Back to Journals » International Journal of General Medicine » Volume 15
Total Meat Intake is Associated with Life Expectancy: A Cross-Sectional Data Analysis of 175 Contemporary Populations
Authors You W ![]() , Henneberg R, Saniotis A, Ge Y, Henneberg M
, Henneberg R, Saniotis A, Ge Y, Henneberg M
Received 29 September 2021
Accepted for publication 30 December 2021
Published 22 February 2022 Volume 2022:15 Pages 1833—1851
DOI https://doi.org/10.2147/IJGM.S333004
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Wenpeng You,1,2 Renata Henneberg,1 Arthur Saniotis,1,3 Yanfei Ge,4,5 Maciej Henneberg1,6
1Biological Anthropology and Comparative Anatomy Research Unit (BACARU), Adelaide Medical School, University of Adelaide, Adelaide, SA, Australia; 2FAPAB Research Center, Avola SR, 96012, Sicily, Italy; 3Department of Anthropology, Ludwik Hirszfeld Institute of Immunology and Experimental Therapy, Polish Academy of Sciences, Wroclaw, Poland; 4Australian Graduate School of Management (Executive MBA Candidate), University of New South Wales, Sydney, New South Wales, Australia; 5Community Services, Health & Lifestyle, Technical and Further Education, Adelaide, South Australia, 5000, Australia; 6Institute of Evolutionary Medicine, University of Zürich, Zurich, Switzerland
Correspondence: Wenpeng You, Adelaide Medical School, University of Adelaide, Adelaide, SA, 5005, Australia, Email [email protected]
Background: The association between a plant-based diet (vegetarianism) and extended life span is increasingly criticised since it may be based on the lack of representative data and insufficient removal of confounders such as lifestyles.
Aim: We examined the association between meat intake and life expectancy at a population level based on ecological data published by the United Nations agencies.
Methods: Population-specific data were obtained from 175 countries/territories. Scatter plots, bivariate, partial correlation and linear regression models were used with SPSS 25 to explore and compare the correlations between newborn life expectancy (e(0)), life expectancy at 5 years of life (e(5)) and intakes of meat, and carbohydrate crops, respectively. The established risk factors to life expectancy – caloric intake, urbanization, obesity and education levels – were included as the potential confounders.
Results: Worldwide, bivariate correlation analyses revealed that meat intake is positively correlated with life expectancies. This relationship remained significant when influences of caloric intake, urbanization, obesity, education and carbohydrate crops were statistically controlled. Stepwise linear regression selected meat intake, not carbohydrate crops, as one of the significant predictors of life expectancy. In contrast, carbohydrate crops showed weak and negative correlation with life expectancy.
Conclusion: If meat intake is not incorporated into nutrition science for predicting human life expectancy, results could prove inaccurate.
Keywords: meat intake, ecological study, life expectancy, vegetarian, evolution, agriculture
Introduction
Life expectancy at birth is the measure synthetically describing mortality in a population. It is estimated that 20–30% of human life expectancy is determined by genetic factors, and 70–80% is determined by environmental factors.1 Life expectancy at 5 years of age is similarly influenced by genetic factors, while it excludes neonatal, infant and early childhood mortality that depends heavily on environmental factors, especially hygiene and infection controls. These percentages, however, have not received a general scientific consensus. What is clearer is the genetic/environmental interplay that informs human health. Nutrition offers the means to improve health and well-being and acts as a significant predictive factor of healthy aging, so it appears as one of the major determinants of life expectancy.2
Extensive studies regarding the role of conventional meat containing diets and vegetarian diet (excluding meat3) in increasing our life expectancy have been controversial and circumstantial.2 Since the early Paleolithic period, meat consumption (understood as intake of parts of any animal bodies) has constituted a proportion of the hominin diet.4 It has been argued that consumption of meat, as a high-quality component of the hominin diet, allowed increases in body and brain sizes while at the same time permitting reduction of the size of the gastrointestinal tract producing typically human increased brain weight/body weight ratios.5–7
The effects of meat eating on human health have been debated in nutrition and diet research for a long time. Over the last 50 years, although the associations between meat eating and illness are circumstantial and controversial8–11 to some extent, they have prompted the spread of vegetarianism and veganism, based on the assumption that non-meat diets provide more health benefits than diets that include meat.12–14 Moreover, it has been argued that vegetarianism and veganism form a part of “trendy” Western consumerist lifestyles – only accessible to privileged “white” people.15 Vegetarianism that has been prevalent in Western countries has been subject to prejudice,15 low self-esteem, and low psychological adjustment.16
To date, there has been prevailing research stating that vegetarians tend to have greater life expectancy compared with non-vegetarians in some populations, particularly among Seventh-day Adventists.14,17 However, lack of population representativeness and failure to remove the influence of lifestyle in these studies have been heavily criticised.18 Thus, the suggestion that vegetarian diet improves longevity is questionable. For example, several studies with large sample sizes conducted in Australia18 and the United Kingdom19,20 did not show that meat eating correlated negatively with life expectancy after controlling for health-related elements of lifestyles.
Meat intake has been associated with adverse health issues, but the evidence in support of this hypothesis is limited and reliant on epidemiologic associations as opposed to clinical trials, which are supposed to reveal a cause-and-effect relation.21–25 For instance, epidemiological studies in humans could not reveal a direct relationship between nitrite and/or nitrate, which has been assumed as the major carcinogenic factor derived from meat consumption, and cancer development.25
Before agriculture was introduced (circa 11–9000 years ago), human ancestors could not grow, harvest and store the majority of plant-based products as the staple food. Plant foods are mostly accessible only in particular seasons of the year.26 Contrariwise, animals, including large game, small animal, fish and some insects, could constantly provide humans with meat as the staple food.5,26–30
Although modern agriculture diversifies our diet components and offers us many food choices, meat is still one of the significant food components worldwide.31 Modern nutritional science has revealed that meat provides complete nutrition. Modern food technology is capable of producing artificially all meat components, so that in special situations complete meat contents can be introduced into a diet without including actual muscle tissue of animals. This, however, does not argue against the benefits of eating meat. On the contrary, it supports that meat contents are necessary for good human nutrition. Availability of artificially produced meat may provide a solution for people who are ethically opposed to killing animals.
This population-based study, using data collected by the United Nations and its agencies, tests the hypothesis that, worldwide, populations with more meat consumption have greater life expectancies.
Materials and Methods
Data Selection Criteria and Data Sources
The data for this study were selected in consideration of the following criteria:
a) Listed all the countries/territories of the world (research subjects) with data on meat intake, and then collected other variables that were matched with this list. A set of data consisting of 175 populations with all required information available was obtained for this study. This covers approximately 90% of the world.
b) Considered the 3 years’ delayed presentation of effects of meat intake on metabolic/physical changes possibly affecting health adversely.
c) Included the major potential confounding factors, such as total calories consumed, wealth measured by the gross domestic product (GDP PPP), urbanization, obesity and education levels.
A whole set of data is attached to this article (Appendix 1).
1) The independent variables are the cross-population food supply data32 on food groups of total meats (“flesh of animals used for food, The FAO 201833”), cereals, starchy roots, sugar and sweeteners (sugars). These variables are expressed in grams per person per day in each population. In order to avoid random errors occurring during the data collection and integration, each variable was averaged for the years 2011–2013. These most up-to-date data were captured from the Food Balance Sheet published by the United Nations Food and Agricultural Organization (FAO).
Cereals, starchy roots and sugars are primarily energy sources that do not provide a large nutrient range. They have been clustered and new variable “carbohydrate crops” was created as the independent contrast variable to meat. Another reason for clustering is that meat used to provide over 50% energy needs before the introduction of agriculture circa 11–9000 years ago,26 while carbohydrate foods eventually became a source of over 50% of current human energy needs.32
Additionally, we extracted the world meat intake data (g/day/capita) for all the years with the available FAO data (1961–2013) as the independent variable to correlate with the worldwide longitudinal life expectancy for the same years.
In terms of meat source included in this study, it is necessary to highlight that, in order to reflect the real meat consumption in human diet, we included total meat intake, instead of a particular animal meat or a particular group of animal meat as the predicting variable. As per the FAO, meat is defined as “flesh of animals used for food”, and total meat includes beef and veal, buffalo meat, pig meat, mutton and lamb, goat meat, horse meat, chicken meat, goose meat, duck meat, turkey meat, rabbit meat, game meat and offal.33
2) The dependent variables in the analysis were the population level life expectancy at birth (e(0)), and at 5 years (e(5)) for both sexes calculated for the period of 2010–2015 by region, subregion and country published by the United Nations.34 The child mortality rate before age 5 years (average of years 2011–2013) was also extracted from the World Bank data35 as another dependent variable.
3) The potential confounding variables are population-specific data on:
i) Total calories intake (kcal/capita/day) which was the average for the 3 years (2011–13) as per FAO Food Balance Sheet32
The relationship between total energy intake, rather than that of particular nutrients in the diet, and life span has been debated in animal and human models36–38 so it needed to be controlled for.
ii) GDP PPP, purchasing power parity in 2011 US dollars for comparability among countries as per the World Bank data39
Income and wealth, as a measure of socioeconomic status, have been less frequently used but are an important variable along with education and occupation in affecting human health and life span.40,41
iii) Urbanization, the percentage of the population living in urban areas as determined by the United Nations (UN) Population Division’s World Urbanization Prospects42
Urbanization implies considerable changes in the living habits of extant humans, easy access to health care,43 how they earn their livelihoods, dietary regimes, and the wide range of environmental factors to which humans are exposed.43–46 Consequently, some researchers have assumed that urban populations are healthier than their rural counterparts.43
iv) Obesity levels as measured by the prevalence of adult individuals with the body mass index (BMI) equal to or exceeding 30 kg/m2 were obtained from WHO.47 Obesity is a result of metabolic imbalances and is considered as a risk factor for a number of non-communicable diseases.
We have also used information on the percentage of vegetarians in countries (N=30) that had this information available and on the level of education as measured by the percentage of adults (>25 years old) with completed primary school education (World Development Indicators).48 These latter data were available only for 103 countries, and the rationale for exploring the relationship between the level of education and e(0) is that education may affect eating habits and domestic food preparation.
Data Analysis
Our data analysis proceeded in five steps to examine the association between meat intake and life expectancies and child mortality at the population level:
1. Scatter plots were produced with the cross-population data (not transformed) in Microsoft Excel® to explore and visualize the strength, shape and direction of worldwide cross-sectional association between meat intake and life expectancy and mortality variables.
To highlight the hypothesis and facilitate the readership to understand the meaning of this study, the correlation between total meat intake and e(0) was explored in each WHO region with the scatterplots.
2. Bivariate (Pearson’s r and Spearman’s rho) correlations were performed to evaluate the direction and strength of the correlations between all the variables across all countries. Log transformed data were used to improve homoscedasticity of data distributions. “Curve estimation” function of the SPSS was used to explore shape of relationships between logarithmed data. In all cases linear relationships were better or equal to the long list of possible other relationships including logarithmic, inverse, quadratic, cubic, compound, power, growth, S-curve, exponential and logistic. Distributions of residuals around linear regression lines were close to normal (Appendix 2). Thus, linear relationships were consistently used in our analyses of log-transformed variables.
Nonparametric correlation analysis was conducted to examine whether the Pearson’s correlations between logarithmed values of life expectancy/mortality and all variables differ due to potentially non-homoscedastic distributions of variables.
3. Partial correlation of Pearson’s moment-product approach was performed to identify the worldwide correlations between meat intake and life expectancy/mortality independent of the potential confounding variables, energy intake, urbanization, GDP PPP and obesity.
4. Standard multiple linear regression was conducted to identify and rank the variables that had the greatest predicting effects on life expectancies and mortality.
Since life expectancies and mortality measures are strongly correlated (Table 1), most further analyses were carried out only for the life expectancy at birth.
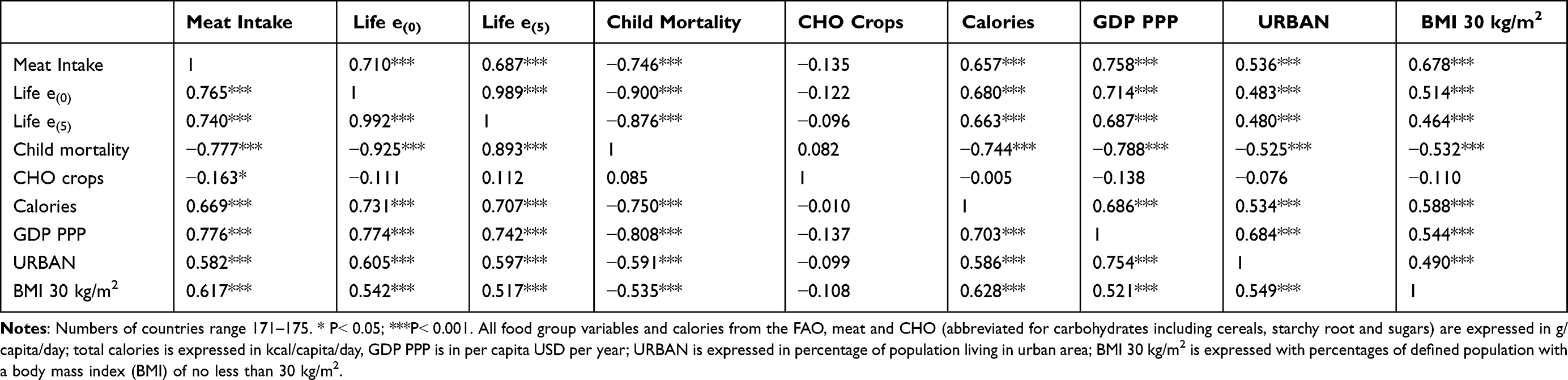 |
Table 1 Pearson's r (Above the Diagonal) and Nonparametric “rho” (Below the Diagonal) Coefficients of Correlation Between All Variables Studied (Log-Transformed Variables) |
To compare the magnitudes of contribution of meat intake and carbohydrate crops to life expectancy stepwise linear regression analysis was repeated twice when meat intake and carbohydrate crops were excluded, respectively. The decrease of R2 due to exclusions of meat intake and carbohydrate crops was respectively calculated and compared.
5. Countries grouped for the association analysis.
Human diet patterns, varying in different food components, may be affected by the food availability type in a particular region, socio-economic status and by cultural beliefs. In order to demonstrate that a correlation exists between meat availability and life expectancy regardless of these factors, countries were grouped for correlation analyses. The criteria for grouping countries were:
1) Developed and developing world defined by the United Nations;49
2) Six regions grouped by WHO:50 African Region (AFRO), Region of the Americas (AMRO), South-East Asia Region (SEARO), European Region (EURO), Eastern Mediterranean Region (EMRO), and Western Pacific Region (WPRO);
3) Countries sharing specific characteristics such as geography, culture, development role or socio-economic status,51 Organisation for Economic Co-operation and Development (OECD),52 Asia-Pacific Economic Cooperation (APEC),53 Southern African Development Community (SADC),54 the Arab World,55 Latin America (LA), and Asia Cooperation Dialogue (ACD).56 All the population listings were sourced from their official websites for matching, except LA which is self-classified based on the region primarily speaking romance languages.
4) In particular, two country clusters that are associated with overall health benefits are created for exploring the relationships between the level of total meat intake and e(0):
A list of countries that have the percentage of vegetarian population segment was accessed through the extensive internet search. Its summary can be accessed at https://en.wikipedia.org/wiki/Vegetarianism_by_country#cite_note-2. This list was matched to the populations with the data on life expectancy.
Countries primarily on the Mediterranean diet were grouped. The Mediterranean diet is a way of eating that is based on the traditional cuisines of Greece, Italy and other countries that border the Mediterranean Sea. It includes meat but also primarily plant-based food, such as olive oil, grains, vegetables, fruits, nuts and herbs. Due to the combination of food components, the Mediterranean diet is considered a comprehensively healthy diet and has been associated with a reduction in all-cause mortality in most of observational studies.57,58 However, it is not clear if a portion of a particular food component, such as total meat can improve its health effect leading to greater life expectancy. We extracted the countries bordering the Mediterranean Sea and matched them to the list of countries with available data on e(0) for creating a country group, Mediterranean diet.
5) Countries above and below the average meat intake The FAO 2018.33
The population list was also stratified into two population groupings based on our calculated mean daily meat intake. The high meat intake group was comprised of populations with more than 138.82 g/day/capita meat consumption on daily basis; and the low meat intake group included those populations with less than 138.82 g/day/capita on daily basis. The relationships between meat eating and life expectancies were examined in these two population groups, respectively.
Bivariate correlations, partial correlation of Pearson’s moment-product and multiple linear regression analysis were conducted with SPSS v. 25 on the log-transformed variables. Microsoft Excel® was used for scatter plots of raw data (not log transformed). The significance of association was kept at the 0.05 level, but 0.01 and 0.001 levels were also reported. Standard multiple linear regression analysis criteria were set at probability of F to enter ≤0.05 and probability of F to remove ≥0.10.
Results
Figure 1 shows, globally, the cross-sectional association between meat intake and life expectancies and child mortality. Life expectancies show linear positive regression on meat consumption, while child mortality is negatively exponentially related to meat intake. All regressions show strong correlations – meat intake explains at least 50% of variance in life expectancy and mortality.
 |
Figure 1 The worldwide cross-sectional association between meat intake and life expectancy at birth, at 5 years of age and child mortality below the age of 5 years. Notes: Data sources: Meat consumption is expressed in g/capita/day and extracted from the FAO website. Life expectancy data are measured with at birth and 5 years old respectively and extracted from the United Nations. Mortality rate was extracted from the World Bank website. |
The relationship trend was observed in the WHO regions except in SEARO (Figure 2).
 |
Figure 2 The relationship between meat intake and life expectancy at birth in each WHO region. Notes: The cross-sectional association between predicting variable (meat intake) and dependent variables (life expectancy at birth) was graphed for each WHO region in the scatterplots above, respectively. Data sources: meat consumption is expressed in g/capita/day and extracted from the FAO website. Life expectancy is measured at birth. Unit of axis: the X-axis – Meat consumption (kg/person/year); the Y-axis – Life expectancy at birth (year). |
Table 1 presents, worldwide, that, in Pearson’s r analysis, e(0) shows significant and strong correlation with meat intake (r=0.710, p<0.001) and weak and negative correlation with carbohydrate crops intake (r=−0.111, p=0.150). Other measures of life expectancy and mortality show similar relationships. Nonparametric correlations indicate similar relationships between variables studied (Table 1).
Table 2 indicates that in partial correlation analysis life expectancies and child mortality correlate significantly with meat intake when controlling for carbohydrate crops intake, urbanization, GDP PPP, calories, and obesity. However, with meat intake and the same potential confounding factors being kept constant, carbohydrate crops do not correlate with life expectancy and child mortality at all. This may imply that meat intake correlates with life expectancy not because of its energy contribution, but rather due to other nutrient effects.
 |
Table 2 Pearson's r, and Partial Correlations Between Meat Intake and Life Expectancies and Child Mortality |
Table 3 shows that meat intake is identified as the one of the variables that have a significant influence on life expectancies and child mortality when all the six variables, GDP PPP, calories, meat, urban, obesity and carbohydrate crops are included as predictors in multivariate linear regression analysis.
 |
Table 3 Results of Multiple Linear Regression Analyses to Identify Significant Predictors of Life Expectancy e(0), e(5) and Child Mortality (n=171–175) |
When meat is excluded as one of the predicting variables respectively in linear regression, adjusted R2 decreases by about 0.03. Carbohydrate crops are not a significant predictor of life expectancies/mortality in either model regardless of whether meat is included as one of the predicting variables or not. Statistically, this means that carbohydrate foods do not contribute to the change of life expectancy nor child mortality. This finding corresponds to the lack of correlation of carbohydrate intake with life expectancies in Pearson’s r correlation, Spearman’s rho and partial correlation analysis.
Table 4 shows that, in general, meat intake is correlated with life expectancy in different population groupings regardless of cultural backgrounds, socioeconomic status, meat intake level and geographic locations of the clustered countries.
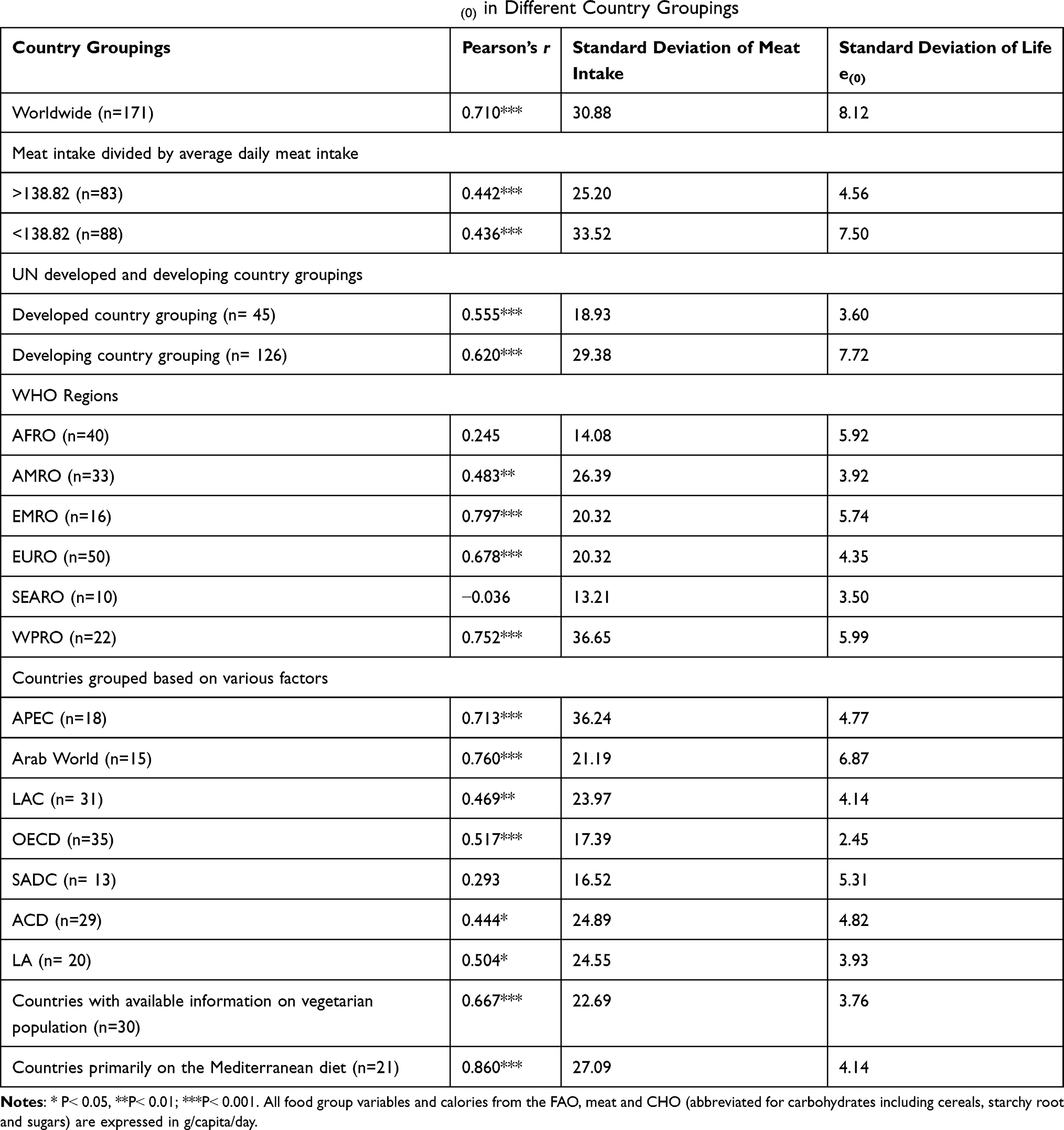 |
Table 4 Correlation of Meat Intake to Life Expectancy e(0) in Different Country Groupings |
Meat intake correlates with life expectancy in population groupings with high meat intake (r=0.442, p<0.001, n=83), low meat intake (r=0.436, p<0.001, n=88), high socioeconomic status (r=0.555, p<0.001, n=45) and low socioeconomic status (r=0.620. p<0.001, n=126).
Based on the WHO region classifications, the correlation is observed in all regions except in SEARO. This may be due to similar diet patterns in SEARO countries with little difference in the amount of meat intake and similar life expectancies. This is statistically presented with the smallest standard deviations of meat intake (SD=13.21) and e(0) (SD=3.50) compared to other WHO Regions.
The correlations between meat intake and life expectancy are also observed in country groupings of the Arab World (geographically scattered in Asia and Africa, r=0.760, p<0.001), LA (r=0.504, p<0.05) and LAC (located in Americas only, r=0.469, p<0.001) featured with the similar cultures, respectively. The trends are also present in functional alliances, albeit some comprise developed countries only and others comprise both developing and developed countries (Table 4). Education has two possible effects on longevity and nutrition. It potentially improves health care, especially care for child health, and it may influence the food preparation in households and individual food choices that are partially informed by understanding the physiological role of nutrients. Since we could obtain uniform data for education levels for a smaller number of countries than those included in main analyses, we have conducted some analyses separately. We have chosen the percentage of adults who completed full primary education as the index of education in the country. This has been done in preference to other education indices that separate females from males or use higher levels of educational achievement because these characterise only parts of the entire population. In the partial correlation analysis keeping all other variables statistically constant, education correlates significantly (p=0.001) but weakly (r=0.334) with life expectancy and at a similar level (r=0.237, p=0.021) with meat consumption.
In the regression analysis (Table 5), education is an important contributor to life expectancy similar to caloric consumption while meat consumption has a significant effect on life expectancy at age 5 years.
 |
Table 5 A Multiple Regression Analysis to Identify Significant Predictors of the Life Expectancy at Birth (e(0)) in a Set of 103 Countries for Which Information About the Education Level Was Available |
Interestingly, among countries with available percentages of vegetarians, meat intake still has a moderately strong correlation with e(0) (r=0.667, p<0.001, n=30, Table 4). Unsurprisingly, populations with lower percentage of vegetarians have greater life expectancy, though the relationship is only marginally significant likely due to small sample size (r=−0.303, p=0.0518, n=30).
In the Mediterranean diet country grouping, the strong relationship trend was observed that high total meat intake is associated with greater e(0) (r=0.860, p<0.001, n=21, Table 4). This may suggest that, regardless of suggested beneficial health effects of Mediterranean diet, more total meat intake may benefit e(0) in the populations primarily on this diet.
Discussion
This ecological study examined the relationship between meat intake and life expectancy at birth e(0), at age 5 years e(5) and child mortality at a population level. Our statistical analysis results indicate that countries with the greater meat intake have greater life expectancy and lower child mortality. This relationship is independent of the effects of caloric intake, socioeconomic status (GDP PPP), obesity, urbanization (lifestyle) and education. Of course, nutritional variations among countries include many more variables than those included into this study. Diet composition, food preparation methods, cultural dietary constraints, availability of some nutrients and a number of other variables should have been considered to obtain a complete picture of meat’s importance in human diet. However, even with these possible analytical inadequacies, our statistical analyses indicate a significant role that meat plays in influencing variation of survival and mortality.
Meat has advantages over food of plant origin in containing complete protein with all essential amino acids, is rich in vitamins, in particular vitamin B12, and all essential minerals. It has a significant role not only for maintenance of health, development and proper growth59 but also has played an important evolutionary role in ancestral hominins for approximately 2.6 million years.60,61
Benefits of meat eating include better physical growth and development,62 optimal breastfeeding of neonates, and offspring growth.63 Human adaptation to meat eating and mechanism to digest and metabolise meat6,59,62,64–67 have been supported by studies in human dietary evolution. This may also be reflected in the importance of meat eating for human’s whole life span.5,60,68 Culturally, meat production and eating have also been integrated into human societies.62,69–72
A study of more than 218,000 adults from over 50 countries around the world suggests that consuming unprocessed meat regularly can reduce the risk of early death and can increase human longevity.73 A recent dietary advice published by Lancet Public Health advocates an increase of dietary meat in order to benefit our heart health and longevity.74 This study also highlights that saturated fat in meat may be cardio protective, as well as, that meat contains many vitamins and the essential amino acids for human health and well-being.73,74
Recent epidemiological literature highlights that increasing meat consumption, especially in its processed forms, may have adverse health effects, such as cancer,8 cardiovascular disease,75 obesity31,76–78 and diabetes.79 However, there has been no clinical trial evidence to consolidate the putative negative effects of processed meat consumption for human health.21 The aforementioned epidemiological literature is not reflected in the healthy food guidelines published by the government authorities for general public. These guidelines always include meat as a major human dietary component. One reason for their position could be a lack of evidence-based research that demonstrates negative aspects of meat consumption in the general human population.80–83 Statistically, the finding of this study unequivocally indicates that meat eating benefits life expectancy independently.
Meat contains high protein with all the essential amino acids, and is a good source of minerals (iron, phosphorus, selenium and zinc) and vitamins (B12, B6, K, choline, niacin, riboflavin). Simply put – a human animal consuming a body of another animal gets practically all constituent compounds of its own body. Recently, massive agricultural production and advanced food manufacturing technologies have made it possible to replace the beneficial nutrients of meat with other agricultural industry products and/or synthetic chemicals. For example, proteins are easy to obtain by incorporating nuts and beans into diet. Vitamin B12 can be absorbed adequately from cheese, eggs, milk, and artificially fortified pills, and iron can be found in legumes, grains, nuts, and a range of vegetables.84,85 Relying on meat nutrient replacements and available food products, well-planned vegetarian diets, including vegan diets, are nutritionally adequate and are appropriate for various individuals during all stages of life,84,85 but it is only because their nutritional composition adequately imitates and replaces what is commonly provided by meat. These technological developments provide an opportunity for individuals to select their dietary behaviours based on religious and ethical concerns. Traditionally, meat has been included in many human diets in order to provide humans engaged in high physical activity levels with substrate for muscle tissue synthesis and recovery support, increased bone density, and oxygen transport.84 Currently, however, dieticians are able to construct sport-specific diets for athletes based on vegetarian foods.84
Since many beneficial nutrients found in meat can now be replaced by vegetarian sources, increasing numbers of people have questioned whether meat consumption is necessary.84 Over the past decades, a number of studies have advocated that vegetarian or plant-based diets may contribute to low mortality rate, and high life expectancy. These studies have received criticism due to questionable study designs:
1) Health effects of a vegetarian diet may be only a perceived benefit. The correlation identified between vegetarianism and high life expectancy may not necessarily depend on their diets, but rather on the lifestyles that vegetarians maintain.18 It is important to acknowledge that vegetarians (especially in western countries) tend to be more “health-conscious”, with overall healthier lifestyle patterns than other people. Two studies conducted among British people have shown that vegetarians and non-vegetarians had very little20 and even no difference19 in life expectancy if other healthy lifestyle factors were considered. A study on the cohort consisting of 243,096 adults in Australia revealed that the protective effects of variations of vegetarian diets (semi-vegetarians or pesco-vegetarians) on life expectancy depended on multiple potential confounding factors, such as age, smoking and alcohol consumption, history of type 2 diabetes and cardiovascular diseases.18 Therefore, it is apparent that the advocacy of vegetarianism to increase longevity may have been biased.15
2) Vegetarianism study designs were flawed in that research subjects were not representative of the general population.86 With the exception of India and some Buddhist cultures, vegetarianism is practiced by a small percentage of world population. On this note, the Seventh-day Adventist cohort has been over researched in order to demonstrate the relationship between vegetarianism and life expectancy.12–14 However, studies in non-Adventist vegetarians have shown nil or very weak correlation between vegetarian diet and longevity.86 Importantly, the Seventh-day Adventist population engages in a beneficial life-style, which includes non-smoking, marital maintenance, regular exercise and maintaining normal body weight.87,88
Furthermore, a study conducted by Singh et al. showed that vegetarians did not benefit from their meat-free diet.12 However, Singh et al. have proposed that low meat consumption increases life expectancy in humans.12 This claim does not concur with our finding, which argues that more meat eating may increase human life expectancy. This discrepancy may arise due to several biases in Singh et al’s study: 1) The cohorts recruited for the study were not representative of global ethnicities. All the cohorts were derived from developed countries only (the United Kingdom, Germany and the United States). A majority of individuals in these countries did not succumb to mortality due to nutritional deficiency from low meat consumption, as they had access to nutrition supplements and good-quality Medical services.89–93 2) More potential confounders of the relationship between meat intake and life expectancy, such as total diet intake and urban lifestyle, could have been included for data analysis (with the exception of aging). 3) Levels of meat intake were only considered as three categories: zero, very low and low. This reduced the accuracy of the correlation due to the limited variation of meat intake quantity as the independent variable.
People on vegetarian diets may be able to maintain “health” because they avoid potential meat-related nutrient deficiencies through one or more of the following ways:
1) Taking meat nutrient replacements to meet essential nutrient needs.
2) Eating a vegetarian diet and identifying as vegetarian are two different things. Ruby (2012) and Rosenfeld and Burrow3,69 have concluded that the majority of self-identified vegetarians may still eat meat occasionally. This would allow them to absorb the unique nutrients from meat.69
3) Many vegetarians do not follow meat-free diets from birth. Instead, many have decided to avoid eating meat at some point during their adult lives.94 Thus, their dietary limitations missed the period of critical growth and development – childhood and early adolescence.
4) Many vegetarians include dairy products in their diets (eg, Hindus). These contain animal proteins and minerals in proportions similar to meat.
Saturated fat in red meat has been associated with the onset of atherosclerosis. However, this hypothesis has been based on observational or animal studies, instead of randomised controlled trials, a standard study designed to identify the causal relationship.95 Therefore, this conclusion has been subject to debate.96,97 Studies have revealed that low-fat diets reduced serum cholesterol, but they did not reduce cardiovascular disease incidence or mortality.98 The healthy diet recommendation advises people that their diet should have less saturated fat, but more polyunsaturated fat. Interestingly, when saturated fat is replaced with polyunsaturated fat in diet, cardiovascular events or mortality are not convincingly reduced.99 We are advancing the correlation between total meat, instead of red meat, and life expectancy. This hypothesis is supported by a systematic review concluding that total meat consumption did not facilitate the onset of atherosclerosis.100
Another finding in this study is that carbohydrate crops correlate with life expectancy weakly and negatively. This finding is supported by several ethnological and archaeological studies, which concluded that the transition to cereal-based diets caused a reduction in life expectancy74,101–103 because cereals tend to have lower nutritional value.
The correlation between meat and life expectancy was observed in all country groupings except in SEARO where small variation of meat consumption and life expectancies reduces covariance. It is worth noting that, in this study, countries on the Mediterranean diet have greater e(0) if there is more total meat in their diet. This finding may be sufficient to form the contrast to either beneficial or detrimental health benefit of the Mediterranean diet. Socioeconomic level is associated with mortality and e(0) due to a variety of reasons. However, the majority of countries bordering Mediterranean Sea are developing economics, and have high mortality rates for chronic diseases, such as cardiovascular diseases and cancers. The correlation between the Mediterranean diet and low incidence or low prevalence rates of chronic diseases might be sporadic in the studies in the populations surrounding the Mediterranean Sea because their high mortality rates or low e(0) have eliminated the patients with chronic diseases.
Previous studies controversially showed the health effects of selected meat groups, in particular red meat, on human health.100 However, a series of rigorous systematic reviews which were simultaneously published, concluded that there is a lack of sufficient evidence to show that red meat and processed meat contributes to cardiovascular diseases,104–106 cancer mortality and incidence104,106,107 and all-cause mortality.105 Although the red meat and processed meat have been associated with negative health outcomes, meat eating people are still determined to be omnivores due to their values and preferences.108 Therefore, dietary guidelines recommendation published in a reputable nutrition and diet journal advised that adults can maintain their current level of intake of red meat and processed meat.109
Contrary to the majority of studies that have focused on health effect of red meat, this study argues that total meat consumption, in general, benefits people health, which leads to greater longevity. This hypothesis is supported by a study conducted by Campbell advocating that total meat consumption may offset the detrimental effect of red meat on people’s health.100,110
Several strong points in this study need to be noted:
1) Independent variable, total meat (animal flesh), instead of different categories of meat was selected for the correlation analysis,4,111 which allows us 1) To reflect that human ancestors ate any available meat, and also various modern populations consume all sorts of meat in broad circumstances.31,112 2) To remove the potential and conflicting influence of different food cooking methods on health.113–118 3) To eliminate the bias from processing aids, preservatives and additives in ready-to-eat meat, which may pose adverse health effects to humans.8,119
2) Populations across the globe (representing about 90% of extant humans) were considered in this study as units. Data included in this study were aggregated at the population level, so that they include information relevant for all people in each population. Thus, we did not study a “sample” but practically the whole population. This had the advantage in overcoming the common biases in studies of limited sample size.
3) Data representativeness determines who the study results are targeted at. Apparently, data representativeness must be considered for all studies in order to avoid a defect in the study design.18 The argument that vegetarians have long life spans is questionable since most of the studies supporting this statement were conducted within the specific groups of people, such as Seventh-day Adventists. This argument may also be biased due to the “healthy cohort effect”, which drives health conscious people to be more likely to be recruited and remain in the study cohort than non-health conscious people.15,120
4) Reporting bias in nutrition studies has been a constant issue as food intake data must be reported by volunteers accurately and truthfully. However, a number of studies have shown that people tend to underreport energy intake121 and overreport healthy food consumption.122
5) Cross-sectional data at a population level used in this study may offer more accurate estimates of e(0) and meat intake than individual-based data adopted in nutrition studies. Data on e(0) and meat intake in this study were collected by observing all the populations at the same period of time, which provides general comparability.
6) Compared to previous sample-based studies (ecological studies posited on collecting relevant data), more potential confounders have been included in this study for analysing the relationship between meat intake and e(0).
Study Limitations and Strengths
Firstly, the intrinsic limitation conceptualized as the “ecological bias” or “ecological fallacy” exists in this ecological analysis.31,123 Population level data have been applied for analysing the correlation between meat intake and e(0). Therefore, this correlation might not necessarily be valid at an individual level.76,123
Secondly, the nature of the relationship between meat intake and longevity is longitudinal. However, the method adopted in this study is cross-sectional data analysis, which may not necessarily reflect the actual longitudinal relationship in particular populations.
However, the constant and significant correlation between meat intake and e(0) may increase the possibility of the true correlation at an individual level. The relationship identified in this study may have shed light at further studies within the cohorts with large sample size, high representativeness and long life period at an individual level.76,123
It is necessary to analyse the strengths of this study as well.
Firstly, an ecological study approach offers the advantage of including more data for correlation analyses between meat intake and e(0) in different modelling. Furthermore, the data included in this study tend to avoid the bias in the previous studies at the individual levels.
Secondly, other variables, which were not included in this study, such as dietary patterns determining differences in quantities of meat intake, may have confounded the relationship between meat intake and e(0). However, their potential influence could not be analysed and removed owing to the lack of the availability of such data. Like in other correlation analyses, the influence of variable residuals, which were controlled for in this study, might have not been eliminated completely.
Thirdly, GDP PPP may be a comprehensive life expectancy contributor. For instance, populations with greater GDP PPP may have higher meat affordability, better medical service and better education level. Each factor may contribute to life expectancy in its unique way, but it is impossible to collect all these data and include them as the potential separate confounders in the data analyses to remove their competing effects on life expectancy.
Finally, ideally, the food group variables included in this study should be the true consumed quantities, rather than their supply quantity as food wastage was not considered during data collection.124
Conclusions
This study has shown that meat intake is positively associated with life expectancy at national level. The underlying reasons may be that meat not only provides energy but also complete nutrients to human body. From the evolutionary point of view, meat has arguably been an indispensable component in human diet for millions of years, which is evidenced, genetically, by meat digesting enzymes and digestive tract anatomy. The complete nutritional profile of meat and human adaptation to meat eating have enabled humans to gain many physical benefits, including greater life expectancy. Meat intake, or its adequate replacement, should be incorporated into nutritional science to improve human life expectancy.
Abbreviations
WHO, World Health Organization; FAO, The Food and Agriculture Organization of the United Nations; UN, The United Nations; GDP PPP, Gross domestic product at Purchasing Power Parity; BMI, body mass index; SES, socioeconomic status.
Data Sharing Statement
All data for this study are freely available from the United Nations agencies’ official websites. The aim for using the data in this study complies with the terms and conditions set by the relevant UN agencies. Therefore, there is no need to apply for formal permission before using the data in this study. The data sources have been detailed in the “Materials and Methods”.
Ethics Approval and Consent to Participate
Human data involved in this research carry only negligible risk and are existing in the format that contains only non-identifiable data about human beings. Therefore, the Human Research Ethics Committee the University of Adelaide has exempted from ethical review (Reference 35404).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. Hjelmborg J. Genetic influence on human lifespan and longevity. Twin Res Human Gene. 2007;10(Supplement):34.
2. Cannella C, Savina C, Donini L. Nutrition, longevity and behavior. Arch Gerontol Geriatr. 2009;49:19–27. doi:10.1016/j.archger.2009.09.008
3. Ruby MB. Vegetarianism. A blossoming field of study. Appetite. 2012;58(1):141–150. doi:10.1016/j.appet.2011.09.019
4. Lawrie RA, Ledward DA. Lawrie’s Meat Science.
5. Leonard WR, Robertson ML. Evolutionary perspectives on human nutrition: the influence of brain and body size on diet and metabolism. Am J Hum Biol. 1994;6(1):77–88. doi:10.1002/ajhb.1310060111
6. Aiello LC, Wheeler P. The expensive-tissue hypothesis: the brain and the digestive system in human and primate evolution. Curr Anthropol. 1995;36(2):199–221. doi:10.1086/204350
7. Henneberg M. Evolution of the human brain: is bigger better? Clin Exp Pharmacol Physiol. 1998;25(9):745–749. doi:10.1111/j.1440-1681.1998.tb02289.x
8. You W, Henneberg M. Prostate cancer incidence is correlated to total meat intake–a cross-national ecologic analysis of 172 countries. APJCP. 2018;19(8):2229. doi:10.22034/APJCP.2018.19.8.2229
9. You W, Henneberg M. Meat consumption and prostate cancer incidence - global and regional associations. BJU Int. 2016;118:6–20.
10. Li T-C, Chijiwa K, Sera N, et al. Hepatitis E virus transmission from wild boar meat. Emerg Infect Dis. 2005;11(12):1958. doi:10.3201/eid1112.051041
11. Waters AE, Contente-Cuomo T, Buchhagen J, et al. Multidrug-resistant Staphylococcus aureus in US meat and poultry. Clin Infect Dis. 2011;52(10):1227–1230. doi:10.1093/cid/cir181
12. Singh PN, Sabaté J, Fraser GE. Does low meat consumption increase life expectancy in humans? Am J Clin Nutr. 2003;78(3):526S–532S. doi:10.1093/ajcn/78.3.526S
13. Le LT, Sabaté J. Beyond meatless, the health effects of vegan diets: findings from the Adventist cohorts. Nutrients. 2014;6(6):2131–2147. doi:10.3390/nu6062131
14. Orlich MJ, Singh PN, Sabaté J, et al. Vegetarian dietary patterns and mortality in Adventist Health Study 2. JAMA Intern Med. 2013;173(13):1230–1238. doi:10.1001/jamainternmed.2013.6473
15. MacInnis CC, Hodson G. It ain’t easy eating greens: evidence of bias toward vegetarians and vegans from both source and target. Group Process Intergroup Relat. 2017;20(6):721–744. doi:10.1177/1368430215618253
16. You W, Symonds I, Henneberg M. Low fertility may be a significant determinant of ovarian cancer worldwide: an ecological analysis of cross-sectional data from 182 countries. J Ovarian Res. 2018;11(1):68. doi:10.1186/s13048-018-0441-9
17. Beeson WL, Mills PK, Phillips RL, et al. Chronic disease among Seventh‐Day Adventists, a low‐risk group. Rationale, methodology, and description of the population. Cancer. 1989;64(3):570–581. doi:10.1002/1097-0142(19890801)64:3<570::AID-CNCR2820640303>3.0.CO;2-4
18. Mihrshahi S, Ding D, Gale J, et al. Vegetarian diet and all-cause mortality: evidence from a large population-based Australian cohort-the 45 and Up Study. Prev Med. 2017;97:1–7. doi:10.1016/j.ypmed.2016.12.044
19. Key TJ, Thorogood M, Appleby PN, et al. Dietary habits and mortality in 11 000 vegetarians and health conscious people: results of a 17 year follow up. BMJ. 1996;313(7060):775–779. doi:10.1136/bmj.313.7060.775
20. Appleby PN, Key TJ, Thorogood M, et al. Mortality in British vegetarians. Public Health Nutr. 2002;5(1):29–36. doi:10.1079/PHN2001248
21. Rosenbaum PR. Observation and Experiment: An Introduction to Causal Inference. Harvard University Press; 2017.
22. Teicholz N. The Big Fat Surprise: Why Butter, Meat and Cheese Belong in a Healthy Diet. Simon and Schuster; 2014.
23. Celada P, Bastida S, Sánchez-Muniz FJ. To eat or not to eat meat. That is the question. Nutr Hosp. 2016;33(1):177–181. doi:10.20960/nh.29
24. WHO-IARC. IARC Monographs evaluate consumption of red meat and processed meat. The International Agency for Research on Cancer; 2015.
25. Bouvard V, Loomis D, Guyton KZ, et al. Carcinogenicity of consumption of red and processed meat. Lancet Oncol. 2015;16(16):1599–1600. doi:10.1016/S1470-2045(15)00444-1
26. Cordain L, Miller JB, Eaton SB, et al. Plant-animal subsistence ratios and macronutrient energy estimations in worldwide hunter-gatherer diets. Am J Clin Nutr. 2000;71(3):682–692. doi:10.1093/ajcn/71.3.682
27. Richards MP, Hedges REM, Jacobi R, et al. FOCUS: gough’s Cave and Sun Hole Cave human stable isotope values indicate a high animal protein diet in the British Upper Palaeolithic. J Archaeol Sci. 2000;27(1):1–3. doi:10.1006/jasc.1999.0520
28. Jaouen K, Richards MP, Le Cabec A, et al. Exceptionally high delta(15)Nδ 15 N values in collagen single amino acids confirm Neandertals as high-trophic level carnivores. Proc Natl Acad Sci USA. 2019;116(11):4928–4933. doi:10.1073/pnas.1814087116
29. Eaton SB, Cordain L. Evolutionary aspects o f diet: old genes, new fuels. World Rev Nutr Diet. 1997;81:26–37. doi:10.1159/000059599
30. Eaton SB, Konner M. A consideration of its nature and current implications. N Engl J Med. 1985;312(5):283–289. doi:10.1056/NEJM198501313120505
31. You W, Henneberg M. Meat consumption providing a surplus energy in modern diet contributes to obesity prevalence: an ecological analysis. BMC Nutr. 2016;2:1–1.
32. FAO. FAOSTAT-food balance sheet; 2015. Available from: http://faostat3.fao.org/.
33. The, F.A.O. Products from slaughtered animals; 2018.
34. United Nations Department of Economic and Social Affairs Population Division. World population prospects: life expectancy at birth (both sexes combined) by region, subregion and country, 1950–2100 (years); 2017.
35. The World Bank. Mortality rate, under-5 (per 1000 live births); 2020. Available from: https://data.worldbank.org/indicator/SH.DYN.MORT.
36. Mair W, Piper MD, Partridge L. Calories do not explain extension of life span by dietary restriction in Drosophila. PLoS Biol. 2005;3(7):e223. doi:10.1371/journal.pbio.0030223
37. McCay C, Crowell MF, Maynard LA. The effect of retarded growth upon the length of life span and upon the ultimate body size. 1935. Nutrition. 1989;5:155–171.
38. Sohal RS, Weindruch R. Oxidative stress, caloric restriction, and aging. Science. 1996;273(5271):59–63. doi:10.1126/science.273.5271.59
39. The World Bank: International Comparison Program database: World Development Indicators. GDP (current US$) per capita per year; 2010. Available from: http://data.worldbank.org.
40. Duncan GJ, Daly MC, McDonough P, et al. Optimal indicators of socioeconomic status for health research. Am J Public Health. 2002;92(7):1151–1157. doi:10.2105/AJPH.92.7.1151
41. House JS, Kessler RC, Herzog AR. Age, socioeconomic status, and health. Milbank Q. 1990;68:383–411. doi:10.2307/3350111
42. World Health Organization. Urbanization and health. World Health Organization; 2010. Available from: http://www.who.int/bulletin/volumes/88/4/10-010410/en/.
43. Allender S, Foster C, Hutchinson L, et al. Quantification of urbanization in relation to chronic diseases in developing countries: a systematic review. J Urban Health. 2008;85(6):938–951. doi:10.1007/s11524-008-9325-4
44. Zhang X, Nicosia SV, Bai W. Vitamin D receptor is a novel drug target for ovarian cancer treatment. Curr Cancer Drug Targets. 2006;6(3):229–244. doi:10.2174/156800906776842939
45. Brett M. R, Jennifer B. P, Thomas A. S, Brett M. R, Jennifer B. P, Thomas A. S. Epidemiology of ovarian cancer: a review. Cancer Biol Med. 2017;14(1):9. doi:10.20892/j.issn.2095-3941.2016.0084
46. Jordan SJ, Whiteman DC, Purdie DM, et al. Does smoking increase risk of ovarian cancer? A systematic review. Gynecol Oncol. 2006;103(3):1122–1129. doi:10.1016/j.ygyno.2006.08.012
47. The World Health Organization. GHO | by category | obesity (body mass index ≥ 30), age-standardized (%) - Estimates by country. World Health Organization; 2017; Available from: http://apps.who.int/gho/data/view.main.CTRY2450A.
48. UNESCO. Educational attainment, at least completed primary, population 25+ years, female (%), I.f. Statistics, Editor. The World Bank Group; 2020. Available from: http://uis.unesco.org/.
49. United Nations Statistics Division. Composition of macro geographical (continental) regions, geographical sub-regions, and selected economic and other groupings; 2013. Available from: http://unstats.un.org.
50. World Health Organization. WHO regional offices; 2018. Available from: http://www.who.int.
51. The United Nations Educational Scientific and Cultural Organization. UNESCO Regions-Latin America and the Caribbean; 2014. Available from: http://www.unesco.org.
52. The OECD. List of OECD member countries; 2015. Available from: http://www.oecd.org.
53. Asia-Pacific Economic Cooperation. Member Economies-Asia-Pacific Economic Cooperation; 2015. Available from: http://www.apec.org.
54. South Africa Development Community. Southern African Development Community: member States; 2015. Available from: http://www.sadc.int.
55. The World Bank. Arab world data. Available from: http://data.worldbank.org.
56. Asia Cooperation Dialogue. Member countries; 2018. Available from: http://www.acddialogue.com.
57. Arnett DK, Blumenthal RS, Albert MA, et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2019;74(10):e177–e232. doi:10.1016/j.jacc.2019.03.010
58. Dinu M, Pagliai G, Angelino D, et al. Effects of popular diets on anthropometric and cardiometabolic parameters: an umbrella review of meta-analyses of randomized controlled trials. Adv Nutr. 2020;11(4):815–833. doi:10.1093/advances/nmaa006
59. Baltic MZ, Boskovic M. When man met meat: meat in human nutrition from ancient times till today. Procedia Food Sci. 2015;5:6–9. doi:10.1016/j.profoo.2015.09.002
60. Leonard WR. Food for thought: dietary change was a driving force in human evolution. Sci Am. 2003;13:62–71.
61. Leonard WR, Robertson ML, Snodgrass JJ, et al. Metabolic correlates of hominid brain evolution. Comp Biochem Physiol A Mol Integr Physiol. 2003;136(1):5–15. doi:10.1016/S1095-6433(03)00132-6
62. Smil V. Should We Eat Meat?: Evolution and Consequences of Modern Carnivory. John Wiley & Sons; 2013.
63. Psouni E, Janke A, Garwicz M. Impact of carnivory on human development and evolution revealed by a new unifying model of weaning in mammals. PLoS One. 2012;7(4):e32452. doi:10.1371/journal.pone.0032452
64. Henneberg M, Sarafis V, Mathers K. Human adaptations to meat eating. Hum Evol. 1998;13(N3–4):229–234. doi:10.1007/BF02436507
65. Chivers DJ, Hladik CM. Morphology of the gastrointestinal tract in primates: comparisons with other mammals in relation to diet. J Morphol. 1980;166(3):337–386. doi:10.1002/jmor.1051660306
66. Sussman RW. Species-specific dietary patterns in primates and human dietary adaptations. The evolution of human behavior: primate models. Albany: State University of New York Press; 1987: 151–179.
67. Milton K. Primate diets and gut morphology: implications for hominid evolution. Food Evol. 1987;4:93–115.
68. Leonard WR, Robertson ML. Nutritional requirements and human evolution: a bioenergetics model. Am J Hum Biol. 1992;4(2):179–195. doi:10.1002/ajhb.1310040204
69. Rosenfeld DL, Burrow AL. The unified model of vegetarian identity: a conceptual framework for understanding plant-based food choices. Appetite. 2017;112:78–95. doi:10.1016/j.appet.2017.01.017
70. Ehrlich PR. Human Natures: Genes, Cultures, and the Human Prospect. Island Press; 2000.
71. Bulliet RW. Hunters, Herders, and Hamburgers: The Past and Future of Human-Animal Relationships. Columbia University Press; 2005.
72. Twigg J. Vegetarianism and the meanings of meat. Sociol Food Eating. 1983;5:18–30.
73. Salim Y. Components of heart healthy diet may differ from what was previously thought, in European Society for Cardiology. Munich; 2018.
74. Mente A, Yusuf S. Evolving evidence about diet and health. Lancet Public Health. 2018;3(9):e408–e409. doi:10.1016/S2468-2667(18)30160-9
75. Snowdon DA, Phillips RL, Fraser GE. Meat consumption and fatal ischemic heart disease. Prev Med. 1984;13(5):490–500. doi:10.1016/0091-7435(84)90017-3
76. You W, Henneberg M. Meat in modern diet, just as bad as sugar, correlates with worldwide obesity: an ecological analysis. J Nutr Food Sci. 2017;6(517):4.
77. Grantham JP, Staub K, Rühli FJ, et al. Modern diet and metabolic variance–a recipe for disaster? Nutr J. 2014;13:15. doi:10.1186/1475-2891-13-15
78. Henneberg M, Rühli FJ, Gruber P, et al. Alanine transaminase individual variation is a better marker than socio-cultural factors for body mass increase in healthy males. Food Nutr Sci. 2011;2(10):1054–1062. doi:10.4236/fns.2011.210141
79. Talaei M, Wang YL, Yuan JM, et al. Meat, dietary heme iron, and risk of type 2 diabetes mellitus: the Singapore Chinese Health Study. Am J Epidemiol. 2017;186(7):824–833. doi:10.1093/aje/kwx156
80. USDA. All about the protein foods group; 2015. Available from: https://www.choosemyplate.gov/protein-foods.
81. United States Department of Agriculture. Choose my plate; 2018.
82. Government of Victoria. Better health channel- fruit and vegetables; 2014.
83. Nutrition Australia. The healthy living pyramid; 2018. Available from: http://www.nutritionaustralia.org.
84. Rogerson D. Vegan diets: practical advice for athletes and exercisers. J Int Soc Sports Nutr. 2017;14(1):36. doi:10.1186/s12970-017-0192-9
85. Marsh K, Zeuschner C, Saunders A. Health implications of a vegetarian diet: a review. Am J Lifestyle Med. 2012;6(3):250–267. doi:10.1177/1559827611425762
86. Kwok CS, Umar S, Myint PK, et al. Vegetarian diet, Seventh Day Adventists and risk of cardiovascular mortality: a systematic review and meta-analysis. Int J Cardiol. 2014;176(3):680–686. doi:10.1016/j.ijcard.2014.07.080
87. Phillips RL. Role of life-style and dietary habits in risk of cancer among seventh-day adventists. Cancer Res. 1975;35(11 Part 2):3513–3522.
88. Butler TL, Fraser GE, Beeson WL, et al. Cohort profile: the Adventist health study-2 (AHS-2). Int J Epidemiol. 2008;37(2):260–265. doi:10.1093/ije/dym165
89. You W, Henneberg M, Tovée MJ. Relaxed natural selection contributes to global obesity increase more in males than in females due to more environmental modifications in female body mass. PLoS One. 2018;13(7):e0199594. doi:10.1371/journal.pone.0199594
90. You W, Henneberg M. Cancer incidence increasing globally: the role of relaxed natural selection. Evol Appl. 2017;00::1–13.
91. You W-P, Henneberg M. Type 1 diabetes prevalence increasing globally and regionally: the role of natural selection and life expectancy at birth. BMJ Open Diabetes Res Care. 2016;4(1):e000161. doi:10.1136/bmjdrc-2015-000161
92. Budnik A, Henneberg M, Rosenfeld CS. Worldwide increase of obesity is related to the reduced opportunity for natural selection. PLoS One. 2017;12(1):e0170098. doi:10.1371/journal.pone.0170098
93. Staub K, Henneberg M, Galassi FM, et al. Increasing variability of body mass and health correlates in Swiss conscripts, a possible role of relaxed natural selection? Evol Med Public Health. 2018;2018:116–126. doi:10.1093/emph/eoy012
94. Beardsworth A, Keil E. Vegetarianism, veganism, and meat avoidance: recent trends and findings. Br Food J. 1991;93(4):19–24. doi:10.1108/00070709110135231
95. Harcombe Z, Baker JS, Cooper SM, et al. Evidence from randomised controlled trials did not support the introduction of dietary fat guidelines in 1977 and 1983: a systematic review and meta-analysis. Open Heart. 2015;2(1):e000196. doi:10.1136/openhrt-2014-000196
96. Mozaffarian D. The great fat debate: taking the focus off of saturated fat. J Am Diet Assoc. 2011;111(5):665–666. doi:10.1016/j.jada.2011.03.030
97. Willett WC. The great fat debate: total fat and health. J Am Diet Assoc. 2011;111(5):662.
98. DuBroff R, de Lorgeril M. Fat or fiction: the diet-heart hypothesis. BMJ Evid Based Med. 2021;26(1):3–7. doi:10.1136/bmjebm-2019-111180
99. Sacks FM, Lichtenstein AH, Wu JHY, et al. Dietary fats and cardiovascular disease: a presidential advisory from the American Heart Association. Circulation. 2017;136(3):e1–e23. doi:10.1161/CIR.0000000000000510
100. Campbell WW. Animal-Based and Plant-Based Protein-Rich Foods and Cardiovascular Health: A Complex Conundrum. Oxford University Press; 2019:8–9.
101. O’Keefe JH
102. Sands DC, Morris CE, Dratz EA, et al. Elevating optimal human nutrition to a central goal of plant breeding and production of plant-based foods. Plant Sci. 2009;177(5):377–389. doi:10.1016/j.plantsci.2009.07.011
103. Michael S. The Borderlands of Science, Where Sense Meets Nonsense. Oxford University Press; 2003:250.
104. Vernooij RW, Zeraatkar D, Han MA, et al. Patterns of red and processed meat consumption and risk for cardiometabolic and cancer outcomes: a systematic review and meta-analysis of cohort studies. Ann Intern Med. 2019;171(10):732–741. doi:10.7326/M19-1583
105. Zeraatkar D, Han MA, Guyatt GH, et al. Red and processed meat consumption and risk for all-cause mortality and cardiometabolic outcomes: a systematic review and meta-analysis of cohort studies. Ann Intern Med. 2019;171(10):703–710. doi:10.7326/M19-0655
106. Zeraatkar D, Johnston BC, Bartoszko J, et al. Effect of lower versus higher red meat intake on cardiometabolic and cancer outcomes: a systematic review of randomized trials. Ann Intern Med. 2019;171(10):721–731. doi:10.7326/M19-0622
107. Han MA, Zeraatkar D, Guyatt GH, et al. Reduction of red and processed meat intake and cancer mortality and incidence: a systematic review and meta-analysis of cohort studies. Ann Intern Med. 2019;171(10):711–720. doi:10.7326/M19-0699
108. Valli C, Rabassa M, Johnston BC, et al. Health-related values and preferences regarding meat consumption: a mixed-methods systematic review. Ann Intern Med. 2019;171(10):742–755. doi:10.7326/M19-1326
109. Johnston BC, Zeraatkar D, Han MA, et al. Unprocessed red meat and processed meat consumption: dietary guideline recommendations from the Nutritional Recommendations (NutriRECS) Consortium. Ann Intern Med. 2019;171(10):756–764. doi:10.7326/M19-1621
110. O’Connor LE, Kim JE, Campbell WW. Total red meat intake of≥ 0.5 servings/d does not negatively influence cardiovascular disease risk factors: a systemically searched meta-analysis of randomized controlled trials. Am J Clin Nutr. 2017;105(1):57–69. doi:10.3945/ajcn.116.142521
111. The FAO. Products from slaughtered animals; 2018.
112. Tantamango-Bartley Y, Knutsen SF, Knutsen R, et al. Are strict vegetarians protected against prostate cancer? Am J Clin Nutr. 2015;103(1):153–160. doi:10.3945/ajcn.114.106450
113. Kazerouni N, Sinha R, Hsu CH, et al. Analysis of 200 food items for benzo [a] pyrene and estimation of its intake in an epidemiologic study. Food Chem Toxicol. 2001;39(5):423–436. doi:10.1016/S0278-6915(00)00158-7
114. Knize M, Sinha R, Brown ED, et al. Heterocyclic amine content in restaurant-cooked hamburgers, steaks, ribs, and chicken. J Agric Food Chem. 1998;46(11):4648–4651. doi:10.1021/jf980639a
115. Knize M, Sinha R, Rothman N, et al. Heterocyclic amine content in fast-food meat products. Food Chem Toxicol. 1995;33(7):545–551. doi:10.1016/0278-6915(95)00025-W
116. Knize M, Sinha R, Salmon CP, et al. Formation of heterocyclic amine mutagens/carcinogens during home and commercial cooking of muscle foods. J Muscle Foods. 1996;7(3):271–279. doi:10.1111/j.1745-4573.1996.tb00603.x
117. Sinha R, Gustafson DR, Kulldorff M, et al. 2-Amino-1-methyl-6-phenylimidazo [4, 5-b] pyridine, a carcinogen in high-temperature-cooked meat, and breast cancer risk. J Natl Cancer Inst. 2000;92(16):1352–1354. doi:10.1093/jnci/92.16.1352
118. Sinha R, Knize MG, Salmon CP, et al. Heterocyclic amine content of pork products cooked by different methods and to varying degrees of doneness. Food Chem Toxicol. 1998;36(4):289–297. doi:10.1016/S0278-6915(97)00159-2
119. National Research Council (US) Committee on Diet, N., and Cancer. 8 Food Additives, Contaminants, Carcinogens, and Mutagens, in Diet, Nutrition, and Cancer: Directions for Research. Washington (DC): National Academies Press (US); 1983.
120. Mealing NM, Banks E, Jorm LR, et al. Investigation of relative risk estimates from studies of the same population with contrasting response rates and designs. BMC Med Res Methodol. 2010;10(1):26. doi:10.1186/1471-2288-10-26
121. Horner NK, Patterson RE, Neuhouser ML, et al. Participant characteristics associated with errors in self-reported energy intake from the Women’s Health Initiative food-frequency questionnaire. Am J Clin Nutr. 2002;76(4):766–773. doi:10.1093/ajcn/76.4.766
122. Miller TM, Abdel-Maksoud MF, Crane LA, et al. Effects of social approval bias on self-reported fruit and vegetable consumption: a randomized controlled trial. Nutr J. 2008;7(1):18. doi:10.1186/1475-2891-7-18
123. Morgenstern H. Ecologic studies in epidemiology: concepts, principles, and methods. Annu Rev Public Health. 1995;16(1):61–81. doi:10.1146/annurev.pu.16.050195.000425
124. Siervo M, Montagnese C, Mathers JC, et al. Sugar consumption and global prevalence of obesity and hypertension: an ecological analysis. Public Health Nutr. 2014;17(3):587–596. doi:10.1017/S1368980013000141
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.