Back to Journals » International Journal of General Medicine » Volume 15
Traditional Chinese Medicine Decoctions Improve Longevity Following Diagnosis with Stage IV Esophageal Squamous Cell Carcinoma: A Retrospective Analysis
Authors Li H, Ma C, Chang S ![]() , Xi Y, Shao S, Chen M, Ren J, Sun M, Dong L
, Xi Y, Shao S, Chen M, Ren J, Sun M, Dong L
Received 28 October 2021
Accepted for publication 11 January 2022
Published 16 February 2022 Volume 2022:15 Pages 1665—1675
DOI https://doi.org/10.2147/IJGM.S346536
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Honglin Li,1,* Chunzheng Ma,1,* Sisi Chang,2 Yutan Xi,2 Shuai Shao,2 Mengli Chen,2 Juan Ren,2 Mingyue Sun,1 Liang Dong1
1Oncology Department, Henan Provincial Hospital of Traditional Chinese Medicine, Zhengzhou, Henan Province, People’s Republic of China; 2Oncology Department, Henan Provincial University of Traditional Chinese Medicine, Zhengzhou, Henan Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Honglin Li, Oncology Department, Henan Provincial Hospital of Traditional Chinese Medicine, No. 6 Dongfeng Road, Zhengzhou, 450002, People’s Republic of China, Email [email protected] Chunzheng Ma, Oncology Department, Henan Provincial Hospital of Traditional Chinese Medicine, No. 6 Dongfeng Road, Zhengzhou, 450002, People’s Republic of China, Email [email protected]
Objective: Traditional Chinese medicine (TCM) is an ancient form of personalized medicine and may improve morbidity and mortality in patients with esophageal cancer. This retrospective study aimed to evaluate the utility of TCM in the treatment of stage IV esophageal squamous cell carcinoma (SCC).
Methods: We collected the medical records of patients with stage IV SCC admitted to Henan Provincial Hospital of Traditional Chinese Medicine and Linzhou Hospital of Traditional Chinese Medicine between July 2017 and June 2020. We used univariate and multivariate analyses to determine if the use of TCM improved patient prognosis. Moreover, cluster analysis was used to classify the patients according to TCM syndrome type and identify the most frequently used combinations of remedies.
Results: After that 402 patients were included in PSM, of which 196 (48.8%) were treated with traditional Chinese medicine. TCM prolonged the survival time of patients with stage IV esophageal SCC (P=0.084), and was an independently associated with prognosis as demonstrated by Cox multivariate regression analysis [risk ratio (RR) =0.543, 95% confidence interval (CI): 0.390– 0.755, P< 0.001]. Association analysis revealed 75 cases (38.26%) had obstruction of phlegm and qi syndrome, 53 cases (27.04%) had phlegm and blood stasis syndrome, 38 cases (19.39%) had yang-qi deficiency syndrome, and 30 cases (15.31%) had heat retention and fluid consumption syndrome.
Conclusion: Treatment with TCM derived therapies may increase the survival time of patients with stage IV esophageal SCC. Since these patients were diagnosed with different TCM syndromes, individualized TCM therapy is essential for improving symptoms and survival.
Keywords: esophageal cancer, survival time, traditional Chinese medicine syndrome type, syndrome differentiation, syndrome treatment
Introduction
Esophageal cancer is a deadly, yet understudied, malignant tumor of the digestive system.1 Its morbidity and mortality rank 8th and 6th in the world respectively, with reported 5-year survival rates between 15–25%.2,3 In particular, Asian countries experience the greatest disease burden from esophageal cancer, with over 75% of cases worldwide arising in this region. China alone accounts for 50% of esophageal cancer cases worldwide, with 188,000 deaths reported in 2015.4–6
Many studies have examined the use of traditional Chinese medicine (TCM) in the treatment of esophageal cancer.7–9 These reports suggest that TCM based therapies may both enhance the efficacy of and reduce side effects from Western treatments, as well as directly induce apoptosis in tumor cells. However, little is known about indications for treatment based on TCM criteria, and there is a lack of available data regarding usage rates and outcomes associated with TCM based therapies among patients with advanced esophageal squamous cell carcinoma (SCC), the most common form of esophageal cancer.
Like the majority of cancers, the standard of care for esophageal cancer is a combination of chemotherapy, radiotherapy, and/ or surgery.10,11 In China, patients are often treated with a comprehensive approach utilizing both conventional and TCM derived therapies.12 The TCM treatment arm relies on the principle of “Bian Zheng Lun Zhi”, or “treatment based on syndrome differentiation”.12 This process involves observing, listening to, and questioning the patient, alongside a basic physical examination, in order to prescribe the best remedy. Correct syndrome differentiation is vital for the efficacy of TCM.
Personalized or precision medicine has existed for centuries in China under the umbrella of TCM. Deciphering meaningful patterns from “treatment based on syndrome differentiation” is the first step in translating this system into a scientific language. Network or cluster analysis is an important tool which can explore the relationship between Chinese herbal formulae and corresponding TCM syndromes and to identify synergy between treatment combinations.13 Under a network framework, one can begin to define the relationship between herbal properties and curative effects with the goal of uncovering the therapeutic principles of TCM.
In this study, we evaluated the medical records of patients with stage IV esophageal SCC who were treated at the Henan Hospital of Traditional Chinese Medicine and Linzhou Hospital of Traditional Chinese Medicine. We report patient outcomes associated with both conventional treatment (chemotherapy, radiotherapy and/or surgery) and TCM based treatment. Moreover, using network analysis, we examine syndrome differentiation and associated herbal remedies prescribed for these patients.
Materials and Methods
Study Design
This retrospective, real-world study was approved by the Ethics Committee of Henan Provincial Hospital of Traditional Chinese Medicine[2019(40)], and informed consent was waived. Patients were divided into a TCM and non-TCM group based on the usage of TCM decoctions. Since this study has no potential harm to the included cases, we applied for exemption from the informed consent process. This study abides by the Helsinki declaration.
Patients
We collected the medical records of inpatients admitted to the Oncology Department of Henan Provincial Hospital of Traditional Chinese Medicine and Linzhou Hospital of Traditional Chinese Medicine from July 2017 to June 2020.
Inclusion criteria: (1) diagnosis of esophageal cancer based on the WHO (2010) definition of esophageal carcinoma; (2) diagnosis with stage IV esophageal SCC confirmed by pathology; (3) patients in the TCM group must have received TCM based treatment for more than 3 months.
Exclusion criteria: (1) patients with more than two kinds of malignant tumors; (2) patients experiencing acute illness; (3) patients participating in other studies.
TCM Syndrome Differentiation and TCM Treatment
Standards of syndrome differentiation and diagnosis are described in “Internal Medicine of Traditional Chinese Medicine”, the “12th Five-Year Plan” national textbook for higher education published by the Chinese Press for Traditional Chinese Medicine in 2012.14 For greater reliability, two doctors (with the title of associate chief physician or higher) assessed each patient for syndrome differentiation and prescribed relevant treatments. Patients were divided into four primary disease categories: (1) phlegm-qi stagnation syndrome, (2) phlegm-blood stasis syndrome, (3) Yang-qi deficiency syndrome, and (4) heat retention and fluid consumption syndrome (sometimes grouped with yin-deficiency). Other syndromes with small sample sizes were attributed to the most relevant primary syndrome.
Evaluation Indicators and Evaluation Methods
We retrieved medical records from the health information system (HIS) of each hospital to obtain each patient’s age, number of concomitant diagnoses, clinical stage and pathological type of esophageal cancer, and TCM syndrome diagnosis. We collected additional information on each patient’s survival status and treatment regimen by telephone and outpatient visits. The deadline for follow-up was June 30, 2020. The study endpoint was death or status at the last follow-up, and data collection was considered complete if the patient died during the study. In this group, survival time was defined as the number of months between the time of diagnosis and the time of death. In patients who survived to the data collection endpoint, the survival time was defined as the number of months between the time of diagnosis and the last follow-up and considered truncated (censored) data. The survival data from missing subjects were treated as truncated data, and the survival time was the number of months between the time of diagnosis and the last follow-up appointment.
Data Processing
The names, classifications, and nature flavor meridians of drugs were all standardized with reference to Pharmacopoeia of the People’s Republic of China (2015)15 and Traditional Chinese medicine.16 We reviewed each TCM in order to capture and group all synonymous TCM treatments that can appear with different names. For example, we recorded “Fried Atractylodes” as “Atractylodes”, “Radix Dipsaci of Sichuan” as “Radix Dipsaci”, and “Radix Astragali preparate” as “Astragalus” and so on. If a single TCM had multiple nature flavor meridians, statistics were made for each meridian. Processing alters properties such as efficacy and toxicity for each treatment, so similar products undergoing different processing procedures are classified as separate drugs in our analysis.
Data Mining
SPSS Modeler 14.1 (SPSS, Chicago, IL, USA) statistical software was used for association analysis of frequently used TCM drugs (prescribed in ≥ 10% of cases) according to different syndrome types. The level of significance was calculated using two indicators, support (s) and confidence (c). We defined the a priori conditions as follows: 10% for support degree, 90% for confidence coefficient, antecedents ≤ 5, and lift ≥ 1. Lift was calculated by dividing the confidence of a rule by the support of the consequent.
Statistical Methods
Categorical variables were expressed as n (%), and the differences between the TCM group and the control group were tested using the chi-square (χ2) test. According to the desired protocol, data such as age are represented as categorical variables. If the P value was greater than 0.05, the difference was not considered statistically significant. A Kaplan-Meier curve was used to evaluate overall survival (OS) in the TCM group and the control group. The Log Rank test was used to calculate the survival difference between the two groups and analyze the factors related to the OS of patients with stage IV esophageal SCC. A Cox regression model was used for multivariate analysis of combinatorial variables. The statistical analysis was performed using SPSS 23.0 (IBM, Armonk, New York, USA) and GraphPad Prism 8.0 (GraphPad Corporation, College Station, CA, USA).
Results
Baseline Characteristics
We collected data from a total of 880 patients with esophageal cancer admitted to the hospital between July 2017 to June 2020. During the case registration process, 28 patients were lost to follow-up, 14 patients refused treatment, 3 patients were older than 90 years old, and 11 patients died of other diseases. Patients were divided into Chinese medicine group and non-Chinese medicine group, and patients with no statistical difference in the distribution of chemotherapy confounding factors between the two groups were screened by 1:1 propensity score matching (PSM). Therefore, a total of 402 cases were included in the study, including 196 patients who were prescribed TCM and 206 patients who were not. The baseline characteristics and clinical characteristics are shown in Table 1.
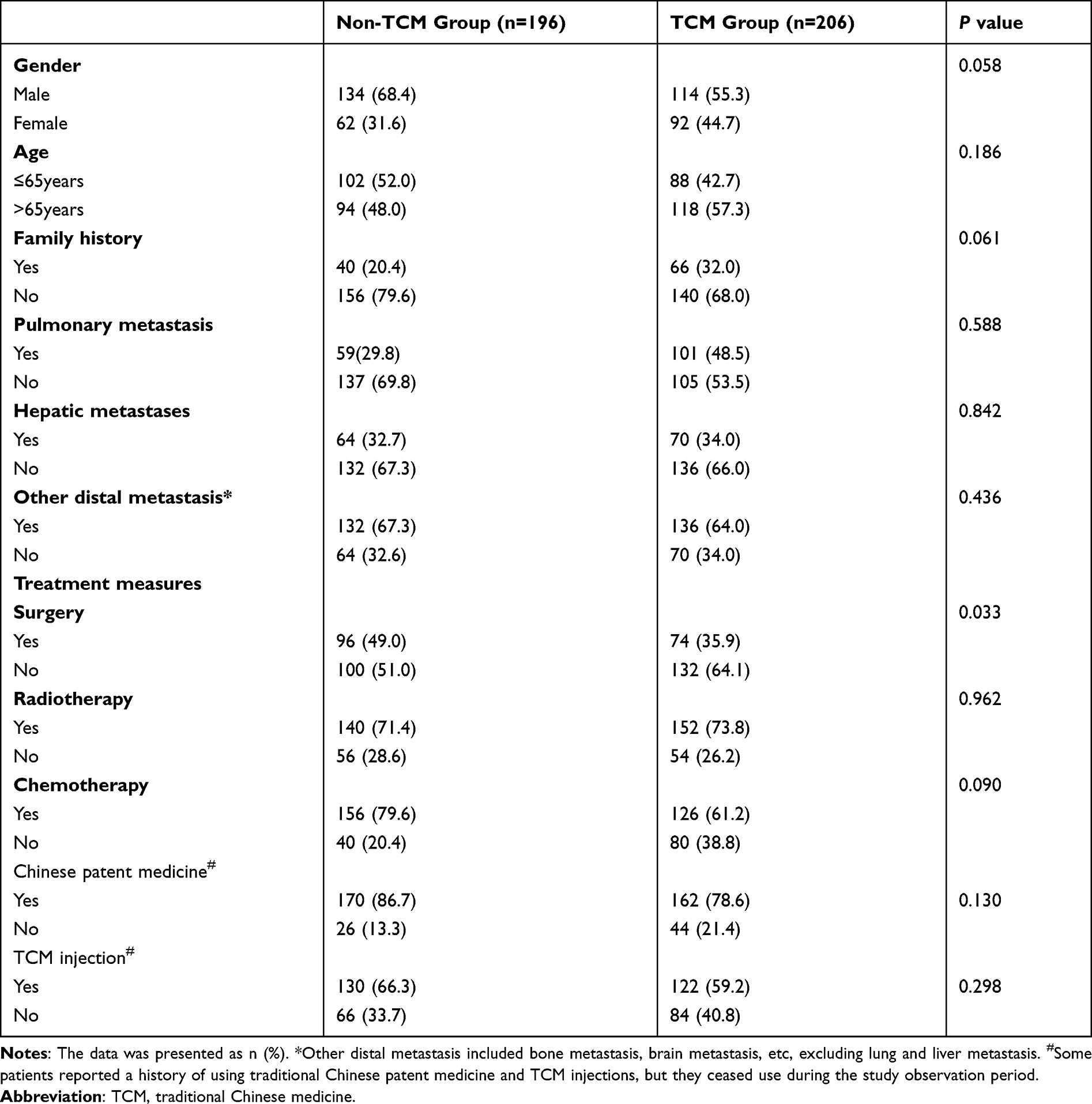 |
Table 1 Baseline Survival Data and Clinical Characteristics of Patients with Stage IV SCC |
Survival Analysis of Patients with Stage IV Esophageal Squamous Cell Carcinoma
Kaplan-Meier survival curves for the two groups of patients are shown in Figure 1. The median survival time of stage IV patients receiving TCM was 16 months, while patients not receiving TCM had a median survival time of only 14 months. Moreover, the survival rates of patients in the TCM group (93.9% at 6 months, 75.5% at 12 months, and 28.2% at 24 months) were higher than those in the non-TCM group (90.2% at 6 months, 62.8% at 12 months, and 24.2% at 24 months) (Log Rank test P=0.084).
 |
Figure 1 Overall survival time of stage IV patients with esophageal cancer. Patients in the non-TCM group are shown in red and patients in the TCM group are shown in blue. Patients in the TCM group show improved survival characteristics (Log Rank test: P=0.084). |
We identified factors that may influence patient survival and prognosis by Log Rank univariate analysis (see Table 2). In addition to TCM (P=0.084), surgery (P<0.001) and radiotherapy (P=0.016) appear to positively impact survival, while liver metastasis (P=0.035) and lung metastasis (P=0.02) negatively impact survival. The variables which did not significantly impact prognosis included gender, age, a family history of cancer, expression of the tumor markers CEA and CA199, treatment with chemotherapy, and the presence other distant metastases (P>0.05).
 |
Table 2 Log-Rank Univariate Analysis of Factors Which May Influence Survival Time Following Diagnosis with Stage IV Esophageal SCC |
Cox multivariate regression analysis shows that TCM (RR=0.543, 95% CI: 0.390–0.755, P<0.001), surgery (RR=0.266, 95% CI: 0.194–0.365, P<0.001), radiotherapy (RR=0.422, 95% CI: 0.299–0.595, P<0.001), and lung metastasis (RR=1.532, 95% CI: 1.121–2.094, P=0.007) were independent factors which positively influenced the overall survival time of patients with stage IV esophageal SCC (Table 3).
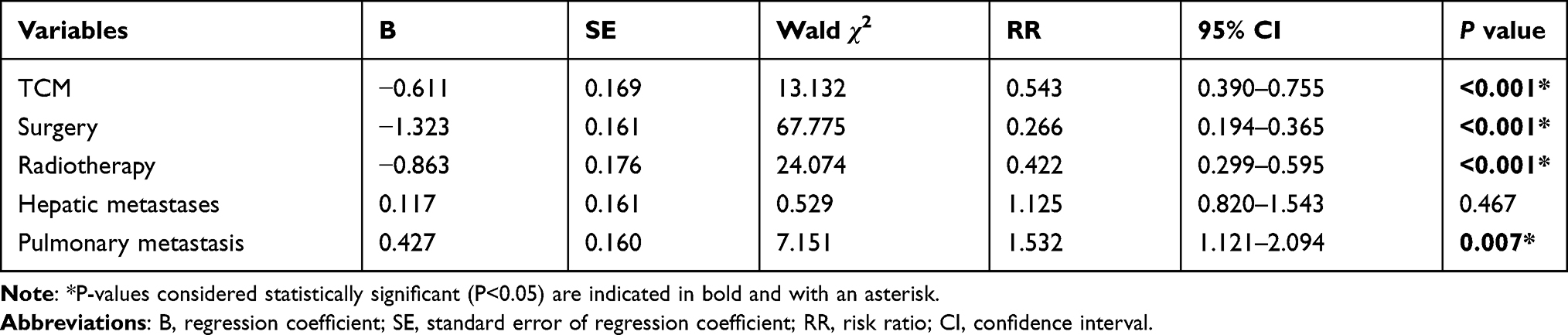 |
Table 3 Cox Multivariate Regression Analysis of Factors Influencing Survival Time Following Diagnosis with Stage IV Esophageal Squamous Cell Carcinoma |
Frequency of TCM Syndrome Types and Treatments
A fourth of all cancer patients admitted to the participating hospitals received a primary diagnosis of esophageal cancer during the study period. At the time of admission, these patients presented with fatigue, poor appetite, pain, and dysphagia. A total of 196 patients had recorded TCM syndromes, among which 75 cases (38.26%) had obstruction of phlegm and qi syndrome, 53 cases (27.04%) had phlegm and blood stasis syndrome, 38 cases (19.39%) had yang-qi deficiency syndrome, and 30 cases (15.31%) had heat retention and fluid consumption syndrome.
TCM practitioners prescribed treatments described in “Chinese Materia Medica”.17 A total of 273 prescriptions were written for 196 patients, using a total of 319 Chinese traditional medicines, of which 77 prescriptions were repeat prescriptions for 77 patients. We counted the frequency of TCM remedies appearing in more than 40 cases (Table 4). We found that Atractylodes macrocephala was the most frequently used drug [155 (56.77%) in 273 prescriptions], followed by Tuckahoe [125 (45.78%)], Codonopsis [117 (42.85%)] and dried tangerine peel [108 (39.56%)]. Doctors most frequently prescribed drugs in the tonifying deficiency category [53 (16.61%)], followed by bronchodilators for relieving phlegm and cough [28 (8.77%)] and Qi-regulating drugs [23 (7.21%)] (Table 5).
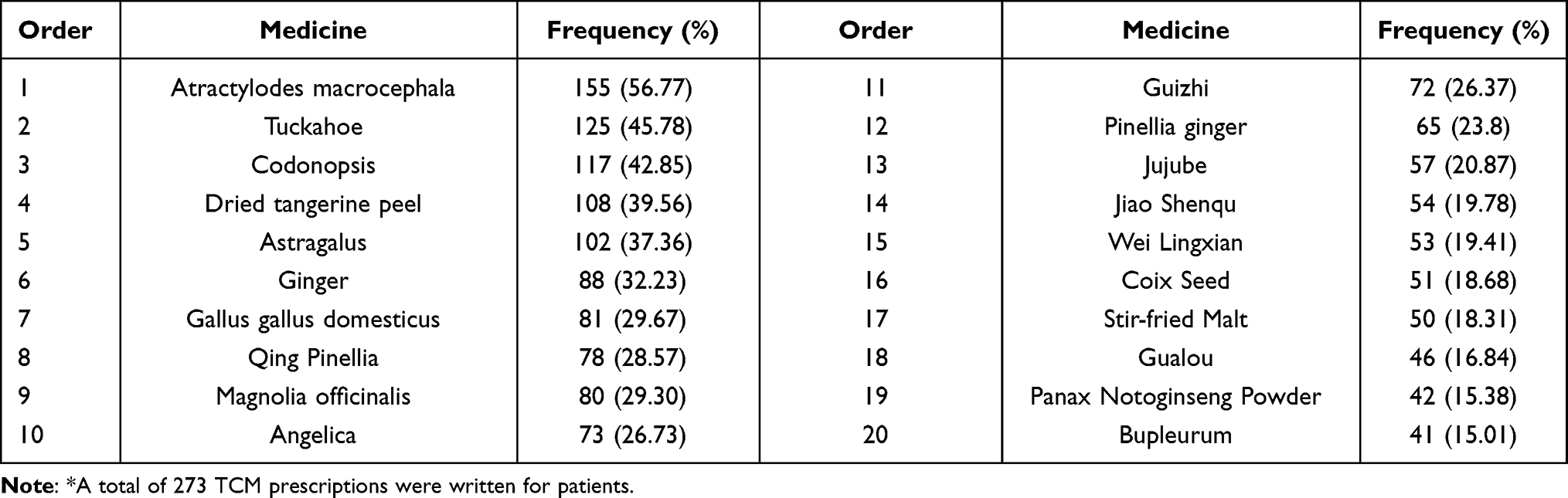 |
Table 4 Prescribing Frequency of the Most Common Chinese Medicines* |
 |
Table 5 Top 8 TCM Treatment Categories* |
Cluster Analysis of TCM Syndrome Differentiation and Medication Combinations
We used association analysis to identify the indications for frequently prescribed drugs (prescribed for more than 35 patients). Association rules are used in data mining to detect relationships between values of categorical variables. A standard association rule is the implication X→Y (s, c), where X (antecedent) and Y (consequent) are frequent items in a transactional database and the intersection of X and Y is non-empty. The level of significance is given by two indicators, support (s) and confidence (c). The measure “support” is the proportion of transactions in the dataset that contain X and Y and the measure “confidence” is the proportion of transactions containing X in which item Y also appears. We include another measure called lift which reflects the correlation between an antecedent and consequent. We present the association rules for commonly prescribed TCM remedies in Table 6.
 |
Table 6 Association Analysis of Frequently Prescribed TCM Therapies for Esophageal Cancer |
According to our cluster analysis, the core drug pairs for patients with Yang-qi deficiency syndrome (synergistic drugs are in parentheses) are agrimony and ginger (red ochre), malt and ginger (caulis spatholobi), radix aucklandiae and poria cocos (caulis spatholobi), and fructus corni (Rehmannia glutinosa) (Table 6). These are prescribed to enrich the blood and strengthen the spleen and stomach. The core drug pairs for patients with phlegm and blood stasis syndrome were centipede and dangshen (whole scorpion), centipede and pinellia (whole scorpion), cattail pollen and pinellia (excrementum pteropi), seed of garden balsam and gecko (air potato yam), and cattail pollen (excrementum pteropi), which are mainly derived from insects and used to promote blood circulation, resolve masses, and eliminate phlegm and qi. Patients with obstruction of phlegm and qi syndrome were prescribed drugs such as medicated leaven (malt and pinella) which also clear qi and dissolve phlegm, promote blood circulation and resolve masses. The core drug pairs for patients with heat retention and fluid consumption syndrome included radix ophiopogonis (radix scrophulariae), radix scrophulariae and radix paeoniae rubra (radix ophiopogonis), aspongopus (bletilla hyacinthina reichb), fructus aurantii immaturus and rheum officinale (peach kernel), and orange peel and cassia twig (amomum cardamomum). These are thought to replenish yin and relieve fever. All the primary drugs for each syndrome type and their prescribing relationships are shown in Figure 2.
 |
Figure 2 Association analysis identifies synergistic drug pairs by syndrome type. Association analysis was used to identify pairs of drugs commonly prescribed for (A) Yang-qi deficiency syndrome, (B) heat retention and fluid consumption syndrome, (C) phlegm and blood stasis syndrome and (D) obstruction of phlegm and qi syndrome. The width of the line between nodes indicates the frequency of co-prescribing. For example, in panel A, we see that, large-headed atractylodes is commonly prescribed with pinella and almost never prescribed with tangerine peel for yang-qi deficiency. |
Discussion
Esophageal cancer is a prevalent malignant tumor in Asian countries, and is primarily caused by exposure to environmental carcinogens.6,18–20 Most cases have few symptoms in early stages, and as such onset is insidious leading to poor treatment options.21–23 Therefore, the objective of this study was to evaluate the use of Traditional Chinese Medicine (TCM) alongside conventional Western therapies such as chemotherapy and radiation. We have shown that the use of TCM decoctions is associated with increased longevity following diagnosis of stage IV esophageal squamous cell carcinoma (SCC). As demonstrated by multivariate Cox analysis, this effect was independent of use with any particular conventional treatment.
Network analysis was used to classify patients with TCM diseases of dysphagia. It is believed diseases of dysphagia arise from liver qi invading the stomach, failure of stomach qi to descend, adverse rising of stomach-qi aggravated local esophageal lesions, and dysfunctions of the liver, spleen and stomach leading to phlegm accumulation and phlegm and blood stasis. This further impairs swallowing, increases phlegm and salivation, and patients were prone to severe choking, salivation, extreme emaciation, and deficiency of vital qi. Therefore, the TCM practitioners’ observation of “deficiency of vital qi” may be a prognostic factor for the survival of patients with esophageal cancer.
In this real-world study (RWS),24 patients with esophageal cancer were taken as the research objects. Most patients were in an advanced stage at diagnosis, with more than 60% experiencing lymph node metastasis and distal metastasis. Therefore, overall patient prognosis was poor. In the treatment of esophageal cancer with TCM, “Bian Zheng Lun Zhi”, or “treatment based on syndrome differentiation”, formed the foundation of patient care.25 We found that patients with yang-qi deficiency syndrome were primarily prescribed drugs which enrich the blood and strengthen the spleen and stomach. Patients with phlegm and blood stasis syndrome or obstruction of phlegm and qi syndrome were prescribed drugs which increase circulation, resolve masses, and clear phlegm and qi. Patients with heat retention and fluid consumption syndrome were given treatments believed to replenish yin, lower body temperature, and relieve fever.
Even in a disease mainly manifested by “real” symptoms, drugs which promote tonification, or improved flow of qi or bodily energy, were widely prescribed to esophageal cancer patients by TCM practitioners (Table 5). These treatments are thought to tonify the spleen, regulate qi, and nourish the blood (encourage the movement of qi and blood throughout the body). This enhances the clearing of phlegm, disperses masses, and promotes circulation. In the treatment of heat retention and fluid consumption syndrome, drugs carrying the properties of yin-nourishing were used, such as radix ophiopogonis and radix scrophulariae, alongside remedies such as rehmannia glutinosa and angelica sinensis which relieve fever with sweet and warm herbs and nourish the blood (Figure 2). Further studies are necessary to elucidate the molecular factors and biological mechanisms underlying the observations of TCM physicians.26–30
This study had some limitations. Clinical evidence patterns are primarily determined by clinical observations and the experience of physicians. Even though standards in medical textbooks guide TCM therapy,14 TCM is difficult to generalize. Since the diagnosis and treatment of diseases in TCM are based on syndrome differentiation, the diversity of clinical syndromes determines the complexity of treatment. For example, we had to group less commonly seen TCM syndromes within our four primary categories based on clinical manifestation. Moreover, as this was a retrospective analysis, we could not obtain all information which may be relevant to patient prognosis such as the degree of tumor differentiation, location and size of the lesions, and the presence of other tumor markers. Due to the limitations of the retrospective design, the findings of this study will be further evaluated in a prospective cohort study or a randomized controlled trial at a later stage. This study will explore the influence of specific TCM therapies on survival to provide further credible clinical evidence for the treatment of esophageal cancer with TCM.
Conclusions
This retrospective cohort study shows that TCM treatment is a prognostic protective factor for patients with stage IV esophageal SCC and appears to increase long term survival by two months. It is undeniable that in the real world, TCM is useful in the treatment of esophageal cancer, whether in syndrome differentiation or as an adjunct to Western medicine.31,32 A comprehensive approach based on TCM may reduce adverse reactions from Western therapies, increase treatment sensitivity, and reduce the chance of reoccurrence. In this study, the individualistic nature of “treatment based on syndrome differentiation” was key to improving longevity in stage IV SCC patients.
Role of the Sponsor
The sponsors had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Abbreviations
TCM, Traditional Chinese medicine; TCM group, Traditional Chinese medicine Group; Non-TCM group, Non-Traditional Chinese medicine Group; B, Regression Coefficient; SE, Standard Error of regression coefficient; RR, Risk Ratio; CI, Confidence Interval; WHO, World Health Organization; SCC, Squamous Cell Carcinoma; HIS, Health Information System; CEA, Carcino-embryonic antigen; CA199, Carbohydrate antigen199.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This retrospective, real-world study was approved by the Ethics Committee of Henan Provincial Hospital of Traditional Chinese Medicine [2019(40)], and informed consent was waived. Since this study has no potential harm to the included cases, we applied for exemption from the informed consent process. We keep patient data strictly confidential and this study abides by the Helsinki declaration.
Funding
This work was supported by the Henan Provincial Administration of traditional Chinese Medicine [2019JDZX031]; the National Natural Science Foundation of China [81804057]; and Henan Science and Technology Department Science and Technology Research Project [202102311118].
Disclosure
The authors declare no conflicts of interest for this work.
References
1. Enzinger PC, Mayer RJ. Esophageal cancer. N Engl J Med. 2003;349(23):2241–2252. doi:10.1056/NEJMra035010
2. Yin M, Zhang S, Guo L, et al. Analysis of cancer incidence and mortality in Henan province, 2012. Henan Med Res. 2016;v.25(01):1–10.
3. Cheng Y, Chen H, Wu S, et al. Esophageal squamous cell carcinoma and prognosis in Taiwan. Cancer Med. 2018;7(9):4193–4201. doi:10.1002/cam4.1499
4. Lancet T; The Lancet. GLOBOCAN 2018: counting the toll of cancer. Lancet. 2018;392(10152):985. doi:10.1016/S0140-6736(18)32252-9
5. Chen W, Sun K, Zheng R, et al. Report of cancer incidence and mortality in different areas of China, 2014. Chin Cancer. 2019;27(001):1–14.
6. Malhotra GK, Yanala U, Ravipati A, Follet M, Vijayakumar M, Are C. Global trends in esophageal cancer. J Surg Oncol. 2017;115(5):564–579. doi:10.1002/jso.24592
7. Zhang Y, Shen Q, Li J. Traditional Chinese medicine targeting apoptotic mechanisms for esophageal cancer therapy. Acta Pharmacol Sin. 2016;37(3):295–302. doi:10.1038/aps.2015.116
8. Ying J, Zhang M, Qiu X, Lu Y. The potential of herb medicines in the treatment of esophageal cancer. Biomed Pharmacother. 2018;103:381–390.
9. Wu T, Yang X, Zeng X, Eslick GD. Traditional Chinese medicinal herbs in the treatment of patients with esophageal cancer: a systematic review. Gastroenterol Clin North Am. 2009;38(1):153–167, x. doi:10.1016/j.gtc.2009.01.006
10. Napier KJ, Scheerer M, Misra S. Esophageal cancer: a review of epidemiology, pathogenesis, staging workup and treatment modalities. World J Gastrointest Oncol. 2014;6(5):112–120. doi:10.4251/wjgo.v6.i5.112
11. Kato H, Nakajima M. Treatments for esophageal cancer: a review. Gen Thorac Cardiovasc Surg. 2013;61(6):330–335. doi:10.1007/s11748-013-0246-0
12. Jiang M, Lu C, Zhang C, et al. Syndrome differentiation in modern research of traditional Chinese medicine. J Ethnopharmacol. 2012;140(3):634–642. doi:10.1016/j.jep.2012.01.033
13. Li S. Framework and practice of network-based studies for Chinese herbal formula. J Chin Integr Med. 2007;5(5):489–493.
14. Wu M, Wang Y. Internal Medicine of Traditional Chinese Medicine.
15. National Pharmacopoeia Committee Pharmacopoeia of the People’s Republic of China.
16. Gao X. Traditional Chinese Medicine. People’s Medical Publishing House; 2000.
17. Chang Z, Jia D, Bare J. Chinese Materia Medica. PMPH-USA; 2015.
18. Kamangar F, Chow WH, Abnet CC, Dawsey SM. Environmental causes of esophageal cancer. Gastroenterol Clin North Am. 2009;38(1):27–57, vii.
19. Umar SB, Fleischer DE. Esophageal cancer: epidemiology, pathogenesis and prevention. Nat Clin Pract Gastroenterol Hepatol. 2008;5(9):517–526. doi:10.1038/ncpgasthep1223
20. Lin Y, Totsuka Y, He Y, et al. Epidemiology of esophageal cancer in Japan and China. J Epidemiol. 2013;23(4):233–242. doi:10.2188/jea.JE20120162
21. He S, Wei P. Research summary of tumor treatment from sputum. J Pract Trad Chin Intern Med. 2004;18(6):486.
22. Short MW, Burgers KG, Fry VT. Esophageal cancer. Am Fam Physician. 2017;95(1):22–28.
23. Sohda M, Kuwano H. Current status and future prospects for esophageal cancer treatment. Ann Thorac Cardiovasc Surg. 2017;23(1):1–11. doi:10.5761/atcs.ra.16-00162
24. Kang D. Discussion on real world research. J Chin Med Abstracts Oncol. 2017;9(2):100–103.
25. Liu J, Li L, Zhao Y. Research progress of TCM syndrome types and treatment of esophageal cancer. Chin Arch Trad Chin Med. 2017;7:142–144.
26. Wang Q, Yao S. Molecular basis for cold-intolerant yang-deficient constitution of traditional Chinese medicine. Am J Chin Med. 2008;36(5):827–834. doi:10.1142/S0192415X08006272
27. Xue R, Fang Z, Zhang M, Yi Z, Wen C, Shi T. TCMID: traditional Chinese medicine integrative database for herb molecular mechanism analysis. Nucleic Acids Res. 2013;41(D1):D1089–1095. doi:10.1093/nar/gks1100
28. Zhang R, Zhu X, Bai H, Ning K. Network pharmacology databases for traditional Chinese medicine: review and assessment. Front Pharmacol. 2019;10:123.
29. Chao J, Dai Y, Verpoorte R, et al. Major achievements of evidence-based traditional Chinese medicine in treating major diseases. Biochem Pharmacol. 2017;139:94–104. doi:10.1016/j.bcp.2017.06.123
30. Liu C, Chen J, Yang S, et al. iTRAQ-based proteomic analysis to identify the molecular mechanism of Zhibai Dihuang Granule in the Yin-deficiency-heat syndrome rats. Chin Med. 2018;13:2.
31. Nie J, Zhao C, Deng LI, et al. Efficacy of traditional Chinese medicine in treating cancer. Biomed Rep. 2016;4(1):3–14. doi:10.3892/br.2015.537
32. Xiang Y, Guo Z, Zhu P, Chen J, Huang Y. Traditional Chinese medicine as a cancer treatment: modern perspectives of ancient but advanced science. Cancer Med. 2019;8(5):1958–1975. doi:10.1002/cam4.2108
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.