Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 19
Transition from Continuous Subcutaneous Insulin Infusion to IDeg-Based Regimens in Hospitalized T2DM Patients: A Single-Center Retrospective Analysis
Authors Dong R, Gu L ![]() , Li H, Hu Y, Liu H, Kou X, Zhao Y, Zhao M, Shi B
, Li H, Hu Y, Liu H, Kou X, Zhao Y, Zhao M, Shi B ![]() , Guo H, Qiang W
, Guo H, Qiang W ![]()
Received 15 August 2025
Accepted for publication 17 December 2025
Published 13 January 2026 Volume 2026:19 557994
DOI https://doi.org/10.2147/DMSO.S557994
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Halis Akturk
Ruiqing Dong,1,* Lifan Gu,2,* Heping Li,1 Yuanna Hu,3 Hui Liu,4 Xuna Kou,1 Yukun Zhao,1 Meng Zhao,1 Bingyin Shi,1 Hui Guo,1 Wei Qiang1
1Department of Endocrinology and Metabolism, The First Affiliated Hospital of Xi’an Jiaotong University, Xi’an, 710061, People’s Republic of China; 2School of Future Technology, Xi’an Jiaotong University, Xi’an, 710049, People’s Republic of China; 3Department of Pain, The First Affiliated Hospital of Xinjiang Medical University, Urumqi City, 830017, People’s Republic of China; 4Biobank, The First Affiliated Hospital of Xi’an Jiaotong University, Xi’an, 710061, People’s Republic of China
*These authors contributed equally to this article
Correspondence: Hui Guo, Department of Endocrinology and Metabolism, The First Affiliated Hospital of Xi’an Jiaotong University, No. 277 Yanta West Road, Xi’an, Shaanxi, 710061, People’s Republic of China, Tel/Fax +86-29-85323974, Email [email protected] Wei Qiang, Department of Endocrinology and Metabolism, The First Affiliated Hospital of Xi’an Jiaotong University, No. 277 Yanta West Road, Xi’an, Shaanxi, 710061, People’s Republic of China, Tel/Fax +86-29-85323974, Email [email protected]
Background: Chinese patients with type 2 diabetes mellitus (T2DM) often initiate insulin therapy in the hospital, requiring rapid glycemic control and simplified post-discharge plans. Few clinical studies have focused on the transition protocols for continuous subcutaneous insulin infusion (CSII).
Objective: To evaluate the efficacy, safety, and patient satisfaction of transitioning from CSII to three treatment regimens: insulin degludec (IDeg), insulin degludec/insulin aspart (IDegAsp), or insulin degludec and liraglutide (IDegLira).
Methods: Clinical information and continuous glucose monitoring (CGM) data were retrospectively collected from 171 patients in a single center. Patient satisfaction and quality of life were assessed using standardized questionnaires in a three-month follow-up.
Results: After transition, mean glucose (MG) and glucose management indicator (GMI) decreased, while time in range (TIR) increased significantly. Coefficient of variation (CV) and time above range (TAR) decreased. Time below range (TBR) was unchanged in IDegAsp and IDegLira groups but slightly increased in the IDeg group (0.60% [0.00%, 1.60%] vs 1.10% [0.00%, 3.40%], P = 0.003). IDegAsp and IDegLira groups showed higher TIR and lower MG, GMI, CV, TAR, and TBR. 64.3% of IDegLira patients required one or fewer additional medications. Patient satisfaction was highest in the IDegLira group, with hypoglycemia avoidance, better weight management, fatigue prevention and less anxiety.
Conclusion: All three regimens enabled a smooth transition after CSII therapy. IDegAsp and IDegLira demonstrated superior glycemic control and reduced variability compared to IDeg. IDegLira was more convenient and associated with higher patient satisfaction.
Keywords: type 2 diabetes mellitus, insulin degludec, insulin degludec/insulin aspart, insulin degludec and liraglutide, continuous glucose monitoring
Introduction
Type 2 diabetes mellitus (T2DM) represents a significant public health concern. Basal insulin, a cornerstone in the management of T2DM, plays a crucial role in achieving glycemic control. The effectiveness of basal insulin is modulated by factors such as β-cell function, dietary habits, body weight, and the presence of complications.
Notably, there is a marked difference in the initiation of insulin therapy between Chinese patients and those in Europe and America; a substantially higher proportion of Chinese patients commence insulin therapy during hospitalization.1,2 During the limited duration of hospital stays, three primary objectives must be accomplished. Firstly, the rapid correction of hyperglycemia followed by the development of a regimen tailored to the individual’s glucose profile. Secondly, the stabilization of blood glucose levels during the transition from intensive insulin therapy to antidiabetic regimen after discharge, with a particular focus on minimizing the incidence of hypoglycemia. Thirdly, the simplification of the treatment regimen while ensuring its efficacy, which is vital for enhancing patient adherence post-discharge.
Another prominent characteristic of Chinese patients with T2DM initiating insulin therapy is the early dysfunction of β-cells and deficiencies in early-phase insulin secretion, which contribute to more pronounced postprandial hyperglycemia.3–5 Monotherapy with basal insulin may be insufficient for achieving comprehensive glycemic control. In recent years, novel therapeutic options have emerged, including premixed insulin formulations with second-generation insulin analogs and rapid-acting insulin analogs, as well as combination formulations of basal insulin and glucagon-like peptide-1 receptor agonists (GLP-1RA).6 Premixed insulin, noted for its rapid onset and prolonged duration of action, is particularly effective for postprandial glycemic control. In contrast, GLP-1RA offer additional advantages such as glycemic reduction, weight loss, and a low risk of hypoglycemia, thereby presenting a novel strategy for the management of T2DM. A prominent example of premixed insulin is insulin degludec/insulin aspart (IDegAsp), which, with once or twice daily administration, provides both mealtime coverage and comprehensive 24-hour basal coverage, and is frequently prescribed.7–10 An exemplary combination of basal insulin and GLP-1RA is insulin degludec and liraglutide (IDegLira), which enhances glycemic control by reducing fasting blood sugar (FBS) and postprandial glucose without increasing the risk of hypoglycemia or weight gain. Moreover, this formulation has demonstrated cardiovascular benefits.11,12
This single-center retrospective clinical study aims to compare the glycemic control among three insulin or combination formulations containing insulin degludec (IDeg) - IDeg, IDegAsp, and IDegLira in hospitalized Chinese patients with T2DM. In contrast to previous research, which primarily focuses on the long-term efficacy and safety of various antihyperglycemic agents, this study emphasizes on the insulin initiation regimens and the transition at discharge for hospitalized patients.10,13,14 Furthermore, the study utilizes continuous glucose monitoring (CGM) to provide a comprehensive assessment of glycemic profiles, with a particular attention on the risk of hypoglycemia. Additionally, it examines the convenience of medication use and patient compliance based on the drug combination regimen at discharge.
Methods
Study Design and Participants
In this retrospective, single-center study, we recruited inpatients admitted to the Department of Endocrinology and Metabolism of the First Affiliated Hospital of Xi’an Jiaotong University from June 1, 2023 to June 30, 2024. Our study was conducted in accordance with the ethical standards of the Declaration of Helsinki and was approved by the Ethics Committee of the First Affiliated Hospital of Xi’an Jiaotong University (Approval No. XJTU1AF2023LSK-458). The Ethics Committee exempted the study from obtaining informed consent since it did not include any interventions affecting treatment.
Patients who met the following criteria were included in the current study: 1) aged ≥18 years with the diagnosis of T2DM; 2) patients on continuous subcutaneous insulin infusion (CSII) therapy were switched to regimens based on IDeg, IDegAsp, or IDegLira, with equivalent conversion of basal insulin components and insulin pump basal rates, and utilized the CGM device. The exclusion criteria were as follows: 1) patients receiving systemic corticosteroids or other medication affected glucose level; 2) patients with malignant tumors or a history of malignant tumors; 3) patients with severe infections or Cushing’s syndrome, and other conditions that affect blood glucose levels; and 4) incomplete clinical or CGM data.
In this retrospective study, the allocation to the three IDeg-based regimens was determined by standardized clinical decision-making during the patient’s hospitalization. After achieving initial glycemic control with CSII, physicians selected the most appropriate regimen for each patient based on an evaluation of individual clinical characteristics. Decision-making factors included, but were not limited to, body mass index (BMI) and the presence of complications or comorbidities—notably, the presence of atherosclerotic cardiovascular disease was a consideration for selecting the GLP-1RA-containing regimen (IDegLira). An equivalent basal dose conversion (whereby the daily basal insulin dose from the pump was directly used as the starting dose for the degludec component) was conducted in all three IDeg-based regimens.15
Data Source and CGM Parameters
Comprehensive data, including demographic characteristics, clinical features, laboratory parameters, anti-diabetic treatment with either insulin or other anti-diabetic drugs, existing complications and comorbidities, and CGM data, were collected. CGM data was obtained through the Sibionics Dynamic Blood Glucose Monitor, which generating a daily record of 288 continuous sensor values.
Glycemic variability metrics derived from CGM included mean glucose (MG), glucose management indicator (GMI), standard deviation (SD) and coefficient of variation (CV), time in range (TIR), time above range (TAR), time below range (TBR), time in tight range (TITR), low blood glucose index (LBGI), and high blood glucose index (HBGI), and the mean of daily differences (MODD). The definitions of the percentages of time spent in different ranges of glucose and the calculations of the glycemia risk index are detailed as follows: TIR: 3.9–10.0 mmol/L, TAR: > 10.0 mmol/L, TBR: < 3.9 mmol/L, TITR: 3.9–7.8 mmol/L. The calculation of these parameters are based on the international guidelines and consensus regarding CGM.16–18
Follow-Up Post-Discharge
The data were collected from patients via a telephone follow-up call, which was conducted three months after discharge as a clinical routine using the Treatment Related Impact Measures-Diabetes (TRIM-D) and the 12-item Short Form Health Survey version 2 (SF-12 v2). TRIM-D consists of 28 items measured on a 5-point scale with higher scores indicating greater satisfaction with diabetes treatment. Besides an overall score, TRIM-D items consist of five domains of impact: Treatment Burden, Daily Life, Diabetes Management, Compliance, and Psychological Health.19 The SF-12 is a shortened version of the 36-item Short Form Health Survey, two component scores are measured, namely the general health, physical functioning, role limitations due to physical problems, bodily pain, role limitations due to emotional problems, mental health, vitality, social functioning, physical summary component score and the mental component summary score; the items cover eight scales designed to assess various aspects of quality of life in the general population.20
Sample Size Consideration
Although a formal a priori power calculation was not performed for this retrospective study, we conducted a post hoc estimation to assess the robustness of our sample size. This estimation was based on the TIR data from a previous randomized trial comparing IDegAsp and IDegLira, which reported a mean TIR difference of 10.0% with a standard deviation of 15.0%.6 Using these parameters (α = 0.05, power = 80%) for a three-arm ANOVA, the estimated total sample size required was 144 participants. Our final cohort of 171 participants exceeds this conservative estimate.
Statistical Analysis
Statistical analysis was performed using SPSS 26.0 software. For normally distributed continuous variables, means ± standard deviations  , were reported, with between-group comparisons assessed via t-tests for two groups and one-way ANOVA for multiple groups. Non-normally distributed data were presented as medians with interquartile ranges [M (Q1, Q3)], and analyzed using non-parametric methods. Percentages were used for categorical data, with group differences evaluated by Pearson’s χ2 test. Statistical significance was set at P < 0.05.
, were reported, with between-group comparisons assessed via t-tests for two groups and one-way ANOVA for multiple groups. Non-normally distributed data were presented as medians with interquartile ranges [M (Q1, Q3)], and analyzed using non-parametric methods. Percentages were used for categorical data, with group differences evaluated by Pearson’s χ2 test. Statistical significance was set at P < 0.05.
Results
Demographics and Clinical Characteristics of the Patients
As demonstrated in Table 1, a total of 171 patients were enrolled in the study, with 55 (32.2%) switched to the anti-diabetic regimen based on IDeg, 60 (35.1%) in the IDegAsp group, and 56 (32.7%) in the IDegLira group after CSII. At baseline, the cohort had a mean age of 53.07 years, with 72.51% being male. The mean BMI was recorded at 24.84 kg/m2, the mean HbA1c was 10.34%, and the median duration of diabetes was 5 years. The majority of patients were previously managed with oral anti-diabetic drugs or insulin. No significant differences were observed among the three groups concerning age, gender, duration of diabetes, HbA1c levels, diabetic kidney disease, and pre-hospital anti-diabetic regimens, facilitating a focused comparison of treatment effects. And patients in the IDegLira group exhibited a significantly greater BMI (IDeg: 24.18 ± 3.13; IDegAsp: 24.74 ± 2.84; IDegLira: 25.57 ± 2.52; P = 0.040) and a higher prevalence of diabetic peripheral vascular disease (IDeg: 72.7%; IDegAsp: 55.0%; IDegLira: 94.6%; P < 0.001) and fatty liver disease (IDeg: 23.6%; IDegAsp: 15.0%; IDegLira: 39.3%; P = 0.010) compared to the other two groups.
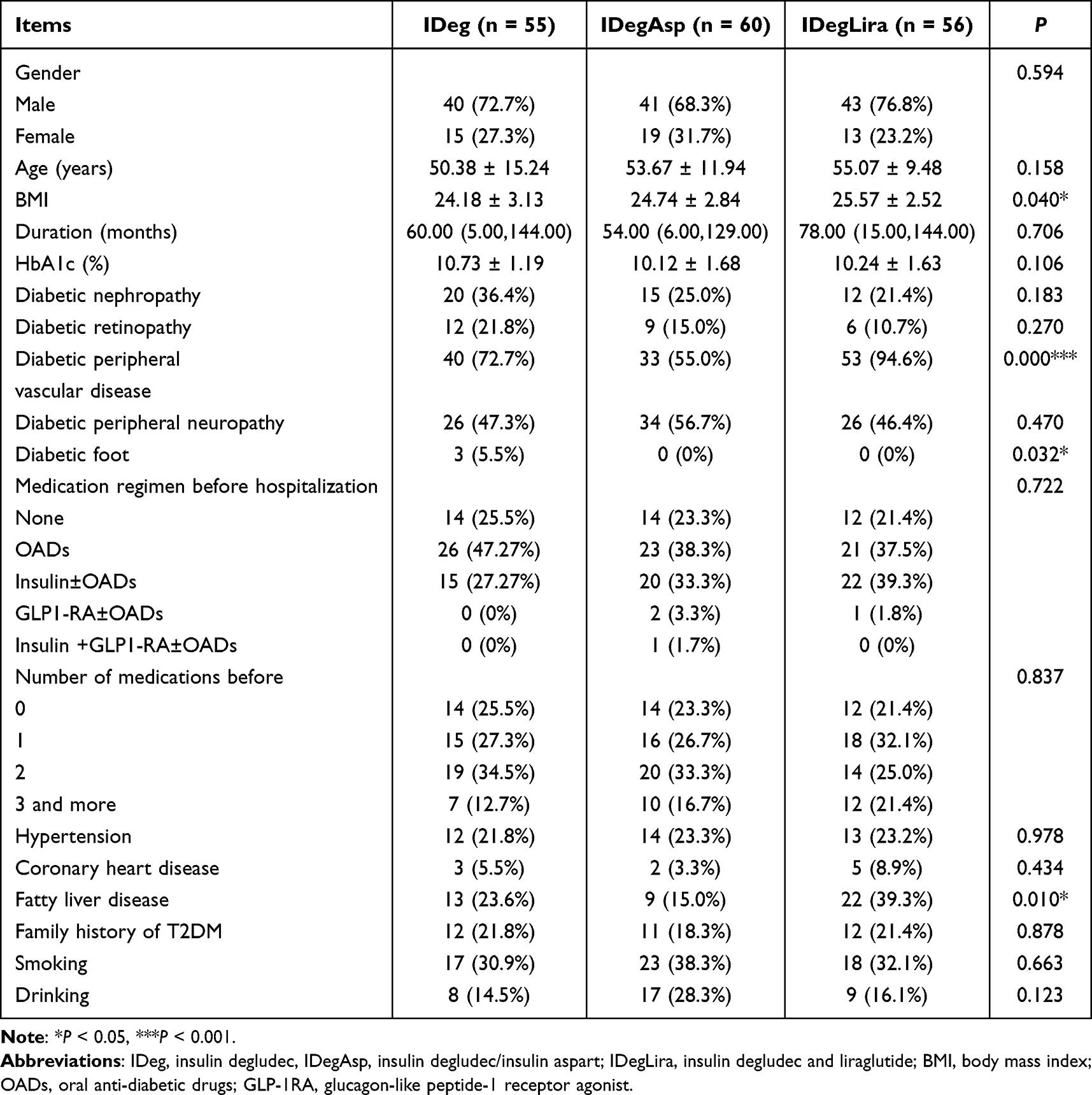 |
Table 1 Baseline Characteristics of the Participants |
Transition From CSII to IDeg, IDegAsp or IDegLira
As a clinical study on the transition from CSII to alternative insulin regimens, the evaluation of therapeutic efficacy and safety was conducted in a two-step process. The first step was to assess whether a smooth transition could be achieved, and the second step was to compare the merits of the three post-transition regimens. For each comparison, we assessed overall glucose control, glycemic variability, and the associated risks of hyperglycemia and hypoglycemia. To ensure a thorough evaluation of glycemic control, CGM was utilized, with the CGM parameters detailed in Table 2.
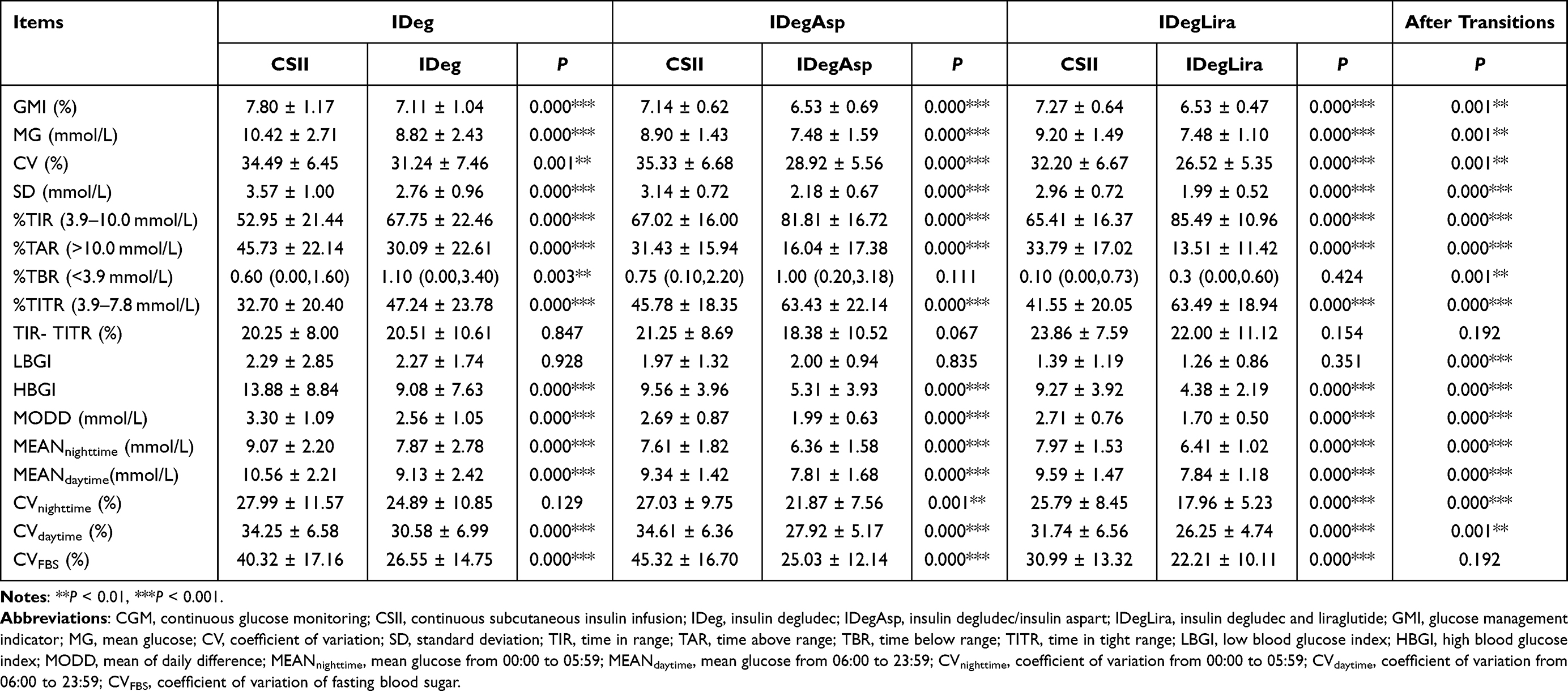 |
Table 2 Comparison of CGM Parameters During CSII Period and After Transition |
Post-transition, we observed advantages in overall glucose control indicators, including GMI and MG decreased, as well as TIR and TITR increased in all three groups. The IDegLira group exhibited the lowest GMI (P < 0.001) and MG (P < 0.001), followed by the IDegAsp group, with the IDeg group showing the highest values, while the TIR (P < 0.001) and TITR (P < 0.001) trends were opposite. Both IDegAsp and IDegLira groups met the internationally recommended target.18
Furthermore, indicators for assessing glycemic variability also decreased, such as the CV and SD. The parameters for inter-day variation including MODD and the CV of FBS (CVFBS) decreased post-transition compared to pre-transition levels. Further analysis showed that CVdaytime (06:00–23:59) and CVnighttime (00:00–05:59) decreased in all three groups, although the decrease in CVnighttime in the IDeg group was not statistically significant. The CV for all three groups post-transition adhered to the targets set by the Chinese guidelines and consensus statements (33%).21,22 The IDegLira group demonstrated the lowest CV values for both daytime and nighttime, followed by the IDegAsp group, while the IDeg group exhibited the highest values. Meanwhile, both MODD and CVFBS exhibited a decline post-transition, with the lowest values in the IDegLira group and the highest in the IDeg group. However, a statistically significant difference was observed only in MODD post-transition.
As the risk for hyper-and hypoglycemia is concerned, the TAR and HBGI decreased across all three groups. Notably, the TBR (0.60% [0.00%, 1.60%] vs 1.10% [0.00%, 3.40%], P = 0.003) increased after transitioning to IDeg, but remained within the safe threshold of less than 4%. No significant changes were observed in the other two groups. For each group, no significant difference was observed in the LBGI when comparing post-transition values to those during the CSII period. The IDegLira group exhibited the lowest TAR (P < 0.001), HBGI (P < 0.001), TBR (P = 0.001) and LBGI (P < 0.001), followed by the IDegAsp group, with the IDeg group showing the highest values.
Nocturnal Hypoglycemia
The concern about hypoglycemia frequently leads to apprehension among both patients and healthcare providers regarding the administration of basal insulin. Consequently, we conducted a further assessment of nocturnal hypoglycemia basal insulin-based treatment regimens post-transition. A total of 18 hypoglycemia events (< 3.9 mmol/L for ≥ 15 consecutive minutes) was detected, with 8/55 in the IDeg group, 7/60 in the IDegAsp group, and 3/56 in the IDegLira group. Specifically, nocturnal blood glucose levels below 3.9 mmol/L and 3.0 mmol/L, as detected by CGM, were observed in 6 (10.9%) and 2 (3.6%) patients in the IDeg group, 4 (6.7%) and 3 (5.0%) in the IDegAsp group, and 2 (3.6%) and 1 (1.8%) in the IDegLira group, respectively. However, subsequent verification using fingerstick blood glucose measurements revealed that none of these patients exhibited levels below 3.9 mmol/L. This discrepancy suggests that CGM readings may have overestimated the incidence of nocturnal hypoglycemia.
The analysis of nocturnal nadir glucose levels revealed distinct patterns among the treatment groups, as illustrated in Figure 1. In the IDeg group, the highest proportion of the nadir occurred later than the conventional 03:00, indicating a delayed onset of the lowest glucose levels. In contrast, the highest proportion of the nadirs in the IDegAsp and IDegLira groups were more uniformly distributed throughout the night. Across all three groups, fewer than 10% of patients exhibited a nadir in nocturnal blood glucose around 03:00. Specifically, 4.0%, 6.7% and 4.7% of the nadir glucose were observed between 02:45 and 03:15 in the IDeg, IDegAsp, and IDegLira groups, respectively. Notably, the distribution of nocturnal glucose nadirs exhibited an upward trend in the IDeg group, with 62.0% the nadirs occurring after 03:00. In the IDegAsp and IDegLira groups, 50.8% and 48.4% of the nadirs, respectively, were observed after 03:00.
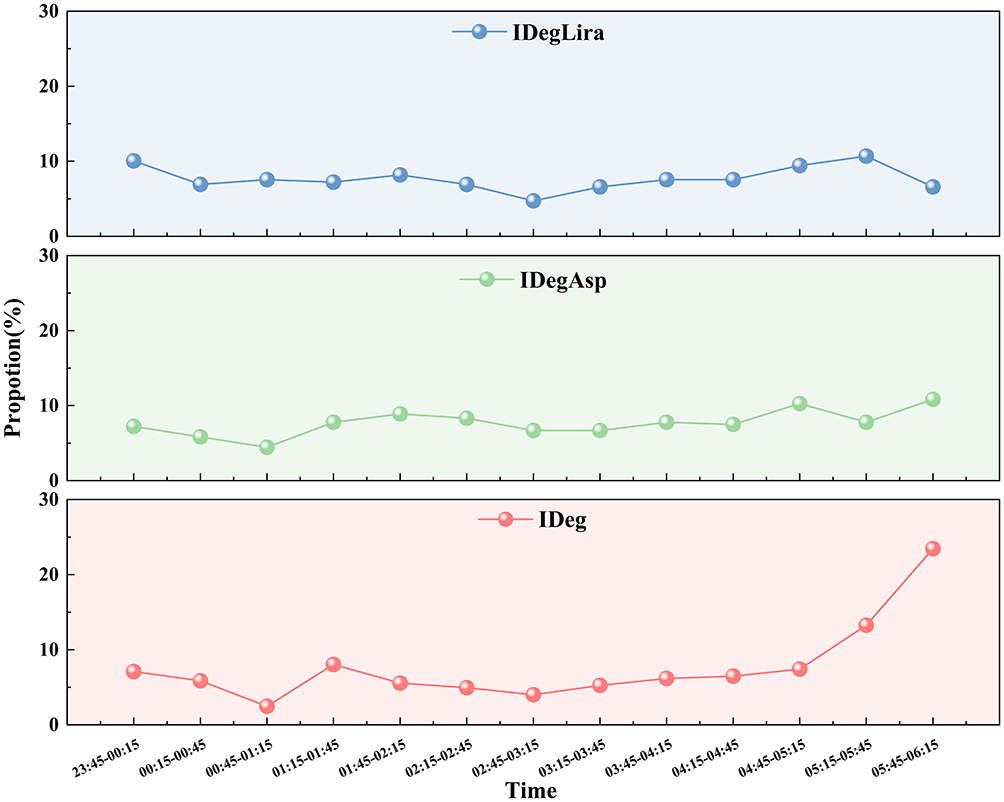 |
Figure 1 Distribution of nadir of nocturnal blood glucose. Abbreviations: IDeg, insulin degludec; IDegAsp, insulin degludec/insulin aspart; IDegLira, insulin degludec and liraglutide. |
Combined Anti-Diabetic Regimens
The simplicity of the antidiabetic medication is essential for enhancing patient adherence. As depicted in Figure 2, we assessed the antidiabetic regimens prescribed at hospital discharge. Seventy-three percent of patients in the IDeg group and 86.7% in the IDegAsp group required a combination of two or more antidiabetic drugs, while 64.3% patients in the IDegLira group required a combination of only one or less. Moreover, 76.4% and 38.3% of patients in the IDeg and IDegAsp groups, respectively, required the co-administration of rapid-acting insulin, and none in the IDegLira group. There was a significant difference in the utilization of other anti-diabetic drugs among the three treatment groups (P < 0.001).
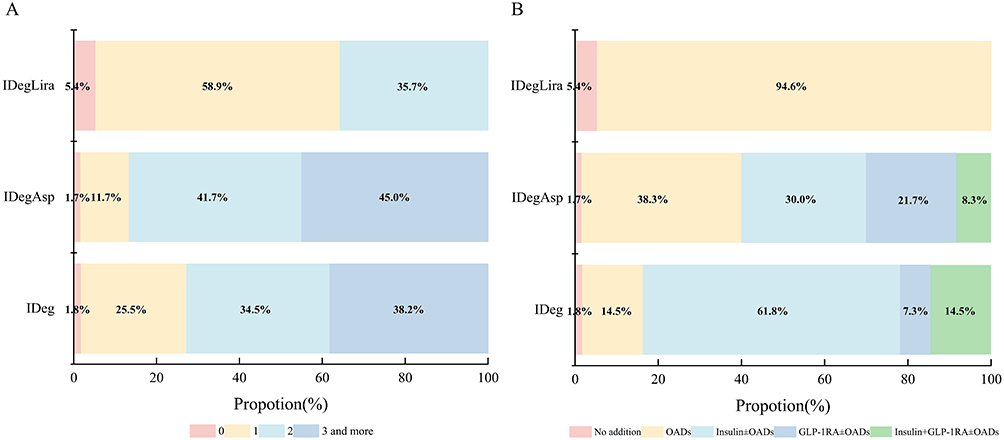 |
Figure 2 Comparison of combined medications at the time of hospital discharge. (A) Number of combined medications. (B) Combined medication regimens. Abbreviations: IDeg, insulin degludec; IDegAsp, insulin degludec/insulin aspart; IDegLira, insulin degludec and liraglutide; OADs, oral anti-diabetic drugs; GLP-1RA, glucagon-like peptide-1 receptor agonist. |
Compliance and HRQOL
The TRIM-D was developed as a disease-specific patient-reported outcomes measure to evaluate the impact of diabetes treatment for both type 1 and type 2 diabetes, encompassing a wide range of pharmacological treatments and delivery methods.23 The SF-12, a generic and well-established health-related quality of life (HRQOL) measure that has been commonly used in both general populations and various patient cohorts.24
Among the participants, 113 (66.1%) patients completed the TRIM-D questionnaire, while 107 (62.6%) patients completed the SF-12 v2 (Table 3). Notably, the IDegLira regimen was the most satisfactory to patients, particularly in terms of reducing hypoglycemia (P < 0.01), managing weight (P < 0.001), and enhancing vitality (P < 0.001). Additionally, patients receiving IDeg reported higher levels of nervousness and anxiety, whereas those in the IDegLira group reported the lowest incidence of these psychological symptoms. Analysis of the results of HRQOL (Table 3) indicated that patients in the IDegAsp group exhibited superior performance in terms of social functioning (P < 0.05).
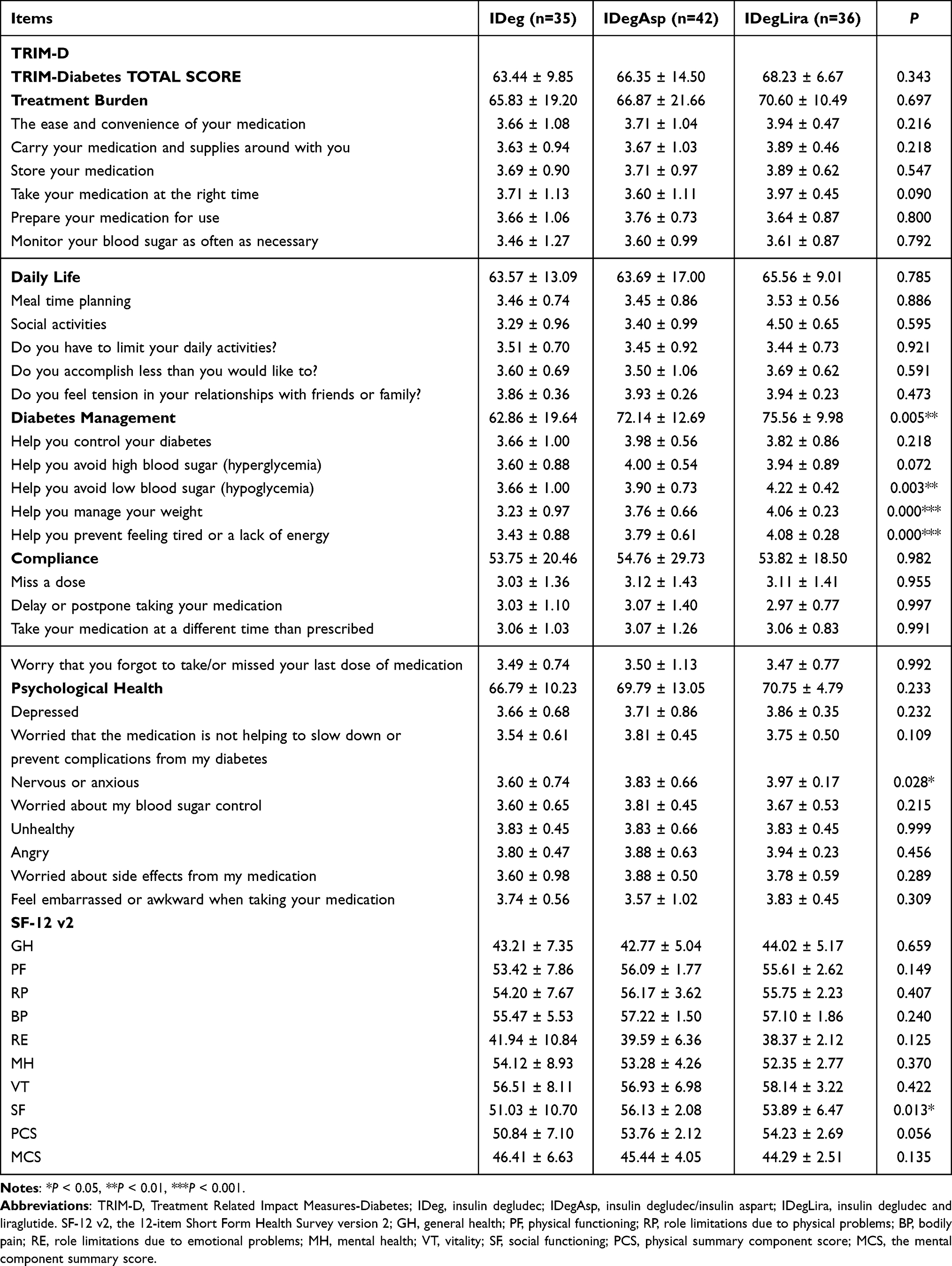 |
Table 3 The Results of TRIM-D and SF-12 V2 at 3-Month Follow-Up |
Discussion
While the long-term efficacy and safety of insulin therapies are well-established, the clinical strategies for managing the transition to outpatient regimens remain poorly defined. Our research specifically targets this evidence gap by evaluating outcomes in the immediate post-discharge phase, a period of high vulnerability, with the goal of optimizing care continuity. To augment the efficacy of intensive therapy, we selected patients who received CSII for intensive insulin therapy. Given the pronounced postprandial hyperglycemia characteristic of Chinese T2DM patients, we opted for three treatment regimens: IDeg, IDegAsp, and IDegLira. Our retrospective study yielded three primary findings: First, all three regimens enabled a smooth transition after CSII therapy. Second, IDegAsp and IDegLira demonstrated superior glucose control, reduced intra- and inter-day glycemic variability, and a lower risk of hypoglycemia compared to IDeg. Third, patients in the IDegLira group exhibited the highest satisfaction to the post-discharge treatment regimen, which can be attributed to the simplification of the treatment regimen.
At baseline, most variables exhibited no statistically significant differences, while the IDegLira group exhibited a higher prevalence of diabetic peripheral vascular disease and elevated BMI, indicating a prioritization of treatment choices for cardiovascular and weight-related benefits, which aligns with current clinical guidelines that consider the complex risks associated to T2DM.25–28 Specifically, the elevated BMI and diabetic peripheral vascular disease may be linked to an increased risk of fatty liver disease, highlighting the complex interplay between diabetes mellitus and metabolic dysfunction-associated fatty liver disease, Sun’s research further corroborates this by identifying an increased risk of vascular complications in patients with T2DM and fatty liver disease.29–31
Evaluation was conducted from both objective glycemic indices and patient perspectives. Glycemic assessment was performed in a two-step strategy. First, we evaluated whether the three treatment regimens could achieve a smooth transition. The evaluation was conducted from three aspects: 1) Overall glycemic control: After regimen conversion, GMI and MG significantly decreased in all three groups, corresponding to significant increases in TIR and TITR. Notably, TIR in the IDegAsp and IDegLira groups even reached the long-term control targets recommended by Chinese guidelines for general T2DM patients.22 Considering that most inpatients had not yet resolved hyperglycemic toxicity, and some patients had more relaxed glycemic control targets due to advanced age or high risk, these results further confirmed the effective blood glucose control of the three regimens. 2) Glycemic variability: After regimen conversion, the overall glycemic variability (CVdaytime, CVnighttime, CV) and inter-day glycemic variability (CVFBS, MODD) in all three groups, except for CVnighttime in the IDeg group, further decreased compared with the CSII period. Specifically, CVnighttime and CVFBS these two parameters which were more related with basal insulin, remained stable after transition in the IDeg group and significantly decreased in the IDegAsp and IDegLira groups, indicated a high therapeutic predictability. 3) Risks of hyperglycemia and hypoglycemia: After regimen conversion, TAR and HBGI, representing the risk of hyperglycemia, further decreased in all three groups. TBR increased in the IDeg group, likely due to the increased risk of hypoglycemia associated with multiple daily injections (MDI) with rapid-acting insulin in most patients in this group. However, compared with the CSII period, LBGI, reflecting both the duration and intensity of hypoglycemia, showed no statistical difference, indicating no increased risk of severe hypoglycemia. In the IDegAsp and IDegLira groups, there were no statistical differences in TBR and LBGI before and after regimen conversion, indicating a safer and smoother transition for these two regimens. Moreover, the changes in TBR after regimen conversion in all three groups also suggested that the increase in TIR was mainly attributed to the reduction in TAR, that is, further improvement of hyperglycemia. The above results indicate that after initial stabilization of blood glucose through CSII, all three regimens could achieve effective blood glucose control and a smooth transition, especially the IDegAsp and IDegLira regimens.
Subsequently, a comparative analysis was conducted among the three groups, focusing on three key dimensions: overall glycemic control, glycemic variability, and the risks of hyperglycemia and hypoglycemia. In terms of overall glycemic control, the IDegLira and IDegAsp groups exhibited comparable levels of GMI, MG, and TIR, which were significantly superior to those observed in the IDeg group. This superiority in glycemic control is likely attributable to the effective postprandial glucose management achieved by both IDegLira and IDegAsp, aligning with the findings of Kawaguchi et al, who reported delayed postprandial insulin secretion in Chinese patients with T2DM.6 This also elucidates the observed superiority of the IDegLira and IDegAsp groups in terms of overall and daytime glycemic variability compared to the IDeg group. The nighttime CV was likewise more favorable in the IDegLira and IDegAsp groups than in the IDeg group, likely due to the carryover effect of postprandial glucose fluctuations into the nocturnal period, which may influence the temporary adjustment of pre-sleep insulin doses. Furthermore, both MODD and CVFBS, which are indicators of daytime glycemic variability, were found to be lowest in the IDegLira group, followed by the IDegAsp group, and highest in the IDeg group. The results of TAR and HBGI indicated that the IDegAsp and IDegLira groups demonstrated better performance in controlling hyperglycemia compared to the IDeg group. Conversely, the results of TBR and LBGI revealed that the IDegAsp and IDegLira groups had a lower risk of hypoglycemia than the IDeg group. This difference is likely due to the higher insulin doses and more frequent MDI regimens used in the IDeg group, which are associated with an increased risk of hypoglycemia.
Diabetes treatment should be patient-centered. From the patient perspectives, we compared the convenience of the discharge insulin regimens across the three groups and assessed patient quality of life and satisfaction through telephone follow-ups utilizing the TRIM-D and SF-12 V2 questionnaires. At discharge, over half of the patients in the IDegLira group required only one or no additional antidiabetic medications, which was superior to the other two regimens. This simplification of treatment could enhance patient compliance and the sustainability of post-discharge glucose control plans, which is consistent with findings from a study in Italy.32 At a three-month follow-up post-discharge, patients using IDegLira reported superior blood glucose management, characterized by effective weight management, reduced hypoglycemic episodes, and improved vitality. These benefits are likely due to the weight-loss and lower hypoglycemia risk associated with liraglutide in the IDegLira regimen, which further contributes to enhanced vitality. The slightly poorer blood glucose control and higher levels of nervousness or anxiety reported by patients in the IDeg group may be attributed to the insufficient glycemic control and inconvenience of MDI.
In addition to our primary research objectives, several ancillary findings emerged from our study. Nocturnal hypoglycemia serves as a critical safety metric for evaluating basal insulin therapies. The management of T2DM with insulin thus requires a nuanced balance, aiming to optimize glucose control while simultaneously minimizing the risk of hypoglycemia, regardless of the specific insulin preparation employed. Presently, the majority of studies focus on the severity of hypoglycemic events, with less attention given to the timing of these occurrences.33–36 The traditional practice of using 03:00 capillary blood glucose measurements, as popularized by the Diabetes Control and Complications Trial, to identify nocturnal hypoglycemia, may not be applicable for IDeg, as the glycemic nadir for IDeg does not consistently occur at this time.37 The glycemic nadir was observed to be nearly uniformly distributed across the night, with no significant clustering around 03:00 in the IDegAsp and IDegLira groups. This finding suggests a need to reevaluate standard monitoring times for nocturnal hypoglycemia, and underscores the importance of CGM.
The novelty of this study is its concentration on the initial insulin therapy during hospitalization and the transition post-discharge, facilitated by the initial use of insulin pumps and CGM for determining initial dosages. By employing CGM and incorporating parameters such as TITR, LBGI and HBGI, our assessment of glucose control and the risks of both hyperglycemia and hypoglycemia is enhanced. We advocate for the use of CGM to comprehensively assess nocturnal hypoglycemia. For treatment regimens involving IDeg, particular attention should be given to blood glucose levels at and after 4:00. Moreover, we also assessed outcomes related to patient-level adherence and quality of life.
The single-center, retrospective design of our study may limit the generalizability of our findings to other healthcare settings with different patient populations and clinical practices. Furthermore, the three-month follow-up period primarily captures short-term outcomes and does not inform on long-term adherence or the durability of glycemic control. Therefore, future research with larger, multicenter cohorts and longer follow-up periods is necessary to validate and expand upon our results.
Conclusion
Our study demonstrates the clinical efficacy of all three IDeg-based therapies in glucose control for hospitalized patients with T2DM. IDegAsp and IDegLira demonstrated superior glycemic control and reduced variability compared to IDeg. IDegLira was more convenient and associated with higher patient satisfaction. However, these findings and their generalizability should be interpreted considering the single-center, retrospective design and short follow-up duration of our study.
Abbreviations
CGM, Continuous Glucose Monitoring; CV, Coefficient of Variation; CSII, Continuous Subcutaneous Insulin Infusion; FBS, Fasting Blood Sugar; GMI, Glucose Management Indicator; HBGI, High Blood Glucose Index; IDeg, Insulin degludec; IDegAsp, Insulin degludec/insulin aspart; IDegLira, Insulin degludec and liraglutide; LBGI, Low Blood Glucose Index; MG, Mean Glucose; MODD, Mean of Daily Differences; OADs, Oral Anti-diabetic Drugs; SD, Standard Deviation; T2DM, Type 2 Diabetes Mellitus; TAR, Time Above Range; TBR, Time Below Range; TIR, Time in Range; TITR, Time in Tight Range; TRIM-D, Treatment Related Impact Measures-Diabetes; GLP-1RA, Glucagon-like Peptide-1 Receptor Agonist; SF-12 v2, 12-item Short Form Health Survey version 2.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
Ethical approval was obtained from the Ethics Committee of the First Affiliated Hospital of Xi’an Jiaotong University (No. XJTU1AF2023LSK-458) and the committee approved exemption from written informed consent from the patients.
Acknowledgments
The authors acknowledge the effort of all the participants.
Author Contributions
Ruiqing Dong and Lifan Gu were responsible for Data curation, Software and Writing – original draft. Heping Li led the data curation and project administration efforts, with support from Yukun Zhao in both roles. Yuanna Hu, Hui Liu, Xuna Kou, and Meng Zhao also participated in Data curation. Bingyin Shi was responsible for Conceptualization, Project administration, Funding acquisition and Supervision. Hui Guo and Wei Qiang were responsible for Conceptualization, Methodology, Funding acquisition and Writing – review & editing. All authors took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was funded by Key Research and Development Program of Shaanxi Province (No. 2023-ZDLSF-40 and No. 2021LL-JB-06), and National Innovation Center for Advanced Medical Devices (No. NMED2023AGP-013 and No. NMED2023AGP-014). No funding body participated in the design of the study and the collection, analysis, and interpretation of data and the writing of the paper.
Disclosure
The authors have no conflicts of interest to declare.
References
1. Chen M, Zhang P, Zhao Y, et al. Where to initiate basal insulin therapy: inpatient or outpatient department? Real-world observation in China. Diab Metab Syndrome Obes. 2022;15:3375–13. doi:10.2147/DMSO.S386230
2. Brod M, Alolga SL, Meneghini L. Barriers to initiating insulin in type 2 diabetes patients: development of a new patient education tool to address myths, misconceptions and clinical realities. Patient. 2014;7(4):437–450. doi:10.1007/s40271-014-0068-x
3. Saisho Y. β-cell dysfunction: its critical role in prevention and management of type 2 diabetes. World J Diabetes. 2015;6(1):109–124. doi:10.4239/wjd.v6.i1.109
4. Mosenzon O, Raz I. Intensification of insulin therapy for type 2 diabetic patients in primary care: basal-bolus regimen versus premix insulin analogs: when and for whom? Diab Care. 2013;36 Suppl 2(Suppl 2):S212–218. doi:10.2337/dcS13-2007
5. Kataoka M, Venn BJ, Williams SM, et al. Glycaemic responses to glucose and rice in people of Chinese and European ethnicity. Diabet Med. 2013;30(3):e101–107. doi:10.1111/dme.12080
6. Kawaguchi Y, Miyamoto S, Hajika Y, et al. Efficacy of IDegLira versus IDegAsp therapy in patients with type 2 diabetes: a randomized crossover study by isCGM. Adv Ther. 2022;39(6):2688. doi:10.1007/s12325-022-02138-w
7. Philis-Tsimikas A, Astamirova K, Gupta Y, et al. Similar glycaemic control with less nocturnal hypoglycaemia in a 38-week trial comparing the IDegAsp co-formulation with insulin glargine U100 and insulin aspart in basal insulin-treated subjects with type 2 diabetes mellitus. Diabetes Res Clin Pract. 2019;147:157–165. doi:10.1016/j.diabres.2018.10.024
8. Kaneko S, Chow F, Choi DS, et al. Insulin degludec/insulin aspart versus biphasic insulin aspart 30 in Asian patients with type 2 diabetes inadequately controlled on basal or pre-/self-mixed insulin: a 26-week, randomised, treat-to-target trial. Diabetes Res Clin Pract. 2015;107(1):139–147. doi:10.1016/j.diabres.2014.09.026
9. Luo Q, Zhou L, Zhou N, et al. Cost-effectiveness of insulin degludec/insulin aspart versus biphasic insulin aspart in Chinese population with type 2 diabetes. Front Public Health. 2022;10:1016937. doi:10.3389/fpubh.2022.1016937
10. Yang W, Ma J, Hong T, et al. Efficacy and safety of insulin degludec/insulin aspart versus biphasic insulin aspart 30 in Chinese adults with type 2 diabetes: a Phase III, open‐label, 2:1 randomized, treat‐to‐target trial. Diabetes Obesity Metab. 2019;21(7):1652. doi:10.1111/dom.13703
11. Holst JJ, Buse JB, Rodbard HW, et al. IDegLira improves both fasting and postprandial glucose control as demonstrated using continuous glucose monitoring and a standardized meal test. J Diabetes Sci Technol. 2015;10(2):389. doi:10.1177/1932296815610124
12. King AB, Philis-Tsimikas A, Kilpatrick ES, et al. A fixed ratio combination of insulin degludec and liraglutide (IDegLira) reduces glycemic fluctuation and brings more patients with type 2 diabetes within blood glucose target ranges. Diabetes Technol Ther. 2017;19(4):255. doi:10.1089/dia.2016.0405
13. He X, Chen L, Wang K, et al. Insulin adherence and persistence among Chinese patients with type 2 diabetes: a retrospective database analysis. Patient Preference Adherence. 2017;11:237–245. doi:10.2147/PPA.S123389
14. Niu YL, Zhang Y, Song ZY, et al. Efficacy and safety of insulin degludec/insulin aspart versus biphasic insulin aspart 30 in patients with type 2 diabetes: a meta-analysis of randomized controlled trials. Iran J Public Health. 2024;53(2):313–322. doi:10.18502/ijph.v53i2.14916
15. Chinese Society of Endocrinology, Chinese Diabetes Society, Chinese Endocrinologist Association. China Insulin Pump Clinical Guideline(2021). Chin J Endocrinol Metab. 2021;37(08):679–701 doi:10.3760/cma.j.cn311282-20210428-00265.
16. Frontoni S, Di Bartolo P, Avogaro A, et al. Glucose variability: an emerging target for the treatment of diabetes mellitus. Diabetes Res Clin Pract. 2013;102(2):86–95. doi:10.1016/j.diabres.2013.09.007
17. Danne T, Nimri R, Battelino T, et al. International consensus on use of continuous glucose monitoring. Diabetes Care. 2017;40(12):1631–1640. doi:10.2337/dc17-1600
18. Battelino T, Alexander CM, Amiel SA, et al. Continuous glucose monitoring and metrics for clinical trials: an international consensus statement. Lancet Diabetes Endocrinol. 2023;11(1):42–57. doi:10.1016/S2213-8587(22)00319-9
19. Brod M, Hammer M, Christensen T, et al. Understanding and assessing the impact of treatment in diabetes: the treatment-related impact measures for diabetes and devices (TRIM-Diabetes and TRIM-Diabetes Device). Health Qual Life Outcomes. 2009;7(1):83. doi:10.1186/1477-7525-7-83
20. Fong DYT, Chan BKY, Li S, et al. Average and individual differences between the 12-item MOS Short-form Health Survey version 2 (SF-12 V.2) and the veterans RAND 12-item Health Survey (VR-12) in the Chinese population. Health Qual Life Outcomes. 2022;20:102. doi:10.1186/s12955-022-02010-z
21. Chinese Diabetes Society. Clinical application guideline for blood glucose monitoring in China (2021 edition). Chin J Diabetes Mellitus. 2021;13(10):936–948 doi:10.3760/cma.j.cn115791-20210810-00436
22. Chinese Society of Endocrinology, National Innovation Center for Advanced Medical Devices. Expert consensus on the clinical application of ambulatory glucose profile report (2023 edition). Chin J Diabetes Mellitus. 2024;16(02):190–201 doi:10.3760/cma.j.cn115791-20231120-00325.
23. Brod M, Christensen T, Hammer M, et al. Examining the ability to detect change using the TRIM-Diabetes and TRIM-Diabetes Device measures. Qual Life Res. 2011;20(9):1513–1518. doi:10.1007/s11136-011-9886-7
24. Wan EYF, Eyt Y, Chin WY, et al. Evaluation of the responsiveness of Short Form-12 Health Survey version 2 (SF-12v2) in Chinese patients with hypertension in primary care. Qual Life Res. 2019;28(10):2851–2857. doi:10.1007/s11136-019-02225-6
25. Chinese Diabetes Society. Guideline for the prevention and treatment of type 2 diabetes mellitus in China (2020 edition). Chin J Endocrinol Metab. 2021;37(04):311–398 doi:10.3760/cma.j.cn115791-20210221-00095
26. Davies MJ, Aroda VR, Collins BS, et al. Management of hyperglycemia in type 2 diabetes, 2022. a consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2022;45(11):2753–2786. doi:10.2337/dci22-0034
27. ElSayed NA, Aleppo G, Bannuru RR. American diabetes association professional practice committee. 9. pharmacologic approaches to glycemic treatment: standards of care in diabetes—2024. Diabetes Care. 2023;47(Supplement_1):S158–S178. doi:10.2337/dc24-S009
28. Kalra S, Das AK, Sahay RK, et al. Consensus recommendations on GLP-1 RA use in the management of type 2 diabetes mellitus: South Asian task force. Diab Ther. 2019;10(5):1645. doi:10.1007/s13300-019-0669-4
29. Sun W, Liu D, Yang T, et al. Increased risk of vascular complications in patients with type 2 diabetes and fatty liver disease. BMC Endocr Disord. 2024;24(1):235. doi:10.1186/s12902-024-01766-3
30. Eslam M, Newsome PN, Sarin SK, et al. A new definition for metabolic dysfunction-associated fatty liver disease: an international expert consensus statement. J Hepatol. 2020;73(1):202–209. doi:10.1016/j.jhep.2020.03.039
31. Tanase DM, Gosav EM, Costea CF, et al. The intricate relationship between type 2 Diabetes Mellitus (T2DM), Insulin Resistance (IR), and Nonalcoholic Fatty Liver Disease (NAFLD). J Diabetes Res. 2020;2020:3920196. doi:10.1155/2020/3920196
32. Fadini GP, Buzzetti R, Fittipaldi MR, et al. IDegLira for the real-world treatment of type 2 diabetes in Italy: protocol and interim results from the REX observational study. Diab Ther. 2022;13(8):1483–1497. doi:10.1007/s13300-022-01287-z
33. Goldenberg RM, Aroda VR, Billings LK, et al. Effect of insulin degludec versus insulin glargine U100 on time in range: SWITCH PRO, a crossover study of basal insulin-treated adults with type 2 diabetes and risk factors for hypoglycaemia. Diab Obes Metab. 2021;23(11):2572–2581. doi:10.1111/dom.14504
34. Özçelik S, Çelik M, Vural A, et al. Outcomes of transition from premixed and intensive insulin therapies to insulin aspart/degludec co-formulation in type 2 diabetes mellitus: a real-world experience. Arch Med Sci. 2021;17(1):1–8. doi:10.5114/aoms.2020.93264
35. Wang R, Luo S, Xiao Z, et al. Efficacy and safety of fixed-ratio combination insulin degludec/liraglutide in type 2 diabetes: a systematic review and meta-analysis of randomised controlled trials. Diabetes Metab Res Rev. 2024;40(3):e3752. doi:10.1002/dmrr.3752
36. Kaneko S, da Rocha Fernandes JD, Yamamoto Y, et al. A Japanese Study Assessing glycemic control with use of IDegAsp Co-formulation in patients with type 2 diabetes in clinical practice: the JAGUAR study. Adv Ther. 2021;38(3):1638–1649. doi:10.1007/s12325-021-01623-y
37. Škrha J, Škrha J, Škrha J, et al. Glucose variability, HbA1c and microvascular complications. Rev Endocr Metab Disord. 2016;17(1):103–110. doi:10.1007/s11154-016-9347-2
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.