")
Back to Journals » Patient Preference and Adherence » Volume 17
Topical Corticosteroid Phobia Among Parents of Children with Atopic Dermatitis (Eczema)- A Cross-Sectional Study
Authors Albogami MF , AlJomaie MS, Almarri SS, Al-Malki S, Tamur S, Aljaid M, Khayat A, Alzahrani A
Received 23 August 2023
Accepted for publication 26 October 2023
Published 2 November 2023 Volume 2023:17 Pages 2761—2772
DOI https://doi.org/10.2147/PPA.S431719
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Video abstract of "Topical corticosteroid phobia" [ID 431719].
Views: 209
Maha Fayez Albogami,1 Muneer S AlJomaie,2 Saad Saleh Almarri,3 Sultan Al-Malki,4 Shadi Tamur,4 Maryam Aljaid,4 Abdullah Khayat,4 Ahmad Alzahrani4
1College of Medicine, Taif University, Taif, Saudi Arabia; 2Department of Pediatrics, Taif Children Hospital, Taif, Saudi Arabia; 3Department of Pediatrics, Ministry of Health, Taif, Saudi Arabia; 4Department of Pediatrics, College of Medicine, Taif University, Taif, Saudi Arabia
Correspondence: Ahmad Alzahrani, Email [email protected]
Background: Anxiety about using topical corticosteroids (TCS) for childrens among parents and caretakers is a common cause of treatment failure and an overall decline in the child’s quality of life. The purpose of this study was to examine the perspectives and worries of parents of Atopic dermatitis (AD) children regarding TCS. Additionally, we investigate the degree of phobia in relation to the use of the TCS.
Materials and Methods: A convenience sample of 301 parents of children who had been identified with atopic dermatitis from two hospitals in Taif city were enrolled in this study. Parents who chose to participate were sent a questionnaire measuring their level of fear of TCS using the TOPICOP© scale, which also included inquiries about their demographics and clinical characteristics. Multivariate analysis was used to determine what factors influence people’s overall levels of fear.
Results: The median global TOPICOP score was 66.6% (IQR 60.4– 75%), SD 12.83%, which showed that nearly two-thirds of the participants showed corticosteroid phobia. A multifactorial ANOVA model showed that parents who had a female child with AD and mothers who had experienced drug allergies had a significant influence on TOPICOP scores (P< 0.05).
Conclusion: Topical corticosteroid phobia is widespread among parents of children patients with AD in Taif. Regarding the utilization of TCS, we place a strong emphasis on the significant role that physicians play as sources of reliable information and proper education.
Keywords: atopic dermatitis, caregivers, steroid phobia, topical corticosteroid
Introduction
Atopic dermatitis (AD) is an inflammatory skin disease characterized by itching and redness in multiple skin areas.1 The exact pathogenesis of AD is unknown, but it has been suggested that an interaction between genetic and environmental factors causes it. Environmental factors are associated with both local and systemic immune dysregulation in patients with AD who have a compromised skin barrier due to genetic predisposition.2–4 TCS remain an important component of therapy, and when used appropriately, TCS is highly effective, has a low relapse rate, and causes few local and systemic adverse effects. However, many parents of children affected by AD had significant fear and anxiety about using it,5,6 which causes therapeutic failures due to poor adherence. The Topical Corticosteroids phobia (TCP) may have a significant impact on the everyday activities of the parents of children patients with AD, in particular, due to the fact that the age at which AD is most common is also the age at which the parent-child bond is at its most profound. The identification of TCP is thus an essential step in treating patients with AD.7,8
Due to rapid urbanization in recent years, the prevalence of AD has significantly increased in Saudi Arabia, which has imposed a burden on children and their caregivers and the healthcare system.9,10 Many studies showed the phobia might be increased by the information displayed on the Internet, social media, among family, friends, and even information provided by medical professionals about the long-term use of TCS.11–13 TOPICOP is a tool used to measure corticosteroid phobia, which has excellent psychometric properties and should be easy to use in everyday clinical practice for clinicians and researchers.7,14 The widespread fear of steroids has made people hesitant to use TCS, which has exacerbated the disease.15 The development of efficient health education programs that can target appropriate communities and reduce TCP depends on a thorough understanding of the specific characteristics and causes that generate fear among people regarding TCS usage. Thus this study aimed to assess the degree of local corticosteroid phobia and to assess the parent’s knowledge about atopic dermatitis in Taif, Saudi Arabia.
Materials and Methods
This multicenter study was conducted in two hospitals (Alhada Armed Forces hospital and Children hospital) in Taif city, Saudi Arabia. A convenience sample of 301 parents of children who suffered from AD who attended the outpatient department of these two hospitals from 23 January to 28 April 2021 was included in our study. The participants were explained about the need and benefits of the study, and consent was taken. Ethical approval was taken from the Research and Ethics Committee of Taif University (Application number 42–159). Permission was also taken from the administration of two hospitals were taken to collect responses from the parents. We have confirmed in our revised manuscript that our study complies with the Declaration of Helsinki.
The data was collected from all parents of children with AD using a validated questionnaire (TOPICOP).16 In all cases, the patient’s allergist confirmed the AD diagnosis. Therefore, all patients with AD were included, and parents were asked to fill out the self-filling questionnaire for their affected children under 16 years old.
The questionnaire was originally developed in English; however, it was translated into Arabic and then back-translated into English by an independent expert person who had excellent proficiency in both languages in order to ensure translation accuracy. The translated questionnaire was initially pilot tested on 25 parents of children with atopic dermatitis to discover and overcome any issues in the questionnaire.
The questionnaire is divided into four parts. The first part had a written explanation of the study as well as a consent form that had to be signed by the respondent. At the same time, the second part of the questionnaire included the patient’s sociodemographic data, dermatological condition, and previous prescription of TCS. The third part had items concerned with patients who had been prescribed topical steroids only, where they were additionally asked to comment on whether they had benefitted from their use and if they had experienced any side effects. Finally, the last part included the TOPICOP© score items.
Data Management and Statistical Analysis
After gathering the responses from the participants, it was then entered in a Microsoft excel sheet and subjected to statistical analysis using the SPSS software version 27 (IBM Corp. USA). Frequency and percent were used as descriptive statistics for categorical variables such as gender, age, and educational level. Mean, standard deviation (SD), and median with interquartile range (IQR) were used as descriptive statistics depending on the normality of data for presenting continuous variables and the scores of TOPICOP items. TOPICOP questionnaire included 12 questions with a 4-point Likert scale with possible answers of strongly disagree (0), disagree (1), agree (2), and strongly agree (3). Six items in the questionnaire assessed the parents’ knowledge and beliefs toward using a topical corticosteroid, three items assessed the parents’ fear of topical corticosteroid, and three items assessed their behavior toward its use with possible scores of Knowledge and beliefs, fears, behavior, and Global TOPICOP score of 18, 9, 9, and 36 respectively. In representing these scores, the percent of score according to possible score used representing scores up to 100 for each scale (a higher score represents higher negative beliefs and a high level of worry).16 Students’ t-test and Analysis of variance (ANOVA) were used to compare the TOPICOP item scores between different categorical variables. A significance value (p-value) was set at <=0.05.
Results
Our analysis included responses from 301 parents who had children diagnosed with AD. The socio-demographic analysis showed that 163 (54.2%) were male children, 137 (45.5%) were aged 1–5 years, and 74 (24.6%) were between 6–10 years. About 136 (45.2%) of the mothers belonged to the age group of 20–29 years, and 137 (45.5%) of the fathers had the age of 30–39 years. Considering the educational level of mothers and fathers, 45.2% of mothers had a bachelor’s degree, and 37.2% had secondary school. In comparison, 54.8% of fathers had a bachelor’s and 26.2% had a secondary school level of education (Table 1). The assessment of the history of allergies showed that 23.3% of fathers and 19.9% of mothers suffer from asthma, while 24.6% of mothers and 24.3% of fathers suffer from allergic rhinitis. In addition, Food allergy and drug allergies were reported in 18.9% and 13.3% of mothers and 16.5% and 11.3% of fathers. Moreover, 23.3% of mothers and 15.9% of fathers had eczema (Table 2).
 |
Table 1 The Demographic Factors of Children and Their Parents |
 |
Table 2 Parental History of Different Allergy as Reported by the Participants |
The assessment of the history of allergies among children, as reported by the parents, revealed that 23.9% of the children were diagnosed with eczema at an age lower than three months, while 27.6% in age between 3–6 months, and 17.9% were between 6–12 months indicated that 69.4% of children were diagnosed with eczema at an age younger than one year. 36.2% of parents described the eczema condition of their children as stable, and 36.2% were getting better. Considering other allergies, 27.2% of children suffer from a food allergy, 26.2% from asthma, 23.6% from allergic rhinitis, and 13% from drug allergy (Table 3).
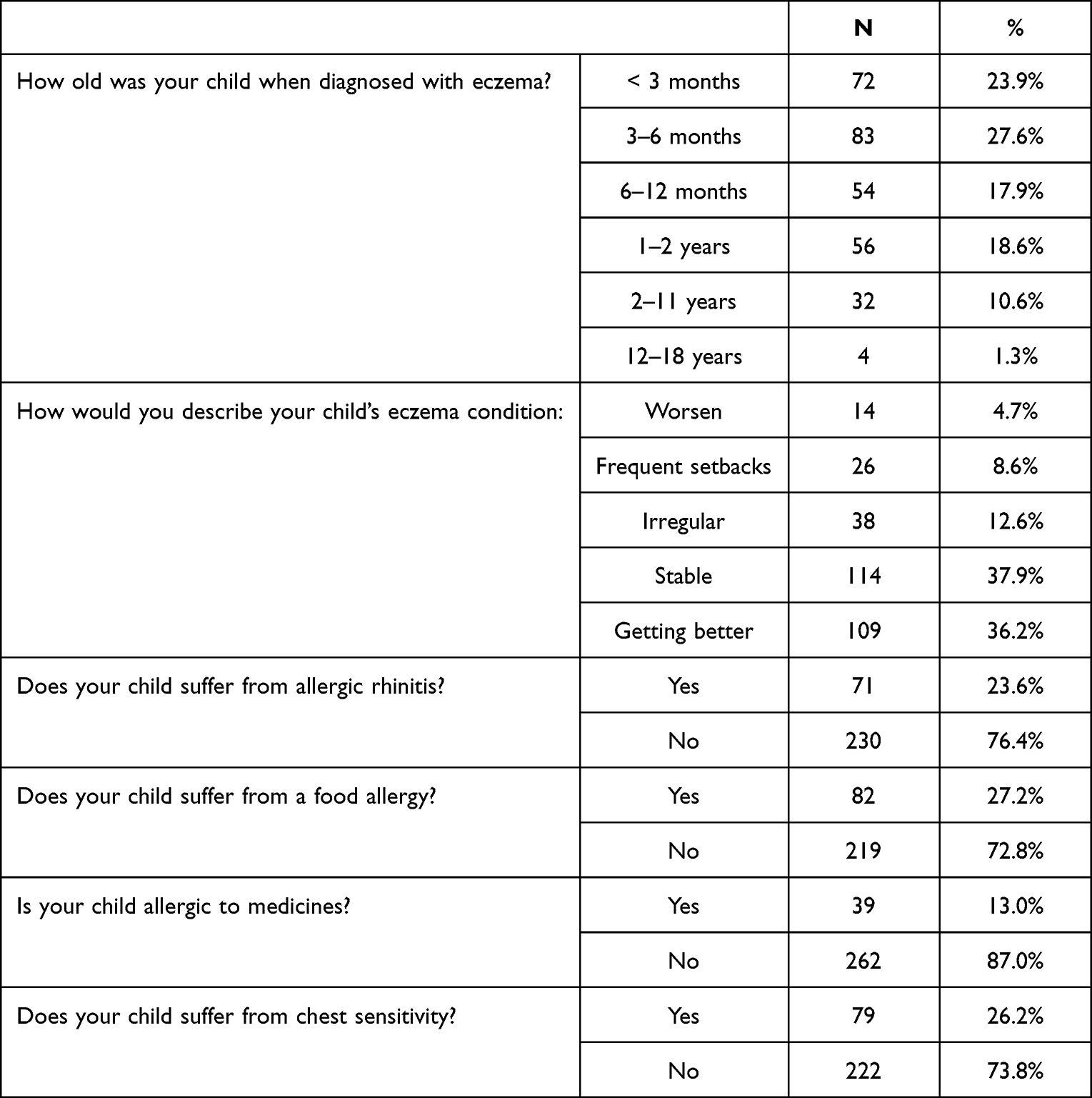 |
Table 3 Child History of Allergy According to Parents |
The practices towards management of child eczema among parents showed that 45.8% of the parents would always use moisturizing creams on their child’s eczema. In comparison, 27.2% of them reported that they always prevent their children from certain foods because of eczema, and 35.9% reported sometimes. Considering TCS usage, 26.2% reported always using them, while 51.8% sometimes reported patterns, and 6% never used them. Natural oils were never used by 22.9% of parents; 22.3% reported rarely using them, while 24.6% reported always using them (Figure 1).
 |
Figure 1 Parental Practices Toward Management of Child’s Eczema. |
The items in the TOPICOP were classified based on the three aspects measured: Knowledge and beliefs, Fears, and Behaviors. The median score for Knowledge and beliefs was found to be 62.5% (IQR 50–75%) with an SD of 16.4%. For the subdomain “Fears”, the median score was 75% (IQR 58.3–83.3%) SD 9.71%, and for “Behaviors”, it was found to be 75% (IQR 66.6–44.4%), SD 9.3%. The median global TOPICOP score was 66.6% (IQR 60.4–75%), SD 12.83% (Table 4).
 |
Table 4 Questionnaire Components on Degree of Topical Steroid Phobia |
The questionnaire also had supplementary questions pertinent to our local context. It was observed that 30.2% and 25.9% of the parents strongly agree with the effectiveness of TCS in short and long periods, respectively. About 25.2% of them strongly agreed that TCS becomes useless after repeated use. The majority of the participants believed that TCS treats the symptoms and does not treat the cause. It was found that 43.8% agreed that TCS makes eczema worse. Moreover, 70.5% of the participants were afraid of using TCS despite not knowing its side effects, and 74.8% of them have a fear of using TCS on their children for long periods. Considering using of TCS, it was observed that 21.6% of the participants reported that they did not follow physicians’ instructions for using TCS. The main fears of TCS were fear that TCS cream getting into the child’s mouth and fear that, in the long term, it would change the color of his skin or deform it. Furthermore, 45.5% of the participants reported that they faced some side effects from using TCS, and 44.5% stopped using it because of these side effects (Table 5).
 |
Table 5 Additional Questions Related Knowledge, Beliefs, Fear and Practices Related to Use Topical Corticosteroid in the Treatment of Their Child’s Eczema |
The comparison of the Global TOPICOP and subdomain scores based on different socio-demographic variables is given in Table 6. The mean Global TOPICOP score was found to be 48 ± 32.23. It was found that mean scores for all the domains except for fears were significantly higher among parents who had a female child with AD, where the Global TOPICOP was found to be comparatively higher in parents of female children (33.57 ± 5.79) than male children (31.27 ± 6.29), p<0.05. There were no statistically significant differences observed between Saudi and non-Saudi parents for TOPICOP scores except for the subdomain Knowledge and beliefs, which was significantly higher in non-Saudi parents (p=0.038). The global TOPICOP scores were found to be significantly higher among parents who had children aged 6–10 years (33.89 ± 6.68) and 10–15 years (33.77± 7.06) compared to the lower age group (p=0.012). No statistically significant differences were found for global TOPICOP scores between different educational levels of mothers and fathers. The global TOPICOP and the three subdomains were significantly higher among those who relied on the internet as a reliable source of information about topical corticosteroids (p<0.05). Similarly, the scores for global TOPICOP and the three subdomains were significantly higher in parents who agreed that they worried about the information that friends and family share with them about TCS and its damages (p<0.05). Also, the severity of eczema in a child did not show any significant differences in global TOPICOP and the three subdomains scores (p>0.05) (Table 6).
 |
Table 6 Comparison of TOPICOP Scores Between Different Participants Characterize |
A factorial ANOVA model was performed to see the effect of independent categorical variables on the Global TOPICOP scores (dependent variable). The analysis showed that only the gender of the child (female) had a significant influence on the Global TOPICOP score with a small size effect (F(1300) =7.319, ηp2 =2,6%, p = 0.007). Also, the drug allergy in the mother significantly influenced the global TOPICOP scores with a very small size effect (F(1300) =2.752, ηp2 =1.0%, p = 0.048). All other independent variables did not have an influence on the Global TOPICOP scores in this model (p>0.05) (Table 7).
 |
Table 7 Factorial ANOVA |
Discussion
The current research shows that widespread anxiety about TCS exists in Taif among the families of pediatric patients with AD. In Saudi Arabia, there has been a lack of research evaluating TCP in caregivers of AD-affected children. Adherence to TCS can be improved by investigating the factors affecting TCP. Numerous studies evaluating TCP in individuals with AD or their parents have found that it is widespread and negatively affects adherence.14,17,18 Our research also indicates that worrying about using too much cream contributes to a fear of TCS. Thus, TCP may set off a cascade of events that ultimately leads to treatment failure: decreased compliance leading to lengthy and frequent relapses, which in turn leads to weakened confidence in the treatment and ultimately decreased compliance. However, the term “corticosteroid phobia” itself may be misleading. Irrational fear is what defines a phobia. Parents have a legitimate reason to be fearful of TCS due to warnings from many different sources, including peers, family, the internet, and even conventionally trusted sources like doctors and pharmacists. The right information given to parents is crucial. Patients learn about corticosteroids from their doctors, other medical professionals, family and friends, the media, journals, and the internet,11,19,20 with doctors being the primary knowledge source.21
Our findings suggest that parents’ fear and anxiety about TCS are not grounded in rational considerations. Nevertheless, the majority of the participants in this study reported that, in their opinion, TCS is dangerous regardless of the particular side effects and that the treatment’s drawbacks are not outweighed by its benefits. Previous research has found that cutaneous side effects and failure to thrive are the primary concerns with TCS.8,11,22 Several studies emphasized the significance of the doctor-patient relationship in alleviating concerns about TCS.8,18,22,23 In the research, we limited our analysis to examining how the need for reassurance from the patient’s doctor was associated with TCS fear, and we did not observe any significant relationship between the two. However, as our findings show that TCP is aimed directly at treatment safety, it is imperative that family pediatricians and physicians devote a regular portion of their consultation time to determining patients’ concerns and worries about TCS. This will allow them to dispel myths and increase their patients’ trust in the treatment and their compliance with it by providing them with reliable information. The findings of this study revealed that a majority of parents had received further education on how to manage their child’s AD. However, education did not appear to alleviate individuals’ TCS-related anxiety. Evidence shows that parents who initially demonstrated steroid phobia were more likely to report finding education helpful and to show improved perceptions of TCS. There is evidence to suggest that parents whose attitudes toward TCS steroids initially appeared unfavorable were more likely to report finding therapeutic education beneficial and to demonstrate improved perceptions after receiving such therapeutic education.19 The findings of Lee et al19 demonstrated that a simple therapeutic education, such as a dermatologist leading a patient counseling session on TCS for 10–15 minutes, increased compliance among patients.
A multifactorial ANOVA model showed that parents who had a female child with AD and mothers who had drug allergies had a significantly high phobia. It can be argued that parents of the female child could be more concerned about AD as it may have a negative impact on their social life and future.24 It is also reported that girls were more embarrassed, self-conscious, upset, and sad because of AD.25 We can also hypothesize that it is more challenging for females to present in class with symptoms of AD because they are more focused on social aspects of school life, including body image, compared to males.26 This could be a possible explanation for the higher TCP among parents of the female child. However, our findings did not show any significant relationship between the severity of eczema and TOPICOP scores. This is similar to the findings of previous studies, which reported that severity is not related to TCP.8,11,18,22 Improved family education could possibly reduce medical costs and disease burden, as suggested by a study on Danish children that outlined the relationship between parental-reported healthcare utilization, medication consumption, and TCP and pediatric AD severity and found that a high global TOPICOP score and low parental educational level resulted in delayed treatment of AD flares.27
This research does have limitations. First, due to the limited sample size, the results may be biased and cannot accurately represent the characteristics of the entire population of Saudi Arabia. Second, there is the likelihood of social desirability bias due to the fact the findings were based on self-reporting, making it impossible to provide neutral data related to actual TCS usage. Third, there is the possibility that socioeconomic position, attitude, doctor-patient relationship, inconsistencies in information obtained, and individual doctors’ perspectives on TCS could all have played a role in the findings. Finally, it’s important to examine how educating parents about TCS through novel media works and what impact it has on parents. Therefore, more research is needed to examine the effects of parental education on improving results.
Conclusion
Our findings corroborated the high prevalence of corticosteroid phobia among parents of patients with AD, which negatively affects medication adherence. Physicians should investigate the meaning of this fear and work with the parents of children with AD to help them get over their fear of steroids so that they can effectively follow treatment guidelines. The concerned children and/or their families are severely impacted by the effects of atopic dermatitis. Inappropriate disease management, resulting in unnecessary suffering for children and their parents, is a direct consequence of low levels of compliance. Treatment anxiety, especially regarding TCS, is understandable due to the prevalence of misleading information, much of which originates from friends, relatives, and pharmacists. Physicians can further alleviate their patients’ concerns and improve their quality of life by first empathizing with the parents who are experiencing the skin condition.
Acknowledgments
The authors would like to acknowledge the ethics committee of Taif University. The researchers would like to acknowledge the Deanship of Scientific Research, Taif University for funding this work. The authors would like also to extend their sincere thanks to the High Altitude Research Center at Taif University. Furthermore, we would like to express our gratitude to the Alhada Armed Forces Hospital and Taif Children Hospital administrations for facilitating data collection.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Deckers IA, McLean S, Linssen S, Mommers M, van Schayck CP, Sheikh A. Investigating international time trends in the incidence and prevalence of atopic eczema 1990–2010: a systematic review of epidemiological studies. PLoS One. 2012;7(7):7. doi:10.1371/journal.pone.0039803
2. Leung DY. New insights into atopic dermatitis: role of skin barrier and immune dysregulation. Allergol Int. 2013;62(2):2. doi:10.2332/allergolint.13-RAI-0564
3. Konstantinou GN, Konstantinou GN, Koulias C, Petalas K, Makris M. Further understanding of neuro-immune interactions in allergy: implications in pathophysiology and role in disease progression. J Asthma Allergy. 2022;15:1273–1291. doi:10.2147/JAA.S282039
4. Gaspar NK, Aidé MK. Atopic dermatitis: allergic dermatitis or neuroimmune dermatitis? An Bras Dermatol. 2016;91(4):479–488. doi:10.1590/abd1806-4841.20164211
5. Lambrechts L, Gilissen L, Morren M. Topical corticosteroid phobia among healthcare professionals using the TOPICOP score. Acta Derm Venereol. 2019;99(11):1004–1008. doi:10.2340/00015555-3220
6. El Hachem M, Gesualdo F, Ricci G, et al. Topical corticosteroid phobia in parents of pediatric patients with atopic dermatitis: a multicentre survey. Ital J Pediatr. 2017;43(1):22. doi:10.1186/s13052-017-0330-7
7. Stalder JF, Aubert H, Anthoine E, et al. Topical corticosteroid phobia in atopic dermatitis: international feasibility study of the TOPICOP score. Allergy Eur J Allergy Clin Immunol. 2017;72(11):1713–1719. doi:10.1111/all.13189
8. Aubert‐Wastiaux H, Moret L, Le Rhun A, et al. Topical corticosteroid phobia in atopic dermatitis: a study of its nature, origins and frequency. Br J Dermatol. 2011;165(4):808–814. doi:10.1111/j.1365-2133.2011.10449.x
9. Fatani MI, Al Sheikh AA, Alajlan MA, et al. National Saudi Consensus statement on the management of atopic dermatitis (2021). Dermatol Ther. 2022;12(7):1551–1575. doi:10.1007/s13555-022-00762-6
10. Alakeel A, Al Sheikh A, Alraddadi AA, et al. Management of atopic dermatitis in adults in Saudi Arabia: consensus recommendations from the Dermatological Expert Group. Clin Cosmet Investig Dermatol. 2022;15:1435–1445.
11. Charman CR, Morris AD, Williams HC. Topical corticosteroid phobia in patients with atopic eczema. Br J Dermatol. 2000;142(5):931–936. doi:10.1046/j.1365-2133.2000.03473.x
12. Saito-Abe M, Futamura M, Yamamoto‐Hanada K, Yang L, Suzuki K, Ohya Y. Topical corticosteroid phobia among caretakers of children with atopic dermatitis: a cross-sectional study using TOPICOP in Japan. Pediatr Dermatol. 2019;36(3):311–316. doi:10.1111/pde.13784
13. Bos B, Antonescu I, Osinga H, Veenje S, Jong K, Vries TW. Corticosteroid phobia (corticophobia) in parents of young children with atopic dermatitis and their health care providers. Pediatr Dermatol. 2019;36(1):100–104. doi:10.1111/pde.13698
14. Mueller SM, Itin P, Vogt DR, et al. Assessment of “corticophobia” as an indicator of non‐adherence to topical corticosteroids: a pilot study. J Dermatolog Treat. 2017;28(2):
15. Chin HW, Jang HS, Jang BS, et al. A study on utilization of alternative medicine for patients with atopic dermatitis. Korean J Dermatol. 2005;43(7):903–911.
16. Moret L, Anthoine E, Aubert-Wastiaux H, et al. TOPICOP©: a new scale evaluating topical corticosteroid phobia among atopic dermatitis outpatients and their parents. PLoS One. 2013;8(10):e76493. doi:10.1371/journal.pone.0076493
17. Krejci-Manwaring J, Tusa MG, Carroll C, et al. Stealth monitoring of adherence to topical medication: adherence is very poor in children with atopic dermatitis. J Am Acad Dermatol. 2007;56(2):
18. Smith SD, Hong E, Fearns S, Blaszczynski A, Fischer G. Corticosteroid phobia and other confounders in the treatment of childhood atopic dermatitis explored using parent focus groups. Australas J Dermatol. 2010;51(3):
19. Lee JY, Her Y, Kim CW, et al. Topical corticosteroid phobia among parents of children with atopic eczema in Korea. Ann Dermatol. 2015;27(5):
20. Gustavsen HE, Gjersvik P. Topical corticosteroid phobia among par- ents of children with atopic dermatitis in a semirural area of Norway. J EurAcad Dermatol Venereol. 2016;30(1):168. doi:10.1111/jdv.12670
21. Li AW, Yin ES, Antaya RJ. Topical corticosteroid phobia in atopic dermatitis a systematic review. JAMA Dermatol. 2017;153(10):
22. Hon KL, Kam WY, Leung TF, et al. Steroid fears in children with eczema. Acta Paediatr. 2006;95(11):11. doi:10.1080/08035250600612298
23. Fischer G. Compliance problems in paediatric atopic eczema. Australas J Dermatol. 1996;37(Suppl 1):S10–S13. doi:10.1111/j.1440-0960.1996.tb01070.x
24. Faught J, Bierl C, Barton B, Kemp A. Stress in mothers of young children with eczema. Arch Dis Child. 2007;92(8):683–686. PMID: 17412743; PMCID: PMC2083902. doi:10.1136/adc.2006.112268
25. Datta D, Sarkar R, Podder I. Parental stress and quality of life in chronic childhood dermatoses: a review. J Clin Aesthet Dermatol. 2021;14(9 Suppl 1):S19–S23.
26. Chernyshov PV, Ho RC, Monti F, et al. Gender differences in self-assessed health-related quality of life in children with atopic dermatitis. J Clin Aesthet Dermatol. 2016;9(8):19–24.
27. Gerner T, Haugaard JH, Vestergaard C, et al. Healthcare utilization in Danish children with atopic dermatitis and parental topical corticosteroid phobia. Pediatr Allergy Immunol. 2021;32(2):331–341. doi:10.1111/pai.13394
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.