Back to Journals » Patient Preference and Adherence » Volume 17
Towards a Therapy for Geographic Atrophy: A Patient’s Experience
Authors Enoch J ![]() , Ghulakhszian A, Sekhon M, Crabb DP, Taylor DJ, Dinah C
, Ghulakhszian A, Sekhon M, Crabb DP, Taylor DJ, Dinah C ![]()
Received 17 August 2022
Accepted for publication 9 December 2022
Published 1 February 2023 Volume 2023:17 Pages 299—310
DOI https://doi.org/10.2147/PPA.S386662
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Jamie Enoch,1 Arevik Ghulakhszian,2 Mandeep Sekhon,3 David P Crabb,1 Deanna J Taylor,1 Christiana Dinah2,4
1Department of Optometry and Visual Sciences, City, University of London, London, UK; 2Ophthalmology Department, London North West University Healthcare NHS Trust, Central Middlesex Hospital, London, UK; 3Centre for Applied Health and Social Care Research, Kingston and St George’s, University of London, London, UK; 4Department of Brain Sciences, Imperial College, London, UK
Correspondence: Christiana Dinah, Ophthalmology Department, London North West University Healthcare NHS Trust, Central Middlesex Hospital, Acton Lane, London, NW10 7NS, UK, Tel +44 208 453 2253, Email [email protected]
Purpose: Geographic atrophy (GA) is the advanced form of the non-neovascular (dry) type of age-related macular degeneration. Presently, GA cannot be treated. However, new therapies administered by intravitreal injection are in late-stage development. These can slow down, but do not stop or reverse, GA progression. The acceptability of these emerging therapies to people with GA is currently unknown. The present case study explores the perspectives of a person living with GA who took part in the terminated Phase 3 clinical trial of Lampalizumab, a candidate intravitreal treatment for GA. We explored this patient’s perspective on the retrospective acceptability of regular Lampalizumab injections, and the prospective acceptability of future intravitreal therapies for GA.
Patients and Methods: A 78-year-old woman living in the UK was recruited as part of a mixed-methods pilot study and interviewed by telephone, regarding: her experience of the Lampalizumab trial injections; and her thoughts regarding emerging intravitreal therapies for GA. The Framework Method was used for initial inductive analysis of the interview transcript. Subsequently, deductive analysis was undertaken, informed by the Theoretical Framework of Acceptability (TFA).
Results: For this participant, intravitreal injections in the Lampalizumab trial were acceptable, although streamlining processes within the clinic would have improved the patient experience. Regarding prospective acceptability of new intravitreal therapies, the participant considered a delay in progression of GA a valuable goal. Potential discomfort, anxiety and inconvenience associated with regular intravitreal injections would be acceptable in the context of preserving her vision for as long as possible.
Conclusion: Analysis of one participant’s experience demonstrates the value of exploring GA patients’ unique views on the acceptability of new intravitreal treatments. Larger prospective studies will provide more insight that help to optimise treatment design and delivery, thereby maximising likelihood of adherence and persistence when these therapies eventually arrive in clinic.
Keywords: geographic atrophy, qualitative, case study, acceptability
Introduction
Geographic atrophy (GA) is a late-stage form of age-related macular degeneration (AMD) as classified with the Beckmann classification system,1 for which no approved treatments currently exist. In GA, retinal lesions slowly expand over several years until central vision is lost. Estimates suggest there are approximately 5 million people worldwide living with GA,2 and GA accounts for approximately one-quarter of legal blindness in the UK.3 While treatment for nAMD leads to improvement in vision, there is currently no therapy for GA, a significant area of unmet need. However, new therapies for GA are currently in development which could transform treatment pathways for people living with the condition.4 In Phase 2 trials, two intravitreal injection treatments have been shown to slow the average rate of GA growth by up to 30% when delivered monthly.5,6 One of these treatments, pegcetacoplan, has met its primary endpoint at 24 months in a global phase 3 trial, demonstrating a reduction in GA lesion growth by 22%.7
Intravitreal therapies are an established mode of treatment for patients with nAMD and other retinal diseases, typically demonstrating a rapid and substantial improvement in vision within weeks of commencing treatment.8,9 Various modalities are under investigation for the management of GA including sustained delivery implants (Brimonidine),10 and intravitreal and suprachoroidal gene therapy,11 which would reduce the burden of injections. However, regular intravitreal therapies remain the frontrunners, with positive Phase 3 results recently reported.7,12 These intravitreal therapies for GA currently in late phase trials would slow the progression of, rather than halt or reverse, visual loss. Therefore, it is still unknown how acceptable such treatments will be for people living with GA. This acceptability dimension is especially pertinent in GA, given that even with the rapid efficacy of nAMD intravitreal injections,13 patients report significant treatment-related burdens such as anxieties or discomfort related to the injection procedure, long travel and waiting times, and impacts on accompanying relatives or caregivers.14,15
We define acceptability, in accordance with Sekhon et al's definition in their Theoretical Framework of Acceptability (TFA), as a
Multi-faceted construct that reflects the extent to which people delivering or receiving a healthcare intervention consider it to be appropriate, based on anticipated or experienced cognitive and emotional responses to the intervention16
Acceptability can be assessed using the TFA before, during or after engagement with an intervention; and acceptability can be considered retrospectively, looking back on an intervention that has taken place, or prospectively, looking forward to an anticipated intervention. To begin exploring this complex question of the acceptability of new GA therapies, we are conducting a qualitatively-driven mixed-methods pilot study, the protocol for which is described elsewhere.17 The aim of the pilot study is to explore the acceptability of current intravitreal treatments in late-stage development, and thereby influence service delivery and future treatment design to support patients’ adherence to and persistence with therapy.
Nested within the pilot study, the purpose of the present study was to explore the unique experience of one particular participant, who had participated in a - now terminated - clinical trial of Lampalizumab for GA. Phase 3 trials of Lampalizumab, delivered by intravitreal injection every four or six weeks, failed to achieve their primary endpoint, to reduce the enlargement of GA lesions compared to sham treatment.18 The participant understood that if she were in the treatment arm of the Phase 3 Lampalizumab trial, the treatment would slow down but not reverse GA and hopefully help preserve her central vision for longer.
The participant’s perspective is particularly unique, as someone who has experienced regular intravitreal injections for GA (albeit in an unusual trial context), and could therefore comment on acceptability of these emerging treatments both retrospectively and prospectively. Accordingly, our aim in the current study was to explore the retrospective and prospective acceptability of regular intravitreal injections for slowing the progression of GA for this particular participant.
Methods
A case study involves exploration of a complex, real-world situation or event within its specific context.19 The present study could be considered as an instrumental case study,20 whereby we explore a single case in all its complexity in order to provide illustrative insights into a broader issue.
Data Collection and Participant Details
The participant was a white British woman living with GA, in her 70s, retired, and living alone. She was involved in the Lampalizumab trial for 18 months between 2016 and 2018. Best corrected visual acuity at the time of the interview was 6/24 (logMAR 0.6) in both eyes. Ocular images for this participant are displayed in Figure 1A (right eye) and Figure 1B (left eye).
 |
Figure 1 (A) Image of Right Eye using Heidelberg Spectralis. Near infrared shows geographic atrophy lesion with foveal island spared. Bscan shows loss of RPE and photoreceptor layer with hypertransmission consistent with geographic atrophy. (B) Image of Left Eye using Heidelberg Spectralis. Near infrared shows geographic atrophy lesion which has encroached on the fovea. Bscan similar findings to (A). |
After obtaining consent, data were collected from the participant’s medical records, as well as a semi-structured interview conducted on 26 July 2021, lasting approximately 90 minutes. We used an interview topic guide previously developed as part of our larger mixed-methods pilot study,17 focused on the prospective acceptability of new emerging treatments for GA. We supplemented this topic guide with additional questions relating to the participant’s experience of involvement in the Lampalizumab clinical trial. The interview was audio-recorded and transcribed verbatim.
Ethical approval for the pilot study (within which this case study was nested) was granted by the Health Research Authority on 23 March 2021 (IRAS Project ID: 287824). Written informed consent to participate in the study, and for the publication of their clinical details, was obtained from the participant.
Data Analysis
The Framework Method of qualitative analysis was used to analyse the data.21,22 The Framework Method is particularly suitable for facilitating collaborative analysis, and the use of a framework matrix to structure the data provides a transparent “audit trail” from the raw data to generation of themes.
The various stages of analysis were initially conducted by one author (JE). The first stage involved initial familiarisation with the participant’s transcript, conducting several re-readings. Subsequently, inductive coding took place, with initial “open codes” developed in order to encapsulate interesting, meaningful elements of the transcript. A framework matrix was developed, with relevant parts of the transcript charted into a table with each row denoting a different code. The software NVivo 12 Pro (QSR International, Melbourne, Australia) was used to sort the qualitative data into this analytical framework.
The resulting initial framework was discussed as a team, with all authors consulted to consider and refine the appropriateness of the coding and categorisation. Subsequently, where relevant, codes were sorted deductively into the corresponding constructs of Sekhon et al’s Theoretical Framework of Acceptability (TFA).16 The TFA facilitated analysis of the participant’s retrospective experience of Lampalizumab injections, and exploration of her prospective attitudes towards emerging GA treatments.
Respondent validation took place following initial data analysis, with the participant reading drafts of this case study to ensure the analysis and interpretations in this paper faithfully reflected her experiences and impressions.
Results
Living with Geographic Atrophy
Although not the central focus of the study, the participant discussed various functional, psychological and social impacts of living with GA, understanding of which helps to contextualise her hopes for treatment. She discussed the impact of GA particularly on reading and driving cessation (”The biggest difference I’ve noticed since this has got rapidly worse is reading. And a close second would be having to stop car driving. But clearly that’s never coming back.”); her emotional reactions to GA; and how GA affects her family life. The participant was nuanced about the difficulties caused by GA, finding workarounds to functional challenges in order to continue with her habitual activities, but experiencing frustration and distress about the losses and changes caused by GA (“I hate the additional complexity of having to deal with everything”). The supplementary table provides detailed exploration of the participant’s experience of the impacts of GA.
Acceptability of Intravitreal Injections for GA
Our analysis of the participant’s account drew on the Theoretical Framework of Acceptability (TFA),16 as illustrated in Table 1. This framework allows for consideration of factors that may influence a person’s willingness to potentially accept an intervention, in this case regular intravitreal injections treatments for GA. Within the TFA, acceptability was considered from two time points: retrospectively (looking back at GA treatment in the specific context of the Lampalizumab trial) and prospectively (considering new intravitreal GA treatments in the pipeline).
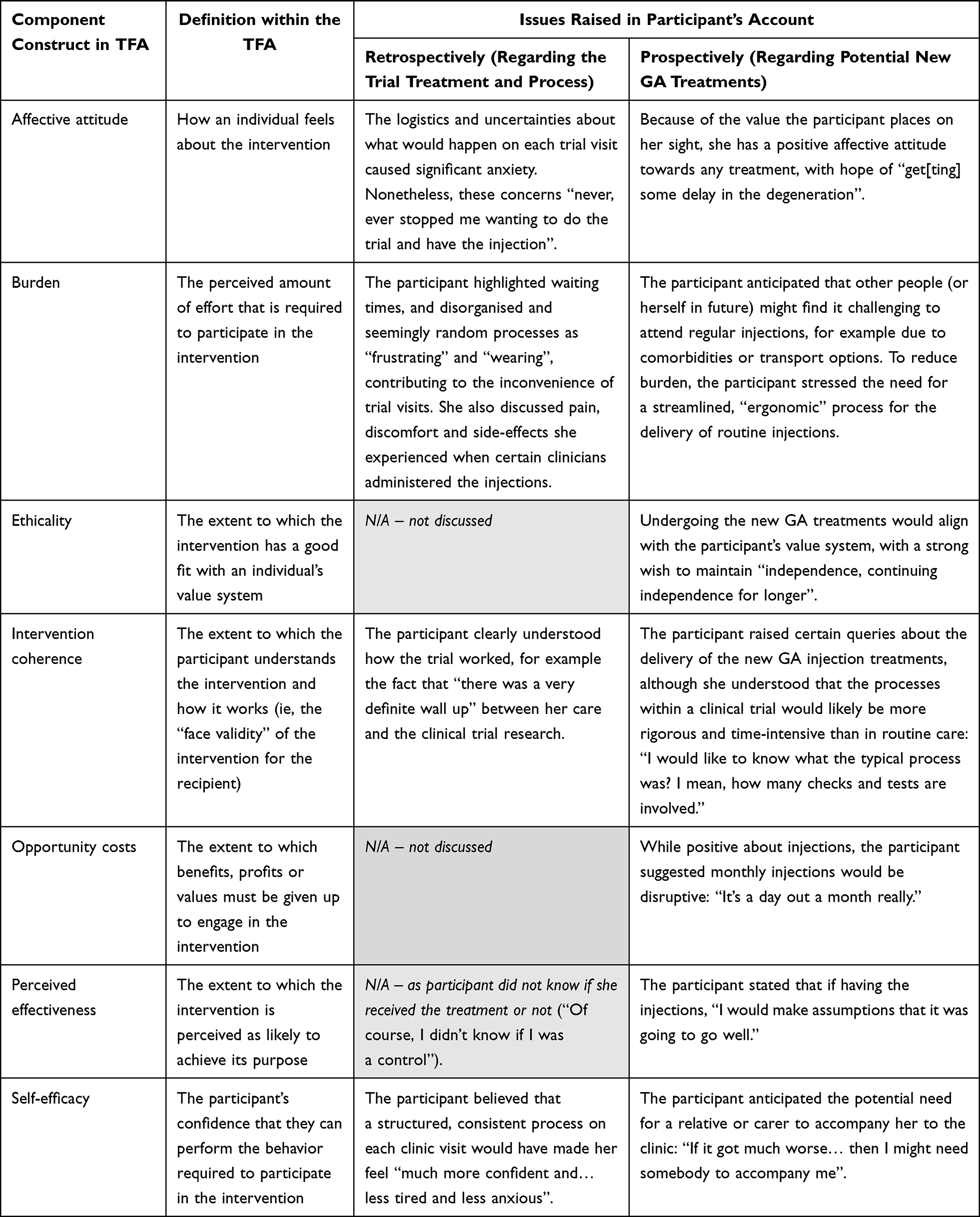 |
Table 1 Component Constructs of Sekhon et al’s Theoretical Framework of Acceptability (TFA); Construct Definitions; and Issues Discussed by Participant Relevant to Retrospective Acceptability of the Trial Intervention and Prospective Acceptability of Potential New Treatments |
Affective Attitude
The Affective attitude construct of the TFA considers how an individual feels about an intervention. Reflecting on experiences of injections during the Lampalizumab trial, the participant discussed experiencing anxiety and uncertainty after injections linked to the severity of the side effects:
I mean there were a few times when it was quite painful and quite sore and quite inflamed. I did want to ring up and say, you know look, is this all right? I was anxious about it overnight.
The anxiety here specifically related to concerns about whether the side effects were significant and potentially required medical intervention. The participant related that such side effects were generally not long-lasting and the anxiety surrounding these lessened over time:
Well, I knew that the pain would go away. I knew that the gravely-ness or the blobs would go away [laughs]. So I did stop worrying about it, yes. But it didn’t happen until a little way into the trial because the first person doing it was so expert.
The participant reasoned that people with GA who had previously had anti-VEGF treatment for nAMD might be less anxious about intravitreal injections, since much of her anxiety stemmed from waiting times and delays that made her feel uncertain about when she would receive an injection:
I suppose the people who have wet macular degeneration and have been having jabs in their eyes for years, probably have a much less anxious approach to it than I have, based on 18 months of a trial, you know? I imagine that they’re probably much more used to it and much less worried that it’s actually going to happen.
The participant reflected on the significant impact of the injecting clinician on her experience of each injection. Indeed, one factor that reassured the participant at the start of the trial was the consistency and familiarity of the clinical team treating her, and trust in their experience:
There was somebody who started off doing it who was tremendous. After that, various people did it. I must say seniority had nothing to do with it [laughs]. Some were just better at it than others. Or maybe it was just my better day.
The participant was very clear that despite many suggestions on how the experience and process of participating in such a trial could be improved, she had a very positive experience engaging with staff working on the trial:
I’ve talked to you a lot about the bad things on it, haven’t I? But the staff were almost always kind and as helpful as they could be. The admin staff were under immense pressure, but almost always managed to give me a cup of tea.
The participant discussed how her experience of the Lampalizumab trial related to her affective attitude towards the new emerging treatments for GA. Despite some of the negative feelings and anxiety that accompanied each visit to the clinic during the trial, she was clear that her attitude towards future intravitreal injections would be positive:
I mean having thought about it, I think I would put up with that [experience of the trial] again if I was going to get some delay in the degeneration.
Indeed, for this participant, the small treatment effect and inconveniences associated with the emerging GA treatments would not be off-putting: “I think I would have the treatment at almost any cost”. When asked about the possibility of injections being delivered in the community, the participant felt that while “the idea of doing it locally is excellent” and convenient, she might feel “slightly unbacked up if anything were to go a bit awry” compared to a hospital setting.
While positive overall about the prospect of injections for GA, the participant was aware that her attitude towards the intravitreal injections and monthly clinic visits could change over time, depending on her situation and possible comorbidities:
Suppose I manage to hit, I don’t know, 85 with arthritis and all the rest of it [laughs]. I might be looking on it a bit differently.
Burden
The TFA construct of “Burden” relates to the effort required to participate in an intervention, in this case GA treatment.
When retrospectively considering her experience of the Lampalizumab trial, the participant highlighted the burdensome experience of waiting times in the clinic. While she recognised that long waiting times were “part of the process”, waiting around could be “extremely frustrating”. This was particularly the case when waiting times increased beyond the considerable time the participant had already factored into the clinic visit:
Sometimes things went wrong and drove you mad. Like somebody forgot to order the eye drops. So at the end of the four hours, you found you had an[other] hour and a half’s wait.
For the participant, it was not only the length of clinic visits, but also the limited organisation of the various trial processes, that intensified the inconvenience:
I mean it was not a very comfortable process in itself because there were so many parts to it, so there were so many waits… Of course, I appreciate that this research process was likely to be more extensive than actual treatment.
Crucially, the inconvenience never overwhelmed the participant’s motivation to proceed with injections, in the hope of supporting the trial and potentially benefitting from slowing down of the GA progression:
I mean it never, ever stopped me wanting to do the trial and have the injection. But the morning I woke up when it was that morning, [I thought to myself], “Oh no” [laughs]. Whereas I’m sure if you were doing it routinely and you weren’t having so much uncertainty about it, it would be better.
This exchange demonstrates the participant’s commitment to the trial, despite the anxiety and uncertainty she felt in advance of each clinic visit.
Distinct from the burdens of the trial processes, the participant also specifically highlighted burdens of sporadic pain and discomfort of the injection treatment, depending on the administering clinician:
I do recall that first of all there was getting your eye in to the right state and at the right time, so it definitely was anaesthetised. Then there was an enormous amount to do with hygiene and protection of the eye. Then that rather horrid business of putting the little clips on the eye to pull it back.
Sometimes it was painful. It partly depended on the practitioner. There were some who were superb and you wouldn’t have known they’d been near your eye, and then others - and despite the anaesthetic, it jolly well hurt, for a short time.
Similarly, the participant also highlighted the sporadic presence of unsettling side effects post-injection:
Sometimes there were side effects afterwards which could be quite nasty. A general feeling of sort of powdery-ness in the eye, soreness and on one or two occasions, large floating blobs. Which didn’t hurt at all but were rather weird. On other occasions, you wouldn’t have known you’d had it. So I was more affected by who I saw coming down the corridor than the general worry about it.
Considering the new GA injections, one potential burden the participant considered, more for others than for herself, was the logistical ease of traveling to attend for regular injections:
I think I’m fortunate in having enough money to be able to arrange travel… I used to be very impressed and horrified by people who’d been through what I’d been through and who were going to go and wait for the bus… and I guess they were also going home to a house in which they were the only occupant… So I do think ease of getting there would be a big factor.
Here, the participant shows awareness of how GA patients’ unique living situations and contextual circumstances could differentially influence the convenience and feasibility of regular injection visits.
Nonetheless, the participant was clear that no burden would have deterred her from persisting with injections during the trial (“there was nothing that would have stopped [me] having it”), or from initiating the new GA treatments. For example, the participant did not regard the potential increased risk of nAMD as a definitive drawback (although of course “not something I would wish for”), once reassured by the clinical researchers that anti-VEGF injections could likely be delivered on the same day and hospital visit as the GA injections:
The additional risk of getting wet AMD wouldn’t be an off-put, although I would much rather it didn’t happen. And it wouldn’t be an extra session every month.
Ethicality
The Ethicality construct of the TFA focuses on the extent to which an intervention has a good fit with an individual’s value system. The participant’s positive attitude towards GA treatment related to the high value she places on her vision:
You’d walk a lot further to help your sight perhaps than you even would to help your hearing or your arthritis or [laughs] whatever, you know - whatever.
This primacy placed on sight by the participant related to the desire for “continuing independence for longer”, and “on a practical level, any delay in losing the ability to read”. She rationalised that the precise benefits of treatment will differ substantially from person to person, for example reflecting that, “I think one of the greatest pains people have is having to give up driving”. She would also value the injections’ potential to provide “a bit of peace of mind” for the participant’s family, as injections to slow the GA progression could mean “less worry [for them] about how I’m feeling and possibly getting on”.
Intervention Coherence
Intervention coherence in the TFA is the extent to which participants understand an intervention and how it works. The participant was clear about the purpose, design and constraints of the trial, and understood that she could not necessarily know if she had benefitted from the intervention:
Of course one never knew whether one was a control… I got absolutely nothing. But when I went back for my next appointment, I don’t think any comparison was made. Because of course they weren’t allowed to, if you see what I mean. There was a very definite wall up between the people who are looking after you and the people who are conducting the trial and in possession of all that information.
This demonstrates the participant’s understanding of the research as an activity distinct from her clinical care, rather than equating trial participation with personalised care (a common misunderstanding known as the therapeutic misconception).23
Prospectively, anticipating new emerging GA treatments, the participant understood that these would help “get some delay in the degeneration”, rather than stopping or reversing the degeneration. Her uncertainties around future treatments related more to the processes of the injection delivery, aligning with her concerns about waiting times and a lack of streamlined processes during the trial: “I would like to know what was the typical process? I mean how many checks and tests are involved.”
Opportunity Costs
Opportunity costs refer to the extent to which benefits, profits or values have to be given up to engage in an intervention.
The participant did not discuss Opportunity Costs in the context of retrospective acceptability of the trial intervention. However, in terms of prospective acceptability of new therapies, the participant reflected that an injection every month could be disruptive, because even if the clinic visit itself were quick, with travel to and from clinic, it would still take up the whole day:
I think it would be the disruption to… life, if it was monthly. Because that comes round quite quickly. It’s a day out a month really.
Perceived Effectiveness
Within the TFA, perceived effectiveness relates to the extent to which an intervention is perceived as likely to achieve its purpose. The participant could not reflect on this retrospectively in the context of the trial, because she did not know if she received the treatment or not (“Of course, I didn’t know if I was a control”). However, looking forward, she anticipated that new injections for GA would be effective for her, stating, “I would make assumptions that it was going to go well.” At the same time, the participant was also aware that the likely timescale of concluding clinical trials and approving any new GA treatments might mean that she herself would not have the opportunity to benefit from treatment:
By the time it’s been through all its clinical trials and all the rest of it, I’m pretty sure this treatment is going to be too late for me. That’s a shame but it’s the way it is.
Self-Efficacy
The TFA construct of Self-efficacy refers to a person’s confidence that they can perform behaviors required to participate in the intervention. In the participant’s view, a logical flow and transparent, consistent processes (“a bit of ergonomics… so that people flowed through”) could have reduced the anxiety and fatigue that accompanied each visit, and provided a sense of confidence and reassurance. As the participant stated:
Having been through a process which you feel has been efficient and planned… really would help. However I do recognise the realities under which the NHS is working and the tremendous effort that the staff put in.
Regarding confidence to attend for injections in future, the participant anticipated that if her sight worsened to a certain point, she might need to be accompanied to the clinic for injections:
But if it got much worse - when it gets much worse - then I might need somebody to accompany me… I think it would be unlikely to be a family member because they’re all working. So I’d have to make another arrangement.
This clearly illustrates that the level of treatment acceptability will not necessarily remain stable for each individual, but will vary across the - potentially lifelong - course of the GA injections.
Discussion
Summary of Learnings from the Case Study
This case study provides a unique window into an individual’s experience of receiving monthly intravitreal Lampalizumab therapy for geographic atrophy in the UK within a clinical trial.
Using the TFA, we demonstrate the multi-faceted aspects of patient acceptability as they relate to regular intravitreal injections for GA for this specific participant. It is clear that she places great value on her sight which significantly outweighs the anxieties and concerns associated with anticipating the intravitreal injection or even potential side-effects. As such, she considered a delay in progression of GA a valuable goal, and the associated potential discomfort, anxiety and inconvenience acceptable in the context of preserving her vision for as long as possible. This resonates with previous reports about the experiences of people with neovascular AMD receiving anti-VEGF injections, that these patients may fear further deterioration of vision more than the injections themselves.24,25 It also aligns with Caswell et al’s case study of an individual with GA, who would opt for any treatment to maintain vision regardless of the burdens.26 The participant in our case study anticipated that the significant burden of frequent hospital visits and long waiting times could become a deterrent in the future, for example if she were to develop other co-morbidities or to require support from others to attend regular injections. Nonetheless, the participant frequently highlighted the specific, unique nature of her circumstances and experiences with regard to her participation in the trial and views on the injections, and recognised that receiving treatment in clinic would be a distinct experience. Additionally, recent Phase 3 clinical trial results of intravitreal therapies suggest that injections given every-other-month – which clearly for this participant would be less burdensome – may be similarly efficacious to monthly injections. The DERBY and OAKS trials of APL-2 demonstrate a marginal difference in GA growth reduction between the monthly and every-other-month treatment regimen (19% reduction for eyes treated monthly vs 16% reduction for eyes treated every-other-month in DERBY; 22% reduction for eyes treated monthly vs 18% reduction for eyes treated every-other-month in OAKS).7
The participant advocated a more streamlined, efficient process if intravitreal therapies for GA become available in the clinic. Given the widespread availability of retinal imaging modalities in the community,27 and proposed connectivity between hospital eye services and community optometrists,28,29 intravitreal injection services for GA may be best established as a hybrid model, with imaging in the community and treatment visits in hospital, reducing the burden on patients. In the UK, where the participant is based, intravitreal injections are currently delivered in hospital only; as part of our larger pilot study, we explore the thoughts of participants on the acceptability of possible injection delivery in the community.
Strengths and Limitations
This case study is a starting point towards understanding how patients with conditions like GA experience the complex journey towards a new treatment. We align with the view of Todres, Galvin and Holloway,30 who emphasise the importance of considering processes or “journeys”, and not solely outcomes, within a humanised, person-centred vision of healthcare:
There is increasing evidence… citizens are worried that the more personal dimensions of care are being neglected in favor of “bottom line” outcomes; the quality of the journey is just as important as the destination.
A strength of the case study method is that it provides rich, in-depth description and analysis of one participant’s “journey”, in a level of detail, comprehensiveness and granularity that would be challenging using quantitative (or certain other qualitative) methodologies.
A significant limitation of this case study relates to the timing of the data collection. Firstly, the interview with the participant took place almost three years after the Lampalizumab trial was terminated. While qualitative research does not seek to “control” for recall bias,31 it is important to consider that the account shared by the participant was not contemporaneous with the experiences she described, and so clinical trial processes may have since evolved. Secondly, many case studies integrate a longitudinal approach to data collection in order to explore change and developments over time. In our case study, while numerous interactions with the participant took place, there was only one substantial research interview, several years after trial termination.32 Lastly, as our patient was a participant in a clinical trial evaluating efficacy of regular intravitreal injections for GA, her views may be less likely to reflect that of the general population with GA. Clinical trial participants in several different fields of medicine have been shown to be unrepresentative of patients encountered in real-world clinical practice.33 In ophthalmology, trial participants treated with ranibizumab have represented a narrower spectrum of patient profiles than participants in non-interventional studies.34
Conclusion
As trials for new GA treatments continue apace, it is important to consider the acceptability of the interventions under investigation for those living with the condition. Incorporating qualitative research into or alongside these trials will allow for real-time exploration of issues around the participants’ views on acceptability of treatment. Such insights may enable refinement of design and/or delivery of interventions that yield optimal outcomes, due to improved uptake of and adherence to therapies when they eventually arrive in clinic. Our case study supports the need for larger, prospective research studies to explore the complexities of GA treatment acceptability in diverse populations.
Abbreviations
AMD, age-related macular degeneration; Anti-VEGF,anti-vascular endothelial growth factor; GA, geographic atrophy; nAMD, neovascular age-related macular degeneration; OCT, optical coherence tomography; TFA, Theoretical Framework of Acceptability.
Ethics Approval and Informed Consent
Ethical approval for the pilot study within which this case study was nested was granted by the Health Research Authority on 23 March 2021 (IRAS Project ID: 287824). Written informed consent to participate in the study, and for the publication of their clinical details, was obtained from the participant. The study was performed in accordance with the Helsinki Declaration of 1964, and its later amendments.
Consent for Publication
The participant provided written consent for the case study to be published, after reading and providing feedback on several iterations of the report. The signed consent form is available on request.
Acknowledgments
We are incredibly grateful to the participant who shared her experience with us, which provided the basis for this article. She provided invaluable and detailed advice and feedback as the article evolved. She has chosen to remain anonymous, but is first author of this article in all but name.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The pilot study referred to in the article, within which this case study was nested, has been supported by: the National Institute for Health Research (NIHR) Enabling Involvement Fund (EIF; grant number EIFApp ID: 397); the City, University of London School of Health Sciences Higher Education Innovation Fund (HEIF); and Apellis Pharmaceuticals (Grant ID: AMR-000001). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript for this case study.
Disclosure
Jamie Enoch, Arevik Ghulakhszian, Mandeep Sekhon and Deanna J Taylor declare that they have no competing interests.
David P Crabb reports grants from Roche, grants and personal fees from Santen, grants and personal fees from Apellis, grants from Allergan, personal fees from Thea, personal fees from Bayer and personal fees from Centervue, outside the submitted work. DPC receives funding from the Innovative Medicines Initiative 2 Joint Undertaking under grant 116076 (Macustar). This joint undertaking receives support from the European Union’s Horizon 2020 research and innovation program and European Federation of Pharmaceutical Industries and Associations (EFPIA). The communication reflects the author’s view and that neither IMI nor the European Union, EFPIA, or any Associated Partners are responsible for any use that may be made of the information contained therein.
Christiana Dinah has served on advisory boards for Novartis, AbbVie, Ora Clinical, Roche and Apellis. CD is on the scientific advisory board for Ora Clinical, has received speaker fees from Roche and Novartis and holds a research grant from Apellis.
The authors report no other conflicts of interest in this work.
References
1. Ferris III FL, Wilkinson CP, Bird A, et al. Clinical classification of age-related macular degeneration. Ophthalmology. 2013;120(4):844–851. doi:10.1016/j.ophtha.2012.10.036
2. Wong WL, Su X, Li X, et al. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: a systematic review and meta-analysis. Lancet Glob Health. 2014;2(2):e106–e116. doi:10.1016/S2214-109X(13)70145-1
3. Chakravarthy U, Bailey CC, Johnston RL, et al. Characterizing disease burden and progression of geographic atrophy secondary to age-related macular degeneration. Ophthalmology. 2018;125(6):842–849. doi:10.1016/j.ophtha.2017.11.036
4. Dinah C, Enoch J, Ghulakhszian A, Taylor DJ, Crabb DP. Intravitreal treatment for geographic atrophy: coming soon to a patient near you? Eye. 2021;36:1121–1123. doi:10.1038/s41433-021-01591-1
5. Jaffe GJ, Westby K, Csaky KG, et al. C5 inhibitor Avacincaptad pegol for geographic atrophy due to age-related macular degeneration: a randomized pivotal phase 2/3 trial. Ophthalmology. 2021;128(4):576–586. doi:10.1016/j.ophtha.2020.08.027
6. Liao DS, Grossi FV, El Mehdi D, et al. Complement C3 inhibitor pegcetacoplan for geographic atrophy secondary to age-related macular degeneration: a randomized phase 2 trial. Ophthalmology. 2020;127(2):186–195. doi:10.1016/j.ophtha.2019.07.011
7. Heier J, Singh R, Wykoff C, et al. Efficacy of intravitreal pegcetacoplan in geographic atrophy: 24-month results from the phase 3 OAKS and DERBY trials. Available from: https://investors.apellis.com/static-files/78d1b209-7324-4c4c-8b20-bf7778493bae.
8. Rosenfeld PJ, Brown DM, Heier JS, et al. Ranibizumab for neovascular age-related macular degeneration. NEJM. 2006;355(14):1419–1431. doi:10.1056/NEJMoa054481
9. Heier JS, Brown DM, Chong V, et al. Intravitreal aflibercept (VEGF trap-eye) in wet age-related macular degeneration. Ophthalmology. 2012;119(12):2537–2548. doi:10.1016/j.ophtha.2012.09.006
10. Kuppermann BD, Patel SS, Boyer DS, et al. Phase 2 study of the safety and efficacy of brimonidine drug delivery system (Brimo DDS) generation 1 in patients with geographic atrophy secondary to age-related macular degeneration. Retina. 2021;41(1):144–155. doi:10.1097/IAE.0000000000002789
11. Kovacs KD, Ciulla TA, Kiss S. Advancements in ocular gene therapy delivery: vectors and subretinal, intravitreal, and suprachoroidal techniques. Expert Opin Biol Ther. 2022;22(9):1193–1208. doi:10.1080/14712598.2022.2121646
12. Iveric Bio. Iveric bio announces positive topline data from zimura® GATHER2 phase 3 clinical trial in geographic atrophy [internet]. Parsippany, New Jersey. Available from: https://investors.ivericbio.com/news-releases/news-release-details/iveric-bio-announces-positive-topline-data-zimurar-gather2-phase.
13. Finger RP, Daien V, Eldem BM, et al. Anti-vascular endothelial growth factor in neovascular age-related macular degeneration - A systematic review of the impact of anti-VEGF on patient outcomes and healthcare systems. BMC Ophthalmol. 2020;20(1):294. doi:10.1186/s12886-020-01554-2
14. Thier A, Holmberg C. The patients’ view: age-related macular degeneration and its effects–a meta-synthesis. Disabil Rehabil. 2022;44(5):661–671. doi:10.1080/09638288.2020.1775901
15. Boyle J, Vukicevic M, Koklanis K, et al. Experiences of patients undergoing repeated intravitreal anti-vascular endothelial growth factor injections for neovascular age-related macular degeneration. Psychol Health Med. 2018;23(2):127–140. doi:10.1080/13548506.2016.1274040
16. Sekhon M, Cartwright M, Francis JJ. Acceptability of healthcare interventions: an overview of reviews and development of a theoretical framework. BMC Health Serv Res. 2017;17(1):88. doi:10.1186/s12913-017-2031-8
17. Enoch J, Ghulakhszian A, Crabb DP, Dinah C, Taylor DJ. Acceptability of intravitreal injections in geographic atrophy: protocol for a mixed-methods pilot study. BMJ Open. 2021;11(4):e049495. doi:10.1136/bmjopen-2021-049495
18. Holz FG, Sadda SR, Busbee B, et al. Efficacy and safety of lampalizumab for geographic atrophy due to age-related macular degeneration: chroma and spectri phase 3 randomized clinical trials. JAMA Ophthalmol. 2018;136(6):666–677. doi:10.1001/jamaophthalmol.2018.1544
19. Thomas G. A typology for the case study in social science following a review of definition, discourse, and structure. Qualitative Inquiry. 2011;17(6):511–521. doi:10.1177/1077800411409884
20. Stake RE. Case studies. In: Denzin N, Lincoln Y, editors. Strategies of Qualitative Inquiry. London: SAGE Publications; 2003:134–164.
21. Ritchie J, Spencer L. Qualitative data analysis for applied policy research. In: Analysing Qualitative Data. London: Routledge; 1994:173–194.
22. Gale NK, Heath G, Cameron E, Rashid S, Redwood S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med Res Methodol. 2013;13(1):117. doi:10.1186/1471-2288-13-117
23. McCormick JB. How should a research ethicist combat false beliefs and therapeutic misconception risk in biomedical research? AMA J Ethics. 2018;20(11):1100–1106.
24. Droege KM, Muether PS, Hermann MM, et al. Adherence to ranibizumab treatment for neovascular age-related macular degeneration in real life. Graefes Arch Clin Exp Ophthalmol. 2013;251(5):1281–1284. doi:10.1007/s00417-012-2177-3
25. Joko T, Nagai Y, Mori R, et al. Patient preferences for anti-vascular endothelial growth factor treatment for wet age-related macular degeneration in japan: a discrete choice experiment. Patient Prefer Adherence. 2020;14:553–567. doi:10.2147/PPA.S228890
26. Caswell D, Caswell W, Carlton J. Seeing beyond anatomy: quality of life with geographic atrophy. Ophthalmol Ther. 2021;10(3):367–382. doi:10.1007/s40123-021-00352-3
27. Reeves BC, Scott LJ, Taylor J, et al. The Effectiveness, cost-effectiveness and acceptability of Community versus Hospital Eye Service follow-up for patients with neovascular age-related macular degeneration with quiescent disease (ECHoES): a virtual randomised balanced incomplete block trial. Health Technol Assess. 2016;20(80):1.
28. Hau S, Ehrlich D, Binstead K, Verma S. An evaluation of optometrists’ ability to correctly identify and manage patients with ocular disease in the accident and emergency department of an eye hospital. Br J Ophthalmol. 2007;91(4):437–440. doi:10.1136/bjo.2006.105593
29. Banes MJ, Culham LE, Bunce C, Xing W, Viswanathan A, Garway-Heath D. Agreement between optometrists and ophthalmologists on clinical management decisions for patients with glaucoma. Br J Ophthalmol. 2006;90(5):579–585. doi:10.1136/bjo.2005.082388
30. Todres L, Galvin KT, Holloway I. The humanization of healthcare: a value framework for qualitative research. Int J Qual Stud Health Well-Being. 2009;4(2):68–77. doi:10.1080/17482620802646204
31. Galdas P. Revisiting bias in qualitative research: reflections on its relationship with funding and impact. In: International Journal of Qualitative Methods. Los Angeles, CA: SAGE Publications; 2017:1609406917748992.
32. Elliott D, Husbands S, Hamdy FC, Holmberg L, Donovan JL. Understanding and improving recruitment to randomised controlled trials: qualitative research approaches. Eur Urol. 2017;72(5):789–798. doi:10.1016/j.eururo.2017.04.036
33. Kennedy-Martin T, Curtis S, Faries D, Robinson S, Johnston J. A literature review on the representativeness of randomized controlled trial samples and implications for the external validity of trial results. Trials. 2015;16(1):1–14. doi:10.1186/s13063-015-1023-4
34. Ziemssen F, Feltgen N, Holz FG, et al. Demographics of patients receiving Intravitreal anti-VEGF treatment in real-world practice: healthcare research data versus randomized controlled trials. BMC Ophthalmol. 2017;17(1):1–20. doi:10.1186/s12886-017-0401-y
 © 2023 The Author(s). This work is published by Dove Medical Press Limited, and licensed under a
Creative Commons Attribution License.
The full terms of the License are available at http://creativecommons.org/licenses/by/4.0/.
The license permits unrestricted use, distribution, and reproduction in any medium, provided the
original author and source are credited.
© 2023 The Author(s). This work is published by Dove Medical Press Limited, and licensed under a
Creative Commons Attribution License.
The full terms of the License are available at http://creativecommons.org/licenses/by/4.0/.
The license permits unrestricted use, distribution, and reproduction in any medium, provided the
original author and source are credited.