Back to Journals » Advances in Medical Education and Practice » Volume 6
Time-motion studies of internal medicine residents' duty hours: a systematic review and meta-analysis
Authors Leafloor C, Lochnan H, Code C, Keely E, Rothwell D, Forster A, Huang A
Received 16 June 2015
Accepted for publication 7 August 2015
Published 17 November 2015 Volume 2015:6 Pages 621—629
DOI https://doi.org/10.2147/AMEP.S90568
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Video abstract presented by Cameron W Leafloor.
Views: 478
Cameron W Leafloor,1 Heather A Lochnan,2,3,6 Catherine Code,2,4 Erin J Keely,2,3,6 Deanna M Rothwell,5,6 Alan J Forster,2,4–6 Allen R Huang2,6,7
1Faculty of Medicine, 2Department of Medicine, 3Division of Endocrinology and Metabolism, 4Division of General Internal Medicine, 5Performance Measurement and Innovation, 6Ottawa Hospital Research Institute, 7Division of Geriatric Medicine, The Ottawa Hospital and University of Ottawa, Ottawa, ON, Canada
Background: Since the mid-1980s, medical residents' long duty hours have been under scrutiny as a factor affecting patient safety and the work environment for the residents. After several mandated changes in duty hours, it is important to understand how residents spend their time before proposing and implementing future changes. Time-motion methodology may provide reliable information on what residents do while on duty.
Purpose: The purpose of this study is to review all available literature pertaining to time-motion studies of internal medicine residents while on a medicine service and to understand how much of their time is apportioned to various categories of tasks, and also to determine the effects of the Accreditation Council for Graduate Medical Education (ACGME)-mandated duty hour changes on resident workflow in North America.
Methods: Electronic bibliographic databases were searched for articles in English between 1941 and April 2013 reporting time-motion studies of internal medicine residents rotating through a general medicine service.
Results: Eight articles were included. Residents spent 41.8% of time in patient care activities, 18.1% communicating, 13.8% in educational activities, 19.7% in personal/other, and 6.6% in transit. North American data showed the following changes after the implementation of the ACGME 2003 duty hours standard: patient care activities from 41.8% to 40.8%, communication activities from 19.0% to 22.3%, educational activities from 17.7% to 11.6%, and personal/other activities from 21.5% to 17.1%.
Conclusion: There was a paucity of time-motion data. There was great variability in the operational definitions of task categories reported in the studies. Implementation of the ACGME duty hour standards did not have a significant effect on the percentage of time spent in particular tasks. There are conflicting reports on how duty hour changes have affected patient safety. A low proportion of time spent in educational activities deserves further study and may point to a review of the educational models used.
Keywords: time-motion studies, residents’ duty hours, workflow, systematic review
Introduction
Changes to resident physician duty hours around the world have been marked by the following events: the untimely death of Libby Zion in a New York City hospital in 1984,1 the 2003 European Working Time Directive,2 the mandates as described by the Accreditation Council for Graduate Medical Education (ACGME) 2003 and 2011 regulations,3 and the Institute of Medicine 2008 report.4
The initial 2003 ACGME limit set a maximum 80-hour work week. A stricter enforcement of the ACGME regulations as well as no more than 16 continuous work hours for first-year residents was subsequently implemented in 2011.3 The effects and effectiveness of changes in duty hours on patient care and safety as well as resident education have been challenging to document.
Time-motion studies have been used by industry to understand how people do their work in order to determine areas of inefficiency and to improve workflow.5 The use of this study technique in health care settings is emerging. Understanding in detail exactly what a resident does while he/she is on duty provides vital information that can be used to design new models of health care delivery in academic health care centers. These studies help providers understand how much time is spent on resident education, time at the bedside, time spent doing administrative work, etc. Time-motion data collection is subject to less bias and can allow for residency training programs and hospital administrators to design a duty system which best optimizes patient care activities, patient safety, educational activities, and the quality of life of the residents themselves.
The primary objective of this study was to discover whether time-motion studies of internal medicine residents on inpatient general medicine units around the world showed consistency in time spent on a variety of tasks. A secondary objective was to see if there was any effect of the ACGME guidelines on the proportion of time spent on tasks in North American study sites. With changing duty hours restricting in-hospital work hours, we hypothesize that residents would be spending less time on education and personal tasks in order to finish their daily clinical duties. We also hypothesize that restricted duty hours will result in less time spent in direct care of patients.
In general, internists care for more hospitalized patients than most other specialties and serve as the backbone of inpatient clinical services. Understanding how time is spent and measuring change as future duty hour amendments and residency training program changes are implemented are needed to ensure that those changes result in the desired improvements. By understanding how residents have spent their time in past studies, we will be able to compare future time-motion analyses to determine if any significant changes are occurring to resident work life and to what effect.
Methods
This study followed the guidelines as described in the meta-analysis of observational studies in epidemiology.6 Searches were conducted on the electronic bibliographic databases of MEDLINE, PubMed, Cochrane library, and CINAHL for articles between the years of 1941 and April 2013. The search terms used are listed in Table 1.
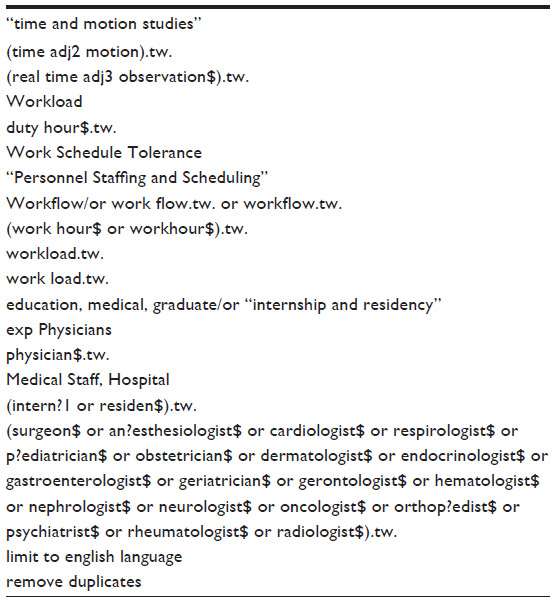 | Table 1 Search terms used for the electronic bibliographic database queries |
Records identified
The computer-generated list of records and references from potential articles were screened, and records were retained according to the inclusion and exclusion criteria described below. To limit bias and error, the remaining records were reviewed to assess their eligibility. The full-length articles of retained records were obtained and read through for their suitability for inclusion into the meta-analysis. A full institutional review for ethical issues was requested and deemed not required since this study represents an analysis of previously published data.
Inclusion and exclusion criteria
Only papers published in English, or previously translated to English, were considered. Any articles which included internal medicine residents as well as residents from other specialties were accepted as long as the data on the internal medicine residents could be extracted. Studies involving internal medicine residents in any year of their training were considered. Only direct observation time-motion studies were included. Self-surveys or other methods of time motion such as paging residents and asking them what they are doing at the present moment and how long it will take them to complete their current task were excluded. One study by Nerenz et al7 was excluded because its paper-based tracking method was thought to be unreliable. We tested a similar paper-based time-motion study using a spreadsheet to record tasks within 2.5-minute blocks, as described in the study, and found that the data gathered were inaccurate; additionally, the article did not show all of the time allotted to each task in its defined categories.
Data synthesis
In preparation for the design of a future time-motion study, a resident-led focus group helped to define and validate, a priori, nine categories of tasks residents performed when they were on duty. Three focus group iterations were done involving a total of 22 participants from the University of Ottawa Internal Medicine training program. These included eleven postgrad year (PGY)-1, seven PGY-2, and four PGY-3 residents, including two chief medical residents. The residents constructed from their experiences a prototypical “Day in the life of a Senior/Junior resident” upon which to frame the discussions. They reviewed and discussed an initial list of task categories extracted from the published literature. A final set of nine categories were defined: direct patient care, indirect patient care, communication, documentation, education, administrative, nonphysician tasks, personal, and transit. Consensus was reached using a modified Delphi technique. We initially tried to apply the nine categories of tasks in the meta-analysis; however, the heterogeneity of the studies and the differences in categories presented did not make this feasible. Data from the included studies were pooled into five categories that we felt could be extracted from the data presented. These categories are listed below.
Patient care activities
Patient care activities (collapsing direct and indirect patient care and documentation) were defined as activities which would alter the course of a patient’s stay in hospital or affect continuing posthospital care. These activities included direct communication with the patient, clinical computer work, clinical documentation, orders, procedures, and looking up test results.
Communication activities
Communication activities included verbal communications such as telephoning family members, paging and speaking to other physicians and health care workers, and sign-over rounds. Written communications were considered to be documentation and included with patient care activities.
Transit
Transit was defined to be any means of getting to and from the hospital, or traveling within the facility.
Education
Education was defined as any activity during which residents had the opportunity to learn and/or gather new information. Examples include bedside rounds, formal teaching sessions, clinical case reviews, attending seminars, literature searches, and reading.
Personal/other
Personal/other (collapsing personal, administrative, and nonphysician tasks) was defined as time spent on anything else during the observation period, including such activities as sleeping, eating, personal conversations, personal business, and performing nonphysician tasks such as bringing samples down to a lab.
All included articles were read for data pertaining to the study. Authors were contacted for missing data if possible.
Analysis
Data were pooled, and descriptive statistics generated. The secondary objective as to whether ACGME-mandated changes to duty hours had any effect on the proportion of time spent on different tasks was analyzed using a two tailed t-test. All analyses were done using R version 3.0.1 (http://www.r-project.org).
Results
Study characteristics
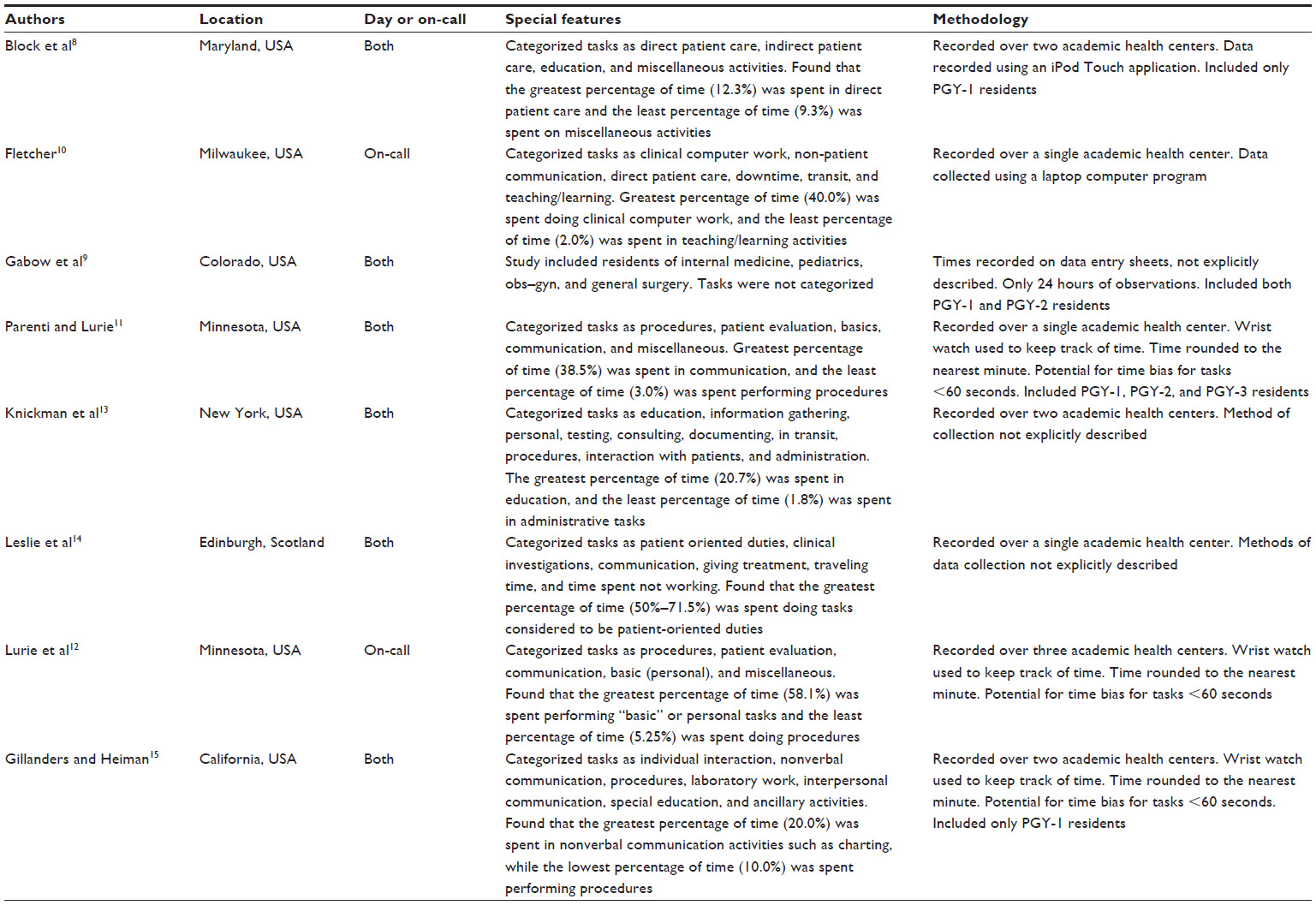
One hundred and eighty-seven records came from an initial search of electronic bibliographic databases. An additional 282 records were added from the reference lists of articles screened from the initial list and through a second search resulting in a total of 468 records. Four hundred and forty-seven records were excluded, and 21 full-text articles were assessed in detail. A final eight articles were included and are listed in Table 2.8–15 A row representing the publication of the ACGME 2003 regulations is included as a marker. The total number of residents followed in the included articles ranged from 29 to 35.12 The average of the reported total observation time was 387.6 hours. Two studies did not include their total observation time,11,12 for which the authors were contacted via email and either did not reply or no longer had the data. There were two studies which did not have information on education,11,12 and two studies did not have information about transit time.11,15 For those articles which did not report the total observation hours,11,12 the average percentage of time in all categories was summed and used as the total observation time in order to obtain appropriate time per task analysis needed for the meta-analysis. After the data from these studies were placed into the standardized categories, the percentage of time spent on each category was calculated. All studies took place in teaching hospitals. Figure 1 shows the data collection flow diagram, based on the Preferred Reporting Items for Systematic Reviews and Meta-analyses guidelines.16 Table 2 shows the summary data from the included studies. Table 3 lists the characteristics of the studies.
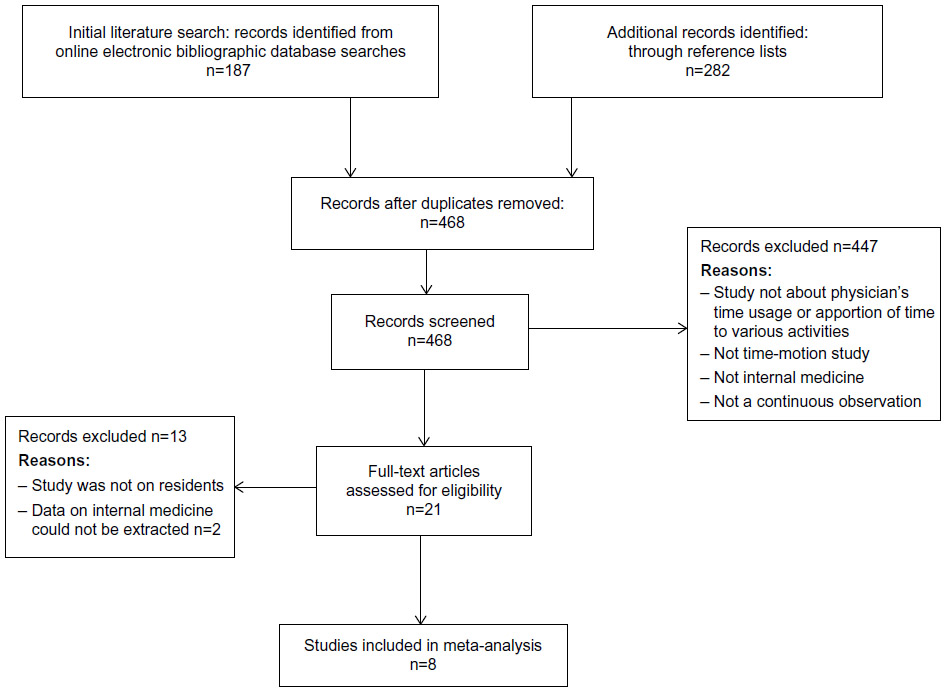 | Figure 1 The data collection flow diagram. |
 | Table 2 Published time-motion studies on/or including internal medicine residents |
 | Table 3 Characteristics of the included studies |
Data pooling
For the majority of the included papers, the authors presented the average time spent on tasks and the average time apportioned to a specific category. The average percentage of time spent per task was placed into one of the five standard categories, summed, and then using the total time of observations for that study, a new percentage of time and total hours of time spent on that category was calculated. Table 2 shows the data reported in chronologic order based on the publication dates of the papers. Table 4 shows the number of hours spent in each category of task, and Table 5 shows the data as a percentage of the total observation time.
 | Table 4 Total number of hours each study recorded per category |
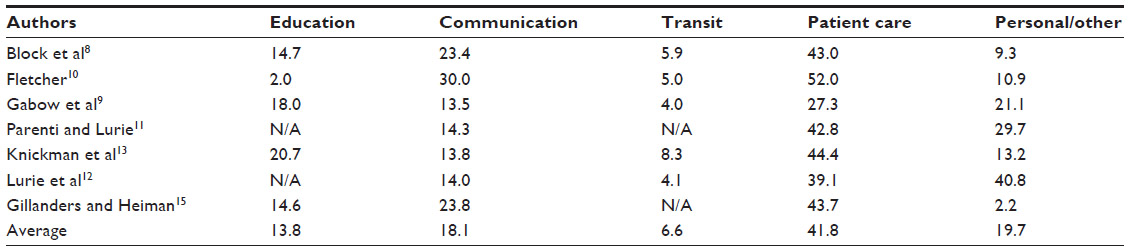 | Table 5 Percentage of time each study recorded per category |
Global analysis
Analysis of all eight articles, including the Leslie et al14 study conducted in the UK, showed that residents spent the most amount of time in patient care-related activities at 41.8% of their time. The remainder of their time was spent as follows: personal/other 19.7%, communication 18.1%, education 13.8%, and transit 6.6%. Since the ACGME regulations do not apply to the UK, the subsequent subanalyses included only the seven published studies from North America.
Subanalyses
Patient care activities
We were not able to separate patient care activities into direct/indirect categories from the included studies due to the heterogeneity of the data presented within each study. The largest portion of a resident’s shift work was spent in patient care activities with an average time spent of 41.8% (range: 27.3%–52.0%). The study by Gabow et al reported a significantly lower time (27.3%) allocated to patient care.9 This study only shadowed two residents, each for a single 24-hour period, during which the two residents slept for a significant portion (15% for the junior and 28% for the senior resident), and this most likely accounts for low patient care-related activities. There was a nonsignificant (P>0.05) decrease in the proportion of time spent in direct patient care after 2003, from an average of 42.5% before 2003 to 40.8% afterward.
Communication
Communication is essential between physicians, patients and their loved ones, and hospital staff. On average, residents spend 18.1% (range: 13.7%–30.0%) of their day in verbal communication. There was a nonsignificant (P>0.05) increase in the proportion of time spent communicating after 2003, from an average of 16.5% before 2003 to 22.3% afterward.
Education
Two studies11,12 which did not include data in this category were not represented in the analysis. The average amount of time spent in education across all the included studies was 13.8% (range: 2.0%–20.1%). There was a nonsignificant (P>0.05) decrease in the proportion of time spent in educational activities from 17.7% before 2003 to 11.6% afterward.
Transit
Two studies11,15 which did not include data in this category were not represented in the analysis. The average amount of time across all the included studies spent in transit for a resident was 6.6% (range: 4.2%–7.7%).
Personal/other activities
Although not statistically significant, there was a decrease in the percentage of time spent on personal or miscellaneous activities across the included studies from 21.5% prior to 2003 to 13.8% afterward. A resident on average spent approximately 3.3 hours of a 24-hour duty shift doing “nonwork-related activities”.
Discussion
The eight studies included in this systematic review and meta-analysis spanned the years 1971–2013 in a variety of locations. Overall, the pooled data showed a low percentage (13.8%) of total time spent in educational activities. The subgroup analysis with the studies done in North America, where the effects of the ACGME-mandated changes would be felt, showed no significant changes. This finding challenges our hypothesis that activities of education and of a personal nature would be the areas self-selected by residents to decrease in order to focus on patient care and communication activities to time-manage within the duty hour limitations. The results show that time-motion studies, when designed well, are a valid way of determining the task activities of internal medicine residents when they are on duty during an inpatient clinical service.
Patient care activities and communication activities
There was no change found (42.2%–40.8% of time) in patient care activities before and after 2003. There are no data to determine if residents are spending less time at the bedside, in order for them to complete the same volume of work in a shorter time period. However, total time attributed to patient care may have remained unchanged as the use of information technologies including mobile devices has proportionally increased. The included studies did not report the use of these technologies. The deployment and use of electronic health record systems may result in residents spending more time completing some tasks such as computerized provider order entry and other electronic documentation, which has consistently been shown to take longer to complete compared to using traditional pen and paper.17 The increased time using electronic systems would be added to patient care activities in this study.
As training programs and hospitals explore implementing resident float or shift scheduling, one would expect an increase in handover time. The proportion of time spent in communication increased from 16.5% to 22.3% post-2003 but was statistically nonsignificant. An unintended consequence of increased handovers as a result of meeting duty hour restrictions is an association shown by Denson et al18 to an increase in patient adverse events including mortality rates. Conversely however, two studies of general surgery19 inpatients and Medicare beneficiaries20 showed no overall increase in risk of mortality or morbidity post-2011 duty hour changes. Laine et al21 have also shown that decreased duty hours may slow clinical processes or impair the quality of care, but it is not associated with an increase in patient morbidity, adverse events, or hospital length of stay. This disagreement in the literature about the effects of duty hour restrictions on patient care deserves further research.
Educational activities
The low percentage of time attributable to participation in educational activities (17.6% before 2003; 11.6% afterward) is of concern. A survey by Jagsi et al22 showed that residents reported an increase in self-learning (research), a decrease in faculty teaching, and an overall decrease in the quality of their education after the 2003 duty hour changes. A similar study by Fitzgibbons et al23 reported that residents felt a decrease in the quality of their education with the 2011 change in duty hours. The educational model for internal medicine residents possibly needs to be reviewed.
Personal/other activities
Resident physicians’ lives are stressful, both outside and inside the hospital setting. The number of on-call shifts, lack of sleep, increasing work, and the emotional attachment to their patients all contribute to their perceived stress.24 Residents often report that they have no time for personal activities and frequently function with little sleep. The data showed a decreasing trend in time spent in personal activities from 21.5% to 13.8%, suggesting an erosion of downtime; however, no studies reported on resident lifestyle or exhaustion post-duty hour changes.
Limitations
The included papers were heterogeneous in method, subjects, and the type of tasks recorded, making it difficult to extract and pool the data. The time data from the included studies were extracted and analyzed in one of five standardized categories. Those studies with missing data or had unusual numbers would affect the calculation of time percentages. The small number of included time-motion studies makes statistical testing less valid.
Conclusion
This systematic review, the first of its kind, has shown that time-motion studies are a useful method by which to determine what internal medicine residents do while they were on duty. The number of studies using the time-motion methodology is sparse. There is a lack of standardization across the studies in the observation and tracking of time management. Duty hour restrictions mandated by the ACGME in 2003 and 2011 have resulted in minimal changes in resident workflow and the time apportioned to tasks as reported in North American studies. The published literature is divided on the association between changes in duty hours and patient care adverse events.
The consistently low percentage of time apportioned to educational activities on general medicine rotations in teaching hospitals may highlight the need to review the educational model for internal medicine residents.
A standardized set of task categories could be promoted at national or international organizations to help with future studies. Further research is required to clarify whether time-motion data can be used to develop and test new workflows for internal medicine residents in the academic teaching environment.
Acknowledgment
This research was supported by funds from the Department of Medicine, through a grant for innovation in medical teaching, and by the Ottawa Hospital.
Author contributions
All authors were involved in the concept and design of the study and the interpretation of the results. ARH, CWL, and AJF were involved in the acquisition and selection of the studies included in the analysis. CWL, DMR, and AJF were involved in the statistical analysis. CWL drafted the first version of the manuscript, and all authors contributed to the critical revision of the paper and agree to be accountable for all aspects of the work.
Disclosure
None of the authors have any financial or nonfinancial competing interests to declare.
References
Asch DA, Parker RM. The Libby Zion case. One step forward or two steps backward. N Engl J Med. 1988;318:771–775. | |
Directive 2003/88/EC of the European Parliament and of the Council of 4 November 2003 concerning certain aspects of the organisation of working time. Off J Eur Union. 2003:9–19. [OJ L 299. 18.11.2003]. Available from: http://eur-lex.europa.eu/legal-content/EN/TXT/?uri=celex:32003L0088. | |
The Accreditation Council for Graduate Medical Education Approved 2011 Standards. Available from: http://www.acgme.org/acgmeweb/Portals/0/PDFs/Common_Program_Requirements_07012011%5B2%5D.pdf. Accessed June 19, 2015. | |
Ulmer C, Wolman DM, Johns MME, editors. Resident Duty Hours: Enhancing Sleep, Supervision, and Safety. Insitute of Medicine Report. Washington, DC: The National Academies Press; 2009. | |
Brannick M, Levine E, Morgeson F. Job and Work Analysis. Methods Research and Applications for Human Resource Management. 2nd ed. Thousand Oaks, CA: Sage Publications; 2007. | |
Stroup DF, Berlin JA, Morton SC, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA. 2000;283:2008–2012. | |
Nerenz D, Rosman H, Newcomb C, et al. The on-call experience of interns in internal medicine. Medical Education Task Force of Henry Ford Hospital. Arch Intern Med. 1990;150(11):2294–2297. | |
Block L, Habicht R, Wu AW, et al. In the wake of the 2003 and 2011 duty hours regulations, how do internal medicine interns spend their time? J Gen Intern Med. 2013;28(4):495. | |
Gabow PA, Karkhanis A, Knight A, Dixon P, Eisert S, Albert RK. Observations of residents’ work activities for 24 consecutive hours: implications for workflow redesign. Acad Med. 2006;81(8):766–775. | |
Fletcher KE. The composition of intern work while on call. J Gen Intern Med. 2013;28(4):495. | |
Parenti C, Lurie N. Are things different in the light of day? A time study of internal medicine house staff days. Am J Med. 1993;94(6):654–658. | |
Lurie N, Rank B, Parenti C, Woolley T, Snoke W. How do house officers spend their nights? A time study of internal medicine house staff on call. N Engl J Med. 1989;320(25):1673–1677. | |
Knickman JR, Lipkin M Jr, Finkler SA, Thompson WG, Kiel J. The potential for using non-physicians to compensate for the reduced availability of residents. Acad Med. 1992;67(7):429–438. | |
Leslie PJ, Williams JA, McKenna C, Smith G, Heading RC. Hours, volume, and type of work of preregistration house officers. BMJ. 1990; 300(6731):1038–1041. | |
Gillanders W, Heiman M. Time study comparisons of 3 intern programs. J Med Educ. 1971;46(2):142–149. | |
Shamseer L, Moher D, Clarke M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ. 2015;349:g7647. | |
Asaro PV, Boxerman SB. Effects of computerized provider order entry and nursing documentation on workflow. Acad Emerg Med. 2008;15: 908–915. | |
Denson JL, McCarty M, Fang Y, Uppal A, Evans L. Increased mortality rates during resident handoff periods and the effect of ACGME duty hour regulations. Am J Med. 2015. [In press]. | |
Rajaram R, Chung JW, Jones AT, et al. Association of the 2011 ACGME resident duty hour reform with general surgery patient outcomes and with resident examination performance. JAMA. 2014;312:2374–2384. | |
Patel MS, Volpp KG, Small DS, et al. Association of the 2011 ACGME resident duty hour reforms with mortality and readmissions among hospitalized Medicare patients. JAMA. 2014;312:2364–2373. | |
Laine C, Goldman L, Soukup JR, Hayes JG. The impact of a regulation restricting medical house staff working hours on the quality of patient care. JAMA. 1993;269:374–378. | |
Jagsi RM, Shapiro JM, Weissman JSP, Dorer DJP, Weinstein DFM. The educational impact of ACGME limits on resident and fellow duty hours: a pre-post survey study. Acad Med. 2006;81: 1059–1068. | |
Fitzgibbons SC, Chen J, Jagsi R, Weinstein D. Long-term follow-up on the educational impact of ACGME duty hour limits: a pre-post survey study. Ann Surg. 2012;256(6):1108–1112. | |
Buddeberg-Fischer B, Klaghofer R, Stamm M, Siegrist J, Buddeberg C. Work stress and reduced health in young physicians: prospective evidence from Swiss residents. Int Arch Occup Environ Health. 2008;82: 31–38. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.