Back to Journals » International Journal of General Medicine » Volume 18
Thyroid Status and Pulmonary Thromboembolic Extent: Is There an Association in Patients with Pulmonary Embolism?
Authors Peng YF, Luo M, Luo HJ, Ma LY
Received 26 December 2024
Accepted for publication 20 May 2025
Published 10 June 2025 Volume 2025:18 Pages 2989—2993
DOI https://doi.org/10.2147/IJGM.S514365
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
You-Fan Peng,1,2 Miao Luo,2 Huai-Jun Luo,3 Li-Ya Ma1
1Department of Respiratory and Critical Care Medicine, Affiliated Hospital of Youjiang Medical University for Nationalities, Baise, People’s Republic of China; 2Life Science and Clinical Medicine Research Center, Affiliated Hospital of Youjiang Medical University for Nationalities, Baise, People’s Republic of China; 3Department of Radiology, Affiliated Hospital of Youjiang Medical University for Nationalities, Baise, People’s Republic of China
Correspondence: You-Fan Peng, Department of Respiratory and Critical Care Medicine, Affiliated Hospital of Youjiang Medical University for Nationalities, No. 18 Zhongshan 2nd Road, Baise, Guangxi, 533000, People’s Republic of China, Email [email protected]
Background: Thyroid dysfunction has been associated with thrombotic diseases. However, the association between thyroid status and pulmonary thromboembolic extent remains unclear in patients with pulmonary embolism (PE). Thus, this study investigated the association between thyroid status and pulmonary thromboembolic extent and elucidated the clinical significance of thyroid status assessment in patients with PE.
Methods: We retrospectively analyzed data from 118 patients with PE. Pulmonary thromboembolic extent was assessed with computerized tomography obstruction index.
Results: Serum free triiodothyronine (FT3) levels were significantly higher in PE patients with greater pulmonary thromboembolic extent than in those with lesser pulmonary thromboembolic extent (4.33[4.04– 4.98] vs 4.17[3.33– 4.66] pmol/L, p=0.017), but not for serum free thyroxine (FT4) levels (15.33[13.43-16.94] vs 15.36[13.75-17.82] pmol/L, p=0.908) and serum thyroid stimulating hormone (TSH) levels (1.84[1.01-3.00] vs 1.49[0.74-2.58] uIU/mL, p=0.273). Multivariable linear regression analysis revealed that higher serum FT3 levels were independently associated with greater pulmonary thromboembolic extent in patients with PE (β=0.235, p=0.013).
Conclusion: Higher serum FT3 levels were associated with greater pulmonary thromboembolic extent in patients with PE. This finding suggests that the possibility of extensive pulmonary thromboembolic extent should be noticed for PE patients with higher serum FT3 levels.
Keywords: pulmonary embolism, pulmonary thromboembolic extent, thyroid status
Introduction
Thyroid hormones, essential hormones secreted by the thyroid gland, play a crucial role in maintaining metabolic homeostasis.1 Clinical evaluations of thyroid hormone levels directly reflect thyroid functional status.2 Thyroid hormones have an important influence on coagulation system,3 with hyperthyroidism demonstrating causal relationships with reduced anticoagulant factor levels.4 Coagulation and fibrinolytic system alterations occur in hyperthyroid and hypothyroid states, and high thyroid hormone levels promote procoagulant activity and suppress fibrinolysis.5 In recent years, accumulating evidence has established notable associations between thyroid dysfunction and thrombotic diseases.6–8 Interestingly, thyroid dysfunction has been linked to clinical outcomes in patients with pulmonary embolism (PE).9 However, to our knowledge, limited study has examined the association between thyroid status and pulmonary thromboembolic extent in patients with PE. Therefore, this study examined this association to elucidate the clinical significance of thyroid status assessment in patients with PE.
Methods
The study retrospective included 118 patients diagnosed with PE at the Affiliated Hospital of Youjiang Medical University for Nationalities between January 2020 to October 2024. All patients with PE were identified based on clinical diagnostic information through electronic medical records. The diagnosis of PE was confirmed by computerized tomography pulmonary angiography (CTPA).10 Patients with PE receiving thrombolytic therapy prior to admission were excluded from this study. The study was approved by the Ethical Committee at the Affiliated Hospital of Youjiang Medical University for Nationalities and followed the principles of Declaration of Helsinki. Given the retrospective nature of the study, a waiver of informed consent was granted by the Ethical Committee of the Affiliated Hospital of Youjiang Medical University for Nationalities. The data of patients were maintained with confidentiality.
The study data, which included demographic and clinical characteristics, laboratory investigation results, and imaging examination results, were collected from electronic medical records. The demographic and clinical characteristics included sex, age, height, weight, smoking history, medication history, and comorbidity.The laboratory investigation results included prothrombin time (PT), activated partial thromboplastin time (APTT), thrombin time (TT), D-dimer, free triiodothyronine (FT3), free thyroxine (FT4), and thyroid stimulating hormone (TSH), and the imaging examination results included color Doppler ultrasonography for lower-extremity deep venous thrombosis (LEDVT) assessment and CTPA. Body mass index (BMI) was calculated by dividing weight in kilograms by the square of height in meters.
Pulmonary thromboembolic extent was assessed by computerized tomography obstruction index, and the computerized tomography obstruction index was calculated according to CTPA findings using the formula: Σ(n ⋅ d) /40×100%, where n represents the value of the proximal thrombus in the pulmonary arterial tree, corresponding to the number of affected distal segmental branches (minimum, 1; maximum, 20), and d represents the degree of obstruction (minimum, 0; maximum, 2).11
Categorical variables are reported as frequency (percentage), and continuous variables are reported as median (interquartile range) given their nonnormal distribution. Differences in continuous variables were analyzed by Mann-Whitney U-test, and differences in categorical variables were analyzed by chi-square test. Univariable linear regression analysis was initially used to analyze potential factors associated with pulmonary thromboembolic extent in patients with PE. Subsequently, multivariable linear regression analysis was applied to identify independent factors, following verification of key regression assumptions including linearity, independence, residual normality, homoscedasticity, and multicollinearity. All statistical analyses adopted two-tailed test with statistical significance defined at p <0.05. Statistical analyses were performed using IBM SPSS Statistics version 25.0 (IBM Corporation, Armonk, NY, USA).
Results
The results of comparison in characteristics of patients with PE stratified by the median of pulmonary thromboembolic extent are presented in Table 1. Significantly higher serum FT3 levels were observed in PE patients with greater pulmonary thromboembolic extent than in those with lesser pulmonary thromboembolic extent (4.33[4.04–4.98] vs 4.17[3.33–4.66] pmol/L, p=0.017); however, serum FT4 levels (15.33[13.43-16.94] vs 15.36[13.75-17.82] pmol/L, p=0.908) and serum TSH levels (1.84[1.01-3.00] vs 1.49[0.74-2.58] uIU/mL, p=0.273) showed no significant differences. In addition, PE patients with greater pulmonary thromboembolic extent exhibited significantly higher frequency of LEDVT history (p=0.006), higher plasma D-dimer levels (p=0.002), and lower plasma PT levels (p=0.045) than in those with lesser pulmonary thromboembolic extent. Sex (p=0.379), age (p=0.998), BMI (p=0.587), smoking history (p=0.923), chronic obstructive pulmonary disease (COPD) history (p=0.182), APTT (p=0.072), and TT (p=0.258) showed no significant differences between the groups.
 |
Table 1 The Characteristics of Patients with PE Stratified by the Median of Pulmonary Thromboembolic Extent |
The results of univariable and multivariable linear regression analyses between thyroid status and pulmonary thromboembolic extent in patients with PE are detailed in Table 2. Univariable linear regression analysis revealed that LEDVT history (β=0.264, p=0.004), higher plasma D-dimer levels (β=0.355, p<0.001), and higher serum FT3 levels (β=0.204, p=0.027) were significantly associated with greater pulmonary thromboembolic extent in patients with PE; however, no significant associations were found between serum FT4 levels (β=-0.057, p=0.541) or serum TSH levels (β=-0.070, p=0.454) and pulmonary thromboembolic extent in patients with PE. In subsequent multivariable linear regression analysis adjusted for sex, age, BMI, smoking history, LEDVT history, COPD history, PT, APTT, TT, and D-dimer, higher serum FT3 levels maintained an independent association with greater pulmonary thromboembolic extent in patients with PE (β=0.235, p=0.013), and higher plasma D-dimer levels were independently associated with greater pulmonary thromboembolic extent in patients with PE (β=0.332, p<0.001).
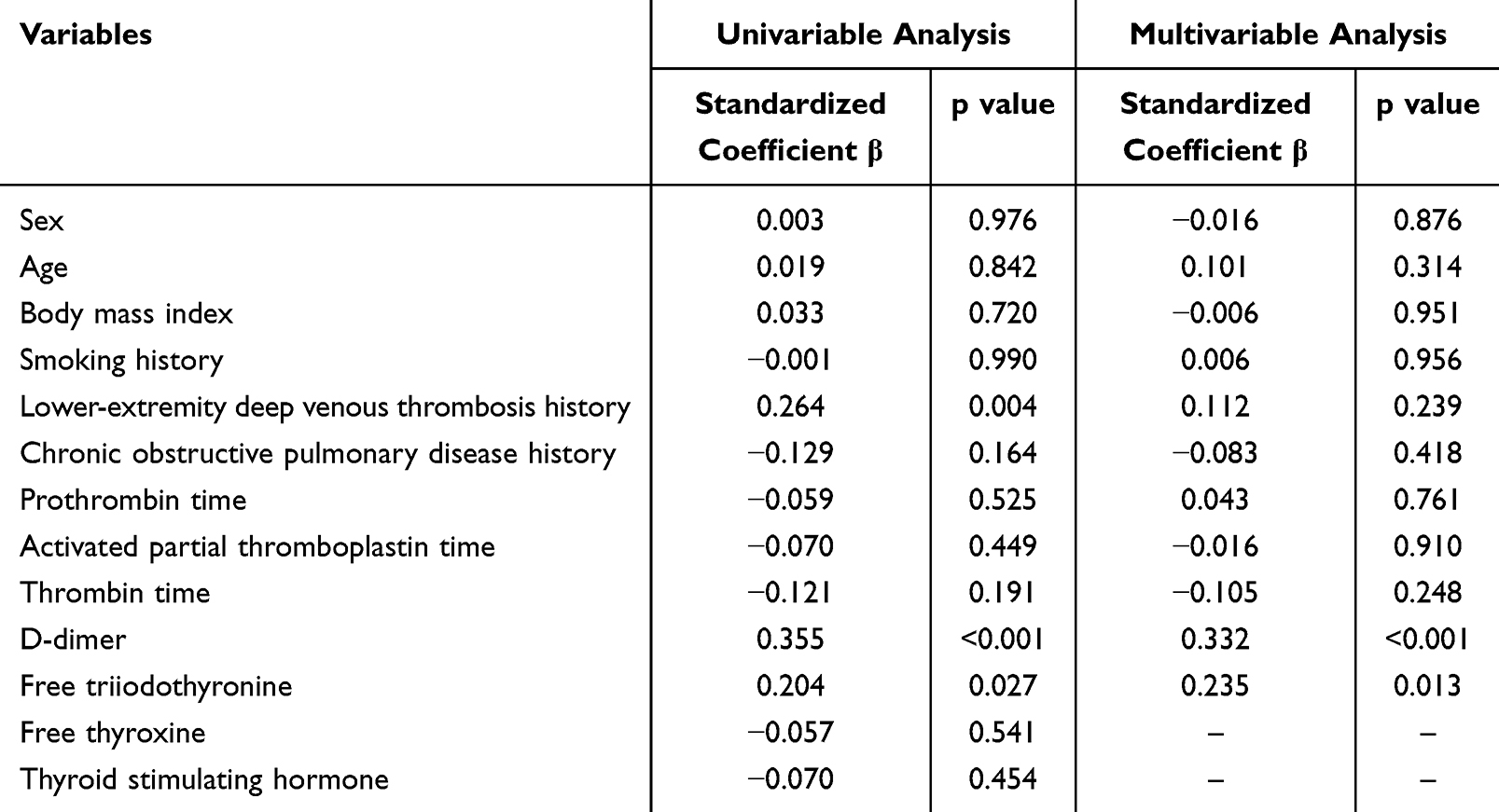 |
Table 2 Univariable and Multivariable Linear Regression Analyses Between Serum FT3 Levels and Pulmonary Thromboembolic Extent in Patients with PE |
Discussion
Thyroid hormones are involved in the regulation of coagulation disorders, and hyperthyroidism enhances coagulation activity and increases thrombotic risk,12 whereas overt hypothyroidism may predispose patients to an increased risk of bleeding.13 Hyperthyroidism has been reported to be associated with cardiovascular diseases such as myocardial infarction, atrial fibrillation, and myocarditis.14–16 It has been shown that increased thyroid hormones may result in coronary vascular degeneration and plaque instability, manifesting as more high-grade coronary stenoses, plaque burden, and high-risk plaque features.17 Clinical observation in euthyroid patients with acute myocardial infarction has revealed an inverse correlation between serum FT3 levels and international normalized ratio,18 suggesting that higher serum FT3 levels may be associated with thrombosis risk. A positive correlation between serum FT3 levels and factor IX activity has been demonstrated in patients with hypothyroidism,19 implying FT3 may mediate the enhancement of coagulation through factor IX activation. Experimental evidence by Shih et al indicated that triiodothyronine (T3) treatment increased the production of fibrinogen and multiple coagulation factors, suggesting T3 promotes blood clotting dependent the transcriptional regulation of fibrinogen and coagulation proteins.20 In hypothyroid animal models, T3 administration modulates the transcription of coagulation factors in hepatic and vascular tissues, resulting in longer PT and shorter APTT.21 Notably, T3 has been also shown to increase the amounts of coagulant proteins including factor II, factor X, and fibrinogen.22 Thus, the effects of FT3 on coagulation pathways may provide mechanistic insights into the observed association between higher serum FT3 levels and greater pulmonary thromboembolic extent in patients with PE.
D-dimer, a biomarker of intravascular thrombosis, has been regarded as a predictor of disease severity in patients with acute PE.23,24 Türedi S et al demonstrated a positive association between D-dimer levels and pulmonary embolism severity in acute PE.25 Our study identified an independent association between with higher plasma D-dimer levels and greater pulmonary thromboembolic extent in patients with PE, suggesting the clinical utility of D-dimer for evaluating pulmonary thromboembolic extent in patients with PE.
This investigation has several limitations. First, the relatively small sample size may weaken the statistical power and the generalizability of findings. Second, the cross-sectional design cannot provide causal inference regarding the association between serum FT3 levels and pulmonary thromboembolic extent in patients with PE. Third, echocardiographic measurements have been associated with clinical outcomes in patients with PE;26 however, our study did not evaluate the role of echocardiographic measurements in patients with PE.
In summary, this study revealed a positive association between serum FT3 levels and pulmonary thromboembolic extent in patients with PE. This finding indicates that PE patients exhibiting higher serum FT3 levels may require additional notice for possible extensive pulmonary thromboembolic extent. However, the prognostic value of serum FT3 levels needs be further confirmed by prospective studies in patients with PE.
Data Sharing Statement
Data are available upon reasonable request from the corresponding author.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Taylor PN, Albrecht D, Scholz A, et al. Global epidemiology of hyperthyroidism and hypothyroidism. Nat Rev Endocrinol. 2018;14(5):301–316. doi:10.1038/nrendo.2018.18
2. Boelaert K, Franklyn JA. Thyroid hormone in health and disease. J Endocrinol. 2005;187(1):1–15. doi:10.1677/joe.1.06131
3. Squizzato A, Gerdes VE, Ageno W, Büller HR. The coagulation system in endocrine disorders: a narrative review. Intern Emerg Med. 2007;2(2):76–83. doi:10.1007/s11739-007-0026-X
4. Li X, Lin P, Qi M, Zhou H, Liang Z. Impact of thyroid function on coagulation and venous thromboembolism: a two-sample Mendelian randomization study. J Thromb Thrombolysis. 2024;57(7):1145–1153. doi:10.1007/s11239-024-03025-7
5. Elbers LPB, Fliers E, Cannegieter SC. The influence of thyroid function on the coagulation system and its clinical consequences. J Thromb Haemost. 2018;16(4):634–645. doi:10.1111/jth.13970
6. Fandler-Höfler S, Pilz S, Ertler M, et al. Thyroid dysfunction in cerebral venous thrombosis: a retrospective cohort study. J Neurol. 2022;269(4):2016–2021. doi:10.1007/s00415-021-10776-3
7. Alsaidan AA, Alruwiali F. Association between hyperthyroidism and thromboembolism: a retrospective observational study. Ann Afr Med. 2023;22(2):183–188. doi:10.4103/aam.aam_105_22
8. van Zaane B, Squizzato A, Huijgen R, et al. Increasing levels of free thyroxine as a risk factor for a first venous thrombosis: a case-control study. Blood. 2010;115(22):4344–4349. doi:10.1182/blood-2009-11-253724
9. Pohl KR, Hobohm L, Krieg VJ, et al. Impact of thyroid dysfunction on short-term outcomes and long-term mortality in patients with pulmonary embolism. Thromb Res. 2022;211:70–78. doi:10.1016/j.thromres.2022.01.014
10. Konstantinides SV, Meyer G, Becattini C, et al. ESC guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS): the task force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC). Eur Respir J. 2019;54(3):1901647. doi:10.1183/13993003.01647-2019
11. Qanadli SD, El Hajjam M, Vieillard-Baron A, et al. New CT index to quantify arterial obstruction in pulmonary embolism: comparison with angiographic index and echocardiography. AJR Am J Roentgenol. 2001;176(6):1415–1420. doi:10.2214/ajr.176.6.1761415
12. Davis PJ, Mousa SA, Schechter GP. New interfaces of thyroid hormone actions with blood coagulation and thrombosis. Clin Appl Thromb Hemost. 2018;24(7):1014–1019. doi:10.1177/1076029618774150
13. Squizzato A, Romualdi E, Büller HR, Gerdes VE. Clinical review: thyroid dysfunction and effects on coagulation and fibrinolysis: a systematic review. J Clin Endocrinol Metab. 2007;92(7):2415–2420. doi:10.1210/jc.2007-0199
14. Kim HJ, Kang T, Kang MJ, Ahn HS, Sohn SY. Incidence and mortality of myocardial infarction and stroke in patients with hyperthyroidism: a nationwide cohort study in Korea. Thyroid. 2020;30(7):955–965. doi:10.1089/thy.2019.0543
15. Noue K, Guo R, Lee ML, et al. Iodine-induced hyperthyroidism and long-term risks of incident atrial fibrillation and flutter. J Clin Endocrinol Metab. 2023;108(10):e956–e962. doi:10.1210/clinem/dgad250
16. Lai TF, Liu Z. Hyperthyroidism and fulminant myocarditis in an adolescent with iodine-induced hyperthyroidism: a case report. SAGE Open Med Case Rep. 2024;12:2050313X241305257. doi:10.1177/2050313X241305257
17. Beyer C, Plank F, Friedrich G, Wildauer M, Feuchtner G. Effects of hyperthyroidism on coronary artery disease: a computed tomography angiography study. Can J Cardiol. 2017;33(10):1327–1334. doi:10.1016/j.cjca.2017.07.002
18. Li L, Guo CY, Yang J, et al. Negative association between free triiodothyronine level and international normalized ratio in euthyroid subjects with acute myocardial infarction. Acta Pharmacol Sin. 2011;32(11):1351–1356. doi:10.1038/aps.2011.118
19. Erem C, Kavgaci H, Ersöz HO, et al. Blood coagulation and fibrinolytic activity in hypothyroidism. Int J Clin Pract. 2003;57(2):78–81. doi:10.1111/j.1742-1241.2003.tb10430.x
20. Shih CH, Chen SL, Yen CC, et al. Thyroid hormone receptor-dependent transcriptional regulation of fibrinogen and coagulation proteins. Endocrinology. 2004;145(6):2804–2814. doi:10.1210/en.2003-1372
21. Salloum-Asfar S, Boelen A, Reitsma PH, van Vlijmen BJ. The immediate and late effects of thyroid hormone (triiodothyronine) on murine coagulation gene transcription. PLoS One. 2015;10(5):e0127469. doi:10.1371/journal.pone.0127469
22. Niessen RW, Pfaffendorf BA, Sturk A, et al. The influence of insulin, beta-estradiol, dexamethasone and thyroid hormone on the secretion of coagulant and anticoagulant proteins by HepG2 cells. Thromb Haemost. 1995; 74(2):686–692.
23. Johnson ED, Schell JC, Rodgers GM. The D-dimer assay. Am J Hematol. 2019;94(7):833–839. doi:10.1002/ajh.25482
24. Geissenberger F, Schwarz F, Probst M, et al. D-dimer predicts disease severity but not long-term prognosis in acute pulmonary embolism. Clin Appl Thromb Hemost. 2019;25:1076029619863495. doi:10.1177/1076029619863495
25. Türedi S, Karahan SC, Menteşe A, et al. Investigation of relationship between the D-dimer and ischemia-modified albumin levels with the radiological imaging-based pulmonary embolism severity score in acute pulmonary embolism. Anadolu Kardiyol Derg. 2010;10(4):346–352. doi:10.5152/akd.2010.094
26. Kültürsay B, Keskin B, Tanyeri S, et al. Prognostic impact of the tricuspid annular plane systolic excursion/pulmonary arterial systolic pressure ratio in acute pulmonary embolism. Anatol J Cardiol. 2024;28(10):479–485. doi:10.14744/AnatolJCardiol.2024.4110
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.