Back to Journals » ImmunoTargets and Therapy » Volume 13
Thrombopoietin Receptor Agonists in Post-Hematopoietic Cell Transplantation Complicated by Prolonged Thrombocytopenia: A Comprehensive Review
Authors Elsayed A ![]() , Elsayed B, Elmarasi M
, Elsayed B, Elmarasi M ![]() , Elsabagh AA, Elsayed E, Elmakaty I
, Elsabagh AA, Elsayed E, Elmakaty I ![]() , Yassin M
, Yassin M ![]()
Received 8 February 2024
Accepted for publication 8 August 2024
Published 13 September 2024 Volume 2024:13 Pages 461—486
DOI https://doi.org/10.2147/ITT.S463384
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sarah Wheeler
Abdelrahman Elsayed,1 Basant Elsayed,1 Mohamed Elmarasi,1 Ahmed Adel Elsabagh,1 Engy Elsayed,2 Ibrahim Elmakaty,1 Mohamed Yassin2,3
1Department of Medical Education, Hamad Medical Corporation, Doha, Qatar; 2College of Medicine, Qatar University, Doha, Qatar; 3Hematology Section, National Center for Cancer Care and Research (NCCCR), Doha, Qatar
Correspondence: Ibrahim Elmakaty; Mohamed Yassin, Email [email protected]; [email protected]
Abstract: Hematopoietic cell transplantation (HCT) is a well-established procedure that has become a therapeutic mainstay for various hematological conditions. Prolonged thrombocytopenia following HCT is associated with a significant risk of morbidity and mortality, yet no universally recognized treatment protocol exists for such a complication. First-generation thrombopoietin receptor (TpoR) agonists as well as second-generation agents are known for their role in enhancing platelet production, and their use is expanding across various thrombocytopenic conditions. Therefore, we conducted this comprehensive review of the literature to provide an updated evaluation of the use of TpoR agonists and explore their efficacy and safety in the treatment of extended post-HCT thrombocytopenia. The literature search was conducted using PubMed database from 1996 through December 2023, using a predefined strategy with medical subject headings terms. We identified 64 reports on the utility of TpoR agonists, five of them were randomized controlled trials and the rest were retrospective observational studies and case series, with a total number of 1730 patients. Second-generation TpoR agonists appear more convenient than subcutaneous recombinant human thrombopoietin (rhTpo) as they can be orally administered and exhibit similar efficacy in platelet recovery, as indicated by recent trial results. Among these agents, avatrombopag, unlike eltrombopag, does not require any dietary restrictions, which could be more favorable for patients. However, eltrombopag remains the most extensively studied agent. TpoR agonists had promising effects in the treatment of post-HCT thrombocytopenia with a good safety profile so far, highlighting the potential benefit of their use.
Keywords: hematopoietic cell transplantation, thrombocytopenia, thrombopoietin receptor agonists, recombinant human thrombopoietin, romiplostim, eltrombopag
Introduction
Hematopoietic cell transplantation (HCT) is a well-established, multi-step procedure involving the collection of hematopoietic stem cells, conditioning the patient with a regimen before infusing the stem cells, and ultimately reestablishing a new hematopoietic and immunological system.1 It initially emerged in the early 1960s as a rescue treatment for cancer patients following intense chemotherapy and radiation treatments, as well as to address severe hematopoietic system deficits.2 Since then, it has expanded into an adoptive immunological therapy for many conditions, including malignant and non-malignant hematological conditions and autoimmune diseases.3 HCT is classified as autologous or allogeneic based on the source of hematopoietic cells. In autologous HCT, after receiving a preparative regimen, the patient’s hematopoietic cells taken out before undergoing intense chemotherapy are reintroduced into the patient’s body. The sources of hematopoietic cells in autologous HCT can be from a related or nonrelated donor or umbilical blood cord units.4
Historically, the most feared outcomes of HCT are the relapse of the underlying condition and graft-versus-host disease (GVHD). Relapse of the underlying condition is frequently the main cause of mortality within the first four years following transplantation. Beyond this time, however, there is a considerable chance that patients will experience long-term survival provided they avoid recurrence.5 Despite the continuous evolution of HCT practice, GVHD is still a considerable threat to all patients. A trial testing the effects of using preemptive prednisolone therapy in patients with allogeneic HCT compared to placebo did not find a significant effect on the incidence or the severity of acute graft-versus-host disease (aGVHD), which is reported to contribute by as high as 50% to non-relapse-related mortality.6 Multiple studies report increased rates of GVHD incidence over the years. For instance, a study aimed to analyze the trends in the incidence and outcome of chronic graft-versus-host disease (cGVHD) over 12 years reported that the incidence has increased over time, even after adjusting for factors, such as donor type, graft type, and conditioning intensity.7 On the other hand, many studies reported improved mortality for HCT patients. The number of individuals who have undergone autologous and allogeneic HCT and survived is steadily rising. For patients who have maintained remission during the first two to five years after transplantation, it is estimated that around 80–90% of them will still be alive during the following ten years.5 These findings of increased survival and decreased rates of complications have been consistent among many studies that compared earlier versus recent eras of HCT practice.8–11 Given the improved survival rates observed among post-HCT patients, a convergence with the general population’s lifespan underscores the urgency of addressing the associated long-term complications. A salient concern in this regard is post-transplant thrombocytopenia, a protracted condition that poses a substantial risk of morbidity for post-HCT patients. Despite the magnitude of this issue, a universally recognized treatment protocol for post-transplant thrombocytopenia has yet to be established. Thrombopoietin receptor (TpoR) agonists, including both first-generation and second-generation agents, have emerged as pivotal interventions due to their demonstrated efficacy in augmenting platelet production. The utilization of these agents is progressively expanding across diverse thrombocytopenic conditions. Consequently, we embarked on an exhaustive literature review to deliver an updated and comprehensive assessment of the use of TpoR agonists. Our aim is to explore the efficacy and safety of these agents specifically in the context of treating prolonged post-HCT thrombocytopenia.
Materials and Methods
Search Strategy and Selection Criteria
The review focus was centered on peer-reviewed clinical papers involving the use of first-generation TpoR agonists (recombinant human thrombopoietin [rhTpo]) and second-generation TpoR agonists (eltrombopag, romiplostim, avatrombopag, lusutrombopag, and herombopag) in patients who underwent HCT due to malignant and non-malignant hematologic conditions and had thrombocytopenia either due to poor graft function, delayed platelet engraftment, secondary failure of platelet engraftment or in few instances to test the efficacy of TpoR agonist to facilitate and speed the process of platelet engraftment. Studies were set as not eligible if it was in a foreign language, exceptions were made for a few studies about rhTpo that were reported in Chinese. Animal studies were not included.
A comprehensive search strategy was employed in the PubMed database, covering the period from 1996 to the first of November 2023, with the aim of thoroughly investigating the utilization of TpoR agonists in addressing thrombocytopenia following HCT. The predefined search strategy incorporated medical subject headings (MeSH) terms such as “Thrombopoietin”, “Hematopoietic Stem Cell Transplantation”, and “Thrombocytopenia”. The articles identified underwent assessment for eligibility by two independent reviewers, considering relevance. Subsequently, the selected articles were retrieved and subjected to full-text assessment by two reviewers independently, adhering to inclusion and exclusion criteria. Data were then extracted from the included articles and presented in tables.
Included Articles
The summary of the electronic search strategy is presented using Figure 1. Our initial search identified 239 articles that underwent title and abstract screening for relevance. Of those, only 82 articles underwent full-text retrieval and assessment, and few studies were found ineligible for inclusion and were excluded, yielding a total of 64 studies to undergo data extraction and to be summarized in two tables. The first table includes ten studies on the use of rhTpo in patients with thrombocytopenia post-HCT, covering 777 patients. Meanwhile, the second table comprises 54 studies on the utilization of second-generation TpoR agonists.
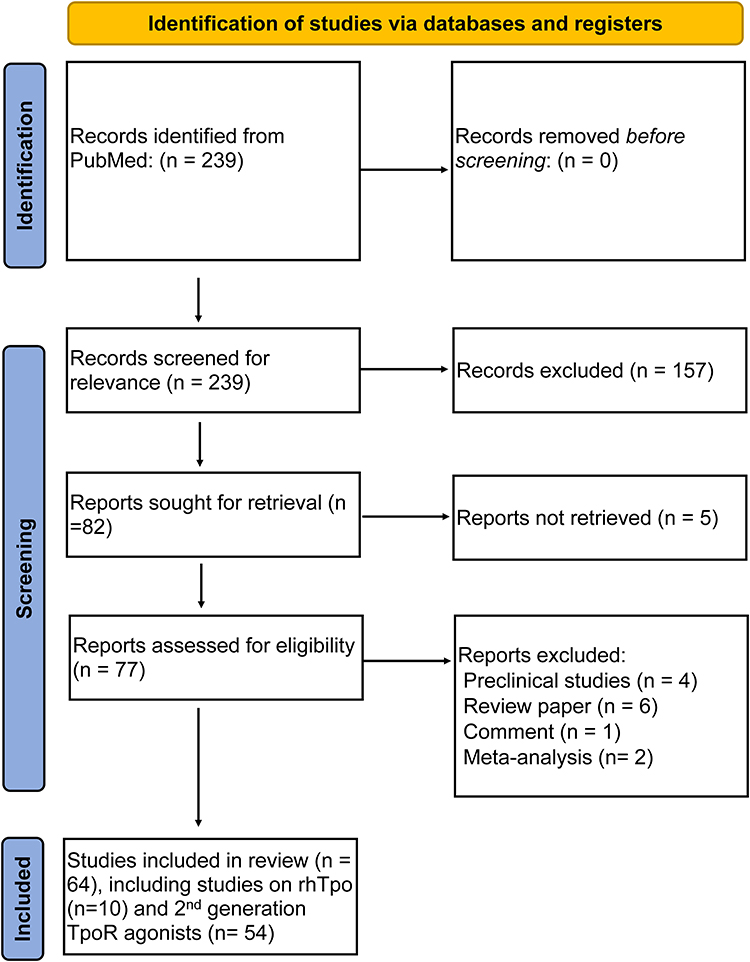 |
Figure 1 Flowchart summarizing the findings of our search strategy. Abbreviations: rhTpo, recombinant human thrombopoietin; TpoR, thrombopoietin receptor. |
Post-HCT Thrombocytopenia
Pathophysiology of Idiopathic Post-HCT Thrombocytopenia
Following myeloablative conditioning and autologous stem cell rescue, all patients experience profound thrombocytopenia, which is caused by bone marrow aplasia brought on by high-dose chemotherapy and/or total body irradiation (TBI). Following autologous hematopoietic progenitor cell transplantation (HPCT), the return to normal blood leukocyte and platelet counts typically occurs within the first month after transplant, with rising blood cell counts of lymphocytes, granulocytes, platelets, and eventually erythrocytes.12 Post-transplant thrombocytopenia can be caused by a variety of reasons, including GVHD, infections (such as cytomegalovirus), immune-mediated factors, drug-related factors (such as ganciclovir and valganciclovir), disease recurrence, and thrombotic microangiopathy.13,14 Historically, post-transplant thrombocytopenia was categorized as either secondary failure of platelet recovery (SFPR) or prolonged isolated thrombocytopenia (PIT).15 PIT is defined as the need for thrombocyte suspension transfusions for more than 60 days following HCT or sufficient engraftment of all peripheral blood lineages, except for platelets, being < 20x109/L. On the other hand, SFPR is defined as losing independence on platelet transfusions for seven straight days after allogeneic HCT with a number of thrombocytes < 20x109/L from over 50x109/L. According to the reports, PIT and SFPR occur in 12–20% and 20–40% of patients, respectively.16 Post-HCT thrombocytopenia and lower initial posttransplant platelets are considered poor prognostic indicators as they reflect poor engraftment, can cause bleeding, and have been associated with higher mortality rates.12,17
There are two basic theories explaining the origin of protracted isolated thrombocytopenia, while the precise etiology is unknown. Anti-platelet autoantibodies, splenic sequestration, or other conditions may cause normal platelets produced by the bone marrow to be prematurely destroyed in the peripheral circulation. Alternately, poor megakaryocyte differentiation may result in insufficient platelet production.18 One study measured glycocalicin index (GCI), a parameter that reflects platelet turn-over, serum thrombopoietin (Tpo) that is inversely proportional to megakaryocytes activity (ie, elevated in aplastic anemia) and circulating B-cells producing anti-GPIIb-IIIa in patients with or without thrombocytopenia post-HCT and patients with aplastic anemia, immune thrombocytopenia, and healthy individuals has found that CGI and Tpo levels in patients with post-HCT thrombocytopenia were similar to patients with aplastic anemia, suggesting a major role of impaired thrombocytosis as a cause of thrombocytopenia,14 with similar conclusions were reported in other study.19 In addition, antiplatelet antibodies were also detected in patients with thrombocytopenia proving the possible role of autoantibodies in the development of post-HCT thrombocytopenia and consistent with other findings in the literature as well.20 These findings conclude a complex, multifactorial pathophysiology behind persistent post-HCT thrombocytopenia that remains not fully understood until now.
Treatment of Idiopathic Post-HCT Thrombocytopenia
Despite the advancements in the practice of HCT, definitive treatment regimens for post-HCT thrombocytopenia have not been established yet. Historically, the mainstay treatment of post-HCT thrombocytopenia was repeated platelets transfusion that has been used during the pancytopenia phase post-HCT, along with other blood products to maintain patients’ blood components.21 Potential morbidities associated with repetitive platelet transfusions include transfusion reactions, platelet alloimmunization, and increased costs.22 As a result, huge efforts were put to decrease the need for platelet transfusions and reduce bleeding complications.
Thrombopoietin and Thrombopoietin Receptors
TpoR also known previously as C-MPL or CD110 was first identified in the early 1990s.23,24 The human TpoR is made up of various components. Its 466 amino acid extracellular portion has two cytokine receptor motifs (CRMs). In addition, there is a transmembrane section made up of 22 amino acids, followed by a cytoplasmic portion consisting of 122 amino acids.25 Of the two extracellular CRMs, it seems that ligand binding occurs at the motif that is furthest from the membrane which also functions as a regulator when in the unbound state, preventing the cytokine receptor motif closest to the membrane from continuously signaling.26
Tpo also known as C-MPL ligand, the glycoprotein composed of 332-amino acid, is the most potent cytokine that physiologically regulates platelet production, produced continuously in the liver and other organs, travels via the bloodstream to the bone marrow where it promotes the early emergence of numerous hematopoietic lineages.27,28 Tpo levels are usually inversely proportional to thrombocytes in the blood and marrow megakaryocyte abundance.29 Regulation of Tpo is thought to involve complex processes, one proposed mechanism is that Tpo is produced continuously and the abundance of platelets that have TpoRs binds, absorbs Tpo, and breaks it down, thus reducing Tpo levels when there is a high platelet count and when the platelet count is low, Tpo is not degraded and increases in the blood.30,31 This model explains states of marrow failure such as aplastic anemia; however, it does not explain the unexpected decrease in Tpo levels in immune thrombocytopenia observed by some studies.32,33 The theory was then adjusted after noticing elevated bone marrow megakaryocytes, which naturally express TpoRs explaining why blood Tpo is decreased in this disorder. Yet, the theory still does not explain the relationship between Tpo production and the abundance of platelets or megakaryocytes in other disorders such as reactive thrombocytosis associated with inflammation, or infection. Multiple factors that might induce increased Tpo levels have been described in the literature highlighting the complexity and multifactorial nature of Tpo regulation.26
First Generation of Thrombopoietic Agents
Two molecules were developed in the early nineties that were found to have a stimulating activity on the thrombopoietic effects. The first was rhTpo, a glycosylated compound manufactured using Chinese hamster ovary (CHO) cells, encompassing the complete native human amino acid sequence. Administration of a sole rhTpo dose led to a rise in platelet count, commencing around the fifth day for the majority of patients and reaching its zenith at an average of day 12.34 Pegylated human recombinant megakaryocyte growth and development factor (PEG-rHuMGDF), a truncated polypeptide Mpl-ligand derivatized with poly-(ethylene glycol), was produced in E-coli and had the first 163 amino acids of the human Tpo in its sequence,35 an induced megakaryocyte endoreduplication and proliferation in vitro and in vivo. Changes in platelet production and function produced by PEG-rHuMGDF returned to baseline within two weeks after discontinuing treatment. Initial studies showed that PEG-rHuMGDF increases platelet production in a linear log-dose-dependent manner by stimulating megakaryocyte endoreduplication and new megakaryocyte formation from marrow hematopoietic progenitors in nonhuman primates.36
Although PEG-rHuMGDF initially showed promise in early clinical trials by being safe and effective at increasing platelet levels, the development of neutralizing antibodies and severe thrombocytopenia in around 8% of exposed patients due to its homology with the native Tpo led to discontinuation of trails in the United States.37,38 On the other side, similar adverse effects were not encountered with the use of rhTpo. Only a single study has reported that a patient tested positive for non-neutralizing transient antibodies to full length which was not associated with any clinical consequences.34 As this finding was not reported elsewhere it did not hinder the clinical development of that potentially beneficial medication that has an array of indications, particularly in China where it was approved for the treatment of chemotherapy-induced thrombocytopenia (CIT).39–41 The use of rhTpo for the treatment of post-HCT thrombocytopenia was investigated by many studies in the past with ongoing efforts to prove its benefits.42 Table 1 summarizes the available studies on the use of rhTpo for the treatment of post-HCT thrombocytopenia treatment. A cross all the reported nine studies that included more than 700 patients, rhTpo was reported to demonstrate a degree of efficacy for promoting platelet recovery after HCT and treatment of platelet engraftment failure.42–51 A trial including 120 patients who underwent allogeneic HCT were randomized to receive rhTpo from day-1 post-transplant revealed a statistically significant cumulative incidence of platelet engraftment was significantly higher in the rhTpo group than in the control group on day-60 post-transplantation (91.7 ± 3.8% vs 74.5 ± 5.8%, P = 0.041) as well as a significantly lower rate of delayed platelet engraftment in the RhTpo group (8.3%, 5/60) than in the control group (23.3%, 14/60) (P = 0.024).46 Another study included a cohort of 24 patients who underwent allogeneic HCT, 20 with DPE and four with SFPR have demonstrated a significant difference in overall response when compared to a historical group as 11 (45.8%) patients in the rhTpo group achieved platelet engraftment after 28 days of treatment versus the historical control group (12.2%, p < 0.001).46
 |
Table 1 Summary of ten Reported Studies on the Use of rhTpo for the Treatment of Post-HCT Thrombocytopenia |
Oprelvekin, a recombinant human interleukin 11 analogs that received the United States food and drug administration (FDA) approval for the prevention of CIT in patients with non-myeloid malignancies after demonstrating modest efficacy as per multiple studies in the literature.41,52 For instance, a meta-analysis demonstrated a reduction in the time needed for platelet counts to reach 50 × 109/L (weighted mean difference [WMD] = −4.19 days; 95% CI: −5.01, −3.37), the time to reach 100 × 109/L (WMD = −4.45 days; 95% CI: −4.85, −4.06), platelet transfusion volume (WMD = −6.14 units; 95% CI: −9.20, −3.09) in patients with acute leukemia patients with CIT.53 Despite the reported benefits of oprelvekin in patients with CIT, the FDA did not recommend oprelvekin following myeloablative chemotherapy due to increased rates of adverse effects such as edema, conjunctival bleeding, hypotension, and tachycardia, in addition to other fatal adverse effects reported in the post-marketing period of the drug. Few studies were conducted in China on the use of oprelvekin for the treatment of patients post-HCT have demonstrated faster platelet recovery time as compared to placebo and have also reported adverse effects associated with the use of oprelvekin.54–56 These adverse effects, along with the high cost of rhIL-11 led the manufacturer to discontinue producing the drug in the United States.57
Second Generation of TpoR Agonists
Second-generation TpoR agonists are short peptide sequences that serve as analogs that activate TpoRs, unlike the first-generation molecules, they have no sequence homology with Tpo, therefore eliminating the dilemma of autoantibodies formation to endogenous Tpo.58 Late in the nineties of the last century, efforts finally discovered a 14-amino acid peptide was among the earliest identified molecules, which was able to bind to and activate the TpoR, with even higher affinity by thousands after it was dimerized.59,60 With covalently linking the tandem peptide dimers with two disulfide-bonded human IgG1 kappa light chains, the stability, and half-life of that molecule were extended, yielding the novel peptide TpoR agonist Romiplostim.58 Romiplostim was approved by the FDA for the treatment of immune thrombocytopenia (ITP) in adults and children aged one and above. Later, another non-peptide TpoR agonists were developed that showed efficacy for the treatment of many thrombocytopenia-related conditions such as eltrombopag that was FDA approved for many conditions such as ITP and refractory aplastic anemia, avatrombopag and lusutrombopag that are FDA approved and hetrombopag that is being under investigation currently. Efforts have been focusing on the promising benefits of these novel drugs for patients with post-HCT platelet engraftment failure and here we highlight the latest evidence for the benefits and adverse effects of utilizing these medications from this aspect. Table 2 provides a summary of all the reported studies on the utility of second-generation TpoR agonist agents.61–114
 |
Table 2 Summary of 54 Studies Done to Assess the Efficacy and Safety of Second-Generation TpoR Agonists for the Treatment of Thrombocytopenia |
Romiplostim (AMG 531, Nplate®, Romiplate®)
Since 1997, the primitive structure of the first molecule that had no sequence homology with Tpo started developing as an anticipated substitute for first-generation TpoR agonists.59 Romiplostim, a peptide TpoR agonist that’s structure was achieved by linking four of the 14-amino-acid peptides to the C-terminus of an IgG1 Fc fragment creating a peptibody. Using polyglycine linkers, two of the four 14-amino-acid peptides were attached to the Fc-gamma chain. The peptibody has functional constant domains (CH2 and CH3) that can bind to the FcRn receptors which internalize it and then release it back into the circulation by exocytosis thus explaining its prolonged half-life.115
Although it is believed that romiplostim has lower affinity than native Tpo, it produces an immediate activation cascade starting with phosphorylation of the receptor and initiation of the JAK2 and STAT5 pathways stimulating CFU-Mk growth and increased megakaryocyte ploidy in a dose-dependent fashion.116 It was approved by the FDA in 2008 for ITP and administered weekly as a subcutaneous injection at a dose of 1 to 10 mcg/kg and also approved for patients with radiation injury-related thrombocytopenia. In addition romiplostim has been tested for patients with chemotherapy-induced thrombocytopenia,117–120 myelodysplastic syndrome with thrombocytopenia,121–123 perioperative thrombocytopenia,124,125 in approved in Japan for thrombocytopenia in aplastic anemia after studies have shown benefit for its use there.126,127
The utility of romiplostim use in patients with thrombocytopenia post-HCT has been questioned in multiple case reports and retrospective case series reported in Table 2.108,110,113,114 The only available prospective trial in this context reported that 18 patients achieved a sustained platelet (>50x 109/L) of 24 patients with delayed platelet engraftment (n = 10) and secondary thrombocytopenia (n = 14) due to either GVHD or infection. In addition, a hemoglobin response was also observed in 21 of 22 patients and a response in neutrophil counts in four patients who had <1000x 109/L before treatment initiation.89 However, spontaneous recovery could not be excluded as the cause of these effects because the study lacked a control group. Another retrospective study included 13 pediatric patients with SFPR (n = 9) and engraftment failure (n = 4) reported platelet transfusion independence after one week of treatment with romiplostim despite a platelet count of <10x109/L before treatment initiation.102 As with other TpoR agonists, the response to romiplostim seems to correlate inversely with low bone marrow functionality reflected by low megakaryocyte counts on bone marrow biopsies, which is thought to explain the cause of resistance to the treatment of romiplostim in some of the reported cases.19,108
Eltrombopag (SB497115, Promacta®, Revolade®)
Eltrombopag is the first non-peptide Tpo agonist identified by using screening strategies of chemical libraries.128 Interestingly, many compounds were found to display bioactivity on TpoRs, Hydrazone compounds were described as thrombopoietin receptor mimetics as they were found to be activating STAT proteins in a Tpo responsive cell line.129 As a member of the bioarylhydrazone class of chemical compounds, eltrombopag has a metal chelate group in the center with an acidic (COOH) group at one end and lipophilic (CH3) groups at the other end.115 In vitro eltrombopag is a highly potent activator of the STAT and MAPK signaling pathways and induces the differentiation of bone marrow precursor cells and proliferation of Tpo-dependent cell lines. In cells expressing other factors other than TpoRs, eltrombopag did not show activity on these cascades highlighting that the activation of JAK/STAT by eltrombopag is due to the specific activation of the Tpo.108 Similar to all nonpeptide TpoR agonists eltrombopag binds to the transmembrane region of the TpoR at the histidine 499 amino acid, therefore it does not compete with Tpo for the binding site and its effects seem to be additive to Tpo in various in vitro experiments.130
In 2008, eltrombopag was initially approved as the first oral agent to increase platelet count and to be used for rare blood disorders, mainly ITP, and later its utility has been expanding after many clinical trials proved its efficacy.131 These approvals were based on evidence from trials on conditions such as aplastic anemia,132–134 and thrombocytopenia due to Hepatitis C-related cirrhosis.135,136 Among the TpoR agonists, eltrombopag is the most studied agent in the context of post-HCT thrombocytopenia with 24 reports of case series and retrospective studies and three published clinical trials including 687 patients (Table 2), as well as few case reports. Collectively, eltrombopag has demonstrated efficacy in raising platelet counts for patients with SFPR or PIT post HCT and decreasing platelet transfusion dependence. A recent trial including 60 patients randomized to receive eltrombopag or placebo demonstrated a statistically significant difference in the rates of achieving platelet count 50,000/µL (the study’s secondary endpoint) despite having a nonsignificant difference between the eltrombopag group and the placebo group at a threshold of 30,000/µL (the study’s primary endpoint) and therefore highlighting the efficacy of eltrombopag in raising platelet counts aside from the spontaneous recovery of platelets.76
On the other side, a prospective single-armed trial analyzed the efficacy of eltrombopag treatment from day one after transplantation until platelet count exceeded 50,000/µL for 14 consecutive days in 12 patients undergoing allogeneic transplantation compared to a historical cohort that concluded no statistically significant between the two groups in regards to partial and complete platelet engraftment.77 Therefore questioning the need for routine administration of anti-TpoR agents for patients undergoing HCT. Eltrombopag was shown to be effective for the treatment of SFPR and DPR, a study on a total of 86 adult patients post HCT, 16 with PT and 71 with SFPR reported overall response for platelet recovery was 72%, including 73% in the SFPR group and 67% in the PT group without a statistical significance between the groups and a longer time to response for patients with PT compared with those with SFPR with a median of 93 days and 60 days respectively.90 Another retrospective study on 46 patients who underwent HCT reported that 23 patients responded to treatment and the cumulative incidence of successful platelet recovery was 48%. The cumulative incidences of platelet recovery were 38% among patients with DPR and 50% among those with SFPR for allogeneic transplantation, respectively.68
Although eltrombopag displayed consistent safety and tolerability in the majority of the studies, few studies reported adverse events that required discontinuation of the drug. Only a single study reported that one of 39 adult patients who received treatment for PGF developed two episodes of grade II deep vein thrombosis.63 Eltrombopag was also associated with transaminitis, a case series on eight adult patients with PGF reported three events of grade two liver enzyme elevations were reported but resolved with conservative treatment.74 Another study on 43 pediatric patients with PIT and SFPR reported liver injury occurred in six children (14%) where transaminases were 2.5 times higher than the normal value or the bilirubin level was twice the normal value, however, treatment was continued.84 Similarly another study reported that five patients out of 38 had similar events.92 Hyperbilirubinemia (grade III) was also reported in six out of 24 patients and was significantly higher in the treatment group of a recent trial.76 However, a study reported that metabolites of eltrombopag interact with the laboratory measurements of bilirubin and therefore cause inaccurate bilirubin measurements.137
Avatrombopag (E5501, AKR-50, YM-477, Doptelet®)
Avatrombopag is a newer non-peptide Tpo memetic and three times more potent than eltrombopag in raising platelet counts.138 Like other non-peptide agents, it has similar pharmacological properties such as being orally available and its binding site at the transmembrane domain that does not compete with endogenous Tpo at its distal domain binding site. The combination of avatrombopag with Tpo increased the number of differentiations of CD34+ to megakaryocytes to about 200% of that generated with Tpo only reflecting the additive properties with endogenous Tpo and its effect to induce differentiation of human stem cells.139 A phase-I clinical trial revealed that avatrombopag caused platelet count to increase after 3–5 days post-administration, with maximum changes of >370 × 109/L over baseline with 20 mg daily after 13–16 days in healthy individuals demonstrating that its effect on platelet counts depended on dose, concentration and treatment duration.131 Avatrombopag induces proliferation of human TpoR-expressing murine Ba/F3 cells in a concentration-dependent manner in in vitro experiments with a maximum activity similar to that of rhTpo activating the downstream signaling cascade through tyrosine phosphorylation of STAT3 and STAT5, and threonine phosphorylation of MAPK (ERK) activating PI3K/AKT and MAPK signaling pathways.140 Similar to eltrombopag, without TpoR no response was noted.141
Avatrombopag was the first drug to be approved for the treatment of thrombocytopenia in cirrhosis patients undergoing elective procedures by the FDA in 2018. Approval was based on large phase II and III clinical trials assessing its clinical utility in this patient population that showed both efficacy and safety.142,143 Further studies have demonstrated similar efficacy of avatrombopag. A phase-II clinical trial on Japanese patients with CLD and thrombocytopenia have illustrated a significant improve in platelet counts as compared to placebo with no marked adverse effects.144 In 2019, the usage of avatrombopag has been expanded to include patients with thrombocytopenia due to ITP that failed to improve with other treatments as clinical trials provided evidence of the overall benefits of avatrombopag which was tolerated and effective for the treatment of chronic ITP.145,146 Recent post-hoc analysis on Phase III trial data by Jurczak et al, 2018 has demonstrated consistent conclusions and highlighted the high durability of response to treatment.147 Moreover, a study on patients with ITP treated with romiplostim or eltrombopag showed that patients achieved very high response rates even in those without initial response following switching to avatrombopag which illustrated the value of switching between TpoR agonists when prior TpoR agonists do not provide adequate effectiveness, convenience, or tolerability and potency of avatrombopag.148 In addition, avatrombopag, when compared to other TpoR agents, has practical oral dosing with a single pill strength as compared to rhTpo, has lower hepatoxicity rates, and does not require dietary restrictions in opposition to eltrombopag that requires to be only taken one to two hours before food for good absorption of the drug and to obtain a baseline liver function tests for starting the medication.149
So far, the utility of avatrombopag for post-HCT thrombocytopenia has been tested in three recent studies including 104 patients only where significant findings emerged. The first study, conducted on 61 patients, highlighted avatrombopag effectiveness, revealing an overall response rate of 68.9% and a complete response rate of 39.3% in patients with SFPR and DPE. Notably, the presence of adequate megakaryocytes prior to treatment was associated with a significantly higher likelihood of achieving both overall and complete responses.65 The second study involving 16 patients focused on avatrombopag combined with mesenchymal stem cells (MSCs). This combination exhibited promising outcomes with 81.3% achieving a complete response, suggesting that this regimen could expedite platelet recovery after transplantation.75 The third study, conducted on 30 pediatric patients with SFPR, PGF, and for promoting engraftment of platelets post-HCT, revealed a notably higher overall response rate (91%) and complete response rate (78%). This study identified different patient groups, distinguishing their response rates based on graft function. Specifically, avatrombopag was significantly more effective in the engraftment-promotion group compared to the PGF/SFPR recovery group. Risk factors such as severe GVHD and inadequate megakaryocytes were associated with reduced complete response rates.64 Importantly, all three studies reported avatrombopag as a well tolerated and potentially effective treatment option for post-HCT thrombocytopenia in adults and children, although the combination with MSCs in one study showed promise but also a severe adverse event leading to mortality most likely related to cytomegalovirus infection.
Lusutrombopag (S-888711, Mulpleta®)
Lusutrombopag was initially identified by Shionogi & Company, Limited, as a non-peptide second-generation TpoR agonist that shares similar pharmacological properties as other non-peptide TpoR agonists such as being orally bioavailable and acting on the transmembrane domain of human TpoRs found in megakaryocytes.150,151 A Trial of multiple studies was conducted to evaluate the impact of food and calcium carbonate on the pharmacokinetics of lusutrombopag in healthy subjects. The results from 48 patients indicated that lusutrombopag exposure remained largely unchanged, with only a minor decrease when taken with food, and there was no significant effect when coadministered with calcium carbonate, suggesting that lusutrombopag administration does not require specific restrictions regarding meals or mineral supplements, unlike eltrombopag.152 Initial and recent trials have demonstrated the efficacy of lusutrombopag for the treatment of cirrhosis Child-Pugh class A and B patients with thrombocytopenia who are planned to undergo surgical or dental procedures.153 Newer trials have addressed cirrhosis patients with Child-Pugh Class C and thrombocytopenia. The analysis of data from multiple studies demonstrated that lusutrombopag effectively increased platelet counts in these patients and was found to be safe and well tolerated, with no treatment-related serious adverse events.154,155 Lusutrombopag was initially approved by the FDA for the treatment of cirrhosis patients with thrombocytopenia who are planned to undergo surgical or dental procedures as well as for patients with ITP. Given the novelty of the drug, its benefits and safety for patients with post-HCT thrombocytopenia or compared to other TpoR agonists have not been examined so far in the literature, although theoretically, it might be a promising option in the future.
Herombopag (Hengqu®)
Herombopag is a second-generation nonpeptide TpoR agonist that was developed first by Jiangsu Hengrui pharmaceutical by structural modification of eltrombopag to improve potency.156 Herombopag has the same mechanism of action as eltrombopag but with greater potency as evidenced by both in vitro and in vivo experiments.157,158 According to the national medical products administration, herombopag has received it is first approval in China as a treatment for chronic ITP that is refractory to immunotherapy and as a conditional approval for the treatment of aplastic anemia.
As a promising treatment option for post-HCT thrombocytopenia, only a single pilot study has tested herombopag for its efficacy in 17 patients who had platelet engraftment failure after HCT as part of acute myelogenous leukemia (AML) population, compared to a matched historical cohort of patients.61 Results from this study showed a statistically significant higher incidence of partial platelet engraftment (PPE – A platelet count exceeding 20,000/μL for seven consecutive days without transfusion) and complete platelet engraftment (CPE – A platelet count exceeding 50,000/μL for seven consecutive days without transfusion) in the herombopag group as compared to placebo group with a median time to PPE and CPE of 13 days (range 8–24), 20 days (range 14–45), respectively. In addition to the demonstrated efficacy, herombopag was well tolerated among the patients with no grade IV adverse effects reported.
Safety and Adverse Events
The safety profile of recombinant rhTpo in treating post-HSCT thrombocytopenia has been questioned across multiple studies. In Nash et al’s 2000 study involving 37 patients, no significant adverse effects were observed, establishing an initial safety baseline for rhTpo. A similar finding was stated by Wolff et al, who reported no serious adverse events or neutralizing antibodies in 33 breast cancer patients treated with rhTpo following high-dose chemotherapy and autologous bone marrow transplantation (ABMT). Subsequent studies, including Lui et al and Han et al, echoed these results, with no significant adverse effects reported in 19 and 120 patients, respectively. Additionally, Wang et al and Song et al both noted the absence of severe adverse events, further reinforcing rhTpo’s safety. Minor adverse events were occasionally reported, such as grade I pain at the injection site (Sun et al, 2019) and localized pain leading to treatment discontinuation in two patients (Tang et al, 2020). Overall, the collective data suggest that rhTpo is generally well tolerated with minimal safety concerns in the context of post-HSCT thrombocytopenia.
Second-generation TpoR agonists, including Eltrombopag, Romiplostim, and Avatrombopag, exhibit varied safety profiles in the management of post-HSCT thrombocytopenia. Eltrombopag has been the most extensively studied with consistent findings supporting its safety and efficacy. Pasvolsky et al conducted a phase 2a trial involving 12 patients, demonstrating a median time to platelet engraftment of 66 days without significant toxicity or dose reductions, even at maximal doses. Yaman et al observed no treatment discontinuations due to adverse events among 18 pediatric patients, highlighting its well-tolerated nature in younger populations. Similarly, Giammarco et al and Gupta et al reported favorable safety profiles with Eltrombopag, noting minimal adverse effects and effective platelet recovery in their respective studies. Although most of the studies reported no significant concerns regarding the safety of eltrombopag, few studies reported adverse effects that in most of the times did not results in treatment discontinuation such as transaminitis,73,74,84,87,90,92,97 hyperbilirubinemia,76,92 thromboembolism, and bone marrow fibrosis.85 Kırcalı et al, 2023 for instance, reported that one patient discontinued eltrombopag treatment because of two consecutive venous thromboembolisms and reported that mild bone marrow fibrosis developed in five patients that was however clinically insignificant. Another study reported that the longer the duration of treatment response, the higher the grade of bone marrow fibrosis was noticed.71 Other nonspecific symptoms such as nausea and vomiting have been reported in few studies.67 Given the current data, these agents generally appear safe and effective in clinical use, supporting their role in managing post-HSCT thrombocytopenia.
Limitations
Despite the promising safety profiles and potential efficacy observed with recombinant thrombopoietin agonists (rhTpo) such as romiplostim, as well as second-generation TpoRas like eltrombopag in treating post-HSCT thrombocytopenia, the existing studies have several notable limitations. Studies investigating rhTpo and second-generation agents frequently suffer from small sample sizes and a lack of control groups, which restricts the applicability of their findings across broader patient populations. Similarly, research on second-generation TpoRas, as highlighted in studies by Nampoothiri et al and Qiu et al, often relies on retrospective analyses involving diverse patient cohorts and varying dosing regimens and till now very few randomized controlled trials have been published. This heterogeneity in study designs, patient demographics and the absence of reported effect sizes complicates direct comparisons and meta-analyses, potentially hiding nuanced safety and efficacy outcomes.
In addition, given the complicated clinical course and the comorbid conditions of most of the patients who undergo HSCT, even the reported adverse effects can be hardly attributed to the use of TPO-Ras. Moreover, the scarcity of long-term safety data for both rhTpo and second-generation TpoRas raises concerns about the emergence of unforeseen adverse events, such as bone marrow fibrosis. These collective limitations emphasize the critical necessity for large-scale, well-designed prospective trials with standardized protocols. Such studies are essential to definitively assess the efficacy, safety profiles, and optimal clinical use of rhTpo and even the newer second-generation TpoRas in the management of post-HSCT thrombocytopenia, which is currently being rarely reported on few occasions that are mostly case reports and case series.
Conclusion
Clinical studies of second-generation TpoR agonists, including romiplostim, eltrombopag, avatrombopag, and herombopag demonstrated promising effectiveness in promoting platelet recovery post-HCT, albeit with variations in response rates. Second-generation TpoR agonists seem to be more convenient than subcutaneous rhTpo as they are orally administered with a reasonable platelet recovery as. Figure 2 shows a simplified flowchart for the suggested use of second-generation TpoR agonists in post-HCT thrombocytopenia. Nevertheless, the overall efficacy and safety of TpoR agonist agents post-HCT necessitate further exploration through larger, well-structured clinical trials to optimize their use and ensure their place in standard clinical practice.
 |
Figure 2 Flowchart illustrating our suggestions for second-generation TpoR agonists use in post-HCT thrombocytopenia. A SFPR definition: losing Independence on platelet transfusions for seven straight days after allogeneic HCT with a number of thrombocytes < 20x109/L from over 50x109/L. PIT definition: the need for thrombocyte suspension transfusions for more than 60 days following HCT or sufficient engraftment of all peripheral blood lineages, except for platelets, being < 20x109/L. BThere is currently no evidence supporting the early use of TpoR agonists to accelerate the recovery of platelet counts. * Regular individualized follow-up including screening, prevention, and counseling for all patients based on the recommendations from the guidelines. ** Investigations are based on clinical suspicion and may include laboratory work-up and histologic confirmation. + Suggested based on the level of evidence from the literature, taking into consideration the availability, costs and pharmacological properties of different agents. #Does not require dietary restriction (versus eltrombopag which is only taken one to two hours before food for good absorption). Abbreviation: HCT, hematopoietic cell transplantation; TpoR, thrombopoietin receptor; GVHD, graft versus host disease; SFPR, secondary failure of platelet recovery; PIT, prolonged isolated thrombocytopenia; LFT, liver function tests; BMB, bone marrow transplant; SC, subcutaneous. |
Abbreviations
aGVHD, acute graft-versus-host disease; AML, acute myelogenous leukemia; cGVHD, chronic graft-versus-host disease; CHO, Chinese hamster ovary; CIT, chemotherapy-induced thrombocytopenia; CPE, complete platelet engraftment; CRMs, cytokine receptor motifs; FDA, food and drug administration; GCI, glycocalicin index; GVHD, graft-versus-host disease; HCT, hematopoietic cell transplantation; HPCT, hematopoietic progenitor cell transplantation; ITP, immune thrombocytopenia; MeSH, medical subject headings; MSCs, mesenchymal stem cells; PEG-rHuMGDF, Pegylated human recombinant megakaryocyte growth and development factor; PIT, prolonged isolated thrombocytopenia; PPE, partial platelet engraftment; rhTpo, recombinant human thrombopoietin; SFPR, secondary failure of platelet recovery; TBI, total body irradiation; Tpo, thrombopoietin; TpoR, thrombopoietin receptor; TpoR, thrombopoietin receptor; WMD, weighted mean difference.
Acknowledgments
This review did not receive any specific grants from funding agencies in the public, commercial, or not-for-profit sectors. We affirm that all authors involved in this manuscript were not precluded from accessing the information used in this study, and we collectively accept responsibility for the submission of this manuscript for publication.
Funding
Open Access funding provided by the Qatar National Library.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Balassa K, Danby R, Rocha V. Haematopoietic stem cell transplants: principles and indications. Br J Hosp Med. 2019;80(1):33–39. doi:10.12968/hmed.2019.80.1.33
2. Thomas E, Storb R, Clift RA, et al. Bone-marrow transplantation (first of two parts). New Engl J Med. 1975;292(16):832–843. doi:10.1056/NEJM197504172921605
3. Sureda A, Bader P, Cesaro S, et al. Indications for allo- and auto-SCT for haematological diseases, solid tumours and immune disorders: current practice in Europe, 2015. Bone Marrow Transplant. 2015;50(8):1037–1056. doi:10.1038/bmt.2015.6
4. Saad A, de Lima M, Anand S, et al. Hematopoietic cell transplantation, version 2.2020, NCCN clinical practice guidelines in oncology. J Nat Compreh Can Netw. 2020;18(5):599–634.
5. Majhail NS. Long-term complications after hematopoietic cell transplantation. Hematol/Oncol Stem Cell Therapy. 2017;10(4):220–227. doi:10.1016/j.hemonc.2017.05.009
6. Weissinger EM, Metzger J, Schleuning M, et al. A multicenter prospective, randomized, placebo-controlled phase II/III trial for preemptive acute graft-versus-host disease therapy. Leukemia. 2021;35(6):1763–1772. doi:10.1038/s41375-020-01059-3
7. Arai S, Arora M, Wang T, et al. Increasing incidence of chronic graft-versus-host disease in allogeneic transplantation: a report from the center for international blood and marrow transplant research. Biol Blood Marr Transplant. 2015;21(2):266–274. doi:10.1016/j.bbmt.2014.10.021
8. Gooley TA, Chien JW, Pergam SA, et al. Reduced mortality after allogeneic hematopoietic-cell transplantation. New Engl J Med. 2010;363(22):2091–2101. doi:10.1056/NEJMoa1004383
9. McDonald GB, Sandmaier BM, Mielcarek M, et al. Survival, nonrelapse mortality, and relapse-related mortality after allogeneic hematopoietic cell transplantation: comparing 2003–2007 versus 2013–2017 cohorts. Ann Internal Med. 2020;172(4):229–239. doi:10.7326/M19-2936
10. Nishiwaki S, Akahoshi Y, Morita-Fujita M, et al. Improvements in allogeneic hematopoietic cell transplantation outcomes for adults with ALL over the past 3 decades. Blood Adv. 2022;6(15):4558–4569. doi:10.1182/bloodadvances.2022008032
11. Penack O, Peczynski C, Mohty M, et al. How much has allogeneic stem cell transplant-related mortality improved since the 1980s? A retrospective analysis from the EBMT. Blood Adv. 2020;4(24):6283–6290. doi:10.1182/bloodadvances.2020003418
12. Ninan MJ, Flowers CR, Roback JD, Arellano ML, Waller EK. Posttransplant thrombopoiesis predicts survival in patients undergoing autologous hematopoietic progenitor cell transplantation. Biol Blood Marr Transplant. 2007;13(8):895–904. doi:10.1016/j.bbmt.2007.04.001
13. Nash RA, Gooley T, Davis C, Appelbaum FR. The problem of thrombocytopenia after hematopoietic stem cell transplantation. Oncologist. 1996;1(6):371–380. doi:10.1634/theoncologist.1-6-371
14. Yamazaki R, Kuwana M, Mori T, et al. Prolonged thrombocytopenia after allogeneic hematopoietic stem cell transplantation: associations with impaired platelet production and increased platelet turnover. Bone Marrow Transplant. 2006;38(5):377–384. doi:10.1038/sj.bmt.1705444
15. First LR, Smith BR, Lipton J, Nathan DG, Parkman R, Rappeport JM. Isolated thrombocytopenia after allogeneic bone marrow transplantation: existence of transient and chronic thrombocytopenic syndromes. Blood. 1985;65(2):368–374. doi:10.1182/blood.V65.2.368.368
16. Bruno B, Gooley T, Sullivan KM, et al. Secondary failure of platelet recovery after hematopoietic stem cell transplantation. Biol Blood Marr Transplant. 2001;7(3):154–162. doi:10.1053/bbmt.2001.v7.pm11302549
17. Zaja F, Geromin A, Patriarca F, et al. Prognostic significance of delayed thrombocytopenia after allogeneic stem cell transplant. Am J Hematol. 2011;86(9):790–792. doi:10.1002/ajh.22086
18. Bielski M, Yomtovian R, Lazarus HM, Rosenthal N. Prolonged isolated thrombocytopenia after hematopoietic stem cell transplantation: morphologic correlation. Bone Marrow Transplant. 1998;22(11):1071–1076. doi:10.1038/sj.bmt.1701499
19. Zhang X, Fu H, Xu L, et al. Prolonged thrombocytopenia following allogeneic hematopoietic stem cell transplantation and its association with a reduction in ploidy and an immaturation of megakaryocytes. Biol Blood Marr Transplant. 2011;17(2):274–280. doi:10.1016/j.bbmt.2010.09.007
20. Sivakumaran M, Hutchinson RM, Pringle H, et al. Thrombocytopenia following autologous bone marrow transplantation: evidence for autoimmune aetiology and B cell clonal involvement. Bone Marrow Transplant. 1995;15(4):531–536.
21. Jekarl DW, Kim JK, Han JH, et al. Transfusion support in hematopoietic stem cell transplantation. Blood Res. 2023;58(S1):S1–s7. doi:10.5045/br.2023.2023004
22. Bernstein SH, Nademanee AP, Vose JM, et al. A multicenter study of platelet recovery and utilization in patients after myeloablative therapy and hematopoietic stem cell transplantation. Blood. 1998;91(9):3509–3517. doi:10.1182/blood.V91.9.3509
23. Souyri M, Vigon I, Penciolelli JF, Heard JM, Tambourin P, Wendling F. A putative truncated cytokine receptor gene transduced by the myeloproliferative leukemia virus immortalizes hematopoietic progenitors. Cell. 1990;63(6):1137–1147. doi:10.1016/0092-8674(90)90410-G
24. Vigon I, Mornon JP, Cocault L, et al. Molecular cloning and characterization of MPL, the human homolog of the v-mpl oncogene: identification of a member of the hematopoietic growth factor receptor superfamily. Proc Natl Acad Sci USA. 1992;89(12):5640–5644. doi:10.1073/pnas.89.12.5640
25. Kaushansky K. Thrombopoietin: a tool for understanding thrombopoiesis. J Thromb Haemost. 2003;1(7):1587–1592. doi:10.1046/j.1538-7836.2003.00273.x
26. Sabath DF, Kaushansky K, Broudy VC. Deletion of the extracellular membrane-distal cytokine receptor homology module of Mpl results in constitutive cell growth and loss of thrombopoietin binding. Blood. 1999;94(1):365–367. doi:10.1182/blood.V94.1.365.413a46_365_367
27. Wendling F. Thrombopoietin: its role from early hematopoiesis to platelet production. Haematologica. 1999;84(2):158–166.
28. Kato T, Matsumoto A, Ogami K, Tahara T, Morita H, Miyazaki H. Native thrombopoietin: structure and function. Stem Cells. 1998;16(5):322–328. doi:10.1002/stem.160322
29. Koike Y, Yoneyama A, Shirai J, et al. Evaluation of thrombopoiesis in thrombocytopenic disorders by simultaneous measurement of reticulated platelets of whole blood and serum thrombopoietin concentrations. Thromb Haemost. 1998;79(6):1106–1110. doi:10.1055/s-0037-1615024
30. Fielder PJ, Gurney AL, Stefanich E, et al. Regulation of thrombopoietin levels by c-mpl-mediated binding to platelets. Blood. 1996;87(6):2154–2161. doi:10.1182/blood.V87.6.2154.bloodjournal8762154
31. Yang C, Li YC, Kuter DJ. The physiological response of thrombopoietin (c-Mpl ligand) to thrombocytopenia in the rat. Br J Haematol. 1999;105(2):478–485.
32. Mukai HY, Kojima H, Todokoro K, et al. Serum thrombopoietin (TPO) levels in patients with amegakaryocytic thrombocytopenia are much higher than those with immune thrombocytopenic purpura. Thromb Haemost. 1996;76(5):675–678. doi:10.1055/s-0038-1650641
33. Nagasawa T, Hasegawa Y, Shimizu S, et al. Serum thrombopoietin level is mainly regulated by megakaryocyte mass rather than platelet mass in human subjects. Br J Haematol. 1998;101(2):242–244. doi:10.1046/j.1365-2141.1998.00683.x
34. Vadhan-Raj S, Murray LJ, Bueso-Ramos C, et al. Stimulation of megakaryocyte and platelet production by a single dose of recombinant human thrombopoietin in patients with cancer. Ann Internal Med. 1997;126(9):673–681. doi:10.7326/0003-4819-126-9-199705010-00001
35. Kuter DJ, Begley CG. Recombinant human thrombopoietin: basic biology and evaluation of clinical studies. Blood. 2002;100(10):3457–3469. doi:10.1182/blood.V100.10.3457
36. Harker LA, Marzec UM, Hunt P, et al. Dose-response effects of pegylated human megakaryocyte growth and development factor on platelet production and function in nonhuman primates. Blood. 1996;88(2):511–521. doi:10.1182/blood.V88.2.511.bloodjournal882511
37. Basser RL, O’Flaherty E, Green M, et al. Development of pancytopenia with neutralizing antibodies to thrombopoietin after multicycle chemotherapy supported by megakaryocyte growth and development factor. Blood. 2002;99(7):2599–2602. doi:10.1182/blood.V99.7.2599
38. Li J, Yang C, Xia Y, et al. Thrombocytopenia caused by the development of antibodies to thrombopoietin. Blood. 2001;98(12):3241–3248. doi:10.1182/blood.V98.12.3241
39. National Library of Medicine. [Consensus on clinical diagnosis, treatment and prevention management of chemotherapy induced thrombocytopenia in China(2018)]. Zhonghua zhong liu za zhi. 2018;40(9):714–720. Polish
40. Al-Samkari H, Soff GA. Clinical challenges and promising therapies for chemotherapy-induced thrombocytopenia. Exp Rev Hematol. 2021;14(5):437–448. doi:10.1080/17474086.2021.1924053
41. Xu Y, Song X, Du F, et al. A randomized controlled study of rhTPO and rhIL-11 for the prophylactic treatment of chemotherapy-induced thrombocytopenia in non-small cell lung cancer. J Cancer. 2018;9(24):4718–4725. doi:10.7150/jca.26690
42. Sun YQ, Kong Y, Zhang XH, et al. A novel recombinant human thrombopoietin for treating prolonged isolated thrombocytopenia after allogeneic stem cell transplantation. Platelets. 2019;30(8):994–1000. doi:10.1080/09537104.2018.1557613
43. Nash RA, Kurzrock R, DiPersio J, et al. A Phase I trial of recombinant human thrombopoietin in patients with delayed platelet recovery after hematopoietic stem cell transplantation. Biol Blood Marr Transplant. 2000;6(1):25–34. doi:10.1016/S1083-8791(00)70049-8
44. Wolff SN, Herzig R, Lynch J, et al. Recombinant human thrombopoietin (rhTPO) after autologous bone marrow transplantation: a phase I pharmacokinetic and pharmacodynamic study. Bone Marrow Transplant. 2001;27(3):261–268. doi:10.1038/sj.bmt.1702772
45. Liu DH, Huang XJ, Liu KY, et al. Safety of recombinant human thrombopoietin in adults after related donor haploidentical haematopoietic stem cell transplantation: a pilot study. Clin Drug Invest. 2011;31(2):135–141. doi:10.1007/BF03256939
46. Han TT, Xu LP, Liu DH, et al. Recombinant human thrombopoietin promotes platelet engraftment after haploidentical hematopoietic stem cell transplantation: a prospective randomized controlled trial. Ann Hematol. 2015;94(1):117–128. doi:10.1007/s00277-014-2158-1
47. Wang H, Huang M, Zhao Y, et al. Recombinant human thrombopoietin promotes platelet engraftment and improves prognosis of patients with myelodysplastic syndromes and aplastic anemia after allogeneic hematopoietic stem cell transplantation. Biol Blood Marr Transplant. 2017;23(10):1678–1684. doi:10.1016/j.bbmt.2017.06.010
48. Song Y, Zhou F, Song NX, et al. Impact on platelet recovery of recombinant human thrombopoietin in severe aplastic anemia patients with allogeneic hematopoietic stem cell transplantation. Zhonghua xue Ye xue Za Zhi. 2018;39(3):207–211.
49. Tang B, Huang L, Liu H, et al. Recombinant human thrombopoietin promotes platelet engraftment after umbilical cord blood transplantation. Blood Adv. 2020;4(16):3829–3839. doi:10.1182/bloodadvances.2020002257
50. Gu J, Liu J, Li X, et al. Recombinant human thrombopoietin improved platelet engraftment after autologous hematopoietic stem cell transplantation in patients with newly diagnosed multiple myeloma. Cancer Med. 2021;10(21):7641–7649. doi:10.1002/cam4.4294
51. Cao Y, Wang M, Shen B, et al. Efficacy of recombinant human thrombopoietin for the treatment of secondary failure of platelet recovery after allogeneic HSCT. Clin Appl Thromb. 2022;28:10760296211068037. doi:10.1177/10760296211068037
52. Tepler I, Elias L, Smith JW, et al. A randomized placebo-controlled trial of recombinant human interleukin-11 in cancer patients with severe thrombocytopenia due to chemotherapy. Blood. 1996;87(9):3607–3614.
53. Liu Z, Wang Y, Yan J, et al. Efficacy and safety of recombinant human interleukin-11 in the treatment of acute leukaemia patients with chemotherapy-induced thrombocytopenia: a systematic review and meta-analysis. J Evaluat Clin Pract. 2020;26(1):262–271. doi:10.1111/jep.13152
54. Li JD, Han XL, Wu S. Effect of recombinant human interleukin 11 on recovery of platelets after peripheral blood hematopoietic stem cell transplantation. Zhongguo shi yan xue ye xue za zhi. 2009;17(1):226–228.
55. Xu XJ, Niu XM, Guo ZW, et al. Effects of recombinant human interleukin 11 on hematological malignancy after allogeneic hematopoietic cell transplantation. Zhonghua Yi xue Za Zhi. 2011;91(2):100–102.
56. Xu YJ, Chen FP, Li XL, Zhao XL, He Q. Effect of recombinant human interleukin 11 on the platelet after hematopoietic stem cell transplantation in patients with leukemia. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2007;32(3):433–436.
57. Cantor SB, Elting LS, Hudson DV, Rubenstein EB. Pharmacoeconomic analysis of oprelvekin (recombinant human interleukin-11) for secondary prophylaxis of thrombocytopenia in solid tumor patients receiving chemotherapy. Cancer. 2003;97(12):3099–3106. doi:10.1002/cncr.11447
58. Hallam S, Provan D, Newland AC. Immune thrombocytopenia – what are the new treatment options? Expert Opin Biol Ther. 2013;13(8):1173–1185. doi:10.1517/14712598.2013.801451
59. Cwirla SE, Balasubramanian P, Duffin DJ, et al. Peptide agonist of the thrombopoietin receptor as potent as the natural cytokine. Science. 1997;276(5319):1696–1699. doi:10.1126/science.276.5319.1696
60. Dower WJ, Cwirla SE, Balasubramanian P, Schatz PJ, Baccanari DP, Barrett RW. Peptide agonists of the thrombopoietin receptor. Stem Cells. 1998;16(2):21–29. doi:10.1002/stem.5530160705
61. Zheng X, Zhang H, Guo W, et al. Herombopag promotes platelet engraftment and decreases platelet transfusion after allogeneic hematopoietic stem cell transplantation. Eur J Haematol. 2023;110(5):527–533. doi:10.1111/ejh.13925
62. Al-Mashdali AF, Gulied A, Bakr MM, Yassin MA. Romiplostim use for thrombocytopenia following allogeneic hematopoietic stem cell transplantation: a case series from a single center in Qatar. Hematology. 2023;28(1):2280872. doi:10.1080/16078454.2023.2280872
63. Kırcalı E, Cengiz Seval G, Öztürk C, et al. Eltrombopag for the treatment of poor graft function following haematopoietic cell transplantation: real-life data. Balkan Med J. 2023;40(1):51–56. doi:10.4274/balkanmedj.galenos.2022.2022-2-48
64. Ruan Y, Cao W, Luo T, et al. Avatrombopag for the treatment of thrombocytopenia in children’s patients following allogeneic hematopoietic stem-cell transplantation: a pilot study. Front Pediat. 2023;11:1099372. doi:10.3389/fped.2023.1099372
65. Zhou M, Qi J, Gu C, et al. Avatrombopag for the treatment of thrombocytopenia post hematopoietic stem-cell transplantation. Therapeut Advan Hematol. 2022;13:20406207221127532. doi:10.1177/20406207221127532
66. Wen B, Zhang X, Chen S, et al. Oral eltrombopag versus subcutaneous recombinant human thrombopoietin for promoting platelet engraftment after allogeneic stem cell transplantation: a prospective, non-inferiority, randomized controlled trial. Hematol Oncol. 2022;40(4):777–786. doi:10.1002/hon.3017
67. Yan F, Lu N, Gu Z, et al. Eltrombopag in the treatment of patients with persistent thrombocytopenia after haploidentical peripheral blood stem cell transplantation: a single-center experience. Ann Hematol. 2022;101(2):397–408. doi:10.1007/s00277-021-04706-6
68. Güven ZT, Çelik S, Eser B, Çetin M, Ünal A, Kaynar L. Eltrombopag for treatment of thrombocytopenia following hematopoietic stem cell transplantation. Turk J Haematol. 2022;39(2):103–108. doi:10.4274/tjh.galenos.2022.2021.0675
69. Karataş A, Göker H, Demiroğlu H, et al. Efficacy of eltrombopag in thrombocytopenia after hematopoietic stem celltransplantation. Turk J Med Sci. 2022;52(2):413–419. doi:10.55730/1300-0144.5328
70. Samarkandi H, Al Nahedh M, Alfattani A, et al. Evaluation of eltrombopag in thrombocytopenia post hematopoietic cell transplantation: rertrospective observational trial. Hematol/Oncol Stem Cell Therapy. 2022;15(1):285–290. doi:10.1016/j.hemonc.2020.07.006
71. Bostankolu Değirmenci B, Yegin ZA, Dikyar A, et al. Eltrombopag may induce bone marrow fibrosis in allogeneic hematopoietic stem cell transplant recipients with prolonged thrombocytopenia. Leukemia Res. 2022;118:106870. doi:10.1016/j.leukres.2022.106870
72. Bortolotti M, Pettine L, Zaninoni A, Croci GA, Barcellini W, Fattizzo B. Efficacy and immunomodulating properties of eltrombopag in aplastic anemia following autologous stem cell transplant: case report and review of the literature. Pharmaceuticals. 2022;15(4). doi:10.3390/ph15040419
73. Matsumoto M, Terada K, Tsuchimochi T, Takahashi S, Noguchi Y, Igarashi S. Efficacy of eltrombopag in children with post-stem cell transplant prolonged isolated thrombocytopenia. Hematol Rep. 2022;14(3):240–244. doi:10.3390/hematolrep14030033
74. Ahn HJ, Byun JM, Kim I, et al. Eltrombopag for post-transplant poor graft function in East Asian patients. J Korean Med Sci. 2022;37(6):e48. doi:10.3346/jkms.2022.37.e48
75. Zhu L, Liu J, Kong P, et al. Analysis of the efficacy and safety of avatrombopag combined with MSCs for the treatment of thrombocytopenia after allogeneic hematopoietic stem cell transplantation. Front Immunol. 2022;13:910893. doi:10.3389/fimmu.2022.910893
76. Ahmed S, Bashir Q, Bassett R, et al. Eltrombopag for post-transplantation thrombocytopenia: results of phase II randomized, double-blind, placebo-controlled trial. Transplantat Cell Ther. 2021;27(5):
77. Pasvolsky O, Shargian L, Rozovski U, et al. Eltrombopag for enhancement of platelet engraftment in patients undergoing allogeneic cord blood transplantation. Leukemia Lymphoma. 2021;62(11):2747–2754. doi:10.1080/10428194.2021.1929957
78. Yaman Y, Elli M, Şahin Ş, et al. Eltrombopag for treatment of thrombocytopenia after allogeneic hematopoietic cell transplantation in children: single-centre experience. Pediat Transplant. 2021;25(5):e13962. doi:10.1111/petr.13962
79. Giammarco S, Sica S, Chiusolo P, et al. Eltrombopag for the treatment of poor graft function following allogeneic stem cell transplant: a retrospective multicenter study. Int j Hematol. 2021;114(2):228–234. doi:10.1007/s12185-021-03153-3
80. Gupta AK, Srinivasan P, Das G, Meena JP, Tanwar P, Seth R. Eltrombopag post autologous hematopoietic stem cell transplant - an emerging indication in younger pediatric patients. Am J Blood Res. 2021;11(2):168–171.
81. Uria-Oficialdegui ML, Alonso L, Benitez-Carabante MI, Renedo B, Oliveras M, Diaz-de-Heredia C. Use of eltrombopag for the treatment of poor graft function after hematopoietic stem cell transplantation in children. Pediat Transplant. 2021;25(4):e14010. doi:10.1111/petr.14010
82. Nampoothiri RV, Ho L, McEwan C, et al. Efficacy and cost analysis of eltrombopag in thrombocytopenia and poor graft function post allogeneic hematopoietic cell transplantation. Bone Marrow Transplant. 2021;56(10):2471–2476. doi:10.1038/s41409-021-01362-2
83. Liu S, Que LP, Huang K, et al. Eltrombopag for thrombocytopenia in 24 children after hematopoietic stem cell transplantation. Zhonghua er ke za zhi. 2021;59(4):311–315. doi:10.3760/cma.j.cn112140-20200715-00727
84. Qiu KY, Liao XY, Huang K, et al. Eltrombopag as first-line treatment for thrombocytopenia among paediatric patients after allogeneic haematopoietic stem cell transplantation. Br J Clin Pharmacol. 2021;87(4):2023–2031. doi:10.1111/bcp.14607
85. Lancman G, Coltoff A, Steinberg A. Romiplostim for thrombocytopenia following allogeneic stem cell transplantation: a case series. Hematol/Oncol Stem Cell Therapy. 2020;13(3):171–174. doi:10.1016/j.hemonc.2018.07.002
86. Aydin S, Dellacasa C, Manetta S, et al. Rescue treatment with eltrombopag in refractory cytopenias after allogeneic stem cell transplantation. Therapeut Advan Hematol. 2020;11:2040620720961910. doi:10.1177/2040620720961910
87. Masetti R, Vendemini F, Quarello P, et al. Eltrombopag for thrombocytopenia following allogeneic hematopoietic stem cell transplantation in children. Pediatr Blood Cancer. 2020;67(5):e28208. doi:10.1002/pbc.28208
88. Gao F, Zhou X, Shi J, et al. Eltrombopag treatment promotes platelet recovery and reduces platelet transfusion for patients with post-transplantation thrombocytopenia. Ann Hematol. 2020;99(11):2679–2687. doi:10.1007/s00277-020-04106-2
89. Peffault de Latour R, Chevret S, Ruggeri AL, et al. Romiplostim in patients undergoing hematopoietic stem cell transplantation: results of a Phase 1/2 multicenter trial. Blood. 2020;135(3):227–229. doi:10.1182/blood.2019000358
90. Bento L, Bastida JM, García-Cadenas I, et al. Thrombopoietin receptor agonists for severe thrombocytopenia after allogeneic stem cell transplantation: experience of the Spanish group of hematopoietic stem cell transplant. Biol Blood Marr Transplant. 2019;25(9):1825–1831. doi:10.1016/j.bbmt.2019.05.023
91. Li S, Wu R, Wang B, et al. Eltrombopag for delayed platelet recovery and secondary thrombocytopenia following allogeneic stem cell transplantation in children. J Pediat Hematol. 2019;41(1):38–41. doi:10.1097/MPH.0000000000001263
92. Fu H, Zhang X, Han T, et al. Eltrombopag is an effective and safe therapy for refractory thrombocytopenia after haploidentical hematopoietic stem cell transplantation. Bone Marrow Transplant. 2019;54(8):1310–1318. doi:10.1038/s41409-019-0435-2
93. Marotta S, Marano L, Ricci P, et al. Eltrombopag for post-transplant cytopenias due to poor graft function. Bone Marrow Transplant. 2019;54(8):1346–1353. doi:10.1038/s41409-019-0442-3
94. Yuan C, Boyd AM, Nelson J, et al. Eltrombopag for treating thrombocytopenia after allogeneic stem cell transplantation. Biol Blood Marr Transplant. 2019;25(7):1320–1324. doi:10.1016/j.bbmt.2019.01.027
95. Rivera D, Bastida JM, Lopez-Corral L, et al. Usefulness of eltrombopag for treating thrombocytopenia after allogeneic stem cell transplantation. Bone Marrow Transplant. 2019;54(5):757–761.
96. Tang C, Chen F, Kong D, et al. Successful treatment of secondary poor graft function post allogeneic hematopoietic stem cell transplantation with eltrombopag. J Hematol Oncol. 2018;11(1):103. doi:10.1186/s13045-018-0649-6
97. Bosch-Vilaseca A, García-Cadenas I, Roldán E, et al. Usefulness of thrombopoietin receptor agonists for persistent clinically relevant thrombocytopenia after allogeneic stem cell transplantation. Eur J Haematol. 2018;101(3):407–414. doi:10.1111/ejh.13132
98. Master S, Dwary A, Mansour R, Mills GM, Koshy N. Use of eltrombopag in improving poor graft function after allogeneic hematopoietic stem cell transplantation. Case Rep Oncol. 2018;11(1):191–195. doi:10.1159/000487229
99. Hartranft ME, Clemmons AB, DeRemer DL, Kota V. Evaluation of romiplostim for the treatment of secondary failure of platelet recovery among allogeneic hematopoietic stem cell transplant patients. J Oncol Pharm Pract. 2017;23(1):10–17. doi:10.1177/1078155215612240
100. Ali S, Gassas A, Kirby-Allen M, Krueger J, Ali M, Schechter T. Eltrombopag for secondary failure of platelet recovery post-allogeneic hematopoietic stem cell transplant in children. Pediat Transplant. 2017;21(6). doi:10.1111/petr.13017
101. Tanaka T, Inamoto Y, Yamashita T, et al. Eltrombopag for Treatment of Thrombocytopenia after Allogeneic Hematopoietic Cell Transplantation. Biol Blood Marr Transplant. 2016;22(5):919–924. doi:10.1016/j.bbmt.2016.01.018
102. Maximova N, Zanon D, Rovere F, Maestro A, Schillani G, Paparazzo R. Romiplostim for secondary thrombocytopenia following allogeneic stem cell transplantation in children. Int j Hematol. 2015;102(5):626–632. doi:10.1007/s12185-015-1821-1
103. Raut SS, Shah SA, Sharanangat VV, et al. Safety and efficacy of eltrombopag in post-hematopoietic stem cell transplantation (HSCT) thrombocytopenia. Ind J Hematol Blood Transf. 2015;31(4):413–415. doi:10.1007/s12288-014-0491-0
104. Fujimi A, Kamihara Y, Hashimoto A, et al. Identification of anti-thrombopoietin receptor antibody in prolonged thrombocytopenia after allogeneic hematopoietic stem cell transplantation treated successfully with eltrombopag. Int j Hematol. 2015;102(4):471–476. doi:10.1007/s12185-015-1806-0
105. Battipaglia G, Ruggeri A, Brissot E, et al. Safety and feasibility of romiplostim treatment for patients with persistent thrombocytopenia after allogeneic stem cell transplantation. Bone Marrow Transplant. 2015;50(12):1574–1577. doi:10.1038/bmt.2015.182
106. Buchbinder D, Hsieh L, Mahajerin A, Puthenveetil G, Soni A, Nugent D. Successful treatment of secondary graft failure following unrelated cord blood transplant with hematopoietic growth factors in a pediatric patient with Fanconi anemia. Pediat Transplant. 2015;19(7):E181–184. doi:10.1111/petr.12564
107. Buchbinder D, Hsieh L, Krance R, Nugent DJ. Successful treatment of post-transplant thrombocytopenia with romiplostim in a pediatric patient with X-linked chronic granulomatous disease. Pediat Transplant. 2014;18(7):E252–254. doi:10.1111/petr.12325
108. DeRemer DL, Katsanevas K, Bradley A, Awan FT. Romiplostim resistance in secondary failure of platelet recovery. J Oncol Pharm Pract. 2013;19(4):369–372. doi:10.1177/1078155212469640
109. Poon LM, Di Stasi A, Popat U, Champlin RE, Ciurea SO. Romiplostim for delayed platelet recovery and secondary thrombocytopenia following allogeneic stem cell transplantation. Am J Blood Res. 2013;3(3):260–264.
110. Bollag RJ, Sterett M, Reding MT, Key NS, Cohn CS, Ustun C. Response of complex immune-mediated thrombocytopenia to romiplostim in the setting of allogeneic stem cell transplantation for chronic myelogenous leukemia. Eur J Haematol. 2012;89(4):361–364. doi:10.1111/j.1600-0609.2012.01832.x
111. Reid R, Bennett JM, Becker M, et al. Use of eltrombopag, a thrombopoietin receptor agonist, in post-transplantation thrombocytopenia. Am J Hematol. 2012;87(7):743–745. doi:10.1002/ajh.23225
112. Calmettes C, Vigouroux S, Tabrizi R, Milpied N. Romiplostim (AMG531, Nplate) for secondary failure of platelet recovery after allo-SCT. Bone Marrow Transplant. 2011;46(12):1587–1589. doi:10.1038/bmt.2011.179
113. Gangatharan SA, Cooney JP. Persistent thrombocytopenia post auto-SCT for AML treated with romiplostim in a patient with HIV. Bone Marrow Transplant. 2011;46(9):1280–1281. doi:10.1038/bmt.2010.298
114. Beck JC, Burke MJ, Tolar J. Response of refractory immune thrombocytopenia after bone marrow transplantation to romiplostim. Pediatr Blood Cancer. 2010;54(3):490–491. doi:10.1002/pbc.22332
115. Kuter DJ. Biology and chemistry of thrombopoietic agents. Semin hematol. 2010;47(3):243–248. doi:10.1053/j.seminhematol.2010.02.005
116. Broudy VC, Lin NL. AMG531 stimulates megakaryopoiesis in vitro by binding to Mpl. Cytokine. 2004;25(2):52–60. doi:10.1016/j.cyto.2003.05.001
117. Al-Samkari H, Marshall AL, Goodarzi K, Kuter DJ. The use of romiplostim in treating chemotherapy-induced thrombocytopenia in patients with solid tumors. Haematologica. 2018;103(4):e169–e172. doi:10.3324/haematol.2017.180166
118. Al-Samkari H, Parnes AD, Goodarzi K, Weitzman JI, Connors JM, Kuter DJ. A multicenter study of romiplostim for chemotherapy-induced thrombocytopenia in solid tumors and hematologic malignancies. Haematologica. 2021;106(4):1148–1157. doi:10.3324/haematol.2020.251900
119. Parameswaran R, Lunning M, Mantha S, et al. Romiplostim for management of chemotherapy-induced thrombocytopenia. Support Care Can. 2014;22(5):1217–1222. doi:10.1007/s00520-013-2074-2
120. Soff GA, Miao Y, Bendheim G, et al. Romiplostim Treatment of Chemotherapy-Induced Thrombocytopenia. J Clin Oncol. 2019;37(31):2892–2898. doi:10.1200/JCO.18.01931
121. Fenaux P, Muus P, Kantarjian H, et al. Romiplostim monotherapy in thrombocytopenic patients with myelodysplastic syndromes: long-term safety and efficacy. Br J Haematol. 2017;178(6):906–913. doi:10.1111/bjh.14792
122. Kantarjian H, Fenaux P, Sekeres MA, et al. Safety and efficacy of romiplostim in patients with lower-risk myelodysplastic syndrome and thrombocytopenia. J Clin Oncol. 2010;28(3):437–444. doi:10.1200/JCO.2009.24.7999
123. Sekeres MA, Kantarjian H, Fenaux P, et al. Subcutaneous or intravenous administration of romiplostim in thrombocytopenic patients with lower risk myelodysplastic syndromes. Cancer. 2011;117(5):992–1000. doi:10.1002/cncr.25545
124. Al-Samkari H, Marshall AL, Goodarzi K, Kuter DJ. Romiplostim for the management of perioperative thrombocytopenia. Br J Haematol. 2018;182(1):106–113. doi:10.1111/bjh.15280
125. Marshall AL, Goodarzi K, Kuter DJ. Romiplostim in the management of the thrombocytopenic surgical patient. Transfusion. 2015;55(10):2505–2510. doi:10.1111/trf.13181
126. Jang JH, Tomiyama Y, Miyazaki K, et al. Efficacy and safety of romiplostim in refractory aplastic anaemia: a Phase II/III, multicentre, open-label study. Br J Haematol. 2021;192(1):190–199. doi:10.1111/bjh.17190
127. Lee JW, Lee SE, Jung CW, et al. Romiplostim in patients with refractory aplastic anaemia previously treated with immunosuppressive therapy: a dose-finding and long-term treatment phase 2 trial. Lancet Haematol. 2019;6(11):e562–e572. doi:10.1016/S2352-3026(19)30153-X
128. Erickson-Miller CL, Delorme E, Tian SS, et al. Preclinical activity of eltrombopag (SB-497115), an oral, nonpeptide thrombopoietin receptor agonist. Stem Cells. 2009;27(2):424–430. doi:10.1634/stemcells.2008-0366
129. Duffy KJ, Darcy MG, Delorme E, et al. Hydrazinonaphthalene and azonaphthalene thrombopoietin mimics are nonpeptidyl promoters of megakaryocytopoiesis. J Med Chem. 2001;44(22):3730–3745. doi:10.1021/jm010283l
130. Yamane N, Tanaka Y, Ohyabu N, et al. Characterization of novel non-peptide thrombopoietin mimetics, their species specificity and the activation mechanism of the thrombopoietin receptor. Eur J Pharmacol. 2008;586(1–3):44–51. doi:10.1016/j.ejphar.2008.02.060
131. Cheng G, Saleh MN, Marcher C, et al. Eltrombopag for management of chronic immune thrombocytopenia (RAISE): a 6-month, randomised, Phase 3 study. Lancet. 2011;377(9763):393–402. doi:10.1016/S0140-6736(10)60959-2
132. Desmond R, Townsley DM, Dumitriu B, et al. Eltrombopag restores trilineage hematopoiesis in refractory severe aplastic anemia that can be sustained on discontinuation of drug. Blood. 2014;123(12):1818–1825. doi:10.1182/blood-2013-10-534743
133. Olnes MJ, Scheinberg P, Calvo KR, et al. Eltrombopag and improved hematopoiesis in refractory aplastic anemia. New Engl J Med. 2012;367(1):11–19. doi:10.1056/NEJMoa1200931
134. Yamazaki H, Ohta K, Iida H, et al. Hematologic recovery induced by eltrombopag in Japanese patients with aplastic anemia refractory or intolerant to immunosuppressive therapy. Int j Hematol. 2019;110(2):187–196. doi:10.1007/s12185-019-02683-1
135. Afdhal NH, Dusheiko GM, Giannini EG, et al. Eltrombopag increases platelet numbers in thrombocytopenic patients with HCV infection and cirrhosis, allowing for effective antiviral therapy. Gastroenterology. 2014;146(2):442–452.e441. doi:10.1053/j.gastro.2013.10.012
136. McHutchison JG, Dusheiko G, Shiffman ML, et al. Eltrombopag for thrombocytopenia in patients with cirrhosis associated with hepatitis C. New Engl J Med. 2007;357(22):2227–2236. doi:10.1056/NEJMoa073255
137. Cheng THT, Tsui TKC, Kwok JSS, et al. Comprehensive characterization and resolution of discrepant spectrophotometric bilirubin results in patients on eltrombopag therapy. Clin Chem Lab Med. 2020;58(10):1713–1723. doi:10.1515/cclm-2019-0684
138. Kuter DJ, Allen LF. Avatrombopag, an oral thrombopoietin receptor agonist: results of two double-blind, dose-rising, placebo-controlled Phase 1 studies. Br J Haematol. 2018;183(3):466–478. doi:10.1111/bjh.15574
139. Fukushima-Shintani M, Suzuki K, Iwatsuki Y, et al. AKR-501 (YM477) in combination with thrombopoietin enhances human megakaryocytopoiesis. Exp Hematol. 2008;36(10):1337–1342. doi:10.1016/j.exphem.2008.04.020
140. Markham A. Avatrombopag: a Review in Thrombocytopenia. Drugs. 2021;81(16):1905–1913. doi:10.1007/s40265-021-01613-y
141. Fukushima-Shintani M, Suzuki K, Iwatsuki Y, et al. AKR-501 (YM477) a novel orally-active thrombopoietin receptor agonist. Eur J Haematol. 2009;82(4):247–254. doi:10.1111/j.1600-0609.2008.01198.x
142. Terrault N, Chen YC, Izumi N, et al. Avatrombopag before procedures reduces need for platelet transfusion in patients with chronic liver disease and thrombocytopenia. Gastroenterology. 2018;155(3):705–718. doi:10.1053/j.gastro.2018.05.025
143. Terrault NA, Hassanein T, Howell CD, et al. Phase II study of avatrombopag in thrombocytopenic patients with cirrhosis undergoing an elective procedure. J Hepatol. 2014;61(6):1253–1259. doi:10.1016/j.jhep.2014.07.007
144. Eguchi Y, Takahashi H, Mappa S, Santagostino E. Phase 2 study of avatrombopag in Japanese patients with chronic liver disease and thrombocytopenia. Hepatol Res. 2022;52(4):371–380. doi:10.1111/hepr.13755
145. Bussel JB, Kuter DJ, Aledort LM, et al. A randomized trial of avatrombopag, an investigational thrombopoietin-receptor agonist, in persistent and chronic immune thrombocytopenia. Blood. 2014;123(25):3887–3894. doi:10.1182/blood-2013-07-514398
146. Jurczak W, Chojnowski K, Mayer J, et al. Phase 3 randomised study of avatrombopag, a novel thrombopoietin receptor agonist for the treatment of chronic immune thrombocytopenia. Br J Haematol. 2018;183(3):479–490. doi:10.1111/bjh.15573
147. Jain S, Gernsheimer T, Kolodny S, Bernheisel C, Vredenburg M, Panch SR. Additional efficacy analysis of avatrombopag phase III data for the treatment of adults with immune thrombocytopenia. Platelets. 2023;34(1):2195016. doi:10.1080/09537104.2023.2195016
148. Al-Samkari H, Jiang D, Gernsheimer T, et al. Adults with immune thrombocytopenia who switched to avatrombopag following prior treatment with eltrombopag or romiplostim: a multicentre US study. Br J Haematol. 2022;197(3):359–366. doi:10.1111/bjh.18081
149. Song AB, Al-Samkari H. An updated evaluation of avatrombopag for the treatment of chronic immune thrombocytopenia. Exp Rev Clin Immunol. 2022;18(8):783–791. doi:10.1080/1744666X.2022.2098119
150. Katsube T, Ishibashi T, Kano T, Wajima T. Population pharmacokinetic and pharmacodynamic modeling of lusutrombopag, a newly developed oral thrombopoietin receptor agonist, in healthy subjects. Clin Pharmacokinet. 2016;55(11):1423–1433. doi:10.1007/s40262-016-0411-6
151. Kim ES. Lusutrombopag: first Global Approval. Drugs. 2016;76(1):155–158. doi:10.1007/s40265-015-0525-4
152. Katsube T, Wajima T, Fukuhara T, Kano T. Effects of food and calcium carbonate on the pharmacokinetics of lusutrombopag, a novel thrombopoietin receptor agonist. Clin Ther. 2019;41(9):1747–1754.e1742. doi:10.1016/j.clinthera.2019.06.004
153. Peck-Radosavljevic M, Simon K, Iacobellis A, et al. Lusutrombopag for the treatment of thrombocytopenia in patients with chronic liver disease undergoing invasive procedures (L-PLUS 2). Hepatology. 2019;70(4):1336–1348. doi:10.1002/hep.30561
154. Alkhouri N, Imawari M, Izumi N, et al. Lusutrombopag is safe and efficacious for treatment of thrombocytopenia in patients with and without hepatocellular carcinoma. Clin Gastroenterol Hepatol. 2020;18(11):2600–2608.e2601. doi:10.1016/j.cgh.2020.03.032
155. Flamm SL, Peck-Radosavljevic M, Fukuhara T, et al. Pharmacokinetic assessment and treatment effect of lusutrombopag in Child-Pugh class c patients: review of patient data from two clinical studies and post-marketing surveillance. Advan Therap. 2022;39(9):4285–4298. doi:10.1007/s12325-022-02237-8
156. Syed YY. Hetrombopag: first Approval. Drugs. 2021;81(13):1581–1585. doi:10.1007/s40265-021-01575-1
157. Xie C, Zhao H, Bao X, Fu H, Lou L. Pharmacological characterization of hetrombopag, a novel orally active human thrombopoietin receptor agonist. J Cell & Mol Med. 2018;22(11):5367–5377. doi:10.1111/jcmm.13809
158. Zheng L, Liang MZ, Zeng XL, et al. Safety, pharmacokinetics and pharmacodynamics of hetrombopag olamine, a novel TPO-R agonist, in healthy individuals. Basic Clin Physiol Pharmacol. 2017;121(5):414–422. doi:10.1111/bcpt.12815
 © 2024 The Author(s). This work is published by Dove Medical Press Limited, and licensed under a
Creative Commons Attribution License.
The full terms of the License are available at http://creativecommons.org/licenses/by/4.0/.
The license permits unrestricted use, distribution, and reproduction in any medium, provided the
original author and source are credited.
© 2024 The Author(s). This work is published by Dove Medical Press Limited, and licensed under a
Creative Commons Attribution License.
The full terms of the License are available at http://creativecommons.org/licenses/by/4.0/.
The license permits unrestricted use, distribution, and reproduction in any medium, provided the
original author and source are credited.