")
Back to Journals » International Medical Case Reports Journal » Volume 16
Too Little, Too Late: A Case of a Swift Fatal Culmination of Amiodarone Induced Pulmonary Toxicity in an Adult Male
Received 8 August 2023
Accepted for publication 3 October 2023
Published 12 October 2023 Volume 2023:16 Pages 679—687
DOI https://doi.org/10.2147/IMCRJ.S433740
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Clement Tan, Pranav Kumar
Department of Respiratory Medicine, Mackay Base Hospital, Mackay, Queensland, Australia
Correspondence: Clement Tan; Pranav Kumar, Email [email protected]; [email protected]
Abstract: Amiodarone is a commonly prescribed antiarrhythmic drug. It can cause a myriad of complications associated with its long-term use, with amiodarone induced pulmonary toxicity being the worst. Amiodarone does this through its destructive properties and its’ ability to accumulate if taken for extended periods of time or in high cumulative doses. Albeit uncommon, the management of amiodarone induced pulmonary toxicity can be straightforward if recognized early. Otherwise, it can lead to severe respiratory failure causing death. In this case report, we aim to highlight the importance of vigilance with clinicians prescribing amiodarone and to spark interests into research for alternative management options of amiodarone induced pulmonary toxicity. This will be done through the description of a case of a 64-year-old male presenting with cough and dyspnoea, who has been on a large dose of amiodarone daily for the past 11 months. He was diagnosed too little, too late, which unfortunately culminated in his rapid fatality. This case is unique for two reasons. The diagnosis of amiodarone induced pulmonary toxicity was through the clinical picture – without the use of invasive investigations. In addition, the futile cessation of amiodarone and use of high dose systemic corticosteroids as a management – which to our knowledge is uncommon in literature.
Keywords: amiodarone, amiodarone induced pulmonary toxicity
Introduction
Amiodarone is a highly effective antiarrhythmic drug that belongs in Class III of the Vaughan-Williams classification system as it works primarily by blocking potassium channels. However, it also exhibits pharmacodynamic actions across the other mechanisms of antiarrhythmics in the classification system.1,2 It is very commonly used to treat supraventricular and ventricular based arrhythmias. It has an iodine containing compound, known as an iodinated benzofuran derivative, which is highly lipophilic, hence can accumulate in fat containing tissues and different organs such as lungs, liver, thyroid, eyes, and heart – mainly highly perfused organs.1,3,4 However, pulmonary toxicity is the most serious of all these complications of amiodarone use.2,5,6 Though it may occur with any dosage, the likelihood of pulmonary toxicity does decrease with lower doses of amiodarone.6 As amiodarone is one of the most prescribed antiarrhythmic medications in Australia and in the other western counterparts, all users and clinicians need to be wary and look out for the complications associated with it.
This case report discusses a 64-year-old male who developed amiodarone induced pulmonary toxicity (APT) to which he eventually succumbed from. It aims to highlight the different ways of diagnosing APT along with the importance of vigilance associated with the use of this antiarrhythmic in all patients, as there is a possibility of irreversible pulmonary toxicity like in the case of this patient – to which the warranted treatment can no longer hold any benefits. The CARE guidelines were used for the reporting of this case.7
Case Report
A 64-year-old male developed a 6-day history of cough with worsening shortness of breath. His cough was episodically productive with white phlegm. There was no green or yellow sputum. He denied any paroxysmal nocturnal dyspnoea, palpitations, chest pain, gastrointestinal or neurological symptoms. At the emergency department due to the nature of his presenting signs and symptoms along with his multiple cardiological background, he was quickly referred and admitted under the joint care of the general medical and cardiology team.
His medical history includes rheumatic heart disease, mechanical aortic valve, non-ischemic dilated cardiomyopathy, atrial fibrillation, hypertension, and hypercholesterolemia. He was a previous heavy smoker with a total of approximately 40 pack years. He also had a large alcohol intake history, with about 20 standard drinks a week. His occupational history only involves school bus driving in his early years, and as a taxi driver in his recent years. He currently takes sacubitril-valsartan, bisoprolol, dapagliflozin, frusemide, thyroxine, warfarin, budesonide-formoterol puffer as well as amiodarone. He had an initial triple chamber pacemaker placed 5 years ago, which was changed very shortly after to a right sided dual chamber pacemaker due to an infection. The patient had an episode of ventricular tachycardia about 11 months prior to this admission and was placed on oral amiodarone 200mg twice a day indefinitely.
On examination, he was afebrile, had a lying blood pressure of 85/63, standing blood pressure of 92/66, a heart rate of 55 beats per minute, tachypnoeic at 26 breaths a minute and oxygen saturations of 90% on room air. His general appearance revealed a thin man, slightly cachexic with visible ribs showing. There was obvious dyspnoea at rest, but he was otherwise alert and oriented. There were no signs of clubbing or carbon dioxide retention. His mucous membrane was moist. There was no appreciable pallor. His jugular venous pressure was 5cm. His heart sounds were dual with the clicking sound of a mechanical aortic valve. He had florid fine crackles bilaterally through both lung fields. These crackles were not cleared on coughing. His abdomen was soft and non-tender. There was no ankle or sacral edema.
Upon admission, his electrocardiogram (ECG) showed a ventricular paced rhythm at a rate of 55 beats per minute that otherwise looked like his previous ECGs before this admission. His covid test and respiratory swabs were negative. His full blood count showed a significant increase in white cell count, high neutrophils, and mildly low haemoglobin. His international normalized ratio (INR) was at 6. His electrolytes and kidney functions were normal. His liver function tests showed raised liver markers. His calcium, magnesium and phosphate levels were mildly decreased. His B-type natriuretic peptide was significantly elevated. His thyroid function tests which included triiodothyronine (T3), thyroxine (T4), thyroid stimulating hormone (TSH), TSH receptor antibodies, anti-thyroid peroxidase and anti-thyroglobulin were completely within normal limits. An autoimmune screen done for the patient returned negative as well. Majority of the patient’s laboratory results can be found in Table 1. Previous echocardiograms done showed severely dilated left and right ventricle, dilated left and right atrium, an ejection fraction of 19%, right ventricular systolic pressure of 78mmHg. His chest x-ray (CXR) taken is shown in Figure 1. A high-resolution computed tomography (HRCT) was also performed several hours after, as shown in Figure 2. Over the course of this event, he would have CXRs taken almost daily, that were all similar to that shown in Figure 1. His initial diagnostic impression was decompensated heart failure with fluid overload.
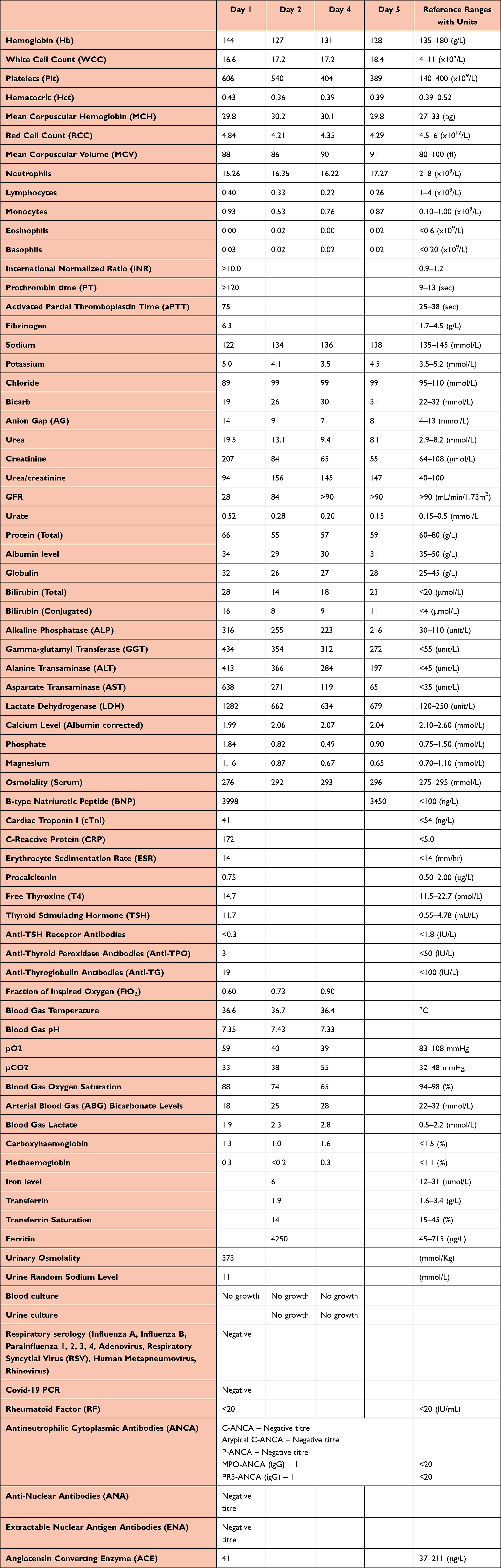 |
Table 1 All Laboratory Results with Reference Ranges and Relevant Units from Day 1, 2, 4 and 5. Reference Ranges Based on Local Pathology Lab Values. Day 3 Purposefully Omitted Due to Minimal Change in Values |
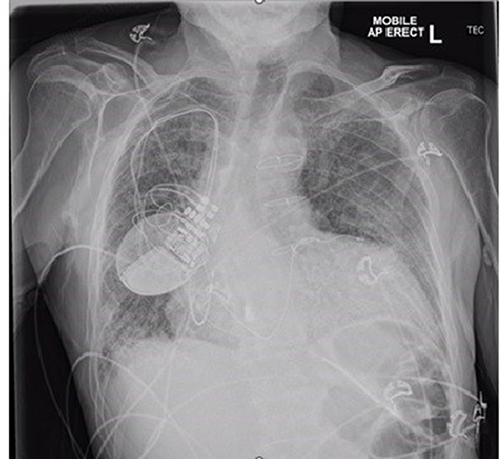 |
Figure 1 CXR image. Diffuse bilateral fine reticular interstitial densities. Peribronchial thickenings. Enlarged heart. No discrete consolidation. |
 |
Figure 2 Axial HRCT images progressing inferiorly; showing diffuse ground glassing with basal predominance, interstitial thickening and traction bronchiectasis, with minimal patchy areas of lobular sparring. Upper lobe emphysematous changes. No areas of consolidation or honeycombing present. |
He was initially managed by being placed on high flow oxygen at 60L/min and a fraction of inspired oxygen (FiO2) at 65%. The rest included intravenous frusemide, withholding of his amiodarone, and changing to digoxin instead. He was initially placed on coverage for pneumonia with ceftriaxone and doxycycline which was later ceased when there was no evidence of pneumonia. Over the subsequent days, the patient developed increasing oxygen requirement and troubles maintaining his oxygen saturations. He had multiple trials of decreasing the flow rates and the FiO2 independently with no success. Instead, his oxygen saturations did progressively decrease to a lowest of 66% despite being back on 60L/min and an increased FiO2 up to 88%. He was later changed to a continuous positive airway pressure (CPAP) device with a peak end expiratory pressure (PEEP) of 9 and FiO2 of 90% that yielded no success as he continued to saturate around 70% to 75%. When the respiratory physician was consulted, the patient was placed on pulsed intravenous methylprednisolone of 1000mg once daily for 3 days with the intention to wean off with oral prednisolone subsequently. In taking with the clinical picture, though 11 months being a relatively short period, the use of 200mg of amiodarone twice daily led to APT in this patient, complicated by decompensated heart failure. Further arterial blood gases performed over his last days, shown in Table 1, showed respiratory acidosis, decreasing trend of partial pressure of oxygen, and an increasing trend of partial pressure of carbon dioxide. The patient received two doses of his pulsed intravenous methylprednisolone before the joint decision was made between family and clinicians for the patient to be transitioned onto the palliative pathway due to an absence of improvement – he was kept on the CPAP and started on a syringe driver for comfort. Unfortunately, the patient succumbed to his type 2 respiratory failure two hours later.
Discussion
Amiodarone induces pulmonary toxicity through a direct cytotoxic effect, an indirect damage through an immunological reaction or through accumulation of phospholipid complexes within the lung parenchyma and/or the pleura.6,8,9 It has also been found to increase the production of toxic-free radicals in tissues.10 APT is less frequent than thyroid and eye complications, but it is deemed to be the most dangerous of all possible complications. The effects of amiodarone on the lung can take on an acute, subacute or a chronic form.9 Some initial pulmonary specific events are bronchospasm, exacerbation of obstructive airway diseases, interstitial pneumonias, acute respiratory distress syndromes, pleural effusion, interstitial thickenings, and diffuse alveolar haemorrhages.3,6,10,11 Masses and nodules are typically formed in later stages of APT.8,12,13
Some risk factors associated with the development of APT include high cumulative doses, prolong duration of use, existing lung diseases and/or multiple comorbidities, increased age, and recent pulmonary angiograms.3,6 Investigations often done to determine if a clinical presentation is APT related are lung function tests and bronchoalveolar lavages. Lung function tests often demonstrate a restrictive picture, and a reduction of diffusion capacity for carbon monoxide by more than 15% from a recent lung function test is a highly sensitive and highly specific finding.6,11,13 Bronchoalveolar lavages done in APT may range from findings such as haemorrhagic lavage return fluid in acute forms, to lymphocytosis, neutrophilia and eosinophilia.3,10 If present, cytology showing foam cells are helpful in making a diagnosis of APT more probable.14
CXR if done may show patchy or diffuse infiltrates, usually bilateral. A HRCT is considered essential in aiding the diagnosis of APT. HRCT, albeit no pathognomonic changes, has the term “amiodarone pneumonitis” which may include ground glass opacities, focal or generalized parenchymal infiltrates unilaterally or bilaterally, interstitial pneumonia (UIP or NSIP), nodules, interstitial or pleural thickening and pleural effusions. High attenuation areas which resemble deposition of iodine compounds within the lung parenchyma may also occur.3,8,12
There is no one definite test to diagnose APT, hence once common differentials are excluded and if the clinical picture is fitting, a diagnosis of APT can then be made.
The management of APT depends on its severity, for mild cases, cessation of amiodarone and replacement with another antiarrhythmic agent may suffice. If in doubt, cardiologists should always be consulted. If it is clinically severe, it could range from the use of mechanical ventilation to corticosteroid use, sometimes aggressively. Prednisolone if used can be commenced at a dose of 0.5–1mg/kg for a year.3,8 With the right starting dosage of prednisolone, patients with APT may achieve partial or complete resolution of their amiodarone induced pulmonary damage.15,16 It is essential to note that after cessation of amiodarone, there could be a duration of worsening symptoms due to its long half-life.10 Conversely, all patients starting therapy on long term oral amiodarone should receive baseline testing of a CXR, lung function test, liver function test along with thyroid function tests – this should be followed up in regular intervals.2,6,10,17
In this report, we have described a case of a late diagnosed APT that developed acutely into type 2 respiratory failure leading to the demise of a 64-year-old male. This patient had been taking 11 months of amiodarone at 200mg twice daily, and he developed episodes of coughing and dyspnoea. A lung function test was not performed for the patient due to the inability of removing his non-invasive ventilation as it causes severe desaturations. This case is unique in the sense that APT was diagnosed clinically instead of the use of bronchoalveolar lavage. Furthermore, despite the quick discontinuation of amiodarone and the use of intravenous pulsed methylprednisolone at high doses, it did not provide any rapid therapeutic relief or positive response as suggested commonly in literature.4,10,15,16 These factors have all contributed to the rapidity and severity of APT in this patient. Though not previously highlighted in literature for the cut off for reversible versus non-reversible drug induced interstitial lung disease, it could be considered that this patient’s APT may very well have been past that of a reversible stage.
Conclusion
In conclusion, amiodarone is a commonly prescribed antiarrhythmic drug that should be monitored regularly due to the possibility of life-threatening pulmonary toxicity. Patients on regular amiodarone should be followed up by their respective specialists regularly for monitoring of possible systemic toxicity – and not solely for pulmonary toxicity. These patients presenting with suspicious APT should get an HRCT along with a lung function test if they are clinically stable to do one. The current consensus for treatment would be for early identification and diagnosis of APT followed by the immediate cessation of amiodarone and the quick aggressive use of systemic corticosteroid therapy.
As this case report has highlighted, because amiodarone can induce its harmful effects in months and can be fatal, clinicians need to be vigilant to look out for possible presentations. A delayed diagnosis may lead to the futile use of systemic corticosteroids and an increase in the risk of mortality. The diagnosis of APT should be considered after other differentials are ruled out and can be made on the basis of clinical picture with or without the use of invasive bronchoscopy and bronchoalveolar lavage. In fact, APT should always be considered on all patients on amiodarone who present with acute or progressive respiratory symptoms and especially those with significant comorbidities.
Data Sharing Statement
All data and findings generated or analyzed during this study are included in this published article.
Ethics Approval and Consent to Participate
Full and written informed consent was obtained from the next of kin of this patient. This case report was conducted and written in accordance with the Townsville Hospital and Health Service Human Research Ethics Committee (EX/2023/QTHS/101997) (Approved and endorsed on the 18th September 2023). No institutional approval was required for the publishing of this case report.
Consent for Publication
The next of kin of this patient and medical personnel involved in the care of the patient have given a full and written consent in line for the publication of this case report which would include the use of clinical details, investigation findings, and various discussions which have occurred.
Author Contributions
Conception and design of the report and approval of the version of the manuscript to be published: CT and PK. Acquisition of data: CT. Drafting the manuscript: CT. Revising the manuscript for intellectual content: CT. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This case report received no funding at any point in time.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Srinivasan M, Ahmad L, Bhindi R, Allahwala U. Amiodarone in the aged. Aust Prescr. 2019;42(5):158–162. doi:10.18773/austprescr.2019.051
2. Goldschlager N, Epstein AE, Naccarelli GV, et al. A practical guide for clinicians who treat patients with amiodarone: 2007. Heart Rhythm. 2007;4(9):1250–1259. doi:10.1016/j.hrthm.2007.07.020
3. Mitrofan CE, Cretu A, Mitrofan C, Bar C, Ghiciuc CM. Amiodarone induced lung disease. Arch Clin Cases. 2022;9(3):126–132. doi:10.22551/2022.36.0903.10217
4. You HS, Yoon JH, Cho SB, et al. Amiodarone-induced multi-systemic toxicity involving the liver, lungs, thyroid, and eyes: a case report. Front Cardiovasc Med. 2022;9:839441. doi:10.3389/fcvm.2022.839441
5. Van Erven L, Schalij MJ. Amiodarone: an effective antiarrhythmic drug with unusual side effects. Heart. 2010;96(19):1593–1600. doi:10.1136/hrt.2008.152652
6. Papiris SA, Triantafillidou C, Kolilekas L, Markoulaki D, Manali ED. Amiodarone: review of pulmonary effects and toxicity. Drug Saf. 2010;33(7):539–558. doi:10.2165/11532320-000000000-00000
7. Gagnier JJ, Kienle G, Altman DG, Moher D, Sox H, Riley D. The CARE guidelines: consensus-based clinical case reporting guideline development. Glob Adv Health Med. 2013;2(5):38–43. doi:10.7453/gahmj.2013.008
8. Wolkove N, Baltzan M. Amiodarone pulmonary toxicity. Can Respir J. 2009;16(2):43–48. doi:10.1155/2009/282540
9. Budin CE, Cocuz IG, Sabău AH, et al. Pulmonary fibrosis related to amiodarone-is it a standard pathophysiological pattern? A case-based literature review. Diagnostics. 2022;12(12). doi:10.3390/diagnostics12123217
10. Terzo F, Ricci A, D’Ascanio M, Raffa S, Mariotta S. Amiodarone-induced pulmonary toxicity with an excellent response to treatment: a case report. Respir Med Case Rep. 2020;29:100974. doi:10.1016/j.rmcr.2019.100974
11. Pitcher WD. Amiodarone pulmonary toxicity. Am J Med Sci. 1992;303(3):206–212. doi:10.1097/00000441-199203000-00012
12. Oyama N, Oyama N, Yokoshiki H, et al. Detection of amiodarone-induced pulmonary toxicity in supine and prone positions: high-resolution computed tomography study. Circ J. 2005;69(4):466–470. doi:10.1253/circj.69.466
13. Camus P, Fanton A, Bonniaud P, Camus C, Foucher P. Interstitial lung disease induced by drugs and radiation. Respiration. 2004;71(4):301–326. doi:10.1159/000079633
14. Martin WJ, Rosenow EC. Amiodarone pulmonary toxicity. Recognition and pathogenesis (Part I). Chest. 1988;93(5):1067–1075. doi:10.1378/chest.93.5.1067
15. Scaramozzino MU, Sapone G, Plastina UR, Nucara M. Amiodarone-induced lung toxicity: a case initially not correctly framed. Cureus. 2023;15(3):e36818. doi:10.7759/cureus.36818
16. Garg J, Agrawal N, Marballi A, et al. Amiodarone induced pulmonary toxicity: an unusual response to steroids. Am J Case Rep. 2012;13:62–65. doi:10.12659/AJCR.882757
17. Lavon O, Goldman R. Adherence to monitoring guidelines of amiodarone adverse reactions. Health Serv Res Manag Epidemiol. 2019;6:2333392819844635. doi:10.1177/2333392819844635
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.