Back to Journals » Clinical Ophthalmology » Volume 17
Topography-Guided LASIK: A Prospective Study Evaluating Patient-Reported Outcomes
Authors Rush SW, Pickett CJ, Wilson BJ, Rush RB ![]()
Received 9 August 2023
Accepted for publication 15 September 2023
Published 25 September 2023 Volume 2023:17 Pages 2815—2824
DOI https://doi.org/10.2147/OPTH.S429991
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Sloan W Rush,1,2 Cory J Pickett,1 Braden J Wilson,3 Ryan B Rush2
1Rush Eye Associates, Amarillo, TX, USA; 2Department of Surgery, Texas Tech University Health Science Center, Amarillo, TX, USA; 3Baylor Scott and White Health, Temple, TX, USA
Correspondence: Ryan B Rush, Southwest Retina Specialists, 7411 Wallace Blvd, Amarillo, TX, 79106, USA, Tel +1 806 351-1870, Email [email protected]
Purpose: To evaluate patient-reported outcomes with a validated patient questionnaire following topography-guided LASIK (TG-LASIK).
Methods: Patients undergoing TG-LASIK using Phorcides analytic software were prospectively enrolled to receive an adapted Patient-Reported Outcomes with LASIK Symptoms and Satisfaction (PROWL) questionnaire before and 26-weeks after treatment. The main study outcome was the change in the Global Vision Satisfaction Index from the PROWL questionnaire.
Results: Forty-six patients underwent treatment and completed the modified PROWL questionnaire before and 26-weeks after TG-LASIK. The Global Vision Satisfaction Index from the modified PROWL questionnaire improved from 4.07 (3.87– 4.26) to 5.00 (4.81– 5.19) after the TG-LASIK treatment (p < 0.0001). The study population’s binocular uncorrected distance visual acuity was 20/16, 20/12.5, and 20/10 or better in 100%, 87.0%, and 15.2% at 26 weeks post TG-LASIK, respectively.
Conclusion: Patient satisfaction as assessed with the modified PROWL questionnaire is very high after undergoing TG-LASIK using Phorcides analytic software. Patient-reported outcomes add another dimension when assessing treatment efficacy beyond change in visual acuity and corneal architecture, and specialists may consider incorporating such assessments into the consenting process and patient education at large.
Keywords: LASIK, topography-guided, Contoura, PROWL, patient-reported outcomes, Phorcides
Introduction
Wavefront-guided (WG) and wavefront-optimized (WFO) ablations have been among the most popular LASIK techniques performed over the past decade,1,2 and conflicting outcomes are reported when the two techniques have been compared.3–6 In recent years, topography-guided LASIK (TG-LASIK) has become popular in the United States, and excellent outcomes have been reported.7,8 Compared to WG and WFO ablations, TG-LASIK offers the theoretical advantage of improving the cornea’s natural shape, thereby enhancing the optics beyond what may be achievable with glasses and/or contact lenses with fewer higher order aberrations.9–12
Researchers have compared various TG-LASIK algorithms for calculating the treatment of astigmatism, focusing mostly on the treatment of manifest refraction versus measured topographic refraction indices with mixed results.13–16More recently, researchers have published outcomes using the Phorcides Analytic Engine software (Phorcides, LLC; MN, USA), a standardized and automated topography analysis algorithm.17 Better postoperative uncorrected distance visual acuity (UDVA) and best-corrected distance visual acuity (CDVA have been reported when employing the Phorcides analytic software compared to conventional techniques based solely upon manifest refraction.18,19
The medical sciences during the past several years have increasingly recognized the importance of patient-reported outcomes, and the authors agree that such outcomes provide the physician with an opportunity to offer a more holistic approach to the care of their patients.20,21 The Patient-Reported Outcomes with LASIK Symptoms and Satisfaction (PROWL) questionnaire are a well-defined and validated survey for assessing patient satisfaction following LASIK.22,23 Although reports using the PROWL questionnaire have been published after WG and WFO ablations,24 there are currently no reports following TG-LASIK. In this study, the authors evaluate patient-reported outcomes with the PROWL questionnaire before and after undergoing TG-LASIK using the Phorcides analytic software.
Methods
The Salus Independent Review Board (IORG0005674-1, Austin, TX, USA) approved this prospective, uncontrolled interventional study of patients who underwent bilateral TG-LASIK from October 2021 through November 2022 at a single private practice institution in Amarillo, TX. All components of this study were in compliance with the tenets of the Declaration of Helsinki and compliant with the Health Insurance Portability and Accountability Act of 1996. Written informed consent was obtained for all participants, and the study was registered on clinicaltrials.gov. prior to subject enrollment (NCT04903301, last accessed on 4–27-23).
The inclusion and exclusion criteria are presented in Table 1. Enrolled subjects underwent bilateral treatment using the Contoura® Vision technique (Alcon Vision, LLC; Fort Worth, TX, USA). The TG-LASIK was performed using the Wavelight FS200 and Wavelight EX500 laser platforms (Alcon Vision, LLC; Fort Worth, TX, USA). The flap dimensions were cut to a depth that ranged from 90 to 110 microns and a diameter from 8.8 to 9.0 mm. The excimer laser input parameters were calculated using the Phorcides analytic software with data captured from manifest refraction, Placido disc corneal imaging (Wavelight Vario Topolyzer; Alcon Vision, LLC; Fort Worth, TX, USA), and dual Scheimpflug anterior and posterior corneal imaging from the Galilei G4 Topographer (Ziemer Ophthalmic Systems AG, Alton, IL, USA) as described by previous investigators.25 All treatment calculations were performed by the same examiner (CJP).
 |
Table 1 Patient Satisfaction with Topography-Guided LASIK. Eligibility Criteria |
The study’s baseline was considered the examination in which the patient was assessed for eligibility and consented/enrolled into the study. Data was collected at baseline and then post-treatment at 1 week (± 2 days), 4 weeks (± 1 week), 12 weeks (± 2 weeks), and 26 weeks (±4 weeks). All the data was stored on a password-protected Microsoft Excel spreadsheet. The preoperative PROWL survey used in this study was adapted from previous studies22,23 and is presented in Figure 1. The modification was done to make the survey more concise so that all of the survey items would fit onto one page. The modified postoperative PROWL survey was identical in every way to the preoperative survey with the exception of the first question which substitutes “glasses or contacts on” with “after LASIK”. Visual acuity was measured in ETDRS letters and converted into logMAR for statistical analysis. The Objective Scatter Index analog score of the ocular surface was measured using the Visiometrics HD Analyzer (Keeler, Malvern, PA, USA). Corneal and total higher order aberrations were measured using the Galilei G4 Topographer and the OPD-Scan III Wavefront Analyzer (Marco Ophthalmic, Jacksonville, FL, USA), and additional refractive measurements were calculated using the VX 120+ (Visionix, Bensenville, IL, USA). The modified PROWL questionnaires, visual acuity measurements, and refractions were conducted by the same examiner in all instances (CJP).
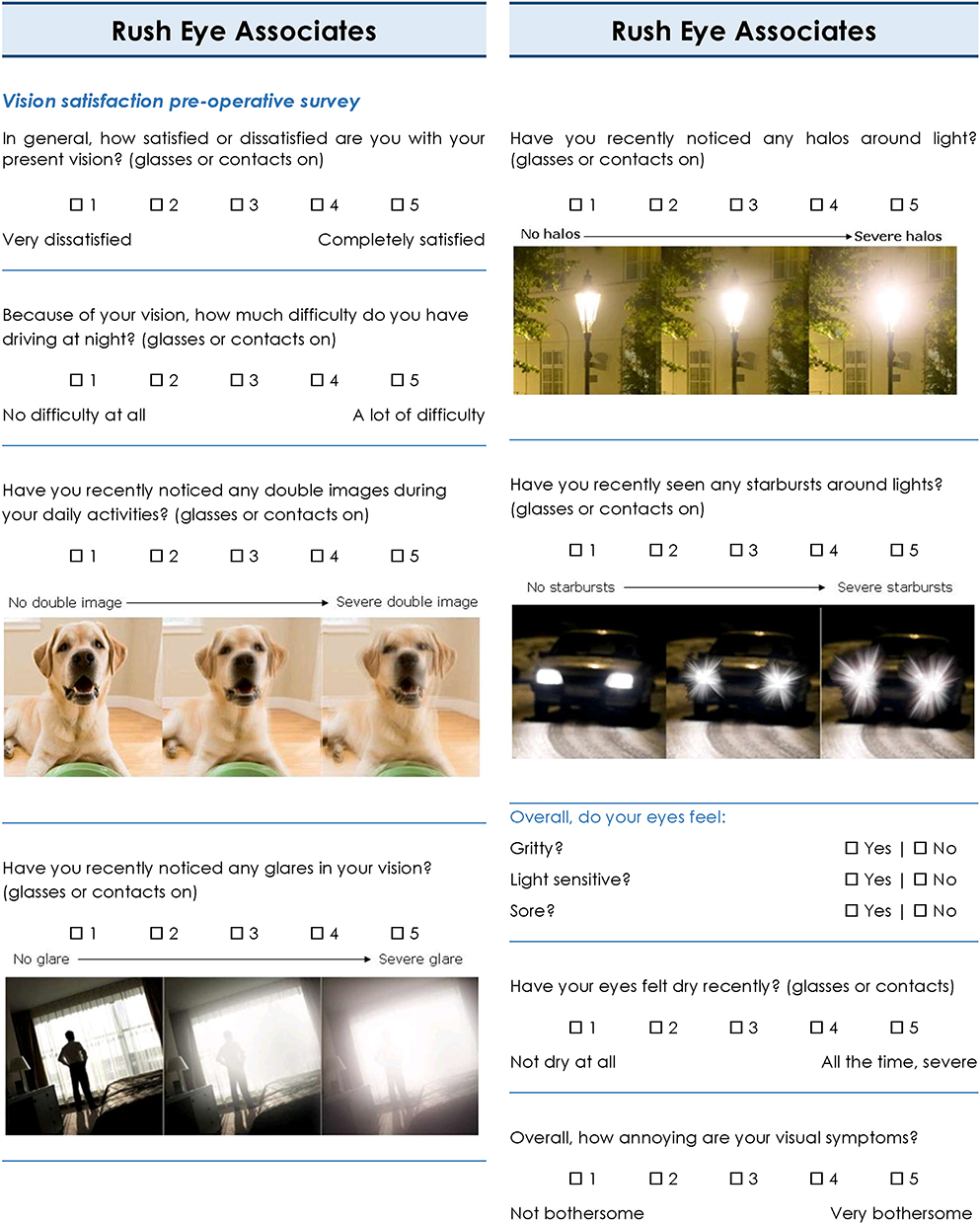 |
Figure 1 Adapted preoperative PROWL survey. |
Outcomes and Statistical Analysis
The primary outcome of the study was change in the Global Vision Satisfaction Index (visual analog score of 0–5 with 5 being most satisfied) from the adapted PROWL survey from baseline to 26-weeks post-treatment.
The study’s power was determined by deriving a standard deviation from the primary outcome for the first 10 enrolled subjects completing the study’s follow-up period. The difference to detect was calculated to be 0.5 (50% of the sampling standard deviation), resulting in 43 subjects as the minimum required number to complete follow-up. The data were analyzed using the JMP 11 software (SAS Institute; Cary, NC, USA). Means were compared using Student’s t-test for numerical values and likelihood ratios for categorical variables. Statistical significance was considered at an alpha level of <0.05.
Results
Fifty-eight consecutive patients meeting eligibility criteria were approached regarding study participation; 49 of the patients elected participation and therefore were enrolled in the study. Forty-six of the 49 enrolled patients were treated and completed the study’s 26-week-long study interval (93.9% completion rate). The 3 patients who failed to complete the study interval were lost-to follow-up and could not be brought back for data collection and therefore excluded from data analysis.
The study population’s age was 31.1 (±4.5) years with 58.7% female. The Binocular CDVA was −0.11 (±0.06) logMAR with Mean Manifest Refraction Spherical Equivalent of 3.55 (±1.79) diopters and Mean Manifest Refraction Refractive Astigmatism 0.90 (±0.63) diopters. The remainder of the baseline characteristics and demographic features are presented in Table 2. There were no adverse events or intra-operative complications occurring during the treatment session for any of the subjects.
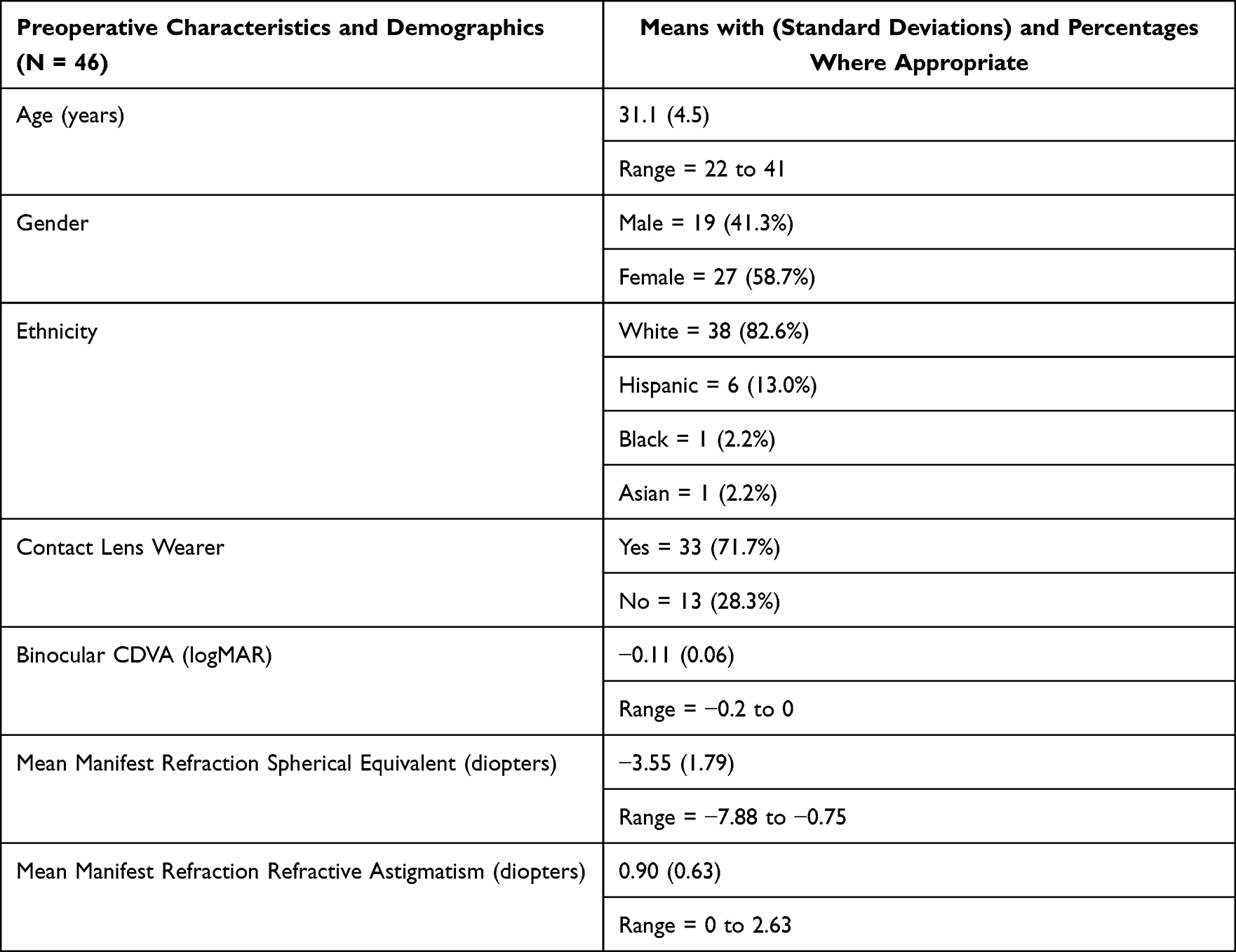 |
Table 2 Patient Satisfaction with Topography-Guided LASIK. Baseline Characteristics and Demographic Features for the Study Population |
Primary Outcome
The modified PROWL survey showed significant improvement on the Global Vision Satisfaction Index (analog score from 1 to 5 with 5 being the most satisfied) from 4.1 (3.9–4.3) preoperatively to 5.0 (4.8–5.2) postoperatively (p < 0.0001) for which 100% of patients reported maximum score of 5 for overall vision satisfaction postoperatively. Subset analysis from the questionnaire showed statistically significant postoperative improvement in night vision, glares, halos, starbursts, dry eye symptoms, and in the global symptomatology assessment (p < 0.01 for all). The only symptom that was not significantly improved was double images (p = 0.17). These findings are summarized in Table 3.
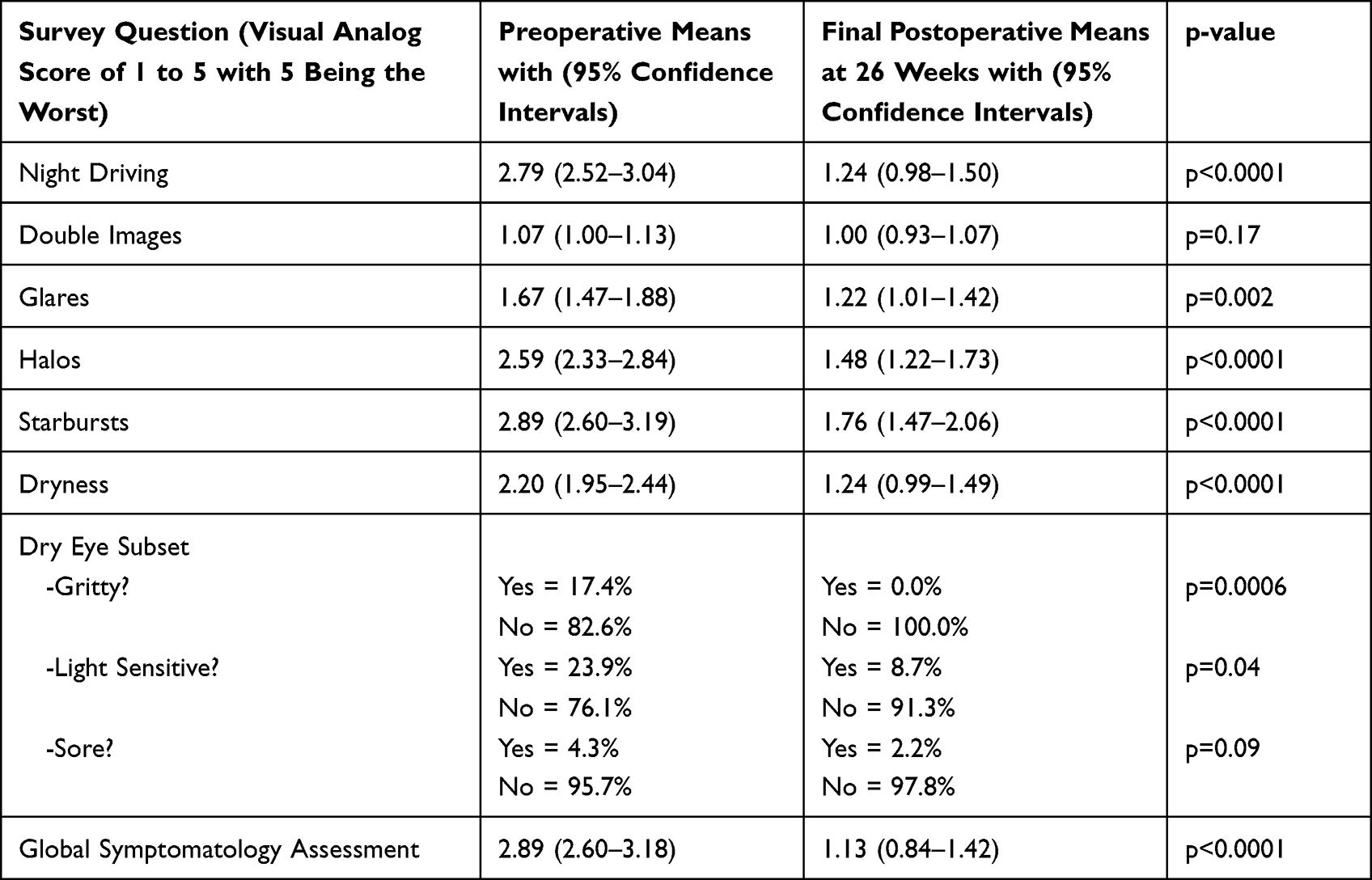 |
Table 3 Patient Satisfaction with Topography-Guided LASIK. Pre- and Postoperative Comparative Analysis of the PROWL Survey (N = 46 Patients) |
Visual Outcomes
These outcomes were previously reported in another study by the authors.26 In summary, the visual outcomes have been displayed in standardized graph format in Figure 2.
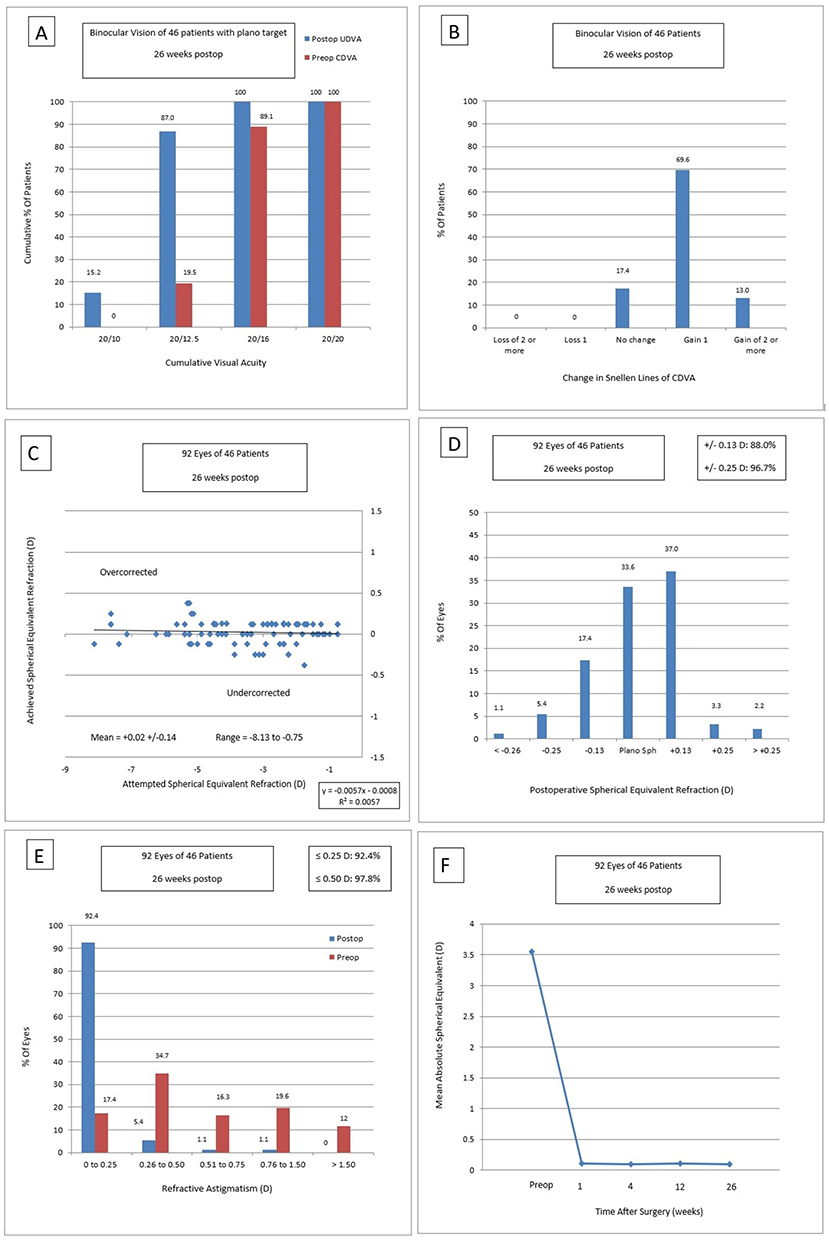 |
Figure 2 Vision and refractive data in standard graphing format including binocular outcomes. (A) Binocular Uncorrected Distance Visual Acuity: The histograph shows cumulative visual acuity binocularly as a percentage of patients reaching a Plano target. (B) Binocular Change in Corrected Distance Visual Acuity: The histograph shows change in Snellen lines of corrected distance visual acuity as a percentage of patients. (C) Spherical Equivalent Attempted vs Achieved: The scatter plot graph shows spherical equivalent attempted (X) versus spherical equivalent achieved (Y). (D) Spherical Equivalent Refractive Accuracy: The histograph shows postoperative spherical equivalent refraction (X) plotted against the percentage of eyes achieving the desired outcome (Y). (E) Refractive Astigmatism: The histograph shows refractive astigmatism (X) plotted against the percentage of eyes achieving the desired outcome (Y). (F) Stability of Spherical Equivalent Refraction: The line graph plots the mean absolute spherical equivalent (Y) over time (X). |
Other Outcomes
Figure 3 displays a graphical representation of the change in the Objective Scatter Index and higher order aberrations over time in the study population during the study interval. There was initial worsening for the objective scatter index but no significant change at the final follow-up interval (p = 0.20). With regard to the higher order aberrations, there were no significant changes in either the corneal higher order aberrations or the total higher order aberrations at the 4 mm optic zone (p = 0.80 and p = 0.94, respectively). By contrast, corneal higher order aberrations at the 6 mm optic zone had a significant increase from 0.39 (0.36–0.43) preoperatively to 0.54 (0.51–0.58) at the final visit (p < 0.0001). However, there was no significant increase in total higher order aberrations under mesopic pupil conditions (Mean = 5.8 ± 0.9 mm) which showed 0.33 (0.28–0.39) preoperatively versus 0.37 (0.32–0.42) postoperatively (p = 0.34).
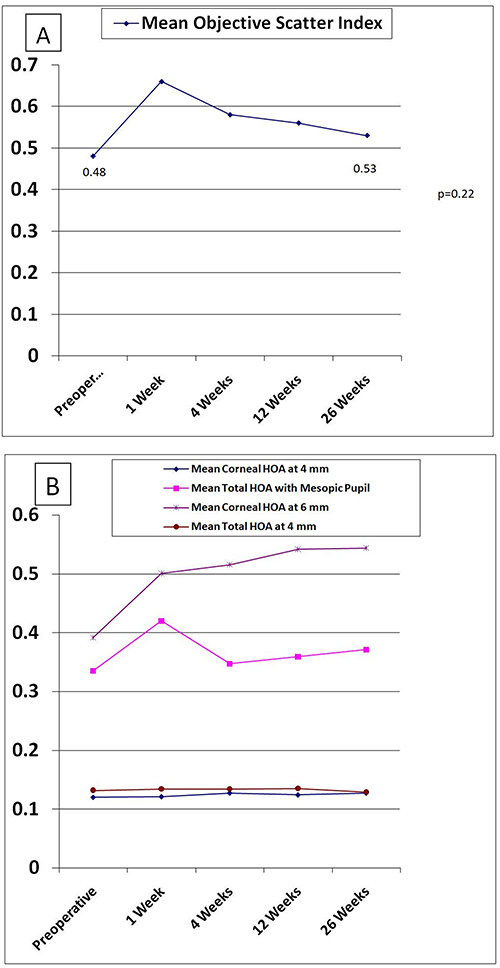 |
Figure 3 Other study outcome measures. (A) Objective Scatter Index. The line graph plots the change in objective scatter indices by analog score (Y) over time (X). (B) Higher Order Aberrations change over time. The line graph plots the change in higher order aberration indices in microns (Y) over time (X). |
There were no postoperative complications were identified during the study interval and no patients underwent an enhancement during the 26-week follow-up period.
Discussion
To our knowledge, this is the first study to report findings associated with TG-LASIK primarily focused on quality of vision from the patient’s perspective. The PROWL questionnaire was originally developed by a joint collaboration among the FDA, Department of Defense, and National Eye Institute in 2009. The PROWL-1 and PROWL-2 studies subsequently validated the first patient reported outcome survey with regard to quality of vision and quality of life after LASIK.22,23 These studies were conducted over a decade ago prior to the advent of topography-guided technology without a standardized LASIK technique which used multiple treatment calculation methods and laser platforms. Furthermore, the original PROWL inventory was web-based and included hundreds of questions on dozens of pages. An advantage of our study is that it consolidated key validated survey items from the PROWL questionnaire into a more controlled environment with a consistent survey administration technique and without being overly tedious and burdensome on the patient to complete. Under these conditions, our findings show that TG-LASIK has a very high patient satisfaction rate. The patient-reported outcomes in this study demonstrate superiority in many aspects when compared to a recent study using WG-LASIK27 in which 25% of those patients reported decreased quality of life relative to our study which had 100% of patients at the maximum level of satisfaction.
In light of the recently expanded FDA patient labeling recommendations for LASIK,28 vision quality measures are paramount when assessing LASIK outcomes and during preoperative counseling with patients. Based upon the findings from this study, the authors believe that, during the informed consent process, surgeons can reasonably include increased difficulty with night vision, glares, halos, starbursts, and dry eye symptoms and the decrease of those same symptoms as both a potential risk and, even more likely, a benefit, respectively, of TG-LASIK. We suspect that many studies that report some of these adverse symptoms after LASIK do not compare these same symptoms to what the patient may have already been experiencing at baseline.29
There is controversy regarding the ideal algorithm for refractive data input into the excimer laser when performing TG-LASIK.30–33 Input entirely derived from the surgeon’s manifest refraction permits the surgeon a certain level of confidence in their own refraction as the primary source of refractive data in cases where talus is considered to have a negligible impact.15 By contrast, Phorcides analytic software has the advantage of accounting for the talus vector of astigmatism in all cases in which it is detected on corneal topographic imaging devices, especially in outlier cases where significant discrepancies among the refractive measurements exist.34 The Phorcides algorithm has the additional benefit of objectively determining treatment parameters, thus allowing greater reproducibility among different surgeons. Similar to other studies,35 the Phorcides analytic software employed in this study produced visual acuity outcomes better than 20/20 in many subjects.
Previous studies have reported induced higher order aberrations post-myopic ablation using both WFO-LASIK and TG-LASIK.36 Our study supports that this small increase in higher order aberration is negligible with respect to visual acuity and quality of vision outcomes. Our findings show that the Objective Scatter Index did not increase to a clinically significant level and that there were no significant postoperative increases for either the total or the corneal higher order aberration at the smaller 4 mm optical zone. These findings may help explain the high patient satisfaction seen on the PROWL questionnaire.
The major limitation of this study is its lack of a comparison or control group as well having only a single study site. Strengths of this study include its prospective design using consistent methodology and calculation techniques, its high patient retention rate following enrollment, being sufficiently powered to detect significance, its use of a validated patient-reported outcome measurement tool, and its emphasis on real-world binocular vision with use of an ETDRS vision chart that measures visual acuity all the way down to 20/10 Snellen equivalent. Future investigations are necessary to validate these findings and compare patient-reported quality of vision outcomes with TG-LASIK without Phorcides analytic software and to other techniques, including other excimer laser platforms using wavefront optimized and wavefront-guided procedures as well as with non-excimer refractive treatments using SMILE and intraocular lens-based procedures. In conclusion, patient satisfaction with the PROWL questionnaire employed in this study is very high after undergoing TG-LASIK using Phorcides analytic software. Patient-reported outcomes add another element to help clinicians assess treatment efficacy beyond change in visual acuity and corneal architecture, and clinicians may consider incorporating such assessments into the consenting process as well as patient education at large.
Abbreviations
TG-LASIK, topography-guided laser in situ keratomileusis; WFO-LASIK, wavefront optimized laser in situ keratomileusis; WG-LASIK, wavefront-guided laser in situ keratomileusis; CDVA, best-corrected distance visual acuity; UDVA, uncorrected distance visual acuity; HOA, higher order aberrations; PROWL, patient-reported outcomes with LASIK; OSI, Objective Scatter Index.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Statement
The study was approved by the Salus Independent Review Board (IORG0005674-1, Austin, TX, USA) in accordance with the Ethical Standards laid down in the Declaration of Helsinki.
Acknowledgments
This study was presented at the 2023 ASCRS meeting during a paper session.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work.
Funding
The Alcon Foundation (Alcon Vision, LLC; Fort Worth, TX, USA) provided a research grant for this study.
Disclosure
The authors report no conflicts of interest in this works.
References
1. Manche E, Roe J. Recent advances in wavefront-guided LASIK. Curr Opin Ophthalmol. 2018;29(4):286–291. doi:10.1097/ICU.0000000000000488
2. Tawfik A, Eid AM, Hasanen R, Moftah IA. Q-value customized ablation (custom-Q) versus wavefront optimized ablation for primary myopia and myopic astigmatism. Int Ophthalmol. 2014;34(2):259–262. doi:10.1007/s10792-013-9828-1
3. Myrowitz EH, Chuck RS. A comparison of wavefront-optimized and wavefront-guided ablations. Curr Opin Ophthalmol. 2009;20(4):247–250. doi:10.1097/ICU.0b013e32832a2336
4. Stonecipher KG, Kezirian GM. Wavefront-optimized versus wavefront-guided LASIK for myopic astigmatism with the ALLEGRETTO WAVE: three-month results of a prospective FDA trial. J Refract Surg. 2008;24(4):S424–30. doi:10.3928/1081597X-20080401-20
5. He L, Liu A, Manche EE. Wavefront-guided versus wavefront-optimized laser in situ keratomileusis for patients with myopia: a prospective randomized contralateral eye study. Am J Ophthalmol. 2014;157(6):1170–1178.e1. doi:10.1016/j.ajo.2014.02.037
6. Padmanabhan P, Mrochen M, Basuthkar S, et al. Wavefront-guided versus wavefront-optimized laser in situ keratomileusis: contralateral comparative study. J Cataract Refract Surg. 2008;34(3):389–397. doi:10.1016/j.jcrs.2007.10.028
7. Holland S, Lin DT, Tan JC. Topography-guided laser refractive surgery. Curr Opin Ophthalmol. 2013;24(4):302–309. doi:10.1097/ICU.0b013e3283622a59
8. Pasquali T, Krueger R. Topography-guided laser refractive surgery. Curr Opin Ophthalmol. 2012;23(4):264–268. doi:10.1097/ICU.0b013e328354adf0
9. Wallerstein A, Gauvin M, Cohen M. Effect of anterior corneal higher-order aberration ablation depth on primary topography-guided LASIK outcomes. J Refract Surg. 2019;35(12):754–762. doi:10.3928/1081597X-20191021-02
10. Kim J, Choi SH, Lim DH, et al. Topography-guided versus wavefront-optimized laser in situ keratomileusis for myopia: surgical outcomes. J Cataract Refract Surg. 2019;45(7):959–965. doi:10.1016/j.jcrs.2019.01.031
11. Toda I, Ide T, Fukumoto T, Tsubota K. Visual outcomes after LASIK using topography-guided vs wavefront-guided customized ablation systems. J Refract Surg. 2016;32(11):727–732. doi:10.3928/1081597X-20160718-02
12. Schallhorn JM, Seifert S, Schallhorn SC. SMILE, topography-guided LASIK, and wavefront-guided LASIK: review of clinical outcomes in premarket approval FDA studies. J Refract Surg. 2019;35(11):690–698. doi:10.3928/1081597X-20190930-02
13. Alpins N. Astigmatism analysis by the Alpins method. J Cataract Refract Surg. 2001;27(1):31–49. doi:10.1016/S0886-3350(00)00798-7
14. Gauvin M, Wallerstein A. AstigMATIC: an automatic tool for standard astigmatism vector analysis. BMC Ophthalmol. 2018;18(1):255. doi:10.1186/s12886-018-0920-1
15. Wallerstein A, Gauvin M, Qi SR, et al. Primary topography-guided LASIK: treating manifest refractive astigmatism versus topography-measured anterior corneal astigmatism. J Refract Surg. 2019;35(1):15–23. doi:10.3928/1081597X-20181113-01
16. Abdelwahab SM, Hamed AM, Bayoumy ASM, Elfayoumi MA. Topography-guided femto-LASIK in virgin eyes: treating manifest versus measured astigmatism. Clin Ophthalmol. 2020;14:4423–4430. doi:10.2147/OPTH.S281736
17. Lobanoff M, Stonecipher K, Tooma T, et al. Clinical outcomes after topography-guided LASIK: comparing results based on a new topography analysis algorithm with those based on manifest refraction. J Cataract Refract Surg. 2020;46(6):814–819. doi:10.1097/j.jcrs.0000000000000176
18. Brunson PB, Mann Ii PM, Mann PM, Potvin R. Clinical outcomes after topography-guided refractive surgery in eyes with myopia and astigmatism - comparing results with new planning software to those obtained using the manifest refraction. Clin Ophthalmol. 2020;14:3975–3982. doi:10.2147/OPTH.S280959
19. Stulting RD, Durrie DS, Potvin RJ, et al. Topography-guided refractive astigmatism outcomes: predictions comparing three different programming methods. Clin Ophthalmol. 2020;14:1091–1100. doi:10.2147/OPTH.S244079
20. Finger RP, Scholl HPN, Holz FG. Patient reported outcomes. Relevance and application in ophthalmology. Ophthalmologe. 2008;105(8):722–726. doi:10.1007/s00347-008-1804-1
21. Scheibler F, Finger RP, Grosselfinger R, Dintsios CM. Patient-reported and patient-weighted outcomes in ophthalmology. Ophthalmologe. 2010;107(3):235–240. doi:10.1007/s00347-009-2037-7
22. Hays RD, Tarver ME, Spritzer KL, et al. Assessment of the psychometric properties of a questionnaire assessing patient-reported outcomes with laser in situ keratomileusis (PROWL). JAMA Ophthalmol. 2017;135(1):3–12. doi:10.1001/jamaophthalmol.2016.4597
23. Eydelman M, Hilmantel G, Tarver ME, et al. Symptoms and satisfaction of patients in the patient-reported outcomes with laser in situ keratomileusis (PROWL) studies. JAMA Ophthalmol. 2017;135(1):13–22. doi:10.1001/jamaophthalmol.2016.4587
24. Yu J, Chen H, Wang F. Patient satisfaction and visual symptoms after wavefront-guided and wavefront-optimized LASIK with the WaveLight platform. J Refract Surg. 2008;24(5):477–486.
25. Stulting RD, Lobanoff M, Mann PM, et al. Clinical and refractive outcomes after topography-guided refractive surgery planned using Phorcides surgery planning software. J Cataract Refract Surg. 2022;48(9):1010–1015. doi:10.1097/j.jcrs.0000000000000910
26. Rush S, Pickett CJ, Rush RB. Patient-reported dry eye outcomes after myopic femtosecond-LASIK: a 6-month prospective analysis. Clin Ophthalmol. 2023;17:2141–2147. doi:10.2147/OPTH.S421369
27. Lee MD, Leibold C, Manche EE. Patient-reported outcomes with wavefront-guided laser in situ keratomileusis (PROWL) study outcomes from a single institution. J Refract Surg. 2023;39(3):198–204. doi:10.3928/1081597X-20230103-01
28. Center for Devices and Radiological Health. Docket Number: FDA-2022-D-1253; 2022.
29. Toda I. Dry Eye After LASIK. Invest Ophthalmol Vis Sci. 2018;59(14):DES109–DES115. doi:10.1167/iovs.17-23538
30. Wallerstein A, Gauvin M. Is Phorcides more likely to give better vision than treating the manifest refraction? J Cataract Refract Surg. 2020;46(10):1451–1452. doi:10.1097/j.jcrs.0000000000000386
31. Yuan Y, Chen Y. Reply: does phorcides software yield inferior topography-guided LASIK accuracy versus targeting the manifest astigmatism? J Refract Surg. 2022;38(11):751. doi:10.3928/1081597X-20221026-02
32. Wallerstein A, Gauvin M. Does phorcides software yield inferior topography-guided LASIK accuracy versus targeting the manifest astigmatism? J Refract Surg. 2022;38(11):750. doi:10.3928/1081597X-20221026-01
33. Wallerstein A, Gauvin M. Comment on: clinical and refractive outcomes after topography-guided refractive surgery planned using Phorcides surgery planning software. J Cataract Refract Surg. 2022;48(12):1478–1479. doi:10.1097/j.jcrs.0000000000001068
34. Brunson P, Mann PM, Mann PM, Potvin R. Comparison of refractive and visual acuity results after Contoura® Vision topography-guided LASIK planned with the phorcides analytic engine to results after wavefront-optimized LASIK in eyes with oblique astigmatism. PLoS One. 2022;17(12):e0279357. doi:10.1371/journal.pone.0279357
35. Motwani M. Predictions of residual astigmatism from surgical planning for topographic-guided LASIK based on anterior corneal astigmatism (LYRA Protocol) vs the phorcides analytic engine. Clin Ophthalmol. 2020;14:3227–3236. doi:10.2147/OPTH.S272085
36. El Awady HE, Ghanem AA, Saleh SM. Wavefront-optimized ablation versus topography customized ablation in myopic LASIK: comparative study of higher order aberrations. Ophthalmic Surg Lasers Imaging. 2011;42(4):314–320. doi:10.3928/15428877-20110421-01
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Patient-Reported Dry Eye Outcomes After Myopic Femtosecond-LASIK: A 6-Month Prospective Analysis
Rush S, Pickett CJ, Rush RB
Clinical Ophthalmology 2023, 17:2141-2147
Published Date: 25 July 2023
Patient Reported Visual Outcomes, Dry Eye Symptoms, and Satisfaction Following Topography-Guided LASIK
Brunson PB, Mann II PM, Hall B
Clinical Ophthalmology 2025, 19:3363-3369
Published Date: 12 September 2025
Multi-Site Study of Patient Reported Vision Quality and Dry Eye Following LASIK
Lobanoff MC, Mann II PM, Parikh M, Brenner J, Hall B
Clinical Ophthalmology 2026, 20:566803
Published Date: 21 March 2026