Back to Journals » Infection and Drug Resistance » Volume 19
Thrombomodulin as a Potentially Complementing Diagnostic Tool in Non-Pneumonic Bacterial Infections
Authors Friedrich K ![]() , Hübner A
, Hübner A ![]() , Galtung N
, Galtung N ![]() , Hecke B, Kappert K
, Hecke B, Kappert K ![]() , Bauer W
, Bauer W ![]()
Received 8 December 2025
Accepted for publication 9 March 2026
Published 1 April 2026 Volume 2026:19 587368
DOI https://doi.org/10.2147/IDR.S587368
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Sandip Patil
Katharina Friedrich,1 Aurelia Hübner,2 Noa Galtung,2 Britta Hecke,1 Kai Kappert,1,3,4 Wolfgang Bauer2
1Institute of Diagnostic Laboratory Medicine, Clinical Chemistry and Pathobiochemistry, Charité – Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Berlin, Germany; 2Department of Emergency Medicine, Charité – Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Berlin, Germany; 3German Center for Cardiovascular Research (DZHK), Partner Site Berlin, Berlin, Germany; 4Department of Laboratory Medicine and Toxicology, Labor Berlin – Charité Vivantes GmbH, Berlin, Germany
Correspondence: Wolfgang Bauer, Department of Emergency Medicine, Charité – Universitätsmedizin Berlin, corporate member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Hindenburgdamm 30, Berlin, 12203, Germany, Tel +49 030 450 552 897, Email [email protected]
Objective: Soluble thrombomodulin (TM) has been proposed as an endothelial injury marker with potential diagnostic value, particularly for severe pneumococcal community-acquired pneumonia (CAP). Its validation could enable clinically meaningful patient stratification and support biomarker-guided therapy. This retrospective study evaluated the associations between serum TM levels and disease severity/origin in 80 patients with suspected acute infection.
Methods: Serum TM concentrations were measured in patients presenting to the emergency department and adjudicated by an expert panel as pneumococcal CAP, non-pneumococcal CAP, other bacterial infections (non-pneumonic), viral pneumonia, or patients with clinically ruled-out infection (controls).
Results: TM levels did not differ significantly between CAP patients and controls or those with other bacterial infections. However, highest TM concentrations were observed in patients with bacterial infections without pneumonia, significantly exceeding control levels. TM levels were not correlated with disease severity in CAP, determined by National Early Warning Score 2 (NEWS2), but were significantly elevated in non-pneumonic bacterial infections of moderate severity (NEWS2 5– 6).
Conclusion: In this cohort, TM was elevated in bacterial non-pneumonic infections but was not a specific marker for pneumococcal CAP. These findings indicate that TM predominantly reflects systemic endothelial injury, a hallmark of more severe bacterial infections, particularly those of non-pneumonic origin.
Keywords: thrombomodulin, community-acquired pneumonia, severity of CAP, pneumococcal pneumonia, bacterial infections
Introduction
Soluble thrombomodulin (TM) is a biomarker of endothelial dysfunction and injury1,2 and potentially plays a role in the pathophysiology of sepsis, infectious and other inflammatory conditions.3,4 Proteolytic cleavage of membrane-bound TM on endothelial cell surfaces leads to the release of soluble TM into the circulation.2 Further, several preclinical studies in experimental sepsis models suggest the therapeutic potential of TM, as the administration of soluble TM can improve coagulopathy, dampen inflammatory responses, and mitigate organ dysfunction.3 In addition, TM values were shown to correlate with disseminated intravascular coagulation.5 It has also been proposed as a potentially valuable tool for assessing the severity and etiology of bacterial community-acquired pneumonia (CAP).6 A recent prospective study by Alpkvist et al explored the diagnostic potential of TM in plasma and sputum for CAP with a focus on pneumococcal infections, hypothesizing that elevated plasma TM reflects endothelial injury and correlates with severe disease.7 Given the global burden of CAP and the need for improved prognostic tools, particularly in high-risk populations, the authors’ hypothesis addresses a clinically relevant gap. The finding that elevated plasma TM correlates with severity only in pneumococcal infection, while intriguing, raises questions about its generalizability to other pathogens and infection sites. Biomarkers such as procalcitonin (PCT), C-reactive protein (CRP), and other endothelial markers have established roles in CAP. In this regard, Yin et al demonstrated in an observational study composed of 573 patients with confirmed CAP that TM had a better ability to predict 30-day mortality than PCT and CRP did.6 Given that CAP etiologies vary globally and often include atypical or viral pathogens, the scope of applicability is limited. Furthermore, non-pneumococcal bacterial infections, whether in the lung or other sites, as well as non-infectious conditions, may influence circulating TM levels. However, to establish TM as a reliable biomarker specifically for pneumococcal CAP, studies require inclusion of both healthy control groups and non-pneumonic bacterial infections. Thus, in this study, we analyzed serum TM from patients enrolled in studies on bacterial infection and sepsis8,9 to test whether elevated TM is associated specifically with pneumococcal CAP when compared with non-pneumococcal pneumonia, non-pneumonic bacterial infections, and non-infected controls.
Materials and Methods
Patients
Patients with and without suspected acute infection were enrolled in prospective observational studies on bacterial infection and sepsis at emergency department presentation.8,9 On the basis of clinical, radiological, laboratory, and microbiological data, two experts adjudicated each case as pneumococcal pneumonia, non-pneumococcal pneumonia, non-pneumonic bacterial infection, viral pneumonia, or no infection (controls). Pneumococcal pneumonia requires (1) adjudicated bacterial or bacterial‒viral coinfection, (2) positive urinary pneumococcal antigen, and (3) radiological infiltration (chest X-ray or computed tomography (CT)). Non-pneumococcal pneumonia patients fulfilled the same criteria but had a negative antigen test; monoviral pneumonia patients were excluded from the bacterial pneumonia groups. Non-pneumonic bacterial infections were defined as bacterial or bacterial‒viral coinfection without pulmonary infiltration, whereas patients without any infection served as controls. Patient severity was evaluated via the National Early Warning Score 2 (NEWS2), which integrates vital parameters to quantify the degree of physiological derangement.10
Sample Collection
Serum was collected during initial routine sampling, processed in 9 mL gel tubes by centrifugation (3000 × g, 10 min), and stored at −80 °C. All participants underwent routine diagnostic testing for infectious disease workup, including urine and blood cultures and a polymerase chain reaction (PCR) panel for 22 respiratory pathogens. Diagnostic laboratory measurements were done by Labor Berlin – Charité Vivantes GmbH under routine conditions.
ELISA Measurement of Serum Thrombomodulin
Serum thrombomodulin was quantified by enzyme-linked immunosorbent assay (ELISA) using the human thrombomodulin/BDCA-3 Quantikine ELISA kit (R&D Systems, #DTHBD0) according to the manufacturer’s instructions. Serum samples were diluted 1:10, and standards ranging from 62.5 to 4000 pg/mL were prepared from reconstituted human thrombomodulin. Assays were performed in 96-well plates (Greiner Bio-One, #655101). Per well, 100 µL assay diluent RD1X was added, followed by 50 µL of serum or standard sample and incubation for 2 h at room temperature. After four washing steps, 200 µL of human thrombomodulin conjugate was added per well and incubated for 2 h at room temperature. Wells were washed four times and incubated with 200 µL substrate solution for 30 min in the dark. The reaction was stopped by adding 50 µL stop solution per well, and absorbance was measured at 450 nm with reference at 570 nm using an Infinite® 200 Pro microplate reader (Tecan).
Statistical Analysis
Statistical analysis was performed via Prism GraphPad 10 (GraphPad Software Inc). To compare more than two groups, the Kruskal‒Wallis test for non-parametric samples with Dunn’s multiple comparison test was employed. For grouped analyses, two-way ANOVA with Holm‒Šídák’s multiple comparisons test was performed. Due to small cohort size, only statistical results of groups with ≥ 3 patients are shown. For correlation analyses, nonparametric two-tailed Spearman correlation was employed. Statistical significance was considered as *p ≤ 0.05; **p < 0.01; ***p < 0.001; ****p < 0.0001.
Results
Within this real-life, heterogeneous cohort of 80 patients presenting to the emergency department with or without suspected acute infection, we identified 17 cases (median age 77, 65% female) of confirmed pneumococcal pneumonia. Serum TM concentrations were measured in these patients, as well as in 9 patients (median age 77, 33% female) with non-pneumococcal bacterial pneumonia, 14 with non-pneumonic bacterial infections (median age 86, 43% female), 2 with viral pneumonia (median age 42.5, 100% female), and 38 patients (median age 71.5, 61% female) were enrolled as healthy controls or with initially suspected but ultimately excluded infection (Table 1). A moderate positive correlation was observed between age and TM levels (Spearman’s r = 0.4; p < 0.0001).
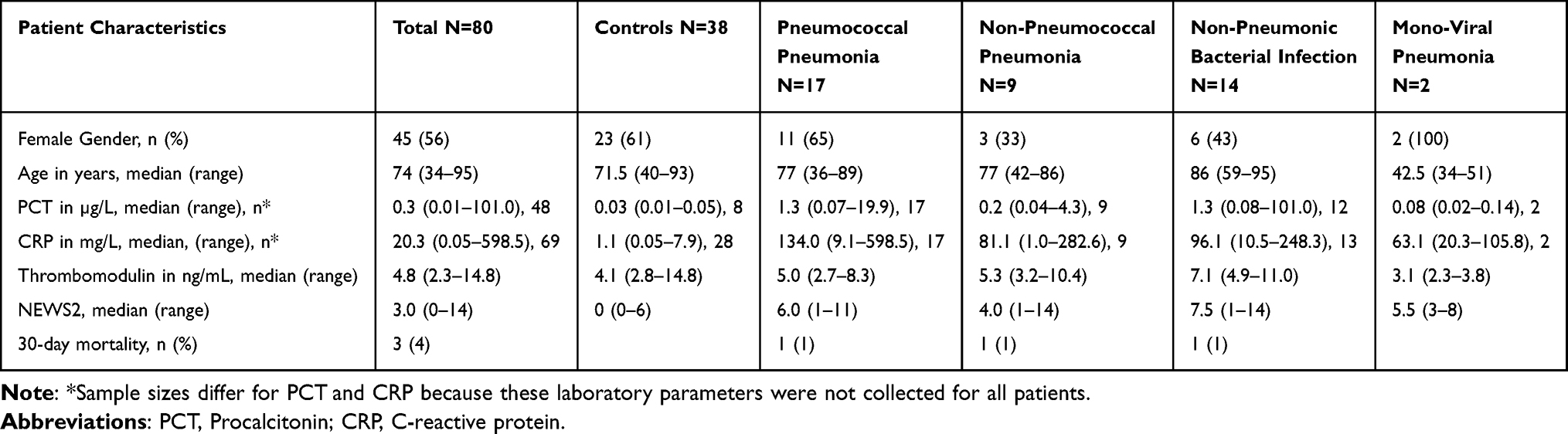 |
Table 1 Characteristics of the Study Population |
As shown in Figure 1, the median serum TM level was 5.0 ng/mL (range 2.7–8.3) in pneumococcal CAP patients and 5.3 ng/mL (range 3.2–10.4) in non-pneumococcal CAP. Patients with other bacterial infections had a median concentration of 7.1 ng/mL (range, 4.9–11.0 ng/mL), indicating that there was no diagnostic distinction between different bacterial infections. In patients with ruled-out infection, TM levels averaged 4.8 ng/mL (range 2.8–14.8), which was not significantly different from CAP, regardless of pneumococcal etiology. Notably, TM levels in non-pneumonic bacterial infections were significantly higher than those in controls (p<0.0001).
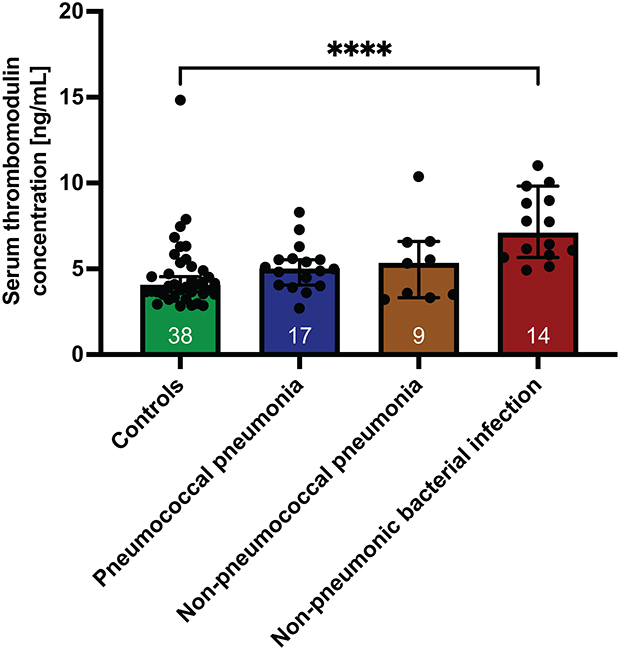 |
Figure 1 Serum thrombomodulin in pneumococcal and non-pneumococcal CAP and non-pneumonic bacterial infection. TM levels of patients with no acute infection (controls, green), pneumococcal pneumonia (blue), non-pneumococcal pneumonia (orange), and non-pneumonic bacterial infection (red). The bars indicate the medians with 95% confidence intervals, and the patient numbers are shown at the bottom of each bar; ****p < 0.0001. |
Next, we examined whether TM levels were correlated with clinical risk, as defined by the NEWS2 (Figure 2). No significant differences were detected among patients at low (NEWS2 0–4), medium (NEWS2 5–6), or high (NEWS2 ≥7) clinical risk within the pneumococcal pneumonia, non-pneumococcal pneumonia, or non-pneumonic bacterial infection groups. Interestingly, within the medium-risk category, patients with non-pneumonic bacterial infections presented with significantly higher TM levels than did those with pneumococcal pneumonia.
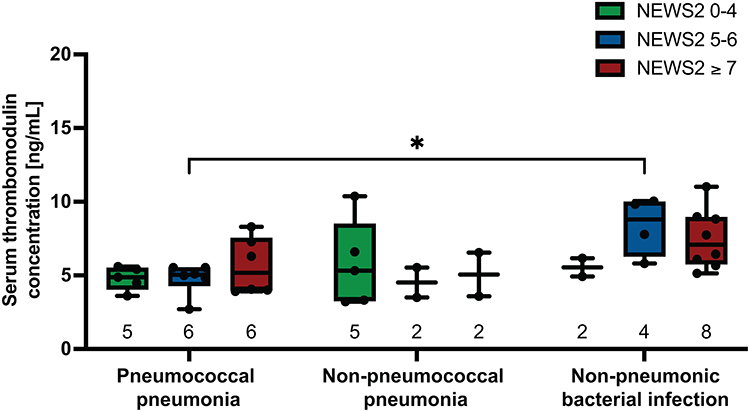 |
Figure 2 Serum thrombomodulin concentrations by clinical risk category. Serum TM levels in patients with low (NEWS2 0–4, green), medium (NEWS2 5–6, blue) and high clinical risk (NEWS2 ≥7, red). Box plots show the interquartile range with a median line, and whiskers indicate minimum and maximum values. Patient numbers are shown below each box; *p < 0.05. |
Interestingly, the correlations between TM and the established clinical NEWS2 as well as between TM and the parameters PCT and CRP, all three of which are used for the diagnosis and monitoring of infection, inflammation and sepsis, were overall moderate (Figure 3). Spearman correlation coefficient ranged from r = 0.3 for TM and NEWS2 (p = 0.008), r = 0.36 for TM and CRP (p = 0.003), and r = 0.51 for TM and PCT compared to r values ranging between 0.52–0.60 comparing standard scores and parameters with each other (Figure 3).
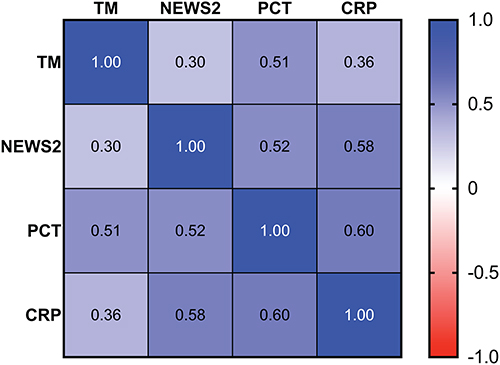 |
Figure 3 Correlation matrix of thrombomodulin, NEWS2, and infection biomarkers. Matrix of Spearman correlation coefficients between the measured soluble TM levels and NEWS2 and standard laboratory biomarkers procalcitonin (PCT) and C-reactive protein (CRP). |
We further assessed the association between TM levels and CAP severity according to the IDSA/ATS guidelines (data not shown). Severe pneumococcal pneumonia had the highest median TM concentration (6.3 ng/mL) compared with non-severe pneumococcal pneumonia (4.9 ng/mL), non-severe non-pneumococcal pneumonia (5.3 ng/mL) and severe non-pneumococcal pneumonia (5.1 ng/mL); however, these differences were not statistically significant.
Discussion
Thrombomodulin (TM) represents an interesting potential biomarker for endothelial activation in bacterial infections. Earlier studies, eg, those of Alpkvist et al and Yin et al, offered valuable and novel contributions by identifying soluble TM as a potentially powerful biomarker for severe (pneumococcal) CAP and opened important avenues for biomarker-guided management of CAP.6,7 In our analysis, we additionally examined a cohort of patients with bacterial infections other than pneumonia. TM levels were not significantly higher in patients with pneumococcal pneumonia than in healthy controls. There was no significant difference in TM concentrations between pneumococcal pneumonia, other bacterial pneumonias, and non-pneumonic bacterial infections. This might be due to low cohort size. Another reason could be that TM levels do not primarily depend on pathogen type or infection site but on other factors, eg. disease severity, comorbidities, age, or epigenetics. Indeed, we found moderate correlation of TM levels with age, disease severity and the infection biomarkers CRP and PCT. Highest correlation was found with PCT, which is a biomarker used for supporting diagnosis and monitoring of severe bacterial infections and sepsis.11 Notably, patients with non-pneumonic bacterial infections, characterized also by higher NEWS2, presented with even higher TM levels than did those with bacterial pneumonias. Within the CAP group, no correlation was observed between TM levels and clinical severity, either in pneumococcal or non-pneumococcal pneumonias.
Conclusions
In conclusion, our findings do not support the notion that TM is a reliable marker for pneumococcal pneumonia in general. It should be highlighted, however, that the limited number of severe CAP cases in our study represents a constraint and warrants cautious interpretation of severity data. These data contrast with the findings of Alpkvist et al, who demonstrated that TM values were specifically correlated with disease severity in pneumococcal pneumonia patients. Thus, further independent studies with larger cohorts are needed to clarify these observations.
The elevated TM levels in patients with moderately severe non-pneumonic bacterial infections indicate, that TM might reflect generalized endothelial injury, as reported in systemic inflammatory states such as sepsis.12 However, larger cohort studies are required before this conclusion can be fully drawn. To realize its clinical potential, future studies must address generalizability, comparative performance, and real-world applicability before recommending TM measurement in routine care.
Abbreviations
TM, Thrombomodulin; CAP, Community-acquired pneumonia; NEWS2, National Early Warning Score 2; PCT, Procalcitonin; CRP, C-reactive protein; CT, Computed tomography; PCR, Polymerase chain reaction; ELISA, Enzyme-linked immunosorbent assay; IDSA/ATS, Infectious Diseases Society of America/ American Thoracic Society.
Data Sharing Statement
The raw data (deidentified participant data) can be obtained upon reasonable request from the corresponding author.
Ethics Approval and Informed Consent
The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). The study was approved by the ethics committee of the Charité – Universitätsmedizin Berlin (EA2/044/20, EA4/167/18 and EA1/107/23) and registered with the German Clinical Trials Register (ID: DRKS00020521 (registered 13/05/2020) and DRKS00017395 (registered 30/09/2019). Informed consent was obtained from all individuals included in this study or their legal guardians or wards.
Acknowledgments
We thank the staff at the emergency department at Campus Benjamin Franklin at Charité – Universitätsmedizin Berlin for their contribution to this study and all participating patients for their support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was conducted without external funding.
Disclosure
Dr Katharina Friedrich reports grants from Investitionsbank Berlin (10209032, 10210792), during the conduct of the study. Prof. Dr. Kai Kappert reports grants from Deutsche Forschungsgemeinschaft / DFG (KA 1820/9-1 and KA 1820/10-1), Senate Department for Urban Mobility, Transport, Climate Action and the Environment, Federal Ministry of Research, Technology and Space (01DK22004B), and Investitionsbank Berlin (10209032, 10210792), outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Conway EM. Thrombomodulin and its role in inflammation. Semin Immunopathol. 2012;34(1):107–6. doi:10.1007/s00281-011-0282-8
2. Boron M, Hauzer-Martin T, Keil J, Sun XL. Circulating thrombomodulin: release mechanisms, measurements, and levels in diseases and medical procedures. TH Open. 2022;6(3):e194–e212. doi:10.1055/a-1801-2055
3. Levi M, Van Der Poll T. Thrombomodulin in sepsis. Minerva Anestesiol. 2013;79(3):294–298.
4. Zhou X, Luo J, Liang X, et al. Plasma thrombomodulin as a candidate biomarker for the diagnosis and prognosis of HBV-related acute-on-chronic liver failure. Infect Drug Resist. 2024;17:1185–1198. doi:10.2147/IDR.S437926
5. Chang P, Sun M, Song H, et al. Study on the predictive value of MASP-1 combined with four thrombotic molecular markers for disseminated intravascular coagulation in patients with severe infection. Infect Drug Resist. 2025;18:5567–5576. doi:10.2147/IDR.S543075
6. Yin Q, Liu B, Chen Y, Zhao Y, Li C. Soluble thrombomodulin to evaluate the severity and outcome of community-acquired pneumonia. Inflammation. 2014;37(4):1271–1279. doi:10.1007/s10753-014-9854-9
7. Alpkvist H, Athlin S, Norrby-Teglund A, Stralin K. Diagnostic and prognostic potential of plasma and sputum thrombomodulin in bacterial community-acquired pneumonia. Infect Dis. 2025;57:1078–87.
8. Diehl-Wiesenecker E, Galtung N, Dickescheid J, et al. Blood calprotectin as a biomarker for infection and sepsis - the prospective CASCADE trial. BMC Infect Dis. 2024;24(1):496. doi:10.1186/s12879-024-09394-x
9. Bauer W, Kappert K, Galtung N, et al. A novel 29-messenger RNA host-response assay from whole blood accurately identifies bacterial and viral infections in patients presenting to the emergency department with suspected infections: a prospective observational study. Crit Care Med. 2021;49(10):1664–1673. doi:10.1097/CCM.0000000000005119
10. Physicians RCo: national Early Warning Score (NEWS) 2: standardising the assessment of acute-illness severity in the NHS. 2017.
11. Maves RC, Enwezor CH. Uses of procalcitonin as a biomarker in critical care medicine. Infect Dis Clin North Am. 2022;36(4):897–909. doi:10.1016/j.idc.2022.07.004
12. Nguyen VT, Nguyen-Phan HN, Hoang BB. Serum thrombomodulin level can predict mortality in patients with sepsis? Med Arch. 2023;77(6):433–439. doi:10.5455/medarh.2023.77.433-439
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.