Back to Journals » Journal of Pain Research » Volume 19
Transitional Pain Services and Clinics: A Scoping Review of Recent Literature
Authors Freitag HE, Melvin RL, Godwin RC, Ness TJ ![]()
Received 11 July 2025
Accepted for publication 7 January 2026
Published 31 January 2026 Volume 2026:19 548214
DOI https://doi.org/10.2147/JPR.S548214
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Giuliano Lo Bianco
Harvy E Freitag,1 Ryan L Melvin,1 Ryan C Godwin,1,2 Timothy J Ness1
1Department of Anesthesiology and Perioperative Medicine, University of Alabama at Birmingham, Birmingham, AL, USA; 2Department of Radiology, University of Alabama at Birmingham, Birmingham, AL, USA
Correspondence: Timothy J Ness, Department of Anesthesiology and Perioperative Medicine, University of Alabama, PBMR 208, 901 19 th St. S, Birmingham, AL, 35205, USA, Tel +1-205-975-9643, Email [email protected]
Purpose: The goal of manuscript is to summarize and synthesize the body of literature on Transitional Pain Services and Clinics (TPS/Cs), highlighting models, outcomes, and implementation considerations.
Methods: Using a published, Artificial Intelligence-assisted, interactive algorithm, PubMed, CINAHL, and SCOPUS listed literature were searched for all articles related to TPS/Cs published in the last 10 years.
Results: 58 relevant articles were identified and grouped into six topics.
Conclusion: Multiple models of TPS/Cs were identified. The most commonly described were multidisciplinary clinics of pain physicians, nurses, psychologists, physiologists, and other health-related personnel. Mostly, retrospective literature suggests that TPS/Cs can effectively bridge acute postoperative pain management with sustained long-term care, particularly for patients at higher risk of chronic postsurgical pain and opioid misuse. More prospective and randomized trials are needed.
Keywords: transitional pain clinic, transitional pain service, opioid use disorder, chronic post-surgical pain
Introduction
Improving pain management and reducing opioid-related complications are international healthcare priorities. This urgency arises in part from the high prevalence of chronic post-surgical pain and the associated potential for long-term opioid use. In many cases, standard perioperative care fails to adequately prevent the transition from acute postoperative pain to chronic pain, leading to escalating opioid doses and increased risk of dependence or misuse.1–3 Against this backdrop, the concept of Transitional Pain Services and/or Clinics has emerged as a promising model to bridge acute pain management in the immediate perioperative and postoperative period with long-term pain care.2,4–8 Numerous models have been described, ranging from stand-alone, post-discharge Transitional Pain Clinics to more global, perioperative multidisciplinary teams (Transitional Pain Services) that then extend cares into the post-discharge perioperative period. For purposes of this review, we will combine an assessment of the recent published literature related to all of these models and will use the combined term of Transitional Pain Service/Clinics (TPS/Cs) to describe them.
TPS/Cs often combine multidisciplinary teams of pain specialists, psychologists, physiotherapists, and other healthcare professionals to proactively address pain and psychosocial factors as patients move from surgery to recovery.3 Key features typically include early risk identification, multimodal pain management, and structured opioid tapering protocols tailored to patients’ needs.1,2,4–7 Early evaluations of these clinics have shown encouraging results.3,4,9 However, the evidence base is still growing, with variability in TPS/C models, patient populations, and outcome measures.2,8 Given the growing interest in integrating TPS/Cs into surgical pathways worldwide, we felt that a scoping review of the existing literature on these programs was warranted.2,8,10 Scoping reviews differ methodologically from systematic reviews and allow for a broader discussion of evolving topics.11 There have been other reviews of TPS/Cs (all included in this manuscript’s citation list) which have typically been written from the viewpoint of single treatment centers. We present here the broader view of multiple centers. As healthcare systems consider implementing or refining TPS/Cs, it is essential to understand the entire range of approaches, the reported effects on opioid tapering and pain outcomes, and the challenges of real-world implementation.8,12
Our specific research questions were the following: {1} what are the core components and models of TPS/Cs designed to support post-surgical cares; {2} what evidence exists on the clinical and patient-reported outcomes (eg, opioid reduction, pain scores, function, quality of life) associated with TPS/Cs; and {3} what barriers, facilitators, and future directions are reported in the literature regarding the implementation of TPS/Cs? Our intent was to describe literature related to the various TPS/C models in an attempt to reveal common goals of effectively guiding the transition from acute to chronic pain care while at the same time identifying key differences in the focus of the various studies and methodological differences such as the duration of follow-up.2,8
Materials and Methods
General
In developing and conducting this review, we followed established methodological guidance using the framework proposed by Arksey and O’Malley11 and the recommendations set out in the PRISMA-ScR extension (https://www.prisma-statement.org/scoping). This review leveraged our published generative Artificial Intelligence (AI) tool13 which was developed and modified to streamline the process of identifying and synthesizing relevant literature. That tool incorporates use of ChatGPT4.0. The tool’s capabilities include generating PubMed, CINAHL, and SCOPUS queries based on user-provided research questions, returning a manageable list of articles for review, and assisting in the iterative refinement of the search process. It is noteworthy that this AI tool functions interactively, requiring user input at critical stages, particularly in the decision-making process for article inclusion or exclusion. The authors of the review played a pivotal role in guiding the AI through iterative cycles of query refinement and article selection, ensuring that the final set of articles closely aligned with the specific research questions. A less focused “human-only” repeat search of PubMed articles using the search terms “transitional” and “pain” and “clinic or service” identified no additional relevant articles. A final manual review of all the cited manuscripts assured veracity of the report.
Search Strategy
A broad and iterative search strategy was employed to locate studies describing or evaluating TPS/Cs. Guided by keywords identified in preliminary scans of the literature, we combined synonyms for “transitional pain service”, “transitional pain clinic”, and “transitional pain program” with search terms related to the postoperative period (eg, “postoperative”, “postsurgical”) and opioid use (eg, “opioid”, “analgesic”, “taper,” “wean”, and “chronic post-surgical pain”). We applied filters for the last 10 years and the searches were confined to English-language, peer-reviewed articles. Two reviewers independently screened the titles and abstracts of the remaining records to assess their relevance to TPS/C interventions and articles were retained for full-text review. The screening and selection decisions are documented in Figure 1, illustrating each step from the initial search through to the final set of included papers. Studies were included if they {1} enrolled post-surgical patients who were at risk of, or already receiving, opioid medications, {2} described or evaluated a formal TPS/C model or closely analogous service bridging acute postoperative care and subsequent outpatient management, and {3} reported at least one relevant outcome pertaining to opioid tapering (eg, dose reduction, cessation rates), pain measures (eg, pain intensity, chronic post-surgical pain incidence) and/or functional improvements (eg, return to work, quality of life). Both experimental and observational designs (eg, randomized controlled trials, cohort studies, prospective and retrospective evaluations, qualitative research) as well as secondary sources (eg, editorial reviews, expert opinions, narrative reviews) were accepted, provided that each described a TPS/C. Studies were excluded if they {1} did not focus on a postsurgical population or {2} detailed a pain management program without transitional components (eg, interventions that ended at discharge without outpatient follow-up or standard chronic pain clinics lacking a perioperative strategy). These criteria were set a priori to retain clarity and consistency throughout the search and screening phases.
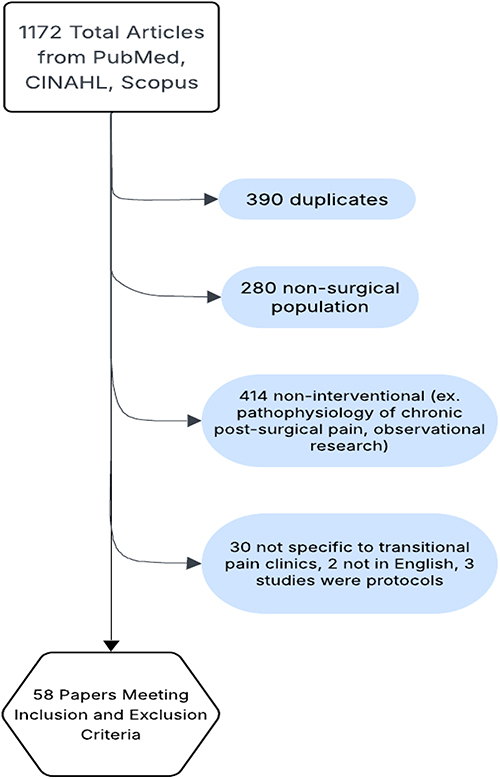 |
Figure 1 Flowchart for article selection. |
Data Analysis and Synthesis
Building on Arksey and O’Malley’s approach to scoping reviews,12 we applied a thematic content analysis to the extracted data. The research team reviewed each study’s reported findings, implementation details, and patient outcomes to identify recurrent themes. These emergent themes were grouped inductively, allowing conceptual categories to arise naturally from the data.
Results
Studies Selected
All records retrieved from the database searches were collected in a reference management program, where duplicates were removed. A total of 1172 articles were initially identified (PubMed, CINAHL, and Scopus). After screening, 390 records were recognized as duplicates and subsequently excluded. The remaining articles were assessed for eligibility and excluded if they did not meet the predefined criteria for this scoping review. This left 58 articles, which were organized into six specific topics for description/discussion.
Topic 1: TPS/Cs for Opioid Tapering and Dependence
Patients with opioid use disorder (OUD) face significant perioperative challenges, particularly when it comes to balancing medication for opioid use disorder (MOUD) with additional opioids needed for surgical pain. Multiple research efforts have examined how TPS/Cs can address this balance, providing structured support to safely taper postoperative opioids while maintaining or adjusting MOUD. Pain management physicians play a pivotal role in guiding perioperative opioid tapering for patients with OUD within transitional pain clinics.
Findings from several studies underscore the importance of these physicians’ detailed involvement in titration protocols, close monitoring, and outcome assessments. In a retrospective cohort study conducted by Liu et al9 at the Johns Hopkins Personalized Pain Program, 50 adult patients on methadone or buprenorphine underwent surgery and received postoperative tapering management. In that study, 46% of patients fully discontinued non-MOUD opioids, a process strongly influenced by physician-led decisions on whether to continue methadone or buprenorphine in the hospital. The same analyses revealed that higher preoperative MOUD doses (a factor typically under physician discretion) were linked to faster tapering. Notably, patients on buprenorphine took 1.79 times longer to cease additional opioids than those on methadone. These results highlight how decisions regarding continuation of MOUD and postoperative opioid dosing can critically shape tapering trajectories. Early work by Huang et al1 illustrated how pain management physicians identified surgical patients at risk for chronic post-surgical pain (CPSP) and worked to reduce excessive opioid prescribing through their new TPS/C model. The authors reported how anesthesiologists oversaw personalized tapering plans immediately after surgery. In their detailed example of a 58-year-old patient with prior substance use, the attending pain physician guided the patient’s weaning to completion in just three weeks postoperatively—an outcome made possible by careful dose adjustments and frequent in-person evaluations of analgesia and withdrawal risk. A broader literature review by Mikhaeil et al2 also pointed to the leadership of anesthesiologists in launching and running TPS/Cs, including the high-volume program at Toronto General Hospital (TGH). Data drawn from TGH between 2014 and 2017 showed that patients who received early postoperative consultation with pain physicians had marked reductions in long-term opioid consumption. For instance, opioid-experienced individuals experienced a 44% decrease in their morphine-equivalent dose, with approximately a quarter of those subjects completely off opioids by six months. By designing standardized taper protocols and selecting multimodal analgesics, anesthesiologists provided structure that significantly shortened the transition from hospital opioids to minimal or no opioids at home. A more in-depth account of these outcomes at TGH was published by Clarke et al4 detailing a single-center observational study of 251 patients followed for six months after surgery. The TPS/C anesthesiologists measured daily opioid intake at discharge and subsequent outpatient visits, customizing taper schedules based on patients’ self-reported pain, any comorbid neuropathic symptoms, and psychosocial factors. Their data indicated that 44.5% of opioid-naïve individuals and 25.6% of those with significant prior opioid exposure fully stopped prescription opioids at six months. Physician decisions on discharge opioid doses appeared central: in opioid-naïve patients, lower initial prescriptions correlated with better long-term weaning success.
Physicians’ role in adjusting pharmacotherapy was exemplified by Weinrib et al14 who reported a case of complex chronic pain and high-dose opioid dependence managed by buprenorphine in conjunction with behavioral therapy. In that instance, anesthesiologists and addiction specialists jointly monitored opioid doses—initially as high as 460 morphine milligram equivalents per day—and transitioned the patient onto a buprenorphine/naloxone combination. Within a week of induction, the patient noted substantial pain relief; by eight months, he was off full opioid agonists entirely. The case underscores how anesthesiologists’ medication choices, careful induction schedules, and vigilant side-effect assessments facilitate safe downward titration, even in patients with multi-decade opioid use histories. These findings align with foundational work by Katz et al5 at TGH, which demonstrated how combining pharmacological therapies with acceptance-based psychological interventions and physiotherapy could significantly mitigate the transition from acute to chronic pain. Recent retrospective data also reinforce the tangible effects of TPS/Cs on long-term opioid trajectories. Ladha et al6 showed that, despite having higher initial opioid dosing needs, patients enrolled in a TPS/C achieved faster monthly reductions compared to a matched cohort at other hospitals. Although not limited to OUD populations, these findings reflect the broader potential of TPS/C to meet the needs of individuals struggling with any degree of opioid dependence. Klimke et al7 similarly argued for expanded use of telehealth and digital monitoring tools to ensure that patients, particularly those in remote or underserved areas, could benefit from the same structured follow-up available in larger academic centers.
Institutional and research initiatives have explored further enhancements to transitional perioperative pain care. For example, a multicenter randomized trial (the NIH-funded KALPAS study) is investigating whether perioperative ketamine, administered either as a continuous infusion or a single bolus, can reduce chronic pain following mastectomy, potentially offering a scalable non-opioid option to mitigate persistent pain and long-term opioid use in surgical patients.15 At Johns Hopkins, multidisciplinary perioperative programs have addressed the high-risk segment of chronic opioid users by integrating behavioral health services, addiction specialists, and robust patient engagement strategies—efforts that have yielded meaningful reductions in overall morphine milligram equivalents.16–18 Vanderbilt University Medical Center launched a similar TPS/C, focused on patients at risk of prolonged opioid use. Early indications suggest significant decreases in long-term opioid requirements.19
Overall, the body of work examining TPS/Cs for patients with OUD and other high-risk populations indicates that coordinated, multidisciplinary efforts help achieve meaningful reductions in postoperative opioid use while sustaining effective pain control. Central to this success are consistent continuation of MOUD, comprehensive psychosocial interventions, thorough case management, and ongoing risk stratification. As more TPS/C models incorporate standardized protocols and digital follow-up, further research, particularly randomized trials, will help refine best practices for aligning opioid tapering strategies with the complex needs of surgical patients who have OUD.
Topic 2: Multidisciplinary Nature of TPS/Cs
Multidisciplinary collaboration lies at the heart of TPS/Cs, enabling a more holistic approach to surgical pain and reducing the risk of chronic postoperative opioid use. Recent research illustrates how various health care disciplines—anesthesiology, psychology, psychiatry, physical therapy, nursing, pharmacy, and social work—integrate within TPS/Cs to provide comprehensive perioperative support. This integrated model is especially critical for high-risk patients, whether they have significant baseline opioid needs, psychological comorbidities, or complex surgical recoveries.
Several investigators have emphasized the central role of personalized, patient-centered care in TPS/Cs. In a mixed-methods study involving patients at The Johns Hopkins Personalized Pain Program, Manoharan et al20 found that patient satisfaction was closely linked to perceived engagement by the TPS/C team, including access to mental health support and clearly defined pain management goals. Participants reported feeling “heard” when psychiatry, psychology, and medical pain specialists worked together, an effect that promoted both opioid tapering success and improved psychological outcomes. Notably, some patients still struggled with logistical barriers, such as continuity of care, highlighting the importance of deliberate coordination among multiple disciplines. The feasibility of such coordination was similarly evident in a report by Tierney et al21 who implemented a TPS/C protocol at the Ottawa Hospital specifically for spine surgery patients. Since spine operations often involve protracted recoveries and high opioid use, this population exemplifies the need for integrated care. Pain specialists collaborated with psychologists to assess patient expectations, while anesthesiologists and allied providers offered both pharmacological and non-pharmacological therapies. Although enrollment and retention rates were high, issues around patient follow-up, including telehealth logistics, underscored that even well-structured multidisciplinary teams must continuously refine methods for reaching patients beyond the hospital. Multidisciplinary TPS/C models have also proven flexible enough to address the needs of specialized populations which will be discussed in Topic 4.
Psychological factors play a critical role in how patients experience and manage post-surgical pain.22–25 Early research demonstrated that smokers were more likely to report higher pain intensity and faced greater challenges in tapering off opioid medications, suggesting that emotional distress and maladaptive coping might exacerbate post-surgical pain experiences.22 Subsequent work on the Sensitivity to Pain Traumatization Scale (SPTS-12) revealed how heightened trauma responses to pain could significantly predict pain interference, opioid use, and persistent anxiety or depression, pointing to the importance of early psychological screening.23 Parallel investigations into CPSP further underscored risk factors such as pain catastrophizing and perceived injustice, as well as protective factors like acceptance, mindfulness, and pain self-efficacy.24,25 Across multiple studies, researchers employed a range of psychometric tools to capture the multifaceted nature of pain and psychological distress.22,24,25 Common measures included the Brief Pain Inventory to gauge pain severity and interference, as well as the Pain Catastrophizing Scale to assess rumination, magnification, and helplessness.22,24,25 The Hospital Anxiety and Depression Scale served to quantify emotional distress, while the SPTS-12 specifically measured trauma-like responses to pain.23,24 In these studies, opioid intake was often standardized through morphine equivalent daily dose calculations, facilitating comparisons and tracking of tapering progress.22,25
Numerous TPS/C protocols integrated psychological therapies designed to modify maladaptive thoughts and behaviors around pain. Cognitive-behavioral therapy aimed to reduce catastrophizing, while Acceptance and Commitment Therapy cultivated psychological flexibility and encouraged engagement in value-based activities despite pain.24,25 Similarly, mindfulness-based interventions were commonly used to foster non-reactive awareness and mitigate emotional distress linked to pain sensations. By personalizing these interventions multidisciplinary TPS/C teams addressed both the physiological and psychological dimensions of recovery. Ultimately, these findings highlight the need for comprehensive, psychologically informed pain management strategies in surgical settings. Screening tools allow clinicians to flag patients at risk for chronic pain and problematic opioid use, enabling earlier and more targeted interventions.23,24 Multiple lines of evidence suggest that such TPS/Cs models can significantly improve pain outcomes and facilitate successful opioid tapering. As research in this domain continues, further refinement of psychometric measures and psychological therapies will likely yield even more effective methods to prevent and manage CPSP as discussed in the next section. Taken together, these studies reveal a consistent trend: the multidisciplinary nature of TPS/Cs enhances both clinical outcomes and patient experiences across varying surgical contexts. By uniting professionals from multiple fields under a common framework, TPS/Cs can deliver individualized treatment plans that address physical, psychological, social, and economic dimensions of care.
Topic 3: TPS/Cs for CPSP Prevention & Management
As noted in the prior sections, there have been recent studies that have reinforced the premise that TPS/C strategies, which include thorough preoperative evaluations, personalized analgesic regimens, ongoing patient education, and interprofessional coordination, can substantially improve pain trajectories following major surgery. By prioritizing both pharmacological and psychosocial dimensions of perioperative care, TPS/Cs effectively reduce the likelihood that acute pain will transition to chronic, debilitating pain states. A narrative review by Moka et al26 presented a European viewpoint of TPS/Cs, underlining how they can bridge acute and chronic pain care by integrating risk stratification, early multimodal interventions, and telehealth-based follow-up. Likewise, the Veterans Affairs (VA) Healthcare System has adopted TPS/C frameworks for high-risk surgical cohorts. As described by Dunworth et al,10 structured screening and continuity of care can substantially reduce CPSP and unnecessary opioid use. An editorial by Vanneman et al11 underscored the importance of identifying “moderate-staying-moderate” pain trajectories, particularly in cardiac surgery. Their stated goal was to intervene early and potentially avert persistent pain conditions. Lomanowska et al27 detailed how knowledge translation initiatives at TGH expanded best practices in perioperative pain management, while Kojic and Clarke,28 who were also at TGH, emphasized bridging the acute-to-chronic transition through comprehensive patient education, functional pain assessments, and structured opioid-weaning protocols. The TRUSt trial,29 a controlled trial performed in the Netherlands, randomized subjects into TPS/C-directed cares or to standard-of-care treatment. In this study, they demonstrated that, while short-term postoperative recovery scores may not differ substantially, TPS/Cs confer measurable benefits in reducing long-term opioid use and persistent surgical pain.
Some publications have emphasized the role of TPS/Cs in preventing and managing CPSP among diverse patient populations. Mikhaeil et al2 described that a broad, multidisciplinary TPS/C framework was able to facilitate postoperative opioid weaning in a way that aligned with minimizing chronic pain risk. Other authors have focused on the prevalence of CPSP in major surgeries more broadly e.g.30,31 Huang et al identified the interplay of high-dose opioid prescriptions, unaddressed psychosocial factors, and insufficient post-discharge planning as central contributors to chronic postoperative pain.30 Their observations underscored the necessity of TPS/C programs to integrate education, early therapy initiation, and active tapering schedules for at-risk patients. Katz et al,32 meanwhile, emphasized how assessing factors such as pain catastrophizing and using structured mental health assessments were able to detect individuals who might benefit from Acceptance and Commitment Therapy or other psychological interventions. These approaches, they found, could arrest or at least slow the spiraling transition to CPSP if delivered soon after surgery. Lavand’homme33 further contextualized this dynamic by pointing to the four-to-six-week subacute recovery window during which poorly managed acute pain can become more deeply ingrained. By maintaining contact with patients through telehealth, phone calls, and in-person evaluations, TPS/C practitioners are able to intervene promptly if neuropathic or severe nociceptive pain emerges. Clarke et al34 corroborated these insights by demonstrating how preventive analgesia, ranging from ketamine infusions to nerve blocks, worked best when paired with robust outpatient guidance.
Topic 4: TPS/Cs for Special Populations
Pediatric
TPS/Cs have shown particular promise in addressing the unique pain management needs of various surgical subpopulations including pediatric patients, whose clinical and psychosocial vulnerabilities often lead to prolonged pain or opioid dependence when not adequately supported. In pediatric contexts, persistent post-operative pain can lead to detrimental effects on quality of life, such as absences from school, social isolation, and mental health disturbances. A retrospective review by Haynes et al35 examined 31 children aged 0–18 years who experienced post-operative pain beyond the expected recovery period and found neuropathic pain to be the most common presentation (64%), with orthopedic, general, cardiac, and trauma-related surgeries frequently implicated. More than half of these pediatric patients (55%) achieved complete pain resolution, and seven out of eight children on opioids were successfully weaned off with assistance of the TPS/C. In their report, the authors underscored the need for a dedicated TPS/C to enable early intervention, reduce the incidence of persistent pain and streamline comprehensive, multimodal treatment approaches in pediatric populations.35 Isaac et al similarly emphasized preventive measures in children through the development of a Pediatric Transitional Pain Service at The Hospital for Sick Children in Toronto.36 Their initiative included pre-surgical risk assessments, careful opioid stewardship, routine post-operative follow-ups, and psychological support, all designed to reduce reliance on analgesics and enhance recovery. Early data showed that only 2.6% of children in this program transitioned to chronic pain clinics, a dramatic decrease from the 20% historically expected among pediatric surgical patients.36 Together, these pediatric studies reinforce how targeted interventions within the first few months after surgery can avert chronic pain syndromes and limit long-term opioid use.
Veterans
Veteran (sub)populations bring additional complexities, including high rates of mental health issues, substance use disorders, and the potential for post-traumatic stress disorder. In one initiative at the Salt Lake City Veterans Administration (VA) Medical Center, Buys et al implemented a multidisciplinary TPS/C to address these concerns.37 Among 213 veterans undergoing major orthopedic and cardiothoracic operations, frequent follow-ups (99% within 14 days and 96% with additional follow-up by 30 days) coupled with a multimodal pain management strategy helped reduce new chronic opioid use from 14% (historical) to only 0.7% among previously opioid-naïve individuals. Chronic opioid users also saw notable benefits, with 43.3% discontinuing opioids entirely by 90 days. A related study by the same group investigated opioid use in veterans having surgery at a VA facility with a TPS/C and compared them with surgical cares at a non-VA hospital lacking a TPS/C.38 Veterans at the VA facility required less opioids at discharge and in the first 90 days after surgery. They were also less likely to fill any prescriptions past 90 days after discharge. These findings highlight how specific environments may inadvertently prolong opioid use and underscore the importance of uniform pain management protocols. Buys et al37 also reported on the program’s design and effectiveness by presenting data related to high-risk veterans who benefited most from intensive pre-surgical education, structured tapering, and close coordination among care teams. Collectively, the veteran-focused studies indicated that early, consistent follow-up, combined with multimodal pain therapies and tight communication between inpatient and outpatient care teams, significantly reduces prolonged opioid use and improved post-surgical outcomes.
Transplant Patients
Another special surgical population includes transplant patients. Yu et al3 documented how these subjects, who frequently face immunosuppressant side effects and steroid-induced pain, benefited from targeted collaborations among pain medicine, psychiatry, and physical therapy. A separate, single-patient case report by Meng et al39 detailed the use of medical cannabis within a TPS/C framework to facilitate opioid reduction in a liver transplant patient. This study highlighted the breadth of therapeutic modalities that multidisciplinary teams can deploy. Although cannabis-based interventions require careful consideration, especially in immunocompromised patients, the report underscored the TPS/C’s role in adapting to individual patient needs and exploring adjunctive therapies responsibly.
Obstetrics
A particularly unique population for which TPS/Cs are being established is the obstetric population. Blanco and Ansari40 have described their TPS/C which is dedicated to pain evaluation, treatment, and follow-up in pregnant patients as well as other women undergoing gynecological surgeries. They report that by using traditional TPS/C elements of care they have reduced the amount of opioids used at discharge from the hospital and at a 90-day follow-up.
Trauma
Trauma surgery patients, who often require repeated operations and grapple with significant functional impairment, present another patient group likely to benefit from TPS/Cs. Flynn et al41 reported on four complex trauma cases, each managed by a multidisciplinary team comprising anesthesiologists, psychiatrists, therapists, and rehabilitation specialists. Psychological interventions proved critical in managing anxiety and post-traumatic stress symptoms, pointing to the complex interplay between mental health and persistent postsurgical pain. Even in patients who demonstrated opioid relapses, ongoing psychiatric care, and medical management through that TPS/C helped them transition to safer regimens.
Orthopedics
Orthopedic surgery is another area where TPS/C has made notable inroads. Featherall et al42 showed that a comprehensive TPS/C approach after total joint arthroplasty was associated with a striking reduction in opioid use at 90 days. Patients were more likely to discontinue opioid therapy promptly when they received preoperative psychological counseling, multimodal analgesic management including perioperative nerve blocks, and consistent outpatient follow-up. Similar findings related to thoracic surgery have been discussed by Tong et al.43 In all of these special populations, early identification of patients at risk for chronic pain, strategic use of both non-pharmacologic and pharmacologic therapies, and robust continuity of care were the core principles of successful transitional pain programs, even in populations often burdened with comorbid conditions. Collectively, these findings demonstrate that TPS/Cs, when tailored to each population’s needs, can alleviate suffering, prevent unnecessary opioid dependence, and pave the way for broader adoption of integrated pain management strategies.
Topic 5: Role of Telehealth and “Virtual” TPS/Cs
Recent studies underscore the growing role of telehealth in supporting TPS/Cs and, by extension, improving patient outcomes around pain management and opioid tapering.44–47 One piece of evidence comes from the use of mobile health applications, as demonstrated by the “Manage My Pain” (MMP) mobile health application study.44 In that study, researchers observed that more than half of the patients in their TPS/C consented to use MMP and completed registration, indicating relatively high acceptance of a telehealth solution. Notably, retention rates at 30 and 90 days compared favorably to industry benchmarks, although a sizable portion of patients never logged a first entry or dropped off within the first month. These findings highlight the promise of app-based interventions in facilitating self-management of pain but also point to the importance of early onboarding support and sustained engagement strategies.44,47
Video-based telehealth platforms have also been effective in addressing service disruptions and expanding TPS/C access.45 A case study from the Veterans Health Administration illustrated rapid adoption of video consultations during the COVID-19 pandemic, ensuring continuity of care despite widespread limitations of in-person visits.45 Challenges ranged from limited technical infrastructure to patient-related barriers (such as older adults having difficulty with technology). Regulatory flexibilities and provider education paved the way for virtual TPS/C services to succeed.45 The authors reported that telehealth not only allowed ongoing opioid tapering and pain management but also improved access for veterans in remote locations. Other TPS/Cs have reported that they also provide telehealth consultations, which help overcome barriers of distance or mobility, especially for those who cannot easily visit the clinic.48,49 Some TPS/C programs have a dedicated helpline for quick responses to withdrawal symptoms or medication concerns.8 These telehealth components reduce the risk that patients will lose contact with their care team once their immediate postoperative phase is over, and they offer clinicians invaluable data on fluctuating pain levels or emergent issues.47,50
A recent study at the University of Texas Health Science Center at Houston reported on a “Virtual” TPS/C protocol for spine surgery patients suggests that telehealth can substantially reduce opioid dependence and improve behavioral health outcomes.46 Incorporating cognitive behavioral therapy as part of the remote pain management regimen, the program demonstrated impressive tapering success rates among both opioid-naïve and opioid-exposed individuals. Reductions in anxiety, depression, and pain levels were similarly encouraging. Further, patient engagement remained high, with minimal emergency department visits—a finding that echoes growing evidence that virtual TPS/C solutions can be both cost-effective and clinically impactful if well-integrated into standard care pathways.46
Collectively, these studies underscore the potential for telehealth, whether delivered through mobile apps or video platforms, to enhance the reach and effectiveness of TPS/Cs. High rates of initial uptake and positive clinical outcomes indicate patient willingness to incorporate technology into their pain management journeys, provided the platforms are user-friendly, integrated with clinical workflows, and supported by robust onboarding and follow-up protocols. As healthcare systems continue to refine telehealth offerings, evidence suggests that combining behavioral health strategies with technology-based pain tracking and consultation can be a powerful tool for promoting better recovery trajectories after surgery.44–47
Topic 6: How to Implement TPS/Cs & Assess Their Outcomes
The real challenge for TPS/Cs lies in implementing these programs in a way that aligns with clinical workflows and garners support from all stakeholders.49,51 Hospitals that have pioneered TPS/C initiatives have emphasized the importance of beginning with strong institutional buy-in. A championing team of anesthesiologists, psychologists, and nursing staff, and clear data demonstrating the cost-effectiveness of structured pain management are strong arguments for support from hospital administrators.47,50 By illustrating how uncontrolled chronic postoperative pain can lead to more readmissions, higher healthcare expenditures, and prolonged opioid dependence, proponents of TPS/Cs make a compelling case for institutional funding and dedicated staffing.49,52 Once organizational support is secured, TPS/Cs typically identify patients at risk for persistent pain early in the surgical process.53,54 This step often includes using validated screening measures which assess catastrophizing and anxiety, thereby flagging those patients who are most vulnerable.31,54 Coordination with inpatient pain services ideally allows for a seamless handover once the patient is discharged or moves from inpatient to outpatient care.55,56
A crucial element of successful TPS/C implementation is the development of standardized protocols for both opioid tapering and multimodal pain strategies.54,57 Instead of relying on ad hoc decisions, many clinics establish clear guidelines, outlining how quickly and by what dose increments opioids should be reduced.48,55 This approach is supported by a robust regimen of non-opioid analgesics (eg, NSAIDs, acetaminophen, gabapentinoids) and, in certain cases, regional anesthesia or adjuvant therapies like ketamine.51 Psychological interventions, ranging from Cognitive-Behavioral Therapy to Acceptance and Commitment Therapy, help patients develop healthier attitudes toward pain and reduce maladaptive coping behaviors.50,54 Physical therapy and exercise, meanwhile, bolster functional recovery and can further lower the need for opioid use.55
Beyond clinical benefits, TPS/Cs have also been examined for their economic impact. A quasi-experimental evaluation by Yoo et al54 at multiple Veterans Affairs (VA) centers as part of a multi-center evaluation, indicated that while TPS/C patients had more outpatient visits, they did not experience any overall increase in medical costs. In fact, for patients who did not have a history of chronic opioid use, there were measurable reductions in inpatient expenses suggesting that multidisciplinary, early-intervention strategies can pay dividends for both patients and healthcare systems.
Ensuring sustainability hinges on continuous evaluation.58,59 In many TPS/Cs, clinicians collect metrics such as morphine equivalent daily use at various intervals such as in the immediate post-discharge period, at 30 days, and up to six months. These metrics are used to gauge tapering success.50,60 Validated pain scales, like the Brief Pain Inventory, along with measures of psychological distress (eg, the Hospital Anxiety and Depression Scale), help determine whether patients are improving in terms of both physical pain relief and emotional well-being.54,60 Periodic review of these outcomes not only confirms whether the TPS/C is meeting its goals but also highlights areas for improvement.48,50 For instance, a spike in dropout rates might prompt a closer look at patient education materials or the frequency of scheduled follow-ups.55,56 Ultimately, the long-term viability of a TPS/C often depends on forging partnerships with primary care practices and specialists who will manage patients once the formal follow-up period in the clinic ends.58,59 Clear handover documentation—summarizing the patient’s tapering progress, ongoing psychological needs, and recommended monitoring schedules—helps ensure consistency once the patient leaves the direct purview of the surgical team.40,53 In parallel, presenting cost-related data, such as reductions in hospital readmissions and emergency department visits, reassures hospital administrators that a TPS/C is a wise investment rather than an extra expense.49,52 These concrete steps, from securing early buy-in and implementing systematic protocols to leveraging digital tools and robust outcome tracking, demonstrate how TPS/Cs can move from an appealing concept to a sustainable reality for both patients and healthcare systems alike.
Several studies highlighted the importance of hospital-level commitment in driving TPS/C success.52,53 Supportive infrastructure, such as dedicated pain service personnel, resources for ongoing data collection, and consistent follow-up pathways, facilitates a smoother transition from inpatient to outpatient care.55,59 In turn, having more transparent metrics (eg, morphine equivalent daily dose measurements, validated pain scales) enables clinicians to continuously refine protocols. Physicians who oversee perioperative pain, often with specific expertise in acute and transitional pain management, appear to be particularly effective when working within an institution that values interdisciplinary collaboration and which invests in continuing education, and endorses data-driven strategies for opioid stewardship.1,3,50 Although some studies explicitly cite anesthesiologists’ leadership in these domains, the unifying principle is a dedicated pain team committed to bridging the gap between surgery and longer-term recovery.2,53 Meanwhile, the inclusion of psychological support and patient education across many TPS/Cs reflects growing recognition that effective post-surgical pain management extends beyond pharmacology.3,14 Counseling, cognitive-behavioral therapy, and other psychosocial interventions have been associated with greater readiness for tapering, improved mood, and more positive functional outcomes.8,14 These interventions can be critical for patients with high baseline pain anxiety or opioid tolerance, particularly if undertaken as part of a consistent follow-up schedule that addresses both physical and psychosocial challenges.3 On the logistical front, ensuring that patients have regular contact (via in-person visits or telehealth) helps them navigate obstacles such as medication side effects, unresolved pain flares, or concerns about withdrawal.47,50 This structured engagement can lower the risk of patients falling through the cracks of fragmented care.
Discussion
This review sought to clarify the state of the literature on TPS/Cs as an emerging model designed to prevent CPSP and mitigate opioid dependence. Our first research goal/question sought to identify the core components and models of TPS/Cs. A majority of the published reports reviewed here reported on multidisciplinary transitional pain clinics with most reports coming out of North America, in particular TPS/Cs in Toronto, Baltimore, and Salt Lake City. These centers incorporated the services of pain physicians, psychologists/psychiatrists, specialized nurses, physiotherapists, pharmacists, social workers, and other health care personnel to provide personalized care for often complex patients. However, other reports, particularly those from European sites, described TPS/Cs that were often less expansive and often represented continuity-of-care clinics with primarily pain physician and/or psychologist expertise available. We did not identify studies from Asian, African, or South American sources. There was also no data suggesting a superiority of one model over another and so implementation of any form of TPS/C is likely to have merit. Newer technologies such as smart phone apps and implementation of telemedicine technologies are the cutting edge of TPS/C treatment that will need assessment since these may allow expansion of TPS/C cares to remote sites.
Our second goal/question related to TPS/Cs related to the evidence of altered outcomes which support their development and use. An overarching theme observed in these studies was the emphasis on early risk stratification as a predictor of outcomes and as an indication for alterations in management. Namely, the identification of patients who are at heightened risk for CPSP or prolonged opioid use before or shortly after surgery was demonstrated to be predictive of outcome and was utilized for the “personalization” of the provided services. As noted above, TPS/Cs typically engage multidisciplinary teams to address risk factors proactively. Such a strategy contrasts with more traditional approaches wherein acute pain is managed primarily in the hospital, sometimes leaving patients without structured outpatient follow-up once discharged.2 The evidence suggests that when TPS/Cs incorporate diverse modalities, ranging from non-opioid pharmacotherapies and psychosocial interventions to physical therapy, patients are more likely to achieve meaningful tapering of opioids and better long-term functional outcomes.3,4 Unfortunately, as evidenced by the summary of studies given in Table 1, most reports related to TPS/Cs are retrospective in nature and with limited control comparisons. Few employed any prospective strategies and fewer utilized randomization to any treatment groups. As in all pain research there are ethical limitations to assignment to “non-treatment” groups and use of historical comparison groups is often the norm rather than the exception. Despite these methodological limitations, the examined studies have consistently identified that the introduction of TPS/Cs and their additional clinical cares are associated with reductions in opioid use, reductions in pain scores, and improved quality of life measures. Despite these positive indications, key gaps remain in terms of consistency and generalizability. Variation across TPS/C models is notable, spanning differences in team composition, duration of follow-up, and use of adjunct services like psychological counseling or telehealth.10,15 These discrepancies make it challenging to draw universally applicable guidelines about optimum staffing ratios, specific tapering algorithms, or standardized timepoints for patient evaluation.2,53 Moreover, while certain TPS/Cs emphasize early outpatient supervision with robust psychological support, others focus on refining immediate perioperative strategies, such as providing a range of regional blocks and adjuvant medications to reduce opioid requirements.1,4 Each approach has shown merit, yet heterogeneity underscores the need for larger comparative studies to pinpoint the core elements that reliably produce favorable outcomes.
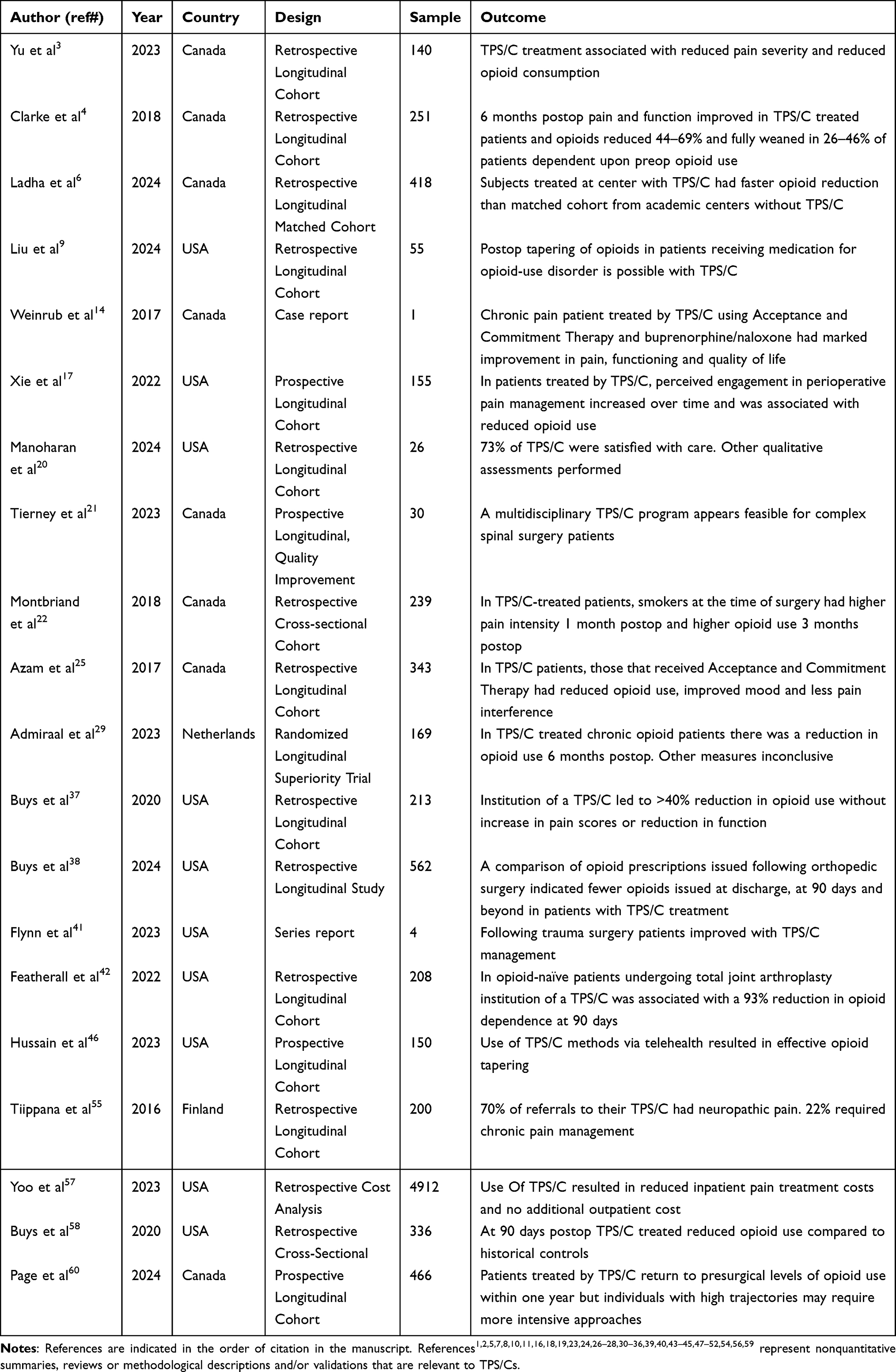 |
Table 1 Summary of Studies of TPS/Cs in Order of Citation |
Our third goal/question in this review was to identify barriers, facilitators and future directions needed for the development and assessment of TPS/Cs/. There is clearly a need for ongoing research to address several unanswered questions. Although many studies report success in reducing opioid consumption and improving pain scores, there are relatively few which conducted rigorous cost analyses or long-term evaluations beyond six to twelve months.10,53 More extensive economic models or randomized trials could elucidate whether TPS/Cs ultimately offset their operating costs by lowering hospital readmissions, emergency visits, or the burden of chronic opioid use.49,52 A common sense result of demonstrating cost savings in association with the implementation of TPS/Cs is that there would be more financial support for TPS/Cs. One can make the argument that improving patient care through use of TPS/Cs is the “right” thing to do, but generally this argument falls upon deaf ears in the financial halls of health institutions. However, history related to the cost effectiveness of hospice care61 in the United States demonstrated that once cost savings were definitively demonstrated, the most resistant administrators demanded its implementation. One of the additional future directions for TPS/Cs relate to adapting their protocols for diverse populations. For instance, pediatric versus geriatric patients or those with complex comorbidities35–38 may need specialized cares. Tailoring transitional services to meet specialized needs might necessitate additional training or resource allocation, but these modifications could further extend the benefits of TPS/Cs. As noted before, future directions need also include an assessment of technologies that allow for TPS/C related cares while at home. These include the use of smart phone apps and the expansion of telemedicine services.
Certain methodological constraints deserve mention. The lack of uniform outcome reporting across studies made it challenging to aggregate data quantitatively or identify definitive causal relationships.2,53 Most available evidence originates from single-center experiences with limited sample sizes, restricting generalizability. Despite these limitations, the converging evidence on opioid tapering, CPSP prevention, and patient satisfaction indicates that TPS/Cs are poised to fill a crucial gap in perioperative care.
Conclusions
In summary, the existing literature reviewed here suggests that TPS/Cs can effectively bridge acute postoperative pain management with sustained long-term care, particularly for patients at higher risk of CPSP and opioid misuse. TPS/Cs come in many forms. The most common reports suggest that success hinges on a proactive, multidisciplinary framework, robust institutional support, and consistent monitoring protocols that target both pain control and responsible opioid stewardship. As healthcare systems worldwide grapple with rising pain management challenges, well-integrated TPS/Cs appear to offer a promising avenue for the desired outcomes of fostering safer surgical recoveries and mitigating chronic opioid dependence. The barriers which exist for development of TPS/Cs primarily relate to the need for institutional support. Further research, including larger trials and cost–benefit analyses, will help refine these models, clarify best practices, and expand their reach in diverse clinical settings.
Acknowledgments
Nothing to acknowledge.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Huang A, Katz J, Clarke H. Ensuring safe prescribing of controlled substances for pain following surgery by developing a transitional pain service. Pain Manag. 2015;5:97–15. doi:10.2217/pmt.15.7
2. Mikhaeil J, Ayoo K, Clarke H, Wąsowicz M, Huang A. Review of the transitional pain service as a method of postoperative opioid weaning and a service aimed at minimizing the risk of chronic post-surgical pain. Anaesthesiol Intensive Ther. 2020;52:148–153. doi:10.5114/ait.2020.96018
3. Yu HC, Kleiman V, Kojic K, et al. Prevention and management of chronic postsurgical pain and persistent opioid use following solid organ transplantation: experiences from the Toronto general hospital transitional pain service. Transplantation. 2023;107:1398–1405. doi:10.1097/TP.0000000000004441
4. Clarke H, Azargive S, Montbriand J, et al. Opioid weaning and pain management in postsurgical patients at the Toronto general hospital transitional pain service. Can J Pain. 2018;1:236–247. doi:10.1089/24740527.2018.1501669
5. Katz J, Weinrib A, Fashler SR, et al. The Toronto general hospital transitional pain service: development and implementation of a multidisciplinary program to prevent chronic postsurgical pain. J Pain Res. 2015;8:695–702. doi:10.2147/JPR.591924
6. Ladha KS, Vachhani K, Gabriel G, et al. Impact of a transitional pain service on postoperative opioid trajectories: a retrospective cohort study. Reg Anesth Pain Med. 1975;202; 49:650–655. doi:10.1136/rapm-2023-104709
7. Klimke R, Ott A, Romero CS, et al. Transitional pain service: an update. Curr Pain Headache Rep. 2024;28:457–464. doi:10.1007/s11916-024-01239-1
8. Philips BD, Liu SS, Wukovits B, et al. Creation of a novel recuperative pain medicine service to optimize postoperative analgesia and enhance patient satisfaction. HSSJ. 2010;6:61–65. doi:10.1007/s11420-009-9135-6
9. Liu O, Leon D, Gough E, Speed T, Hanna M, Jaremko K. A retrospective analysis of perioperative medications for opioid-use disorder and tapering additional postsurgical opioids via a transitional pain service. Br J Clin Pharmacol. 2024;90:3010–3027. doi:10.1111/bcp.16118
10. Dunworth S, Barbeito A, Nagavelli H, et al. Transitional pain service: optimizing complex surgical patients. Curr Pain Headache Rep. 2024;28:141–147. doi:10.1007/s11916-023-01204-4
11. Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int. J Soc Res Methodol. 2005;8:19–32. doi:10.1080/1364557032000119616
12. Vanneman MW, Kiwakyou LM, Harrison TK, Mariano ER. Heartfelt healing: charting new trajectories in postsurgical pain. Anesth Analg. 2024;138:1187–1191. doi:10.1213/ANE.0000000000006871
13. Godwin RC, Bryant AS, Wagener BM, et al. IRB-draft-generator: a generative AI tool to streamline the creation of institutional review board applications. SoftwareX. 2024;25:101601. doi:10.1016/j.softx.2023.101601
14. Weinrib AZ, Burns LC, Mu A, et al. A case report on the treatment of complex chronic pain and opioid dependence by a multidisciplinary transitional pain service using the ACT matrix and buprenorphine/naloxone. J Pain Res. 2017;10:747–755. doi:10.2147/JPR.s124566
15. Wang J, Doan LV, Axelrod D, et al. and the NCATS Trial Innovation Network. Optimizing the Use of Ketamine to Reduce Chronic Postsurgical Pain in Women Undergoing Mastectomy for Oncologic Indication: study Protocol for the KALPAS multicenter randomized controlled trial. Trials. 2024;25:67. doi:10.1186/s13063-023-07884-y
16. Hanna MN, Speed TJ, Shechter R, et al. An innovative perioperative pain program for chronic opioid users: an academic medical center’s response to the opioid crisis. Am J Med Qual. 2018;33:1–9. doi:10.1177/1062860618777298
17. Xie A, Hsu YJ, Speed TJ, et al. Patient engagement and prescription opioid use in perioperative pain management. J Opioid Manag. 2022;18:421–433. doi:10.5055/jom.2022.0736
18. Speed TJ, Hanna MN, Xie A. The personalized pain program: a new transitional perioperative pain care delivery model to improve surgical recovery and address the opioid crisis. Qual Manag Health Care. 2024;33:61–63. doi:10.1097/QMH.0000000000000450
19. Edwards D. Building a transitional pain service: vanderbilt experience. ASRA Newsletter. 2021;46. doi:10.52211/asra020121.013
20. Manoharan D, Xie A, Hsu YJ, et al. Patient experiences and clinical outcomes in a multidisciplinary perioperative transitional pain service. J Pers Med. 2024;14:31. doi:10.3390/jpm14010031
21. Tierney S, Magnan M-C, Zahrai A, McIssac D, Poulin P, Stratton A. Feasibility of a multidisciplinary transitional pain service in spine surgery patients to minimise opioid use and improve perioperative outcomes: a quality improvement study. BMJ Open Qual. 2023;
22. Montbriand JJ, Weinrib AZ, Azam MA, et al. Smoking, pain intensity, and opioid consumption 1-3 months after a major surgery: a retrospective study in a hospital-based transitional pain service. Nicotine Tob Res. 2018;20:1144–1151. doi:10.1093/ntr/ntx094
23. Fashler SR, Pagé MG, Svendrovski A, et al. Predictive validity and patterns of change over time of the sensitivity to pain traumatization scale: a trajectory analysis of patients seen by the transitional pain service up to two years after surgery. J Pain Res. 2022;15:2587–2605. doi:10.2147/JPR.S370497
24. Weinrib AZ, Azam MA, Birnie KA, Burns LC, Clarke H, Katz J. The psychology of chronic post-surgical pain: new frontiers in risk factor identification, prevention, and management. Br J Pain. 2017;11:169–177. doi:10.1177/2049463717720636
25. Azam MA, Weinrib AZ, Montbriand J, et al. Acceptance and commitment therapy to manage pain and opioid use after major surgery: preliminary outcomes from the Toronto general hospital transitional pain service. Can J Pain. 2017;1:37–49. doi:10.1080/24740527.2017.1325317
26. Moka E, Aguirre JA, Sauter AR, Lavand’homme P. Chronic postsurgical pain and transitional pain services: a narrative review highlighting european perspectives. Reg Anesth Pain Med. 2025;50:205–212. doi:10.1136/rapm-2024-105614
27. Lomanowska AM, Tahir R, Choo C, et al. Knowledge translation initiatives at the transitional pain service: insights from healthcare provider outreach and patient education. BMC Health Serv Res. 2025;25:169. doi:10.1186/s12913-025-12301-y
28. Kojic K, Clarke H. Important considerations with respect to reducing the transition from acute to persistent postoperative pain. Expert Opin Pharmacother. 2021;22:779–782. doi:10.1080/14656566.2021.1892073
29. Admiraal M, Hermanns H, Hermanides J, et al. The effectiveness of a transitional pain service in patients undergoing surgery with an increased risk of developing chronic postsurgical pain (trust study): a randomized clinical trial. J Clin Anesth. 2023;91:111262. doi:10.1016/j.jclinane.2023.111262
30. Huang A, Azam A, Segal S, et al. Chronic postsurgical pain and persistent opioid use following surgery: the need for a transitional pain service. Pain Manag. 2016;6:435–443. doi:10.2217/pmt-2016-0004
31. Terkawi AS, Ottestad E, Altirkawi OK, et al. Transitional pain medicine; new era, new opportunities, and new journey. Anesthesiol Clin. 2023;41:383–394. doi:10.1016/j.anclin.2023.03.007
32. Katz J, Weinrib AZ, Clarke H. Chronic postsurgical pain: from risk factor identification to multidisciplinary management at the Toronto general hospital transitional pain service. Can J Pain. 2019;3:49–58. doi:10.1080/24740527.2019.1574537
33. Lavand’homme P. Transition from acute to chronic pain after surgery. Pain. 2017;158(4 Suppl 1):S50–S54. doi:10.1097/jpain.0000000000000809
34. Clarke H, Poon M, Weinrib A, Katznelson R, Wentlandt K, Katz J. Preventive analgesia and novel strategies for the prevention of chronic post-surgical pain. Drugs. 2015;75:339–351. doi:10.1007/s40265-015-0365-2
35. Haynes N, Mclean C, Collins J, de Lima J. Persistent post-operative pain in children – an argument for a transitional pain service in pediatrics. Pain Manag Nurs. 2022;23:784–790. doi:10.1016/j.pmn.2022.06.004
36. Isaac L, Rosenbloom BN, Tyrrell J, Ruskin DA, Birnie KA. Development and expansion of a pediatric transitional pain service to prevent complex chronic pain. Front Pain Res. 2023;4:1173675. doi:10.3389/fpain.2023.1173675
37. Buys MJ, Bayless K, Romesser J, et al. Multidisciplinary transitional pain service for the veteran population. Fed Pract. 2020;37:70–75. doi:10.12788/fp.0053
38. Buys MJ, Anderson Z, Bayless K, et al. Postsurgical Opioid prescribing among veterans using community care for orthopedic surgery at non-VA hospitals compared to a VA hospital with a transitional pain service: a retrospective cohort study. Reg Anesth Pain Med. 2025;50:531–537. doi:10.1136/rapm-2023-105162
39. Meng H, Hanlon JG, Katznelson R, et al. The prescription of medical cannabis by a transitional pain service to wean a patient with complex pain from opioid use following liver transplantation: a case report. Can J Anesth. 2016;63:307–310. doi:10.1007/s12630-015-0525-6
40. Blanco R, Ansari T. Transitional pain services updates and a novel service for the obstetric population. Curr Opin Anesthesiol. 2024;37:513–519. doi:10.1097/ACO.0000000000001417
41. Flynn HK, Manoharan D, Hsu YJ, et al. A multidisciplinary transitional pain service to improve pain outcomes following trauma surgery: a preliminary report. Scand J Pain. 2023;23:613–619. doi:10.1515/sjpain-2022-0083
42. Featherall J, Anderson JT, Anderson LA, et al. A multidisciplinary transitional pain management program is associated with reduced opioid dependence after primary total joint arthroplasty. J Arthroplasty. 2022;37:1048–1053. doi:10.1016/jarth.2022.02.032
43. Tong L, Solla C, Staack JB, May K, Tran B. Perioperative pain management for thoracic surgery: a multilayered approach. Semin Cardiothorac Vasc Anesth. 2024;28:215–229. doi:10.1177/10892532241235750
44. Slepian PM, Peng M, Janmohamed T, et al. Engagement with manage my pain mobile health application among patients at the transitional pain service. Digital Health. 2020;6:1–7. doi:10.1177/2055207620962297
45. Hunter OO, Mariano ER, Harrison TK. Leveraging video telehealth for the transitional pain service in response to COVID-19. Reg Anesth Pain Med. 2021;46:460–461. doi:10.1136/rapm-2020-101742
46. Hussain M, Norgeot B, Zaafran A, et al. Virtual transitional pain service delivered via telehealth is effective in preventing new and persistent opioid use amongst post-surgical spine patients. medRxiv. 2023. doi:10.1101/2023.08.18.23294272
47. Skoric J, Lomanowska AM, Janmohamed T, et al. Predicting clinical outcomes at the Toronto general hospital transitional pain service via the manage my pain app: machine learning approach. JMIR Med Inform. 2025:
48. Al-Saidi I, Russell A, Dizdarevic A. The acute perioperative pain service: impact, organization, and future directions. Curr Pain Headache Rep. 2023;27:399–405. doi:10.1007/s11916-023-01133-2
49. Sun EC, Mariano ER, Narouze S, et al. Making a business plan for starting a transitional pain service within the US healthcare system. Reg Anesth Pain Med. 2021;46:727–731. doi:10.1136/rapm-2021-102669
50. Clarke H, Waisman A, Aternali A, et al. Ten years of transitional pain service research and practice: where are we and where do we go from here? Reg Anesth Pain Med. 2025;50:188–203. doi:10.1136/rapm-2024-105609
51. Clarke H. Transitional pain medicine: novel pharmacological treatments for the management of moderate to severe postsurgical pain. Expert Rev Clin Pharmacol. 2016;9:345–349. doi:10.1586/17512433.2016.1129896
52. Zubieta CS, Shabet C, Lin J, et al. Financial model for a transitional pain service at a large tertiary academic center in the USA. Reg Anesth Pain Med. 2025;50:1–4. doi:10.1136/rapm-2023-104992
53. Sand AE, Powell TE, Marry HT, et al. The pre-operative evaluation clinic: an underutilized service in optimizing analgesic outcomes in patients on buprenorphine, methadone, and naltrexone for substance use disorder or chronic pain. J Pain Res. 2024;17:3267–3275. doi:10.2147/JPr.5471160
54. Rim F, Liu SS, Kelly M, et al. Preoperative pain screening and optimization by a perioperative pain service to support complex surgical patients: no patient left behind. Br J Anaesth. 2024;132:437–439. doi:10.1016/j.bja.2023.11.024
55. Tiippana E, Hamunen K, Heiskanen T, Nieminen T, Kalso E, Kontinen VK. New approach for treatment of prolonged postoperative pain: APS out-patient clinic. Scand J Pain. 2016;12:19–24. doi:10.1016/j.sjpain.2016.02.008
56. Admiraal M, Hermanides J, Hollmann MW, Hermanns H. Evaluation of health care providers satisfaction with the implementation of a transitional pain service. J Clin Med. 2023;12:537. doi:10.3390/jcm12020537
57. Yoo M, Buys MJ, Nelson RE, et al. Effect of multidisciplinary transitional pain service on health care use and costs following orthopedic surgery. Fed Pract. 2023;40:418–425a. doi:10.12788/fp.0438
58. Buys MJ, Bayless K, Romesser J, et al. Opioid use among veterans undergoing major joint surgery managed by a multidisciplinary transitional pain service. Reg Anesth Pain Med. 2020;45:847–852. doi:10.1136/rapm-2020-101797
59. Shechter R, Speed TJ, Blume E, et al. Addressing the opioid crisis one surgical patient at a time: outcomes of a novel perioperative pain program. Am J Med Qual. 2020;35:5–15. doi:10.1177/1062860619851170
60. Pagé MG, Katz J, Darville R, et al. One-year opioid consumption trajectories among individuals receiving multidisciplinary postsurgical care: a single-center observational study from the Toronto general hospital transitional pain service. Reg Anesth Pain Med. 2024;50:542–552. doi:10.1136/rapm-2024-105344
61. Aldridge M, Brody A, May P, Moreno J, McKendrick K, Li L. Hospice saves costs for families: evidence from 16 years of medicare survey data. Health Serv Res. 2021;56(Suppl 2):6–7. doi:10.1111/1475-6773.13720
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.