Back to Journals » Cancer Management and Research » Volume 13
Topical Application of Pseudomonas aeruginosa-Mannose Sensitive Hemagglutinin (PA-MSHA) for Refractory Lymphatic Leakage Following Lymphadenectomy in Patients with Gynecological Malignancies
Authors Zhou R, Xu J, He J ![]() , Gong Y, Wang H, Linghu H
, Gong Y, Wang H, Linghu H
Received 21 February 2021
Accepted for publication 20 May 2021
Published 21 June 2021 Volume 2021:13 Pages 4873—4878
DOI https://doi.org/10.2147/CMAR.S307700
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Alexandra R. Fernandes
Rong Zhou,* Jie Xu,* Jingke He, Yao Gong, Hui Wang, Hua Linghu
Department of Obstetrics & Gynecology, The First Affiliated Hospital of Chongqing Medical University, Chongqing, 400016, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hua Linghu
Department of Obstetrics and Gynecology, The First Affiliated Hospital of Chongqing Medical University, Chongqing, 400016, People’s Republic of China
Tel +86-23-89011090
Fax +86-23-68811487
Email [email protected]
Purpose: To observe the feasibility and efficacy of Pseudomonas aeruginosa-mannose sensitive hemagglutinin (PA-MSHA) in refractory lymphatic leakage following lymphadenectomy among patients with gynecological cancers.
Patients and Methods: Ten cases with post-operative massive lymphatic leakage were collected, in which patients failed to respond to conservative treatment. Topical PA-MSHA injection of a single dose (2mL) was performed through drainage tube or transvaginal catheter into pelvic or peritoneal cavity. Drainage volumes and side effects were recorded.
Results: The incidence of refractory lymphatic leakage following pelvic and para-aortic lymphadenectomy was 2.44% (10/409). All ten patients (100%) had quick recovery and were discharged within 72 hours. Among them, one patient (10%) experienced fever and six patients (60%) experienced abdominal pain, one of which was moderate and relieved by routine analgesic treatment. During 11 (6– 38) months of follow-up time, no long-term side effect was observed.
Conclusion: Topical injection of PA-MSHA of a single dose appears a feasible and effective treatment for refractory post-operative lymphatic leakage.
Keywords: Pseudomonas aeruginosa-mannose sensitive hemagglutinin (PA-MSHA) injection, pelvic and para-aortic lymphadenectomy, lymphatic leakage, chylous leakage
Introduction
Post-operative lymphatic or chylous leakage following lymph node dissection is an iatrogenic complication, of which the two main leading causes are the injuries of lymphatic vessels and the consequent differential pressure.1,2 The interruption of lymphatic circulation causes the differential pressure between the crevasse and its surrounding space, thus making lymphatic fluid leak out into the interstitial space or coelomic cavity. Patients often present with increased pelvic/abdominal drainage output or vaginal discharge, and a few complaints of abdominal distension. The discharge is usually characterized by clear yellow liquid or milky appearance, and the latter is caused by injuries of lacteal ducts, namely chylous leakage. In clinical practice, lymphatic and chylous leakage are administrated in similar management with similar pathogenesis and symptoms. With the spread of laparoscopy and harmonic scalpel techniques, the lymphatic leakage could be transiently blocked during the operation by the effect of carbon dioxide (CO2) pressure and the coagulation of lymphatic vessels, making it challenging to immediately notice the leakage.3 The difficulties in diagnosis and lack of consensus of diagnosis contribute to poor recognition of lymphatic leakage.
With significant prolonged hospitalization and discomfort, attention to this complication has been recently raised in those gynecological cancer patients who received laparoscopic lymphadenectomy.4 Conservative treatments, including fat-free diet, parenteral nutrition, and drainage, are partially effective with prolonged hospital stay but less efficient in those refractory cases. Several successful surgeries have been reported,5,6 but surgical treatment is still controversial with demands for surgical technical at a high level and difficulties in identifying leakage sites at re-operated fields. Consequently, optimal treatments towards lymphatic leakage are still in need.
PA-MSHA has been recently identified as an immune modulator and anti-cancer reagent against malignancies.7–9 In the present study, PA-MSHA was introduced to ten patients with refractory lymphatic leakage, according to successful treating experience in lymphatic leakage following neck dissection.10,11 The efficacy and side effects of PA-MSHA were observed to provide further evidence for lymphatic leakage treatment in clinical practice.
Patients and Methods
Clinical Data
From January 2017 to September 2019, ten gynecological cancer patients with similar lymphadenectomy extent were collected who developed massive lymphatic/chylous leakage following laparoscopic lymphadenectomy and failed to respond to conservative treatments. The cancer type, patients’ age, the extent of surgery, the peak volume per day before treatment, chyle test results, and previous treatment modalities were recorded (Table 1). Informed consent was acquired from each patient. This study was conducted in accordance with the Declaration of Helsinki and all experimental protocols were approved by the Committee of the First Affiliated Hospital of Chongqing Medical University.
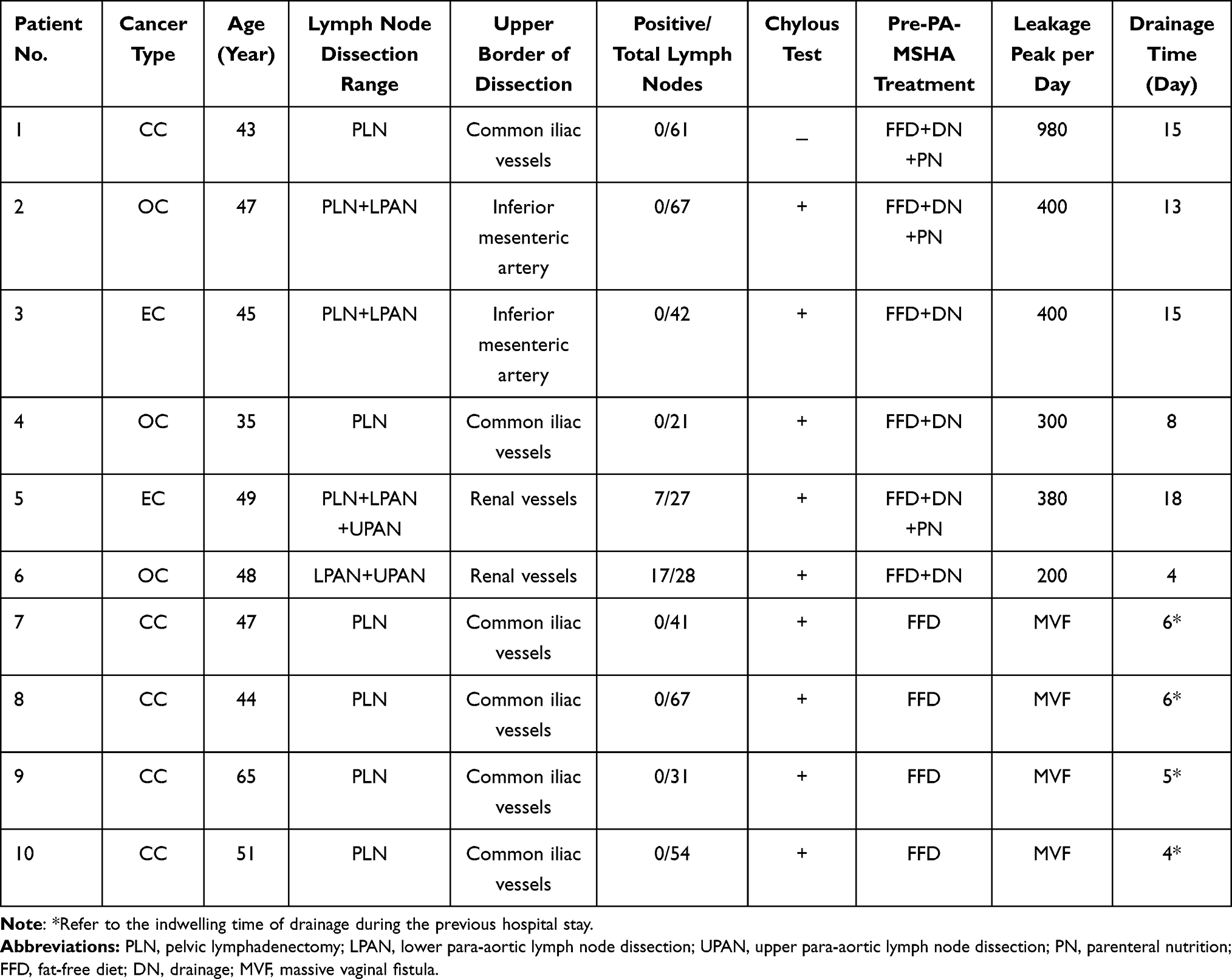 |
Table 1 Patients’ Demographics and Clinical Characteristics |
Lymphadenectomy
According to NCCN guidelines and Clinical Practice Guidelines in Gynecological Oncology, the lymph node dissection range was decided depending on patients’ physical status as well as pre-operative radiographic data. The pelvic lymphadenectomy (PLN) includes the pelvic lymph node region with upper border of common iliac vessels. The lower para-aortic lymph node dissection (LPAN) includes the para-aortic lymph node region with upper border of the inferior mesenteric artery. The upper para-aortic lymph node dissection (UPAN) includes the para-aortic lymph node region with upper border of renal vessels. Lymphadenectomy extent, number, and upper border of each patient are illustrated in Table 1.
Diagnostic Criteria
The diagnosis of lymphatic leakage should be considered based on massive abdominal/pelvic drainage or vaginal discharge (>200 mL per day or >1000 mL in total) with the appearance of clear yellow or milky liquid and the symptom of abdominal distension. The diagnosis of refractory lymphatic leakage should be considered in a situation where conservative treatments, including drainage, parenteral nutrition, and fat-free diet, were received but ineffective (persistent drainage or discharge without obvious decreases (decrease <50mL)). Lymphatic leakage with a positive chyle test result further supports the diagnosis of chylous leakage.12
Treatment of Pseudomonas aeruginosa Injection
The medication of Pseudomonas aeruginosa-mannose sensitive hemagglutinin (PA-MSHA) was produced by Beijing Wanteer Biopharmaceutical Company Limited (co., Ltd.), with the trade name Wantepu ’An, (1.0mL/ dose), which contains a total bacteria count of 1.6×109~2.0×109 per mL. For patients with retained indwelling drainage, 2.0 mL undiluted PA-MSHA with 30 mL of normal saline was injected through the drainage tube into the pelvic cavity, which were then clamped for 24 hours to prevent medication leakage and re-opened after that. When drainage was less than 20 mL/d with a normal diet, the tube was removed and the patient was then discharged. For patients without indwelling drainage retained, the PA-MSHA injection was performed after transvaginal catheterization (16F). Six hours’ immobilization was instructed to prevent the medicine leakage. Once the injection was started, no diet modification would be performed. All methods were carried out in accordance with relevant references.10,11
Results
Ten gynecological cancer patients with similar lymphadenectomy extent were collected who developed massive lymphatic/chylous leakage following laparoscopic lymphadenectomy and failed to respond to conservative treatments. The incidence of refractory lymphatic leakage was 2.44% (10/409). Among 10 refractory cases, four patients presented with massive vaginal leakage after being discharged. With iatrogenic urinary tract injuries and infection excluded, they were then readmitted 11–21 days after operation. The other six cases were noted because of a persistent large amount of drain output (200–1000mL/d) during hospitalization. After PA-MSHA injection, leakage outputs of each patient were regularly recorded, which turned out to be timely and satisfactorily decreased. The four readmitted patients with the massive vaginal discharge had their discharge amount significantly reduced 6–8 hours after injection. Symptoms of discharge turned to be vaginal spotting within 24 hours and completely stopped within 72 hours. The other six patients with retained tubes had their drain output significantly reduced and had their pelvic drainage tube removed within 48 hours. All patients (100%) had quick recovery and were discharged within 72 hours. The follow-up time ranged from 6–38 months, of which the median is 11 months. During the follow-up time, there was not any fluid in the abdominal or pelvic cavity observed through regular ultrasound tests.
Medication-associated side effects were observed and recorded (Table 2), and there were no severe complications observed during follow-up. Six patients had abdominal pain after PA-MSHA administration: one patient (10%) complained of moderate abdominal pain which was relieved by analgesic treatment of tramadol injection; Five patients (50%) had mild abdominal pain which was spontaneously ameliorated an hour later without treatment. Only one patient (10%) had fever four hours after PA-MSHA injection which was relieved after physical cooling therapy. Four patients (40%) experienced an uneventful recovery without any discomfort. No medication-related allergy was observed, and no patient was found to be complicated with infection, necrosis, hematoma, and wound dehiscence. During the follow-up time, no long-term side effects occurred in any patient.
 |
Table 2 PA-MSHA Treatment Outcomes |
Discussion
Lymphatic/chyle leakage following pelvic and para-aortic lymphadenectomy has been recently noticed in gynecological malignancies, of which the incidence is reported to be 1.20%-3.00%.13 The incidence of refractory cases, which fails to respond to conservative treatment, occupies more than half in the study of Chen et al among patients with neck dissection,10 was 2.44% in the present study.
Primarily recommended conservative treatments, including diet modification, persistent drainage, and octreotide therapy, are time-consuming and usually prolong hospital stay. Diet modification is reported to diminish chyle production and promote spontaneous fistula closure. Octreotide therapy mainly inhabits the secretion of multiple hormones and promotes chyle leakage closure potentially by decreasing blood flow to the hepatic, portal, and splanchnic circulation.14 In refractory cases where conservative modalities are less effective, patients suffer from indwelling tube-associated discomfort and develop metabolic, infective complications and malnutrition during long-term diet and drainage, which causes extra costs and threatens patients’ life quality. After the failure of conservative management, the effectiveness of surgical treatment, embolization under lymphangiography,15 and topical injection of PA-MSHA have been proved in the cases, among which the treatment of PA-MSHA has been a spotlight for its least invasiveness. In the present study, after the failure of conservative treatment as self-control, the feasibility and quick therapeutic effect of topical injection of PA-MSHA have also been proved towards refractory lymphatic leakage, similar to the promising results in neck dissection associated chyle fistula.10,11 Despite the common limitation in sample size, 100% cure rates were observed without any long-term side effects in three studies including ours, besides one patient being cured after a second injection.11
The medication of PA-MSHA has been genetically engineered originally as an immunoadjuvant against cancer.7–9 PA-MSHA can promote apoptosis of cancer cells by inhibiting proliferation, invasion, and migration by inducing immune cells,7–9 through activation of the hedgehog, EGFR, and PTEN/AKT pathway.16–18 The tenuous and upright fimbriae on its surface are recognized to activate immune response,10 which may play the role of plugging the stoma of the lymphatic fistula. PA-MSHA has also been reported to regulate inflammation and then ameliorate the prognosis of rats with septic shock.19,20 Induced inflammation by PA-MSHA is possibly another potential mechanism to treat lymphatic leakage through promotion of lymphatic vessels rehealing. But there is still a lack of related studies revealing specific therapeutic mechanisms towards lymphatic leakage.
Pelvic and para-aortic lymphadenectomy are essential parts of surgical staging for early-stage patients and cytoreduction for advanced-stage patients in gynecological malignancies. The safety of lymphadenectomy should be raised by effective treatment towards complications, as well as further strategies of prophylaxis, such as individualized lymph nodes dissection21 and sentinel lymph node mapping22 to avoid unnecessary dissections, and treatment of PA-MSHA before conservative management.23
The promising results of cure rate and acceptable side effects of this medication provide clinicians with a non-invasive, convenient, and economical treatment towards refractory lymphatic leakage. Future prospective studies with an enlarged sample size could be performed to further verify the feasibility of this medication and relevant pharmacological studies to explore the mechanism of treating lymphatic leakage.
To our knowledge, this is the first report regarding the application of PA-MSHA for lymphatic leakage in gynecological malignancies. Another strength of this study should be that follow-up work was done well and none of these patients were lost. Some limitations of this study should be considered. Since the incidence of refractory lymphatic leakage is low, the results of this study were compromised by the small sample size and retrospective nature. Despite these limitations, the high cure rate and quick effect through observation still encourage us to raise attention to this promising therapy.
Conclusions
The PA-MSHA appears a feasible and effective medication towards lymphatic leakage following pelvic and para-aortic lymphadenectomy in gynecological malignancies.
Acknowledgment
We thank Prof. Xin-Liang Su, in the Department of Endocrine and Breast Surgery, The First Affiliated Hospital of Chongqing Medical University, for his introduction of this medicine for such patients. This work was supported by grants from the National Natural Science Foundation of China (NSFC No. C81572562).
Author Contributions
Rong Zhou and Jie Xu contributed equally to this paper. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Pei-quan Li QL, Liu K-J, Sun Y-X, Zhao X-X, Xie L, Zhi-jun H. Risk factors and treatment of lymph leakage after laparoscopic gynecological malignant tumor lymph node dissection. Chin J Endosc. 2018. doi:10.1055/a-0658-5783
2. hao CHZE-. Prevention and management of lymphorrhea or chylorrhea after gastric surgeries. Chin J Pract Surg. 2017;37(4):355–358.
3. Han LP, Zhang HM, Abha HD, Liu T, Zhang XP. Management and prevention of chylous leakage after laparoscopic lymphadenectomy. Eur Rev Med Pharmacol Sci. 2014;18(17):2518–2522.
4. Frey MK, Ward NM, Caputo TA, Taylor J, Worley MJ
5. Shimajiri H, Egi H, Yamamoto M, Kochi M, Mukai S, Ohdan H. Laparoscopic management of refractory chylous ascites using fluorescence navigation with indocyanine green: a case report. Int J Surg Case Rep. 2018;49:149–152. doi:10.1016/j.ijscr.2018.06.008
6. Liu J, Zhang H, Du Q, Yao S. Successful laparoscopic treatment of chylous ascites after pelvic lymphadenectomy: a case report and peanut oil application. J Minim Invasive Gynecol. 2018;25(5):923–926. doi:10.1016/j.jmig.2017.12.028
7. Zhang C, Zhang Z, Wang L, et al. Pseudomonas aeruginosa-mannose sensitive hemagglutinin injection treated cytokine-induced killer cells combined with chemotherapy in the treatment of malignancies. Int Immunopharmacol. 2017;51:57–65. doi:10.1016/j.intimp.2017.08.003
8. Liu J, Duan X. PA-MSHA induces apoptosis and suppresses metastasis by tumor associated macrophages in bladder cancer cells. Cancer Cell Int. 2017;17:76. doi:10.1186/s12935-017-0445-3
9. Zhao X, Wu X, Yu W, et al. PA-MSHA inhibits proliferation and induces apoptosis in human non-small cell lung cancer cell lines with different genotypes. Mol Med Rep. 2016;14(6):5369–5376. doi:10.3892/mmr.2016.5869
10. Chen Q, Zou X, Ma Y, et al. Pseudomonas aeruginosa-mannose sensitive hemagglutinin injection therapy for the treatment of chyle fistula following neck dissection. Head Neck. 2020;42(4):725–731. doi:10.1002/hed.26054
11. Wei T, Liu F, Li Z, Gong Y, Zhu J. Novel management of intractable cervical chylous fistula with local application of pseudomonas aeruginosa injection. Otolaryngol Head Neck Surg. 2015;153(4):561–565. doi:10.1177/0194599815584917
12. Weniger M, D’Haese JG, Angele MK, Kleespies A, Werner J, Hartwig W. Treatment options for chylous ascites after major abdominal surgery: a systematic review. Am J Surg. 2016;211(1):206–213. doi:10.1016/j.amjsurg.2015.04.012
13. Guo Shu-Huan HL-P, Liu T, Zhang X-P, Gao M. Prevention of chylous leakage after laparoscopic lymphadenectomy. Chin J Endosc. 2014;20(12).
14. Chen Q, Chen Y, Su A, et al. Ultrasound-guided percutaneous injection of Pseudomonas aeruginosa-mannose sensitive hemagglutinin for treatment of chyle fistula following neck dissection: two case reports. Medicine. 2020;99(5):e18816. doi:10.1097/MD.0000000000018816
15. Hur S, Jun H, Jeong YS. Novel interventional radiological management for lymphatic leakages after gynecologic surgery: lymphangiography and embolization. Gland Surg. 2021;10(3):1260–1267. doi:10.21037/gs-2019-ursoc-10
16. Xiu D, Cheng M, Zhang W, Ma X, Liu L. Pseudomonas aeruginosa-mannose-sensitive hemagglutinin inhibits chemical-induced skin cancer through suppressing hedgehog signaling. Exp Biol Med. 2020;245(3):213–220. doi:10.1177/1535370219897240
17. Cheng X, Wang B, Jin Z, et al. Pseudomonas aeruginosa-mannose-sensitive hemagglutinin inhibits pancreatic cancer cell proliferation and induces apoptosis via the EGFR pathway and caspase signaling. Oncotarget. 2016;7(47):77916–77925. doi:10.18632/oncotarget.12844
18. Yin T, Ou-Yang X, Jiao F, Huang L, Tang X, Ren B. Pseudomonas aeruginosa mannose-sensitive hemagglutinin inhibits proliferation and invasion via the PTEN/AKT pathway in HeLa cells. Oncotarget. 2016;7(24):37121–37131. doi:10.18632/oncotarget.9467
19. Zhang W, Sun J, Shen X, Xue Y, Yuan S, Wang X. Effect of PA-MSAH preprocessing on the expression of TLR-4-NF-kappaB pathway and inflammatory factors in the intestinal tract of rats with septic shock. Exp Ther Med. 2019;17(4):2567–2574. doi:10.3892/etm.2019.7247
20. Zhu H, Wang S, Shen L, Wang W, Zhao F, Cao T. Effects of Pseudomonas aeruginosa mannose-sensitive hemagglutinin (PA-MSHA) pretreatment on septic rats. Int Immunopharmacol. 2013;17(3):836–842. doi:10.1016/j.intimp.2013.09.006
21. Rousselin A, Bendifallah S, Timoh KN, et al. Patterns of care and the survival of elderly patients with high-risk endometrial cancer: a case-control study from the FRANCOGYN group. EJSO. 2017;43(11):2135–2142. doi:10.1016/j.ejso.2017.07.019
22. Della Corte L, Giampaolino P, Mercorio A, et al. Sentinel lymph node biopsy in endometrial cancer: state of the art. Transl Cancer Res. 2020;9(12):7725–7733. doi:10.21037/tcr.2020.04.21
23. Long Q, Zhang J, Wei B, Qi J, Li H. The effect of subcutaneous local spraying of Pseudomonas aeruginosa preparation to reduce postoperative drainage time in patients with breast cancer. Gland Surg. 2020;9(6):2064–2070. doi:10.21037/gs-20-797
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.