Back to Journals » Clinical Ophthalmology » Volume 14
Transepithelial Accelerated Corneal Collagen Cross-Linking: Two-Year Results
Authors Cunha AM ![]() , Sardinha T, Torrão L
, Sardinha T, Torrão L ![]() , Moreira R, Falcão-Reis F, Pinheiro-Costa J
, Moreira R, Falcão-Reis F, Pinheiro-Costa J ![]()
Received 8 March 2020
Accepted for publication 30 June 2020
Published 14 August 2020 Volume 2020:14 Pages 2329—2337
DOI https://doi.org/10.2147/OPTH.S252940
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Ana Maria Cunha,1 Tiago Sardinha,2 Luís Torrão,1 Raúl Moreira,1 Fernando Falcão-Reis,1,3 João Pinheiro-Costa1,4
1Department of Ophthalmology, Centro Hospitalar De São João, Porto, Portugal; 2Faculty of Medicine, University of Porto, Porto, Portugal; 3Department of Surgery and Physiology, Faculty of Medicine, University of Porto, Porto, Portugal; 4Department of Biomedicine, Faculty of Medicine, University of Porto, Porto, Portugal
Correspondence: Ana Maria Cunha
Department of OphthalmologyJoão, Centro Hospitalar De São, Avenida Prof. Hernâni Monteiro, 4202 – 451, Porto, Portugal
Tel +351 225512100
Fax +351 225513669
Email [email protected]
Purpose: To report 2-year outcomes of trans-epithelial accelerated corneal collagen crosslinking (TE-ACXL) procedure in the treatment of progressive keratoconus patients.
Patients and Methods: Twenty-four eyes from 24 patients who underwent TE-ACXL (6mW/cm2 for 15 minutes) were included in this retrospective interventional study. Best-corrected visual acuity (BCVA), keratometry values, thinnest corneal thickness (PachyMin) and topometric indexes were analysed preoperatively and at 6-month, 12-month, 18-month and 24-month postoperative. Progression was assessed by increase ≥ 1.00D in maximum keratometry (Kmax); increase ≥ 1.00D in corneal astigmatism; decrease ≥ 2% in PachyMin; increase ≥ 0.42 in D-index.
Results: There were no complications during or after TE-ACXL. No significant differences (Δ) were observed between baseline and 12-month or 24-month postoperative: ∆BCVA (− 0.08 ± 0.25, p=0.190; − 0.04 ± 0.17, p=0.588), ∆Kmax (− 0.08 ± 1.32, p=0.792; − 1.04 ± 1.89, p=0.135), ∆Astigmatism (− 0.15 ± 0.89, p=0.485; − 0.24 ± 1.38, p=0.609), ∆PachyMin (− 0.56 ± 15.70, p=0.882; 0.56 ± 18.74, p=0.931), ∆Index Surface Variation (∆ISV) (− 2.11 ± 10.27, p=0.395; − 4.67 ± 17.32, p=0.442), ∆Index Vertical Asymmetry (∆IVA) (− 0.05 ± 0.17, p=0.208; − 0.08 ± 0.26, p=0.397), ∆Index Height Decentration (∆IHD) (0.00 ± 0.02, p=0.368; − 0.01 ± 0.04, p=0.484), ∆KI (0.00 ± 0.05, p=0.851; 0.01 ± 0.06, p=0.877) and ∆D-index (0.15 ± 1.14, p=0.572; 0.06 ± 1.36, p=0.892). Eleven to 33% of patients had disease progression at 24-month postoperative according to the parameters used to determine progression.
Conclusion: Although some patients maintain disease progression, TE-ACXL seems to be a safe and effective treatment for keratoconus over the 2-year follow-up period. Studies with longer follow-up periods and larger patient cohorts are recommended.
Keywords: cornea, keratoconus, disease progression, transepithelial, cross-linking
Introduction
Keratoconus is the most common corneal ectasia, described as a progressive, bilateral and asymmetric disorder.1 The cornea assumes a conical shape after irregular stromal thinning and protrusion, resulting in irregular astigmatism, myopia and subsequent mild to marked deterioration of quality of vision.1,2 This condition seems to emerge in the second decade of life and progresses until the middle age.2
The aetiology of the disease is not well understood. Some authors point out an absence of cellular infiltration and vascularization and categorise keratoconus as a noninflammatory disease.1 The recent scientific literature shows a multifactorial cause, including a genetic predisposition and environmental factors that may induce local inflammation through inflammatory mediators and oxidative stress.2,3 Proteolytic enzymes, cytokines and free radicals seem to be the main cause of the stromal thinning.3 There is a positive correlation between keratoconus and eye rubbing, atopy, ocular allergy, Down syndrome, connective tissue disorders (Ehlers-Danlos, Marfan syndrome), Leber’s congenital amaurosis and mitral valve prolapse.2,4
Any patient with an irregular astigmatism should be suspected of having keratoconus.1 Nowadays, corneal topography and pachymetry are the most useful tools in the diagnosis and evaluation of keratoconus since they can document elevation maps and corneal thickness.2,3
Over the past twenty years keratoconus treatment has evolved.5,6 Previously, treatment mainly included strategies to improve visual acuity (eg: rigid contact lens, corneal rings and penetrating keratoplasty) and none of them changed the natural history of the disease.4 Corneal collagen crosslinking (CXL) has recently been shown to be effective as a minimally invasive treatment to slow or stop progression of keratoconus.2,7 CXL is the only treatment option that focuses on disease pathology and increases the biomechanical rigidity of the cornea.8 Ultraviolet A (UVA) radiation reacts with riboflavin molecules (vitamin B2) which generate oxygen free radicals that will interact with the corneal stroma increasing intra and interfibrillar covalent bonds between the collagen fibrils, establishing crosslinks between collagen molecules and microfibrils and increasing corneal rigidity.7–10
The conventional Dresden Protocol of corneal collagen crosslinking (C-CXL) was first described by Wollensack et al in a prospective non-randomized clinical trial that aimed at stopping progression of the disease.11 This involves an epithelial debridement (facilitate stromal riboflavin absorption), application of a 0.10% riboflavin 5-phosphate solution for 30 minutes and exposure to UVA (365 nm, 3 mW/cm2) radiation for 30 minutes. The total energy dissipated is 5.4 J/cm2,7,11 debriding corneal epithelium increases the risk of infection, sub-epithelial haze, sterile corneal infiltrates, corneal scarring, endothelial damage and pain and delays visual rehabilitation.8
Accelerated protocols evolved to shorten the treatment duration and reduce the postoperative complications of previous protocols. According to the Bunsen-Roscoe law, the same photochemical effect can be achieved by reducing illumination time and correspondingly increasing irradiation intensity.6,7 Long-term efficacy and safety of trans-epithelial accelerated corneal crosslinking (TE-ACXL) on progressive keratoconus treatment is not fully understood. This protocol may surpass some disadvantages of conventional protocol, making it a more appealing and promising treatment option. Nevertheless, TE-ACXL also have disadvantages derived the trans-epithelial technique, due to epithelium acts as a barrier to riboflavin and oxygen,12,13 and the accelerated procedure, based on the Bunsen-Roscoe law, does not take into consideration biological effect in the tissues.14 Considering its advantages and disadvantages, more studies to evaluate the role of this protocol in keratoconus treatment are needed.
In the current study, the authors report 2-year outcomes of TE-ACXL procedure in the treatment of patients with progressive keratoconus.
Patients and Methods
This is a retrospective interventional study carried out on 24 eyes with diagnosis of progressive keratoconus which underwent TE-ACXL (6mW/cm2 for 15 minutes) between 2016 and 2018 at Ophthalmology Corneal Department of Centro Hospitalar Universitário de São João. This study was performed in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Centro Hospitalar Universitário de São João. Written informed consent was obtained from all patients or legal guardian, in patients under the age of consent, before surgical interventions. Medical records of all patients who underwent TE-ACXL were analysed between December 2018 and January 2019.
The inclusion criteria were age between 14 and 32 years, pachymetry at the thinnest point (PachyMin) ≥ 380 µm or more and documented progression of keratoconus. The diagnosis of progressive keratoconus was defined as 1 or more of the following changes in the previous 6 months: an increase ≥ 1.00 diopter (D) in maximum keratometry (Kmax), a 2% decrease in PachyMin, an increase ≥ 1.00 D in corneal cylinder.
The exclusion criteria were previous history of cornea surgery, apical corneal scarring, delayed epithelial healing, severe dry eye, ocular infections, connective tissue disease, pregnancy and lactation.
All patients had preoperative, at 6, 12, 18 and 24-month postoperative evaluation. Best-corrected visual acuity (BCVA) was recorded using a Snellen chart and converted to the logarithm of minimal angle of resolution (logMAR) units for statistical analysis. Mean keratometry (Kmean), Kmax, Astigmatism (K2-K1), PachyMin, index of surface variance (ISV), index of vertical asymmetry (IVA), index of height decentration (IHD), keratoconus index (KI) and Belin/Ambrósio D-index were recorded using Oculus Pentacam (Pentacam HR, Oculus Optikgeräte GmbH, Wetzlar, Germany). Keratoconus Classification (KC) is according to Pentacam HR® Ktc Score System.
To assess progression at 12-month and 24-month postoperative the following parameters were used: an increase ≥ 1.00 D in Kmax, an increase ≥ 1.00 D in corneal astigmatism (K2-K1), a decrease ≥ 2% in thinnest pachymetry and an increase ≥ 0.42 in D-index.
Surgical Technique
The procedure was carried out under aseptic conditions in an operative room. Oxybuprocaine hydrochloride 4 mg/mL anaesthetic drops were instilled on the ocular surface. TE-ACXL was carried out through intact corneal epithelium, 0.25% riboflavin, benzalkonium chloride (BAC), ethylenediamine tetra-acetic acid (EDTA) and trometamol (Tris), and 0.45% phosphate buffer saline preparation was applied to the cornea every 3 minutes for 30 minutes, and then the anterior chamber flare was assessed to confirm the saturation of the corneal stroma. Afterwards, cornea was exposed to the UVA light with an intensity of 6 mW/cm2 for 15 minutes. During this period, riboflavin solution was administered every 5 minutes and a sterile balance sodium solution every 2 minutes to preclude excessive corneal dehydration. The total dose intensity was 5.4 J/cm2.
Postoperative Care
Antibiotic eye drops (ofloxacin 0.30%) for a week, topical steroids eye drops (fluorometholone 0.10%) for three months and sodium hyaluronate 0.20% as needed were administered postoperatively. Follow-up of the patient was scheduled for day 1 postoperatively and subsequently at 3, 6, 12, 18 and 24 months postoperatively.
Statistical Analysis
For the description of the samples’ characteristics, data are presented as counts and proportions for categorical variables, and as mean and standard deviation for continuous variables. The prospective variation in keratometric indices was calculated subtracting the readings at baseline from the readings at different follow-up points (ie a positive delta value implies an increase in the readings of that specific parameter). For comparison of preoperative and postoperative variables, paired t-tests were used. Multiple-related samples were compared with 1-way repeated measures ANOVA test. The significance level was set at 0.05. Statistical analysis was conducted using SPSS statistical software package version 24 (SPSS inc., Chicago IL., USA).
Results
Twenty-four eyes of 24 patients (20 males and 4 females) fulfilled the inclusion criteria and were included in the study. Mean age of this study population was 19.16 ± 4.21 years (range from 14 to 30 years). Baseline characteristics such as demographic, clinical, visual, keratometric, pachymetric and topographic parameters are displayed in Table 1. The preoperative mean of KC was 2.79 ± 0.67. The most frequent grade of KC was 3 (N = 10), the second was 3.50 (N = 6). The distribution of KC grade at baseline is presented in Figure 1. The mean differences (Δ) between baseline and 6, 12, 18 and 24 months postoperative are shown in Table 2. From the 24 eyes included in the study, all of them complete the 6-months follow-up, 18 eyes complete the 12-months follow-up, 10 eyes complete the 6-months follow-up, 9 eyes complete the 6-months follow-up. All surgical procedures were performed uneventfully and there were no complications registered during the follow-up.
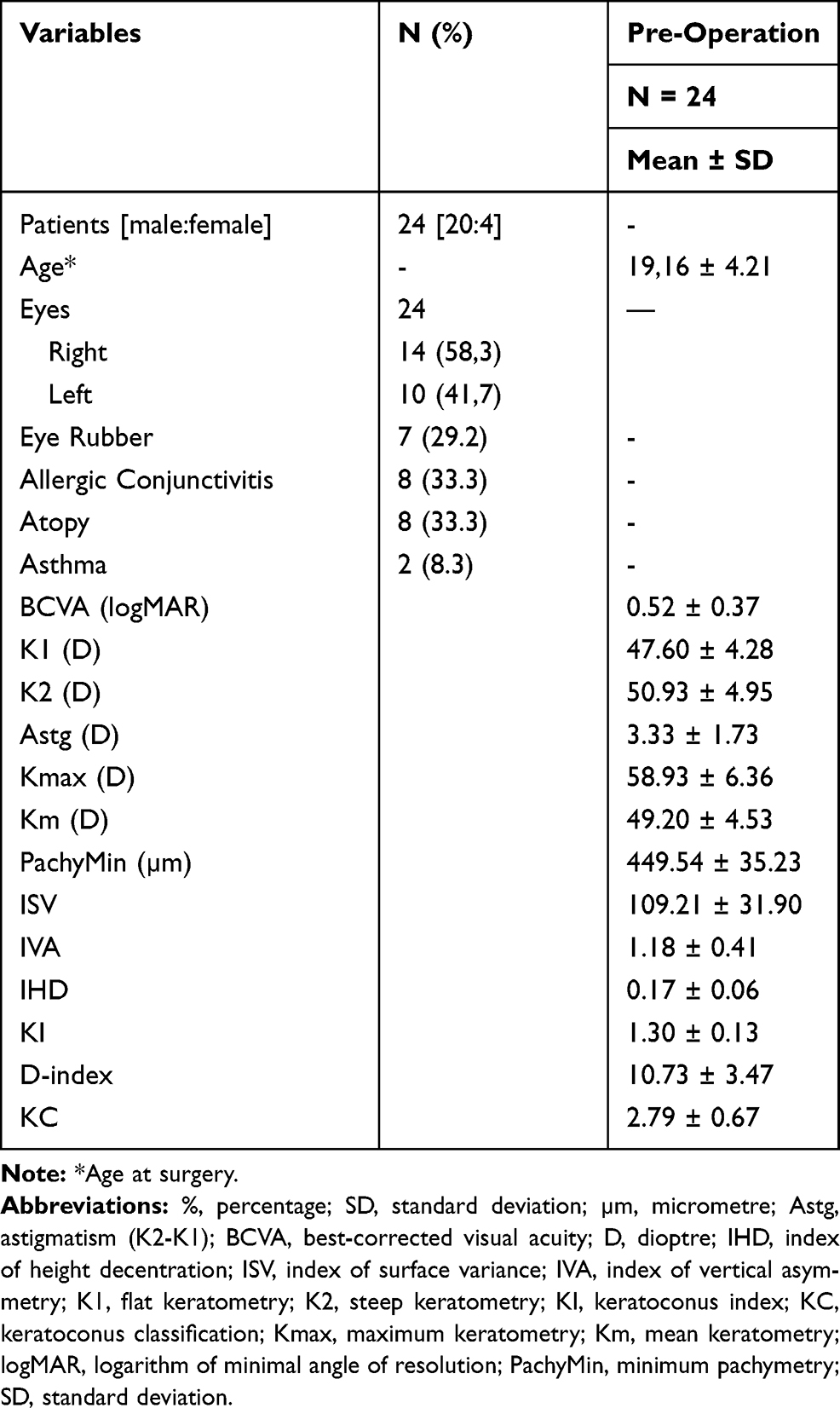 |
Table 1 Baseline Demographic, Clinical, Visual, Corneal Topographic, Tomographic and Pachymetric Characteristics of Patients Undergoing Transepithelial Accelerated Crosslinking |
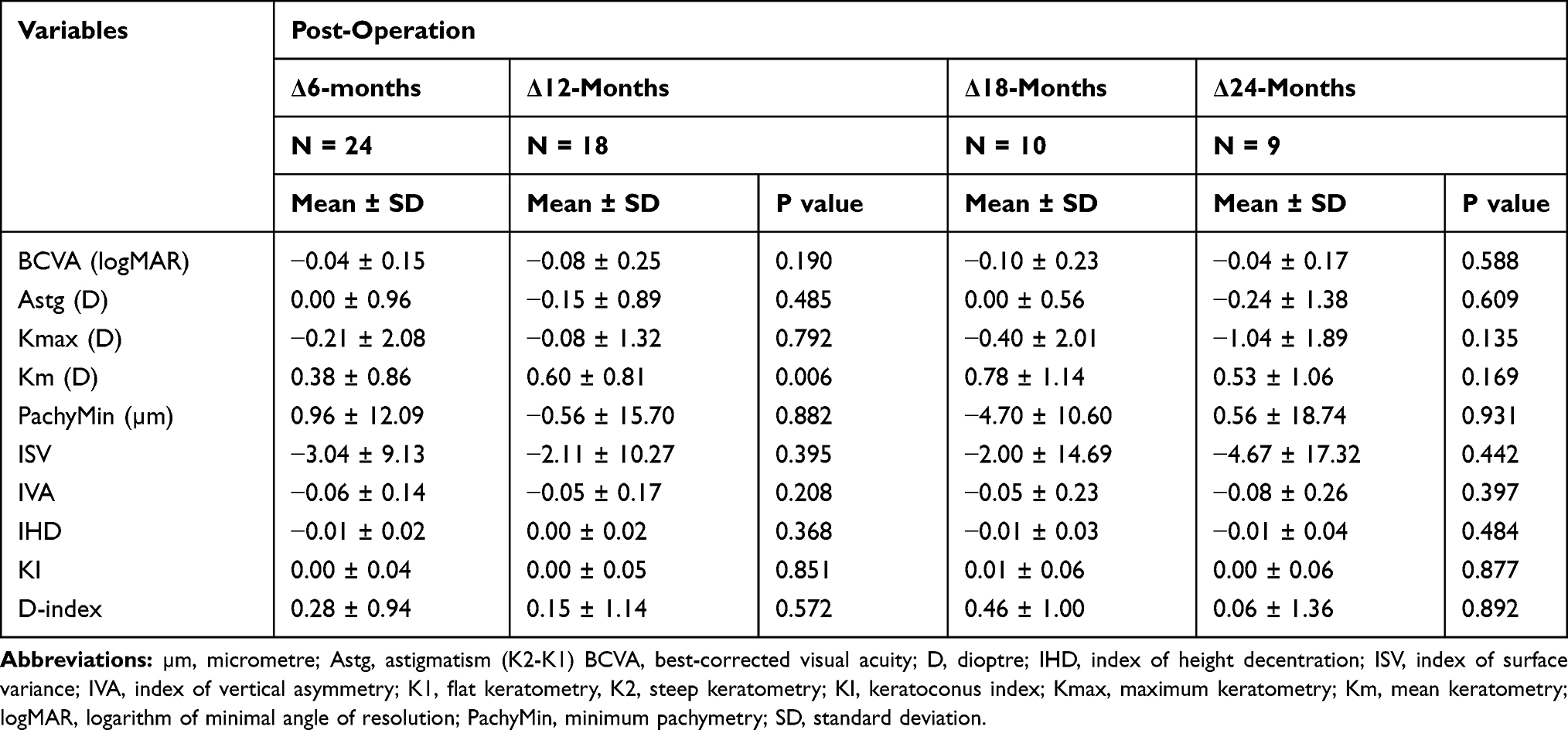 |
Table 2 Mean Changes in Visual, Corneal Tomographic, Topographic and Pachymetric Parameters Between 6, 12, 18, 24 Months and Baseline Values |
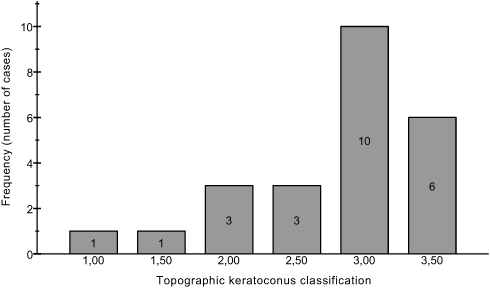 |
Figure 1 Distribution of baseline Keratoconus classification. |
Visual Acuity
The preoperative mean BCVA was 0.52 ± 0.37 logMAR. Mean variation of BCVA was −0.08 ± 0.25 logMAR at 12 months and −0.04 ± 0.17 logMAR at 24 months, postoperatively. After 12 (p = 0.190) and 24 (p = 0.588) months of surgery, there was no significant difference compared to baseline values. Figure 2 compares baseline mean BCVA and changes over time at 6, 12, 18 and 24 months after the procedure.
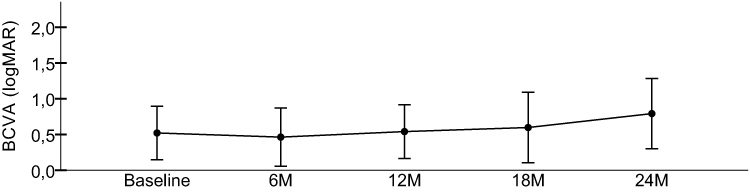 |
Figure 2 Best-corrected visual acuity (BCVA) in LogMAR compared with baseline at 6, 12, 18 and 24 months after trans-epithelial accelerated CXL. |
Keratometry
The preoperative mean Kmax was 58.93 ± 6.36 D and mean Km was 49.20 ± 4.53 D. Mean variation of Kmax was −0.08 ± 1.32 D at 12 months and −1.04 ± 1.89 D at 24 months, postoperatively. At 12 and 24 months of follow-up, no significant changes were found (Kmax, p = 0.792 and p = 0.135). Mean variation of Km was 0.60 ± 0.81 D and 0.53 ± 1.06 D at 12 and 24 months, postoperatively. There was a statistically significant increase in the Km value between baseline and 12-month postoperative (p = 0.006), but the variation of 0.53 D at 24 months was not significant (p = 0.169). Mean variation of corneal astigmatism (K2-K1) was −0.15 ± 0.89 D (p = 0.485) and −0.24 ± 1.38 D (p = 0.609) at 12 and 24 months, respectively. There was no statistically significant difference compared to baseline values. Figures 3 and 4 show the variations of Kmax and Km during follow-up, respectively.
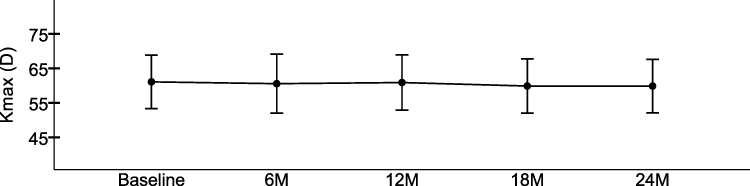 |
Figure 3 Maximum keratometry (Kmax) in dioptres (D) compared with baseline at 6, 12, 18 and 24 months after trans-epithelial accelerated CXL. |
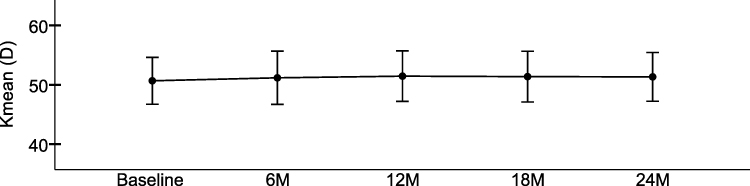 |
Figure 4 Mean Keratometry (Km) in dioptres (D) compared with baseline at 6, 12, 18 and 24 months after trans-epithelial accelerated CXL. |
Pachymetry
The preoperative mean PachyMin was 449,54 ± 35.23 µm. Mean variation of PachyMin was −0.56 ± 15.70 µm and 0.56 ± 18.74 µm at 12 and 24 months, respectively. No statistically significant changes were found after 12 months (p = 0.882) and after 24 months (p = 0.931). Figure 5 shows the variation in pachymetry overtime until 24 months after surgery.
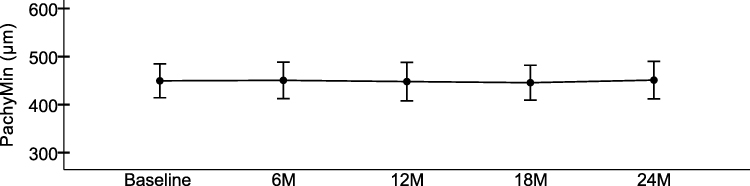 |
Figure 5 Minimum pachymetry (PachyMin) in micrometres (µm) compared with baseline at 6, 12, 18 and 24 months after transepithelial accelerated CXL. |
Topographic Indices
During the follow-up, no significant changes were found in the topographic indices at 12 months (ISV: p = 0.395; IVA: p = 0.208; IHD: p = 0.368; KI: p = 0.851; D-index: p = 0.572) and at 24 months (ISV: p = 0.442; IVA: p = 0.397; IHD: p = 0.484; KI: p = 0.877; D-index: p = 0.892).
Progression
Table 3 shows the progression of patients at 12 and 24 months of follow-up. According to the studied progression parameters, there was an increase ≥ 1D of ∆Kmax in 22.2% (n = 4) and 11.1% (n = 1) of eyes at 12 and 24 months, respectively. An increase ≥ 1D of corneal astigmatism (K2-K1) was observed in 5.6% (n = 1) and 11.1% (n = 1) eyes at 12 and 24 months, respectively. A decrease ≥ 2% in thinnest pachymetry was recorded in 27.8% (n = 5) and 33.3% (n = 3) of eyes at 12 and 24 months, respectively. An increase ≥ 0.42 in D-index was recorded in 44.4% (n = 8) and 22.2% (n = 2) of eyes at 12 and 24 months, respectively.
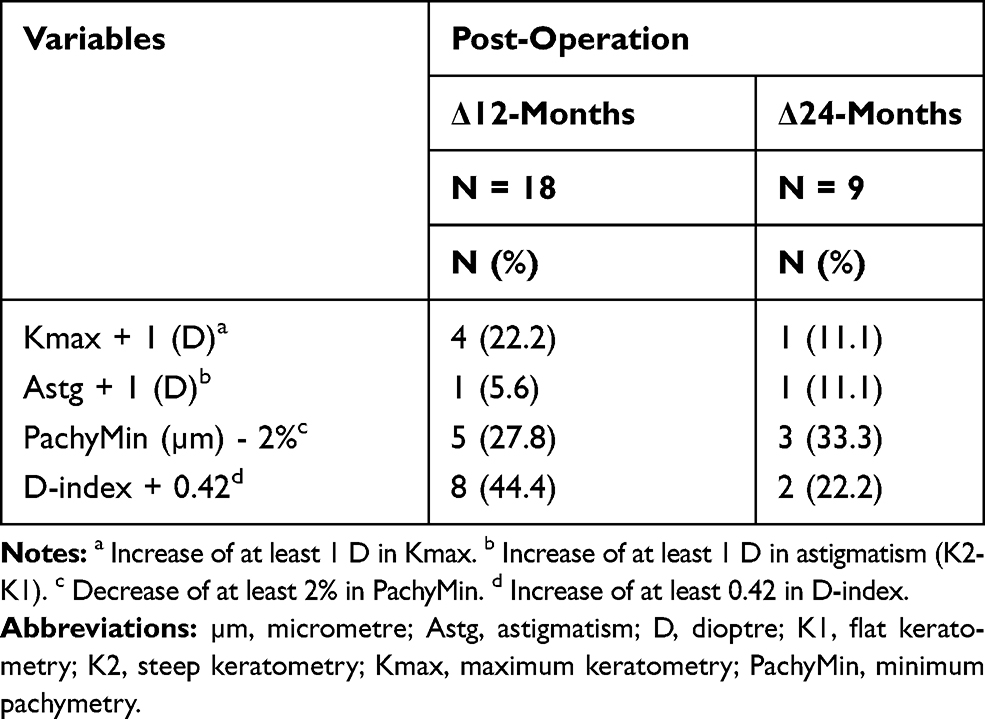 |
Table 3 Evaluation of Parameters Used to Determine Progression of Ectatic Disease |
The statistical analysed in comparing the group that had progression and the group that had no progression in the Kmax, thinnest pachymetry and D-index are summarized in Table 4. The eyes which had progression using Kmax and D-index had no statistically significant differences in the baseline parameters from those which did not have progression.
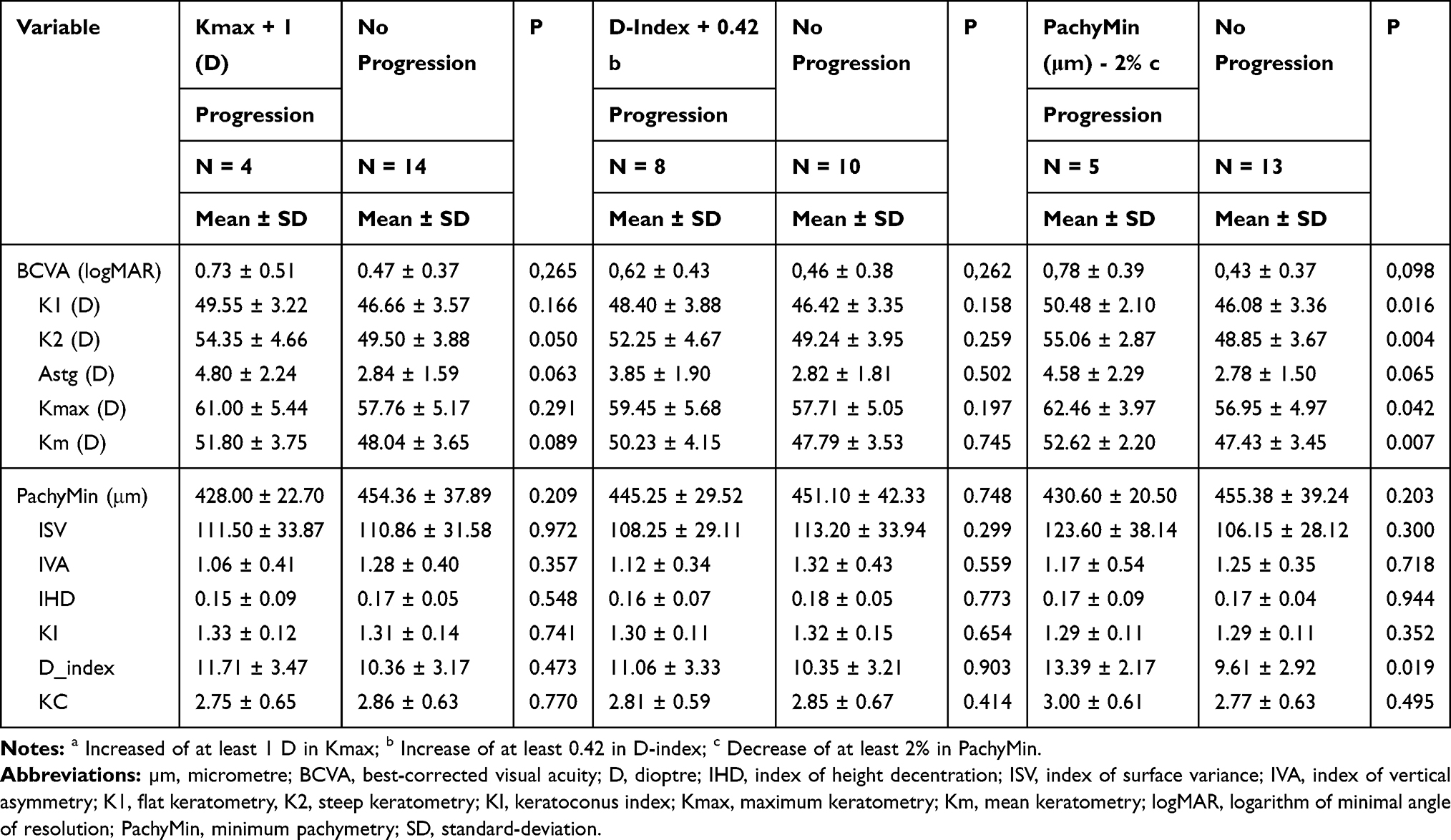 |
Table 4 Mean Changes in Visual, Corneal Tomographic, Topographic and Pachymetric Baseline Parameters Between the Group That Had Progression and the Group That Had No Progression in the Kmax, D-Index and Thinnest Pachymetry |
From the analysed comparative in the thinnest pachymetry, the group which had a decrease ≥ 2% in thinnest pachymetry had higher Kmax, Kmean and D-index values at the baseline in comparison to the group that does not have progression, and this difference was statistically significant in these variables (p = 0.042, p = 0.007; p = 0.019, respectively).
Discussion
Keratoconus is a multifactorial disease, in which several biochemical, physical and genetic factors contribute to the development and progression.2,5
From the several treatment strategies, CXL aims to stop or slow down keratoconus progression.6 Since the C-CXL was first described by Wollensack et al,11 many others modifications have been made to the initial protocol in order to avoid some of its disadvantages.6 The trans-epithelial method had been reported in several studies for its safety and efficacy.8,20,21 This technique is described as pain free, with faster visual recovery and decreased risk of postoperative infection. On the other hand, the epithelium acts as an effective barrier to the penetration of riboflavin. Consequently, chemical enhancers (such as benzalkonium chloride and EDTA) are required to facilitate the passage of riboflavin into the stroma where crosslinking occurs. Moreover, the accelerated protocols were introduced to shorten the surgical time.7,17-21 Although the accelerated protocols theoretic is based on the Bunsen-Roscoe law, it does not take into consideration the effect on the biological tissues. Oxygen is required for crosslinking formation and is more quickly depleted at the higher irradiance required by ACXL procedure. This factor and the intact epithelium could reduce the treatment effect and thus the effectiveness of the crosslinking procedure.
There is a growing evidence of the efficacy and safety of combining the trans-epithelial and accelerated protocols.15,22-29 In the present study, we evaluated the efficacy of TE-ACXL with a specific accelerated protocol (6 mW/cm2 of UVA for 15 minutes); there is scarce published evidence.21,23 Madeira et al had recently concluded that both TE-ACXL (6 mWcm2 for 15 minutes) and C-CXL were similarly effective.23
The current study does not find a significant difference in the visual acuity, as expected, since CXL is a treatment that aims at stopping disease progression and typically has a poorly marked effect on cornea shape. This is in agreement with the study done by Waszczykowska et al (accelerated CXL 6 mW/cm2 for 15 minutes), who report no significant improvement in visual acuity.21 However, the outcomes of previous studies that have investigated trans-epithelial CXL are conflicting, since a mean BCVA remained stable in some studies26,30 and a mean BCVA improved in others.28 These inconsistent outcomes may result from different methodologies used with CXL.
Regarding the keratometry variables, no significant differences were observed between baseline and 12-month or 24-month postoperative at ΔKmax, ΔAstigmatism and ΔPachyMin in our study. These results are consistent with other outcomes using the same protocol (6 mW/cm2 for 15 minutes)21 and others (30 mW/cm2 for 3 minutes;17 45 mW/cm2 for 2 minutes and 40 seconds26).
In this work, we also recorded the pachymetry at the thinnest point, and there were no statistically significant differences between baseline and 12 or 24 months after the procedure. Previous studies have disagreeing results regarding pachymetric outcomes. Zhang et al have described no significant changes after 12 months follow-up after TE-ACXL,29 whereas Akbar et al have demonstrated a significant reduction at 1-year follow-up after TE-ACXL.
Other less studied variables were analysed and there was also no significant change between ISV, IVA, IHD, D-index or KI at baseline and 12 or 24 months after surgery. Thus, the absence of significant difference in BCVA, corneal keratometry, pachymetric and topographic indices indicates that eyes remained stable during the follow-up period.
Several methods have been described in the literature to evaluate progression in keratoconus, despite the absence of a consistent definition and none of them were validated.31 To assess progression were used the following parameters were used: an increase of 1.00 D or more in Kmax, an increase of 1,00 D or more in corneal astigmatism (K2-K1), a decrease of 2% or more in thinnest pachymetry and an increase of 0.42 or more in D-index.32,33
When we analysed the increase ≥ 1,00 D in Kmax, we found that about 22.2% to 11.1% of eyes had progressed at 12 months and 24 months after TE-ACXL. This rate of progression is consistent with published evidence. Huang et al described that 28% of eyes showed progression with TE-ACXL (45mW/cm2 for 5 minutes and 20 seconds).27 Furthermore, Tian et al concluded that Kmax increased in 33% of eyes from progressive keratoconus patients who also underwent TE-ACXL (45mW/cm2 for 5 minutes and 20 seconds).24
Although Kmax is the most commonly used parameter to detect or document ectatic progression, it fails to reflect the degree of ectasia, ignoring the contribution of the posterior cornea to progression, since it represents the steepest anterior corneal curvature taken from a small area. Disease progression can occur with no change in Kmax, because early ectatic change is typically seen on the posterior corneal surface prior to anterior changes.31 Kanellopoulos et al concluded that ISV and IHD may be the most sensitive and specific criteria in the diagnosis and progression of keratoconus.32 Shajari et al in recently published work point out that D-index is the best pointer of keratoconus progression, since it is a multimetric combination parameter composed of pachymetric, anterior and posterior elevation parameters.33 In the current study, there was no significant change between ISV, IVA, IHD, D-index or KI at baseline and 12 or 24 months after surgery. Despite no significant differences, we found that there were still 44.4% and 22.2% of eyes in progression at 12 and 24 months after surgery, respectively, using a 0.42 cut-off of D-index. These higher percentages of progression keratoconus may be due to the fact that D-index has higher sensibility than Kmax.34
When we explore the subgroup of patients who did and did not have progression at 12 months follow-up, the eyes which had a decrease of 2% or more in thinnest pachymetry had higher Kmax, Kmean and D-index values at the baseline in comparison to the group that did not have the progression, and this difference was statistically significant in these variables. This could indicate that in more evolved keratoconus the TE-ACXL could be less effective, due to greater stromal degeneration, biomechanical instability and fewer intact corneal collagen fibrils.35 These patients may require additional and stronger treatment to stop keratoconus progression.
Overall, the patients are stable, which is shown by the almost null differences in Keratometry values and Topographic Indexes after 12 and 24 months of follow-up.
Regarding the study limitations, major drawbacks are inherent to its retrospective nature, the relatively low sample size, and the different time of follow-up limits the analysis of long-term stability, owing to the nonlinear trend of disease progression.
Although some patients maintain disease progression, TE-ACXL seems to be a safe and effective treatment for keratoconus over the 2-year follow-up period. Further studies with longer follow-up periods and larger patient cohorts are recommended.
Abbreviations
BCVA, Best-corrected visual acuity; CXL, Crosslinking; C-CXL, Conventional crosslinking; LogMAR, logarithm of minimal angle of resolution; IHD, Index of height decentration; ISV, Index of surface variance; IVA, Index of vertical asymmetry; K1, Flat Keratometry; K2, Steep Keratometry; KC, Keratoconus classification; Kmax, Maximum keratometry; Km, Mean keratometry; SD, Standard-deviation; TE-ACXL, Trans-epithelial accelerated corneal collagen crosslinking; UVA, Ultraviolet A.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Godefrooij DA, de Wit GA, Uiterwaal CS, et al. Age-specific incidence and prevalence of keratoconus: a nationwide registration study. Am J Ophthalmol. 2017;175:169–172. doi:10.1016/j.ajo.2016.12.015
2. Mas Tur V, MacGregor C, Jayaswal R, et al. A review of keratoconus: diagnosis, pathophysiology, and genetics. Surv Ophthalmol. 2017;62:770–783. doi:10.1016/j.survophthal.2017.06.009
3. Galvis V, Sherwin T, Tello A, et al. Keratoconus: an inflammatory disorder? Eye (Lond). 2015;29:843–859. doi:10.1038/eye.2015.63
4. Sharma N, Rao K, Maharana PK, et al. Ocular allergy and keratoconus. Indian J Ophthalmol. 2013;61:407–409. doi:10.4103/0301-4738.116063
5. Andreanos KD, Hashemi K, Petrelli M, et al. Keratoconus treatment algorithm. Ophthalmol Ther. 2017;6:245–262. doi:10.1007/s40123-017-0099-1
6. Lim L, Lim EWL. A. Review of corneal collagen cross-linking - current trends in practice applications. Open Ophthalmol J. 2018;12:181–213. doi:10.2174/1874364101812010181
7. Medeiros CS, Giacomin NT, Bueno RL, et al. Accelerated corneal collagen crosslinking: technique, efficacy, safety, and applications. J Cataract Refract Surg. 2016;42:1826–1835. doi:10.1016/j.jcrs.2016.11.028
8. Heikal MA, Soliman TT, Fayed A, et al. Efficacy of transepithelial corneal collagen crosslinking for keratoconus: 12-month follow-up. Clin Ophthalmol. 2017;11:767–771. doi:10.2147/OPTH.S129037
9. Hirji N, Sykakis E, Lam FC, et al. Corneal collagen crosslinking for keratoconus or corneal ectasia without epithelial debridement. Eye (Lond). 2015;29:764–768. doi:10.1038/eye.2015.23
10. O’Brart DPS, O’Brart NAL, Aldahlawi NH, et al. Author response: the role of riboflavin concentration and oxygen in the efficacy and depth of corneal crosslinking. Invest Ophthalmol Vis Sci. 2018;59:4451–4452. doi:10.1167/iovs.18-24795
11. Wollensak G, Spoerl E, Seiler T. Riboflavin/ultraviolet-a-induced collagen crosslinking for the treatment of keratoconus. Am J Ophthalmol. 2003;135:620–627. doi:10.1016/S0002-9394(02)02220-1
12. Soeters N, Wisse RP, et al. Transepithelial versus epithelium-off corneal cross-linking for the treatment of progressive keratoconus: a randomized controlled trial. Am J Ophthalmol. 2015;159(5):821–8.e3. doi:10.1016/j.ajo.2015.02.005
13. Chow SSW, Chan TCY, Wong IYH, et al. Early epithelial complications of accelerated trans-epithelial corneal crosslinking in treatment of keratoconus: a case series. Int Ophthalmol. 2018;38(6):2635–2638. doi:10.1007/s10792-017-0734-9
14. Ng AL, Chan TC, Lai JS, Cheng AC. Comparison of the central and peripheral corneal stromal demarcation line depth in conventional versus accelerated collagen cross-linking. Cornea. 2015;34(11):1432–1436. doi:10.1097/ICO.0000000000000626
15. Ameen SS, Mehboob MA, Ali K. Efficacy and safety of transepithelial collagen cross linking for progressive keratoconus. Pak J Med Sci. 2016;32:1111–1115. doi:10.12669/pjms.325.10922
16. Wen D, Song B, Li Q, et al. Comparison of epithelium-off versus transepithelial corneal collagen cross-linking for keratoconus: a systematic review and meta-analysis. Cornea. 2018;37:1018–1024. doi:10.1097/ICO.0000000000001632
17. Tomita M, Mita M, Huseynova T. Accelerated versus conventional corneal collagen crosslinking. J Cataract Refract Surg. 2014;40:1013–1020. doi:10.1016/j.jcrs.2013.12.012
18. Males JJ, Viswanathan D. Comparative study of long-term outcomes of accelerated and conventional collagen crosslinking for progressive keratoconus. Eye (Lond). 2018;32(1):32–38. doi:10.1038/eye.2017.296
19. Kymionis GD, Kontadakis GA, Hashemi KK. Accelerated versus conventional corneal crosslinking for refractive instability: an update. Curr Opin Ophthalmol. 2017;28:343–347. doi:10.1097/ICU.0000000000000375
20. Kortuem KU, Vounotrypidis E, Athanasiou A, et al. Differences in corneal clinical findings after standard and accelerated cross-linking in patients with progressive keratoconus. BMC Ophthalmol. 2017;17:222. doi:10.1186/s12886-017-0610-4
21. Waszczykowska A, Jurowski P. Two-year accelerated corneal cross-linking outcome in patients with progressive keratoconus. Biomed Res Int. 2015;2015:325157. doi:10.1155/2015/325157
22. Olivo-Payne A, Serna-Ojeda JC, Hernandez-Bogantes E, et al. Trans-epithelial accelerated corneal cross-linking for keratoconus in children. Int J Ophthalmol. 2017;10:1919–1921. doi:10.18240/ijo.2017.12.20
23. Madeira C, Vasques A, Beato J, et al. Transepithelial accelerated versus conventional corneal collagen crosslinking in patients with keratoconus: a comparative study. Clin Ophthalmol. 2019;13:445–452. doi:10.2147/OPTH.S189183
24. Tian M, Jian W, Sun L, et al. One-year follow-up of accelerated transepithelial corneal collagen cross-linking for progressive pediatric keratoconus. BMC Ophthalmol. 2018;18:75. doi:10.1186/s12886-018-0739-9
25. Akbar B, Intisar-Ul-Haq R, Ishaq M, et al. Transepithelial corneal crosslinking in treatment of progressive keratoconus: 12 months’ clinical results. Pak J Med Sci. 2017;33:570–575. doi:10.12669/pjms.333.11907
26. Kir MB, Turkyilmaz K, Oner V. Transepithelial high-intensity cross-linking for the treatment of progressive keratoconus: 2-year outcomes. Curr Eye Res. 2017;42:28–31. doi:10.3109/02713683.2016.1148742
27. Huang J, Shen Y, Jian W, et al. Two-year topographic and densitometric outcomes of accelerated (45 mW/cm(2)) transepithelial corneal cross-linking for keratoconus: a case-control study. BMC Ophthalmol. 2018;18:337. doi:10.1186/s12886-018-0999-4
28. Sun L, Li M, Zhang X, et al. Transepithelial accelerated corneal collagen cross-linking with higher oxygen availability for keratoconus: 1-year results. Int Ophthalmol. 2017;38:2509–2517. doi:10.1007/s10792-017-0762-5
29. Zhang X, Sun L, Chen Y, et al. One-year outcomes of pachymetry and epithelium thicknesses after accelerated (45 mW/cm(2)) transepithelial corneal collagen cross-linking for keratoconus patients. Sci Rep. 2016;6:32692. doi:10.1038/srep32692
30. Caporossi A, Mazzotta C, Paradiso AL, et al. Transepithelial corneal collagen crosslinking for progressive keratoconus: 24-month clinical results. J Cataract Refract Surg. 2013;39:1157–1163. doi:10.1016/j.jcrs.2013.03.026
31. Duncan JK, Belin MW, Borgstrom M. Assessing progression of keratoconus: novel tomographic determinants. Eye Vis (Lond). 2016;3:6. doi:10.1186/s40662-016-0038-6
32. Kanellopoulos AJ, Asimellis G. Revisiting keratoconus diagnosis and progression classification based on evaluation of corneal asymmetry indices, derived from Scheimpflug imaging in keratoconic and suspect cases. Clin Ophthalmol. 2013;7:1539–1548. doi:10.2147/OPTH.S44741
33. Shajari M, Steinwender G, Herrmann K, et al. Evaluation of keratoconus progression. Br J Ophthalmol. 2018.
34. Muftuoglu O, Ayar O, Hurmeric V, et al. Comparison of multimetric D index with keratometric, pachymetric, and posterior elevation parameters in diagnosing subclinical keratoconus in fellow eyes of asymmetric keratoconus patients. J Cataract Refract Surg. 2015;41:557–565. doi:10.1016/j.jcrs.2014.05.052
35. Bao F, Geraghty B, Wang Q, et al. Consideration of corneal biomechanics in the diagnosis and management of keratoconus: is it important? Eye Vis (Lond). 2016;3:18. doi:10.1186/s40662-016-0048-4
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.