Back to Journals » Journal of Inflammation Research » Volume 18
Time-Dependent Mortality Predictors in Primary Sjögren’s Syndrome: C-Reactive Protein for Early Risk and Age for Late Outcomes
Authors Chen JQ, Zhang Y, Huang ZW, Yang JY ![]() , Liao JH, Lei CX, Zhang XY, Yu XB
, Liao JH, Lei CX, Zhang XY, Yu XB ![]() , Wu TH, Liu ZH
, Wu TH, Liu ZH ![]() , Tang BJ, Zhou XY, Deng TT, Luo J
, Tang BJ, Zhou XY, Deng TT, Luo J ![]() , Song WJ, Tao QW
, Song WJ, Tao QW
Received 10 March 2025
Accepted for publication 29 October 2025
Published 14 November 2025 Volume 2025:18 Pages 15925—15937
DOI https://doi.org/10.2147/JIR.S522156
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Jia-Qi Chen,1,2 Yan Zhang,1,2 Zi-Wei Huang,1,2 Jian-Ying Yang,3 Jia-He Liao,1,2 Chun-Xin Lei,1,2 Xi-Ya Zhang,1,2 Xin-Bo Yu,1,2 Tzu-Hua Wu,1,2 Zi-Han Liu,1,2 Bo-Jie Tang,1,2 Xuan-Yi Zhou,1,2 Tian-Tian Deng,1,2 Jing Luo,2,* Wei-Jiang Song,4 Qing-Wen Tao2,*
1Graduate School, Beijing University of Chinese Medicine, Beijing, People’s Republic of China; 2Traditional Chinese Medicine Department of Rheumatism, China-Japan Friendship Hospital, Beijing, People’s Republic of China; 3Graduate School, China Academy of Chinese Medical Sciences, Beijing, People’s Republic of China; 4Traditional Chinese Medicine Department, Peking University Third Hospital, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jing Luo, Traditional Chinese Medicine Department of Rheumatism, China-Japan Friendship Hospital, No. 2 Yinghua Dongjie, Chaoyang District, Beijing, 100029, People’s Republic of China, Email [email protected] Qing-Wen Tao, Traditional Chinese Medicine Department of Rheumatism, China-Japan Friendship Hospital, No. 2 Yinghua Dongjie, Chaoyang District, Beijing, 100029, People’s Republic of China, Email [email protected]
Purpose: To identify risk factors for near-term and long-term death in patients with primary Sjogren’s syndrome (pSS).
Patients and Methods: This ambispective cohort study included all patients with pSS treated at China–Japan Friendship Hospital between 2013 and 2023. The time-dependent Cox regression analysis was used for statistical analysis of risk factors, with 3 months and 60 months as the cut-off time points and all-cause death as the primary endpoint.
Results: Among the 1252 included patients, 138 patients had died by the end of follow-up (11.0%). Age at diagnosis, C-reactive protein (CRP) levels and total bilirubin (TBIL) were time-dependent risk factors for mortality. Within 3 months of follow-up, age > 65 years had no effect on mortality, but after 3 months of follow-up, the mortality risk in patients aged > 65 years increased over time (HR 3.97, 95% CI 2.57– 6.13; HR 16.63, 95% CI 5.53– 50.03). CRP > 6.5 mg/L increased the risk of mortality within 3 months (HR=11.45, 95% CI 2.52– 51.95), followed by 3– 60 months (HR=2.94, 95% CI 1.94– 4.45), but did not affect survival after 60 months of follow-up. TBIL > 18.01 μmol/L increased the risk of mortality in pSS patients within 3– 6 months (HR=2.30, 95% CI 1.42– 3.79) but did not increase the risk of mortality in patients with pSS within 3 months of follow-up or after 60 months.
Conclusion: pSS patients with a CRP level > 6.5 mg/L have an 11-fold increased risk of near-term death, whereas pSS patients older than 65 years of age at diagnosis have a 16-fold increased risk of long-term death.
Keywords: sjögren’s syndrome, mortality, risk factors, inflammation
Introduction
Primary Sjögren’s syndrome (pSS) is a chronic progressive autoimmune disease characterized by lymphocytic infiltration of the exocrine glands, commonly manifesting as dryness in the mouth and eyes.1 Because of long-term chronic dryness symptoms, pSS is usually described as a disease that significantly impacts quality of life.2–4 However, more than half of patients with pSS may develop systemic involvement, such as interstitial lung disease (ILD), which can be life-threatening.5 A new international, retrospective, large cohort study revealed that patients with pSS have an all-cause mortality rate that is 1.7–1.9 times higher than that of the general population,6 which is inconsistent with previous inherent knowledge suggesting that pSS affects survival time. Therefore, it is essential to clarify which subset of patients with pSS are at an elevated risk of mortality.
The risk factors for mortality in pSS patients are not yet fully understood. Although age, male sex, cryoglobulinemia, hypocomplementemia, systemic symptoms, pulmonary involvement, thrombocytopenia, liver damage, and the European League against Rheumatism Classification Criteria (EULAR) and the Sjögren’s syndrome Disease Activity Index (ESSDAI) are risk factors for death in patients with pSS,6–13 these factors are related primarily to assessments of disease activity or immune status associated with pSS. There is still a lack of research with regard to the impact of the baseline general condition at the initial visit for pSS on the risk of death several years later. Furthermore, while age is a widely recognized risk factor for mortality in pSS patients, there are almost no studies linking changes in risk factors over time to mortality in this patient population. Existing research typically confines potentially variable factors over time to constant risk assessments. The risk factors for near-term and long-term death in patients with pSS are unclear. To address these knowledge gaps, we utilized over ten years of baseline cohort data to evaluate the risk factors influencing mortality in patients with pSS, with a specific emphasis on analysing the characteristics of risk factors across different periods and summarizing the causes of death.
Patients and Methods
Study Design
We conducted an ambispective cohort study registered in the Clinical Trial (https://clinicaltrials.gov, clinicaltrials.gov, ID: NCT06528197). This study was conducted in accordance with the Declaration of Helsinki and was approved by the Clinical Research Ethics Committee of the China-Japan Friendship Hospital (2024-KY-173). For the retrospective cohort, the requirement for informed consent was waived as the research involved analysis of existing de-identified data. Participants in the prospective cohort provided written informed consent before undergoing study-specific procedures.
Study Population
We identified all patients with pSS who were admitted to China–Japan Friendship Hospital between January 1, 2013, and September 30, 2023. The patient inclusion criteria were as follows: fulfilled the 2002 American–European Consensus Group classification criteria (AECG) or the 2016 American College of Rheumatology (ACR)/EULAR classification criteria for pSS. The exclusion criteria were as follows: 1) refusal to undergo follow-up for the evaluation of death outcomes; 2) the presence of comorbid connective tissue disease at enrolment; or 3) the presence of other conditions (eg, cognitive impairment) that the investigators would consider indicative of ineligibility for enrolment. The primary endpoint was all-cause death or data censoring. The follow-up time ended on February 29, 2024.
Data Collection
The clinical information of the participants at their first visit to China–Japan Friendship Hospital was collected. The outcomes of the participants were followed up by telephone and further confirmed by reviewing the electronic medical records system. The baseline information of the patients was recorded by reviewing the electronic medical records. 1) General demographic data, including the age at which pSS was first diagnosed in our hospital, age of onset, duration of disease, and sex at birth, were collected. 2) Data on common clinical features included dry eyes/mouth, fatigue, and the Reynolds phenomenon, among other variables. ILD was detected via high-resolution computed tomography (HRCT), critically evaluated by two experienced thoracic radiologists, and finally diagnosed by clinicians. The following HRCT characteristics are particularly important: reticular abnormalities, ground‒glass opacities, nodules, consolidation, cysts, honeycombing and bronchiectasis.14 The disease activity of pSS patients was assessed via the ESSDAI.15 3) Laboratory features included leukopenia (<4×109/L), neutropenia (<1.5×10^9/L), lymphopenia (<0.8×10^9/L), erythropenia (3.8×10^9/L), anaemia (haemoglobin <100 g/L), thrombocytopenia (<100×10^9/L), hypokalaemia (<3.5 mmol/L), elevated alanine aminotransferase (ALT, >40 IU/L), elevated aspartate transaminase (AST, >42 IU/L), elevated total bilirubin (TBIL, >23 µmol/L), elevated gamma-glutamyltransferase (GGT, >52 µmol/L), and elevated blood urea nitrogen (BUN, >7.85 mmol/L). 4) Immunological characteristics included high levels of immunoglobulin G (IgG, >16.2 g/L), high levels of immunoglobulin A (IgA, >3.78 g/L), high levels of immunoglobulin M (IgM, >2.63 g/L), low levels of C3 (<0.700 g/L) and C4 (<0.160 g/L), elevated C-reactive protein (CRP, >8 mg/L) and elevated erythrocyte sedimentation rate (ESR, >20 mm/h). The autoantibodies included antinuclear antibodies (ANAs), anti-Sjögren’s syndrome antigen A (anti-SSA), anti-Ro52, anti-Sjögren’s syndrome antigen B (anti-SSB), anti-centromere protein B (anti-CENP-B), anti-ribonucleoprotein (anti-RNP), anti-DNA topoisomerase I (Scl-70), anti-mitochondrial M2 antibody (AMA-M2) and rheumatoid factor (RF). The ANA titre was measured by means of indirect immunofluorescence in HEp2 cells. Anti-SSA, anti-Ro52, anti-SSB, anti-CENP-B, anti-RNP, anti-Scl-70, and anti-AMA-M2 antibodies were used to detect relevant indicators by means of commercial enzyme-linked immunosorbent assay kits. The target antigen for detection of the anti-SSA antibody is Ro60. RF was detected via an immunoturbidimetric assay, and positivity was defined as a concentration greater than 20 IU/mL. All haematological indicators were evaluated at the China–Japan Friendship Hospital.
Statistical Analysis
The data were analysed via R software (version 4.4.1). Ninety percent of the data were missing (<5%), and <10% of all the data were missing. Multiple imputation was used for missing data, and the data before multiple imputation are shown in Supplementary Table 1. Descriptive data are reported as frequencies and percentages or medians with 25th and 75th percentiles, as appropriate. Data normality was detected by the Shapiro‒Wilk test. Comparisons were performed via the χ2 test or Mann‒Whitney U-test, as applicable. Kaplan‒Meier (KM) survival analysis was used to estimate survival time. Potential clinical factors were sequentially screened by univariate Cox proportional hazards (CPH) regression analysis, least absolute shrinkage and selection operator (LASSO) regression analysis, and stepwise regression analysis for factors ultimately included in multivariate CPH analysis. Univariate CPH regression analysis was performed for all potential clinical factors. Clinical factors with P<0.1 in univariate CPH analysis were screened, and these clinical factors were included in LASSO regression analysis for further screening. The number of collapses for LASSO regression analyses was 10, the optimal λ value was selected by cross-validation, and the clinical factors at the optimal λ value were screened (Supplementary Figure 1). Finally, the factors screened by LASSO regression were screened via the stepwise method to determine the final variables that were ultimately included in the multivariate CPH analysis. KM survival analysis was also used to plot survival curves for the finalized risk factors, with haemoglobin, GGT, BUN, CRP and TBIL split into binary variables for plotting survival curves after the optimal clinical inflection point was found via maximally selected rank statistics. The Log rank test was used for comparisons of specific risk factors. The proportional hazard (PH) assumption of the multivariate CPH analysis was tested via Schoenfeld residuals. The multivariate CPH model in this study did not meet the PH assumption and was instead analysed via the time-dependent Cox regression model, with 3 months and 60 months as the cut-off points. The hazard ratios (HRs) and their 95% confidence intervals (CIs) obtained in the time-dependent Cox regression analysis were calculated. A two-sided p value < 0.05 was considered significant.
Results
Baseline Characteristics
A total of 1371 patients with pSS were enrolled, and 119 patients without follow-up data were excluded. Overall, 1252 patients were ultimately enrolled in the study (Supplementary Figure 2). The baseline characteristics are shown in Table 1. Among the 1,252 patients with pSS included, the mean age of the patients with pSS at diagnosis was 58.00 [49.00, 67.00] years, with a marked female predominance (87.1%). The median duration from disease onset was 3 years, ranging from 0 to 44 years. The mean follow-up time was 4 years, ranging from 0 to 11.1 years. At 3 months, 2 years, 3 years, 5 years, and 10 years, the survival rates of the pSS patients were 98.9%, 94.0%, 91.9%, 87.6%, and 80.7%, respectively. By the end of the follow-up, 138 patients had died, and 1114 patients were alive. The overall survival curve is shown in Supplementary Figure 3.
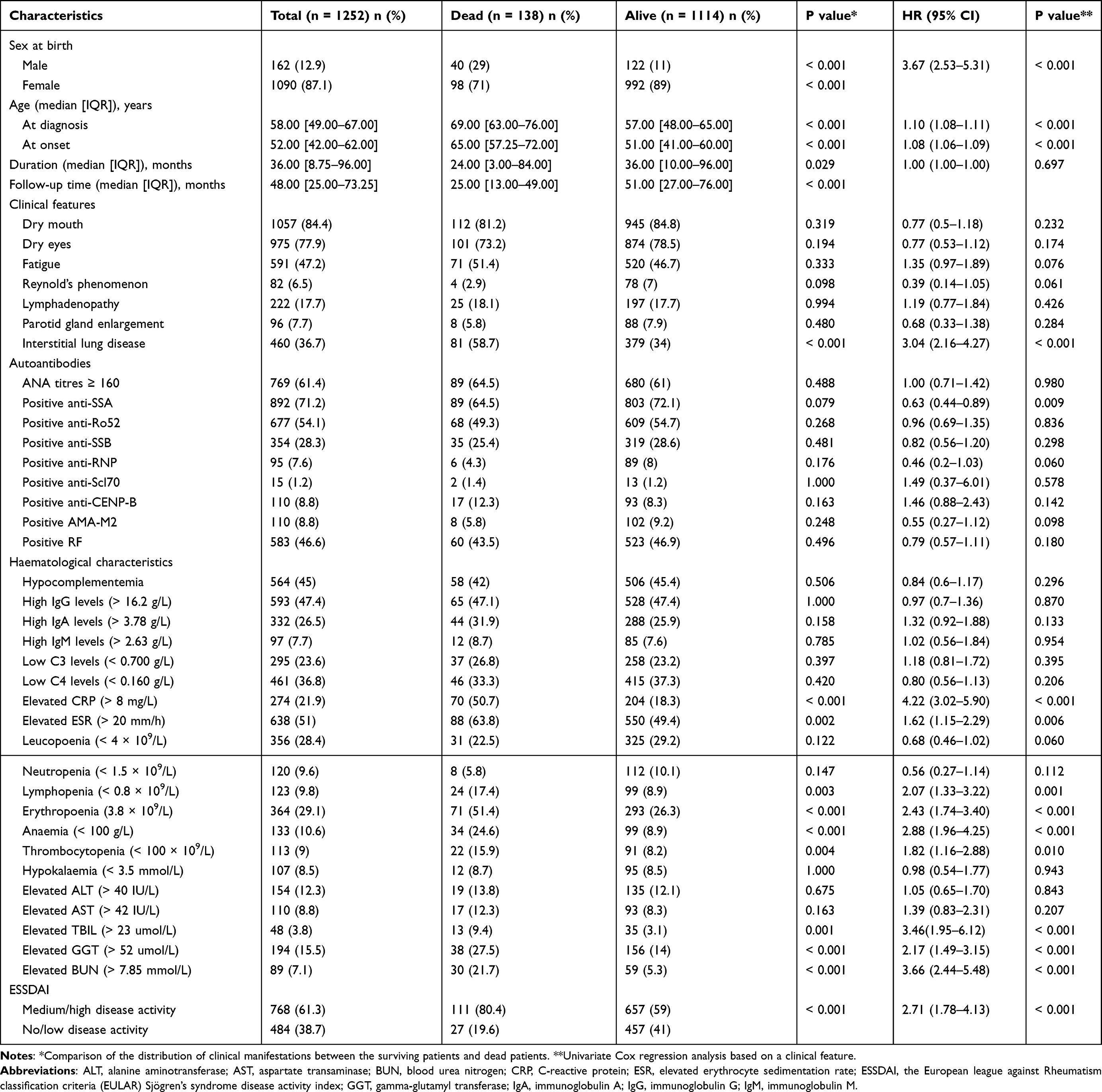 |
Table 1 Demographic and Clinical Characteristics of the Participants and the Associations Between These Characteristics and Death |
The mortality rate of males (29.0%) was significantly higher than that of females (11.0%) (p < 0.001) during the follow-up period. Compared to the pSS patients who survived, the patients who died were older at diagnosis (69.00 [63.00, 76.00] vs 57.00 [48.00, 65.00] years, p < 0.001), had a later age of onset of pSS (65.00 [57.25, 72.00] vs 51.00 [41.00, 60.00] years, p < 0.001), had a higher prevalence of ILD (58.7% vs 34.0%, p < 0.001), and had a shorter disease duration (24.00 [3.00, 84.00] vs 36.00 [10.00, 96.00], p<0.001) and a shorter follow-up time (25.00 [13.00, 49.00] vs 51.00 [27.00, 76.00] months,p < 0.001). Compared to those who survived, pSS patients who died, who died were more likely to have lymphopenia (17.4% vs 8.9%, p=0.003), erythropenia (51.4% vs 26.4%, p<0.001), anaemia (24.6% vs 8.9%, p<0.001), and thrombocytopaenia (15.9% vs 8.2%, p=0.004). The findings were similar for elevated CRP (50.7% vs 18.3%, p<0.001), elevated ESR (63.8% vs 49.4%, p<0.001), elevated TBIL (9.4% vs 3.1%, p=0.001), elevated GGT (27.5% vs 14.4%, p<0.001), and elevated BUN (21.7% vs 5.3%, p<0.001). Furthermore, compared to those who survived, the patients who died in this study had a higher prevalence of medium/high disease activity (80.4% vs 59%, p < 0.001) according to the ESSDAI.
Univariate CPH Analysis of Risk Factors for Mortality in Patients with pSS
As shown in Table 1, the male pSS patients had a higher risk of mortality than die the female patients (HR 3.67, 95% CI 2.53–5.31; p <0.001). pSS patients with an increased age at diagnosis (HR 1.10, 95% CI 1.08–1.11, p <0.001) and increased age at onset (HR 1.08, 95% CI 1.06–1.09, p <0.001) were more likely to die. The mortality risk was higher among pSS patients with ILD (HR 3.04, 95% CI 2.16–4.27, p <0.001), positive SSA (HR 0.63, 95% CI 0.44–0.89, p =0.009), elevated CRP (HR 4.22, 95% CI 3.02–5.90, p <0.001), elevated ESR (HR 1.62, 95% CI 1.15–2.29, p =0.006), lymphopenia (HR 2.07, 95% CI 1.33–3.22, p =0.001), erythropenia (HR 2.43, 95% CI 1.74–3.40, p <0.001), anaemia (HR 2.88, 95% CI 1.96–4.25, p <0.001), thrombocytopenia (HR 1.82, 95% CI 1.16–2.88, p =0.010), elevated TBIL (HR 3.46, 95% CI 1.95–6.12, p <0.001), and elevated GGT (HR 2.17, 95% CI 1.49–3.15, p <0.001), elevated BUN (HR 3.66, 95% CI 2.44–4.13, p <0.001), and ESSDAI ≥5 (HR 2.71, 95% CI 1.78–4.13, p <0.001).
Time-dependent Cox regression analysis of mortality risk in patients with pSS
As shown in Table 2, sex (HR 2.71, 95% CI 1.81–4.06, p <0.001), ESSDAI ≥5 (HR 1.57, 95% CI 1.00–2.48, p =0.049), ILD (HR 1.59, 95% CI 1.10–2.30, p =0.015), anaemia (HR 1.66, 95% CI 1.05–2.61, p =0.030), and elevated GGT (HR 1.57, 95% CI 1.06–2.34, p =0.026) were independent risk factors for mortality in patients with pSS, with relatively constant HRs. Age at diagnosis, elevated CRP, and elevated TBIL were time-dependent risk factors for mortality in patients with pSS (within 3 months versus 3 to 60 months versus after 60 months). Elevated CRP and TBIL levels increased the risk of mortality in pSS patients within 3 months and 3–60 months of follow-up (CRP: HR 14.52, 95% CI 3.21–65.58, p <0.001; HR 2.52, 95% CI 1.67–3.80, p <0.001; TBIL: HR 5.96, 95% CI 1.63–21.77, p=0.007; HR 3.42, 95% CI 1.66–7.06, p<0.001) but did not affect survival after 60 months of follow-up (CRP: HR 0.49, 95% CI 0.14–1.70, p =0.260; TBIL: HR 1.10, 95% CI 0.14–8.66, p=0.931). Over time, the HRs of elevated CRP and elevated TBIL decreased gradually (CRP: HR 14.52 to 2.52 to 0.49; TBIL: HR 5.96 to 3.42 to 1.10). Within 3 months of follow-up, age at diagnosis had no effect on survival (HR 1.01, 95% CI 0.97–1.05, p > 0.05), but after 3 months of follow-up, the mortality risk with respect to age in pSS patients increased over time (HR 1.08, 95% CI 1.06–1.10, p<0.001; HR 1.13, 95% CI 1.08–1.19, p<0.001).
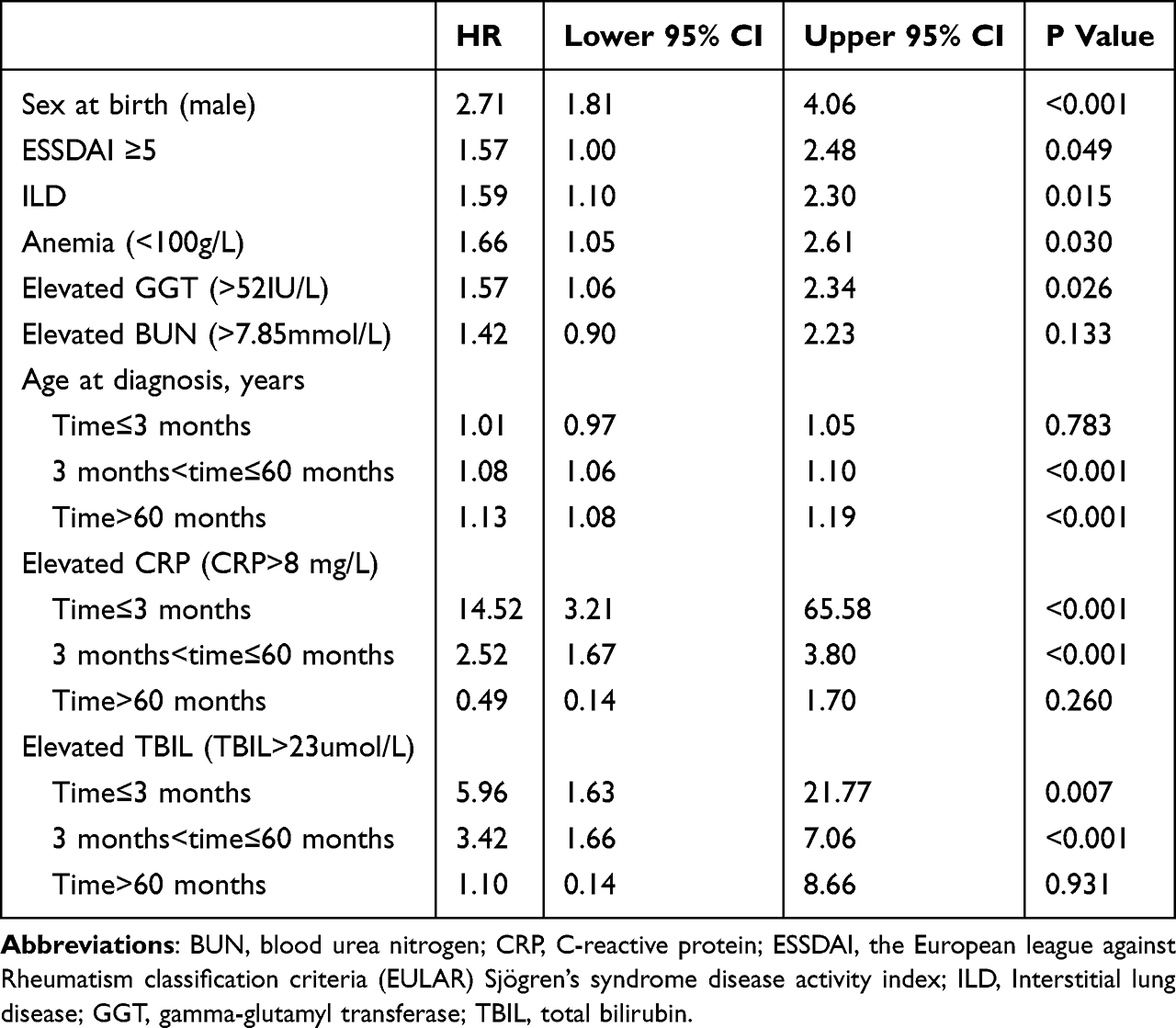 |
Table 2 Time-Dependent Multivariate Analysis for Death in Patients with Primary Sjogren’s Syndrome |
Survival Curve of Risk Factors for Death in Patients with pSS
On the basis of the results of the time-dependent Cox regression analysis, we calculated the clinical inflection points for age at diagnosis, haemoglobin, GGT, BUN, CRP and TBIL and found that 65 years, 102 g/L, 22 IU/L, 7.09 mmol/L, 6.5 mg/L and 18.01 µmol/L were the clinical inflection points for age at diagnosis, haemoglobin, GGT, BUN, CRP and TBIL, respectively. When the new clinical inflection point was used as the basis for classification, the survival curve results revealed that pSS patients aged >65 years, haemoglobin < 102 g/L, GGT > 22 IU/L, or BUN > 7.09 mmol/L had significantly lower survival rates (log rank test <0.001; Figure 1A and D–F). pSS patients aged >65 years at diagnosis had lower survival rates than did patients aged ≤ 65 years (log rank test <0.001, Figure 1G), and this difference appeared to increase after 60 months (70.8% to 93.8% vs 64.9% to 96.4%). pSS patients with CRP >6.5 mg/L had significantly lower survival at 60 months than patients with CRP ≤6.5 mg/L (log rank test <0.001, Figure 1H). However, CRP had no effect on the survival rate of pSS patients after 60 months (log rank test =0.548; Figure 1H). Similar results were observed for TBIL (within 60 months: log rank test <0.001; after 60 months: log rank test =0.702; Figure 1I). In addition, the survival curve results revealed that male patients had decreased survival due to all-cause death compared with female patients (log rank test <0.001, Figure 1A), as did those with ESSDAI scores ≥5 (log rank test <0.001, Figure 1B) and those with ILD (log rank test <0.001, Figure 1C).
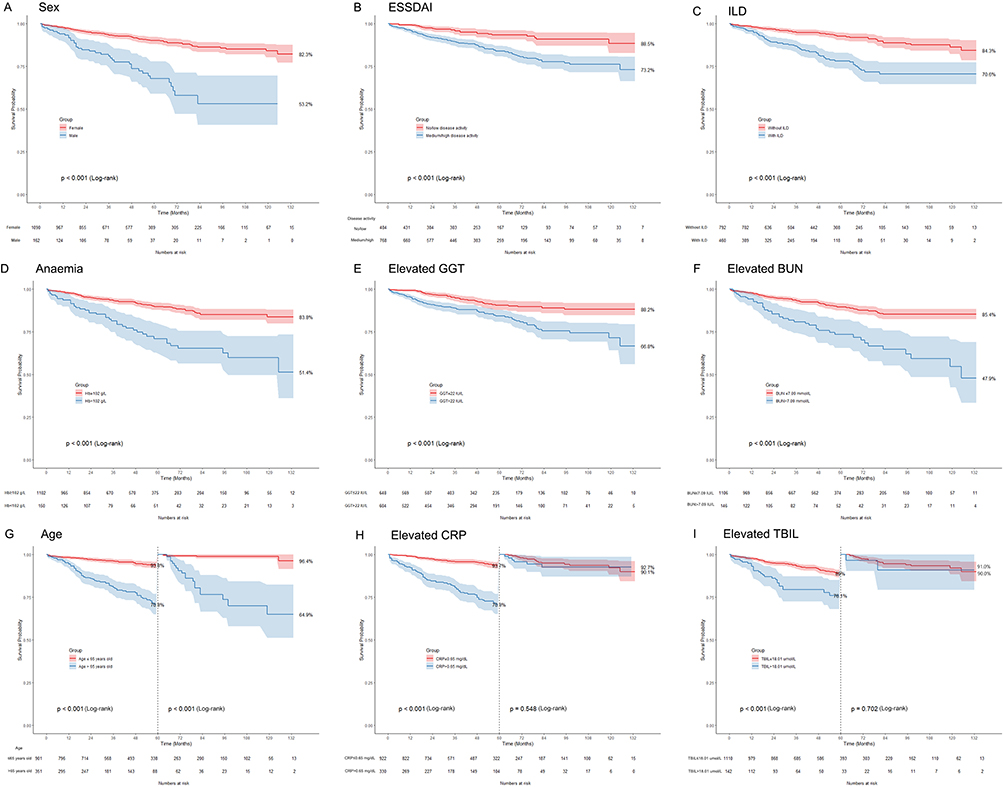 |
Figure 1 Kaplan‒Meier survival plots for the risk of death in patient subgroups. (A) Sex at birth. (B) ESSDAI: Medium/high disease activity (ESSDAI≥5) and no/low disease activity (ESSDAI<5). (C) Interstitial lung disease. (D) Anaemia (Hb<100 g/L). (E) Elevated GGT (>22 µmol/L). (F) Elevated BUN (>7.09 mmol/L). (G) Age at baseline. The data are divided into two segments according to time. (H) Elevated CRP (>6.5 mg/L). Split into two time segments at the cut-off point of 60 months: (I) Elevated TBIL (>18.01 µmol/L). Split into two time segments at the cut-off point of 60 months. |
Sensitivity Analysis
Time-dependent Cox regression analysis was performed again on the basis of new clinical inflection points of age, haemoglobin, TBIL, GGT, BUN and CRP (Table 3). For the three time-dependent variables of age, CRP level and TBIL, we split the data according to the cut-off points of 3 months and 60 months. Within 3 months of follow-up, age > 65 years at diagnosis had no effect on pSS patient survival (HR=0.95, 95% CI 0.32–2.77, p = 0.919), but after 3 months of follow-up, the mortality risk of> 65 years of age at diagnose increased over time (HR 3.97, 95% CI 2.57–6.13, p<0.001; HR 16.63, 95% CI 5.53–50.03, p<0.001). In particular, pSS patients aged > 65 years at diagnosis had a sharply increased risk ratio of all-cause death after 60 months of follow-up (HR=16.63, 95% CI 5.53–50.03; p<0.001). CRP >6.5 mg/L increased the risk of mortality in pSS patients within 3 months (HR=11.45, 95% CI 2.52–51.95, p=0.002), followed by 3–60 months (HR=2.94, 95% CI 1.94–4.45, p<0.001), but did not affect survival after 60 months of follow-up (HR=1.37, 95% CI 0.52–3.63, p=0.526). Over time, the HR of CRP >6.5 mg/L decreased gradually (CRP, HR: 11.45 to 2.94 to 1.39). TBIL >18.01 µmol/L increased the risk of mortality in pSS patients within 3–6 months (HR=2.30, 95% CI 1.42–3.79, p=0.0021) but did not increase the risk of mortality in patients with pSS within 3 months of follow-up (HR=2.21, 95% CI 0.69–7.08, p=0.183) or after 60 months (HR=0.88, 95% CI 0.20–3.27, p=0.862). Other results were similar to those of the first time-dependent Cox regression analysis. In addition, we performed additional analyses for ESR, CRP, and TBIL, as detailed in Supplementary Tables 2–4.
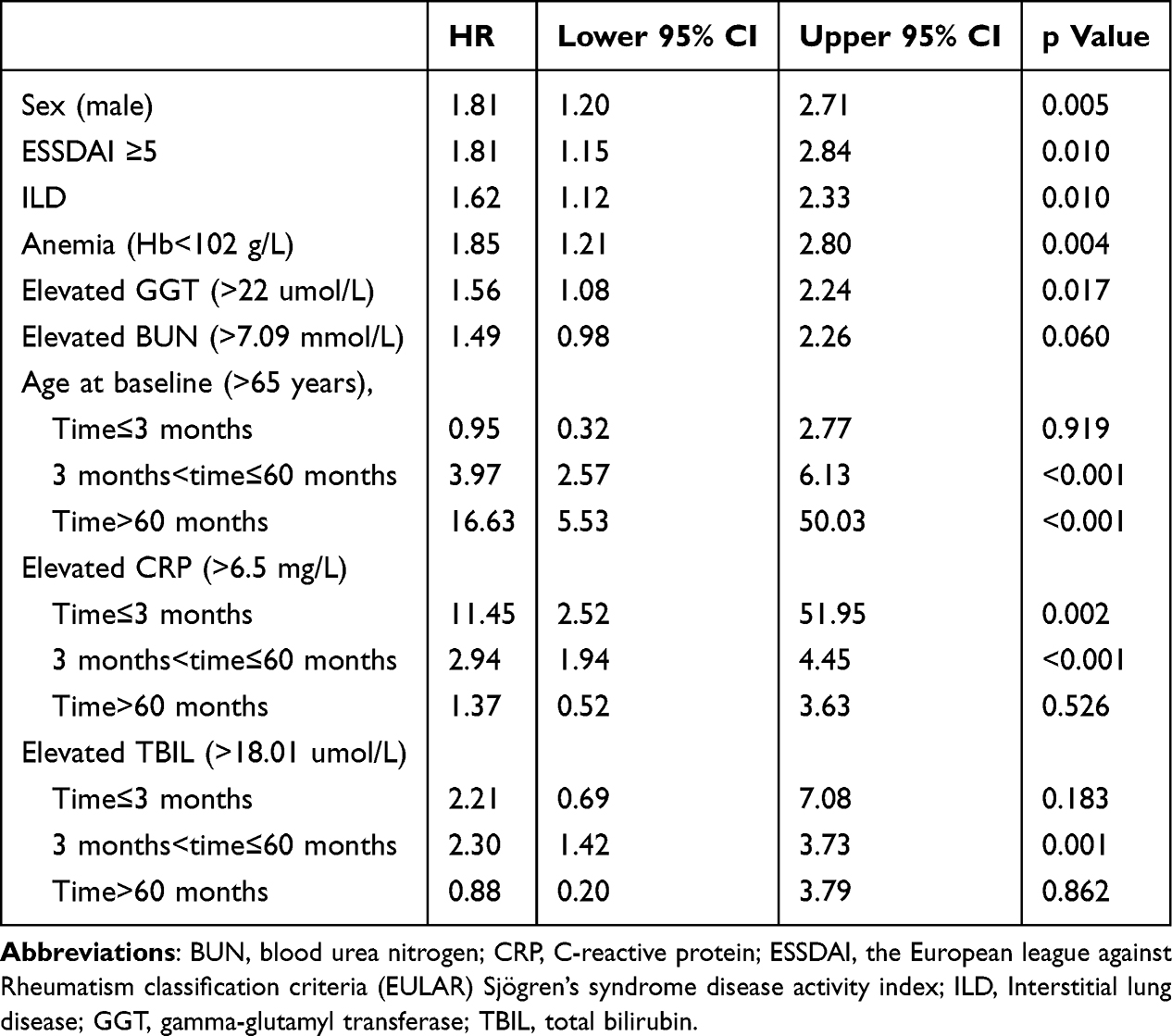 |
Table 3 Time-Dependent Multivariate Analysis of Patients Who Died and Survived with Primary Sjogren’s Syndrome |
Causes of Mortality in Patients with pSS
Infection (55, 39%), malignant tumours (21, 15%) and cardiovascular and cerebrovascular diseases (19, 14%) were the main causes of mortality in the 138 patients who died from pSS (Figure 2). Considering that TBIL and GGT are independent risk factors for death in patients with pSS, we further compared the prevalence of hepatobiliary diseases between living patients and deceased patients and detected no significant differences in the incidence of hepatobiliary diseases or primary biliary cholangitis (PBC) between living patients and deceased patients (Supplementary Table 5). We analyzed causes of death in pSS patients with elevated CRP or TBIL, respectively (Supplementary Table 6 and Supplementary Table 7). We found that the primary cause of death in patients with elevated CRP was infection (33, 44.59%), followed by malignant tumor (11, 14.86%) and respiratory failure (11, 14.86%). The primary cause of death in patients with elevated TBIL was infection (11, 40.74%), followed by Cardiovascular and cerebrovascular diseases (5, 18.52%) and malignant tumor (4, 14.81%).
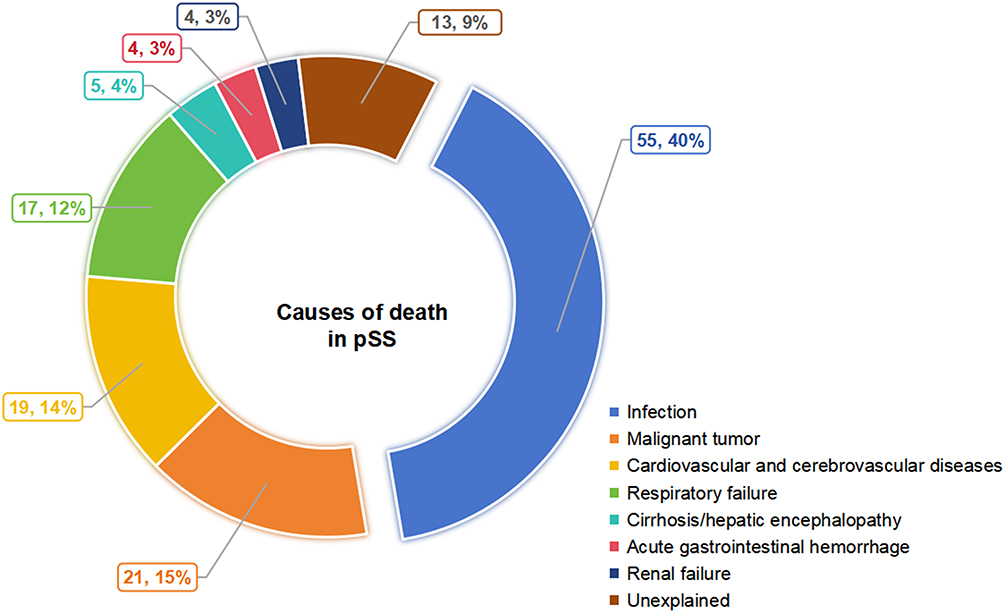 |
Figure 2 Summary of causes of death in patients with primary Sjogren’s syndrome. Abbreviation: pSS, primary Sjogren’s syndrome. |
Discussion
In this study, we followed 1252 pSS patients, of whom 138 died, with long-term follow-up times ranging from 0 to 11.1 years. We present several key risk factors for death in patients with pSS, and we clarify for the first time how time-dependent risk factors change the risk of death over time in patients with pSS. First, in addition to sex and the ESSDAI and ILD, which are often reported to increase the risk of death in patients with pSS, anaemia and GGT are independent risk factors for death in patients with pSS, and the hazard ratios (HRs) do not change over time. Second, this study revealed for the first time that CRP increased the risk of death in pSS patients in the short term but had no effect on death after five years of follow-up. The increased mortality risk of TBIL in pSS patients was stable at 3–6 months. Third, age at diagnosis affects the long-term mortality rate of patients with pSS. The HR of death at the age of diagnosis in patients with pSS increases with increasing age so the risk ratio is not constant; this is especially true for patients older than 65 years, whose 5-year mortality HR is quite high. Abnormalities in these common general biochemical markers provide a more complete picture of pSS patients who are at high risk of death, especially in the short-term and long-term, and such patients would require close monitoring and aggressive treatment. The short-term and long-term risk factors for mortality in pSS discovered in this study, combined with traditional biomarkers, can provide a reference for the mortality of pSS.
We confirmed previous findings that sex, ESSDAI, and ILD are independent risk factors for death in patients with pSS.6,7,10,11,13,16 We found for the first time that elevated CRP increased the risk of death in pSS patients in the short term but had no effect on the long-term prognosis of pSS. pSS patients with elevated CRP are more likely to have ILD,17,18 and CRP levels are often elevated in pSS-ILD patients.17,19,20 A retrospective cohort study revealed that higher levels of ESSDAI and CRP were associated with an increased risk of infection in patients with pSS-ILD.21 A multicentre cohort study has shown that a highly sensitive test for CRP levels can be used to assess cardiovascular disease risk, which is increased in pSS patients.22 In this study, infection was the leading cause of death among pSS patients, and cardiovascular risk was the third leading cause of death. The main cause of death in patients with elevated CRP was infection, followed by malignant tumor and respiratory failure. CRP had the highest risk ratio for death in pSS patients within 3 months, and the effect on death after 5 years was not significantly different, considering that the poor prognosis caused by elevated CRP was more likely to be associated with acute infection. In pSS patients with elevated CRP levels, inflammation should be controlled as soon as possible to lower CRP levels.
We found that anaemia is an independent risk factor for death in patients with pSS, with a less than 2-fold increased risk of death, which has not been mentioned in previous studies. Anaemia is the most common haematological manifestation in patients with pSS, and in most cases, anaemia is caused by immune-mediated chronic disease.23 Haemolytic anaemia, iron deficiency anaemia, and malignant anaemia can also occur in patients with pSS.24,25 Compared with pSS patients, pSS patients combined with systemic lupus erythematosus (SLE) are more likely to have anaemia symptoms.26 Previous studies have shown that decreased haemoglobin levels are associated with the occurrence of haematological malignancies in patients with SLE27 and that such a decrease is an independent risk factor for readmission to the hospital or death in this patient group.28,29 Further research is needed to investigate the mechanisms and impact of anaemia on patients with pSS.
For the first time, we found that elevated TBIL increases the risk of death in pSS patients in the medium term and has no effect on the long-term prognosis of pSS. From the clinical routine threshold to the optimized clinical cut-off point, the window of TBIL increasing the risk of pSS mortality decreased to a stable 3–6 months. Additionally, we identified elevated GGT as an independent risk factor for death in pSS patients. TBIL levels appear to be lower in pSS patients than in healthy individuals.30 The increase in TBIL or GGT in pSS patients indicates that pSS itself leads to liver damage or that PBC is combined with other factors and that liver damage can be a nonexocrine feature of pSS.30 A retrospective cohort study of a Chinese population suggested that liver damage is an independent risk factor for death in patients with pSS.16 pSS is known to be strongly associated with PBC.31 We further analysed the incidence of PBC between patients who died and those who survived with pSS and found no difference. Previous studies have shown that the level of bilirubin correlates with the pathological stage of PBC.32 GGT and TBIL are indicators of poor prognosis in PBC patients, and the survival rate of PBC patients with elevated GGT or TBIL is significantly reduced.33–35 GGT and TBIL levels are greater in pSS patients with PBC than in pSS patients and are positively associated with a high Th17/Treg ratio, which may indicate a better validation status.36 Although the poor prognosis of pSS in this study was not related to the occurrence of PBC, it may be related to the severity or prognosis of PBC. We found that cirrhosis, hepatic encephalopathy and upper digestive tract bleeding caused by liver cirrhosis are not uncommon causes of death in patients with pSS. Among deceased individuals with elevated TBIL, the spectrum of mortality etiologies extends beyond hepatobiliary disorders to include infections, cardiovascular and cerebrovascular diseases, and malignant tumor. According to our results, the effect of TBIL on mortality within 3 months is controversial and is related to the TBIL cut-off value. When patients with PBC are treated with ursodeoxycholic acid, the predictive value of serum bilirubin is lost.37 We found that after five years of follow-up, the effect of TBIL on death in pSS patients disappeared. Ursodeoxycholic acid and other bilirubin-lowering therapies may have interfered with the true association between TBIL and mortality risk. Due to incomplete documentation of medication use in this study, future investigations should prospectively record treatment information to further validate these findings. Therefore, in the evaluation of patients with pSS, those with elevated TBIL levels must be followed up more closely by the clinician in the short term, and GGT and TBIL levels need to be returned to normal levels as soon as possible.
We have shown that the effect of age at diagnosis on the risk of death in pSS patients is not constant and that it has a greater effect on the risk of death in pSS patients with increasing age. The influence of age at diagnosis on the key phenotypic features of pSS is strong and involves symptoms, autoantibodies, and the ESSDAI.38,39 The results of several previous studies revealed that age at diagnosis is a risk factor for death in patients with pSS, and the risk of death in patients with pSS increases 1.09–1.13 times with increasing age.6,8,10 For the first time, we found that age at diagnosis had no effect on death in patients with pSS within 3 months and that age increased the risk of death in patients with pSS from 1.01 to 1.08 years between 30 and 60 months and after >60 months. We further analysed age and found the greatest difference in survival between patients before and after the age of 65 years, with 5-year mortality risk ratios for pSS patients >65 years being 16 times greater than those for pSS patients <65 years. Older patients, especially those older than 65 years, need closer follow-up.
Our results also revealed that infection, malignant tumours and cardiovascular and cerebrovascular diseases were the main causes of pSS-related death, which was basically consistent with the findings of previous studies.6,8–11,13,16 We found that the 2-year, 3-year, 5-year, and 10-year survival rates of pSS patients were 94.0%, 91.9%, 87.6%, and 80.7%, respectively, which were lower than the mortality rates reported in previous studies.6–13,40,41 We also calculated the 3-month survival rate of pSS patients, which was 98.9%. Our survival analysis revealed that the risk ratios for death according to age, CRP level, and TBIL level changed significantly at 3 months and 5 years and that 3 months and 5 years may be critical survival time nodes for pSS patients. In previous studies, cryoglobulins and hypocomplementemia were reported to increase the risk of death in patients with pSS.6,8–10,12,13 Although we did not find significant differences in these three indicators via multivariate regression analysis, univariate analysis revealed that there was a significant difference in these three factors. These differences are due not only to differences in study sources, inclusion criteria, and definitions of organ involvement but also to differences in race, ethnicity, genetics, and environmental factors.
This study had several limitations. Partial baseline data of this study were retrospectively collected, and some specific indicators and comorbidities, such as cryoglobulinemia, were not recorded or analysed. This affected our ability to explore all the risk factors for death associated with pSS. Second, for a few patients, we were unable to identify the specific cause of death. Third, although the relationship between clinical manifestations and death was analysed in this study, the underlying mechanisms could not be elucidated, so this is the direction of our further research.
Conclusion
In conclusion, this study revealed that sex, age at diagnosis, ESSDAI, ILD, anaemia, GGT, CRP, and TBIL are independent risk factors for death in patients with pSS, and they have relatively constant HRs. The influence of diagnostic age, CRP level, and TBIL level on mortality in pSS patients changes over time and has become the main risk factor for mortality in different stages of pSS. Regular testing of these common general biochemical markers can help to identify pSS patients who are at high risk of death more completely and who require close monitoring and aggressive treatment.
Acknowledgments
The authors are grateful to all the participants. The authors would also like to thank the related rheumatology teams. The study was supported by a grant from the Capital’s Funds for Health Improvement (2024-1-4065), Elite Medical Professionals Project of China-Japan Friendship Hospital (NO.ZRJY2024-GG08), China Association of Chinese Medicine Youth Qiu Shi Project (No.2024-QNQS-07), High Level Hospital Clinical Research Funding Specia Project of China-Japan Friendship Hospital (2025-NHLHCRF-JBGS-A-YNZJ-03), and High Level Hospital Clinical Research Funding Specia Project of China-Japan Friendship Hospital (2025-NHLHCRF-PY-36).
Disclosure
Qing-Wen Tao, Jing Luo, Jia-Qi Chen, Zi-Wei Huang, Yan Zhang, Jian-Ying Yang report a pending patent for a system for the development of a screening model for primary Sjogren’s syndrome and its application. The authors report no other conflicts of interest in this work.
References
1. Mariette X, Criswell LA. Primary sjogren’s syndrome. New Engl J Med. 2018;378(10):931–939. doi:10.1056/NEJMcp1702514
2. Meijer JM, Meiners’ PM, Slater JJRH, et al. Health-related quality of life, employment and disability in patients with Sjogren’s syndrome. Rheumatology. 2009;48(9):1077–1082. doi:10.1093/rheumatology/kep141
3. Vujovic S, Desnica J, Stevanovic M, et al. Oral health and oral health-related quality of life in patients with primary Sjogren’s syndrome. Medicina-Lithuania. 2023;59(3).
4. Greenan E, Pilson Q, Gabhann-Dromgoole JN, Murphy CC. Relationship between clinical parameters and quality of life in primary Sjogren’s syndrome: a prospective study. Eye. 2023;37(13):2685–2692. doi:10.1038/s41433-023-02386-2
5. Baldini C, Pepe P, Quartuccio L, et al. Primary Sjogren’s syndrome as a multi-organ disease: impact of the serological profile on the clinical presentation of the disease in a large cohort of Italian patients. Rheumatology. 2014;53(5):839–844. doi:10.1093/rheumatology/ket427
6. Brito-Zerón P, Flores-Chávez A, Horváth IF, et al. Mortality risk factors in primary Sjogren syndrome: a real-world, retrospective, cohort study. Eclinicalmedicine. 2023;61:102062. doi:10.1016/j.eclinm.2023.102062
7. Yazisiz V, Göçer M, Erbasan F, et al. Survival analysis of patients with Sjogren’s syndrome in Turkey: a tertiary hospital-based study. Clin Rheumatol. 2020;39(1):233–241. doi:10.1007/s10067-019-04744-6
8. Theander E, Manthorpe R, Jacobsson LTH. Mortality and causes of death in primary Sjogren’s syndrome - A prospective cohort study. Arthritis Rheumatol US. 2004;50(4):1262–1269. doi:10.1002/art.20176
9. Skopouli FN, Dafni U, Ioannidis JP, Moutsopoulos HM. Clinical evolution, and morbidity and mortality of primary Sjögren’s syndrome. Semin Arthritis Rheum. 2000;29(5):296–304. doi:10.1016/s0049-0172(00)80016-5
10. Singh AG, Singh S, Matteson EL. Rate, risk factors and causes of mortality in patients with Sjogren’s syndrome: a systematic review and meta-analysis of cohort studies. Rheumatology. 2016;55(3):450–460. doi:10.1093/rheumatology/kev354
11. Qian JY, He CM, Li Y, et al. Ten-year survival analysis of patients with primary Sjogren’s syndrome in China: a national prospective cohort study. Ther Adv Musculoskel. 2021;13.
12. Ioannidis JP, Vassiliou VA, Moutsopoulos HM. Long-term risk of mortality and lymphoproliferative disease and predictive classification of primary Sjögren’s syndrome. Arthritis Rheum. 2002;46(3):741–747. doi:10.1002/art.10221
13. Brito-Zerón P, Kostov B, Solans R, et al. Systemic activity and mortality in primary Sjogren syndrome: predicting survival using the EULAR-SS Disease Activity Index (ESSDAI) in 1045 patients. Ann Rheum Dis. 2016;75(2):348–355. doi:10.1136/annrheumdis-2014-206418
14. Luppi F, Sebastiani M, Silva M, et al. Interstitial lung disease in Sjogren’s syndrome: a clinical review. Clin Exp Rheumatol. 2020;38(4):S291–S300.
15. Seror R, Bowman SJ, Brito-Zeron P, et al. EULAR Sjögren’s syndrome disease activity index (ESSDAI): a user guide. RMD Open. 2015;1(1):e000022. doi:10.1136/rmdopen-2014-000022
16. Lin DF, Yan SM, Zhao Y, et al. Clinical and prognostic characteristics of 573 cases of primary Sjogren’s syndrome. Chinese Med J-Peking. 2010;123(22):3252–3257. doi:10.3760/cma.j.issn.0366-6999.2010.22.015
17. Gao H, Zhang XW, He J, et al. Prevalence, risk factors, and prognosis of interstitial lung disease in a large cohort of Chinese primary Sjögren syndrome patients: a case-control study. Medicine. 2018;97(24):e11003. doi:10.1097/md.0000000000011003
18. Zhang K, Li W, He C, He X, Hou J. The ratio of neutrophil to lymphocyte predicts interstitial lung disease and its prognosis in patients with primary Sjögren’s syndrome: a retrospective analysis. Ann Palliat Med. 2021;10(6):6493–6501. doi:10.21037/apm-21-1043
19. Shi L, Han XL, Guo HX, et al. Increases in tumor markers are associated with primary Sjögren’s syndrome-associated interstitial lung disease. Ther Adv Chronic Dis. 2020;11:2040622320944802. doi:10.1177/2040622320944802
20. Li D, Li H, Wang Y, Zhu T. Pulmonary fibrosis in primary Sjögren syndrome: computed tomography, clinical features, and associated clinical factors. Pol Arch Intern Med. 2023;133(2). doi:10.20452/pamw.16394
21. Li H, Jin Y, He J. Respiratory infection risk in primary Sjögren’s syndrome complicated with interstitial lung disease: a retrospective study. Clin Rheumatol. 2024;43(5):1777. doi:10.1007/s10067-024-06923-6
22. Bartoloni E, Baldini C, Schillaci G, et al. Cardiovascular disease risk burden in primary Sjögren’s syndrome: results of a population-based multicentre cohort study. J Intern Med. 2015;278(2):185–192. doi:10.1111/joim.12346
23. Zhou JG, Qing YF, Jiang L, Yang QB, Luo WF. Clinical analysis of primary Sjögren’s syndrome complicating anemia. Clin Rheumatol. 2010;29(5):525–529. doi:10.1007/s10067-009-1366-x
24. Baimpa E, Dahabreh IJ, Voulgarelis M, Moutsopoulos HM. Hematologic manifestations and predictors of lymphoma development in primary Sjögren syndrome: clinical and pathophysiologic aspects. Medicine. 2009;88(5):284–293. doi:10.1097/MD.0b013e3181b76ab5
25. Ramakrishna R, Chaudhuri K, Sturgess A, Manoharan A. Haematological manifestations of primary Sjögren’s syndrome: a clinicopathological study. Q J Med. 1992;83(303):547–554.
26. Szanto A, Szodoray P, Kiss E, Kapitany A, Szegedi G, Zeher M. Clinical, serologic, and genetic profiles of patients with associated Sjögren’s syndrome and systemic lupus erythematosus. Hum Immunol. 2006;67(11):924–930. doi:10.1016/j.humimm.2006.06.006
27. Zhang Y, Li W, Zhang P, et al. Hematological malignancies in systemic lupus erythematosus: clinical characteristics, risk factors, and prognosis-a case-control study. Arthritis Res Ther. 2022;24(1):5. doi:10.1186/s13075-021-02692-8
28. Nangit A, Lin C, Ishimori ML, Spiegel BMR, Weisman MH. Causes and predictors of early hospital readmission in systemic lupus erythematosus. J Rheumatol. 2018;45(7):929–933. doi:10.3899/jrheum.170176
29. Mu L, Hao Y, Fan Y, et al. Mortality and prognostic factors in Chinese patients with systemic lupus erythematosus. Lupus. 2018;27(10):1742–1752. doi:10.1177/0961203318789788
30. Zhang Z, Su Q, Zhang L, Yang Z, Qiu Y, Mo W. Clinical significance of serum bilirubin in primary Sjögren syndrome patients. J Clin Lab Anal. 2020;34(3):e23090. doi:10.1002/jcla.23090
31. Deng X, Li J, Hou S, Ci B, Liu B, Xu K. Prevalence and impact of Sjögren’s syndrome in primary biliary cholangitis: a systematic review and meta-analysis. Ann Hepatol. 2022;27(6):100746. doi:10.1016/j.aohep.2022.100746
32. Drebber U, Mueller JJ, Klein E, et al. Liver biopsy in primary biliary cirrhosis: clinicopathological data and stage. Pathol Int. 2009;59(8):546–554. doi:10.1111/j.1440-1827.2009.02405.x
33. Dickson ER, Grambsch PM, Fleming TR, Fisher LD, Langworthy A. Prognosis in primary biliary cirrhosis: model for decision making. Hepatology. 1989;10(1):1–7. doi:10.1002/hep.1840100102
34. Lammers WJ, van Buuren HR, Hirschfield GM, et al. Levels of alkaline phosphatase and bilirubin are surrogate end points of outcomes of patients with primary biliary cirrhosis: an international follow-up study. Gastroenterology. 2014;147(6):1338–49.e5;quize15. doi:10.1053/j.gastro.2014.08.029
35. Gerussi A, Bernasconi DP, O’Donnell SE, et al. Measurement of gamma glutamyl transferase to determine risk of liver transplantation or death in patients with primary biliary cholangitis. Clin Gastroenterol Hepatol. 2021;19(8):1688–1697.e14. doi:10.1016/j.cgh.2020.08.006
36. Hao LR, Li XF, Gao C, Cao L, Han ZY, Gao H. Th17/Treg cell level and clinical characteristics of peripheral blood of patients with Sjogren’s syndrome complicated with primary biliary cirrhosis. Medicine. 2019;98(24):e15952. doi:10.1097/md.0000000000015952
37. Poupon RE, Balkau B, Guéchot J, Heintzmann F. Predictive factors in ursodeoxycholic acid-treated patients with primary biliary cirrhosis: role of serum markers of connective tissue. Hepatology. 1994;19(3):635–640. doi:10.1002/hep.1840190314
38. Retamozo S, Acar-Denizli N, Horváth IF, et al. Influence of the age at diagnosis in the disease expression of primary Sjögren syndrome. Analysis of 12,753 patients from the Sjögren big data consortium. Clin Exp Rheumatol. 2021;133(6):166–174. doi:10.55563/clinexprheumatol/egnd1i
39. Lee KA, Choi W, Kim J, Lee SH, Kim HR, Kim HS. Elderly-onset primary Sjögren’s syndrome focused on clinical and salivary gland ultrasonographic features. Joint Bone Spine. 2021;88(4):105132. doi:10.1016/j.jbspin.2021.105132
40. Kim HJ, Kim KH, Hann HJ, et al. Incidence, mortality, and causes of death in physician-diagnosed primary Sjogren’s syndrome in Korea: a nationwide, population-based study. Semin Arthritis Rheu. 2017;47(2):222–227. doi:10.1016/j.semarthrit.2017.03.004
41. Alamanos Y, Tsifetaki N, Voulgari PV, Venetsanopoulou AI, Siozos C, Drosos AA. Epidemiology of primary Sjogren’s syndrome in north-west Greece, 1982-2003. Rheumatology. 2006;45(2):187–191. doi:10.1093/rheumatology/kei107
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.