Back to Journals » Patient Related Outcome Measures » Volume 12
Top Priorities for Health Service Improvements Among Australian Oncology Patients
Authors Hall A, Bryant J, Sanson-Fisher R, Grady A, Proietto A, Doran CM
Received 12 November 2020
Accepted for publication 31 March 2021
Published 7 May 2021 Volume 2021:12 Pages 83—95
DOI https://doi.org/10.2147/PROM.S291794
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Lynne Nemeth
Alix Hall,1– 3 Jamie Bryant,1– 3 Robert Sanson-Fisher,1– 3 Alice Grady,2– 4 Anthony Proietto,1– 3 Christopher M Doran5
1Health Behaviour Research Collaborative, School of Medicine and Public Health, Faculty of Health and Medicine, University of Newcastle, Callaghan, NSW, Australia; 2Priority Research Centre for Health Behaviour, University of Newcastle, Callaghan, NSW, Australia; 3Hunter Medical Research Institute, New Lambton Heights, NSW, Australia; 4Hunter New England Local Health District, Population Health, Wallsend, NSW, Australia; 5Centre for Indigenous Health Equity Research, Central Queensland University, Rockhampton, QLD, Australia
Correspondence: Jamie Bryant Email [email protected]
Objective: To determine among a sample of Australian cancer patients receiving outpatient oncology care: 1) the most frequently endorsed general health service improvements selected by patients; 2) for the three most endorsed general health service improvements, the proportion of participants endorsing specific health service changes; and 3) sociodemographic, disease and treatment characteristics associated with the most frequently endorsed general health service improvements.
Methods: A cross-sectional survey was conducted across six outpatient oncology treatment units located in New South Wales, Australia. Patients receiving chemotherapy for any cancer diagnosis at any of six oncology services were recruited. Participants completed an online survey which included the Consumer Preferences Survey. Logistic regression analyses were conducted to identify sociodemographic, disease and treatment characteristics associated with frequently endorsed health service improvements.
Results: A total of 879 eligible patients initiated the survey (72% consent rate). Participants selected a median of two health service improvements. The three most wanted improvements were car parking (56%), up-to-date information about treatment or condition progress (19%), and hospital catering (17%). Age was the only characteristic significantly associated with identifying car parking as a needed improvement.
Conclusion: Achieving high quality cancer care requires understanding of the views and experiences of patients about the quality of care they receive. Car parking and access to information were the two most frequently endorsed general health service changes desired by this sample of participants.
Practice Implication: Future studies could examine whether enacting changes as per patient feedback improves patient perceptions of quality of care, and health outcomes.
Keywords: patient-centered care, cancer, quality of healthcare, patient identified change
Background
Patient-Centred Cancer Care is Considered Optimal Health Care
Patient-centred care is defined by the Institute of Medicine as care that is respectful of, and responsive to, individual patient preferences, needs and values.1 Patient-centred care is considered one of six key elements of high-quality care1 and its importance is reflected internationally in the development of the World Health Organisation’s global strategy on people-centered and integrated health care.2 In the field of cancer care, provision of patient-centred care has been associated with improved psychological outcomes,3 increased medication adherence4 and increased patient satisfaction.5,6 In order to achieve high-quality patient-centred care, it is imperative to understand the views and experiences of patients about the quality of care they receive, and use these perspectives to inform quality improvements to the healthcare system.7
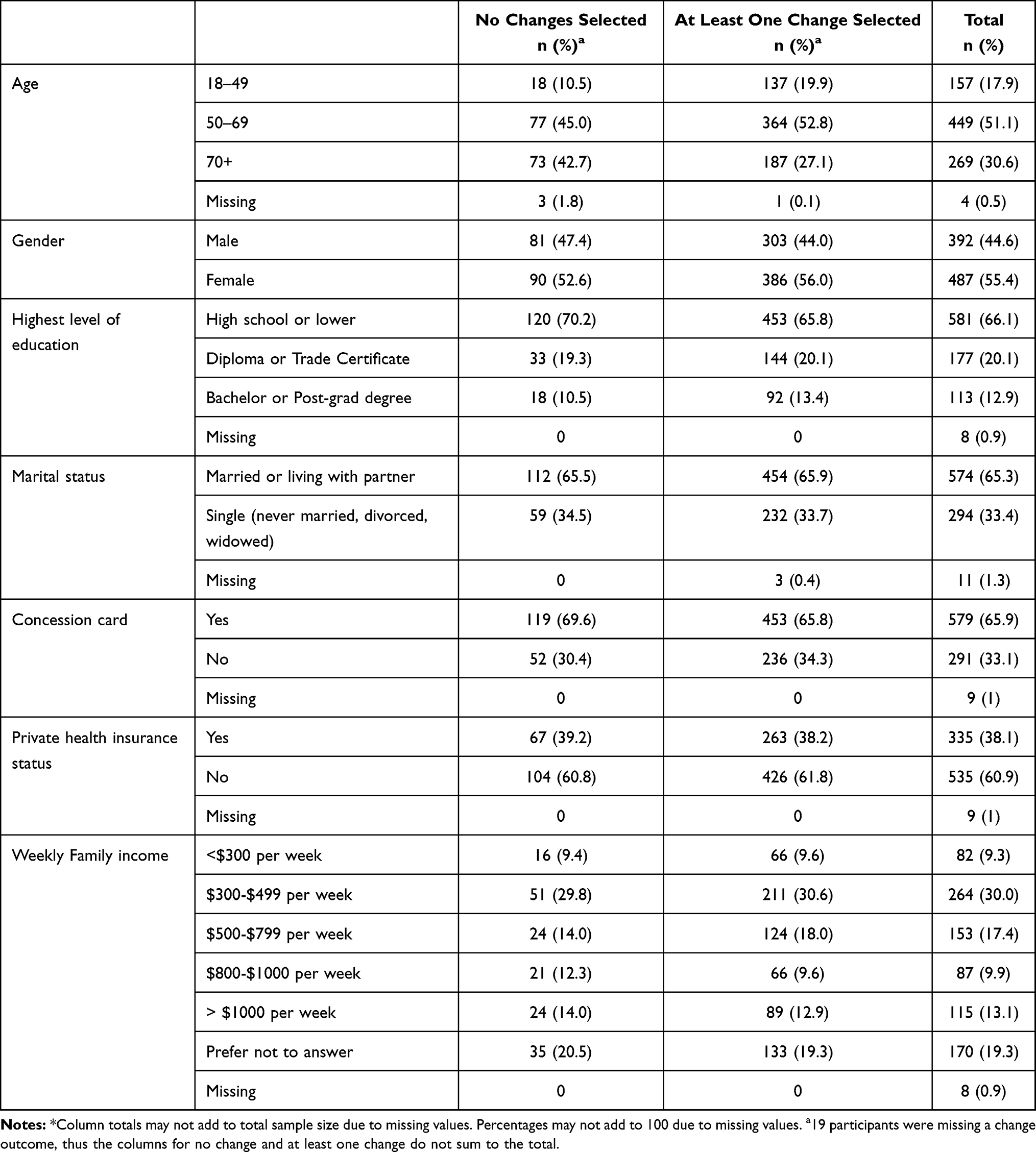 |
Table 1 Sample Characteristics (N= 879*) |
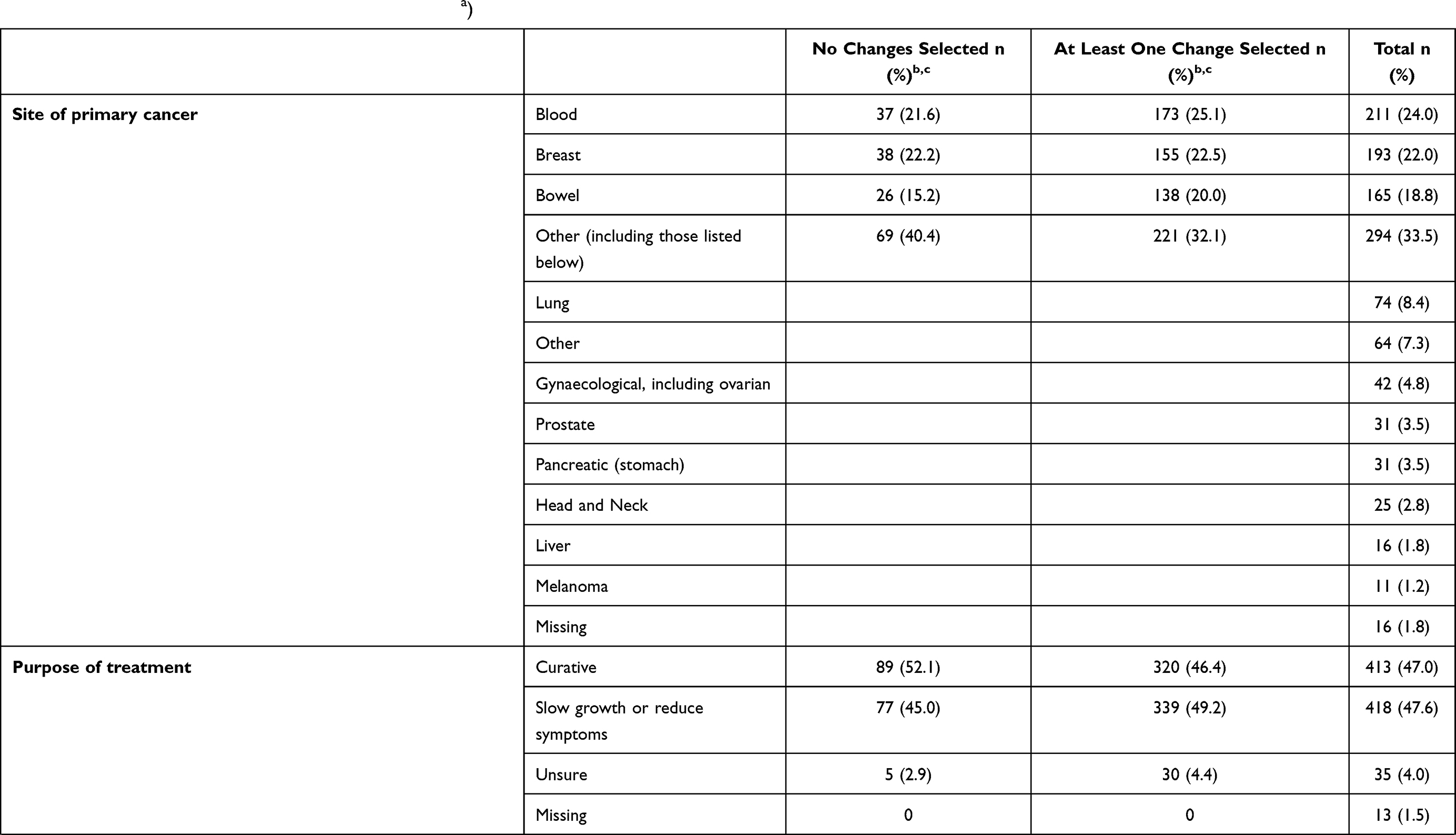 | 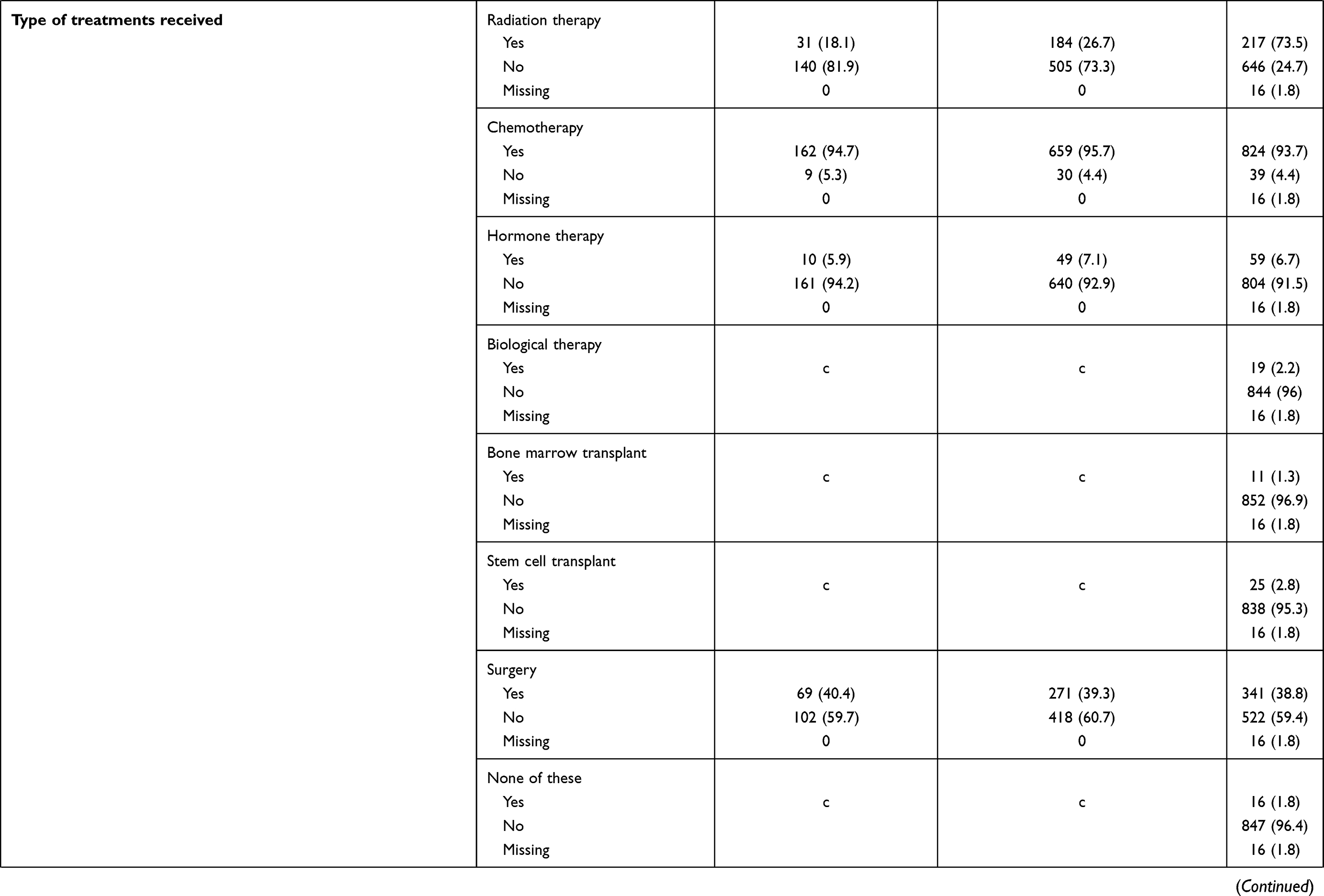 |  |
Table 2 Disease and Treatment Characteristics (N=879 a) |
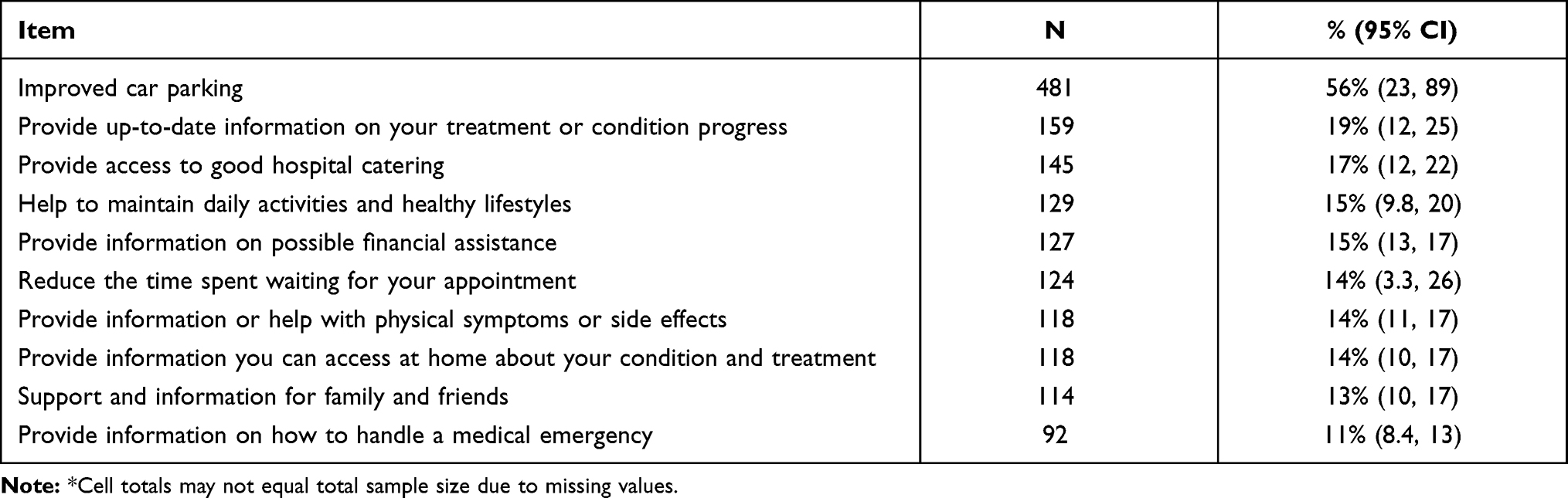 |
Table 3 Top 10 Most Endorsed General Health Service Improvement Items (N=860)* |
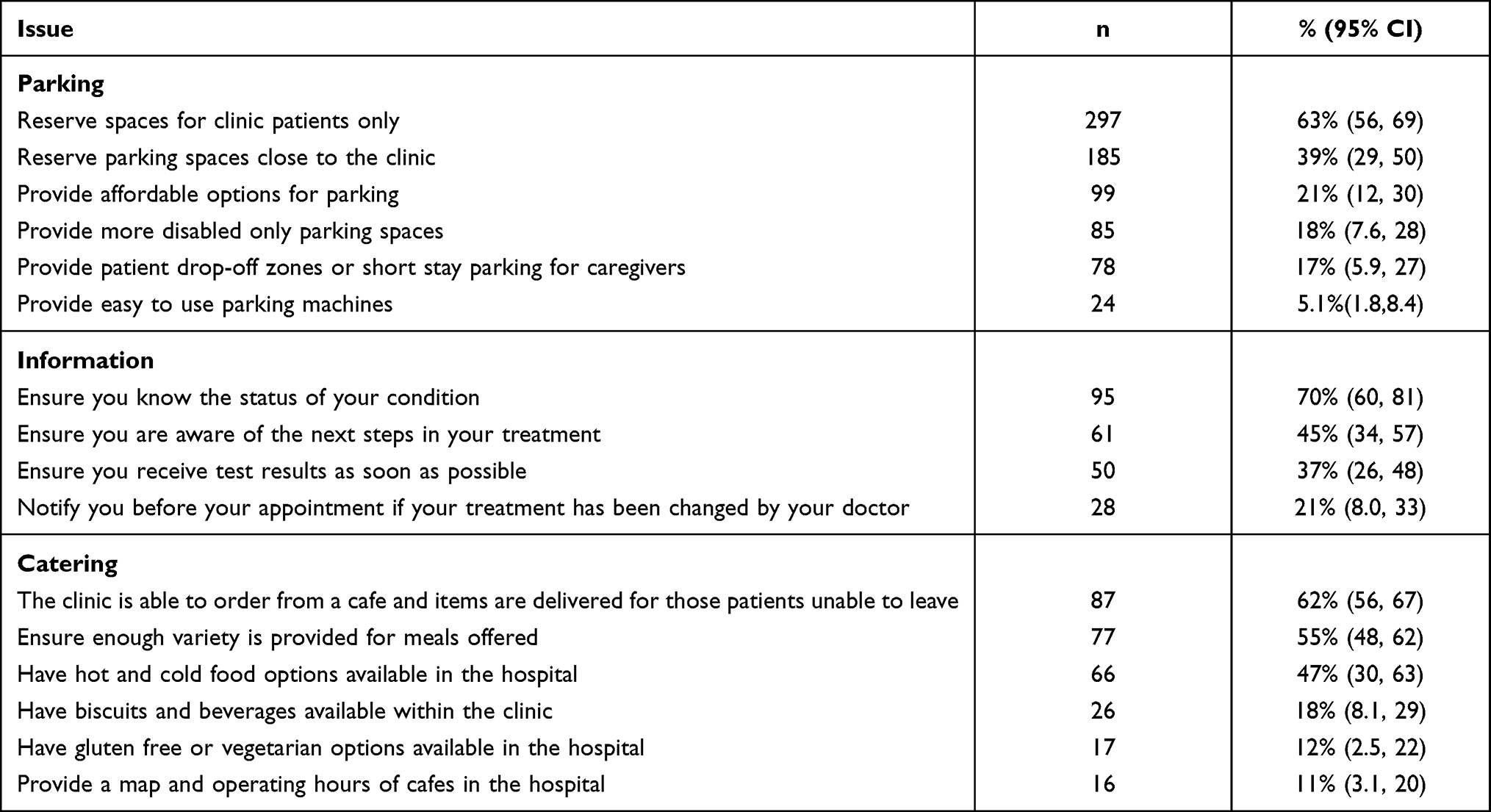 |
Table 4 Frequency and Percentage of Patients Selecting the Specific Initiatives for Improved Car Parking, Information and Catering |
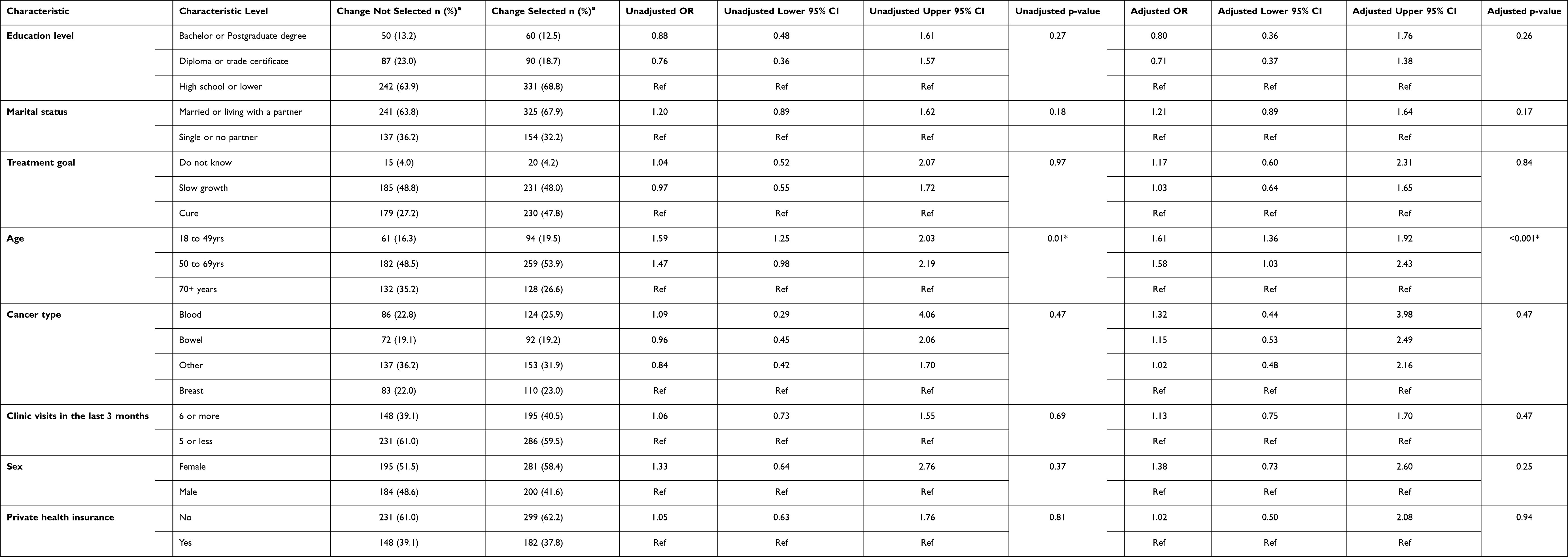 |
Table 5 Characteristics Associated with the Most Frequently Endorsed General Health Service Improvement Item |
Accurate and Clinically Useful Methods are Needed to Capture Patient’s Perspectives
A commonly used method of examining and understanding patient perceptions of the quality of care received is via patient satisfaction surveys, surveys of unmet needs, and other patient-reported outcome measures such as the EORTC QLQ-INFO25, which assesses cancer patients’ perception of information received during different phases of care.8 Such tools ask patients to either reflect on the care they have received, share what is important to them, or report needs that could be addressed by healthcare providers and/or the healthcare system to improve their care. These approaches, however, have some well-documented limitations.9–11 Firstly, most tools only assess patient’s perceptions on broad aspects of care largely related to medical and disease processes, rather than exploring the specific improvements they would like made.11,12 Obtaining more detailed information from patients about specific strategies that they perceive would improve their care increases the accuracy of measurement, and reduces ambiguity as to what changes are seen by patients as most necessary, thus providing more concrete information that may help to better guide changes initiated by the healthcare system10 Secondly, inadequacies in psychometric rigor, including sensitivity to change over time,13 and difficulties in scoring many of the frequently used patient satisfaction and unmet needs surveys have been identified.14
In response to these shortcomings, a new tool titled “The Consumer Preferences Survey” (CPS) was developed to allow collection of detailed data about patient desired health service improvements.12 The CPS is computer administered and uses adaptive questioning and branching to allow users to endorse general actionable changes that would help improve their care and experiences, and then endorse more specific changes based on their previous answers. The CPS was developed using a systematic process that included a literature review, advice and feedback from an expert advisory group, and pilot testing with patients from medical oncology, cardiology, and neurology clinics.12 The measure has good acceptability (easy to complete (97.9%); comprehensive (93.1%; appropriate length (95.5%); clear directions (98.3%), and adequate test-retest reliability (Cohen’s kappa=0.53 across all items) for most items.12 Unlike other tools, the CPS provides a list of concrete and specific changes that patients perceive could be improved.12
Consumer Preferences Survey Data from Large Heterogenous Samples of Cancer Patients Will Help to Inform Health Care Improvements
To date, only two studies have used the CPS to explore cancer patients’ preferences for quality improvements to their care.15,16 Improved car parking and up-to-date information were the most highly endorsed areas in need of improvement.15,16 While these studies provide an indication as to what areas of improvement patients perceive as needed, additional information is still required if health service improvements that reflect patient perceptions and wishes are to be made. For instance, one of these previous studies focused on the perceptions of chronic care patients, receiving care from three hospital departments in New South Wales, Australia, including oncology, neurology and cardiology. While this study included the perceptions of cancer patients, the specific initiatives perceived by cancer patients as needing improvement were not explored.16 The second study explored cancer patients’ perceptions specifically, however, this study included only a sub-sample of patients participating in a larger study, and only focused on the association between the initiatives selected by patients and their quality of life.15 Larger studies that include a diverse range of cancer patients from a range of treatment centres are needed. Such studies should explore both the broad and specific changes patients would like made to their care, as well as those characteristics associated with such changes. Understanding, the characteristics associated with the most frequently endorsed changes will help identify what future support and health service changes are most wanted by cancer patients. Obtaining such information will help to inform what quality improvements should be made to improve the delivery of patient-centred care provided to cancer patients.
Aims
To determine, among a sample of Australian cancer patients receiving chemotherapy at outpatient oncology clinics:
- The most frequently endorsed general health service improvements selected by patients;
- For the three most endorsed general health service improvements, the proportion of participants endorsing specific health service changes; and
- The patient sociodemographic, disease and treatment characteristics associated with the most frequently endorsed general health service improvements by patients.
Methods
Design
This paper reports data collected as part of a stepped wedge cluster randomised controlled trial that aimed to improve the delivery of patient-centred care to cancer patients receiving chemotherapy using a novel consumer-led collaborative approach (Australia and New Zealand Clinical Trials Registry Number ACTRN12614000702617). It also extends previous analyses presented from a sub-sample of patients taking part in the baseline component of this study.15 As the intervention was not successfully implemented according to the pre-specified protocol in any of the sites due to a range of factors (including failure to identify and train sufficient consumer advocates in each setting and difficulty facilitating multi-disciplinary quality of care collaboratives), assessing the effectiveness of the intervention was not possible. Consequently, this paper focuses on presenting an in-depth exploration of the quality improvements identified by a large sample of cancer patients, receiving treatment from a number of cancer treatment centres.
Setting and Participant Eligibility
Six outpatient oncology treatment units located in New South Wales, Australia, participated. Individuals were eligible if they: 1) were aged 18 years or older; 2) were receiving chemotherapy for any cancer diagnosis; 3) had attended the treatment unit on at least one previous occasion and therefore were considered able to reflect on aspects of the treatment centre care where they desired change; 4) were able to complete an English-language survey either independently or with assistance; and 5) could provide informed consent.
Recruitment
Trained research volunteers approached patients in the waiting room or treatment area of the oncology unit and invited participation in the research. Potential participants were provided with a written information statement and assessed for eligibility. Those who were eligible were invited to commence a survey on a tablet computer. Research volunteers recorded information regarding the gender and age of non-consenting participants to allow for determination of consent bias.
Measurement
Participants completed a survey on a tablet computer. Survey items were presented using the online survey system QuON.17 The QuON system is a dynamic online survey platform which allows the use of dynamic branching to ensure participants only received relevant questions. Participants self-reported the following: 1) Socio-demographic information: gender, age, highest level of education, marital status, Aboriginal or Torres Strait Islander status, possession of a concession card, private health insurance status, and weekly family income; 2) Disease and treatment information: site of primary cancer; purpose of treatment; type of treatments received; number of visits to the outpatient clinic in the previous 3 months; 3) Consumer Preferences Survey (CPS): The CPS is a web-based survey that assesses patients views as to which areas of their care could be improved. Patients are presented with 25 items that represent general areas of health care that are organised into four categories: 1) changes to appointment scheduling; 2) changes when arriving at an appointment, 3) changes during a clinical appointment, and 4) changes to assist with managing at home. For most of the 25-items patients are asked to indicate which areas they believe could be improved.15 For those general health service improvements that patients select, they are then prompted to indicate what specific changes could be implemented to improve their care. The number of specific changes presented for patients to select varied from 3–11 depending on the general health service improvement selected. Patients could select as many specific health care changes as they wanted.
Data Analysis
As the intervention was not successfully delivered as planned, data were analysed as an observational study. The top ten most frequently endorsed general health service improvements were calculated and reported. For the top three items, the frequency of patients selecting the specific initiatives suggested to improve these top three areas are also reported. For both of these outcomes, the frequency, percentage and 95% confidence intervals (CIs) are reported for each item. The delete-1 cluster jackknife variance estimation method was used in the calculation of the 95% CIs to account for the complex survey data used in this study, such as the clustered nature of the data and the variable cluster sizes.18 Logistic regression analyses were conducted for the most frequently endorsed general health service improvement item, to identify sociodemographic, disease and treatment characteristics associated with patients identifying this item as an area in need of change. The characteristics assessed in the model were hypothesised to impact on patient’s perceptions of their care and included: age, sex, marital status, education status, private health insurance coverage, cancer type and number of visits to the clinic in the last three months. To control for any possible effect the intervention may have had on the study outcome, an intervention received variable was included in the regression model. For this variable, participants who completed a survey before the intervention begun at their hospital were coded as not having received the intervention, while patients who completed a survey after the intervention was attempted at their hospital were coded as receiving the intervention. The delete-1 cluster jackknife variance estimation method was used to account for clustering by hospital site and for the variable cluster sizes. Listwise deletion was used to remove observations with missing data from the model so that only complete cases were analysed. Characteristics identified at a p-value <0.05 on the Wald statistic were considered statistically significant. The logistic regression model was assessed for potential outliers and violations in the assumption of multicollinearity.
Results
Sample
Of 1272 patients approached, 922 eligible patients agreed to participate (72% consent rate). A total of 879 patients initiated the CPS survey. Table 1 describes the sociodemographic characteristics and Table 2 details the disease and treatment characteristics of all eligible participants. They also provide a description of these characteristics by whether participants reported no changes or if they reported at least one change. Most (81.1%) participants were aged between 50 and 69 years at the time of the study, were female (55.4%), in a partnered relationship (65.3%), and did not have private health insurance (60.9). The most common cancer type was blood (24%) followed by breast (22%). The most common cancer treatment received was chemotherapy (93.7%).
Top Ten Most Frequently Endorsed General Health Service Improvements
Out of the 25 general health service improvement items listed in the CPS, participants selected a median of two items for improvement (range 0 to 19). A total of 171 (20%) patients indicated that they did not believe any of the CPS areas of care required improvement at their outpatient clinic, while 175 (20%) indicated that five or more items required improvement. The top 10 most frequently endorsed general health service improvement items are provided in Table 3. The most frequently endorsed item was improved car parking (56%). However, there was variation between hospitals with regards to the percentage of patients who selected this item as an area in need of improvement (reflected by the wide confidence intervals). Specifically, over 50% of patients from sites 2 (75%), 4 (54%), 5 (68%) and 6 (79%) selected this item as an area for improvement. Whereas, only 37% and 6.6% of patients selected this item from sites 1 and 3, respectively. The second most frequently reported quality improvement item was up-to-date information on the patient’s treatment or condition progress (19%), followed by having access to good hospital catering (17%).
Proportion of Participants Endorsing Specific Health Service Changes
For each general health service improvement item that was endorsed, participants were asked to select from a list, which specific quality improvement initiatives they believe could help to improve that domain. Table 4 presents the percentage and frequency of patients who selected each of the specific initiatives related to the top three most frequently endorsed general health service improvement items for parking, information and catering.
Of the 481 patients who selected car parking as an area in need of improvement, 472 (98%) selected at least one specific quality improvement initiatives for this domain. Reserved car parking for clinic patients was the most frequently selected initiative (63%). Of the 159 patients who selected up-to-date information on their treatment or condition progress as an area for quality improvement, 135 (85%) responded to the specific improvement initiatives listed for this domain. Knowing the status of their cancer (70%) was the most frequently endorsed initiative. Of the 145 patients who endorsed access to good hospital catering as an area for quality improvement, 141 (97%) answered the specific improvement initiatives listed for this area. Being able to order food from a cafe and have it delivered to the clinic if the patient is unable to leave was the most frequently selected initiative (62%).
Characteristics Associated with the Most Frequently Endorsed General Health Service Improvement
A total of 850 (98%) observations were included in the multivariable logistic regression. Table 5 lists the sociodemographic, disease and treatment characteristics associated with the top general health service improvements selected by patients. Age was the only characteristic found to be significantly associated with patient’s selecting “improved car parking” as an area that could be improved. Compared to those aged 70 years and over, patients aged 18–49 years and 50–69 years had significantly higher odds of reporting this item as in need of improvement.
Discussion
This study examined the most frequently endorsed general health service improvements selected by a sample of Australian cancer patients receiving outpatient chemotherapy using a newly developed measure, the Consumer Preferences Survey. It also identified the patient sociodemographic, disease and treatment characteristics associated with the most frequently endorsed general health service improvements.
Overall, one-fifth of participants did not endorse any of the suggested general health service improvements. These findings suggest that only a fifth of participating patients did not perceive that any of the pre-specified changes would improve their care, and were thus potentially satisfied with the care they received. This is in contrast to existing research that has examined cancer patient satisfaction with their treatment experience and the care they receive, which show that patients generally report very high rates of satisfaction.19–21 In particular, a survey of more than 300 cancer patients attending six outpatient clinics in NSW found that more than 90% of patients thought that hospital staff showed them and their family respect, made sure they received correct treatment, and spoke to them in a way they could understand.22 Alternatively, this finding may reflect that the domains assessed by the CPS were not comprehensive, and may not have identified general areas of potential change desired by participants. However, given a fifth of participants identified five or more areas that required improvement, this is unlikely.
Changes to car parking were identified by participants as the most important general health service improvement requiring change, with 56% of patients across all six clinics selecting this domain. This aligns with previous international research that has identified car parking as an important barrier to access to cancer services in the UK.16,23,24 It also aligns with national research among patients attending chronic disease outpatient clinics, where 60% of respondents selected improved car parking as a domain in need of improvement using the CPS.16 Age was the only characteristic found to be significantly associated with patient’s selecting car parking as an area that could be improved.
The availability of parking for clinic patients only that is in close proximity to the treatment centre was identified as the most important specific change that could be made to improve car parking. This finding highlights the utility of using this dynamic approach to surveying patients as it provides specific and actionable changes to health services. It is important to note however that car parking was not a pertinent issue for all treatment centres. For two sites, less than 50% of patients identified car parking as an area in need of improvement. For one of these sites, less than 10% endorsed car parking as an area of change. This highlights the difficulties in generalising patient’s perspectives on quality improvements across sites and emphasises the importance of assessing patient perspectives at the clinic level, and tailoring care towards the needs of patients attending specific treatment centres that have unique characteristics.
Six out of the top 10 general health service improvement items related to participant’s desire for additional information about their cancer and its treatment. This finding is consistent with the unmet needs literature among cancer patients, where information needs have consistently been identified as a key area of unmet need for many patients.5,24 The specific types of information desired by participants were personal information specifically related to their care and treatment, including knowing the status of their condition, the next steps in treatment, and receiving test results as soon as possible. These findings suggest the need for better communication of clinical information from the treatment team to their patients.
Study Strengths and Limitations
A strength of the current study is that it provides detailed data from a large sample of cancer patients across New South Wales. However, as there were only a small number of treatment centres and all treatment centres were located in one state of Australia, the generalisability of the findings to broader Australia and other countries is limited.
Conclusion
Achieving high quality cancer care requires understanding of the views and experiences of patients about the quality of care they receive. Understanding the specific areas of healthcare that patients perceive can be improved provides critical information to advocate for change and provide care that meets patient’s needs, and thus is truly patient centered. Car parking and access to information were the two most frequently endorsed general health service changes desired by this sample of participants. Future studies should examine whether enacting changes as per patient feedback improves patient perceptions of quality of care, and patient outcomes.
Declaration of Helsinki
This study was conducted in accordance with the Declaration of Helsinki.
Abbreviation
CPS, The Consumer Preferences Survey.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
Ethics approval was provided by the Hunter New England Human Research Ethics Committee (13/08/21/4.07) and the University of Newcastle Human Research Ethics Committee (H-2012-0099). Appropriate governance approvals were obtained from all participating treatment centres. All participants provided informed consent for participation.
Consent for Publication
All the authors consent to publish the study in your journal.
Acknowledgments
Infrastructure funding from the University of Newcastle and Hunter Medical Research Institute. Dr Jamie Bryant was supported by an Australian Research Council Post Doctoral Industry Fellowship. We wish to thank study participants, the staff at participating organisations, and our research volunteers for their valuable contributions to this project.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by the Australian Research Council’s Linkage Projects scheme under the project number LP120100618; and a Strategic Research Partnership under the Grant CSR 11-02 from Cancer Council NSW to the Newcastle Cancer Control Collaborative (New-3C).
Disclosure
Dr Jamie Bryant report grants from Cancer Council NSW Strategic Research Partnership Grant, during the conduct of the study. The authors report no other conflicts of interest to declare.
References
1. Committee on Quality of Health Care in America. Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century. National Academy Press; 2001.
2. World Health Organization. WHO Global Strategy on People-Centred and Integrated Health Services: Interim Report. 2015.
3. Dong S, Butow PN, Costa,DSJ, Dhillon HM, Shields CG. The influence of patient-centered communication during radiotherapy education sessions on post-consultation patient outcomes. Patient Educ Couns. 2014;95(3):305–312. doi:10.1016/j.pec.2014.02.008
4. Kahn KL, Schneider EC, Malin JL, et al. Patient centered experiences in breast cancer: predicting long-term adherence to tamoxifen use. Med Care. 2007;45(5):431–439. doi:10.1097/01.mlr.0000257193.10760.7f
5. Mallinger JB, Griggs JJ, Shields CG. Patient-centered care and breast cancer survivors’ satisfaction with information. Patient Educ Couns. 2005;57(3):342–349. doi:10.1016/j.pec.2004.09.009
6. Venetis MK, Robinson JD, Turkiewicz KL, et al. An evidence base for patient-centered cancer care: a meta-analysis of studies of observed communication between cancer specialists and their patients. Patient Educ Couns. 2009;77(3):379–383. doi:10.1016/j.pec.2009.09.015
7. Stewart M. Towards a global definition of patient centred care. BMJ. 2001;322(7284):444–445. doi:10.1136/bmj.322.7284.444
8. Arraras JI, Greimel E, Sezer O, et al. An international validation study of the EORTC QLQ-INFO25 questionnaire: an instrument to assess the information given to cancer patients. Eur J Cancer. 2010;46(15):2726–2738. doi:10.1016/j.ejca.2010.06.118
9. Davies E, Cleary PD. Hearing the patient’s voice? Factors affecting the use of patient survey data in quality improvement. Qual Saf Health Care. 2005;14(6):428–432. doi:10.1136/qshc.2004.012955
10. Hall AE, Bryant J, Sanson-Fisher RW, Fradgley EA, Proietto AM, Roos I. Consumer input into health care: time for a new active and comprehensive model of consumer involvement. Health Expect. 2018;21(4):707–713. doi:10.1111/hex.12665
11. Reeves R, Seccombe I. Do patient surveys work? The influence of a national survey programme on local quality-improvement initiatives. Qual Saf Health Care. 2008;17(6):437–441. doi:10.1136/qshc.2007.022749
12. Fradgley EA, Paul CL, Bryant J, Roos IA, Henskens FA, Paul DJ. Consumer participation in quality improvements for chronic disease care: development and evaluation of an interactive patient-centered survey to identify preferred service initiatives. J Med Internet Res. 2014;16(12):e292. doi:10.2196/jmir.3545
13. Pearce NJ, Sanson-Fisher R, Campbell HS. Measuring quality of life in cancer survivors: a methodological review of existing scales. Psycho-Oncology. 2008;17(7):629–640. doi:10.1002/pon.1281
14. Carey M, Lambert S, Smits R, Paul C, Sanson-Fisher R, Clinton-McHarg T. The unfulfilled promise: a systematic review of interventions to reduce the unmet supportive care needs of cancer patients. Support Care Cancer. 2012;20(2):207–219. doi:10.1007/s00520-011-1327-1
15. Fradgley EA, Bryant J, Paul C, Hall AE, Sanson-Fisher RW, Oldmeadow C. Cross-sectional data that explore the relationship between outpatients’ quality of life and preferences for quality improvement in oncology settings. J Oncol Pract. 2016;12(6):e746–e754. doi:10.1200/JOP.2016.011023
16. Fradgley EA, Oaul CL, Bryant J, Oldmeadow C. Getting right to the point: identifying Australian outpatients’ priorities and preferences for patient-centred quality improvement in chronic disease care. Int J Qual Health Care. 2016;28(4):470. doi:10.1093/intqhc/mzw049
17. Paul D, Wallis M, Henskens F, Nolan K. A Generic Platform for the Collation and Sharing of Web Survey Data. 2013:111–116.
18. Kolenikov S. Resampling variance estimation for complex survey data. Stata J. 2010;10(2):165–199. doi:10.1177/1536867X1001000201
19. Heerdegen ACS, Petersen GS, Jervelund SS. Determinants of patient satisfaction with cancer care delivered by the Danish healthcare system. Cancer. 2017;123(15):2918–2926. doi:10.1002/cncr.30673
20. Lis CG, Rodeghier M, Grutsch JF, et al. Distribution and determinants of patient satisfaction in oncology with a focus on health related quality of life. BMC Health Serv Res. 2009;9(1):190. doi:10.1186/1472-6963-9-190
21. Nguyen TVF, Anota A, Brédart A, et al. A longitudinal analysis of patient satisfaction with care and quality of life in ambulatory oncology based on the OUT-PATSAT35 questionnaire. BMC Cancer. 2014;14(42). doi:10.1186/1471-2407-14-42
22. Tzelepis F, Hanna JH, Paul CL, Boyes AW, Carey ML, Regan T. Quality of patient‐centred care: medical oncology patients’ perceptions and characteristics associated with quality of care. Psycho-Oncology. 2017;26(11):1998–2001. doi:10.1002/pon.4380
23. Cancer Council New South Wales. Cap Parking for Cancer Patients in New South Wales. 2012.
24. Morrison V, Henderson B, Zinovieff F, et al. Common, important, and unmet needs of cancer outpatients. Eur J Oncol Nurs. 2012;16(2):115–123. doi:10.1016/j.ejon.2011.04.004
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.