")
Back to Journals » Clinical Ophthalmology » Volume 17
Timing of Jones Tube Placement After Excision of Nasal or Lacrimal Drainage System Malignancy: A Survey of the American Society of Ophthalmic Plastic and Reconstructive Surgery (ASOPRS)
Authors Kornhauser T, Ponder CM, Dockery PW, Sharabura AB, Brock W, Nguyen J, Pemberton JD
Received 13 June 2023
Accepted for publication 30 August 2023
Published 16 October 2023 Volume 2023:17 Pages 3057—3062
DOI https://doi.org/10.2147/OPTH.S425716
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Tom Kornhauser,1 Christian M Ponder,1 Philip W Dockery,1 Anna B Sharabura,2 Wade Brock,2,3 John Nguyen,4 John D Pemberton1
1Jones Eye Institute, University of Arkansas for Medical Sciences, Little Rock, AR, USA; 2College of Medicine, University of Arkansas for Medical Sciences, Little Rock, AR, USA; 3Arkansas Oculoplastic Surgery, PLLC, Little Rock, AR, USA; 4West Virginia University, Department of Ophthalmology and Visual Sciences, Department of Otolaryngology and Head and Neck Cancer, Morgantown, WV, USA
Correspondence: Tom Kornhauser, Jones Eye Institute, University of Arkansas for Medical Sciences, 4301 W. Markham Street, Little Rock, AR, 72207, USA, Tel +501-686-5822, Fax +501-686-7037, Email [email protected]
Purpose: To elicit, from a survey of oculoplastic surgeons, the timing and reason for delaying Jones tube placement after the excision of nasal or lacrimal drainage system malignancy.
Methods: The authors reviewed current literature and distributed an anonymous survey to 627 members of the American Society of Ophthalmic Plastic and Reconstructive Surgery (ASOPRS) to determine the length of time members wait to perform a Jones tube placement after the removal of nasal or lacrimal drainage system malignancy. The survey also included questions about the rationale for this waiting period.
Results: Fifty-eight members of ASOPRS (9.3%) responded to our survey, 49 (84.4%) of whom had performed Jones tube placement on patients who had an excision of a nasal or lacrimal drainage system malignancy. Nearly 52% of respondents waited one year for Jones tube placement. However, a sizeable number of respondents opted to wait five years (15.1%). The most common rationale for waiting was a concern for tumor recurrence (42 responses).
Conclusion: There is no consensus on when to perform Jones tube placement after the excision of nasal or lacrimal drainage system malignancy. This survey demonstrates a broad array of waiting periods between operations, although most surgeons wait 12 months.
Keywords: Conjunctivodacryocystorhinostomy, cDCR, Jones Tube, Malignant Neoplasm
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Shah has been published for this article.
Introduction
Conjunctivodacryocystorhinostomy (cDCR) with placement of a Jones tube, first performed in 1965 by Lester Jones, has remained the gold standard for the management of upper lacrimal system obstructions.1 Surgeons use Jones tube placement when the upper lacrimal duct system cannot be used to correct symptomatic epiphora.2,3 The 2022–2023 Oculofacial Plastic and Orbital Surgery from the American Academy of Ophthalmology’s Basic and Clinical Science Course states that when a neoplasm is present in the medial canthal area, a complete resection may include removing the puncta and canaliculi. Before considering connecting the lacrimal drainage system with the middle meatus, a histologic examination of the excised tissue should be performed to ensure the tumor was completely removed.4
Additionally, a chapter in “Principles and Practice of Lacrimal Surgery”, published in 2018, states,
If there is no regional or local tumor presence or recurrence, a cDCR with a Lester Jones tube is often performed four to five years after the initial treatment.5
However, no references to those statements were given. Currently, no peer-reviewed literature provides recommendations on the timing of Jones tube placement after the excision of nasal or lacrimal drainage system malignancy. We aim to determine the length of time oculoplastic surgeons wait to perform a Jones tube placement and the rationale for their delay.
Methods
We collected data via a cross-sectional study by distributing an anonymous newly developed web-based survey to 627 active members of the American Society of Ophthalmic Plastic and Reconstructive Surgery (ASOPRS) who were listed in 2020. This study was compliant with Health Insurance Portability and the Accountability Act, and was conducted following the Declaration of Helsinki. Based on the nature of the study being solely a survey with no interventions or experiments involving human subjects, the Institutional Review Board (IRB) approval is not required. The questions asked were:
- Have you ever performed Jones tube placement on patients after they had a nasal or lacrimal drainage system malignancy excision?
- Were you taught a length of time to wait before placing a Jones tube after the excision of a nasal or lacrimal drainage system malignancy, as part of your formal training?
- If you answered yes to question 2, what length of time were you taught to wait?
- What was the rationale for the wait time?
- After performing a Jones tube placement, have you encountered tumor recurrence along the fistula?
Questions 1, 2, and 5 required a “yes” or “no” answer, while questions 3 and 4 were open-ended. The survey was conducted from August 2020 to March 2021. Only respondents who completed more than 50% of the survey were included in the analysis. Results were summarized purely by counts and percentages. The mode was used to summarize the length of time to wait. The data is presented as observational and no additional analyses were performed.
Results
Of the 627 ASOPRS members to whom the survey was distributed, 58 (9.3%) responded. Table 1 shows the results of the survey. A Jones tube placement following the excision of a nasal or lacrimal drainage system malignancy was performed by 49 (84.4%) respondents. Thirty-three (56.9%) respondents received training on the proper timing to carry out a Jones tube placement following the excision of a nasal or lacrimal drainage system malignancy. Those 33 respondents reported the following wait times: 3 months (1 responder [3.0%]), 3–6 months (1 responder [3.0%]), six months (4 responders [12.1%]), one year (17 responders [51.5%]), two years (1 responder [3.0%]), 2–5 years (1 responder [3.0%]), 4–5 years (2 responders [6.0%]), five years (5 responders [15.1%]), and “variable” (1 responder [3%]). The most common (taught) waiting time frame was one year (51.5% of responses, range: 3 to 60 months) between the malignancy resection and a Jones tube placement. The most common reason for delaying a Jones tube placement was a concern for local recurrence (42 responses). Additional rationales were: allowing for appropriate healing time after malignancy resection (12 responses), results of histopathologic diagnosis and tumor margins (6 responses), waiting for symptomatic epiphora to develop (4 responses), waiting for completion of adjuvant treatment (3 responses), and waiting for post-surgical reconstruction (3 responses). Eight (13.8%) respondents reported tumor extension into the nasal cavity through the fistula following a Jones tube placement.
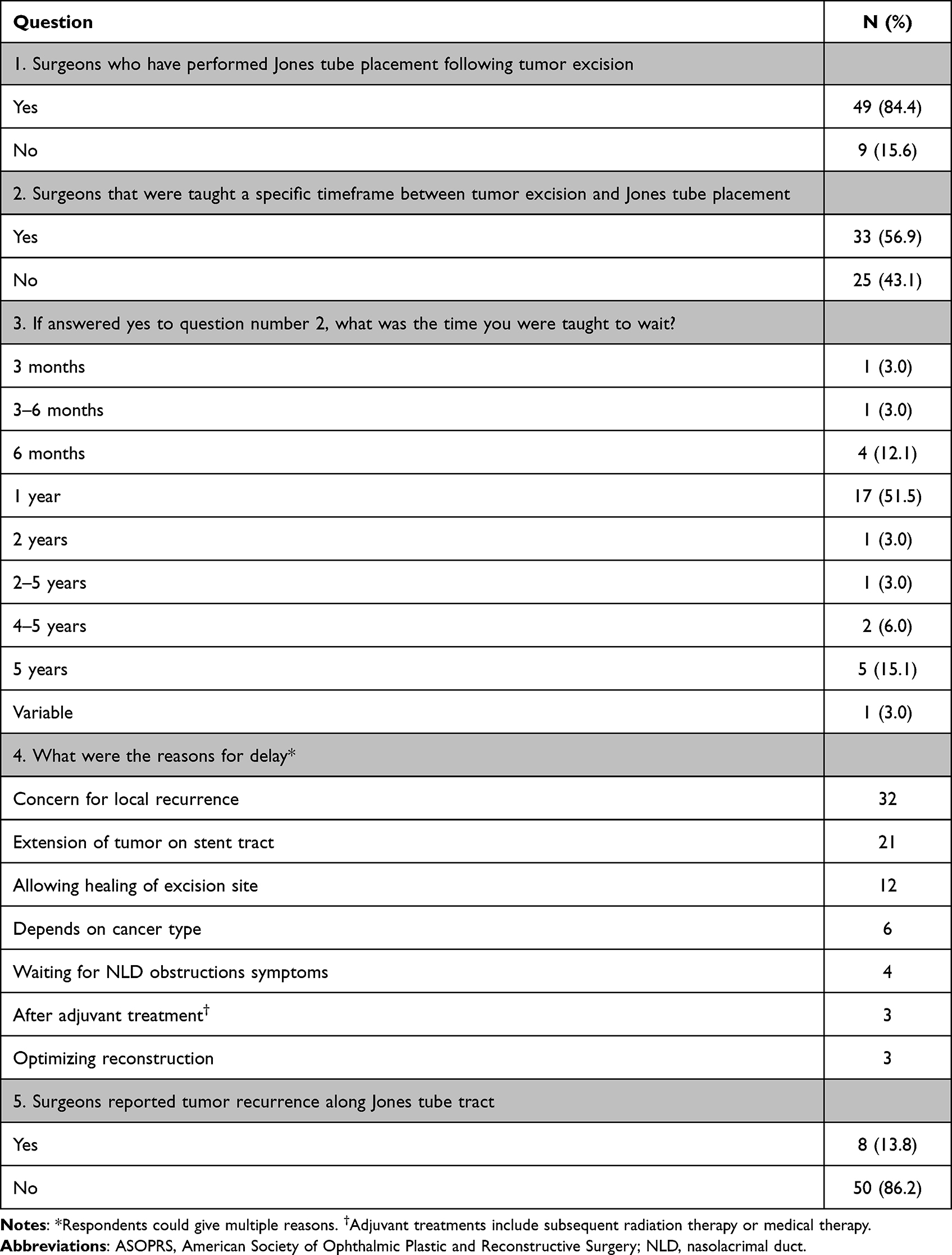 |
Table 1 Survey Results from ASOPRS Members (n=58) |
Discussion
Malignant tumors and their excision are rare causes of lacrimal duct obstruction compared to trauma, infection, and inflammatory conditions. However, malignancy does pose additional concerns, such as recurrence and metastasis.6 The optimal timing for a Jones tube placement after excising nasal or lacrimal drainage system malignancy remains unknown because the literature is limited to information on surgical efficacy, techniques, and complications. Although timing is unknown, survey respondents reported a range of 3 months to 5 years of waiting, with the most frequent time frame reported being one year (51.5% of responses). The most common rationale for waiting before proceeding with Jones tube placement was malignancy recurrence.
We reviewed large case series with long follow-up periods to determine whether the recurrence of malignancy is a reasonable rationale to delay a Jones tube placement. The most significant cohort to date was published by Song et al, where ninety cases of malignant lacrimal sac tumors were monitored. For all participants, the 5-year overall survival rate was 85.7%, and the 5-year progression-free survival rate was 77.9%. Both survival measures between squamous cell carcinoma (69 cases) and non-squamous cell carcinoma showed no significant differences (21 cases).7 Smaller cohorts also experienced a low chance of recurrence after removing lacrimal sac tumors, with follow-up periods of up to 68 months.8–10 Surgical techniques could further reduce the risk of recurrence. Ni et al found that the recurrence rate is directly related to the initial tumor excision technique, with 12.5% recurrence for wide excision versus 43.7% recurrence in cases of isolated lacrimal sac resection.11
Eight surgeons (13.8%) reported tumor recurrence along the Jones tube fistula (question number 5). Due to the nature of the close-ended question, some details remain unknown such as whether the diagnosis of a recurrence along the tube was confirmed histologically or if it was an invasion of the tumor to the adjacent tissue unrelated to the Jones tube. In theory, disruption of the bone barrier in osteotomy and inadvertent incision into the lacrimal sac potentiates dissemination of tumor cells into the nasal cavity and overlying skin. However, the usual surgical procedure is a combined medial maxillectomy and medial orbitotomy for en bloc resection of the tumor.8 This wide excision eliminates the bone as a possible barrier for tumor invasion. After reviewing the current literature, we did not find any documented cases of direct tumor seeding after rehabilitative surgery due to nasal or lacrimal drainage system malignancy.
The rationale for waiting to perform a Jones tube placement based on the cancer type (6 responses) also seems valid as tumor type on pathology and tumor growth pattern are significant determinants of the patient’s prognosis and mortality rate. Although there is not enough information on recurrence based on the specific tumor type, we can possibly deduce that tumors with higher mortality rates point to higher rates of recurrence. For example, papillary squamous carcinoma has a more favorable prognosis (mortality 14%), while transitional cell carcinoma has a poor prognosis, with mortality reaching 100%. Recurrence and mortality rates for nonepithelial lacrimal sac tumors other than lymphoma vary greatly and cannot be generalized due to their rarity. Malignant melanoma is often fatal despite aggressive treatment.12,13 Singh et al reviewed lymphoproliferative tumors involving the lacrimal drainage system. Most tumors (63%) primarily involved the lacrimal sac. The most common sub-type was diffuse large B-cell lymphoma (43%), where successful outcomes could be achieved in all the cases without local recurrence after successful treatment at a mean follow-up of 19 months; however, 15% died of the systemic disease after a mean of 18 months from the time of lacrimal sac involvement.14 Additional rationales are summarized in Table 1.
Calvano et al created a survey to help define current clinical practices regarding the waiting period before cDCR after the excision of medial canthal skin tumors, such as basal cell carcinoma, squamous cell carcinoma, sebaceous cell carcinoma, melanoma, and other adnexal cancers. In this study, most oculoplastic surgeons waited at least 12 months before performing a cDCR. Less than 25% of surgeons will perform a cDCR before 12 months if the patient is diagnosed with basal cell carcinoma, squamous cell carcinoma, sebaceous carcinoma, or melanoma. It was also found that 14% of surgeons observed tumor recurrence following a cDCR surgery.15 The results of our survey corroborate these findings.
Our study’s limitations include a relatively low response rate (9%). This value can likely be explained by the rarity of nasal or lacrimal drainage system malignancies; therefore, surgeons might not fill out the survey because they have not encountered these malignancies before. Questions three and four were open-ended, which contained unstructured answers and were difficult to analyze. Multiple-choice questions would allow better data collection. Another constraint was the limited scope of information gathered in this questionnaire, as some surgeons did not answer all questions. This weakness limits the study’s ability to show some clinically important relationships, such as appropriate timing for specific tumors or whether years of experience or number of cases correlates with a preferred waiting period. Question five was a close-ended binary question (yes/no) about recurrence along the Jones tube fistula after resection, but we should have asked for more details as we were left with unanswered questions. Interesting follow-up questions would have been: if you had seen recurrence along the Jones tube fistula, what type of tumor was it, and how much time passed between the initial tumor excision, placement of the Jones tube, and the tumor’s recurrence? Additionally, this newly developed survey has not undergone a pretesting phase, which could have prevented the aforementioned weaknesses. Finally, the nature of the study as a survey poses a weakness as respondents may skew results with biases.
In the majority of patients, tear production diminishes along with the severity of epiphora during the follow-up period. Consequently, the necessity for cDCR surgery, particularly among elderly patients, might be lessened. Moreover, a notable subset of patients necessitates radiotherapy, which also contributes to reduced tear production due to its impact on ocular surface conditions. Consequently, it could be reasonable to anticipate a natural attenuation of epiphora before resorting to cDCR, particularly among elderly patients and those undergoing radiotherapy.
Finally, future studies or clinical trials may be necessary to determine the most appropriate waiting time for each type of tumor.
Conclusion
While there is no consensus for the waiting period between excising a nasal or lacrimal drainage system malignancy and Jones tube placement, though most surgeons who answered our survey were taught to wait one year between surgeries (51.5%). The main rationales were the concern of recurrence, the extension of the tumor along the Jones tube fistula, proper healing of the excision site, and the type of tumor.
Our literature review suggests that tumor recurrence is uncommon in these rare malignancies and appears to be type specific. Long-term, even lifetime, follow-up is required, as recurrence and metastases can still occur many years after primary management. Based on these findings, we propose that a Jones tube placement can be considered in patients with symptomatic epiphora that affect daily activities. Waiting a year seems prudent based on the results from our survey and literature review.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of this article.
References
1. Steele EA. Conjunctivodacryocystorhinostomy with Jones tube: a history and update. Curr Opin Ophthalmol. 2016;27(5):439–442. doi:10.1097/ICU.0000000000000287
2. Zilelioĝlu G, Gündüz K. Conjunctivodacryocystorhinostomy with Jones tube. Doc Ophthalmol. 1996;92(2):97–105. doi:10.1007/BF02583282
3. Trotter WL, Meyer DR. Endoscopic Conjunctivodacryocystorhinostomy with Jones tube placement. Ophthalmology. 2000;107(6):1206–1209. doi:10.1016/S0161-6420(00)00119-6
4. Korn BS, Burkat CN, Carter KD, et al. 2022–2023 basic and clinical science course, section 07: oculofacial plastic and orbital surgery. Am Acad Ophthalmol. 2022;2022:303.
5. Gangadhara S. Tumors of the Lacrimal Drainage System. In: Javed Ali M, editor. Principles and Practice of Lacrimal Surgery. Springer Nature Singapore Pte Ltd; 2018:420.
6. Coloma-González I, Flores-Preciado J, Ceriotto A, Corredor-Casas S, Salcedo-Casillas G. Lacrimal sac tumors presenting as lacrimal obstruction. Retrospective study in Mexican patients 2007–2012. Archivos de la Sociedad Española de Oftalmología. 2014;89(6):222–225. doi:10.1016/j.oftal.2014.02.009
7. Song X, Wang J, Wang S, Wang W, Wang S, Zhu W. Clinical analysis of 90 cases of malignant lacrimal sac tumor. Graefes Arch Clin Exp Ophthalmol. 2018;256(7):1333–1338. doi:10.1007/s00417-018-3962-4
8. Alabiad CR, Weed DT, Walker TJ, et al. En bloc resection of lacrimal sac tumors and simultaneous orbital reconstruction: surgical and functional outcomes. Ophthalmic Plast Reconstr Surg. 2014;30(6):459–467. doi:10.1097/IOP.0000000000000134
9. Montalban A, Liétin B, Louvrier C, et al. Malignant lacrimal sac tumors. Eur Ann Otorhinolaryngol Head Neck Dis. 2010;127(5):165–172. doi:10.1016/j.anorl.2010.09.001
10. Zhang R, Qian J, Meng F, et al. A staged procedure in the treatment of primary lacrimal sac epithelial malignancy: a retrospective cases analysis. Ophthalmic Plast Reconstr Surg. 2019;35(2):187–192. doi:10.1097/IOP.0000000000001206
11. Ni C, D’Amico DJ, Fan CQ, Kuo PK. Tumors of the lacrimal sac: a clinicopathological analysis of 82 cases. Int Ophthalmol Clin. 1982;22(1):121–140. doi:10.1097/00004397-198202210-00010
12. Kim HJ, Shields CL, Langer PD. Lacrimal sac tumors: diagnosis and treatment. In: Smith and Nesi’s Ophthalmic Plastic and Reconstructive Surgery. Springer; 2021:497–503.
13. Krishna Y, Coupland SE. Lacrimal sac tumors—a review. Asia Pacific J Ophthalmol. 2017;6(2):173–178. doi:10.22608/APO.201713
14. Singh S, Ali MJ. Lymphoproliferative tumors involving the lacrimal drainage system: a major review. Orbit. 2020;39(4):276–284. doi:10.1080/01676830.2019.1634104
15. Calvano CJ, Servat JJ, Black EH. Need for lacrimal bypass surgery after medial canthal tumor resection: survey of current practices. Arch Clin Exp Surg. 2012;2(1):1–7. doi:10.5455/aces.20120527053925
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.