Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 10 » Issue 1
Time trends in coronary revascularization procedures among people with COPD: analysis of the Spanish national hospital discharge data (2001–2011)
Authors de Miguel-Díez J ![]() , Jiménez-García R
, Jiménez-García R ![]() , Hernández-Barrera V
, Hernández-Barrera V ![]() , Carrasco-Garrido P, Bueno H, Puente-Maestu L
, Carrasco-Garrido P, Bueno H, Puente-Maestu L ![]() , Jimenez-Trujillo I
, Jimenez-Trujillo I ![]() , Alvaro-Meca A
, Alvaro-Meca A ![]() , Esteban-Hernandez J
, Esteban-Hernandez J ![]() , de Andrés AL
, de Andrés AL
Received 18 July 2015
Accepted for publication 14 September 2015
Published 22 October 2015 Volume 2015:10(1) Pages 2285—2294
DOI https://doi.org/10.2147/COPD.S92614
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Javier de Miguel-Díez,1 Rodrigo Jiménez-García,2 Valentín Hernández-Barrera,2 Pilar Carrasco-Garrido,2 Héctor Bueno,3 Luis Puente-Maestu,1 Isabel Jimenez-Trujillo,2 Alejandro Alvaro-Meca,2 Jesús Esteban-Hernandez,2 Ana López de Andrés2
1Pneumology Department, Hospital General Universitario Gregorio Marañón, Universidad Complutense de Madrid, Madrid, Spain; 2Preventive Medicine and Public Health Teaching and Research Unit, Department of Health Sciences, Health Sciences Faculty, Rey Juan Carlos University, Alcorcón, Madrid, Spain; 3Centro Nacional de Investigaciones Cardiovasculares, Instituto de investigación i+12, Cardiology Department, Hospital Universitario 12 de Octubre, Universidad Complutense de Madrid, Madrid, Spain
Background: People with COPD suffering from coronary artery disease are frequently treated with revascularization procedures. We aim to compare trends in the use and outcomes of these procedures in COPD and non-COPD patients in Spain between 2001 and 2011.
Methods: We identified all patients who had undergone percutaneous coronary interventions (PCIs) and coronary artery bypass graft (CABG) surgeries, using national hospital discharge data. Discharges were grouped into: COPD and no COPD.
Results: From 2001 to 2011, 428,516 PCIs and 79,619 CABGs were performed. The sex and age-adjusted use of PCI increased by 21.27% per year from 2001 to 2004 and by 5.47% per year from 2004 to 2011 in patients with COPD. In-hospital mortality (IHM) among patients with COPD who underwent a PCI increased significantly from 2001 to 2011 (odds ratio 1.11; 95% confidence interval 1.03–1.20). Among patients with COPD who underwent a CABG, the sex and age-adjusted CABG incidence rate increased by 9.77% per year from 2001 to 2003, and then decreased by 3.15% through 2011. The probability of dying during hospitalization in patients who underwent a CABG did not change significantly in patients with and without COPD (odds ratio, 1.06; 95% confidence interval 0.96–1.17).
Conclusion: The annual percent change in PCI procedures increased in COPD and non-COPD patients. We found a decrease in the use of CABG procedures in both groups. IHM was higher in patients with COPD who underwent a PCI than in those without COPD. However, COPD did not increase the probability of dying during hospitalization in patients who underwent a CABG.
Keywords: COPD, percutaneous coronary intervention, coronary artery bypass graft surgery, hospitalization, length of stay, in-hospital mortality
Background
The association between COPD and coronary artery disease (CAD) is well known.1 In studies of the general population, it has been shown an increased all-cause mortality as well as cardiovascular mortality in patients with COPD.2,3 Patients with mild COPD seem to have even a higher risk of dying from cardiovascular causes than from respiratory insufficiency.4
COPD is highly prevalent among patients with CAD.5 The causal connection between both diseases has historically been cigarette smoking.6 However, a recent epidemiological study has shown that systemic inflammation plays a significant role in both atherogenesis and COPD.7
Other evidence that highlights the close relationship between COPD and CAD is the fact that this pulmonary disease is an independent factor of poor outcome and mortality after coronary revascularization procedures.8 The diagnosis of COPD was, together with other important clinical variables such as age, sex, and left ventricular ejection fraction, a predictor of mortality at 4 years of revascularization in the SYNTAX II score (index that punctuates the complexity of CAD by angiography and it helps to decide the optimal method of revascularization in patients with CAD complex).9 As a result, treatment of CAD in patients with COPD can present therapeutic challenges. Given that COPD is associated with higher risk of adverse events after coronary artery bypass graft (CABG) surgery,10,11 percutaneous coronary intervention (PCI) is now the most commonly used reperfusion procedure for COPD patients undergoing revascularization.6 In fact, patients with COPD currently make up almost 10% of patients undergoing PCI.12 Nonetheless, several studies have reported and elevated the risk of adverse outcomes among patients with COPD after PCI.5,12–14
Secular trends in the use of coronary revascularization procedures have been examined.15 Culler et al16 have identified, in a recent retrospective study, all Medicare beneficiaries undergoing a coronary revascularization procedure between 2008 and 2012. They have observed, on the one hand, that the total number of revascularization procedures peaked in 2010 and declined by >4% per year in 2011 and 2012, and second, that mortality rates remained between 2.1% and 2.2% annually during the study period. However, despite the poor prognosis of patients with COPD after PCI and CABG, no previous studies have evaluated the changes in utilization and outcomes of coronary revascularization procedures over time in these patients. It is possible that may be there have been advances in recent years, not only in surgical techniques, but also in monitoring and anesthesia, which they could have helped to improve results.17
In this study, we used national hospital discharge data to describe and compare trends in the use of coronary revascularization procedures in COPD and non-COPD patients between 2001 and 2011 in Spain. In particular, we analyzed trends in the use of CABG and PCI, patient comorbidities, and in-hospital outcomes such as length of stay (LOS) and in-hospital mortality (IHM).
Methods
A retrospective, descriptive, epidemiological study was conducted using the Spanish National Hospital Database (CMBD, Conjunto Minimo Básico de Datos), which compiles all public and private hospital data, hence covering more than 95% of hospital discharges.18 The CMBD database is managed by the Spanish Ministry of Health, Social Services and Equality and includes patient variables (sex and date of birth), date of admittance, date of discharge, up to 14 discharge diagnoses, and up to 20 procedures performed during hospitalization. The Spanish Ministry of Health, Social Services and Equality sets recording standards and performs periodic audits.18
We selected all surgical admissions of patients who underwent coronary revascularization procedures using the International Classification of Diseases – Ninth Revision, Clinical Modification (ICD-9-CM). The procedure codes used were 36.10–36.19 for CABG and 36.06, 36.07, 36.09, and 0.66 for PCI. Discharges were grouped by COPD status as follows: no COPD and COPD (ICD-9-CM codes: 490–492 and 495–496, respectively). Patients who underwent both CABG and PCI during their hospitalization were excluded.
The outcomes of interest included the percentage of patients who died during hospitalization, defined as IHM and the mean LOS.
Clinical characteristics included information on overall comorbidity at the time of surgery, which was assessed by computing the Charlson comorbidity index (CCI). The index applies to 17 disease categories whose scores are totaled to obtain an overall score for each patient.19 The 17 diseases included in the CCI are myocardial infarction, congestive heart failure, peripheral vascular disease, cerebrovascular disease, dementia, COPD, connective tissue disease, ulcer disease, diabetes, renal disease, hemiplegia, any tumor, leukemia, lymphoma, liver disease, metastatic solid tumor, and AIDS. The index is subsequently categorized into three levels: 0, no disease; 1, one or two diseases; and 2, three or more diseases.20 To calculate the CCI, we used 17 disease categories, excluding COPD and acute myocardial infarction, as described by Thomsen et al.20
Statistical analysis
A descriptive statistical analysis was performed. Rates for COPD and non-COPD patients for each coronary revascularization procedure were calculated in terms of 100,000 inhabitants. We also calculated the yearly age- and sex-specific incidence rates for COPD and non-COPD patients, dividing the number of cases per year, sex, and age group by the corresponding number of people in that population group, according to data from the Spanish National Institute of Statistics, as reported on December 31 of each year.21
In our study, we used joinpoint log-linear regression to identify the years in which changes in tendency occurred in the use of PCI and CABG in patients with and without COPD, as well as to estimate the annual percent change (APC) in each of the periods delimited by the points of change. The analysis started with the minimum number of joinpoints and tested whether the inclusion of one or more joinpoints was statistically significant.22 In the final model, each joinpoint indicated a significant change in the tendency, and the APC was obtained in each of the segments delimited by the joinpoints, using the weighted least squares technique. The Joinpoint Regression Program Version 4.0.4 was used for the analysis.23
In order to test the time trend for IHM, logistic regression analyses were performed with mortality as a binary outcome, using year of discharge, sex, age, and CCI as independent variables. Models were generated for COPD and non-COPD subjects and for the entire population, in order to compare the IHM of those who have the disease and those who do not. Statistical analyses were performed using Stata version 10.1 (StataCorp LP, College Station, TX, USA). Statistical significance was set at P<0.05 (two-tailed).
Ethical aspects
Data confidentiality was maintained at all times according to Spanish legislation. Patient identifiers were deleted before the database was provided to the authors, in order to maintain patient anonymity. It is not possible to identify patients at individual levels, either in this article or in the database. Given the anonymous and mandatory nature of the dataset, it was not necessary to obtain informed consent. The study protocol was approved by the ethics committee of the Rey Juan Carlos University.
Results
From 2001 to 2011, a total of 508,135 admissions of patients who underwent scheduled or unscheduled coronary revascularization procedures were recorded in Spain. Over the study period, 7.17% (n=36,478) of all patients who underwent coronary revascularization procedures had COPD. There were a total of 428,516 PCIs (6.91% [n=29,630] in patients with COPD) and 79,619 CABGs (8.6% [n=6,848] in patients with COPD).
Percutaneous coronary intervention
In patients who underwent a PCI, there was a significant male predominance in patients both with and without COPD (92.82% and 75.54%, respectively). Mean age was 69.78 years (standard deviation [SD], 9.55 years) in patients with COPD and 65.02 years (SD, 11.37 years) in those without COPD (P<0.01).
Patients with COPD who underwent PCIs had higher CCI values compared with those without COPD (56.79% vs 43.75% with one or more coexisting conditions, respectively).
Among those who received a PCI, the median LOS was significantly higher in patients with COPD (7.00 days [interquartile range (IQR) 8.00 days]) compared with those without COPD (6.00 days [IQR 7.00 days]). Also, IHM was significantly higher in patients with COPD (2.97%) compared with patients without COPD (2.12%).
According to the results of the joinpoint analysis, we found that the sex and age-adjusted use of PCI increased by 21.27% per year from 2001 to 2004 and by 5.47% per year from 2004 to 2011 in patients with COPD (Figure 1A). In patients without COPD, the use of PCI increased by 14.7% per year from 2001 to 2005. From 2005 to 2008, it increased by 5.21% per year, and from 2008 to 2011 it also increased by 0.48% per year, but not significantly in both cases (Figure 1B).
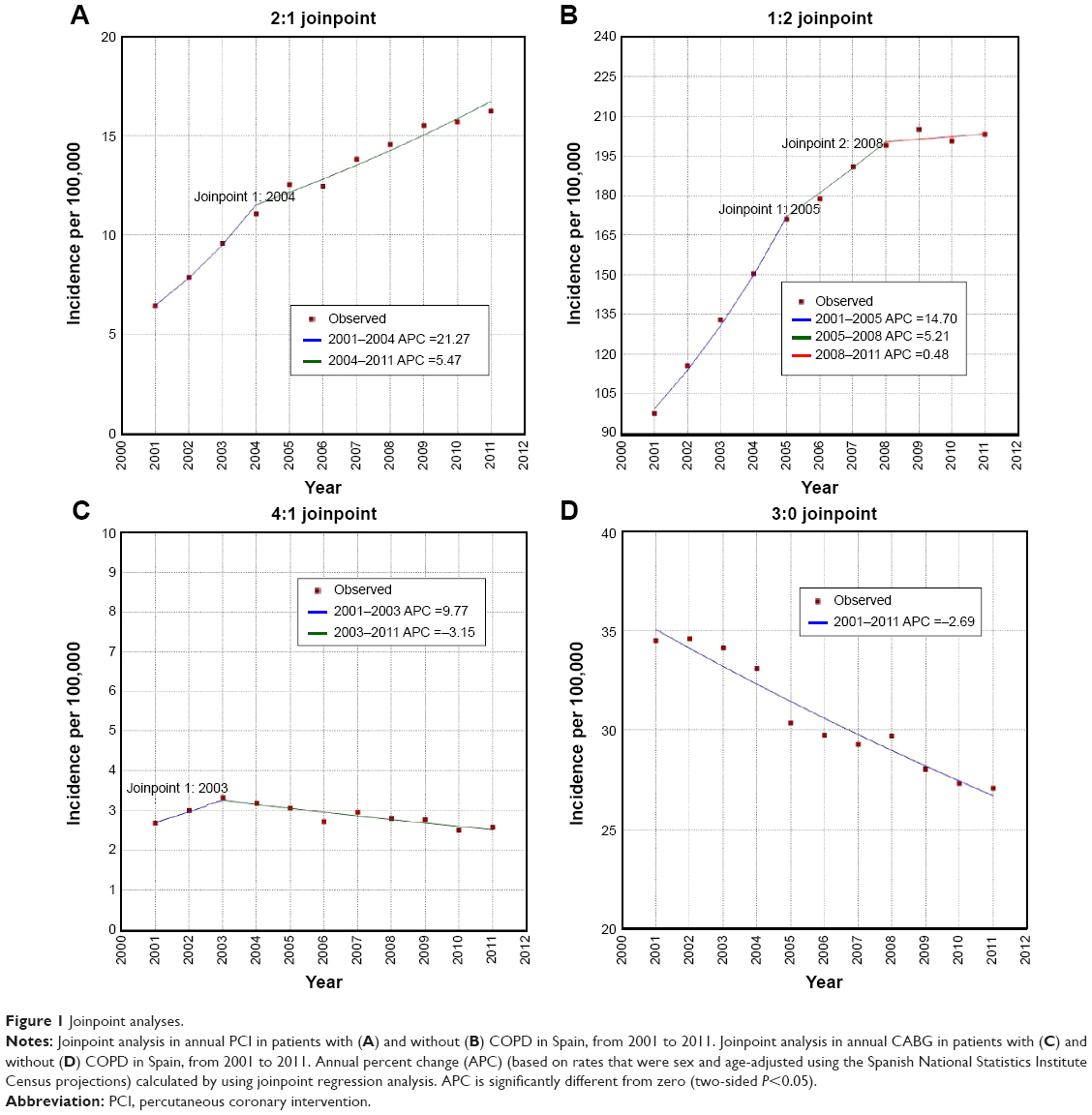 | Figure 1 Joinpoint analyses. |
Table 1 shows time trend outcomes in annual PCIs in patients with and without COPD in Spain, from 2001 to 2011. We found that the mean age of patients with COPD who underwent a PCI was 68.43±8.95 years in 2001 and increased to 70.61±19.85 years in 2011 (P<0.05). The proportion of men decreased significantly from 95.1% in 2001 to 92.05% in 2011. The prevalence of those with a CCI of one or more increased from 46.95% in 2001 to 62.10% (P<0.05).
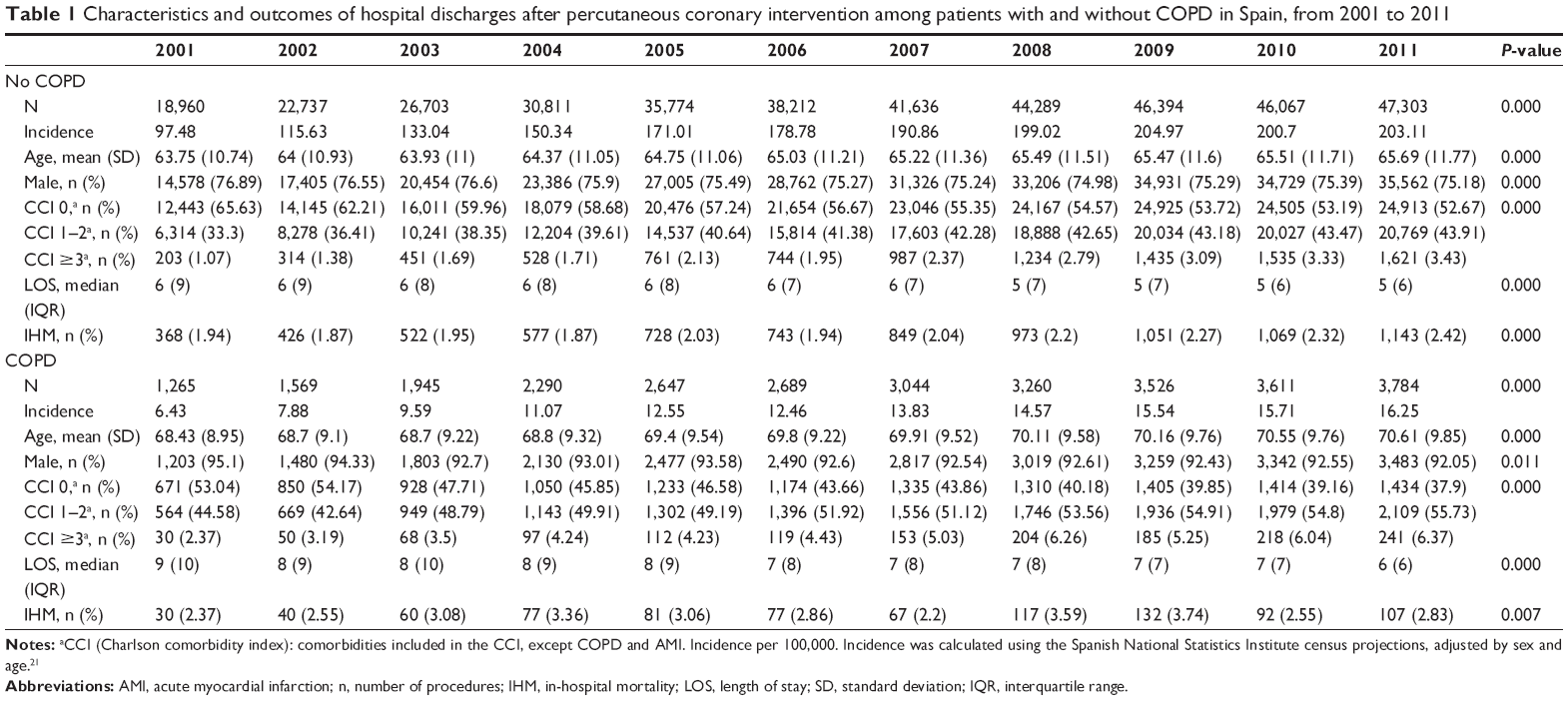 | Table 1 Characteristics and outcomes of hospital discharges after percutaneous coronary intervention among patients with and without COPD in Spain, from 2001 to 2011 |
LOS after PCI decreased significantly over the study period in both groups of patients (P<0.001), showing higher values among those with COPD in all years analyzed (Table 1).
The IHM among those who underwent a PCI increased for those without COPD (from 1.94% in 2001 to 2.42% in 2011, P<0.001). This parameter also increased in patients with COPD (from 2.37% in 2001 to 2.83% in 2011, P<0.01) (Table 1).
As can been seen in Table 2, after multivariate adjustment, the IHM among patients with COPD who underwent a PCI increased significantly from 2001 to 2011 (odds ratio [OR] 1.11; 95% confidence interval [CI] 1.03–1.20).
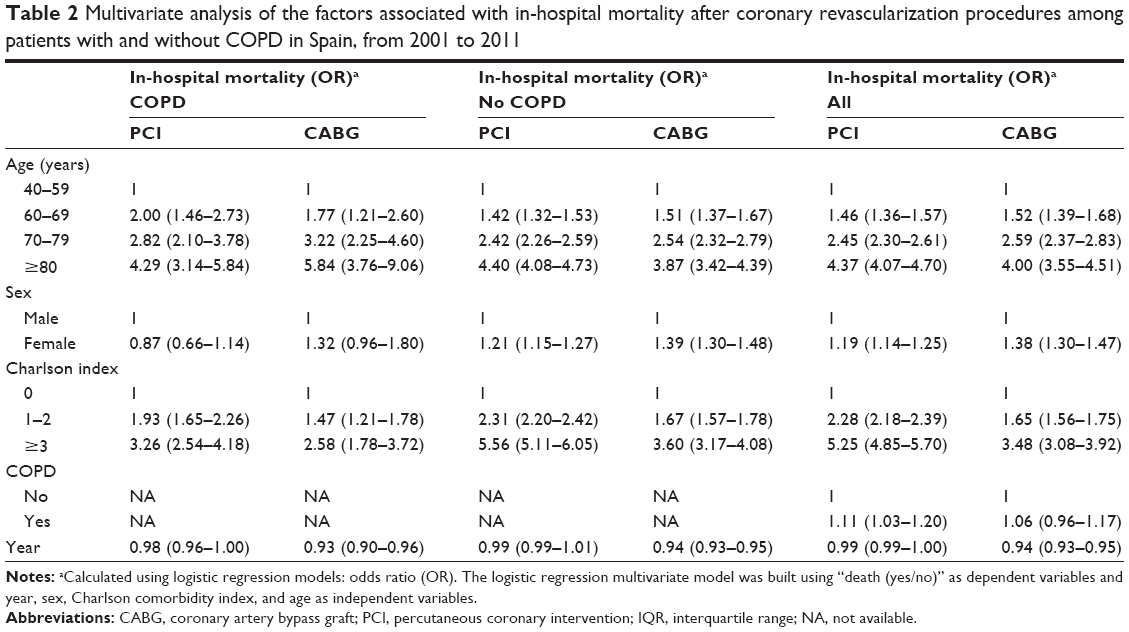 | Table 2 Multivariate analysis of the factors associated with in-hospital mortality after coronary revascularization procedures among patients with and without COPD in Spain, from 2001 to 2011 |
By contrast, the IHM did not change significantly according to sex. On the other hand, the IHM was significantly higher in those with one or two (OR 1.93; 95% CI 1.65–2.26) or three or more (OR 3.26; 95% CI 2.54–4.18) comorbidities associated with COPD.
Coronary artery bypass graft
We found that, in patients who underwent a CABG, the mean age was significantly higher in patients with COPD than in those without COPD (68.48 years [SD 8.42 years] vs 66.72 years [SD 9.55 years]) and there was higher proportion of males undergoing CABG procedures in both groups (93.17% in patients with COPD vs 76.49% in patients without COPD, P<0.05).
In our study, patients with COPD who underwent a CABG had higher CCI values than those without COPD (58.15% vs 51.84% with one or more comorbidities).
In patients with COPD, the IHM was significantly higher than in those without COPD (7.75% vs 7.17%); however, the median LOS was significantly higher in patients with COPD (17.00 days [IQR 17.00 days] compared with those without COPD (15.00 days [IQR 14.00 days]).
Among patients with COPD who underwent CABG, the sex and age-adjusted CABG incidence rate increased by 9.77% per year from 2001 to 2003, then decreased by 3.15% through 2011 (Figure 1C). In patients without COPD, the incidence rate decreased at a constant rate of 2.69% per year over the entire period of study (Figure 1D).
As can be seen in Table 3, over the 11-year study period, the mean age of patients with COPD who underwent CABG was 66.82±8.34 years in 2001 and 69.3±8.45 years in 2011. Significant differences in age were observed (P<0.001). The proportion of men was 94.24% in 2001 and 91.68% in 2011 (no significant differences).
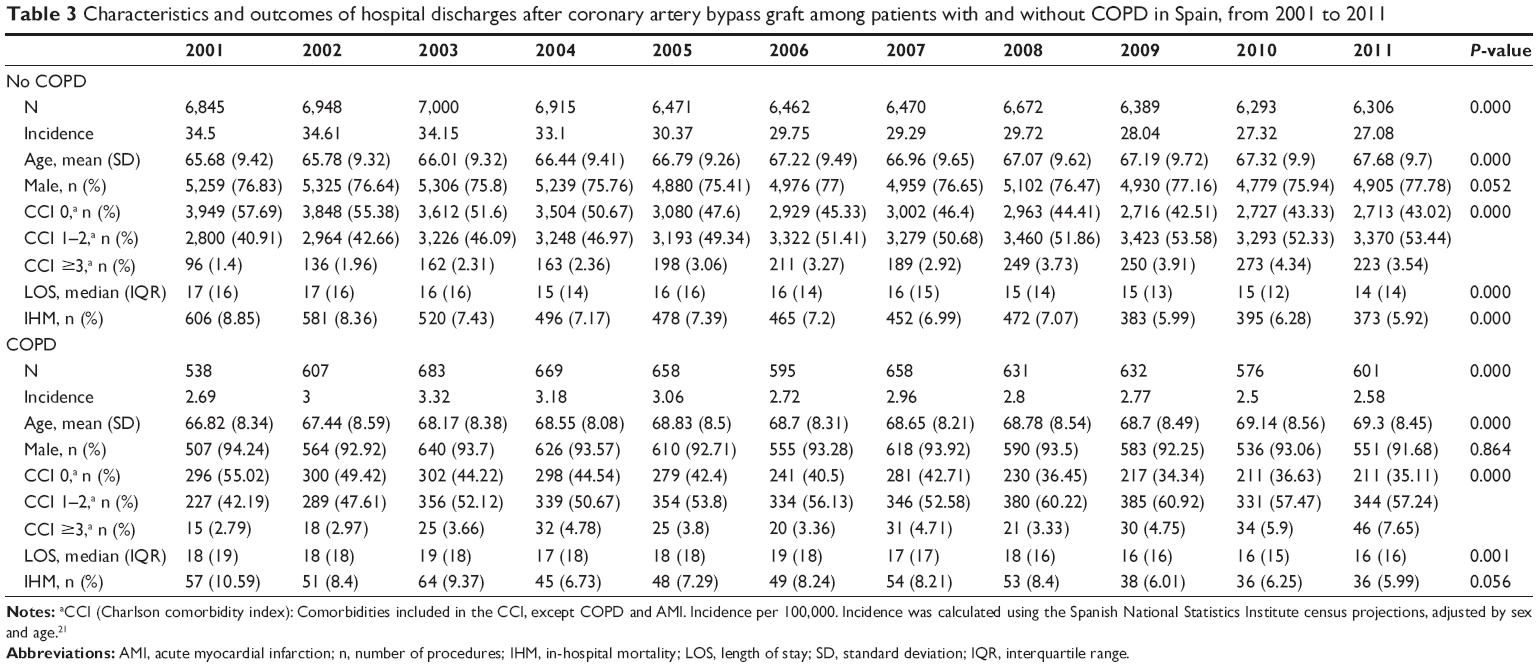 | Table 3 Characteristics and outcomes of hospital discharges after coronary artery bypass graft among patients with and without COPD in Spain, from 2001 to 2011 |
In our study, LOS in patients with COPD decreased significantly from 18 days (IQR, 19 days) in 2001 to 16 days (IQR, 16 days) in 2011 (P<0.01). In patients without COPD, LOS also decreased significantly over the period of study (Table 3).
The IHM decreased significantly for those with and without COPD during the 11-year study period (10.59% in 2001 vs 5.99% in 2011 and 8.85% vs 5.92%, respectively) (Table 3).
After multivariate adjustment, the IHM among patients with COPD who underwent a CABG decreased significantly over the entire study period (OR 0.93; 95% CI 0.90–0.96). On the other hand, it did not change significantly according to sex. Finally, the IHM was significantly higher in patients with COPD with one or two (OR 1.47; 95% CI 1.21–1.78) and with three or more (OR 2.58; 95% CI 1.78–3.72) comorbidities. The probability of dying during hospitalization in patients who underwent a CABG did not change significantly in patients with and without COPD (Table 2).
Discussion
In the present study, we found different trends over the last 11 years in the hospitalizations of subjects with and without COPD who underwent coronary revascularization procedures. Our results reveal that patients with COPD account for 7.17% of all revascularization procedures in Spain. We found an increase in PCI procedure rates from 2001 to 2011; and a decline in hospital admissions for CABG in patients with COPD from 2003 to 2011.
Although there are no previous studies that have assessed the trends in coronary revascularization procedure for COPD over time, our results are consistent with studies conducted in patients with other chronic diseases. So, for example, in patients with diabetes, it has been observed that PCI rates have increased significantly due to advances in stent device technology and adjunctive pharmacology. By contrast, CABG rates have declined due to the fact that this procedure is more invasive than PCI procedures.24,25
In Spain, as other countries, the indications for PCI have become wider over the last years; more hospitals have included units where PCI procedures are conducted; PCI have improved in effectiveness in the last years and have very low morbidity, mortality, and cost compared with CABG. These tendencies have been found in studies conducted elsewhere.26–28
We found that IHM increased significantly over time among COPD patients after PCI. In addition, the IHM was significantly higher in those with one or more comorbidities associated with COPD. Data on patients with COPD undergoing PCI are limited. Previous studies that focused on mortality in patients undergoing PCI suggested worse prognosis in patients with COPD.12,13 More recently, Konecny et al5 have shown that there is a clearly increased mortality rate with each additional level of COPD severity; namely, patients with mild or moderate COPD did better than those with severe COPD who, in turn, did better than those with very severe COPD. Patients without COPD had better survival than those with any level of COPD. In another study in which it was assessed the incidence of COPD in patients with acute ST-segment elevation myocardial infarction undergoing primary PCI and the impact of COPD on the prognostic outcome of this patient population, it was demonstrated that COPD was not an independent predictor of short-term and medium-term mortality.29 Although the inconsistent findings between this study and previous reports remain poorly explained, there are some reasons that may explain the discrepancy. First, the enrollment and exclusion criteria and the diagnosis of COPD may not be identical between the different studies. Second, primary PCI, which was not a criterion for study enrollment in the majority of the recent studies, was performed in all patients in the last study.29 In any case, there are no previous studies that have evaluated the evolution of mortality in these patients over time.
Incomplete revascularization is the frequent final outcome in patients with multivessel coronary disease who undergo PCI. However, the IHM among patients with COPD who underwent a CABG decreased significantly over the entire study period. It did not change significantly according to sex. On the other hand, the IHM was significantly higher in patients with COPD with comorbidities. Leavit et al30 also showed, to assess the long-term survival of patients with COPD undergoing CABG, that the presence of COPD and ≥1 other comorbidity significantly reduced the 10-year survival. In COPD patients with ≥1 other comorbidity, the 10-year survival was 30%, and the incidence rate of death was 9.4 deaths per 100 person years of follow-up.
The probability of dying during hospitalization in patients who underwent a CABG did not change significantly in patients with and without COPD in our study. There are conflicting reports on the impact of COPD on patient outcomes after CABG. Several studies have also demonstrated similar IHM in CABG patients with and without COPD.31–34 Manganas et al34 found no evidence of increased post-CABG mortality in patients with COPD, although these patients demonstrated an increased incidence of postoperative chest infections and atrial fibrillation, and required longer hospital stay. In a large retrospective analysis, Angouras et al35 did not find any difference IHM and major morbidities between patients with and without COPD, although those with COPD had a longer hospital stay and a higher long-term mortality rate. By contrast, other studies have reported an increased risk for long-term mortality and lower survival in COPD patients.30,36,37 So, Saleh et al38 found, in a large retrospective study, that the severity of COPD proved to be a prognostic marker in patients undergoing CABG. More advanced stages of COPD, rather than mild or moderate forms, were found to be significantly associated with early mortality following CABG. To improve the outcomes, it has been suggested that off-pump coronary artery bypass grafting may be more suitable for patients with pulmonary diseases with a lower mortality and morbidity risk as compared with conventional CABG. However, Almassi et al39 did not find benefit to use an off-pump coronary artery bypass approach rather than conventional CABG in COPD patients.
In our investigation, the median LOS for PCI decreased from 9 days in 2001 to 6 days in 2011, among COPD patients, and from 6 to 5 days among non-COPD patients. With regard to CABG, the median was 18 days in 2001 and 16 days in 2011 for those with COPD, with equivalent figures of 17 and 14 days for those without COPD. Postoperative respiratory complications can increase hospital LOS as well as mid-term mortality of CABG patients with severe left ventricular dysfunction.40 These, together with prolonged mechanical ventilation time, have been also identified as independent risk factors of postoperative acute renal failure requiring renal replacement therapy after cardiac surgery in patients with preoperatively normal renal functions, a complication that increases hospital LOS and IHM.41
In patients without COPD who had undergone either a PCI or a CABG, women had worse outcomes than men. However, we have not found differences by sex in patients with COPD. These results contrast with those obtained in other chronic diseases such as diabetes where it has been suggested that the worse effect of diabetes on outcomes in women might be related to the onset mechanism for cardiovascular disease, the success of the revascularization coronary procedure, and the higher burden of cardiovascular risk factors.42,43
We should recognize strength and limitations of the current study. The main strength lies in its large sample size, its 11-year follow-up period, and its standardized methodology maintained constant along the study period. Nevertheless, several limitations warrant consideration. First, a potential source of bias comes from the use of ICD-9-CM diagnosis codes for identifying patients hospitalized for COPD.44,45 It might generate underdiagnosis of COPD, because all patients receiving PCI or CABG did not perform pulmonary function tests. However, the ICD-9-CM codes have been previously used for epidemiological investigations and proved to be a valid method to identify patients suffering from this disease.46,47 In relation to CAD, we have not provided information of this diagnosis, such as ST-elevation myocardial infarction, non-ST-elevation acute coronary syndrome, or stable angina. By contrast, we have provided the entire CAD grouped to have enough statistical power. If we stratify CAD, we would lose power because some clinical categories would have a very small number of subjects. On the other hand, this study and its outcomes were limited to the variables coded which do not include relevant data such as the extent of the coronary disease, the severity of COPD, or the pharmacologic treatment. In addition, the endpoint of this study is limited to short-term mortality and we cannot provide information of long-term mortality. Another limitation of this database is its anonymity (no identifying items such as clinical history number), which makes it impossible to detect whether the same patient was admitted more than once during the same year. In addition, patients who moved from one hospital to another would appear twice.
Nevertheless the administrative database used in our study was introduced in Spain in 1982, is a mandatory register, and its coverage is estimated to be greater than 95%.18 Concerns have been raised about the accuracy of routinely collected datasets; however, these datasets are periodically audited. Consequently, the quality and validity of our dataset have been assessed and shown to be useful for health research.48 Another limitation of our study is the missing causal relationship between IHM and CABG/PCI as patients admitted for cancer and non-cardiovascular were also included, the mortality of whom may not have been affected by the CABG/PCI.
Conclusion
Our results show that the APC in PCI procedures increased over study period in COPD and non-COPD patients. The IHM among patients with COPD who underwent a PCI increased significantly. Other outcome such as LOS was worse among individuals with COPD than those without COPD for PCI although they improved over the entire study period for both groups. Higher comorbidity was associated with higher IHM in PCI procedures in both groups of patients. On the other hand, we found a decrease in the use of CABG procedures in patients with and without COPD. The IHM did not change according to the existence, or not, of COPD among patients who underwent a CABG. These findings emphasize the need for further improvement in the control of cardiovascular risk factors in people with COPD.
Acknowledgment
This study forms part of research funded by Grupo de Excelencia Investigadora URJC-Banco Santander number 30VCPIGI03: Investigación traslacional en el proceso de salud – enfermedad (ITPSE).
Author contributions
All authors contributed toward data analysis, drafting and critically revising the paper, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
Dr Bueno reports having received consulting/speaking fees from Abbott, AstraZeneca, Bayer, BMS-Pfizer, Daiichi Sankyo, Eli Lilly, Ferrer, Menarini, Novartis, Sanofi, Servier, and research grants from AstraZeneca. The other authors report no conflicts of interest in this work.
References
Friedman GD, Klatsky AL, Siegelaub AB. Lung function and risk of myocardial infarction and sudden cardiac death. N Engl J Med. 1976;294(20):1071–1075. | ||
Sidney S, Sorel M, Quesenberry CP Jr, DeLuise C, Lanes S, Eisner MD. COPD and incident cardiovascular disease hospitalizations and mortality: Kaiser Permanente Medical Care Program. Chest. 2005;128(4):2068–2075. | ||
Young RP, Hopkins R, Eaton TE. Forced expiratory volume in one second: not just a lung function test but a marker of premature death from all causes. Eur Respir J. 2007;30(4):616–622. | ||
Calverley PM, Anderson JA, Celli B, et al. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N Engl J Med. 2007;356(8):775–789. | ||
Konecny T, Somers K, Orban M, et al. Interactions between COPD and outcomes after percutaneous coronary intervention. Chest. 2010;138(3):621–627. | ||
Zhang XL, Chi YH, Wang le F, Wang HS, Lin XM. Systemic inflammation in patients with chronic obstructive pulmonary disease undergoing percutaneous coronary intervention. Respirology. 2014;19(5):723–729. | ||
Sin DD, Man SF. Why are patients with chronic obstructive pulmonary disease at increased risk of cardiovascular diseases? The potential role of systemic inflammation in chronic obstructive pulmonary disease. Circulation. 2003;107(11):1514–1519. | ||
Portillo K, Abad-Capa J, Ruiz-Manzano J. Enfermedad pulmonar obstructiva crónica y ventrículo izquierdo. Arch Bronconeumol. 2015;51(5):227–234. | ||
Farooq V, van Klaveren D, Steyerberg EW, et al. Anatomical and clinical characteristics to guide decision making between coronary artery bypass surgery and percutaneous coronary intervention for individual patients: development and validation of SYNTAX score II. Lancet. 2013;381(9867):639–650. | ||
Filsoufi F, Rahmanian PB, Castillo JG, Chikwe J, Kini AS, Adams DH. Results and predictors of early and late outcome of coronary artery bypass grafting in patients with severely depressed left ventricular function. Ann Thorac Surg. 2007;84(3):808–816. | ||
Samuels LE, Kaufman MS, Morris RJ, Promisloff R, Brockman SK. Coronary artery bypass grafting in patients with COPD. Chest. 1998;113(4):878–882. | ||
Selvaraj CL, Gurm HS, Gupta R, Ellis SG, Bhatt DL. Chronic obstructive pulmonary disease as a predictor of mortality in patients undergoing percutaneous coronary intervention. Am J Cardiol. 2005;96(6):756–759. | ||
Enriquez JR, Parikh SV, Selzer F, et al. Increased adverse events after percutaneous coronary intervention in patients with COPD: insights from the National Heart, Lung, and Blood Institute dynamic registry. Chest. 2011;140(3):604–610. | ||
Berger JS, Sanborn TA, Sherman W, Brown DL. Effect of chronic obstructive pulmonary disease on survival of patients with coronary heart disease having percutaneous coronary intervention. Am J Cardiol. 2004;94(5):649–651. | ||
Hsieh TH, Wang JD, Tsai LM. Improving in-hospital mortality in elderly patients after acute coronary syndrome–a nationwide analysis of 97,220 patients in Taiwan during 2004–2008. Int J Cardiol. 2012;155(1):149–154. | ||
Culler SD, Kugelmass AD, Brown PP, Reynolds MR, Simon AW. Trends in coronary revascularization procedures among Medicare beneficiaries between 2008 and 2012. Circulation. 2015;131(4):362–370. | ||
Baillot RG, Joanisse D, Stevens LM, Doyle DP, Dionne B, Lellouche F. Recent evolution in demographic and clinical characteristics and in-hospital morbidity in patients undergoing coronary surgery. Can J Surg. 2009;52(5):394–400. | ||
Conjunto Mínimo Básico de Datos, Hospitales del INSALUD; 2001. Madrid: Instituto Nacional de Gestión Sanitaria, Ministerio de Sanidad y Consumo. Available from: http://www.ingesa.msssi.gob.es/estadEstudios/documPublica/pdf/grds-2001.pdf. Accessed May 4, 2015. Spanish. | ||
Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. | ||
Thomsen RW, Nielsen JS, Ulrichsen SP, Pedersen L, Hansen AM, Nilsson T. The Danish Centre for Strategic Research in Type 2 Diabetes (DD2) study: collection of baseline data from the first 580 patients. Clin Epidemiol. 2012;4:43–48. | ||
Población residente por fecha, sexo y edad. [Population estimates by date, sex, and age]. 2015. Madrid: Instituto Nacional de Estadística. Available from: http://www.ine.es/jaxiT3/Tabla.htm?t=9663. Accessed October 12, 2015. Spanish. | ||
Kim HJ, Fay MP, Feuer EJ, Midthune DN. Permutation tests for joinpoint regression with applications to cancer rates. Stat Med. 2000;19(3):335–351. | ||
National Cancer Institute. Joinpoint Regression Program (Version 4.0.4). Bethesda, MD: Statistical Methodology and Applications Branch, Surveillance Research Program, National Cancer Institute; 2013. | ||
Vamos EP, Millett C, Parsons C, Aylin P, Majeed A, Bottle A. Nationwide study on trends in hospital admissions for major cardiovascular events and procedures among people with and without diabetes in England 2004–2009. Diabetes Care. 2012;35(2):265–272. | ||
Bottle A, Millet C, Khunti K, Majeed A. Trends in cardiovascular admissions and procedures for people with and without diabetes in England, 1996–2005. Diabetologia. 2009;52(1):74–80. | ||
Fokkema ML, James SK, Albertsson P, et al. Population trends in percutaneous coronary intervention: 20-year results from the SCAAR (Swedish Coronary Angiography and Angioplasty Registry). J Am Coll Cardiol. 2013;61(12):1222–1230. | ||
Park SJ, Ahn JM, Kim YH, et al. Temporal trends in revascularization strategy and outcomes in left main coronary artery stenosis: data from the ASAN Medical Center-Left MAIN Revascularization registry. Circ Cardiovasc Interv. 2015;8(3):e001846. | ||
De Luca L, Olivari Z, Farina A, et al. Temporal trends in the epidemiology, management, and outcome of patients with cardiogenic shock complicating acute coronary syndromes. Eur J Heart Fail. Epub 2015 Sep 4. doi:10.1002/ejhf.339. | ||
Sung PH, Chung SY, Sun CK, et al. Impact of chronic obstructive pulmonary disease on patient with acute myocardial infarction undergoing primary percutaneous coronary intervention. Biomed J. 2013;36(6):274–281. | ||
Leavitt BJ, Ross CS, Spence B, et al. Long-term survival of patients with chronic obstructive pulmonary disease undergoing coronary artery bypass surgery. Circulation. 2006;114(1 Suppl):I430–I434. | ||
Michalopoulos A, Geroulanos S, Papadimitriou L, et al. Mild or moderate chronic obstructive pulmonary disease risk in elective coronary artery bypass grafting surgery. World J Surg. 2001;25(12):1507–1511. | ||
Rosenthal GE, Vaughan Sarrazin M, Hannan EL. In-hospital mortality following coronary artery bypass graft surgery in Veterans Health Administration and private sector hospitals. Med Care. 2003;41(4):522–535. | ||
Prapas SN, Panagiotopoulos IA, Hamed Abdelsalam A, et al. Predictors of prolonged mechanical ventilation following aorta no-touch off-pump coronary artery bypass surgery. Eur J Cardiothorac Surg. 2007;32(3):488–492. | ||
Manganas H, Lacasse Y, Bourgeois S, Perron J, Dagenais F, Maltais F. Postoperative outcome after coronary artery bypass grafting in chronic obstructive pulmonary disease. Can Respir J. 2007;14(1):19–24. | ||
Angouras DC, Anagnostopoloulos CE, Ahamogeorgakis TP, et al. Postoperative and long-term outcome of patients with chronic obstructive pulmonary disease undergoing coronary artery bypass grafting. Ann Thorac Surg. 2010;89(4):1112–1118. | ||
Medalion B, Katz MG, Cohen AJ, Hauptman E, Sasson L, Schachner A. Long-term beneficial effect of coronary artery bypass grafting in patients with COPD. Chest. 2004;125(1):56–62. | ||
Canver CC, Nichols RD, Kroncke GM. Influence of age-specific lung function on survival after coronary bypass. Ann Thorac Surg. 1998;66(1):144–147. | ||
Saleh HZ, Mohan K, Shaw M, et al. Impact of chronic obstructive pulmonary disease severity on surgical outcomes in patients undergoing non-emergent coronary artery bypass grafting. Eur J Cardiothorac Surg. 2012;42(1):108–113. | ||
Almassi GH, Shroyer AL, Collins JF, et al. Chronic obstructive pulmonary disease impact upon outcomes: the veterans affairs randomized on/off bypass trial. Ann Thorac Surg. 2013;96(4):1302–1309. | ||
Shapira OM, Hunter CT, Anter E, et al. Coronary artery bypass grafting in patients with severe left ventricular dysfunction–early and mid-term outcomes. J Card Surg. 2006;21(3):225–232. | ||
Doddakula K, Al-Sarraf N, Gately K, et al. Predictors of acute renal failure requiring renal replacement therapy post cardiac surgery in patients with preoperatively normal renal function. Interact Cardiovasc Thorac Surg. 2007;6(3):314–318. | ||
Blöndal M, Ainla T, Marandi T, Baburin A, Eha J. Sex-specific outcomes of diabetic patients with acute myocardial infarction who have undergone percutaneous coronary intervention: a register linkage study. Cardiovasc Diabetol. 2012;11:96. | ||
Lopez de Andres A, Jimenez-García R, Hernandez-Barrera V, et al. National trends in utilization and outcomes of coronary revascularization procedures among people with and without type 2 diabetes in Spain (2001–2011). Cardiovasc Diabetol. 2014;13:3. | ||
De Miguel Díez J, Jiménez García R, Hernández Barrera V, et al. Trends in hospital admissions for acute exacerbation of COPD in Spain from 2006 to 2010. Respir Med. 2013;107(5):717–723. | ||
Tsai CL, Delclos GL, Camargo CA Jr. Emergency department case volume and patient outcomes in acute exacerbations of chronic obstructive pulmonary disease. Acad Emerg Med. 2012;19(6):656–663. | ||
Ginde AA, Tsai CL, Blanc PG, Camargo CA Jr. Positive predictive value of ICD-9-CM codes to detect acute exacerbation of COPD in the emergency department. Jt Comm J Qual Patient Saf. 2008;34(11):678–680. | ||
Stein BD, Bautista A, Schumock GT, et al. The validity of International Classification of Diseases, Ninth Revision, Clinical Modification diagnosis codes for identifying patients hospitalized for COPD exacerbations. Chest. 2012;141(1):87–93. | ||
Ferreira-González I, Cascant P, Pons JM, Mitjavila F, Salas T, Permanyer-Miralda G. Predicting in-hospital mortality with coronary bypass surgery using hospital discharge data: comparison with a prospective observational study. Rev Esp Cardiol. 2008;61(8):843–852. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.