Back to Journals » ClinicoEconomics and Outcomes Research » Volume 18
Total Laboratory Automation for Microbiology Activities: An HTA Analysis in an Italian Laboratory Setting
Authors Foglia E ![]() , Garagiola E, Ferrario L
, Garagiola E, Ferrario L ![]() , Adorisio E, Gagliardi G, Lenoci FD
, Adorisio E, Gagliardi G, Lenoci FD
Received 20 January 2026
Accepted for publication 27 May 2026
Published 15 June 2026 Volume 2026:18 597703
DOI https://doi.org/10.2147/CEOR.S597703
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Giorgio Colombo
Emanuela Foglia,1 Elisabetta Garagiola,1 Lucrezia Ferrario,1 Edmondo Adorisio,2 Giuseppe Gagliardi,2 Francesca Domenica Lenoci2
1HD Laboratory – Healthcare Datascience LAB, Carlo Cattaneo – LIUC University, Castellanza, VA, Italy; 2Di Venere Carbonara Hospital, Bari, BA, Italy
Correspondence: Lucrezia Ferrario, HD Laboratory – Healthcare Datascience LAB, Carlo Cattaneo – LIUC University, Corso Matteotti, 22, Castellanza, VA, 21053, Italy, Tel +39 033 1572504, Email [email protected]
Objective: Microbiology laboratories face increasing challenges related to rising sample volumes, workforce constraints, and the need for improved diagnostic accuracy and efficiency. Total Laboratory Automation (TLA) has emerged as a transformative solution to optimize workflows, enhance safety, and improve resource utilization. This study focuses on urine cultures and the follow-up of positive blood cultures and evaluates the impact of TLA implementation in a microbiology laboratory, assessing efficiency, economic sustainability, and healthcare professionals’ perceptions.
Methods: A Health Technology Assessment (HTA) approach was employed, integrating real-life data from a single-center hospital laboratory in Italy before and after TLA implementation. Key performance indicators (KPIs) were defined through a literature review and expert consensus. Real-life data were collected over two time periods: the pre-automation phase (manual workflow) and post-automation phase (TLA) for urine culture and positive blood culture. The economic and organizational impact was assessed by quantifying human resource efforts, while a qualitative survey captured healthcare professionals’ perceptions regarding automation.
Results: TLA significantly reduced sample processing times, with a 67% decrease in check-in time and a significant reduction in inoculation (up to 100%) and plate reading (− 69%) times, respectively. Economic analysis indicated a 67% reduction in costs for personnel time required to process urine cultures and perform initial workups of positive blood cultures on annual basis with consequent organizational benefits, in terms of time spent in sample processing (− 71%). Healthcare professionals reported improved safety and reduced workload, making them more inclined to adopt TLA, perceived as useful and capable to offer high-quality and demonstrable results.
Conclusion: Findings emphasize TLA potentialities in the management of microbiology procedures overall improvement, empowering the laboratory efficiency and organizational capacity, allowing better investment of the human resources involved.
Keywords: TLA, economic sustainability, organizational assessment, laboratory workflow optimization, automated diagnostic systems
Introduction
Diagnostic tests play a key role in healthcare, with approximately 70% of medical decisions relying on laboratory results,1 particularly guiding and optimizing the management of therapeutic interventions. Within this context, microbiology laboratories are pivotal in detecting and identifying infectious agents, directly influencing patient management and infection control strategies.2 However, these laboratories are facing increasing operational challenges, including rising sample volumes, constrained budgets, and workforce shortages, thus requiring an overall workflow optimization to maintain productivity, while ensuring analytical quality.3
Clinical microbiology has depended on manual techniques, which, despite their reliability, are labor-intensive and increasingly unsustainable in high-throughput settings. The consolidation of diagnostic testing into centralized facilities has further exacerbated the need for efficiency. While laboratory automation has revolutionized areas such as clinical chemistry and hematology, its adoption in microbiology remains relatively recent.4 Total Laboratory Automation (TLA), defined as “the automation of the diagnostic workflow, which includes all steps from inoculation to the final outcome”,5 represents a significant advancement in microbiology setting, with the capability to automate and standardize a wide range of processes, including specimen processing, plate streaking, incubation, and digital visualization.6 In general terms, TLA minimizes manual intervention, reduces human error, and enhances turnaround times, with studies reporting up to a 87% reduction in processing errors and substantial organizational time savings.7–12 Beyond efficiency gains, automation enhances results standardization and quality control, with an overall optimization of the patients’ clinical pathways, minimizing reporting errors and misdiagnosis,13–15 thus also supporting timely therapeutic interventions.12
While evidence supporting TLA benefits is increasing, decisions regarding the adoption of such technologies cannot rely solely on clinical or technical performance indicators. Limited evidence is available concerning the practical implications of TLA implementation in Italian microbiology laboratories, demonstrating both the real-life added value in comparison to the manual methods, and the consequent economic and organizational sustainability. Additionally, understanding the perceptions of healthcare professionals towards these innovations is crucial for successful adoption, implementation and integration into routine practice.16,17
Contemporary Health Technology Assessment (HTA) frameworks emphasize the importance of a multidimensional evaluation approach, incorporating not only effectiveness and efficiency, but also organizational, economic, social, and ethical dimensions. This broader perspective is particularly relevant for complex healthcare technologies such as TLA, which require substantial organizational changes, workflow redesign, and significant initial investments. In such contexts, focusing exclusively on laboratory performance metrics may underestimate the overall value and implications of technology adoption. Instead, evaluating non-clinical domains—such as resource utilization, staff workload, safety, and user acceptance—becomes essential to fully capture the impact of automation on healthcare delivery. Based on these considerations, adopting an HTA approach allows for a comprehensive assessment of TLA implementation, supporting evidence-based decision-making and facilitating the alignment of technological innovation with healthcare system needs, particularly within the Italian context where resource allocation and organizational sustainability are key priorities.
The coverage of the above knowledge gaps in microbiology setting is particularly relevant, as rapid turnaround times are critical for the management of life-threatening infections, requiring continuous process optimization. Based on these premises, the present study aims to address these gaps by evaluating the real-world impact of TLA implementation in a single-center Italian setting, focusing on efficiency, safety, organizational and economic sustainability.
The analysis specifically focuses on urine cultures and the initial workup of positive blood cultures, selected for their high diagnostic relevance and frequency in microbiological testing. Urine cultures represent the most processed samples in microbiology laboratories and are essential for diagnosing urinary tract infections—one of the main drivers of antibiotic prescriptions.18 In contrast, blood cultures are critical for identifying bloodstream infections and sepsis, where prompt diagnosis can significantly influence patient outcomes.19
Due to their clinical significance and high testing volume, these sample types provide a robust basis for evaluating the impact of TLA.
Accordingly, the study addresses the following research questions.
- Research Question 1 - RQ1: “Could the implementation of laboratory automation systems in microbiology be a feasible and sustainable solution from efficiency, economic, organizational and safety standpoints, thereby enhancing the overall effectiveness of microbiology laboratory services?”
- Research Question 2 - RQ2: “What are the perceptions of healthcare professionals (in terms of perceived effectiveness, safety, social, equity and organizational issues), regarding the use of automated technologies in microbiology laboratory settings, and what are the key factors influencing their intention to adopt these innovative solutions within Italian clinical practice?”
By addressing these research questions, the study aims to provide a comprehensive and multidimensional understanding of TLA systems and their potential to improve multidisciplinary performance areas, as well as the economic and organizational sustainability of microbiology laboratories. Through this process, the study conducted offers valuable insights for both policymakers and healthcare professionals, ultimately supporting decision-makers in the adoption of such innovative technologies.
Materials and Methods
To achieve the study objectives, an HTA was performed using the AdHoPHTA framework as proposed by Sampietro-Colom et al20 This framework provided a structured approach for integrating diverse sources of evidence and reliable information to support hospital-based decision-making process regarding technology adoption and investment. The assessment encompassed both clinical and non-clinical dimensions, employing a combination of qualitative and quantitative methodologies to ensure a comprehensive analysis.
For the implementation of the HTA dimensions, a multi-method approach was employed. This methodology, widely recognized in healthcare services research, integrates both qualitative and quantitative techniques to enable a more comprehensive understanding of complex healthcare interventions.21,22
The study followed several phases. It began with a narrative literature review,23 which identified the key indicators used to assess performance in microbiology. These indicators were then organized into relevant categories and used to create a performance measurement dashboard aligned with the study’s objectives. After the validation of this dashboard, the study moved on to testing these indicators in a real-world setting—the microbiology laboratory at Di Venere Carbonara Hospital in Bari. This hospital was ideal for evaluating the current situation (“AS IS”) because it was transitioning from manual systems to full laboratory automation in 2023–2024.
Using the KPIs identified from the literature, the study assessed how automation affected efficiency, cost-effectiveness, and organizational sustainability in the microbiology laboratory at Di Venere Hospital—addressing Research Question 1 (RQ1). To explore Research Question 2 (RQ2), qualitative data was collected to understand how healthcare professionals perceived and accepted the new technology. In line with Health Technology Assessment (HTA) principles, feedback from staff involved in the transition from manual to automated systems was gathered between April and June 2024. The analysis followed the AdHopHTA model, covering areas such as clinical effectiveness, safety, financial impact, organizational changes, ethical and social aspects, and patient perspectives.
Figure 1 synthesizes the study design.
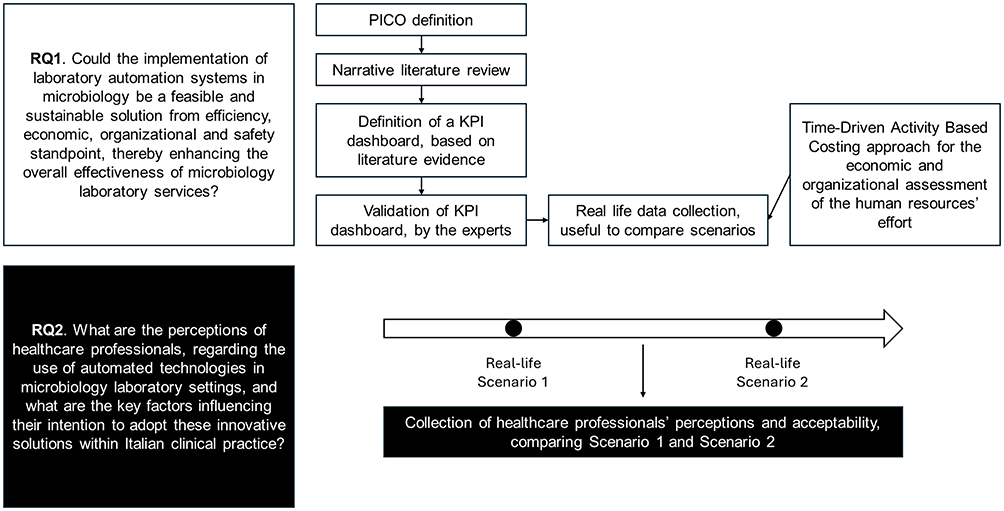 |
Figure 1 Study Design. |
The study compared the following two operational scenarios (Figure 2).
- Scenario 1 – Manual Workflow: the microbiology laboratory operated 6 hours per day, 6 days per week, processing an average of about 18,000 urine samples and about 5400 blood cultures per year coming from the Di Venere Carbonara Hospital. The total test volume processed was about 46,000 per year. The laboratory was staffed by one clinical manager and two technicians. Urine samples were screened using a light scattering method, while positive blood cultures were processed using conventional techniques. The workflow included manual plate streaking, standard incubation systems, biochemical identification (ID) methods, and automated antimicrobial susceptibility testing (AST) instruments. No middleware system, directly connected to the LIS, was in place to integrate these processes and instruments.
- Scenario 2 - Automated Workflow: the microbiology laboratory operated 12 hours per day, 7 days per week, processing an average of 80,400 urine cultures and about 20,000 blood cultures vials per year coming from 6 Hospitals and 32 spokes. The total test volume processed was 365,000 per year. The laboratory was staffed by seven clinical managers and ten technicians. The workflow was supported by a comprehensive automation system, including full middleware integration, automated plate streaking using magnetic beads and calibrated pipette inoculation, automated incubation, and digital plate reading. Additional automation included colony picking and MALDI-TOF sample preparation. Microbial identification was performed using a middleware-connected MALDI-TOF system, and antimicrobial susceptibility testing (AST) was conducted using a middleware-connected automated instrument.
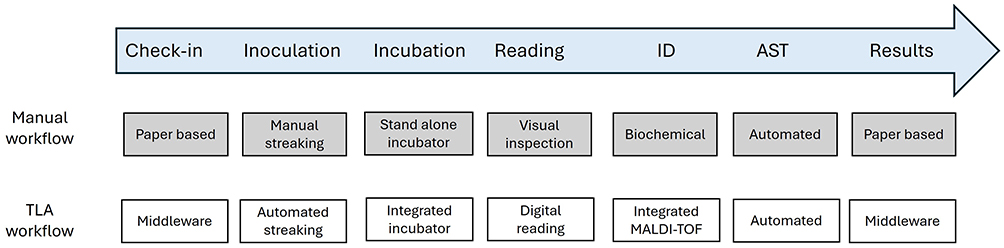 |
Figure 2 Comparison of manual and automated microbiology workflows. Manual and non‑integrated steps are distinguished from fully automated end to end and middleware‑integrated steps along the diagnostic process. |
The Creation of the Key Performance Indicators Dashboard
The narrative literature review started with the identification of both the PICO (Population, Intervention, Comparator, Outcome) approach and the specific search strategy. The following PICO was used in the literature review process: P = “patient/population” = microbiological laboratory activities, focusing on blood and urine samples; I = “intervention” = presence of automated technologies, in terms of streaking, incubation, digital reading (assisted interpretation), colony picking and MALDI preparation, automatic ID method (biochemical/MALDI) and automatic AST instrument; C = “Comparator” = absence of automated technologies, in terms of manual streaking, conventional incubation system, automatic ID method (biochemical) and automatic AST instrument; O = “outcome” = primary outcomes = speed, quality, and accuracy of microbiological laboratory’s activities, timing of microbiological laboratory’s activities.
After the definition of the PICO, guiding the literature review, principal scientific databases were searched: PubMed, Embase and Cochrane Library. The main search terms used for the development of narrative literature review were the followings, thus also included synonyms or periphrasis: “total laboratory automation” or “laboratory automation” or “TLA” or “automation”, “microbiology” or “microbiology laboratory”, “TAT” or “turnaround time”, “TTR” or “time to report”, “inoculation”, “blood culture” and “urine culture”.
The narrative literature review was useful for the definition of a key-performance indicators (KPIs) dashboard, thus identifying the most important measurement aspects related to the introduction of innovative technologies in the microbiology laboratory. Based on the above, out of 552 records screened, only 7 papers were eligible to the present evaluation, for the creation of the performance tool, thus proposing a set of KPIs, concerning efficiency, and organizational factors, all related to the introduction of innovative automated systems.
The KPI dashboard involved six experts (lab healthcare professionals, managers from technology manufacturing companies and academics specialized in healthcare and performance measurement) in a brainstorming session based on a Delphi method24 to identify key priorities for assessing technology performance in a microbiology laboratory setting. Initially, the experts engaged in a brainstorming session to define the main features highlighted in the literature review, leading to the development of a preliminary performance measurement tool. This draft was then circulated among the experts, and a two-round Delphi method process was conducted, allowing the group to reach a strong consensus, thus validating the KPI to be measured.24
The specific dashboard of KPIs, useful to define the added value of TLA with respect to manual methods, is reported in Table 1.
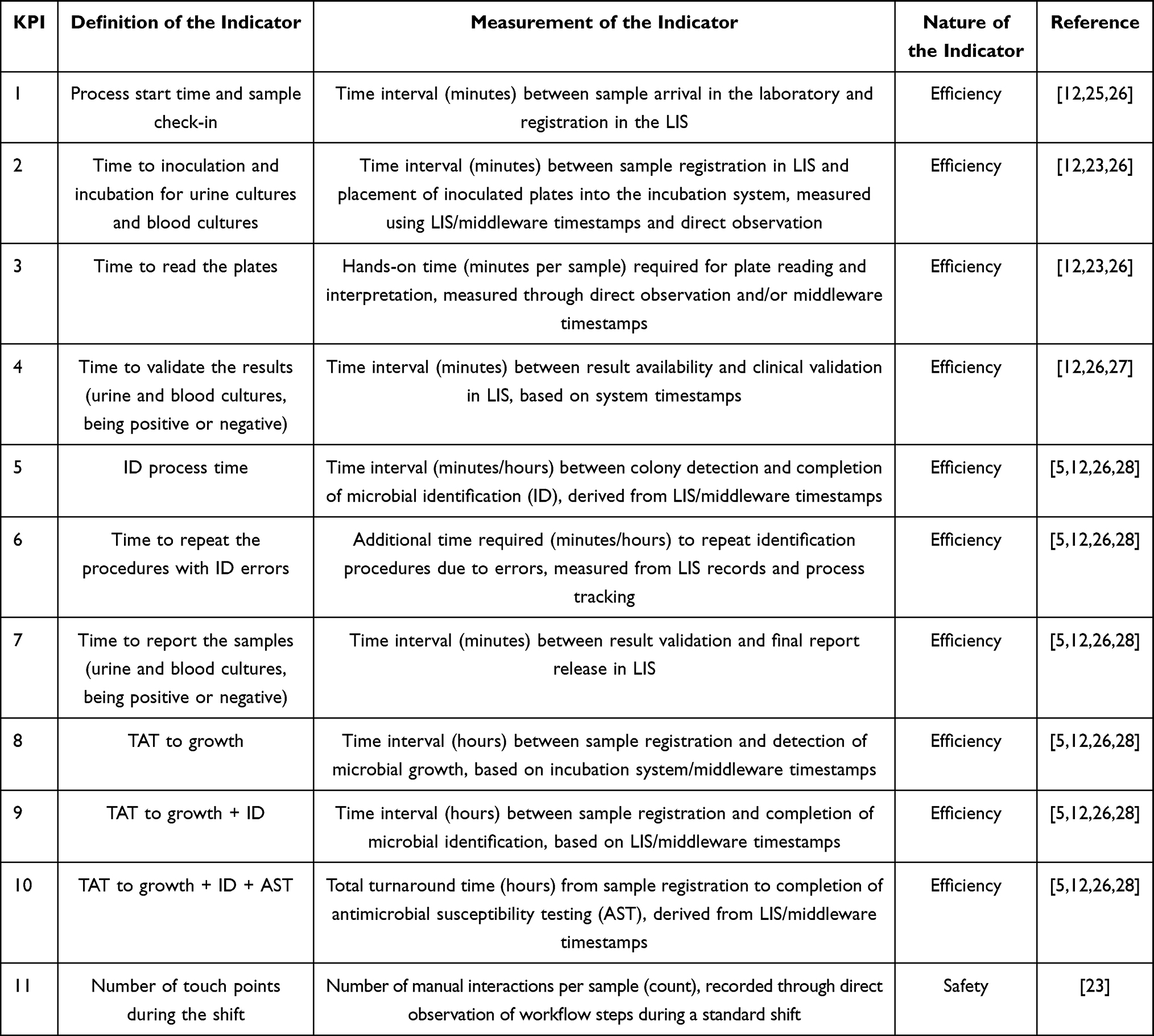 |
Table 1 KPI Dashboard |
Real-Life Data Collection
Anonymized and aggregated data were retrospectively extracted from the Laboratory Information System (LIS) and middleware to assess the real-world performance of innovative technologies in routine clinical practice through predefined KPIs. Time-based indicators were operationalized using standardized start and end timestamps derived from these systems, ensuring consistency and reproducibility across measurements.
All urine cultures and positive blood culture samples processed during the study periods were included in the analysis. Samples with incomplete or inconsistent timestamp data in the LIS or middleware systems were excluded. Additionally, records with missing key process variables required for KPI calculation were not considered in the final analysis. Data completeness was assessed prior to analysis. Missing observations were excluded on a case-by-case basis. Outliers were identified through data consistency checks and inspection of extreme values in process times; implausible values (eg, negative or excessively high time intervals due to system errors) were removed to ensure data reliability.
The analysis was stratified by timeframes corresponding to technological transitions within the hospital, comparing two scenarios: absence (Scenario 1) and presence (Scenario 2) of Total Laboratory Automation (TLA), under varying workload conditions. Scenario 1 reflects routine clinical practice during April–May 2023, prior to the implementation of automated solutions and a single hospital samples workload. Scenario 2 corresponds to May–June 2024, representing a period in which the technologies had been fully implemented, and the learning curve was stabilized when the workload changed with the acquisition of samples from 6 hospitals and 32 spokes consequent to territorial reorganization.
All analyses were conducted at the sample level, ensuring consistency between operational measurements and statistical comparisons.
The data collection was approved by LIUC University Research Ethical Committee (protocol number R13-23 dated 7th July 2023).
Economic and Organisational Impact Assessment
The economic and organizational impact assessment focused exclusively on the costs associated with human resources involved in each phase of the microbiology workflow, specifically in the management of both urine and blood cultures. This approach was justified by the consistency in both the type and quantity of medical devices and consumables used across the two scenarios, thereby minimizing variability in material-related costs.
It is acknowledged that while this analysis excluded capital expenditure, the implementation of automated solutions would require an initial investment. The magnitude of such investment is highly variable and depends on institutional procurement strategies and tendering procedures. Therefore, capital costs were not included in the comparative analysis to preserve generalizability across different healthcare settings, given that structural barriers could influence the investment.
The analysis concentrated solely on human resource utilization, reflecting the differences in process phases between the manual (Scenario 1) and automated (Scenario 2) workflows. A Time-Driven Activity-Based Costing (TDABC) methodology was applied,29,30 enabling a detailed assessment of labor costs. Time spent by clinicians and technicians on each activity was quantified in minutes and monetized based on the Italian National Labor Contracts for each professional category (on average equal to € 65,000 for a clinician and € 32,000 for a laboratory technician).31 This allowed for the calculation of a cost-per-minute rate for each healthcare professional, which was then used to allocate a cost to each activity based on the actual time invested.
Hands-on time was measured through direct observation of laboratory activities and validated using LIS and middleware timestamps when available. For each process phase, the time actively spent by healthcare professionals (clinicians or technicians) was recorded in minutes per sample. These measurements were standardized across repeated observations and averaged to obtain representative time estimates for each activity within both scenarios. The cost per each scenario was calculated considering clinician or technician cost per minutes (average 1.1€ and 0.38€, respectively) and specific roles in the process (eg manual step operated by technician and validation, reporting by clinician).
In Scenario 1, for managing urine cultures, a light scattering test was used to screen for positive or negative samples. If positive, the sample proceeded to manual biochemical identification and automated susceptibility testing. If negative: the result is assessed, validated by a clinician, and reported without a middleware connection.
However, in Scenario 2, the urine sample is processed directly by the BD Kiestra™ TLA solution with BD Synapsys Middleware, which automates all phases up to the digital reading phase. If positive, it proceeds to automated sample preparation for MALDI identification and then transferred to an automated instrument for sample preparation for susceptibility testing on BD Phoenix™ M50. If the digital growth inspection is negative, it’s validated by clinician and reported to the LIS.
Focusing on blood cultures sample, in Scenario 1, the negative bottle was discarded from the incubator by technician, validated by a clinician, and reported to LIS. Positive bottle was manually inoculated, streaked on plates, and after colony growth, manually processed for biochemical identification and processed for automated susceptibility testing. Results were validated and reported to LIS by Clinician.
However, in Scenario 2, negative bottle is discarded from the incubator by technician and managed by the clinician through the Synapsys Middleware and directly reported as negative to the LIS. An aliquot of the positive blood culture is dispensed manually on plates and are then loaded in the automated system BD Kietra™ where streaking, incubation and digital reading takes place. The system also handles the preparation of the MALDI target. Identification is performed by MALDI TOF and susceptibility testing is performed by BD Phoenix™ M50, which is not physically connected to the TLA.
Hands-on time recorded in Scenario 1 was used to estimate the annual hands-on time and related FTE costs the lab would incur if the Scenario 2 workload were processed without TLA. The aim was to evaluate the economic and organizational impact of TLA implementation in terms of time and cost savings that could be reinvested.
Qualitative Questionnaire to Collect Healthcare Professionals’ Perceptions
A qualitative questionnaire was developed to evaluate healthcare professionals’ perceptions of Total Laboratory Automation (TLA). The questionnaire was based on a seven-point Likert scale ranging from –3 (strong negative impact) to +3 (strong positive impact), including a neutral midpoint (0), in line with the approach proposed in the literature evidence by Mitton et al.32
The questionnaire items were derived from established HTA framework,20 and covered multiple domains.
Additionally, the questionnaire assessed the intention to use TLA, recognizing that automation is often perceived as a disruptive innovation. Resistance to change among healthcare professionals can hinder adoption, despite potential efficiency gains. To explore this, the analysis incorporated variables from the Technology Acceptance Model 2 (TAM2), including perceived usefulness, ease of use, image, output quality, job relevance, and results demonstrability.33–38
The questionnaire (whose full version is available as Supplementary Material 1), was administered to selected healthcare professionals and designed to capture comparative perceptions between the pre-automation phase (Scenario 1) and the post-automation phase (Scenario 2).
Statistical Analysis
Continuous variables were expressed as mean ± standard deviation (SD). Prior to inferential analysis, data were assessed for normality, linearity, and homoscedasticity using graphical methods and statistical tests.
Comparisons between the two scenarios (manual vs automated workflow) were performed to assess differences across efficiency, safety, organizational indicators, and HTA-related dimensions. For normally distributed variables, independent samples t-tests were applied. When distributional assumptions were not met, non-parametric alternatives (Mann–Whitney U-test) were considered. Results were structured according to the AdHopHTA framework, and mean values were calculated for each domain.
To explore factors influencing the acceptance and intended use of Total Laboratory Automation (TLA), a linear regression analysis based on the Technology Acceptance Model 2 (TAM2) was conducted. Independent variables included perceived usefulness, perceived ease of use, image, job relevance, output quality, and results demonstrability. A second model included the moderating effect of voluntary use on perceived usefulness.
Model performance was assessed using the adjusted R2, reflecting the proportion of variance explained. Given the limited sample size, regression results should be interpreted as exploratory.
Statistical significance was set at p < 0.05. All analyses were performed using IBM SPSS Statistics version 27.0.
In addition, a sensitivity analysis based on a Bayesian approach was performed to assess the robustness of the economic and organizational results. Bayesian methods provide a comprehensive framework for statistical inference and decision-making by incorporating variability in key parameters. In this study, Gamma distributions were assigned to time-related variables (hands-on time per sample) and corresponding labor costs, reflecting their positive and right-skewed nature. This approach allowed modeling uncertainty around the estimated effort required by healthcare professionals in both scenarios. The analysis estimated the probability that the average cost and time associated with the automated scenario (Scenario 2) were lower than those observed in the manual workflow (Scenario 1). This probabilistic comparison enabled a more robust assessment of the economic and organizational advantages of TLA implementation.
Results
Performance Measurement in the Microbiology Laboratory Setting
The assessment of KPIs within the hospital involved is shown in Table 2.
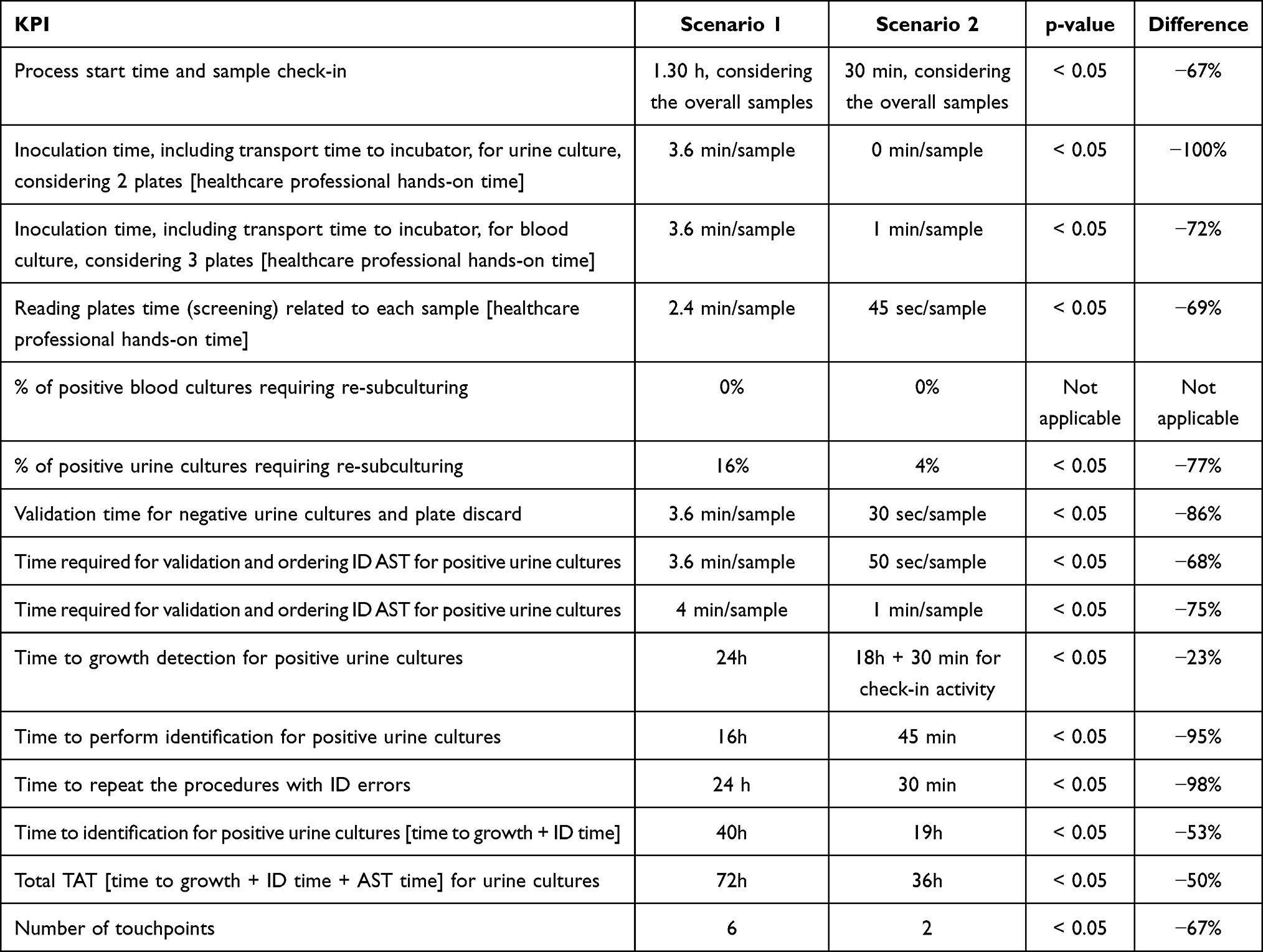 |
Table 2 KPI Measurement |
Based on real-life data collection and focusing on the specific difference between Scenario 1 and Scenario 2, TLA completely eliminates the inoculation hands-on time for urine cultures and reduces the time required for this activity by 72% for the initial work-up (plate inoculation) of positive blood cultures (p-value > 0.05), In addition, Scenario 2 is related to fewer minutes per sample spent to read the plates (2.4 vs 0.75 minutes; −69% with a p-value <0.05). Focusing on urine cultures, thanks to the presence of the middleware the time spent reading the plates (−69%) and the time to validate the results decrease by 86% for samples tested negative, and by 68% for samples tested positive, thus requiring an ID/AST follow-up. The same trend emerged for positive blood cultures, with a reduction equal to 75% with respect to the manual scenario. Time to Identification and Total TAT decrease by 53% and 50% respectively. Concerning the safety profile, Scenario 2 is also characterized by fewer plate touchpoints (p-value < 0.005), resulting in a reduced number of instances in which healthcare professionals need to handle plates that support the growth of potentially pathogenic organisms.
Economic and Organizational Impact
Table 3 depicts a detailed breakdown of process phases, revealing a substantial reduction in hands-on time required per sample in the automated scenario. For negative urine cultures, the overall process time decreased from 15.6 to 2.75 minutes (–82%), translating into a cost averted of 79%. For positive urine cultures, process time was cut by 66%, with a corresponding cost averted of 64%. Similar trends were observed for blood cultures: while negative samples showed a modest 12% hands on cost averted, positive samples yielded a significant 53% decrease in associated personnel costs.
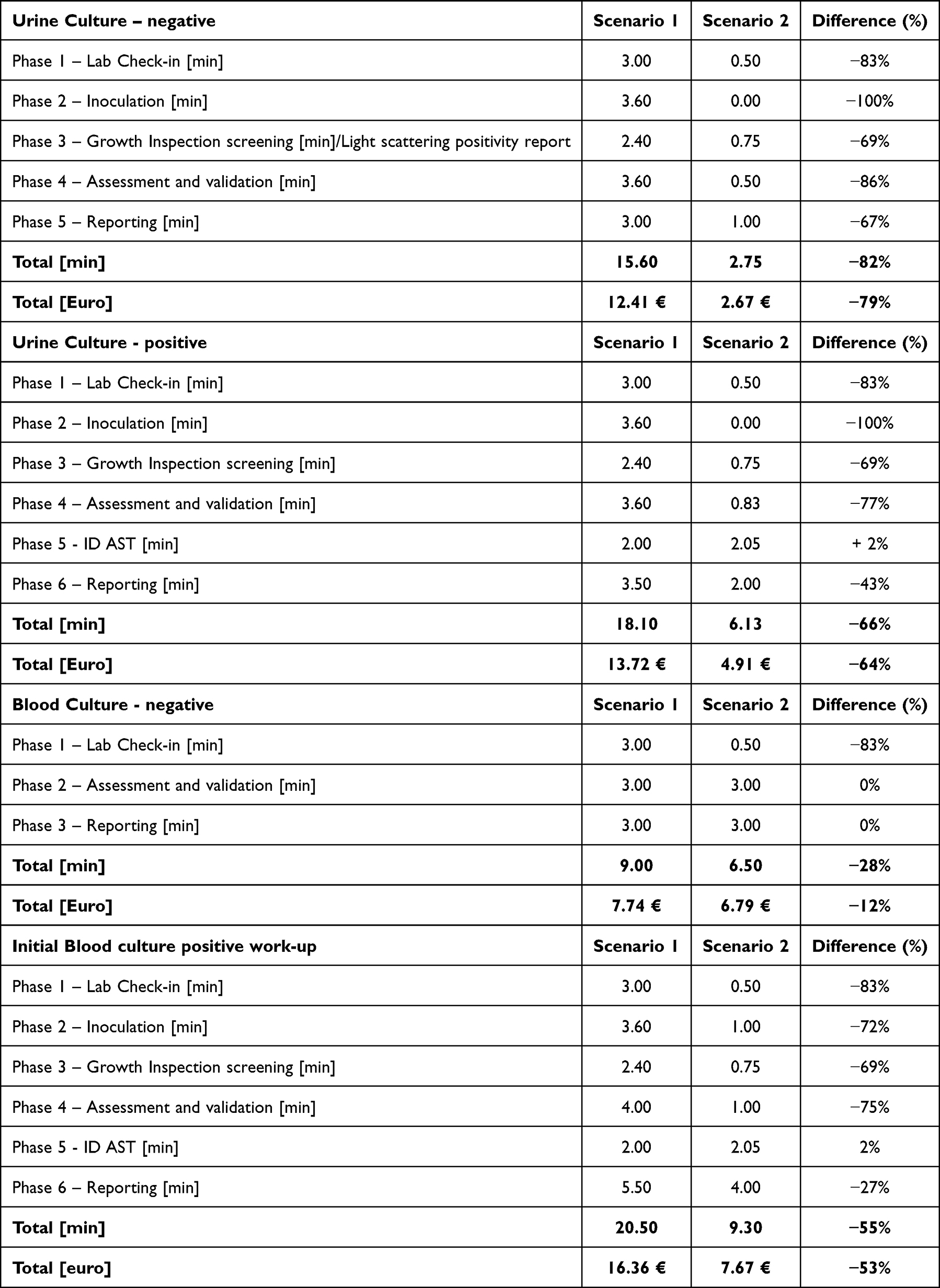 |
Table 3 Organizational Effort in Managing Urine and Blood Cultures |
The probabilistic analysis confirmed that the automated scenario (Scenario 2) was consistently associated with lower hands-on time compared to the manual workflow (Scenario 1). In particular, the probability that TLA required less time for the management of both urine and blood cultures—regardless of whether samples were positive or negative—was equal to 100%. These findings, illustrated in Figures 3 and 4, further support the robustness of the observed reductions in personnel effort associated with the implementation of TLA.
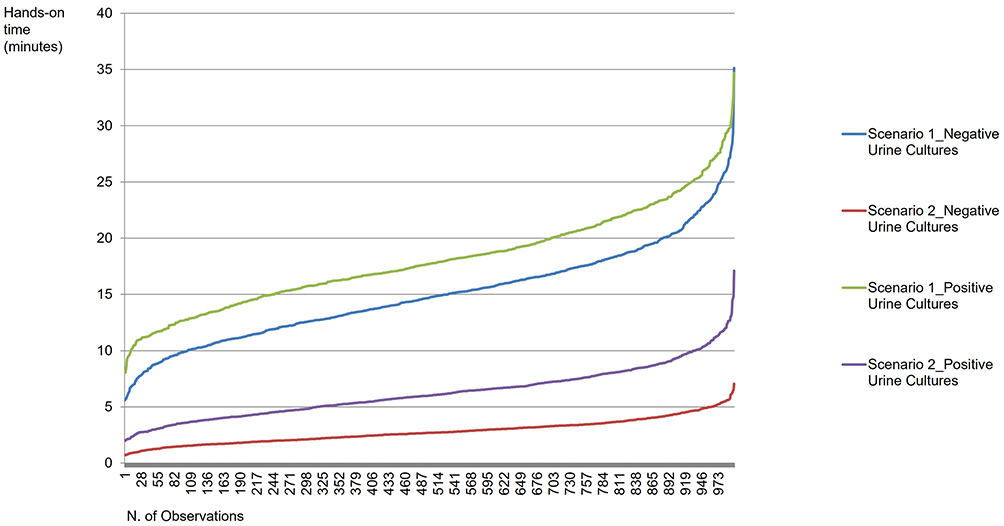 |
Figure 3 Bayesian Gamma Distribution of Hands-on Time for Urine Cultures. Lower curves indicate reduced hands-on time required for urine cultures management. |
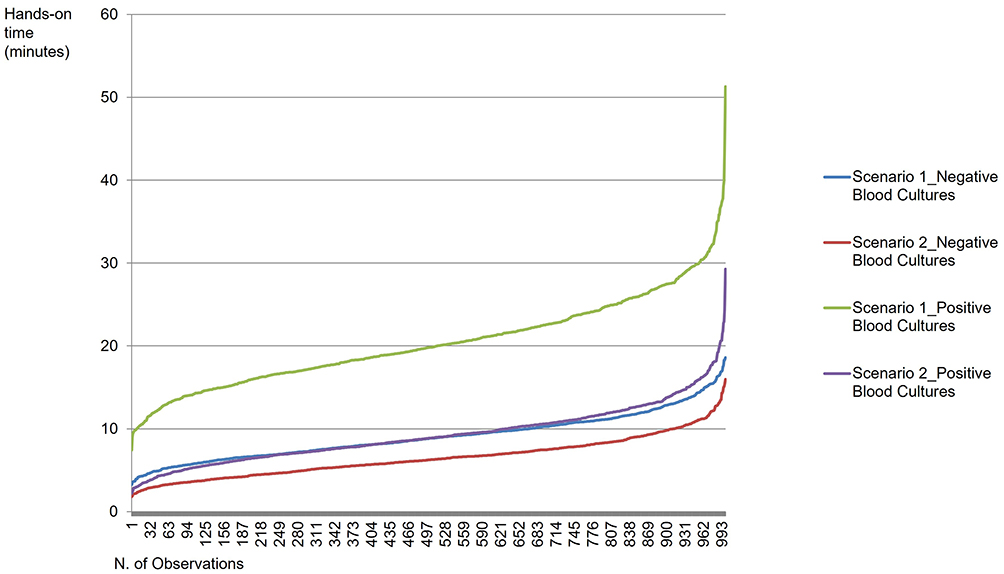 |
Figure 4 Bayesian Gamma Distribution of Hands-on Time for Blood Cultures. Lower curves indicate reduced hands-on time required for blood cultures management. |
To assess the broader organizational impact, these per-sample savings were extrapolated over a 12-month period, considering the year 2024, assuming a workload of 80,400 urine cultures (30% positives) and 20,000 blood cultures vials (19.7% positives). As shown in Table 4, if the same volume of activities was performed without TLA implementation, 25,664 working hours would have been required annually. This means that without TLA, as in Scenario 1, the laboratory would have needed about 60 working hours per day spent in hands on time to manage samples. Assuming a 6-hour shift, this would translate to about 10 full-time equivalents (FTEs) fully dedicated to these manual activities. Conversely, the transition to TLA reduced the annual workload to 7394 hours, corresponding to a 71% reduction in routine manual effort. This translates into the possibility to reinvest 67% of the personnel costs, toward more complex clinical tasks or addressing other organizational priorities, through a cost-opportunity approach.
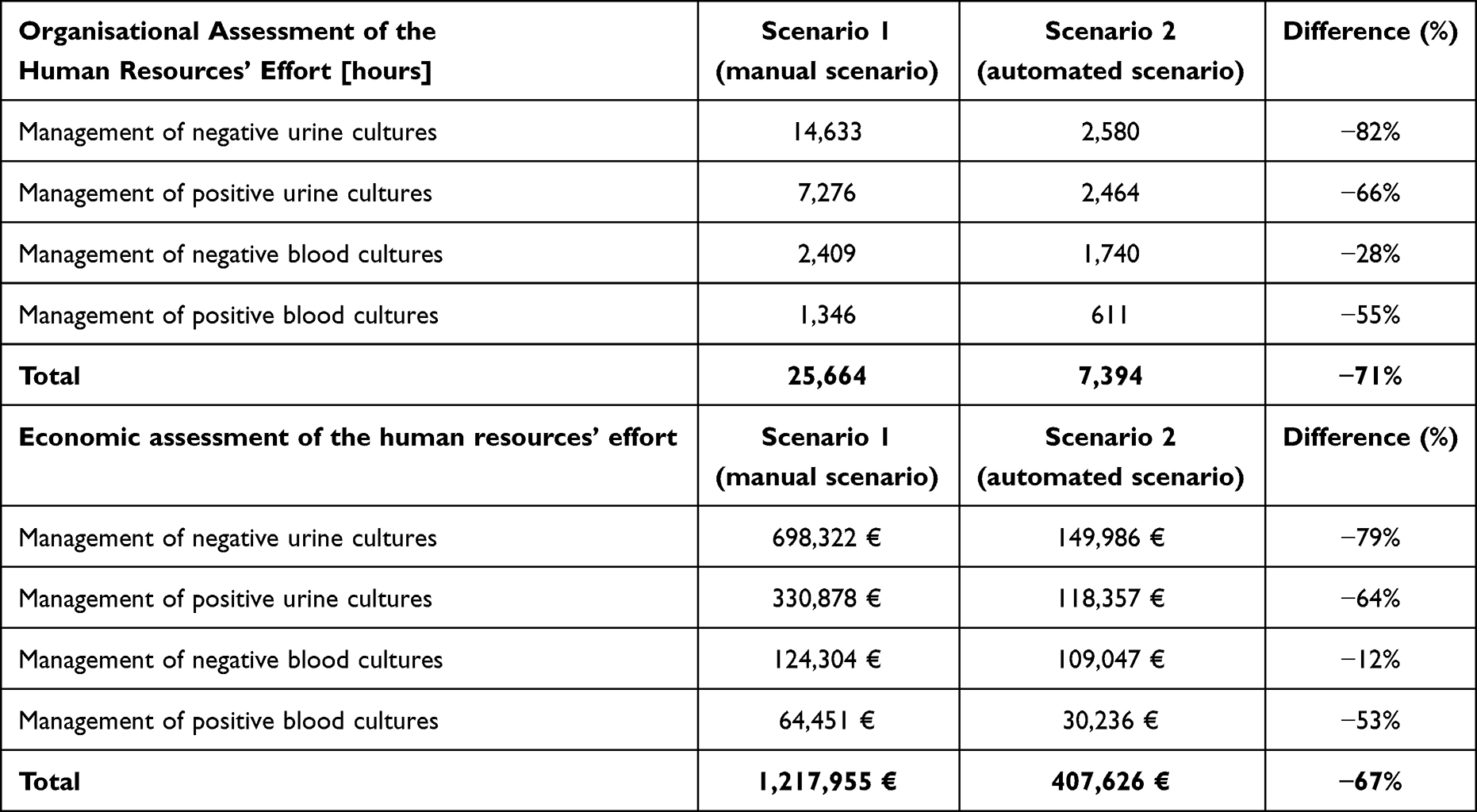 |
Table 4 Time Spent and Economic Assessment for the Management of Samples Processed During a 12-Month Time Horizon, Considering Only the Human Resources’ Effort |
Healthcare Professionals’ Perceptions
The qualitative questionnaire has been filled in by 9 healthcare professionals, currently using TLA in the microbiology setting. Healthcare professionals were equally distributed considering their professional role, being 56% clinical manager and 44% laboratory technician. In general terms, they have been working in laboratory hospital for 11.67±2.84 years, with an expertise within the current healthcare organization equal to 6.78±2.39.
Supplementary Table 1 depicts the healthcare professionals’ perceptions, comparing the investigated scenarios. TLA was perceived as significantly superior to manual methods, particularly in terms of safety (2.28 vs. 0.07, p-value= 0.007) and effectiveness (2.31 vs. 0.36, p-value= 0.002). Respondents reported a marked reduction in occupational exposure to pathogens and fewer errors in sample processing, reporting, and traceability. While no significant differences were observed in equity, social, or legal dimensions (p-value > 0.05), automation was associated with improved laboratory accessibility (1.00 vs. 0.00, p-value= 0.026), shorter diagnostic waiting times (0.67 vs. –0.44, p-value = 0.033), and better compliance with safety standards (2.44 vs. 0.11, p-value = 0.001), including alignment with ISO15189 (1.78 vs. 0.22, p-value = 0.014). Organizationally, the first-year post-implementation required significant staff training and adaptation (–2.11 vs. 0.22, p-value < 0.001). However, TLA improved clinical pathways (p-value = 0.012) and interdepartmental connectivity (p-value = 0.008). Over a 36-month horizon, Scenario 2 (TLA) emerged as the preferred solution (1.15 vs. –0.05, p-value = 0.042).
Regression analysis (Table 5) identified key predictors of TLA adoption: perceived usefulness (β = 0.720, p = 0.038), result quality (β = 0.117, p = 0.023), and demonstrability (β = 0.613, p = 0.004). Conversely, viewing TLA as a status symbol negatively impacted adoption (β = –0.042, p = 0.028), indicating a preference for functional over symbolic benefits. These factors explained a large proportion of the variance (Adjusted R2 = 0.892), in the studied context, although results should be interpreted with caution due to the limited sample size.
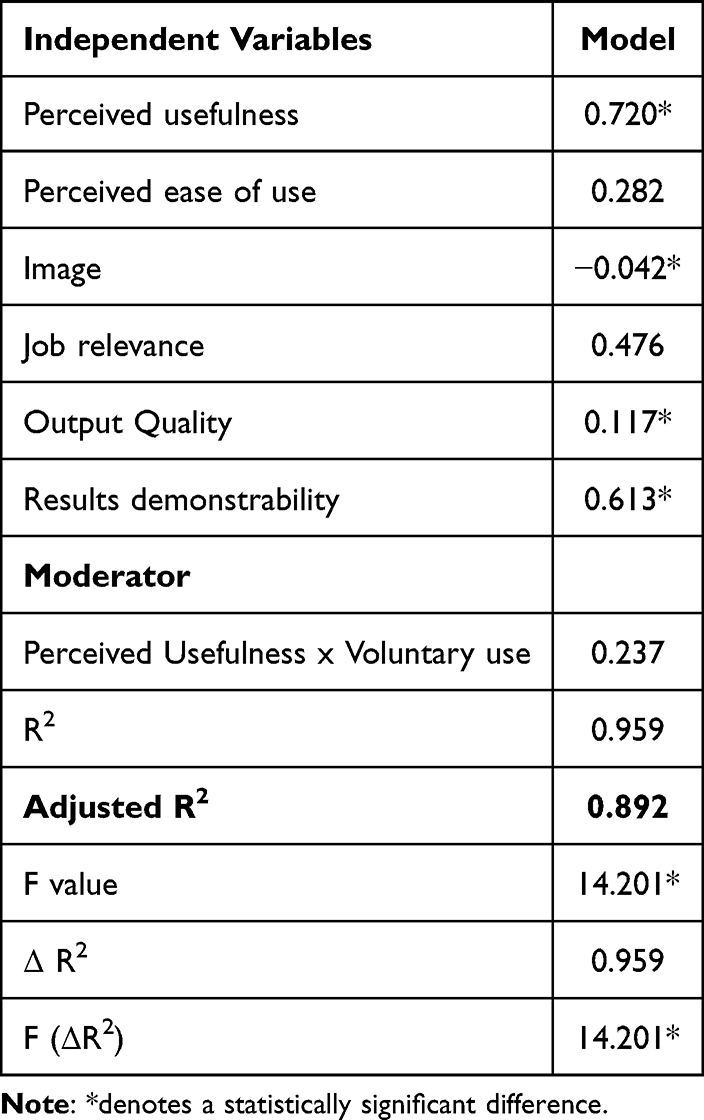 |
Table 5 Regression Model Depicting Factors Impacting on TLA Acceptability and Intention to Use |
Discussion
The results of the present study provide new evidence about the impact of automated technologies in microbiological laboratories, focusing on a range of dimensions including efficiency, economic benefits, social and ethical considerations, and organizational impacts. The findings underscore several key advantages of transitioning from manual to automated processes within microbiological labs, thus being important since innovative medical equipment is a crucial asset that substantially contributes to the effectiveness and healthcare services quality enhancement.39,40
The case study has demonstrated that automated systems are associated with significant improvements in operational efficiency, improving the speed of microbiological activities, with reductions observed in turnaround times and hands-on processing time. This efficiency not only accelerates diagnostic processes but also optimizes resource utilization, leading to sustained improvements in laboratory productivity, thus answering to RQ1. Real-life data collection from the Di Venere Hospital-Carbonara of Bari provided concrete evidence of these benefits. The implementation of TLA led to a substantial reduction in overall hands-on time required for microbiological processing of both blood and urine cultures. Notably, there was a significant decrease in redundant activities, such as repeat subcultures for identification purposes (–77%) and procedures repeated due to identification errors (–98%). These improvements may be explained by the higher yield of discrete colonies, as previously reported,6,28 and the enhanced system integration enabled by middleware, which ensured comprehensive process management and sample traceability. From an organizational perspective, the reduction in TAT aligns with findings that automated systems streamline processes such as specimen processing, incubation, and result interpretation.25 These improvements highlight the substantial efficiency gains and the positive impact on workflow processes that automation can deliver in real-world settings.
In addition, the study underlines the organizational advantages of automation, particularly in terms of reduced personnel time requirements across microbiology activities. The analysis showed a total of 18,279 manual working hours averted per year, primarily due to shorter turnaround times and streamlined workflows. This time saving was then economically valorized, allowing the estimation of a potential benefit of approximately €810,000 annually in terms of reduced human resource effort. However, it is important to note that this figure should not be interpreted as a direct financial saving, but rather as an opportunity cost advantage, which may vary depending on the specific organizational context.41 In practical terms, the time and resources saved through TLA implementation can be strategically reinvested in value-added activities. These may include enhanced clinical advisory services provided by microbiologists, expanded staff training and professional development, or increased laboratory throughput through additional testing capacity. The nature and impact of such reinvestments will vary across healthcare institutions, depending on their strategic objectives, workforce structure, and available resources. As such, the organizational benefits derived from TLA should be viewed as a flexible asset, the value of which depends on careful planning and alignment with local priorities and operational capabilities. The same preference towards automated solutions emerged in considering the healthcare professionals’ perceptions, answering the RQ2. In this view, automated systems were perceived by healthcare professionals as improving the reliability and consistency of pathogen identification processes.
This result aligns with findings from literature, such as the study by Jacot et al,22 which showed high identification performance particularly for gram-negative bacteria TLA was perceived to be safer than the manual processes, contributing to improved safety conditions for healthcare workers and laboratory processes, as also confirmed by literature.27 Professionals highlighted reduced exposure to biohazardous materials and a decrease in reporting, processing, and traceability errors. These findings are supported by studies indicating that automation can decrease handling of biohazardous materials and reduce errors in laboratory processes.42 These advantages were also perceived as contributing to improvements in service quality:
This perception is consistent with literature suggesting that automation may support improved clinical workflows and timeliness.7,8
Moreover, TLA makes laboratory services more accessible to patients, increasing efficiency and capacity.1
Overall, the findings underscore that TLA is widely regarded as a transformative solution in microbiology laboratories, with measurable benefits in terms of efficiency and workflow optimization, alongside perceived improvements in safety and process reliability.
While the transition to automation necessitates an initial investment in training and adaptation, the long-term gains in standardization, productivity, and laboratory performance reinforce its value as a sustainable and scalable innovation.9
Despite the positive findings, this study has some limitations that may affect the generalizability and interpretation of the results. First, the analysis is based on a single-center case study conducted in an Italian hospital involving a small sample size of healthcare professionals in the qualitative analysis, which may limit the applicability of the findings to other healthcare settings. Nevertheless, the KPI dashboard developed in this study could be adapted and scaled to other laboratories using their own real-world data. Moreover, although the limited sample size may constrain the statistical generalizability of perception-based findings, the objective—consistent with HTA principles—was to capture informed stakeholder perspectives through a co-design approach rather than to achieve statistical representativeness. All professionals operating within the laboratory unit were included, ensuring completeness of experiential input. Second, the comparison between pre- and post-automation scenarios is influenced by differences beyond the implementation of TLA, including variations in workload, operating hours, staffing levels, and network expansion. These contextual changes may limit the ability to attribute observed differences exclusively to automation and should be considered when interpreting the results. Third, the relatively short duration of data collection restricts the ability to assess the long-term impacts and sustainability of TLA. While the study captures initial and intermediate outcomes, it does not fully address long-term considerations such as system maintenance, evolving staff competencies, or sustained workflow efficiency.
Fourth, the economic evaluation primarily focuses on labor cost savings. Other potentially significant cost factors—such as expenses related to system upgrades, staff training, and unforeseen technical issues—were not comprehensively analyzed. These hidden or indirect costs could influence the overall cost of TLA over time. Additionally, the analysis focused on laboratory-level outcomes and efficiency measures and did not account for potential downstream effects at the hospital level, such as improved clinical decision-making, faster patient management, or broader system efficiency. Furthermore, some outcomes discussed—such as improvements in diagnostic accuracy or patient-related benefits—were not directly measured and should therefore be interpreted with caution, as perceived rather than objectively demonstrated effects.
These limitations highlight the need for further research, particularly longitudinal studies to comprehensively assess the long-term implications of TLA in clinical microbiology laboratories.
Conclusion
This study provides a multidimensional evaluation of TLA in a real-world microbiology setting, highlighting substantial improvements in workflow efficiency and resource utilization, including marked reductions in hands-on time and turnaround times. From an organizational perspective, these efficiency gains translate into a significant release of workforce capacity, allowing the potential reallocation of personnel effort toward higher-value clinical and organizational activities. These findings should be interpreted as opportunity cost advantages rather than direct financial savings.
In addition, healthcare professionals reported generally positive perceptions of TLA, particularly in terms of workflow optimization and safety, although these findings should be considered exploratory due to the limited sample size.
The findings offer valuable insights for policymakers and healthcare professionals, emphasizing the need for interdisciplinary approaches in technology adoption. Beyond informing decision-making in healthcare planning, this study highlights the importance of collecting real-life data on safety, efficacy, and organizational impact to refine laboratory performance metrics.
Overall, the study supports the role of HTA as a valuable framework for capturing the multidimensional impact of complex healthcare technologies such as TLA, while highlighting the need for further research to strengthen the evidence base.
In conclusion, as healthcare systems continue to evolve, the integration of these technologies will be pivotal in enhancing laboratory operations, and achieving greater overall efficiency.
Ethical Approval
The data collection was approved by LIUC University Research Ethical Committee (protocol number R13-23 dated 7th July 2023).
Informed Consent
All healthcare professionals involved in the qualitative assessment signed a written informed consent form prior to participation in the research activities. The informed consent procedure and related documentation were developed in accordance with the guidelines and requirements provided by the University Research Ethics Committee of LIUC University.
Acknowledgments
The Authors would like to thank all the professionals involved in the study for their valuable support in completing the qualitative questionnaires, leading to the success of the present research activity.
Author Contributions
All authors have accepted responsibility for the entire content of this manuscript and approved its submission. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
Dr Emanuela Foglia reports personal fees from Becton Dickison, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Wians F. Clinical laboratory tests: which, why, and what do the results mean? Lab Med. 2009;40(2):105–16. doi:10.1309/LM4O4L0HHUTWWUDD
2. Moreno-Camacho JL, Calva-Espinosa DY, Leal-Leyva YY, Elizalde-Olivas DC, Campos-Romero A, Alcántar-Fernández J. Transformation from a conventional clinical microbiology laboratory to full automation. Lab Med. 2017;49(1):e1–e8. PMID: 29253199. doi:10.1093/labmed/lmx079
3. Benn N, Turlais F, Clark V, Jones M, Clulow S. An automated metrics system to measure and improve the success of laboratory automation implementation. Clin Lab Med. 2007;27(1):29–39. PMID: 17416300. doi:10.1016/j.cll.2006.12.001
4. Smith KP, Kirby JE. Image analysis and laboratory automation in clinical microbiology: a time for integration and investment. J Clin Microbiol. 2018;56(8):e01400–17. doi:10.1128/JCM.01400-17
5. Burckhardt I. Laboratory automation in clinical microbiology. Bioengineering. 2018;5(4):102. PMID: 30467275. doi:10.3390/bioengineering5040102
6. Croxatto A, Prod’hom G, Faverjon F, Rochais Y, Greub G. Laboratory automation in clinical bacteriology: what system to choose? Clin Microbiol Infect. 2016;22(3):217–235. PMID: 26806135. doi:10.1016/j.cmi.2015.09.030
7. Mutters NT, Hodiamont CJ, de Jong MD, Overmeijer HP, van den Boogaard M, Visser CE. Performance of kiestra total laboratory automation combined with MS in clinical microbiology practice. Ann Lab Med. 2014;34(2):111–117. PMID: 24624346. doi:10.3343/alm.2014.34.2.111
8. Wenzel RP, Edmond MB. Infection control: the case for horizontal rather than vertical interventional programs. Int J Infect Dis. 2010;14 Suppl 4:S3–5. PMID: 20851010. doi:10.1016/j.ijid.2010.05.002
9. Genzen JR, Murray DL, Abel G, et al. Screening and diagnosis of monoclonal gammopathies: an international survey of laboratory practice. Arch Pathol Lab Med. 2018;142(4):507–515. doi:10.5858/arpa.2017-0128-CP
10. Armbruster DA, Overcash DR, Reyes J. Clinical chemistry laboratory automation in the 21st century - amat victoria curam (victory loves careful preparation). Clin Biochem Rev. 2014;35(3):143–153. PMID: 25336760.
11. Dolci A, Giavarina D, Pasqualetti S, Szőke D, Panteghini M. Total laboratory automation: do stat tests still matter? Clin Biochem. 2017;50(10–11):605–611. PMID: 28390779. doi:10.1016/j.clinbiochem.2017.04.002
12. Yarbrough ML, Lainhart W, McMullen AR, Anderson NW, Burnham CD. Impact of total laboratory automation on workflow and specimen processing time for culture of urine specimens. Eur J Clin Microbiol Infect Dis. 2018;37(12):2405–2411. PMID: 30269180. doi:10.1007/s10096-018-3391-7
13. Froment P, Marchandin H, Vande Perre P, Lamy B. Automated versus manual sample inoculations in routine clinical microbiology: a performance evaluation of the fully automated InoqulA instrument. J Clin Microbiol. 2014;52(3):796–802. PMID: 24353001. doi:10.1128/JCM.02341-13
14. Iversen J, Stendal G, Gerdes CM, Meyer CH, Andersen CØ, Frimodt-Møller N. Comparative evaluation of inoculation of urine samples with the copan WASP and BD kiestra InoqulA instruments. J Clin Microbiol. 2016;54(2):328–332. PMID: 26607980. doi:10.1128/JCM.01718-15
15. Bourbeau PP, Ledeboer NA. Automation in clinical microbiology. J Clin Microbiol. 2013;51(6):1658–1665. PMID: 23515547. doi:10.1128/JCM.00301-13
16. Shiferaw KB, Mengiste SA, Gullslett MK, et al. Healthcare providers’ acceptance of telemedicine and preference of modalities during COVID-19 pandemics in a low-resource setting: an extended UTAUT model. PLoS One. 2021;16(4):e0250220. PMID: 33886625. doi:10.1371/journal.pone.0250220
17. Okyere Boadu R, Adzakpah G, Kumasenu Mensah N, et al. Healthcare providers’ perception towards utilization of health information applications and its associated factors in healthcare delivery in health facilities in cape coast metropolis, Ghana. PLoS One. 2024;19(2):e0297388. PMID: 38300933; PMCID: PMC10833587. doi:10.1371/journal.pone.0297388
18. Jacot D, Sarton-Lohéac G, Coste AT, et al. Performance evaluation of the becton dickinson kiestra™ IdentifA/SusceptA. Clin Microbiol Infect. 2021;27(8):1167.e9–1167.e17. PMID: 33031951. doi:10.1016/j.cmi.2020.09.050
19. Peisach N, Krotkov N, Shaye R, et al. Automation of plate inoculation and reading reduces process time in the clinical microbiology laboratory compared with a manual workflow. medRxiv. 2022. doi:10.1101/2022.03.16.22272483
20. Sampietro-Colom L, Lach K, Pasternack I, et al. Guiding principles for good practices in hospital-based health technology assessment units. Int J Technol Assess Health Care. 2015;31(6):457–465. PMID: 26899230. doi:10.1017/S0266462315000732
21. Creswell JW. A Concise Introduction to Mixed Methods Research. Thousand Oaks, CA: Sage Publications; 2014.
22. O’Cathain A, Murphy E, Nicholl J. Why, and how, mixed methods research is undertaken in health services research in England: a mixed methods study. BMC Health Serv Res. 2007;7(1):85. PMID: 17570838. doi:10.1186/1472-6963-7-85
23. Sukhera J. Narrative reviews in medical education: key steps for researchers. J Grad Med Educ. 2022;14(4):418–419. PMID: 35991097. doi:10.4300/JGME-D-22-00481.1
24. Okoli C, Pawlowski SD. The Delphi method as a research tool: an example, design considerations and applications. Inf Manag. 2004;42(1):15–29. doi:10.1016/j.im.2003.11.002
25. Theparee T, Das S, Thomson RB. Total laboratory automation and matrix-assisted laser desorption ionization-time of flight mass spectrometry improve turnaround times in the clinical microbiology laboratory: a retrospective analysis. J Clin Microbiol. 2017;56(1):e01242–17. PMID: 29118171. doi:10.1128/JCM.01242-17
26. Zhang W, Wu S, Deng J, et al. Total laboratory automation and three shifts reduce turnaround time of cerebrospinal fluid culture results in the chinese clinical microbiology laboratory. Front Cell Infect Microbiol. 2021;11:765504. PMID: 34926317. doi:10.3389/fcimb.2021.765504
27. Gonzalez-Ortiz C, Emrick A, Tabak YP, et al. Impact on microbiology laboratory turnaround times following process improvements and total laboratory automation. J Exp Pathol. 2021;2(1). doi:10.33696/pathology.2.012
28. Klein S, Nurjadi D, Horner S, Heeg K, Zimmermann S, Burckhardt I. Significant increase in cultivation of Gardnerella vaginalis, Alloscardovia omnicolens, Actinotignum schaalii, and Actinomyces spp. in urine samples with total laboratory automation. Eur J Clin Microbiol Infect Dis. 2018;37(7):1305–1311. PMID: 29651616. doi:10.1007/s10096-018-3250-6
29. Kaplan RS, Anderson SR. Time-driven activity-based costing. Harv Bus Rev. 2007;85(11):131–138.
30. Keel G, Savage C, Rafiq M, Mazzocato P. Time-driven activity-based costing in health care: a systematic review of the literature. Health Policy. 2017;121(7):755–763. PMID: 28535996. doi:10.1016/j.healthpol.2017.04.013
31. Salary Expert 2025. Available from: https://www.salaryexpert.com/. Accessed November 12, 2025.
32. Mitton C, Smith N, Peacock S, Evoy B, Abelson J. Public participation in health care priority setting: a scoping review. Health Policy. 2009;91(3):219–228. PMID: 19261347. doi:10.1016/j.healthpol.2009.01.005
33. Davis FD. Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS Q. 1989;13(3):319–340. doi:10.2307/249008
34. Venkatesh V, Davis FD. A theoretical extension of the technology acceptance model: four longitudinal field studies. Manage Sci. 2000;46(2):186–204. doi:10.1287/mnsc.46.2.186.11926
35. Holden RJ, Karsh BT. The technology acceptance model: its past and its future in health care. J Biomed Inform. 2010;43(1):159–172. PMID: 19615467. doi:10.1016/j.jbi.2009.07.002
36. Bhattacherjee A, Hikmet N. Physicians’ resistance toward healthcare information technology: a theoretical model and empirical test. Eur J Inf Syst. 2007;16(6):725–737. doi:10.1057/palgrave.ejis.3000717
37. Yarbrough AK, Smith TB. Technology acceptance among physicians: a new take on TAM. Med Care Res Rev. 2007;64(6):650–672. PMID: 17717378. doi:10.1177/1077558707305942
38. Moore GC, Benbasat I. Development of an instrument to measure the perceptions of adopting an information technology innovation. Inf Syst Res. 1991;2(3):192–222. doi:10.1287/isre.2.3.192
39. Triposkiadis F, Brutsaert DL. Evidence-based medicine: past, present, future. J Clin Med. 2025;14(14):5094. PMID: 40725787. doi:10.3390/jcm14145094
40. Wang B. Medical Equipment Maintenance: Management and Oversight. San Rafael, CA: Morgan & Claypool; 2012.
41. Hernandez-Villafuerte K, Zamora B, Feng Y, Parkin D, Devlin N, Towse A. Estimating health system opportunity costs: the role of non-linearities and inefficiency. Cost Eff Resour Alloc. 2022;20(1):56. PMID: 36309687. doi:10.1186/s12962-022-00391-y
42. Farnsworth CW, Wallace MA, Liu A, Gronowski AM, Burnham CD, Yarbrough ML. Evaluation of the risk of laboratory microbial contamination during routine testing in automated clinical chemistry and microbiology laboratories. Clin Chem. 2020;66(9):1190–1199. PMID: 32870987. doi:10.1093/clinchem/hvaa128
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.