was consistent across similar studies conducted in other settings like Slovak,43 China,44 England45 and Japan.46 An Iranian study showed, similar to the current research, that EPDS includes three factors, but they were categorized as euthymic mood, anxiety, and depression.47 These findings reflect the fact that depression, anxiety, and anhedonia are interrelated mental health conditions often observed together, each influencing and exacerbating the others. Research suggests that the co-occurrence of depression and anxiety can intensify anhedonia, creating a cycle where the distress from anxiety fuels depressive symptoms, which in turn enhances anhedonia.48
In this study, the factors analysis explained 53.67% of the variance compared to 87.61% in the Indian,38 64.4% in Japan49 and 58% in Qatari50 studies. This indicates that the factor model captures a substantial portion of the variability in the dataset, suggesting a robust underlying structure. These results support the validity of the EPDS as a reliable measure for assessing postnatal depression. Consistent with other studies, EPDS was administered verbally, as an interview tool rather than self-administered. This approach is essential to accommodate participants with varying literacy levels. Furthermore, such a technique enables the health worker to note the clinical presentation of the mother while interviewing her, which is essential in interpreting the results. However, the EPDS, whether self-administered or interviewer-administered, is an equally effective screening method for identifying postpartum depression.51
Limitations
The study focused on translating the EPDS into Tigrinya, the working language of Eritrea, which is the mother tongue of the largest ethnic group. However, this limits the applicability of the translated EPDS to mothers from other ethnicities who cannot speak the language. In addition, it included only mothers who attended health facilities to immunize their children. Furthermore, a self-administered EPDS might have different results since the current study was interviewer-administered.
Conclusion
In conclusion, the Eritrean adaptation of the EPDS has demonstrated both validity and reliability for identifying postpartum depression within clinical environments. A cut-off score of 11 is recommended for effective screening to ensure reliable sensitivity and specificity. Although the PPV is somewhat low, capturing any number of PPD-affected mothers is significant for both clinical and public health purposes. It is also recommended that special attention be paid to item 10 in EPDS evaluations. It is advised that relevant departments within the Ministry of Health, such as the Family and Community Health Division and the Mental Health Unit, integrate this tool into primary healthcare settings to facilitate early detection and prompt treatment of postpartum depression. Enhancing the screening program’s positive predictive value by targeting at-risk mothers during assessment is recommended.
Abbreviations
PPD, postpartum depression; EPDS, Edinburgh Postnatal Depression Scale; DSM-5, Diagnostic and Statistical Manual Fifth Edition; MDD, major depressive disorder; AUC, area under the curve; ROC, Receiver Operating Characteristic.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
This study received approval from the Research and Ethical Clearance Committees of the School of Public Health and the Asmara College of Health Sciences. The research adhered to ethical principles outlined in the Declaration of Helsinki, ensuring the protection of human subjects in medical research. During data collection, researchers thoroughly explained the study’s purpose and scope to each selected mother, obtaining written informed consent from all participants. Only volunteers were included, and participants had the right to withdraw from the study anytime. Data was collected anonymously, ensuring confidentiality by using the information solely for this research.
Acknowledgments
We would like to extend our heartfelt gratitude to all the participants who generously shared their time and experiences for this study. Your contribution is invaluable to improving maternal health care in Eritrea. We also wish to thank the health facility staff for their unwavering support and assistance during the research process. Your dedication and cooperation were essential to the success of this project.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No fund was received for this research.
Disclosure
The authors declare that they have no competing interests.
References
1. Maternal mental health.
2. American Psychiatric Association, American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5.
3. Hutchens BF, Kearney J. Risk Factors for Postpartum Depression: an Umbrella Review. J Midwifery Womens Health. 2020;65(1):96–108. doi:10.1111/jmwh.13067
4. Ďuríčeková B, Škodová Z, Bašková M. Risk factors associated with postpartum depression and PTSD after birth in a sample of Slovak women. Heliyon. 2024;10(1):e23560. doi:10.1016/j.heliyon.2023.e23560
5. Zhao X-H, Zhang Z-H. Risk factors for postpartum depression: an evidence-based systematic review of systematic reviews and meta-analyses. Asian J Psychiatr. 2020;53:102353. doi:10.1016/j.ajp.2020.102353
6. Wang Z, Liu J, Shuai H, et al. Mapping global prevalence of depression among postpartum women. Transl Psychiatry. 2021;11(1):1–13. doi:10.1038/s41398-021-01663-6
7. Affonso DD, De AK, Horowitz JA, Mayberry LJ. An international study exploring levels of postpartum depressive symptomatology. J Psychosom Res. 2000;49(3):207–216. doi:10.1016/S0022-3999(00)00176-8
8. Bina R. The Impact of Cultural Factors Upon Postpartum Depression: a Literature Review. Health Care Women Int. 2008;29(6):568–592. doi:10.1080/07399330802089149
9. Halbreich U, Karkun S. Cross-cultural and social diversity of prevalence of postpartum depression and depressive symptoms. J Affect Disord. 2006;91(2):97–111. doi:10.1016/j.jad.2005.12.051
10. Joannides P. Postpartum Depression Is Common and Often Untreated | psychology Today.
11. WHO-AIMS Country Profile: Eritrea.
12. JOGH. Mental health in Eritrea: a brief overview and possible steps forward. 2021.
13. Ghebrat Y, Mebrahtu G, Kosia A, Mufunda J, Usman A, Oomen J. Bottlenecks in the provision of quality mental health services in Eritrea. J Eritrean Med Assoc. 2008;3(1):15–18. doi:10.4314/jema.v3i1.49621
14. Cox JL, Holden JM, Sagovsky R. Detection of Postnatal Depression: development of the 10-item Edinburgh Postnatal Depression Scale. Br J Psychiatry. 1987;150(6):782–786. doi:10.1192/bjp.150.6.782
15. Shoaee F, Mohsenpour Z, Najarzadegan MR, et al. Sensitivity and Specificity of the Edinburgh Postnatal Depression Scale (EPDS) among Iranian Mothers: a Psychometric Study. Int J Pediatr. 2019;7:10533. doi:10.22038/ijp.2019.44006.3653
16. Levis B, Negeri Z, Sun Y, Benedetti A, Thombs BD. Accuracy of the Edinburgh Postnatal Depression Scale (EPDS) for screening to detect major depression among pregnant and postpartum women: systematic review and meta-analysis of individual participant data. BMJ. 2020;371:m4022. doi:10.1136/bmj.m4022
17. Shrestha SD, Pradhan R, Tran TD, Gualano RC, Fisher JRW. Reliability and validity of the Edinburgh Postnatal Depression Scale (EPDS) for detecting perinatal common mental disorders (PCMDs) among women in low-and lower-middle-income countries: a systematic review. BMC Pregnancy Childbirth. 2016;16(1):72. doi:10.1186/s12884-016-0859-2
18. Vik K, Aass IM, Willumsen AB, Hafting M. Experiences with the routine use of the Edinburgh Postnatal Depression Scale from health visitors’ and midwives’ perspectives – an exploratory qualitative study. Midwifery. 2021;100:103017. doi:10.1016/j.midw.2021.103017
19. Chan AW, Reid C, Skeffington P, Marriott R. A systematic review of EPDS cultural suitability with Indigenous mothers: a global perspective. Arch Womens Ment Health. 2021;24(3):353–365. doi:10.1007/s00737-020-01084-2
20. Cox J. Thirty years with the Edinburgh Postnatal Depression Scale: voices from the past and recommendations for the future. Br J Psychiatry. 2019;214(3):127–129. doi:10.1192/bjp.2018.245
21. Tsai AC, Scott JA, Hung KJ, et al. Reliability and Validity of Instruments for Assessing Perinatal Depression in African Settings: systematic Review and Meta-Analysis. PLoS One. 2013;8(12):e82521. doi:10.1371/journal.pone.0082521
22. Hosmer DW, Lemeshow S. Applied Logistic Regression.
23. Smith-Nielsen J, Matthey S, Lange T, Væver MS. Validation of the Edinburgh Postnatal Depression Scale against both DSM-5 and ICD-10 diagnostic criteria for depression. BMC Psychiatry. 2018;18(1):393. doi:10.1186/s12888-018-1965-7
24. Bhusal BR, Bhandari N, Chapagai M, Gavidia T. Validating the Edinburgh Postnatal Depression Scale as a screening tool for postpartum depression in Kathmandu, Nepal. Int J Ment Health Syst. 2016;10(1):71. doi:10.1186/s13033-016-0102-6
25. Atuhaire C, Brennaman L, Nambozi G, et al. Validating the Edinburgh Postnatal Depression Scale Against the Diagnostic and Statistical Manual of Mental Disorders, for Use in Uganda. Int J Womens Health. 2023;15:1821–1832. doi:10.2147/IJWH.S427752
26. Tendais I, Costa R, Conde A, Figueiredo B. Screening for Depression and Anxiety Disorders from Pregnancy to Postpartum with the EPDS and STAI. Span J Psychol. 2014;17:E7. doi:10.1017/sjp.2014.7
27. Mandrekar JN. Receiver Operating Characteristic Curve in Diagnostic Test Assessment. J Thorac Oncol. 2010;5(9):1315–1316. doi:10.1097/JTO.0b013e3181ec173d
28. Tesfaye M, Hanlon C, Wondimagegn D, Alem A. Detecting postnatal common mental disorders in Addis Ababa, Ethiopia: validation of the Edinburgh Postnatal Depression Scale and Kessler Scales. J Affect Disord. 2010;122(1–2):102–108. doi:10.1016/j.jad.2009.06.020
29. Khalifa DS, Glavin K, Bjertness E, Lien L. Postnatal depression among Sudanese women: prevalence and validation of the Edinburgh Postnatal Depression Scale at 3 months postpartum. Int J Womens Health. 2015;677. doi:10.2147/IJWH.S81401
30. Joshi U, Lyngdoh T, Shidhaye R. Validation of hindi version of Edinburgh postnatal depression scale as a screening tool for antenatal depression. Asian J Psychiatr. 2020;48:101919. doi:10.1016/j.ajp.2019.101919
31. Mutiso VN, Musyimi CW, Tele A, Alietsi R, Andeso P, Ndetei DM. Edinburgh Postnatal Depression Scale (EPDS) for screening for depression in the first year post delivery in a low-resourced rural setting in Kenya. Transcult Psychiatry. 2023;60(3):476–483. doi:10.1177/13634615211043764
32. Agampodi T, Amarasinghe G, Wickramasinghe A, et al. Incorporating early pregnancy mental health screening and management into routine maternal care: experience from the Rajarata Pregnancy Cohort (RaPCo), Sri Lanka. BMJ Glob Health. 2023;8(9):e012852. doi:10.1136/bmjgh-2023-012852
33. Howard LM, Flach C, Mehay A, Sharp D, Tylee A. The prevalence of suicidal ideation identified by the Edinburgh Postnatal Depression Scale in postpartum women in primary care: findings from the RESPOND trial. BMC Pregnancy Childbirth. 2011;11(1):57. doi:10.1186/1471-2393-11-57
34. Chen C, Okubo R, Okawa S, et al. The prevalence and risk factors of suicidal ideation in women with and without postpartum depression. J Affect Disord. 2023;340:427–434. doi:10.1016/j.jad.2023.08.051
35. Rahmani Ivary F, Fanaei S, Ghahremani S, et al. A systematic review of psychometric properties of the Edinburgh Postnatal Depression Scale in Iranian population. Int J Pediatr. 2019;7:9497. doi:10.22038/ijp.2019.36747.3202
36. Ing H, Fellmeth G, White J, Stein A, Simpson JA, McGready R. Validation of the Edinburgh Postnatal Depression Scale (EPDS) on the Thai–Myanmar border. Trop Doct. 2017;47(4):339–347. doi:10.1177/0049475517717635
37. Moyer SW, Ameringer S, Elswick RK, Nunziato JD, Kinser PA. Exploration of the psychometric properties of the EPDS-US, a validation study. J Affect Disord. 2024;352:193–198. doi:10.1016/j.jad.2024.02.025
38. Priyambada LK, Bakhla AK, Pattojoshi A. Factor structure and internal consistency of Oriya version of Edinburgh Postnatal Depression Scale. Indian J Psychiatry. 2020;62(3):312. doi:10.4103/psychiatry.IndianJPsychiatry_631_19
39. Gausia K, Fisher C, Algin S, Oosthuizen J. Validation of the Bangla version of the Edinburgh Postnatal Depression Scale for a Bangladeshi sample. J Reprod Infant Psychol. 2007;25(4):308–315. doi:10.1080/02646830701644896
40. Roebianto R, Savitri A, Suciyana M. Content validity: definition and procedure of content validation in psychological research. Test Psychom Methodol Appl Psychol. 2023;30(1):5–18. doi:10.4473/TPM30.1.1
41. Reichenheim ME, Moraes CL, Oliveira AS, Lobato G. Revisiting the dimensional structure of the Edinburgh Postnatal Depression Scale (EPDS): empirical evidence for a general factor. BMC Med Res Methodol. 2011;11(1):93. doi:10.1186/1471-2288-11-93
42. Cunningham NK, Brown PM, Page AC. Does the Edinburgh Postnatal Depression Scale measure the same constructs across time? Arch Womens Ment Health. 2015;18(6):793–804. doi:10.1007/s00737-014-0485-9
43. Škodová Z, Bánovčinová Ľ, Urbanová E, Grendár M, Bašková M. factor structure of the Edinburgh postnatal depression scale in a sample of postpartum Slovak women. Int J Environ Res Public Health. 2021;18(12):6298. doi:10.3390/ijerph18126298
44. Song Z, Zhang D, Yang L, et al. Factor structure and longitudinal invariance for the Chinese Mainland version of the Edinburgh postnatal depression scale during pregnancy. Midwifery. 2024;132:103963. doi:10.1016/j.midw.2024.103963
45. Coates R, Ayers S, de Visser R. Factor Structure of the Edinburgh Postnatal Depression Scale in a Population-Based Sample. Psychol Assess. 2017;29(8):1016–1027. doi:10.1037/pas0000397
46. Kubota C, Inada T, Nakamura Y, et al. Stable factor structure of the Edinburgh Postnatal Depression Scale during the whole peripartum period: results from a Japanese prospective cohort study. Sci Rep. 2018;8(1):17659. doi:10.1038/s41598-018-36101-z
47. Montazeri A, Torkan B, Omidvari S. The Edinburgh Postnatal Depression Scale (EPDS): translation and validation study of the Iranian version. BMC Psychiatry. 2007;7(1):11. doi:10.1186/1471-244X-7-11
48. Winer ES, Bryant J, Bartoszek G, Rojas E, Nadorff MR, Kilgore J. Mapping the relationship between anxiety, anhedonia, and depression. J Affect Disord. 2017;221:289–296. doi:10.1016/j.jad.2017.06.006
49. Kubota C, Okada T, Aleksic B, et al. Factor Structure of the Japanese Version of the Edinburgh Postnatal Depression Scale in the Postpartum Period. PLoS One. 2014;9(8):e103941. doi:10.1371/journal.pone.0103941
50. Naja S, Al-Kubaisi N, Chehab M, Al-Dahshan A, Abuhashem N, Bougmiza I. Psychometric properties of the Arabic version of EPDS and BDI-II as a screening tool for antenatal depression: evidence from Qatar. BMJ Open. 2019;9(9):e030365. doi:10.1136/bmjopen-2019-030365
51. Kaminsky LM, Carlo J, Muench MV, Nath C, Harrigan JT, Canterino J. Screening for postpartum depression with the Edinburgh Postnatal Depression Scale in an indigent population: does a directed interview improve detection rates compared with the standard self-completed questionnaire? J Matern Fetal Neonatal Med. 2008;21(5):321–325. doi:10.1080/14767050801995084
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.