Back to Journals » International Journal of General Medicine » Volume 15
Time Window for Acute Stroke Management: A Cross-Sectional Study Among Community Healthcare Practitioners in Primary Care
Authors Yang H ![]() , Huang X
, Huang X ![]() , Yang C, Zhu S, Chen X, Zhang M, Yu X
, Yang C, Zhu S, Chen X, Zhang M, Yu X ![]() , Wang HHX
, Wang HHX ![]()
Received 4 February 2022
Accepted for publication 14 April 2022
Published 29 April 2022 Volume 2022:15 Pages 4483—4493
DOI https://doi.org/10.2147/IJGM.S361189
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Huajie Yang,1,* Xiang Huang,2,* Chunyu Yang,3 Sufen Zhu,4 Xiaoyi Chen,5 Man Zhang,2 Xiao Yu,3 Harry HX Wang3,6,7
1School of Health Technology, Guangdong Open University (Guangdong Polytechnic Institute), Guangzhou, People’s Republic of China; 2Department of Public Health, Sanxiang Community Health Service Centre of Zhongshan, Zhongshan, People’s Republic of China; 3School of Public Health, Sun Yat-Sen University, Guangzhou, People’s Republic of China; 4Nuffield Department of Primary Care Health Sciences, University of Oxford, Oxford, UK; 5School of Nursing, Sun Yat-Sen University, Guangzhou, People’s Republic of China; 6Department of General Practice, The Second Hospital of Hebei Medical University, Shijiazhuang, People’s Republic of China; 7JC School of Public Health and Primary Care, Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong Special Administrative Region
*These authors contributed equally to this work
Correspondence: Harry HX Wang, School of Public Health, Sun Yat-Sen University, Guangzhou, People’s Republic of China, Tel +86 20 87330672, Email [email protected]; [email protected] Huajie Yang, School of Health Technology, Guangdong Open University (Guangdong Polytechnic Institute), Guangzhou, 510091, People’s Republic of China, Tel +86 760 89911522, Email [email protected]
Introduction: Time-to-treatment window is critical for managing acute ischaemic stroke. The community healthcare practitioners (CHPs) who deliver frontline care in the health system play an important role in stroke prevention and treatment.
Methods: A multi-stage sampling design was adopted in Guangdong province, China. A total of 997 CHPs who participated in the survey were divided into two groups (the awareness group vs the unawareness group) according to their knowledge on the time window for stroke management. Logistic regression analysis was performed to explore factors associated with the awareness of “time window”.
Results: Overall, less than half (49.1%) of CHPs were aware of the time window for stroke management. The proportion of CHPs who were able to recognise stroke symptoms were higher in the awareness group (42.7%) than that in the unawareness group (38.8%). Most CHPs (82.9%) in the awareness group had the knowledge about the effectiveness of intravenous thrombolysis in treating acute cerebral infarction, whereas this was perceived by only less than half (43.6%) of CHPs in the unawareness group. Factors associated with the knowledge of time window for stroke management included participation in cerebrovascular disease management training (adjusted odds ratio [aOR]=4.203, 95% CI: 1.707– 10.348, p=0.002), awareness of the time frame for CT initiation (aOR=5.214, 95% CI: 1.803– 15.078, p=0.002) and for urokinase thrombolysis administration (aOR=11.927, 95% CI: 4.393– 32.382, p< 0.001), accurate perceptions about the target for blood pressure lowering (aOR=4.181, 95% CI: 1.713– 10.207, p=0.002) and blood glucose control (aOR=2.446, 95% CI: 1.019– 5.869, p=0.045), and the familiarity with prehospital stroke management principles (aOR=3.593, 95% CI: 1.383– 9.332, p=0.009).
Conclusion: The CHPs need to enhance their ability to address the acute ischaemic stroke onset promptly to provide effective treatment within the beneficial “time window”. This may help improve the stroke chain of survival with better multidisciplinary decision support systems that enable optimal stroke care delivery.
Keywords: time window, stroke, cross-sectional study, primary care
Introduction
Acute stroke is a medical and surgical emergency, with the outcome of care closely related to time to treatment. The period from the onset of stroke to the start of treatment is defined as “time window”. Patients with acute ischaemic stroke should be admitted to the hospital as soon as possible, and receive thrombolytic therapy within 1 hour of admission according to the National Institute of Neurological Disorders and Stroke (NINDS) standards,1 yet substantial efforts are still needed to understand and minimise both prehospital delays and in-hospital delays.2 However, most healthcare providers have difficulties in achieving the NINDS standards, particularly in developing countries.3 Even in developed countries, only 20.0–35.8%4–8 of patients were admitted within the time window for stroke management and prehospital delays are more severe than in-hospital delays.2,9–12
Nevertheless, studies have shown that thrombolytic therapy for patients with acute stroke is not always delivered in time.13–15 The stroke chain of survival highlights a timely administration of thrombolytic therapy after patients arrive at the hospital. As the main decision makers in the emergency care of stroke, physicians should have adequate capacity to recognise and treat stroke accurately and promptly within the beneficial “time window”. Therefore, it is important to understand physicians’ knowledge of and attitudes towards thrombolytic therapy to optimise the use of the therapy. The community healthcare practitioners (CHPs) who deliver frontline care in the health system play an important role in stroke management.16
Since the launch of a comprehensive health care reform in 2009, the Chinese government has established a strengthened primary care system covering both urban and rural areas. The three-tier health system is underpinned by the community-level primary care institutions who provide diagnosis, initial treatment, and triage for acute and chronic medical care coordinated with secondary and tertiary hospitals. The Chinese government has also built a community health service (CHS) infrastructure which allows access to primary care within a 15-minute walking distance. Therefore, the CHPs are positioned as residents’ health gatekeepers, who mainly provide health care services in community health centres (CHCs).17,18 Moreover, in the context of the nationwide delivery of the basic public health service package, the CHPs are responsible for managing chronic conditions including hypertension and diabetes.19 They are also encouraged to attend a variety of continuing medical education and specialised training seminars to enhance the interface between general practice (GP) and specialist care.
Given that the GP practitioners have been engaged in a gatekeeping role, the ability of CHPs to recognise stroke onset as early as possible and further manage the referral via green channel to emergency department at the superior hospital becomes critical. We therefore aimed to evaluate knowledge of time window for stroke management among CHPs in primary care and explore factors associated with the awareness of “time window”.
Methods
Study Design and Subjects
This study selected 9 community health centres (CHCs) including subordinate stations in Pearl River Delta of Guangdong province in southern China using a multi-stage sampling design. In the first stage, we selected three cities, namely Guangzhou, Zhongshan, and Foshan. In the second stage, we randomly chose three districts in each city, respectively. In the third stage, we used a random sampling method to select one CHC in each district, respectively. At present, there are 20 tertiary-level institutions (including universities and colleges) which offer major courses in medicine – ie, nursing course are available in 19 institutions in Guangzhou and 1 institution in Foshan; and clinical medicine courses are available in 6 institutions in Guangzhou. According to the regulations of the National Health Commission of China, all medical practitioners working at the CHCs are required to complete either a standardised GP training programme or on-The-job GP training curriculum. In this study, the targeted subjects were CHPs at CHCs who completed either of the above training activities launched by the Guangdong General Practice Education and Training Centre commissioned by the local health authorities in Guangdong province.
Baseline data were collected between October and December 2018 by the use of a questionnaire with items derived from a previously validated survey conducted in our previous study.20 The questionnaire included items on demographic characteristics, knowledge of the symptoms and treatment of stroke, training on first aid for stroke, and the perceptions about the time window for stroke management. A total of 10 common symptoms of stroke incidence included (1) weakness or numbness in one limb, (2) numbness on one side or distortion of commissure, (3) speech disturbance or difficulty in understanding speech, (4) double gaze to one side, (5) sudden blurring of vision or double vision, (6) dizziness and balance disturbance, (7) sudden chest pain with dyspnoea and sweating, (8) persistent headache, (9) sudden headache or change in headache pattern and vomiting, and (10) disturbance of consciousness or convulsions.
On items related to knowledge of stroke management, the recommended target for lowering blood pressure (ie, systolic blood pressure <140 mmHg and/or diastolic blood pressure <90 mmHg) and blood glucose (ie, fasting blood glucose <7 mmol/L) among stroke patients were consistent with the standards in the Chinese Guidelines for Cerebrovascular Diseases Prevention and Treatment21 and the National Basic Public Health Service Guideline (Third Edition)22 issued by the National Health Commission, China.
Participants’ perceptions about the time window for stroke management were evaluated by using the criteria recommended by the NINDS. These included: (1) CT examinations should be initiated within 25 minutes of the patient’s arrival at the emergency room; (2) CT examination reports should be obtained within 45 minutes after the patient’s arrival at the emergency room; (3) intravenous thrombolytic therapy with rt-PA should be administered within 4.5 hours from symptom onset; (4) intravenous thrombolytic therapy with urokinase should be administered within 6 hours from symptom onset; and (5) intravenous thrombolysis with rt-PA or urokinase is an effective treatment for cerebral infarction.
All items in the questionnaire were discussed through focus groups and panel reviews. Surveys were conducted in an anonymous manner by trained investigators following a standard protocol. The content validity index of the questionnaire was 0.91. Reliability of the questionnaire was assessed through a pilot study among 30 CHPs in Zhongshan. The Cronbach’s alpha was 0.85, and the intra-class correlation coefficient was 0.92, which showed good internal reliability.
Analysis
We used the EpiData software (version 3.1) for data entry. All questionnaires were checked for completeness and data accuracy through double entry. All participants were divided into two groups based on their responses to the question on whether they were aware of time window for stroke management (ie, the time from the stroke onset to hospital arrival and treatment with intravenous thrombolysis) for comparative analysis. We used the SAS software (8.2, SAS Institute Inc., Cary, NC, USA) for data analysis and presented the data as rates. The chi-square test was used to analyse the between-group differences. All significance levels were set to 0.05.
To investigate factors associated with knowledge of the time window for stroke management, we used an unconditional logistic regression model. The variable selection for multiple regression analysis was conducted using a stepwise entry process, with the dependent variable on “knowing the time window for stroke management” (1 = yes, 0 = no). We also applied a univariate logistic regression model where variables on age, gender, education level, job type, professional title, years of working, knowledge of the symptoms and treatment of stroke, and participation in the training on first aid for stroke were taken into account. Variables that were statistically significant in the univariate analysis were included as independent variables in the multivariable logistic regression model using backward LR method. The inclusion and exclusion standard for significant associations were set to 0.05 and 0.10, respectively. The degree of association between independent variables with the dependent variable (ie, “knowing the time window for stroke management”) was estimated by odds ratio (OR) with 95% confidence interval (CI).
Results
Basic Demographic Information
The study consisted of 997 CHPs, of whom less than half (49.1% [490/997]) were aware of the time window for stroke management. There were significant differences with respect to gender, education levels, professions, professional title, and years of working experience (all P<0.05) between the awareness and unawareness groups. Most of the study participants were women. The mean age of CHPs in the awareness group was higher than that in the unawareness group. The proportion of CHPs with junior college education level in the awareness group (57.3%) was higher than that in the unawareness group (51.7%). There were more GP physicians in the awareness group (32.9%) than that in the unawareness group (11.8%). The proportion of CHPs with a professional title below junior level in the unawareness group and awareness group was 18.8% and 15.9%, respectively. The proportion of CHPs with more than 10 years of working experience in the awareness group (42.7%) was higher than that in the unawareness group (36.5%). It was also found that 43.9% and 16.4% of CHPs with a prior working background in the field of internal medicine before working in primary care in the awareness group and the unawareness group, respectively. The proportion of CHPs who worked in CHCs since graduation was higher in the awareness group (30.2% vs 21.1%) when compared to that in the unawareness group (Table 1).
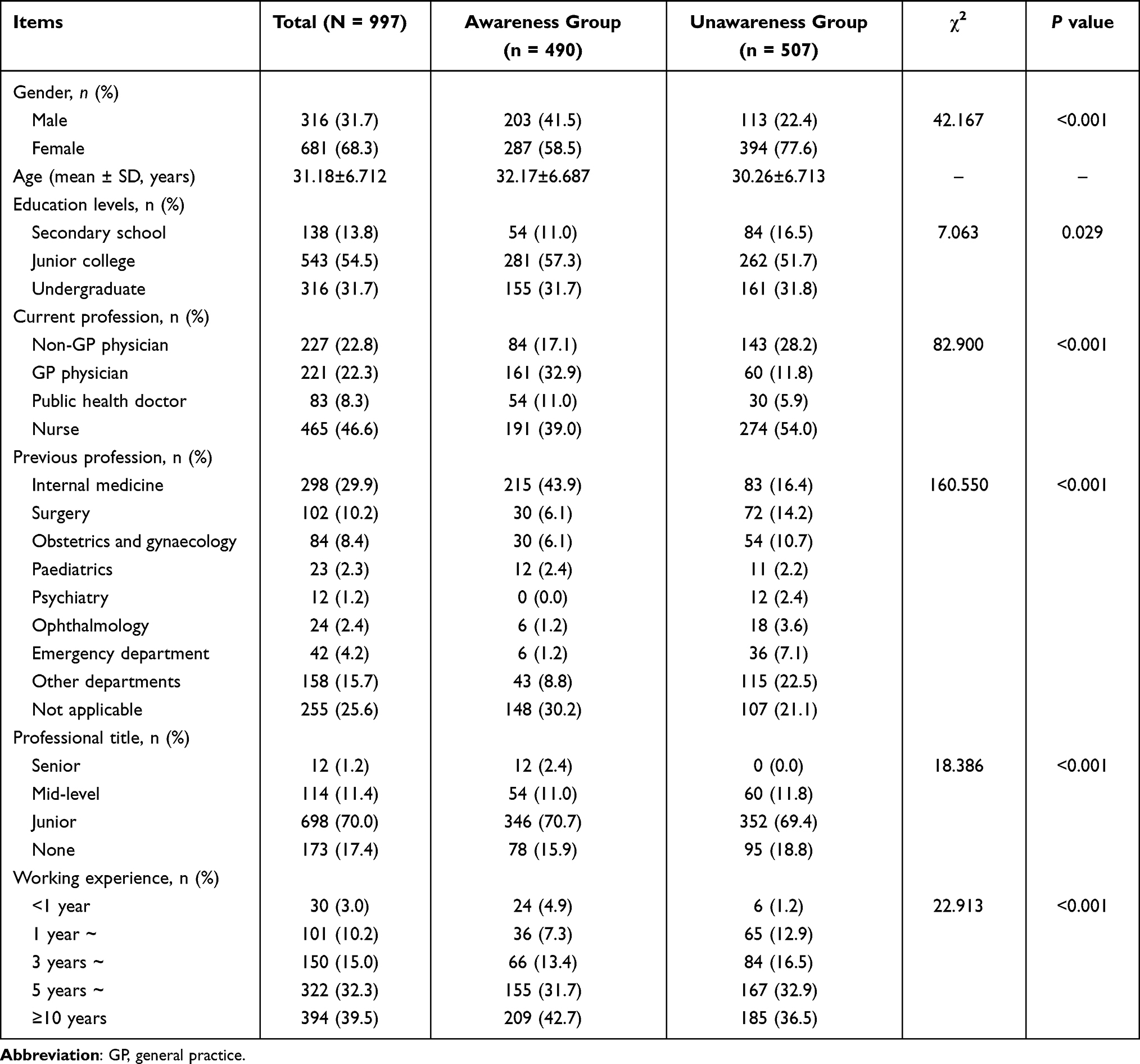 |
Table 1 Demographic Characteristics of Community Healthcare Practitioners |
Perceptions of Symptoms, Treatments and Training on First Aid for Stroke
The proportion of CHPs who knew the guidelines for the management of cerebrovascular disease well (15.8%) was higher in the awareness group than that in the unawareness group (7.1%). The proportion of CHPs who did not know about transient ischaemic attack (TIA) in the unawareness group was 7.1% while all CHPs in the awareness group reported having knowledge of TIA. The proportion of CHPs who did not know about the types of stroke was higher in the unawareness group (3.5%) than that in the awareness group (1.2%). The proportion of CHPs who were able to recognise all 10 symptoms of stroke was higher in the awareness group (42.7%) than that in the unawareness group (38.8%). There were significant differences between the two groups in terms of the familiarity with the guidelines for the prevention and treatment of cerebrovascular diseases, and knowledge of TIA and types of stroke (Table 2).
 |
Table 2 Perceptions About the Symptoms, Treatment and Training of First Aid for Stroke |
The results also showed that in general the CHPs had the knowledge of the documentation of medical history, prehospital management measures, and content of health education for stroke prevention and treatment. However, the knowledge of the medical history documentation and prehospital management was slightly higher among CHPs in the awareness group than that in the unawareness group. The proportion of CHPs in the awareness group who believed that thrombolytic therapy was suitable for cerebral infarction was higher (82.9%) than that in the unawareness group (43.6%). It was also shown that 63.4% and 43.5% of CHPs in the awareness group and unawareness group had accurate perceptions about the treatment target for blood pressure lowering, respectively; and that 67.1% and 57.6% of CHPs in the awareness group and unawareness group had accurate perceptions about the treatment target for fasting blood glucose control, respectively (Table 2).
Of all subjects, 48.8% of CHPs in the awareness group reported participation in training on cerebrovascular disease management, 34.1% reported experiences in community-based screening for early detection of stroke, 25.6% reported attendance in seminars/training on the first aid for stroke, and 11.0% reported attendance in seminars/training on the use of National Institutes of Health Stroke Scale (NIHSS) rating scale. In the unawareness group, 23.5% of CHPS reported participation in training on cerebrovascular disease management, 11.8% reported experiences in community-based stroke screening programmes, 21.2% reported attendance in seminars/training on the first aid for stroke, and 7.1% reported attendance in seminars/training on the use of NIHSS. There were significant differences regarding participation in training on cerebrovascular disease management, experiences in community-based stroke screening programmes, and attendance in seminars/training on the use of NIHSS between the two groups (Table 2).
Perceptions of the Time Window for Acute Ischaemic Stroke Management
Based on the concept on time window for stroke management recommended by the NINDS (Figure 1 Flow chart of time window for stroke treatment based on the NINDS recommendations), it was found that slightly more CHPs in the awareness group (23.2%) believed that the CT examinations should be conducted within 25 minutes of the patient’s arrival at the emergency room when compared to that in the unawareness group (22.4%). A higher proportion of CHPs in the awareness group believed that intravenous thrombolysis with rt-PA or urokinase was an effective treatment for cerebral infarction (82.9% vs 43.5%). The recommendations that the time window for intravenous thrombolytic therapy with urokinase be administered within 6 hours from stroke onset was perceived by a higher proportion of CHPs in the awareness group (68.3%) than that in the unawareness group (21.2%). The differences regarding the time frame for obtaining CT reports, the perceived effectiveness of intravenous thrombolysis for cerebral infarction, and the time frame for intravenous thrombolysis were significant between the two groups (Table 3).
 |
Table 3 Perceptions About the Time Window for Stroke Treatment |
 |
Figure 1 Flow chart of time window for stroke treatment based on the NINDS recommendations. |
Factors Associated with the Knowledge of Time Window for Stroke Management
Results of the multivariable logistic regression demonstrated that factors associated with the knowledge of time window for stroke management included participation in cerebrovascular disease management training, awareness of the time frame for CT initiation and for thrombolysis with urokinase, accurate perceptions about the target for blood pressure lowering and blood glucose control, and the familiarity with prehospital stroke management principles (Table 4).
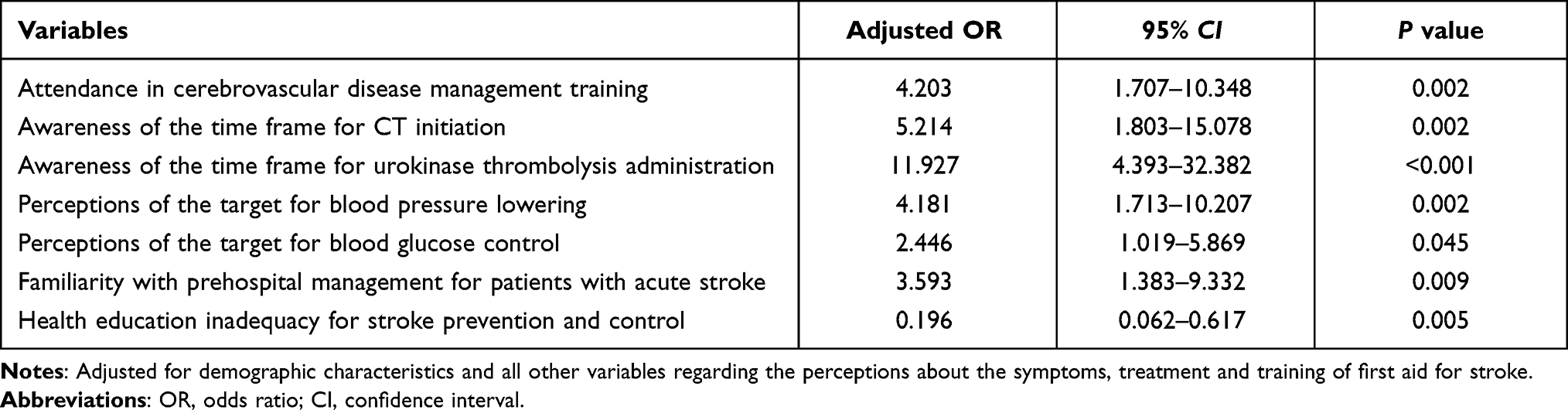 |
Table 4 Factors Associated with Health Care Practitioners’ Knowledge of the Time Window for Stroke Treatment |
Discussion
Existing evidence shows strong association between the time to treatment and the outcome of stroke.23 Hence it is critical for acute stroke management to be delivered in rapid response to the stroke emergency. The concept of “time window” developed by the US NINDS1 indicates the importance of timely treatment for patient with acute stroke and could help in achieving more favourable outcome.
Healthcare practitioners are expected to have advanced understanding and enhanced ability to provide appropriate and prompt treatment for stroke onset as they serve key decision makers and problem solver. The results of this study showed that the education level and the knowledge about the “time window” among CHPs was overall suboptimal, with less than one third having a bachelor degree and less than half who were aware of the time window for stroke management. The finding that GP physicians tended to have a significantly higher awareness rate of the time window than non-GP physicians was consistent with that of another Chinese study.24 This suggests that the nationwide, community-based GP training programme in China may have a positive impact on raising the awareness of emergency stroke care among CHPs.
Lack of knowledge about stroke symptoms and insufficient attention paid to thrombolytic therapy among CHPs may cause pre-hospital delays. We found that 15.8% of the CHPs in the awareness group were very familiar with the current Chinese Guidelines for Cerebrovascular Diseases Prevention and Treatment; and this percentage was almost twice that in the unawareness group. In addition, our results revealed that the CHP’s knowledge of stroke symptoms was insufficient, which was also consistent with findings from other studies.25,26 We also demonstrated a lack of knowledge among CHPs about the time window for stroke management recommended by the NINDS (Table 3). As a consequence, the efficiency of patient management, especially with regard to employing appropriate decision choices after the stroke onset within the limited time window for stroke treatment may be hampered.
Multivariable analysis revealed an association between the training on cerebrovascular disease management and the knowledge of the time window for stroke management. The awareness of the time frame for CT initiation was significantly associated with CHP’s knowledge of the “time window”, which implied a critical role of CT examination in acute stroke treatment. Besides, awareness of the time frame for urokinase thrombolysis administration, accurate perceptions about the target for blood pressure lowering and blood glucose control, and the familiarity with prehospital stroke management principles were also factors significantly associated with the higher likelihood of knowing about the “time window”. This implies the room for improvement in terms of targeted training among CHPs on stroke prevention and treatment.
Previous literature suggested that insufficient attention to thrombolytic therapy and a lack of knowledge of the patient’s initial symptoms among the first-contact healthcare practitioners after the stroke onset may lead to prehospital delay.27,28 Our results showed that the knowledge of the symptoms and types of stroke, indications for thrombolytic therapy, and goals for blood pressure and blood glucose control were inadequate among CHPs. This may be explained by the lack of training on cerebrovascular disease management and limited experiences in screening for people at high-risk for stroke. Moreover, the importance of the use of NIHSS among CHPs was further determined in the regression analysis. Consistent with the mass implementation of the GP education and training in China,29,30 the proportion of GP physicians in the awareness group was nearly twice that of non-GP physicians in the unawareness group in our study. This may suggest the favourable impact of the GP training in China. However, given the overall poor education attainment among CHPs, continuing medical education may still be needed to improve the capacity of CHPs in stroke prevention and treatment.31
Strengths and Weaknesses
The Chinese government has launched nationwide, community-based screening programme for populations at high risks for stroke, which indicates that the importance of stroke prevention and treatment has gained increasing attention. Our study focused on the CHP’s awareness of the time window for stroke management recommended by NINDS, which shall carry implications for international comparison. This would also allow for further in-depth investigations to assess the knowledge of vascular cognitive decline in patients with early stage of cerebral small vessel disease.32 Our study may also inform policy-makers with regard to the provision of health education on stroke prevention and treatment at the community level to improve the stroke management in China. This study has several limitations. Firstly, the study was conducted within three cities in one area of Guangdong province in China where the level of economic and social development is relatively higher than other areas in China. Therefore, the generalisation of the study conclusions may be limited. Secondly, the Chinese health authorities previously categorised CHCs into national-, provincial-, and local-levels based on institutional and manpower structure. However, our study did not consider the ranking levels of CHCs and their interface with tertiary-level hospitals in selecting the sample locations, and therefore how the variations of institution-level resources would impact on healthcare needs33 and the stroke chain of survival34 in the context of multidisciplinary team-based service delivery may warrant further investigations.
Conclusion
Given the increase in stroke incidence, it is critical to improve the awareness of the time window-based strategy to strengthen the ability to respond, recognise and treat acute ischaemic stroke, especially for CHPs who are expected to play a gatekeeping role in the health system. It is also of great importance to achieve seamless and integrated management of prehospital and in-hospital care for stroke to avoid delayed access to emergency care. The CHPs should enhance their ability to address the acute ischaemic stroke onset promptly to provide effective treatment within the beneficial “time window”. This may help in improving the stroke chain of survival with better multidisciplinary decision support systems that enable optimal stroke care delivery.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Statement of Ethics
All research activities were conducted with integrity and in line with the generally accepted ethical principles and ethics approval was granted from the School of Public Health Biomedical Research Ethics Review Committee at Sun Yat-Sen University (Ref: SYSU-SPH-2016027). The survey was conducted under the agreement of the medical staff of CHCs, and all participants provided written informed consent prior to study participation.
Acknowledgments
We would like to appreciate the Guangdong Medical Doctor Association of China for their collaboration in this study.
Funding
National Natural Science Foundation of China (grants 72061137002 and 71904212); Basic and Applied Basic Research Foundation of Guangdong Province (grant 2019A1515011381); Higher Education Reform Project of Guangdong Province (grant 20191206-20); Medical Research Project of Zhongshan city of Guangdong Province (grant 2021J447); Young innovative talents project of colleges and universities of Guangdong Province (grant 2019WQNCX173); Special talent project of Guangdong Open University (Guangdong Polytechnic Institute) (grant RC1923); and Guangdong Philosophy and Social Science Project Planning (grant GD19CGL12), PR China.
Disclosure
The authors have no conflicts of interest to declare in this work.
References
1. Marler JR, Winters-Jones P, Emr M, eds. Proceedings of a National Symposium on Rapid Identification and Treatment of Acute Stroke; 1997. Bethesda, Maryland; National Institutes of Health, National Institute of Neurological Disorders and Stroke: 157-158.
2. Evenson KR, Foraker RE, Morris DL, Rosamond WD. A comprehensive review of prehospital and in-hospital delay times in acute stroke care. Int J Stroke. 2009;4(3):187-199. doi:10.1111/j.1747-4949.2009.00276.x
3. Mishra AK, Iyadurai R. Prehospital and hospital delays for stroke patients treated with thrombolysis: access to health care facility - still a bottle neck in stroke care in developing nation. Australas Emerg Care. 2019;22(4):227–228. doi:10.1016/j.auec.2019.07.003
4. Vidale S, Beghi E, Gerardi F, et al. Time to hospital admission and start of treatment in patients with ischemic stroke in northern Italy and predictors of delay. Eur Neurol. 2013;70(5–6):349–355. doi:10.1159/000353300
5. Chen PM, Nguyen DT, Ho JP, et al. Factors influencing acute stroke thrombolytic treatments in Hispanics in the San Diego region. Austin J Cerebrovasc Dis Stroke. 2018;5(1):1074.
6. Silvestrelli G, Parnetti L, Paciaroni M, et al. Early admission to stroke unit influences clinical outcome. Eur J Neurol. 2006;13(3):250–255. doi:10.1111/j.1468-1331.2006.01187.x
7. Reeves MJ, Arora S, Broderick JP, et al. Acute stroke care in the US: results from 4 pilot prototypes of the Paul Coverdell National Acute Stroke Registry. Stroke. 2005;36(6):1232–1240.
8. Wu ZH, Yang HJ, Huang X, et al. Status and influencing factors of in-hospital emergency treatment delay of patients with stroke. Chin Gen Pract. 2017;20(11):1374–1378.
9. Hong KS, Bang OY, Kim JS, et al. Stroke statistics in Korea: part II stroke awareness and acute stroke care, a report from the Korean stroke society and clinical research center for stroke. J Stroke. 2013;15(2):67–77. doi:10.5853/jos.2013.15.2.67
10. Kim YS, Park SS, Bae HJ, et al. Stroke awareness decreases prehospital delay after acute ischemic stroke in Korea. BMC Neurol. 2011;11(1):2. doi:10.1186/1471-2377-11-2
11. Wang Y, Liao X, Zhao X, et al. Using recombinant tissue plasminogen activator to treat acute ischemic stroke in China: analysis of the results from the Chinese National Stroke Registry (CNSR). Stroke. 2011;42(6):1658–1664. doi:10.1161/STROKEAHA.110.604249
12. Yang H, Zhang J, Xie J, et al. Factors influencing pre-hospital delay among acute ischemic stroke patients in the midlands of China. Int J Cardiol. 2014;172(2):533–534. doi:10.1016/j.ijcard.2014.01.047
13. Zhou Z, Liang Y, Qu H, et al. Plasma homocysteine concentrations and risk of intracerebral hemorrhage: a systematic review and meta-analysis. Sci Rep. 2018;8(1):2568. doi:10.1038/s41598-018-21019-3
14. Zylberstein DE, Skoog I, Björkelund C, et al. Homocysteine levels and lacunar brain infarcts in elderly women: the prospective population study of women in Gothenburg. J Am Geriatr Soc. 2008;56(6):1087–1091. doi:10.1111/j.1532-5415.2008.01724.x
15. Zhao D, Liu J, Wang W, et al. Epidemiological transition of stroke in China: twenty-one-year observational study from the Sino-MONICA-Beijing Project. Stroke. 2008;39(6):1668–1674. doi:10.1161/STROKEAHA.107.502807
16. Al Omari M, Khader Y, Al-azzam SI, et al. Knowledge, attitudes and current practice of Jordanian family physicians about prescribing aspirin in primary and secondary prevention of vascular diseases: a self-reported survey. Eur J Cardiovasc Nurs. 2012;11(1):9–13. doi:10.1016/j.ejcnurse.2010.09.003
17. Wang HHX, Wang JJ, Wong SYS, Wong MCS, Mercer SW, Griffiths SM. The development of urban community health centres for strengthening primary care in China: a systematic literature review. Br Med Bull. 2015;116(1):139–153. doi:10.1093/bmb/ldv043
18. Wang HHX, Mercer SW. Perspective from China. In: Watt GCM, editor. The Exceptional Potential of General Practice. London, UK: CRC Press; 2018:189–192.
19. Wang Y, Hu X-J, Wang HHX, et al. Follow-up care delivery in community-based hypertension and type 2 diabetes management: a multi-centre, survey study among rural primary care physicians in China. BMC Fam Pract. 2021;22(1):224. doi:10.1186/s12875-021-01564-z
20. Yang HJ. Study on stroke in-hospital emergency treatment based on the “Time Window”. Hubei, PR China. Huazhong Univ Sci Technol. 2015. doi:10.7666/d.D731935
21. Liu X, Zhang S, Liu M, et al. Chinese guidelines for cerebrovascular diseases prevention and treatment. People’s Medical Publishing House; 2007.
22. National Health Commission, PRC. Introduction on National Basic Public Health Services. Available from: http://www.nhc.gov.cn/jws/tpxw/201504/49bf80b308fb47dbb138f86b1a49a2fc.shtml. Accessed April 20, 2022.
23. Hacke W, Donnan G, Fieschi C, et al. Association of outcome with early stroke treatment: pooled analysis of ATLANTIS, ECASS, and NINDS rt-PA stroke trials. Lancet. 2004;363(9411):768–774.
24. Wang SF, Xiao WM, Chen YK, Zhang J. Investigation on knowledge of intravenous Thrombolysis treatment of Cerebral infarction among clinicians in Dongguan. Chin J Pract Nerv Dis. 2014;17(1):64–66.
25. Nordanstig A, Jood K, Rosengren L. Public stroke awareness and intent to call 112 in Sweden. Acta Neurol Scand. 2014;130(6):400–404. doi:10.1111/ane.12293
26. Zhou Y. The research on influencing factors of thrombolysis in patients with acute ischemic stroke: based on the cognition and behavioral of neurologists and patients. Huazhong Univ Sci Technol. 2017;05:1.
27. Faiz KW, Sundseth A, Thommessen B, Rønning OM. Patient knowledge on stroke risk factors, symptoms and treatment options. Vasc Health Risk Manag. 2018;14:37–40. doi:10.2147/VHRM.S152173
28. Liang SR, Shao JL, Huang YY, Zhang XY, Huang YM. Meta-analysis of influential factors of pre-hospital delay of patients with acute ischemic stroke. Mod Clin Nurs. 2016;15(12):22–28.
29. Wang HHX, Wang JJ, Zhou ZH, Wang XW, Xu L. General practice education and training in southern China: recent development and ongoing challenges under the health care reform. Malays Fam Physician. 2013;8(3):2–10.
30. Wang HHX, Wang JJ. Developing primary care in China. In: Griffiths SM, Tang JL, Yeoh EK, editors. Routledge Handbook of Global Public Health in Asia. London, UK: Routledge; 2014:584–600. doi:10.4324/9781315818719.ch40
31. Li X, Krumholz HM, Yip W, et al. Quality of primary health care in China: challenges and recommendations. Lancet. 2020;395(10239):1802–1812. doi:10.1016/S0140-6736(20)30122-7
32. Blanco-Rojas L, Arboix A, Canovas D, Grau-Olivares M, Oliva Morera JC, Parra O. Cognitive profile in patients with a first-ever lacunar infarct with and without silent lacunes: a comparative study. BMC Neurol. 2013;13(1):203. doi:10.1186/1471-2377-13-203
33. Hu XJ, Wang HHX, Li YT, et al. Healthcare needs, experiences and treatment burden in primary care patients with multimorbidity: an evaluation of process of care from patients’ perspectives. Health Expect. 2022;25(1):203–213. doi:10.1111/hex.13363
34. Denetclaw TH, Cefalu P, Manila LL, Panagotacos JJ. Needs analysis for educating community pharmacists to interface with prehospital stroke chain of survival. J Stroke Cerebrovasc Dis. 2014;23(2):209–212. doi:10.1016/j.jstrokecerebrovasdis.2012.11.017
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.