Back to Journals » Risk Management and Healthcare Policy » Volume 16
Transitional Care in Patients with Heart Failure: A Concept Analysis Using Rogers’ Evolutionary Approach
Authors Liu S, Xiong XY, Chen H, Liu MD, Wang Y, Yang Y, Zhang MJ, Xiang Q
Received 30 June 2023
Accepted for publication 22 September 2023
Published 6 October 2023 Volume 2023:16 Pages 2063—2076
DOI https://doi.org/10.2147/RMHP.S427495
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Si Liu,1,2 Xiao-yun Xiong,2 Hua Chen,1 Meng-die Liu,1 Ying Wang,1 Ying Yang,1 Mei-jun Zhang,1 Qin Xiang1
1School of Nursing, Nan Chang University, Nan Chang, Jiang Xi, People’s Republic of China; 2Nursing Department, the Second Affiliated Hospital of Nan Chang University, Nan Chang, Jiang Xi, People’s Republic of China
Correspondence: Xiao-yun Xiong, Nursing Department, the Second Affiliated Hospital of Nan Chang University, Min de Road #, Nan Chang, 330006, People’s Republic of China, Tel +86-791-8627-4550, Email [email protected]
Objective: The purpose of this study was to clarify the concept of transitional care in patients with heart failure.
Background: Transitional care is increasingly being applied in patients with heart failure, but the concept of transitional care in heart failure patients is not uniform and confused with other definitions, which limits further research and practice on transitional care for these patients.
Design: Rodgers’ evolutionary concept analysis.
Methods: A comprehensive literature search was conducted using the PUBMED, EMBASE, EBSCO, Chinese Biological Medicine (CBM), CNKI, and WANFANG databases (up to January 26, 2023). We used Rodgers’ evolutionary concept analysis method to identify related concepts, attributes, antecedents, and consequences of transitional care in patients with heart failure.
Results: A total of 33 articles were included. The following attributes belonging to transitional care in patients with heart failure were extracted from the literature: self-care, multidisciplinary collaboration, and information transmission. The antecedents were patients’ health status, the health literacy of patients and caregivers, the role functions of the main implementer and social and medical resources. Consequences were separated into two categories: patient-centered health outcomes (all-cause mortality, health-related quality of life, discharge preparedness, self-care behaviors, satisfaction of patients) and healthcare utilization outcomes (hospital readmission, length of hospital stay, emergency department visits).
Conclusion: This study found that transitional care in heart failure patients is a systemic care process during a vulnerable period that improves patient self-management and coordination between hospital resources and social support systems for continuous management to promote smooth patient transitions between different locations. This concept analysis will inform healthcare providers in designing evidence-based interventions and quality improvement strategies to ensure that transition processes lead to desired outcomes. In addition, this study will also be helpful for developing specific assessment tools to identify patients with HF who need transitional care.
Keywords: concept analysis, heart failure, transitional care, self care, collaboration
Introduction
Heart failure (HF) is a complex clinical syndrome caused by a significant decrease in cardiac output volume due to the structural or functional impairment of ventricular filling or the ejection of blood, which cannot meet the metabolic requirements of the body.1 Similar to most patients with chronic diseases, patients with heart failure typically have multiple comorbidities, complex medication regimens and limited self-management skills. Therefore, HF is characterized by a high risk of morbidity, a high risk of deterioration, a high risk of mortality and the highest risk of early readmission. It has been reported that approximately 64.3 million people worldwide suffer from heart failure,2 and the readmission rates at 30 days and 6 months among HF patients are as high as 25% and 50%, respectively. Within five years of diagnosis, only one in five patients with HF is still alive, and the expenditure of treatment is US $108 billion yearly.3 It is well known that rehospitalization imposes a significant burden on the medical system and individuals; however, recurrent hospitalization due to chronic heart failure (CHF) has become an important epidemiological feature of the disease.4,5 A total of 75% of early-phase readmissions are preventable by reporting, as they mainly result from incomplete hospital management and fragmented care, for instance, the lack of physician adherence to guidelines, patient unawareness of CHF symptom exacerbations, nonadherence to medical therapy and exercise rehabilitation, in addition to the lack of detailed discharge records and suggestions for primary care physicians to develop follow-up schemes.6,7 Therefore, it is an urgent problem to reduce the readmission rate of patients with heart failure worldwide.
Transitional care is a broad range of time-limited services designed to ensure continuity of care and facilitate the smooth transfer of vulnerable individuals affected by any change in care settings or caregivers from one setting to another.8 The emergence of transitional care is an innovative solution designed to address the negative impact of the frequent use of health resources and to improve the integration and continuity of all stages of care for chronic disease patients. At present, transitional care interventions are widely known in the US, Japan and Hong Kong and have been shown to reduce emergency department visits, readmissions and mortality in HF patients. With the increasing application in patients with heart failure, the nature and practice of transitional care is evolving and enriching; nevertheless, a standardized definition has not yet been established, and there is no consensus on how long the transitional care period should last and no standard classification scheme for transitional care services, which limits further research on transitional care in patients with heart failure.
This study used Rodgers’ evolutionary approach to clarify the concept of transitional care by analyzing its application in different studies related to HF to design evidence-based interventions and quality improvement strategies to ensure that transition processes produce desired outcomes.
Methods
Rodgers’ evolutionary conceptual analysis9 was selected to clarify the concept of transitional care for patients with heart failure. Based on the classic conceptual analysis of Walker and Avant, this method (Box 1) improved the representativeness of literature selected for analysis through systematic retrieval and analyzed the development and changes of specific concepts over time.
 |
Box 1 Rodgers’ Evolutionary Method |
Data Sources
We searched the PUBMED, EMBASE, EBSCO, Chinese Biological Medicine (CBM), CNKI, and WANFANG databases to identify relevant reports and manually searched articles from the reference lists of retrieved articles to assemble a comprehensive collection of records about transitional care in patients with HF (up to January 26, 2023). The search terms used were “heart failure”, “heart failure, diastolic”, “heart failure, systolic”, “cardiac failure”, “chronic heart failure”, “congestive heart failure”, “discharge planning”, “transitional care”, “patient discharge”, “continuity of patient care”, and “patient transfer” (Supplementary Material 1). Inclusion criteria were as follows: (1) the subjects were patients with heart failure; (2) the study was related to the concept’s attributes, evolution, antecedents, consequences and relevance to the topic; and (3) studies published in English and Chinese only. Exclusion criteria were as follows: (1) full text was not available; (2) gray literature, texts published in non-peer-reviewed journals, letters to the editor and study protocols; (3) studies that did not have predischarge and postdischarge interventions for HF patients; and (4) patients who did not return to the home after discharge.
We retrieved 3857 records through database searches, and two researchers independently reviewed the studies. After removing duplicates, we found 3620 articles, 3524 of which we excluded by reviewing the title and abstract using general criteria, and 96 full-text articles were assessed for eligibility. We then excluded 65 studies for the following reasons: studies including subjects who were not heart failure patients (n=5); studies in which the results were presented as abstracts (n=12); study protocols (n=3); studies for which the full-text was not available (n=1); articles published in French (n=1); articles that were not relevant to the topic (n=20); articles that were not based on predischarge and postdischarge interventions (n=17); studies in which the patients did not return to home after discharge (n=3); studies with incomplete descriptions of interventions (n=1); and articles that were not peer-reviewed (n=2). Two articles were obtained from the reference lists of retrieved records. We subjected the resulting 33 articles to concept analysis. Figure 1 shows the specific flow chart. For reasons for the final exclusion of 65 studies, see Supplementary Material 2.
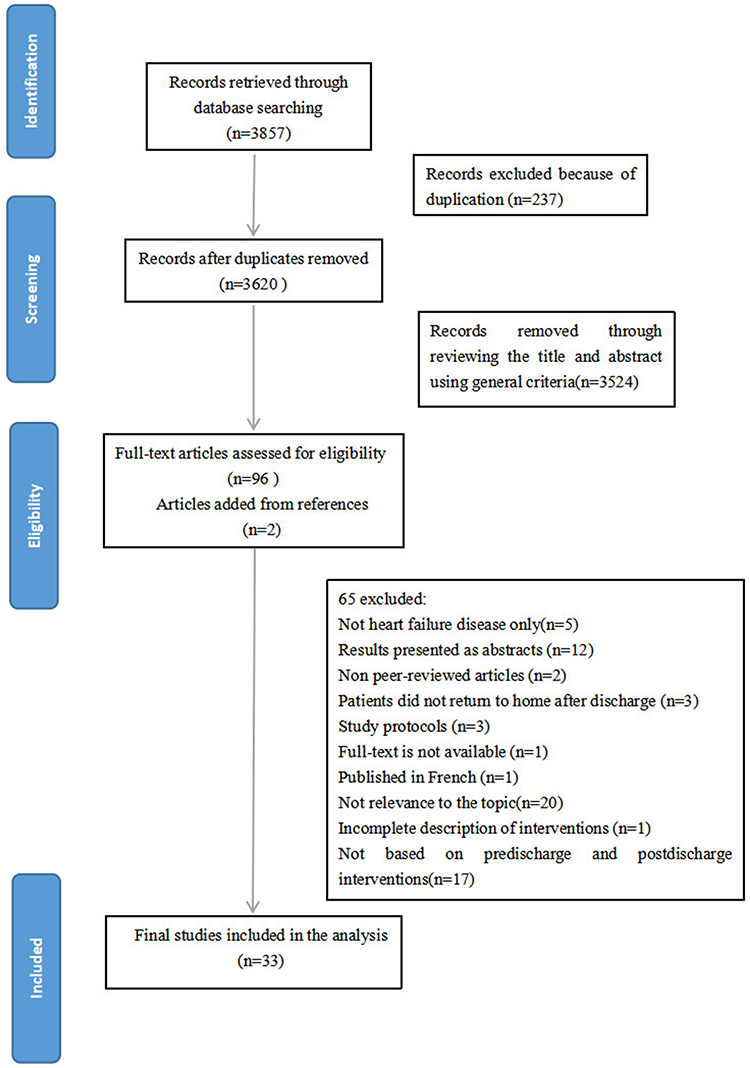 |
Figure 1 Flow diagram for identification of studies for inclusion in concept analysis. |
Results
Evolving Definition and Use of the Concept
The term “transitional” has as an adjective meaning: marked by transition: involving, providing, or consisting of a passage, movement, or change from one state, condition, subject, place, etc., to another.10 In the PubMed subject word tree structure, “transitional care” is the subjunctive of “continuity of patient care”, meaning health care provided during a transition to a different mode of care.11 In 1947, Forest Harriet et al at the University of Pennsylvania initially explored establishing cooperation between hospitals and communities and made plans for the early transfer of patients from hospitals to communities or homes for continued nursing care. In this research, they underlined referral as a continuation of nursing care.12 Subsequently, discharge planning was advocated routinely. Discharge planning used to be seen as something that should be done at a certain point in time while a patient was in hospital. The consideration of the patient as a whole and social health care management paid attention to the entire life cycle of nursing to expand the connotation of “discharge planning”. In this view, the definition of transitional care evolved from discharge planning. In 1966, “transitional care” first appeared in the literature, which described the transitional care nursery provided by the hospital for newborns to adjust to a new extrauterine environment.13 In the 1980s, “transitional care services” emerged, which served to catch post acute patients who were being discharged more quickly (who were possibly sicker), were intended to keep patients from entering an acute care facility or to return to the community; partly, the connotation of transitional care services was broadened by traditional discharge planning to push the early discharge of patients.14 Brooten et al initially used the transitional care model, which combined a discharge plan with routine home follow-up care guided by nurse specialists for low birth weight infants, and then gradually used it in other vulnerable groups.15 In 1995, Rich et al used a nurse-conducted multidisciplinary intervention that included comprehensive education for patients and family, early discharge planning, individual dietary and medical instructions, social-service counseling and intensive follow-up after discharge.16 To our knowledge, this was the first time that transitional care was used in heart failure patients. The vulnerability of the intervention population and the complexity of the interventions were features of transitional care in this report and resulted in more favorable outcomes. In 2002, Harrison and her colleagues designed a model of hospital-to-home transition that was implemented by the usual nurse providers rather than a clinical nurse specialist, and the defined characteristics of transitional care in heart failure patients were the use of a structured, comprehensive, evidenced-based project for counseling and educating and cooperation between the hospital and home nurses and patients to improve self-management and promote health.17 In 2004, Naylor et al described a “transitional care intervention” in heart failure patients, including advanced practice nurse (APN)-directed discharge planning and a routine home follow-up protocol.18 The unique feature of this model was that in hospital and in the home, the same APN developed and applied personal discharge planning. Of the transitional care interventions reviewed, most began immediately after admission and were maintained for a period of time after discharge, including early assessment after admission, patient education and consultation, medication reconciliation, early follow-up after discharge and handoff to posthospital providers.19 Although in previous research, case management was applied, the difference between chronic disease management and transitional care was that transitional care focused on the vulnerable period and a common theme related to the prevention of readmission. Currently, some interventions of transitional care in HF patients stress postdischarge management, but assessing and identifying patients at risk at admission and establishing a comprehensive protocol is essential.
Attributes
Attributes are characteristics of a concept that allow people to discern if the concept is present in a situation.9 It is important to recognize the key attributes of a concept to distinguish it from other concepts.
Self-Care
Due to the long disease course and complex complications, the self-care ability of HF patients plays an important role in the process of disease progression. It is emphasized that the final foothold of the transitional care operation mechanism in patients with heart failure is to improve their self-management skills. Regardless of which transitional care service mode is implemented, the goal is to increase a patient’s understanding of their condition and its links to self-care and promote the involvement of other people in this self-care to enhance compliance with drug therapy, symptom management, dietary care and exercise rehabilitation.20,21 Hoover and his colleagues suggested that22 early recognition of significant changes in health status and appropriate responses to symptoms by HF patients are crucial to successfully reducing HF readmissions. Yu et al described that23 the key element affecting the implementation of transitional care services is self-management in different cultural contexts, and health-related knowledge increases the likelihood of adherence to treatment to improve the health outcomes of individuals through self-efficacy.
Multidisciplinary Collaboration
Multiprofessional teamwork is one of the common themes from existing transitional-care models applied to patients with HF summarized by Albert and her colleagues.24 It is necessary for patients to implement comprehensive multidisciplinary care plans from the beginning to the end of their healthcare journey. Transitions are highly vulnerable episodes, and transitional care for patients with HF is a focused, coordinated and integrated process, which makes it difficult for a single provider alone to offer care; interdisciplinary cooperation is most effective.25 Multiple health care providers, such as physicians, nurses, pharmacists, physiotherapists, dieticians, and social workers, encourage patients and their caregivers to work cohesively to achieve coordinated high-quality care.
Information Transmission
Information transmission in transitional care includes education, communication and collaboration. HF education is tailored and consists of group or individual counseling, skills training, discharge guidance and follow-up arrangements. It is very urgent for HF patients to understand three questions26 at discharge: “What is my diagnosis? What is my medication? When and where is my next appointment”? A coordinator acts as “the hub” in a multidisciplinary team by communicating and collaborating with patients, caregivers and other health care providers, in addition to a link between the hospital and community to promote safe and early patient discharge. During the transition from hospital to home, effective communication is essential to relieve HF patients’ anxieties and worries regarding sudden medical resource removal. To ensure complete and clear information transmission during referral, a checklist or detailed transfer letter is a useful tool for primary care physicians receiving useful discharge summaries to develop subsequent treatment and early follow-up schemes.
Antecedents
Antecedents are events or phenomena that exist generally for the concept to occur.9 Transitional care in patients with HF is preceded by (1) patients’ health status; (2) the health literacy of patients and caregivers; (3) the role functions of the main implementer; and (4) social and medical resources.
Patients’ Health Status
Studies have shown that the decision to implement transitional care for patients with heart failure depends on the patients’ health status.19 Vedel and Khanassov indicated that recurrent attacks of CHF result in frequent use of health care services,7 and Hoover et al described that older adult patients with complex chronic conditions tend to be repeatedly readmitted and experience fragmented care.22 Therefore, it is emphasized that patients with complex treatment procedures and readmission risks are screened within 24 hours of admission. Elderly patients (≥65 years of age) and those with comorbidities, polypharmacy, highest NYHA grade, previous readmission and acquired weakness are the right population.27,28 Psychological discharge readiness is also helpful for patients with HF who are transitioning from the hospital to home, meaning that the patients’ own perspectives of discharge are consistent with those of physicians.
The Health Literacy of Patients and Caregivers
Health literacy is defined as the degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to make appropriate health decisions.29 Evangelista and her colleagues reported that inadequate health literacy is associated with a lack of adherence to discharge instructions, poor medication compliance, and increased readmission and mortality.30 Thus, developing core educational content for heart failure patients in transitional care should carefully consider the patient/family’s cognitive level, education level, lifestyle, values, habits, priorities, and the health expectations.
The Role Functions of the Main Implementer
Nurses with multiple roles are important in the care of patients with HF. They assume the roles of estimator, educator, coordinator, practitioner and evaluator, which make them ideal coleaders in a multidisciplinary transitional care team.31 Tingley et al reported that nurse-driven high-intensity transitional care interventions were identified as the most effective in reducing short-term readmission.25 As pharmacists have the unique ability to provide medication reconciliation and medication education, their core role in improving transitional care services has also been investigated in patients with HF.32 Garnier and her colleagues described that extending pharmacist’s role from professional guidance to the delivery of continuity of care reduces the morbidity and mortality associated with heart failure.26 Patients may feel ashamed that they cannot afford their medications. At this time, a sense of responsibility, empathy, and a nonjudgmental approach from the main executor are critical.33
Social and Medical Resources
The requirement for a decreased readmission rate and reduction in cost for HF patients push health care professionals to think about how to deliver the highest quality of care in the most efficient way. Naylor et al summarized that services for older adults living longer with complex health and social needs remain fragmented, expensive and occasionally inappropriate.34 A variety of transitional care programs and services have been established. Moreover, prior studies have suggested that patients and caregivers attribute failed transitions to abandonment by the health care system after discharge and barriers such as lack of transportation and home care expense deficiency.35 Allen et al suggested that more attention should be paid to low socioeconomic populations during the post-hospital transition process.27 In addition to the component of transitional care involving follow-up and management by primary care physicians, community resources are considerable. In addition, some medical equipment, such as implantable cardioverter defibrillators and communication facilities, may be used as secondary prevention in patients with HF, facilitating the implementation of safe transitional care.1
Consequences
Consequences describe the situations that follow the “occurrence” of the concept.36 Outcomes following transitional care are related to (1) patient-centered health outcomes and (2) healthcare utilization outcomes. The consequences extracted from the literature are listed in Table 1, along with the attributes and antecedents.
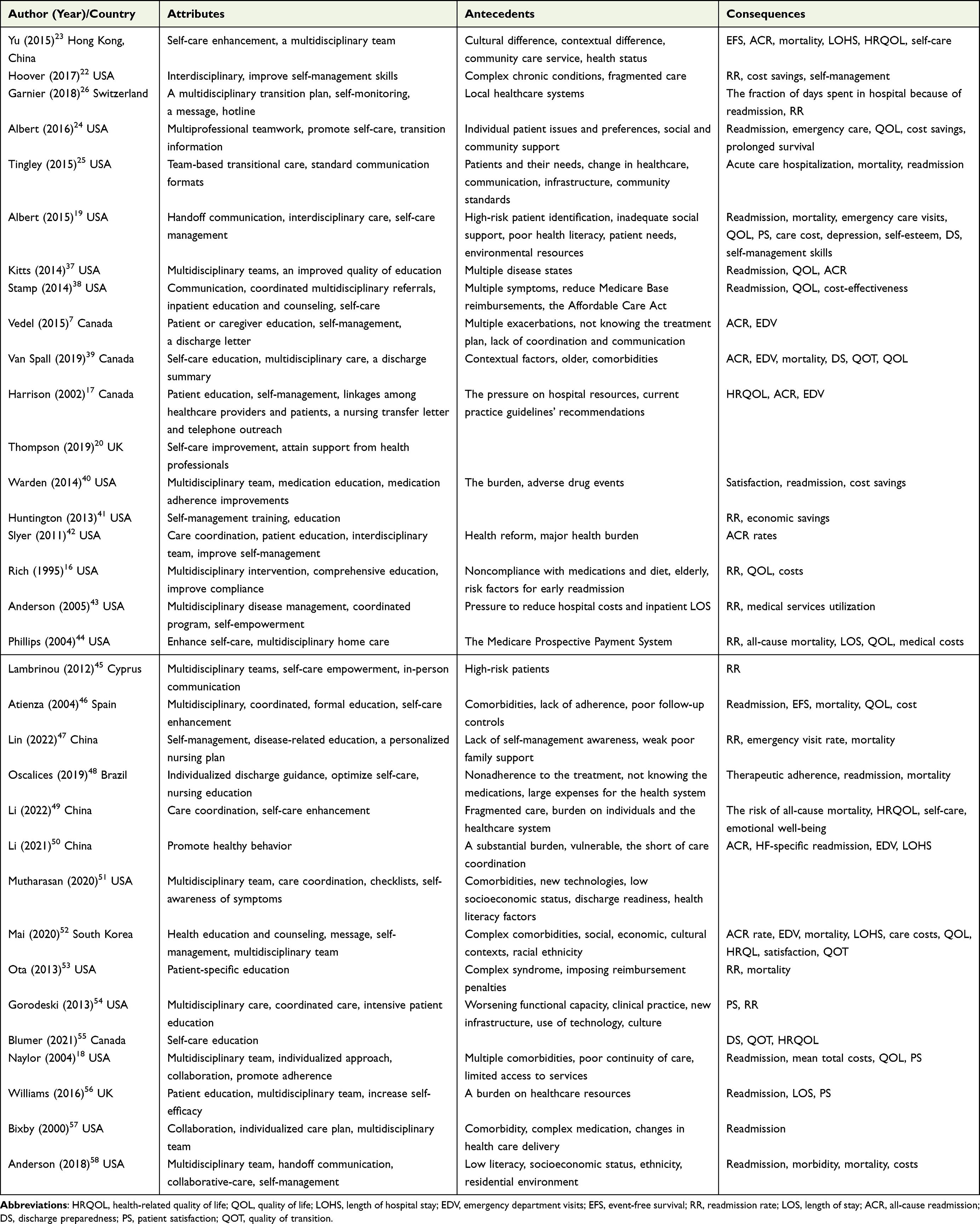 |
Table 1 Characteristics of the Included Studies |
Patient-Centered Health Outcomes
Li and her colleagues reported that nurse-led hospital-to-home transitional care interventions can reduce the risk of all-cause mortality, improve health-related quality of life, and enhance self-care behaviors in patients with heart failure.49 Moreover, transitional care improves medication knowledge, discharge preparedness and the satisfaction of patients.19,39
Healthcare Utilization Outcomes
Hospital readmission was the most common indicator analyzed in many articles. Subsequently, the length of hospital stay and the number of emergency department visits were decreased, and transitional care also showed cost-effectiveness.7,46,50,52 Ota and colleagues assessed 30-day and 90-day readmission rates in HF patients before and after enrollment in the transitional care program, and showed that the program was successful in reducing the number of readmissions regardless of causes.53 Atienza et al reported that the transitional care intervention has potential capacity to reduce management costs, the overall cost of care was reduced in €2063 per patient in the transitional care group.46
Related Concept
Discharge Planning
Discharge planning59 is a centralized, coordinated and multidisciplinary process, and through the cooperation of health professionals, patients and their families, patients can receive continuous care after discharge. The definition of transitional care can be seen as evolving from discharge planning, and it is a method to achieve transition.
Continuity of Care
Continuity of care can be defined as the degree to which a series of discrete healthcare events is experienced as coherent, connected and consistent with a patient’s medical needs and personal context.60 It stresses continuity of caring behavior that is carried out prior to admission and predischarge and postdischarge management. Transitional care focuses on continuity of care during transition and transfer.
Model Case
Mr. Lee, a 72-year-old man, had a history of chronic heart failure disease, hypertension and long-term oral drug treatment. He was hospitalized for chest distress and edema.
His wife and his daughter accompanied him during his admission assessment. After a complete medical history was obtained, a specialist nurse in the ward talked with him and his family to learn which knowledge related to disease and self-management skills, such as self-measured blood pressure, drug use, sodium restriction, dietary care and exercise rehabilitation, he had mastered. The specialist nurse also asked about hypertension management in the local place where Mr. Lee resides. After overall assessment, the specialist nurse contacted the multidisciplinary team who provided coordinated services and made a comprehensive discharge plan. Moreover, the specialist nurse offered intensive education and consultation to improve the patient’s self-care. Mr. Lee’s physical stability returned following his treatment, and he expressed that he felt better. Before discharge, the nurse reaffirmed all discharge education using the teach-back method to confirm that the patient and his family members understood the health information accurately. At the same time, the nurse reminded Mr. Lee and his family to add the department WeChat, follow the public number to reserve his follow-up appointments and carry out daily consultations. To ensure complete and clear information transmission during referral, the physician delivered discharge summaries to patients; thus, the primary care physicians could receive useful information and develop subsequent treatment and management.
After discharge, the patient took oral medication regularly, self-measured his blood pressure at home, paid attention to keeping warm, ate a low-salt diet and light diet and performed Tai Chi exercise. In addition, primary care physicians and nurses made frequent follow-up home visits, and Mr. Lee received online counseling through WeChat when he had questions. After the postdischarge interventions, the patient was more active in social activities, and his quality of life improved.
Final Definition of Transitional Care in Patients with Heart Failure
The definition of transitional care in patients with heart failure is a comprehensive, multidisciplinary, individual-tailored strategy during a vulnerable period to improve patient self-management, the care ability of caregivers and coordination between hospital resources and social support systems for continuous management to promote smooth patient transitions between different locations. A diagram depicting the relationship among antecedents, attributes, and consequences for transitional care in patients with heart failure is shown in Figure 2.
 |
Figure 2 Characteristics of transitional care in patients with heart failure. |
Measurement Tools
Measurement instruments are tools that define the characteristics of the concept.9 At present, there is no specific assessment tool for identifying patients with HF who will require transitional care after hospitalization. Yoshimura et al61 developed the care transitions scale to assess HF patients’ readiness for hospital discharge, but the usefulness of this scale in nursing practice needs to be explored in more studies. The patient’s health status is one reason why healthcare providers apply transitional care to HF patients, and those patients who usually have multiple complications make management difficult. The Charlson comorbidity index and the CHA2DS2-Vasc score are validated scores to assess comorbid burden and clinical prognostic.62,63 Sonaglioni and his colleagues found that CHA2DS2-VASc score is an independent predictive factor for all cause mortality and re-hospitalizations in HF patients aged 75 years and older regardless of atrial fibrillation.64 Shuvy and her colleagues reported that the age-adjusted Charlson comorbidity index is significantly associated with clinical outcome in patients with heart failure.65 Therefore, these clinical prognostic scores might be useful for identifying patients with HF who need transitional care.
Discussion
In previous reports, most studies37,38,40–43 have focused on the interventions and impacts of transitional care in heart failure patients, with little attention given to its mechanism and attributes. To the best of our knowledge, this paper is the first to describe the concept of transitional care in patients with heart failure, aiming to distinguish it from similar concepts, such as discharge planning and continuity of care. As seen from the results of this concept analysis, transitional care in patients with HF is neither discharge planning alone nor continuity of care using case management. To a certain extent, transitional care in HF patients is the clinical situation use of Meleis’s transitions theory.66 It is important to acquire knowledge and information, develop plans, comprehensively assess the problems faced, recognize social support systems, communicate with relevant people, and facilitate better management during the transition process.8 Role insufficiency, role transition, and changes in surroundings when a patient is discharged from the hospital to home all lead to stress and uncertainty for the patient, so establishing a reasonable response pattern is necessary to achieve role supplementation. Compared with other diseases, transitional care in patients with heart failure pays more attention to vulnerable periods and designs comprehensive services that are initiated during hospitalization due to the plateaued readmission rate.
In the process of achieving role supplementation, transitional care interventions, which have multiple components, are beneficial to patient-centered health outcomes. In particular, educating and providing counseling for HF patients to improve their self-care is the prime attribute of transitional care for these patients. However, a previous meta-analysis revealed that approximately 33% of patients with HF have low health literacy,67 thus highlighting the importance of developing an effective educational strategy tailored to each patient’s health literacy to enhance their self-management.
The literature review strongly emphasized communication and collaboration as another feature of transitional care in HF patients. The formulation of a comprehensive, multidisciplinary, individually tailored strategy requires multiple health care providers, such as physicians, nurses, pharmacists, and dietitians, to encourage patients and their caregivers to participate in the decision-making process and quality improvement. Moreover, continuous management in the transition period is also achieved through communication and coordination between hospital resources and the social support system. Common goals, responsibilities, and shared values drive team-based transitional care for HF patients.
Considering the cost-effectiveness of transition-of-care interventions, comprehensively assessing and screening patients with HF who need transitional care after hospitalization is essential and beneficial in practice. A report described that19 risk models used to predict readmission can be used to predict the requirement for transitional care; however, the development of specific assessment tools for identifying patients with HF who need transitional care after hospitalization is urgent.
Transitional care in patients with heart failure is mainly led by nurses. Because medication nonadherence is a risk factor for HF readmission and because of the unique ability to provide education about medication reconciliation,68 the impact of the pharmacist’s role in medication adherence has been emphasized. This is also an evolution of the role functions of the main implementer in the application of transitional care in HF patients. Novel technologies to expand access to pharmacy services could improve the current limitations of transitional care in HF patients.58
In China, studies on transitional care for HF patients are mainly from Hong Kong, implementation in mainland China is scarce, and discharge planning is the research hotspot. In contrast to developed countries, Chinese communities suffer from a lack of medical resources, especially for those living in rural areas. If doctors and nurses working in primary care settings can be involved in the management of heart failure patients’ transitions and cooperate with health care staff in tertiary hospitals, they will provide HF patients with more accessible transitional care services and better management. Therefore, how to build networks to connect these groups in practice deserves further research.
Limitations
Because we retrieved only published literature, articles published in English, Chinese and medical disciplines are limited, and the document collection may be incomplete.
Conclusion
With the increasing application of transitional care in patients with heart failure, there is insufficient evidence to reflect the conceptual content of this phase, so it makes sense to conduct a conceptual analysis of transitional care in this area. The objective of this analysis was to provide conceptual clarity and direction for future research and practice. By analyzing the attributes, antecedents and consequences of transitional care in patients with heart failure, a better understanding of this concept was obtained. This study found that transitional care in HF patients is a systematic care process during a vulnerable period that improves patients’ self-management and coordination between hospital resources and social support systems for continuous management to promote smooth patient transitions between different locations. This concept analysis will offer healthcare providers information in designing evidence-based interventions and quality improvement strategies to ensure that transition processes produce desired outcomes. In addition, it is also helpful for developing specific assessment tools to identify patients with HF who need transitional care.
Acknowledgments
This research received a grant from the National Natural Science Foundation of China (No. 72064028).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA guideline for the management of heart failure: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation. 2013;128(16):1810–1852. doi:10.1161/CIR.0b013e31829e8807
2. Collaborators GB. GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1789–1858. doi:10.1016/S0140-6736(18)32279-7
3. Zhong C, Wong C, Cheung W, et al. Peri-discharge complex interventions for reducing 30-day hospital readmissions among heart failure patients: overview of systematic reviews and network meta-analysis. Perspect Public Health. 2022;142(5):263–277. doi:10.1177/1757913920985258
4. Roger VL. Epidemiology of Heart Failure: a Contemporary Perspective. Circ Res. 2021;128(10):1421–1434. doi:10.1161/CIRCRESAHA.121.318172
5. Kilgore M, Patel HK, Kielhorn A, Maya JF, Sharma P. Economic burden of hospitalizations of Medicare beneficiaries with heart failure. Risk Manag Healthc Policy. 2017;10:63–70. doi:10.2147/RMHP.S130341
6. Van Spall HGC, Rahman T, Mytton O, et al. Comparative effectiveness of transitional care services in patients discharged from the hospital with heart failure: a systematic review and network meta-analysis. Eur J Heart Fail. 2017;19(11):1427–1443. doi:10.1002/ejhf.765
7. Vedel I, Khanassov V. Transitional Care for Patients With Congestive Heart Failure: a Systematic Review and Meta-Analysis. Ann Fam Med. 2015;13(6):562–571. doi:10.1370/afm.1844
8. Shahsavari H, Zarei M, Aliheydari Mamaghani J. Transitional care: concept analysis using Rodgers’ evolutionary approach. Int J Nurs Stud. 2019;99:103387. doi:10.1016/j.ijnurstu.2019.103387
9. Rodgers BL, Knafl KA. Concept Development in Nursing: Foundations, Techniques and Applications. Philadelphia: Saunders; 2000.
10. “transitional”. Merriam-WebsterDictionary; 2023. Available from: https://www.merriam-webster.com/dictionary/transitional.
11. NCBI. Transitionalcare-MeSH-NCBI[EB/OL]; 2023. Available from: https://www.ncbi.nlm.nih.gov/mesh/?term=transitional+care.
12. Listed N. Hospital Referral of patients for continuity of nursing care. Am J Nurs. 1947;47(11):761–764.
13. Desmond MM, Rudolph AJ, Phitaksphraiwan P. The transitional care nursery. A mechanism for preventive medicine in the newborn. Pediatr Clin North Am. 1966;13(3):651–668. doi:10.1016/S0031-3955(16)31875-2
14. Traxler H, Dunaye T. Emerging patterns in transitional care. Health Aff. 1987;6(2):57–68. doi:10.1377/hlthaff.6.2.57
15. Brooten D, Kumar S, Brown LP, et al. A randomized clinical trial of early hospital discharge and home follow-up of very-low-birth-weight infants. N Engl J Med. 1986;315(15):934–939. doi:10.1056/NEJM198610093151505
16. Rich MW, Beckham V, Wittenberg C, Leven CL, Freedland KE, Carney RM. A multidisciplinary intervention to prevent the readmission of elderly patients with congestive heart failure. N Eng J Med. 1995;333(18):1190–1195. doi:10.1056/NEJM199511023331806
17. Harrison MB, Browne GB, Roberts J, Tugwell P, Gafni A, Graham ID. Quality of life of individuals with heart failure: a randomized trial of the effectiveness of two models of hospital-to-home transition. Med Care. 2002;40(4):271–282. doi:10.1097/00005650-200204000-00003
18. Naylor MD, Brooten DA, Campbell RL, Maislin G, McCauley KM, Schwartz JS. Transitional care of older adults hospitalized with heart failure: a randomized, controlled trial. J Am Geriatr Soc. 2004;52(5):675–684. doi:10.1111/j.1532-5415.2004.52202.x
19. Albert NM, Barnason S, Deswal A, et al. Transitions of care in heart failure: a scientific statement from the American Heart Association. Circ Heart Fail. 2015;8(2):384–409. doi:10.1161/HHF.0000000000000006
20. Thompson DR, Ski CF, Clark AM. Transitional Care Interventions for Heart Failure: what Are the Mechanisms? Am J Med. 2019;132(3):278–280. doi:10.1016/j.amjmed.2018.09.028
21. Clark AM, Wiens KS, Banner D, et al. A systematic review of the main mechanisms of heart failure disease management interventions. Heart. 2016;102(9):707–711. doi:10.1136/heartjnl-2015-308551
22. Hoover C, Plamann J, Beckel J. Outcomes of an Interdisciplinary Transitional Care Quality Improvement Project on Self-Management and Health Care Use in Patients With Heart Failure. J Gerontol Nurs. 2017;43(1):23–31. doi:10.3928/00989134-20160901-01
23. Yu DS, Lee DT, Stewart S, Thompson DR, Choi KC, Yu CM. Effect of Nurse-Implemented Transitional Care for Chinese Individuals with Chronic Heart Failure in Hong Kong: a Randomized Controlled Trial. J Am Geriatr Soc. 2015;63(8):1583–1593. doi:10.1111/jgs.13533
24. Albert NM. A systematic review of transitional-care strategies to reduce rehospitalization in patients with heart failure. Heart Lung. 2016;45(2):100–113. doi:10.1016/j.hrtlng.2015.12.001
25. Tingley J, Dolansky MA, Walsh MN. Team-Based Transitions of Care in Heart Failure. Heart Fail Clin. 2015;11(3):371–378. doi:10.1016/j.hfc.2015.03.003
26. Garnier A, Rouiller N, Gachoud D, et al. Effectiveness of a transition plan at discharge of patients hospitalized with heart failure: a before-and-after study. ESC Heart Failure. 2018;5(4):657–667. doi:10.1002/ehf2.12295
27. Allen LA, Smoyer Tomic KE, Smith DM, Wilson KL, Agodoa I. Rates and predictors of 30-day readmission among commercially insured and Medicaid-enrolled patients hospitalized with systolic heart failure. Circ Heart Fail. 2012;5(6):672–679. doi:10.1161/CIRCHEARTFAILURE.112.967356
28. Tian J, Ding F, Wang R, et al. Dynamic Trajectory of a Patient-Reported Outcome and Its Associated Factors for Patients with Chronic Heart Failure: a Growth Mixture Model Approach. Risk Manag Healthc Policy. 2022;15:2083–2096. doi:10.2147/RMHP.S384936
29. Institute of Medicine (US) Committee on Health Literacy. Health Literacy: a Prescription to End Confusion. In: Nielsen-Bohlman L, Panzer AM, Kindig DA, editors. Washington DC: National Academies Press; 2004.
30. Evangelista LS, Rasmusson KD, Laramee AS, et al. Health literacy and the patient with heart failure implications for patient care and research: a consensus statement of the Heart Failure Society of America. J Card Fail. 2010;16(1):9–16. doi:10.1016/j.cardfail.2009.10.026
31. Jaarsma T. Inter-professional team approach to patients with heart failure. Heart. 2005;91(6):832–838. doi:10.1136/hrt.2003.025296
32. Haynes KT, Oberne A, Cawthon C, Kripalani S. Pharmacists’ recommendations to improve care transitions. Ann Pharmacother. 2012;46(9):1152–1159. doi:10.1345/aph.1Q641
33. Retrum JH, Boggs J, Hersh A, et al. Patient-identified factors related to heart failure readmissions. Circ Cardiovasc Qual Outcomes. 2013;6(2):171–177. doi:10.1161/CIRCOUTCOMES.112.967356
34. Naylor MD, Hirschman KB, McCauley K, et al. MIRROR-TCM: multisite Replication of a Randomized Controlled Trial-Transitional Care Model. Contemp Clin Trials. 2022;112:106620. doi:10.1016/j.cct.2021.106620
35. Kangovi S, Barg FK, Carter T, et al. Challenges faced by patients with low socioeconomic status during the post-hospital transition. J Gen Intern Med. 2014;29(2):283–289. doi:10.1007/s11606-013-2571-5
36. Rodgers B, Jacelon CS, Knafl KA. Concept Analysis and the Advance of Nursing Knowledge: state of the Science. J Nurs Scholarsh. 2018;50(4):451–459. doi:10.1111/jnu.12386
37. Kitts NK, Reeve AR, Tsu L. Care transitions in elderly heart failure patients: current practices and the pharmacist’s role. Consult Pharm. 2014;29(3):179–190. doi:10.4140/TCP.n.2014.179
38. Stamp KD, Machado MA. Allen NA.Transitional care programs improve outcomes for heart failure patients: an integrative review. J Cardiovasc Nurs. 2014;29(2):140–154. doi:10.1097/JCN.0b013e31827db560
39. Van Spall HGC, Lee SF, Xie F, et al. Effect of Patient-Centered Transitional Care Services on Clinical Outcomes in Patients Hospitalized for Heart Failure: the PACT-HF Randomized Clinical Trial. JAMA. 2019;321(8):753–761. doi:10.1001/jama.2019.0710
40. Warden BA, Freels JP, Furuno JP, Mackay J. Pharmacy-managed program for providing education and discharge instructions for patients with heart failure. Am j Health System Pharm. 2014;71(2):134–139. doi:10.2146/ajhp130103
41. Huntington MK, Guzman AI, Roemen A, Fieldsend J, Saloum H. Hospital-to-Home: a hospital readmission reduction program for congestive heart failure. S D Med. 2013;66(9):370–373.
42. Slyer JT, Concert CM, Eusebio AM, Rogers ME, Singleton J. A systematic review of the effectiveness of nurse coordinated transitioning of care on readmission rates for patients with heart failure. JBI Libr Syst Rev. 2011;9(15):464–490. doi:10.11124/jbisrir-2011-130
43. Anderson C, Deepak BV, Amoateng-Adjepong Y, Zarich S. Benefits of comprehensive inpatient education and discharge planning combined with outpatient support in elderly patients with congestive heart failure. Congestive Heart Failure. 2005;11(6):315–321. doi:10.1111/j.1527-5299.2005.04458.x
44. Phillips CO, Wright SM, Kern DE, Singa RM, Shepperd S, Rubin HR. Comprehensive Discharge Planning with Postdischarge Support for Older Patients with Congestive Heart Failure: a Meta-analysis. JAMA. 2004;291(11):1358–1367. doi:10.1001/jama.291.11.1358
45. Lambrinou E, Kalogirou F, Lamnisos D, Sourtzi P. Effectiveness of heart failure management programmes with nurse-led discharge planning in reducing re-admissions: a systematic review and meta-analysis. Int J Nurs Stud. 2012;49(5):610–624. doi:10.1016/j.ijnurstu.2011.11.002
46. Atienza F, Anguita M, Martinez-Alzamora N, et al. Multicenter randomized trial of a comprehensive hospital discharge and outpatient heart failure management program. Eur J Heart Fail. 2004;6(5):643–652. doi:10.1016/j.ejheart.2003.11.023
47. Lin X, Ji R, Wang X, Xin R, Chen Q. A systematic review and meta-analysis of the effect of transitional care interventions on the prognosis of patients with heart failure. J Thorac Dis. 2022;14(4):1164–1171. doi:10.21037/jtd-22-102
48. Oscalices MIL, Okuno MFP, Lopes MCBT, Campanharo CRV, Batista REA. Discharge guidance and telephone follow-up in the therapeutic adherence of heart failure: randomized clinical trial. Rev Lat Am Enfermagem. 2019;27:e3159. doi:10.1590/1518-8345.2484.3159
49. Li Y, Fang J, Li M, Luo B. Effect of nurse-led hospital-to-home transitional care interventions on mortality and psychosocial outcomes in adults with heart failure: a meta-analysis. Eur j Cardiovascular Nursing. 2022;21(4):307–317. doi:10.1093/eurjcn/zvab105
50. Li M, Li Y, Meng Q, et al. Effects of nurse-led transitional care interventions for patients with heart failure on healthcare utilization: a meta-analysis of randomized controlled trials. PLoS One. 2021;16(12):e0261300. doi:10.1371/journal.pone.0261300
51. Mutharasan RK. Transitioning Patients with Heart Failure to Outpatient Care. Heart Fail Clin. 2020;16(4):421–431. doi:10.1016/j.hfc.2020.06.003
52. Mai Ba H, Son YJ, Lee K, Kim BH. Transitional Care Interventions for Patients with Heart Failure: an Integrative Review. Int J Environ Res Public Health. 2020;17(8):2925. doi:10.3390/ijerph17082925
53. Ota KS, Beutler DS, Gerkin RD, Weiss JL, Loli AI. Physician-directed heart failure transitional care program: a retrospective case review. J Clin Med Res. 2013;5(5):335–342. doi:10.4021/jocmr1492w
54. Gorodeski EZ, Chlad S, Vilensky S. Home-based care for heart failure: Cleveland Clinic’s “Heart Care at Home” transitional care program. Cleve Clin J Med. 2013;80(Suppl 1):eS20–26. doi:10.3949/ccjm.80.e-s1.05
55. Blumer V, Gayowsky A, Xie F, et al. Effect of patient-centered transitional care services on patient-reported outcomes in heart failure: sex-specific analysis of the PACT-HF randomized controlled trial. Eur J Heart Fail. 2021;23(9):1488–1498. doi:10.1002/ejhf.2312
56. Williams G, Akroyd K, Burke L. Evaluation of the transitional care model in chronic heart failure. Br J Nurs. 2010;19(22):1402–1407. doi:10.12968/bjon.2010.19.22.1402
57. Bixby MB, Konick-McMahon J, McKenna CG. Applying the transitional care model to elderly patients with heart failure. J Cardiovasc Nurs. 2000;14(3):53–63. doi:10.1097/00005082-200004000-00008
58. Anderson SL, Marrs JC. A Review of the Role of the Pharmacist in Heart Failure Transition of Care. Adv Ther. 2018;35(3):311–323. doi:10.1007/s12325-018-0671-7
59. Gonçalves-Bradley DC, Lannin NA, Clemson L, Cameron ID. Shepperd S. Discharge planning from hospital. Cochrane Database Syst Rev. 2022;2(2):CD000313. doi:10.1002/14651858.CD000313.pub6
60. Haggerty JL, Reid RJ, Freeman GK, Starfield BH, Adair CE, McKendry R. Continuity of care: a multidisciplinary review. BMJ. 2003;327(7425):1219–1221. doi:10.1136/bmj.327.7425.1219
61. Yoshimura M, Kawamura M, Hasegawa S, Ito YM, Takahashi K, Sumi N. Development and validation of the Care Transitions Scale for Patients with Heart Failure: a tool for nurses to assess patients’ readiness for hospital discharge. Japan j Nursing Sci. 2023;20(2):e12522. doi:10.1111/jjns.12522
62. Sonaglioni A, Lombardo M, Albini A, et al. Charlson comorbidity index, neutrophil-to-lymphocyte ratio and undertreatment with renin-angiotensin-aldosterone system inhibitors predict in-hospital mortality of hospitalized COVID-19 patients during the omicron dominant period. Front Immunol. 2022;13:958418. doi:10.3389/fimmu.2022.958418
63. Shuvy M, Zwas DR, Keren A, Gotsman I. Value of the CHA2 DS2 -VASc score for predicting outcome in patients with heart failure. ESC Heart Fail. 2020;7(5):2553–2560. doi:10.1002/ehf2.12831
64. Sonaglioni A, Lonati C, Rigamonti E, et al. CHA2DS2-VASc score stratifies mortality risk in heart failure patients aged 75 years and older with and without atrial fibrillation. Aging Clin Exp Res. 2022;34(7):1707–1720. doi:10.1007/s40520-022-02107-x
65. Shuvy M, Zwas DR, Keren A, Gotsman I. The age-adjusted Charlson comorbidity index: a significant predictor of clinical outcome in patients with heart failure. Eur J Intern Med. 2020;73:103–104. doi:10.1016/j.ejim.2019.12.030
66. Meleis AI, Sawyer LM, Im EO, Hilfinger Messias DK, Schumacher K. Experiencing transitions: an emerging middle-range theory. Adv Nurs Sci. 2000;23(1):12–28. doi:10.1097/00012272-200009000-00006
67. Kanejima Y, Shimogai T, Kitamura M, Ishihara K, Izawa KP. Impact of health literacy in patients with cardiovascular diseases: a systematic review and meta-analysis. Patient Educ Couns. 2022;105(7):1793–1800. doi:10.1016/j.pec.2021.11.021
68. McKay C, Park C, Chang J, et al. Systematic Review and Meta-analysis of Pharmacist-Led Transitions of Care Services on the 30-Day All-Cause Readmission Rate of Patients with Congestive Heart Failure. Clin Drug Investig. 2019;39(8):703–712. doi:10.1007/s40261-019-00797-2
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.