Back to Journals » Drug Design, Development and Therapy » Volume 8
Transient hypofibrinogenemia due to allopurinol
Authors Yin Z, Xu J, Li Y, Xia J, Luo D
Received 27 April 2014
Accepted for publication 30 May 2014
Published 2 September 2014 Volume 2014:8 Pages 1231—1233
DOI https://doi.org/10.2147/DDDT.S66868
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
ZhiQiang Yin,1,* JiaLi Xu,2,* YongQiang Li,3,* JiPing Xia,1 Dan Luo1
1Department of Dermatology, 2Department of Oncology, 3Department of Rehabilitation Medicine, The First Affiliated Hospital of Nanjing Medical University, Nanjing, Jiangsu, People's Republic of China
*These authors contributed equally to this work
Abstract: This study reports a case of an 80-year-old male who suffered from drug eruption due to oral allopurinol for the treatment of gout. This patient complained of widespread erythema and maculopapule with itch, and small quantities of purplish-red rash with diffused distribution on four limbs were noted. After he was hospitalized, the area with purpuric rash increased in size, and hypofibrinogenemia was found. After treatment with intravenous infusion of fibrinogen and cryoprecipitate, and continued treatment with high-dose methylprednisolone, the skin rash gradually went away. This is the first report of purpura and hypofibrinogenemia induced by allopurinol and the pathophysiology underlying this reaction remained unknown.
Keywords: purpura, fibrinogen, drug eruption, gout
Introduction
Allopurinol is the primary therapy for the management of gout. The common cutaneous adverse reactions are simple cutaneous manifestations and allopurinol hypersensitivity which is characterized by a spectrum of cutaneous reactions and systemic manifestations. The majority (73%) of allopurinol hypersensitivity patients are Asian.1
Herein, we present a case who suffered from widespread purpuric eruption and hypofibrinogenemia due to oral allopurinol.
Case report
An 80-year-old man presented with a mass of erythema and maculopapule with itch from head to foot without fever for 5 days, and clinical examination revealed that there were small quantities of prunosus macula with diffused distribution on the four limbs. The purplish-red rash was not discolored when we pressed it. Two days before first symptoms, he had been diagnosed with gout and begun to use treatment of oral allopurinol. The patient had also been using other medications, such as antihypertensives and Panax notoginseng saponins, for several years. There had been no other short-term special medication, diet, or exposure before rash. For this reason, we diagnosed the patient’s skin lesion as “drug eruption induced by allopurinol”. On the first day of rash and prior to the current presentation, the routine hematologic tests and liver function tests in the outpatient department showed that platelet function and liver function were within normal range.
After the patient was hospitalized, he was treated with intravenous infusion of methylprednisolone (80 mg once a day). However, the area with purpuric rash increased in size, and the original erythema also gradually turned purplish-red (Figure 1A and B). This patient denied previous similar medical history or family history of hereditary bleeding disorders. On the second and sixth days after hospitalization, platelet function and liver function tests did not reveal any abnormality, and antinuclear antibodies tests were all negative. On the tenth day, coagulation function tests showed fibrinogen level was 0.9 g/L (normal range: 2.0–4.0 g/L, von Clauss assay) and thrombin time was 23.0 seconds (normal range: 15.0–21.0 seconds). Other indices, such as d-dimer, prothrombin time, and activated partial thromboplastin time, were all within normal range. Platelet function and liver function were investigated again, and were noted to have remained normal. Next, we treated this patient with intravenous infusion of fibrinogen (1.0 g) once a day for 3 days, and on day 4, this patient was treated with intravenous infusion of cryoprecipitate (7.75 IU) once. After first infusion of fibrinogen, blood tests of coagulation function revealed an improvement in fibrinogen level (1.0 g/L) and normal thrombin time. After second infusion, blood fibrinogen level was 1.2 g/L. After third infusion of fibrinogen and following infusion of cryoprecipitate, blood fibrinogen level was 1.6 g/L. The liver function tests, d-dimer, and platelet function maintained normal levels throughout. The skin rash gradually went away (Figure 1C). Two days later, reinspection showed blood fibrinogen level had remained at 1.6 g/L. With continued treatment with high-dose methylprednisolone and gradual decrement, no new rash occurred and the patient’s condition gradually improved. After the patient was discharged from hospital, several return visits did not reveal new purpuric rash, and reinspection showed blood fibrinogen level was 1.5 g/L.
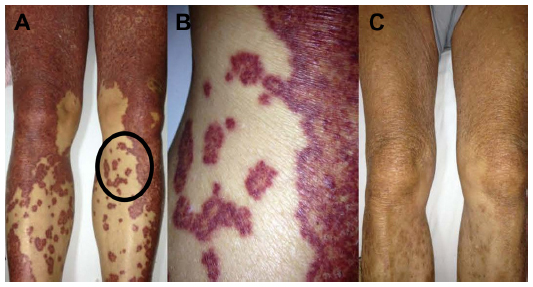 | Figure 1 Skin rash before and after treatment. |
Discussion
Allopurinol, an analog of hypoxanthine, has been used worldwide for the treatment of hyperuricemia and gout for over 40 years. Unfortunately, some patients assuming this medication, developed hypersensitivity reactions ranging from mild cutaneous eruption to more severe clinical manifestations such as allopurinol hypersensitivity syndrome or Steven–Johnson syndrome and lethal toxic epidermal necrolysis.2 Further, the US Food and Drug Administration has reported 236 patients with purpura due to allopurinol, primarily old men. Allopurinol-induced widespread purpura and hypofibrinogenemia has not been reported before, to the best of our knowledge.
Purpuric drug eruption reports in the literature are not scarce, with the relevant drugs including angiotensin II receptor blockers,3 lenalidomide,4 and gefitinib,5 among others. Chen et al reported valproic acid-associated low fibrinogen and delayed intracranial hemorrhage,6 and Matrat et al described two cases of severe hypofibrinogenemia induced by alteplase.7 There have been several reports of hypofibrinogenemia associated with prednisone therapy.8–10 In our case, the patient presented with widespread erythema and maculopapule with pruritus initially, and we found there were small quantities of prunosus macula with diffused distribution on four limbs before glucocorticoid treatment. The purplish-red rash was not discolored when we pressed it. After treatment with high-dose methylprednisolone, the area with purpuric rash increased in size. Fibrinogen determination showed hypofibrinogenemia. After hypofibrinogenemia was corrected, continued high-dose methylprednisolone did not induce new purpura. According to the above points, especially the existence of prunosus macula before glucocorticoid treatment, we considered transient hypofibrinogenemia not to have been induced by methylprednisolone.
According to the World Health Organization’s Uppsala Monitoring Centre for standardized case causality assessment11, the causality in our case was “probable/likely”. “Certain” was inapplicable because this patient refused rechallenge. The informed consent for using the patient’s photo was appropriately obtained.
Patients with hypofibrinogenemia are usually asymptomatic, and bleeding is only seen after trauma.12 This patient presented with widespread erythema and maculopapule with pruritus initially, which indicated potential vasodilatation in dermis and increased small vessel permeability. In such a case of increased vascular permeability, hypofibrinogenemia might more easily lead to hemorrhagic skin lesions.
Drug patch tests (DPTs) are useful in maculopapular rashes, flexural exanthemas, and, if done in situ, in fixed drug eruption also. Their best indication is in acute generalized exanthematous pustulosis or drug reaction with eosinophilia and systemic symptoms, where DPTs are useful in tests involving carbamazepine or proton pump inhibitors but they are not useful in testing involving allopurinol or sulfasalazine.13 We did not carry out DPTs for this patient because of his refusal.
This is the first report of purpura and hypofibrinogenemia induced by allopurinol, and in which the pathophysiology underlying this reaction remained unknown. This patient denied previous similar medical history or family history of hereditary bleeding disorders. After the patient was hospitalized, we did not find any bleeding tendency, and liver function tests, platelet function, d-dimer, prothrombin time, and activated partial thromboplastin time were all within normal range. Fibrinogen level was significantly lower than the normal value, and thrombin time exceeded normal values. Therefore, we speculate that the pathophysiology of hypofibrinogenemia might be a transient decreased fibrinogen production. Probably allopurinol affected the fibrinogen synthesis function of liver temporarily. This case was unique and can serve as a useful reference and warning for clinicians.
Acknowledgments
This work was supported by the National Natural Science Foundation of China (81171518, 81301387) and the Priority Academic Program Development of Jiangsu Higher Education Institutions (JX10231801).
Disclosure
The authors report no conflicts of interest in this work.
References
Ramasamy SN, Korb-Wells CS, Kannangara DR, et al. Allopurinol hypersensitivity: a systematic review of all published cases, 1950–2012. Drug Saf. 2013;36(10):953–980. | |
Calogiuri G, Nettis E, Di Leo E, Foti C, Ferrannini A, Butani L. Allopurinol hypersensitivity reactions: desensitization strategies and new therapeutic alternative molecules. Inflamm Allergy Drug Targets. 2013;12(1):19–28. | |
Foti C, Carbonara AM, Guida S, et al. Frictional purpuric eruption associated with angiotensin II receptor blockers. Dermatol Ther. 2014;27(2):97–100. | |
Kuohung V, Goldberg LJ, Demierre MF. Lenalidomide-induced purpuric eruption: a new adverse cutaneous reaction. J Am Acad Dermatol. 2011;65(3):654–656. | |
Uchimiya H, Higashi Y, Kawai K, Kanekura T. Purpuric drug eruption with leukocytoclastic vasculitis due to gefitinib. J Dermatol. 2010;37(6):562–564. | |
Chen HF, Xu LP, Luo ZY, et al. Valproic acid-associated low fibrinogen and delayed intracranial hemorrhage: case report and mini literature review. Drug Des Devel Ther. 2013;7:767–770. | |
Matrat A, De Mazancourt P, Derex L, et al. Characterization of a severe hypofibrinogenemia induced by alteplase in two patients thrombolysed for stroke. Thromb Res. 2013;131(1):e45–e48. | |
Yokose N, Ogata K, Nakamura K, et al. Hypofibrinogenemia induced by prednisolone therapy in a patient with chronic lymphocytic leukemia complicated with autoimmune hemolytic anemia. Am J Hematol. 1997;55(3):166–167. | |
Miura T, Nakamura M, Tsunematsu Y, Fujimoto J, Meguro T, Yamada K. Hypofibrinogenemia in a girl with Langerhans cell histiocytosis during etoposide and prednisolone therapy. Acta Paediatr Jpn. 1993;35(2):148–150. | |
Al-Mondhiry H. Hypofibrinogenemia associated with vincristine and prednisone therapy in lymphoblastic leukemia. Cancer. 1975;35(1):144–147. | |
Zaki SA. Adverse drug reaction and causality assessment scales. Lung India. 2011;28(2):152–153. | |
Peyvandi F, Haertel S, Knaub S, Mannucci PM. Incidence of bleeding symptoms in 100 patients with inherited afibrinogenemia or hypofibrinogenemia. J Thromb Haemost. 2006;4(7):1634–1637. | |
Barbaud A. Skin testing and patch testing in non-IgE-mediated drug allergy. Curr Allergy Asthma Rep. 2014;14(6):442. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.