Back to Journals » Journal of Hepatocellular Carcinoma » Volume 11
Transarterial Chemoembolization Plus Camrelizumab and Rivoceranib versus Camrelizumab and Rivoceranib Alone for BCLC Stage C Hepatocellular Carcinoma
Authors Zhou WJ, Huang JT, Lu X, Hu D, Hong X, Wang FA, Lv PH, Zhu XL
Received 3 September 2024
Accepted for publication 14 December 2024
Published 20 December 2024 Volume 2024:11 Pages 2515—2524
DOI https://doi.org/10.2147/JHC.S494520
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David Gerber
Wen-Jie Zhou,1,2,* Jin-Tao Huang,1,* Xin Lu,3,* Di Hu,1 Xin Hong,4 Fu-An Wang,2 Peng-Hua Lv,2 Xiao-Li Zhu1
1Department of Interventional Radiology, the First Affiliated Hospital of Soochow University, Suzhou, People’s Republic of China; 2Department of Interventional Radiology, Northern Jiangsu People’s Hospital, Clinical Medical College of Yangzhou University, Yangzhou, People’s Republic of China; 3Department of Radiology, Xuzhou Central Hospital, Xuzhou, People’s Republic of China; 4Department of Interventional Radiology, Affiliated Hospital 2 of Nantong University, Nantong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiao-Li Zhu, Department of Interventional Radiology, The First Affiliated Hospital of Soochow University, 188 Shizi St, Suzhou, 215006, People’s Republic of China, Email [email protected]
Purpose: Camrelizumab and rivoceranib together provide a new first-line treatment approach for unresectable hepatocellular carcinoma (HCC). Meanwhile, transarterial chemoembolization (TACE) is an effective method for the local control of the HCC. The study compared the clinical benefit and safety between TACE with camrelizumab-rivoceranib and camrelizumab-rivoceranib alone for Barcelona Clinic Liver Cancer (BCLC)-C HCC patients.
Patients and Methods: This multi-center retrospective analysis included continuous BCLC-C HCC patients who received camrelizumab-rivoceranib with TACE and camrelizumab-rivoceranib alone from January 2020 to December 2022. The therapeutic response, progression-free survival (PFS), safety, and overall survival (OS) were compared. The quantitative data were compared via the t-test or Mann–Whitney U-test. Comparison of the categorical data was done by chi-square or Fisher’s exact tests. The comparison of PFS with OS was compared by Log rank test. A Multivariate Cox regression test was utilized to identify risk variables for both PFS and OS.
Results: This analysis comprised 132 BCLC-C HCC patients who received camrelizumab-rivoceranib alone (n = 74) or combined treatment (n = 58). The combined group displayed higher partial response (44.8% vs 21.6%, p = 0.004) and total response (55.2% versus 36.5%, p = 0.032) rates than camrelizumab-rivoceranib alone group. The median PFS (13.5 months vs 10.3 months, p = 0.046) and OS (22.8 months vs 18.4 months, p = 0.041) for the combined group was significantly longer relative to the camrelizumab-rivoceranib alone group. Additional risk factors, excluding the therapy option, were a higher alpha-fetoprotein level and Eastern Cooperative Oncology Group performance status. The incident rates of camrelizumab-rivoceranib-related advents were comparable between combined and camrelizumab-rivoceranib alone groups (46.3% vs 51.4%, p = 0.572). The combined group contained 33 patients (56.9%) who experienced temporary post-embolization symptoms.
Conclusion: For BCLC-C HCC patients, TACE may significantly increase the therapeutic effectiveness of camrelizumab-rivoceranib without increasing the risk of camrelizumab-rivoceranib-related complications.
Keywords: hepatocellular carcinoma, camrelizumab, rivoceranib, TACE, survival
Introduction
Hepatocellular carcinoma (HCC) is both highly prevalent and the primary cause of cancer-linked mortality.1–3 Surgical resection is the optimal therapeutic strategy against HCC, but only approximately 20% of HCC patients can be treated with surgical resection.4,5 Transarterial chemoembolization (TACE) is a successful choice of treatment for those individuals who are unable to get surgical resection.6–8 However, TACE is mainly suitable for the Barcelona Clinic Liver Cancer (BCLC)-B patients.8 At the time of diagnosis, 50 to 70% of patients exhibit BCLC-C HCC and are ineligible for ablation, TACE, transplantation, or curative resection.9,10
For individuals with BCLC-C HCC, systematic therapy is regarded as the initial course of treatment.10 Recently, combined systemic treatment based on tyrosine kinase inhibitors plus immune checkpoint inhibitors has become the most commonly used systematic treatment for HCC.11 Recent studies support the enhanced antitumor efficacy of combined therapies having shown both immunomodulatory effects of tyrosine kinase inhibitor agents on tumor microenvironment and a pro-angiogenic action of some pro-tumor immune cells.1 Camrelizumab, a humanized monoclonal antibody of the programmed death (PD)-1, is used as an immune therapy against HCC and has demonstrated a favorable anti-tumor effect and tolerance in HCC.12 According to a study, patients with HCC showed better survival when they used the highly specific small-molecule tyrosine kinase inhibitor rivoceranib for vascular endothelial growth factor receptor-2.13 Camrelizumab with rivoceranib may be utilized as a novel first-line therapeutic alternative for unresectable HCC individuals, according to the CARSE-310 clinical study.13
Many research studies considered that combined TACE and systematic treatment could exhibit a significantly better prognosis than systematic treatment alone when treating HCC.10,14 Jin et al11 have found that combined TACE and immune checkpoint inhibitors plus anti-vascular endothelial growth factor antibody/tyrosine kinase inhibitors exhibited significantly longer overall survival (OS, 22.6 months vs 15.9 months, p < 0.0001), progression-free survival (PFS, 9.9 months vs 7.4 months, p < 0.0001), and higher objective response rate (47.3% vs 27.9%, p < 0.0001) than immune checkpoint inhibitors plus anti-vascular endothelial growth factor antibody/tyrosine kinase inhibitors alone group. TACE can significantly decrease tumor burden, and when the tumor burden is comparatively low, the efficacy of systematic therapy gets enhanced.10 Whether TACE and camrelizumab-rivoceranib can produce synergistic benefits is still unclear. Furthermore, some researchers considered the systemic treatments are indicated only for HCC patients with Child-Pugh class A patients.1,13 However, some researchers also included the Child-Pugh class B patients for the systemic treatments.11 Therefore, whether the camrelizumab-rivoceranib can be used for both patients with Child-Pugh class A and B is still unclear.
The current study elucidated the clinical benefit and safety in BCLC-C HCC patients associated with the combined use of TACE with camrelizumab-rivoceranib.
Materials and Methods
Study Design
This retrospective, multi-center study conformed to the ethical guidelines of the Declaration of Helsinki and was approved by The First Affiliated Hospital of Soochow University and Northern Jiangsu People’s Hospital’s Ethics Committee. Patient consent to review their medical records was not required by the Ethics Committee because this is a respective study. However, the personal information of patients was strictly protected. From January 2020 to December 2022, consecutive BCLC-C HCC patients received camrelizumab-rivoceranib with or without TACE in our hospitals. The patients were divided into combined group (TACE with camrelizumab-rivoceranib) and camrelizumab-rivoceranib alone group according to their treatment methods. The patients’ baseline data, treatment response rates, survival, and adverse event rates of the 2 groups were collected and compared.
The inclusion conditions were: (a) BCLC-C HCC patients; (b) patients exhibiting Child-Pugh grade A-B; and (c) patients showing Eastern Cooperative Oncology Group (ECOG) performance status (PS) 0–1. The conditions for exclusion were: (a) individuals under the age of 18; (b) patients with concurrent malignant tumors; and (c) patients who underwent previous HCC treatments (molecular and immunological treatments, TACE, ablation, or surgery). The criteria used by the American Association for the Study of Liver Diseases formed the foundation for the HCC diagnosis.15 The variables included in the present research were ECOG PS, hepatitis types, gender, blood test, age, liver function test, magnetic resonance imaging (MRI) and/or computed tomography (CT) findings, and alpha-fetoprotein (AFP) test.
Camrelizumab-Rivoceranib Alone Group
Camrelizumab-rivoceranib was administered exclusively to patients in that group. Patients were orally administered rivoceranib 250 mg once daily. Moreover, every two weeks, 200 mg of camrelizumab was given intravenously. Treatment cycles lasted 28 days or until the toxicity became intolerable or the condition of the patient became worse.
Combined Group
Under fluoroscopic guidance, conventional TACE was performed on all patients, comprising 150 mg of 5-fluorouracil, 10 mg of mitomycin, 50 mg of epirubicin, and 10–20 mL of lipiodol. When enhancement was identified in treated tumors or when the suspicion of new intrahepatic lesions was presented on the contrast-enhanced CT/MRI scan during follow-up, a subsequent TACE procedure was performed. When target lesions continued to progress after three TACE sessions or when liver function deteriorated to Child-Pugh C or ECOG PS ≥ 2, TACE was discontinued.
The time frame criterion regarding the combined therapy was established as the simultaneous treatment of TACE with or up to 60 days before camrelizumab. Moreover, the rivoceranib administration was performed concurrently with TACE or camrelizumab.
Assessments
Tumor response on all follow-up cross-sectional CT/MRI scans was determined based on modified Response Evaluation Criteria in Solid Tumors (mRECIST) criteria. The details of mRECIST are shown in the supplementary Table 1. Treatment response was assessed by 2 independent radiologists with at least 10 years of experience at every participating center. OS was evaluated from the initiation of treatment (first cycle) to the most recent follow-up or death, whereas PFS was determined from the initiation of treatment (first cycle) until the progression of the disease, death, or the most recent follow-up. The treatment-related safety was estimated throughout the follow-up period. The severity of the treatment-related adverse events were assessed via the National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE; v 5.0).16
After receiving therapy, the participants were followed up at specific time points (1, 3, and 6 months). Afterward, the individuals were followed up every 6 months until death or the study’s conclusion (December 2023). The follow-up contents included contrast-enhanced CT/MRI, AFP test, and liver function test.
OS was the primary endpoint, while treatment safety, response to therapy, and PFS were the study’s secondary endpoints.
Statistical Analyses
All statistical data was analyzed on SPSS (version 16.0; SPSS, Inc., IL, USA). The quantitative data were presented with the mean with standard deviation (SD) if the data were normally distributed, or median if the data were not normally distributed. The data presented with mean with SD were compared via the t-test and the data presented with median were compared via the Mann–Whitney U-test. Comparison of the categorical data was done by chi-square (χ2) or Fisher’s exact tests. The comparison of PFS with OS was conducted using Kaplan-Meier curves and the Log rank test. A Multivariate Cox regression test was utilized to identify risk variables for both PFS and OS. The results having a p < 0.05 were deemed significant.
Results
Patients
This research comprised 132 BCLC-C HCC patients who received camrelizumab-rivoceranib alone (n = 74) or combined treatment (n = 58) during the study period. Table 1 displays the 132 patients’ baseline data. Between the two groups, the remaining variables were compared except for age, tumor diameter and count, and creatinine level.
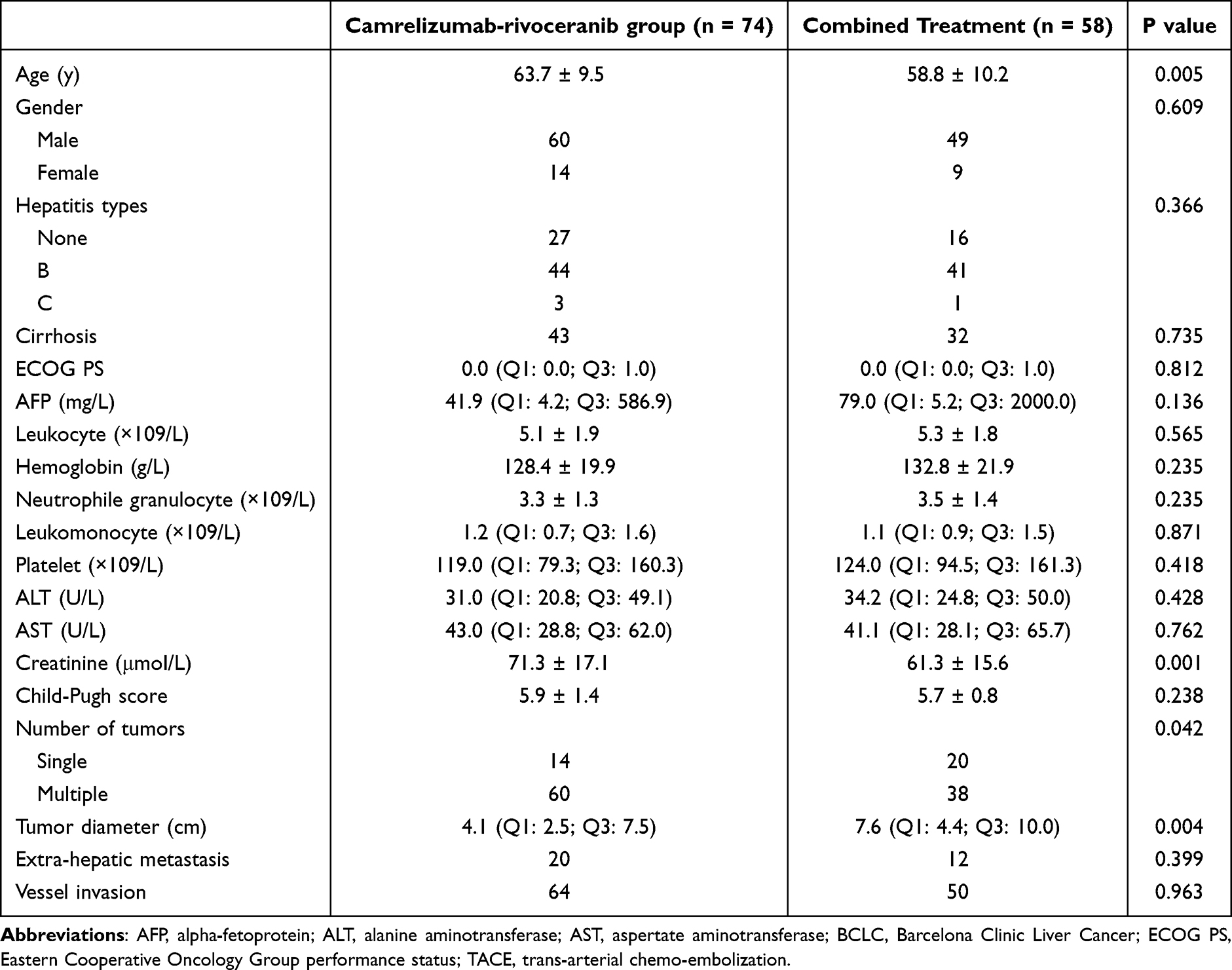 |
Table 1 Baseline Data of the Included Patients |
Response to Treatment
The response to therapy data is presented in Table 2. In comparison to the group treated with camrelizumab-rivoceranib alone, the combined group displayed a significantly greater partial response rate (44.8% vs 21.6%, p = 0.004) and total response rate (55.2% and 36.5%, p = 0.032). The complete response rate (10.4% vs 14.9%, p = 0.442) and progression disease rate (0.0% vs 5.4%, p = 0.130) were comparable between the 2 groups.
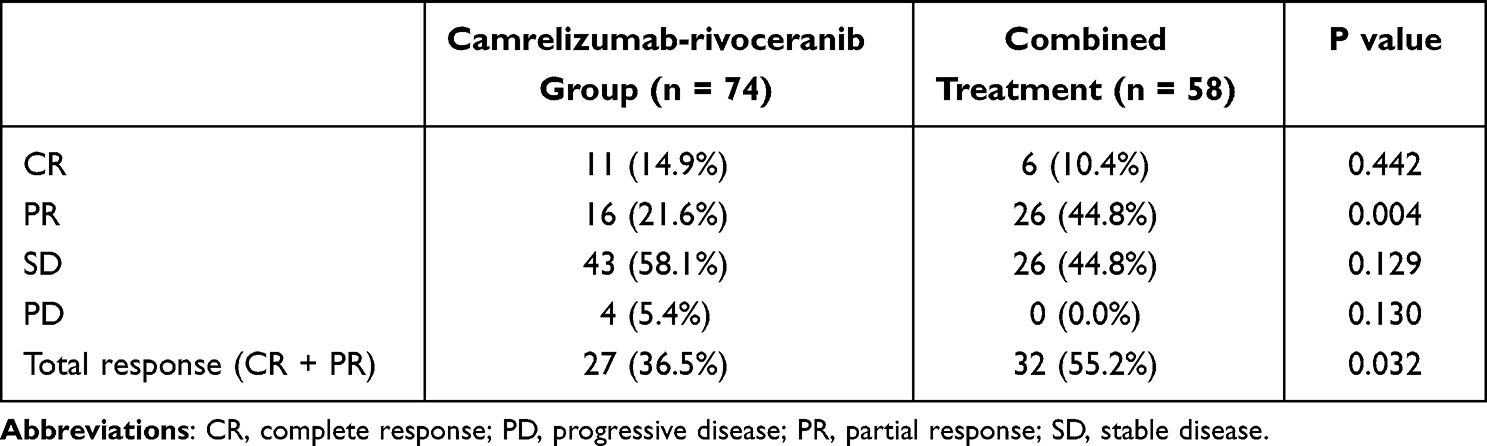 |
Table 2 Treatment Response Between 2 Groups |
Survival
For every patient, 13.0 months was the median follow-up period. In comparison to the camrelizumab-rivoceranib alone group, the median PFS of the combined group was significantly longer (13.5 months vs 10.3 months, p = 0.046). The 1- and 2-year PFS rates in the combined group were 50.1% and 27.4%, respectively (Figure 1). Moreover, in the camrelizumab-rivoceranib alone group, the PFS rates were 37.2% at 1 year and 7.6% at 2 year (Figure 1). Following the multivariate Cox regression analysis, the risk factors associated with shorter PFS were an ECOG PS of 1 (p = 0.010), elevated AFP level (p = 0.012), and the use of camrelizumab-rivoceranib alone (p = 0.035). Table 3 displays details of the analyses.
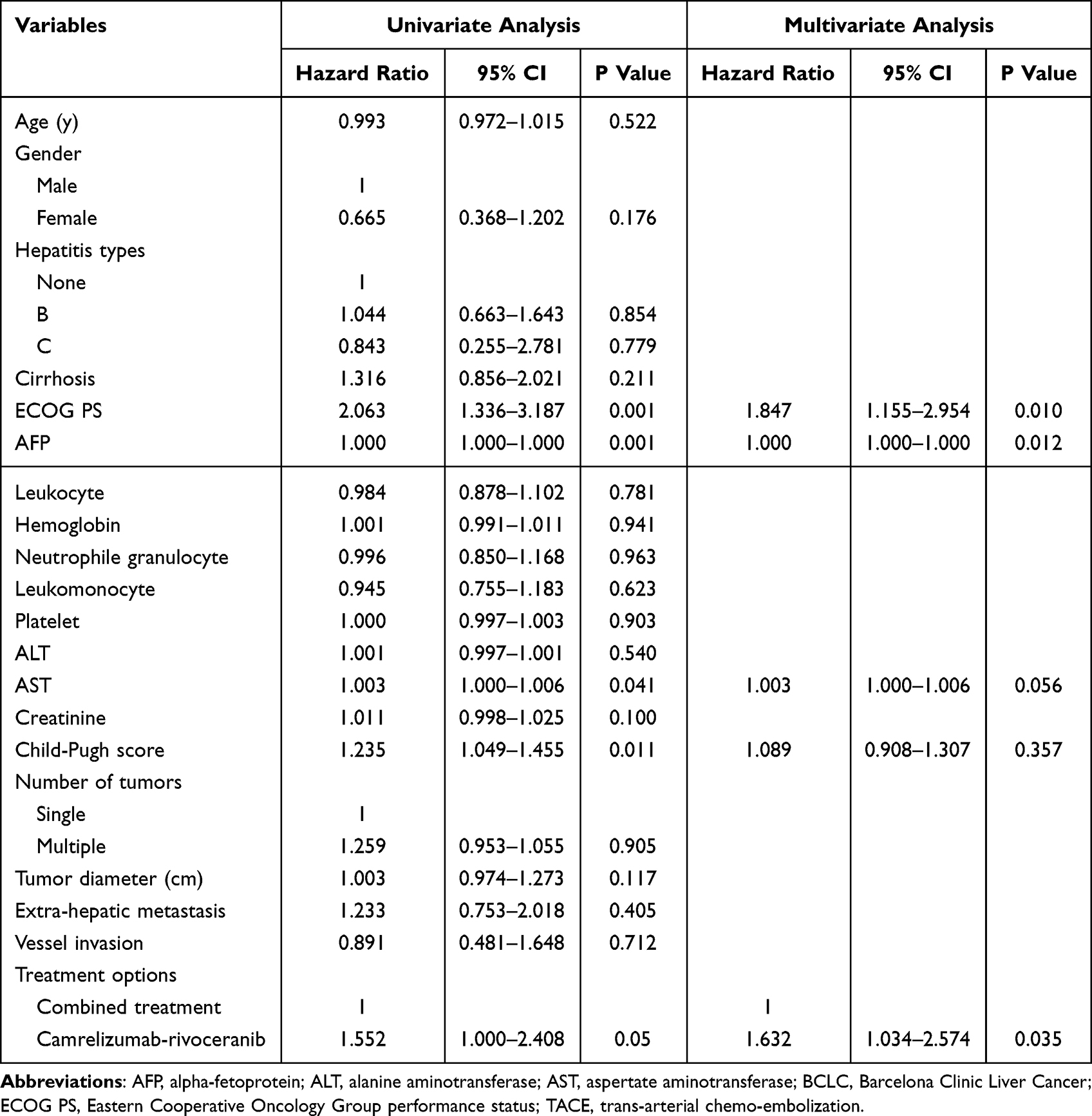 |
Table 3 Predictors of Progression-Free Survival |
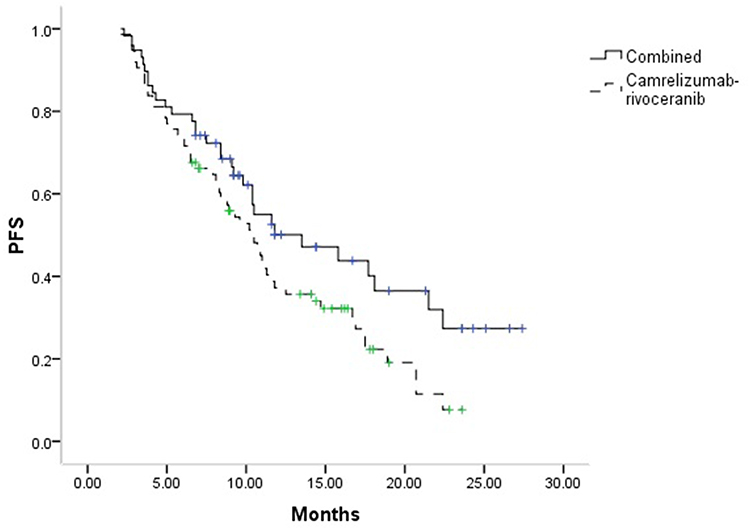 |
Figure 1 The comparison of PFS between 2 groups. |
During the follow-up until the study’s conclusion in December 2023, sixty-seven patients died. Compared to the camrelizumab-rivoceranib alone group, the median OS of the combined group was significantly longer (22.8 months vs 18.4 months, p = 0.041). In the combined group, the OS rates were 74.8% and 45.0% at 1 and 2 years, respectively (Figure 2). The group that received camrelizumab-rivoceranib only had OS rates of 59.2% at 1 year and 35.8% at 2 years, as shown in Figure 2. After performing the multivariate Cox regression analysis, the risk factors of shorter PFS were ECOG PS of 1 (p = 0.001), higher AFP level (p = 0.004), and camrelizumab-rivoceranib alone (p = 0.020). Table 4 provides a comprehensive description of the analyses.
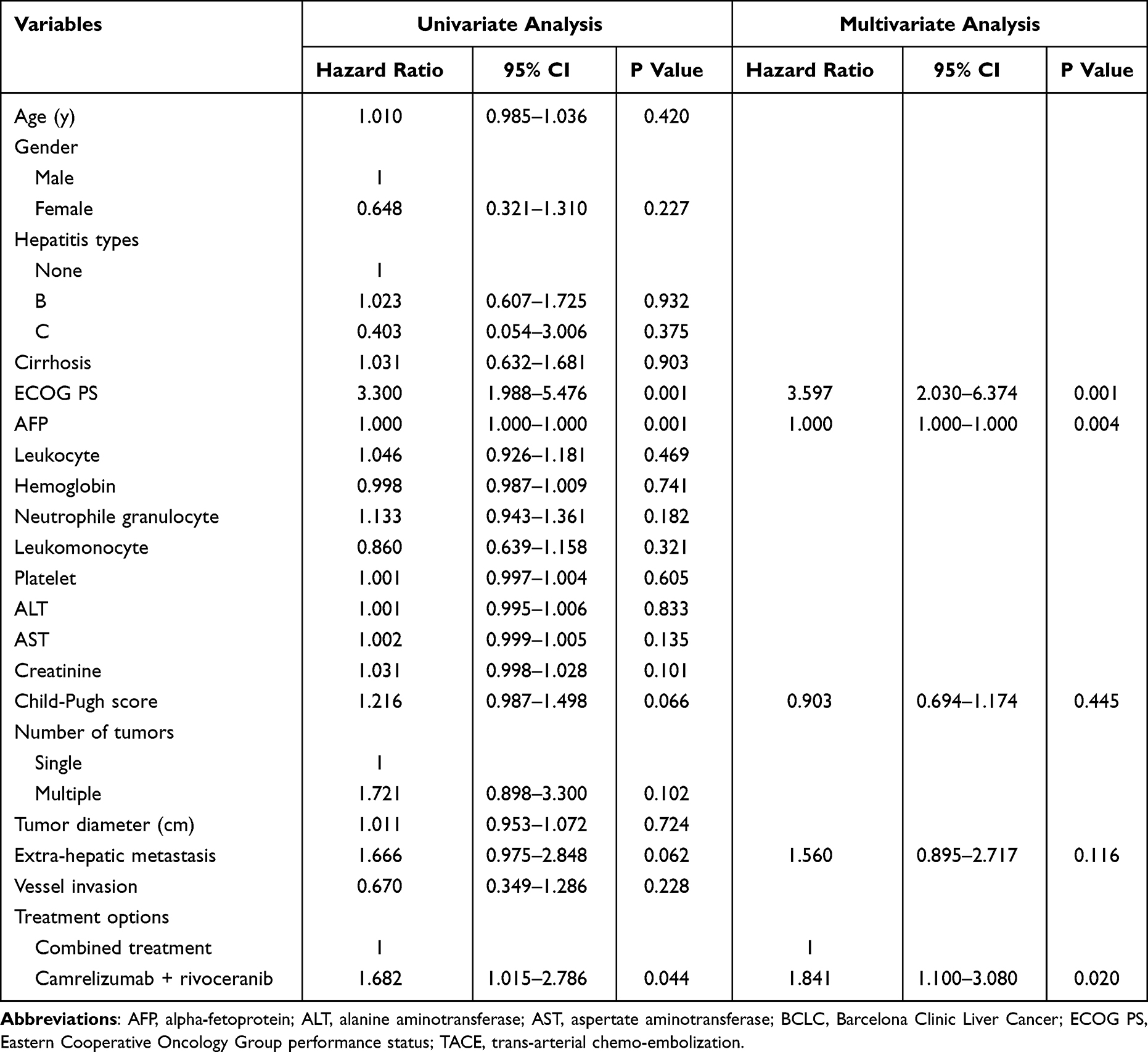 |
Table 4 Predictors of Overall Survival |
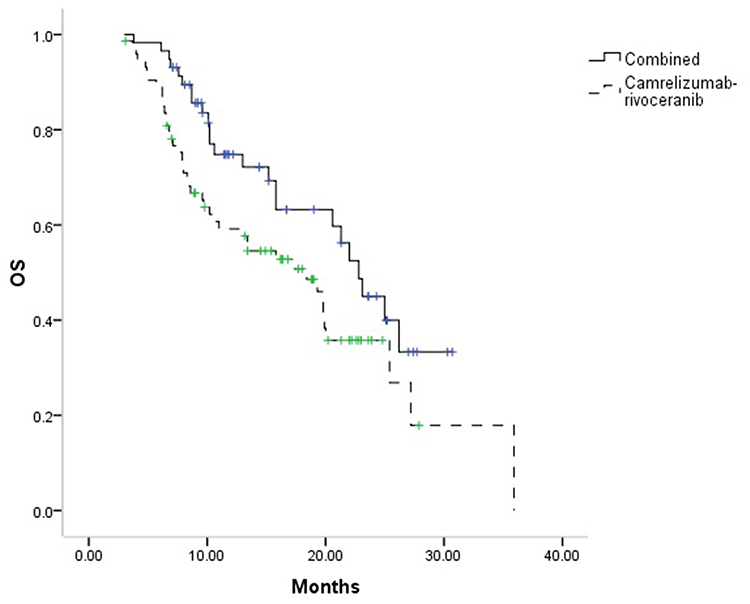 |
Figure 2 The comparison of OS between 2 groups. |
Treatment Safety
The combined group contained 33 patients (56.9%) who experienced temporary post-embolization symptoms, including abdominal pain, fever, and vomiting. These symptoms were successfully managed by symptomatic treatment.
In the combined and camrelizumab-rivoceranib alone groups, the number of patients experiencing adverse events due to the camrelizumab-rivoceranib treatment was 25 (46.3%) and 38 (51.4%), respectively (p = 0.572). Hypertension, palmar-plantar erythrodysaesthesia syndrome, and impaired liver function were the most frequent adverse effects. Grade 4 or 5 adverse events were reported by 5 (8.6%) and 7 (9.5%) of the patients in the combined and camrelizumab-rivoceranib alone groups, respectively, and these patients discontinued the use of medication.
Discussion
In treating BCLC-C HCC, the current study examined the clinical effectiveness and safety of camrelizumab-rivoceranib with and without TACE. Treatment response and survival duration were used to evaluate clinical efficacy, while adverse event reporting was used to determine treatment safety.
Currently, immune checkpoint inhibitors, tyrosine kinase inhibitors, and anti-vascular endothelial growth factor antibodies are thought to be the first-line treatments for advanced HCC.11,13 For unresectable HCC, sorafenib and lenvatinib were regarded as the standard first-line treatments in the last few years.13 The clinical trial of CARES-310 has demonstrated that while treating unresectable HCC, the combined therapy of camrelizumab and rivoceranib exhibited significantly longer PFS (5.6 months vs 3.7 months) and OS (22.1 months vs 15.2 months) compared to sorafenib.13
However, the function of local treatment still holds significant importance and cannot be ignored.11,17 In this study, combined treatment was significantly associated with higher partial and total response rates than camrelizumab-rivoceranib alone. TACE regulates HCC by obstructing the lesions’ feeding arteries, which results in ischemia and hypoxia.18–20 TACE has the potential to increase the expression of PD-1/PD-L1 and cause tumor cell death by releasing proinflammatory cytokines, VEGF, HIF-1α, and tumoral antigens.21 Similarly, Peng et al10 found that the combined treatment group (lenvatinib and TACE) showed significantly higher total response (54.1% vs 25.0%, p < 0.001) and disease control (94.1% vs 73.2%, p < 0.001) rates than lenvatinib only group for treating HCC.
The combination therapy may result in significantly extended OS and PFS durations compared to the use of camrelizumab-rivoceranib alone, highlighting the favorable long-term prognosis of this method in managing the disease. These results may be attributed to the local control effect of TACE. Furthermore, Jin et al17 also considered that immunosuppressive “cold tumors” can become immunosupportive “hot tumors” through TACE, which may improve immune checkpoint inhibitor responsiveness. Cox regression analyses demonstrated that camrelizumab-rivoceranib alone was associated with shorter OS and PFS.
Furthermore, greater AFP level and ECOG PS were also correlated with shorter OS and PFS. The association between worse survival capacity decreased physical condition, and higher HCC malignancy may exist based on these results.
In this study, the combined group had a median PFS of 13.5 months and a median OS of 22.8 months. The results obtained were similar to those observed in prior research using TACE with camrelizumab-rivoceranib for HCC that was unresectable (13.5 and 24.1 months).17 However, the CARES-310 trial showed that camrelizumab-rivoceranib alone exhibited an OS of 22.1 months,13 which was similar to the OS period in the combined group of the present study. These findings may have been attributed to the fact that the CARES-310 trial included BCLC B and C stage patients, while this study only included BCLC C stage patients.
The incidence rates of adverse events associated with camrelizumab-rivoceranib were similar in both groups, with rates of 46.3% and 51.4%, respectively (p = 0.572). This data suggests that TACE does not negatively impact the safety of camrelizumab-rivoceranib therapy. Furthermore, the current research’s incidence rate of adverse events was similar to that of a prior study, including TACE with camrelizumab-rivoceranib for HCC (50.6%).17 Jin et al11 have found that combined group exhibited a higher adverse event rate than systematic treatment alone group (71.4% vs 55.9%). However, the adverse events in the combined group contained both TACE and systematic treatment related adverse events in Jin’s study.11 In the combined group in out study, although TACE led to some post-embolization symptoms, these symptoms were usually temporary and mild. Furthermore, the benefit of the TACE’s effect is more greater than the negative of the post-embolization symptoms. Drug resistance is also a problem when using immunotherapy.22 The mechanism of the resistance may include the etiology of the HCC, tumor intrinsic and extrinsic factors, epithelial-mesenchymal transition, heterogeneity of HCC, antidrug antibodies, and whether a tumor is “hot” vs “cold”.22 If the drug resistance happens, local treatments can be the supplementary treatments for HCC.
This study has some limitations. Firstly, this study’s primary limitation is its retrospective nature. Some variables were not comparable between the 2 groups, including the number of tumors, creatinine level, and tumor diameter. These factors could cause a higher risk of selection bias. However, these factors did not show any correlation with PFS and OS. These results might decrease the possibility of bias. Second, even though these patients were from various centers, there may have been additional bias introduced due to differences in the treatment experiences at each facility. Thirdly, the sample size was small, and further large-scale randomized controlled trials are necessary for better conclusions.
Conclusion
In summary, when compared to the use of camrelizumab-rivoceranib alone, the combination of camrelizumab-rivoceranib with TACE may significantly improve the treatment response and survival in BCLC-C HCC patients Furthermore, this combination may not increase additional adverse events related to camrelizumab-rivoceranib. Thus, it may indicate that TACE and camrelizumab-rivoceranib can produce synergistic benefits.
Acknowledgment
This study was funded by the Natural Science Foundation Project of Jiangsu Province (SBK202302221), Clinical Innovation Cross-translation Program of Soochow University, and Clinical Research Program of First Affiliated Hospital of Soochow University (BXLC010).
Disclosure
The authors reported no conflicts of interest in this work.
References
1. Stefanini B, Ielasi L, Chen R, et al. TKIs in combination with immunotherapy for hepatocellular carcinoma. Expert Rev Anticancer Ther. 2023;23(3):279–291. doi:10.1080/14737140.2023.2181162
2. Zhu HD, Li HL, Huang MS, et al. Transarterial chemoembolization with PD-(L)1 inhibitors plus molecular targeted therapies for hepatocellular carcinoma (CHANCE001). Signal Transduct Target Ther. 2023;8(1):58. doi:10.1038/s41392-022-01235-0
3. Wang YB, Zhang W, Bao L, Lu Y, Hong J. Transarterial chemoembolization with insertion of radioactive seeds for hepatocellular carcinoma. Wideochir Inne Tech Maloinwazyjne. 2023;18(4):645–654. doi:10.5114/wiitm.2023.131539
4. Villanueva A. Hepatocellular Carcinoma. N Engl J Med. 2019;380(15):1450–1462. doi:10.1056/NEJMra1713263
5. Forner A, Reig M, Bruix J. Hepatocellular carcinoma. Lancet. 2018;391(10127):1301–1314. doi:10.1016/S0140-6736(18)30010-2
6. Titano J, Noor A, Kim E. Transarterial chemoembolization and radioembolization across Barcelona clinic liver cancer stages. Semin Intervent Radiol. 2017;34(2):109–115. doi:10.1055/s-0037-1602709
7. Raoul JL, Forner A, Bolondi L, Cheung TT, Kloeckner R, de Baere T. Updated use of TACE for hepatocellular carcinoma treatment: how and when to use it based on clinical evidence. Cancer Treat Rev. 2019;72:28–36. doi:10.1016/j.ctrv.2018.11.002
8. Han K, Kim JH. Transarterial chemoembolization in hepatocellular carcinoma treatment: Barcelona clinic liver cancer staging system. World J Gastroenterol. 2015;21(36):10327–10335. doi:10.3748/wjg.v21.i36.10327
9. Reig M, Forner A, Rimola J, et al. BCLC strategy for prognosis prediction and treatment recommendation: the 2022 update. J Hepatol. 2022;76(3):681–693. doi:10.1016/j.jhep.2021.11.018
10. Peng Z, Fan W, Zhu B, et al. Lenvatinib combined with transarterial chemoembolization as first-line treatment for advanced hepatocellular carcinoma: a phase III, randomized clinical trial (LAUNCH). J Clin Oncol. 2023;41(1):117–127. doi:10.1200/JCO.22.00392
11. Jin ZC, Chen JJ, Zhu XL, et al. Immune checkpoint inhibitors and anti-vascular endothelial growth factor antibody/tyrosine kinase inhibitors with or without transarterial chemoembolization as first-line treatment for advanced hepatocellular carcinoma (CHANCE2201): a target trial emulation study. EClinicalMedicine. 2024;72:102622. doi:10.1016/j.eclinm.2024.102622
12. Xu J, Zhang Y, Jia R, et al. Anti-PD-1 antibody SHR-1210 combined with apatinib for advanced hepatocellular carcinoma, gastric, or esophagogastric junction cancer: an open-label, dose escalation and expansion study. Clin Cancer Res. 2019;25(2):515–523. doi:10.1158/1078-0432.CCR-18-2484
13. Qin S, Chan SL, Gu S, et al. Camrelizumab plus rivoceranib versus sorafenib as first-line therapy for unresectable hepatocellular carcinoma (CARES-310): a randomised, open-label, international Phase 3 study. Lancet. 2023;402(10408):1133–1146. doi:10.1016/S0140-6736(23)00961-3
14. Llovet JM, De Baere T, Kulik L, et al. Locoregional therapies in the era of molecular and immune treatments for hepatocellular carcinoma. Nat Rev Gastroenterol Hepatol. 2021;18(5):293–313. doi:10.1038/s41575-020-00395-0
15. Bruix J, Sherman M. American association for the study of liver diseases. management of hepatocellular carcinoma: an update. Hepatology. 2011;53(3):1020–1022. doi:10.1002/hep.24199
16. Freites-Martinez A, Santana N, Arias-Santiago S, Viera A. Using the common terminology criteria for adverse events (CTCAE - Version 5.0) to evaluate the severity of adverse events of anticancer therapies. Actas Dermosifiliogr. 2021;112(1):90–92. doi:10.1016/j.ad.2019.05.009
17. Jin ZC, Zhong BY, Chen JJ, et al. Real-world efficacy and safety of TACE plus camrelizumab and apatinib in patients with HCC (CHANCE2211): a propensity score matching study. Eur Radiol. 2023;33(12):8669–8681. doi:10.1007/s00330-023-09754-2
18. Llovet JM, Real MI, Montaña X, et al. Arterial embolisation or chemoembolisation versus symptomatic treatment in patients with unresectable hepatocellular carcinoma: a randomised controlled trial. Lancet. 2002;359(9319):1734–1739. doi:10.1016/S0140-6736(02)08649-X
19. Lo CM, Ngan H, Tso WK, et al. Randomized controlled trial of transarterial lipiodol chemoembolization for unresectable hepatocellular carcinoma. Hepatology. 2002;35(5):1164–1171. doi:10.1053/jhep.2002.33156
20. Kudo M. Proposal of primary endpoints for TACE combination trials with systemic therapy: lessons learned from 5 negative trials and the positive TACTICS trial. Liver Cancer. 2018;7(3):225–234. doi:10.1159/000492535
21. Montasser A, Beaufrère A, Cauchy F, et al. Transarterial chemoembolisation enhances programmed death-1 and programmed death-ligand 1 expression in hepatocellular carcinoma. Histopathology. 2021;79(1):36–46. doi:10.1111/his.14317
22. Ladd AD, Duarte S, Sahin I, Zarrinpar A. Mechanisms of drug resistance in HCC. Hepatology. 2024;79(4):926–940. doi:10.1097/HEP.0000000000000237
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.