Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Thoughts on Developing an Early Warning Model for Hospital Violence Risk Events Using Geographic Information Systems
Received 23 September 2025
Accepted for publication 29 December 2025
Published 10 January 2026 Volume 2026:19 569538
DOI https://doi.org/10.2147/JMDH.S569538
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Linda Yoder
Guochen Chen, Chunlei Li
School of Criminology, People’s Public Security University of China, Beijing, People’s Republic of China
Correspondence: Chunlei Li, School of Criminology, People’s Public Security University of China, No. 1 Muxidi Nanli, Xicheng District, Beijing, 100038, People’s Republic of China, Email [email protected]
Abstract: The risk of violence faced by healthcare workers is a widespread challenge in the global healthcare industry. This article examines the feasibility and practical value of developing a spatial prediction and early warning model for hospital violent injury incidents using Geographic Information System(GIS) technology. By integrating multi-source spatiotemporal data and employing spatiotemporal analysis, machine learning, and spatial interpolation methods, the model can identify hotspots and predict the risk of violent events at a micro scale, shifting from passive response to proactive prevention and control. This study not only offers a novel approach for the refined and scientific management of hospital safety but also provides valuable insights for the development of smart hospitals, the application of artificial intelligence, and interdisciplinary integration. Although challenges remain in data integration, privacy protection, and model generalization, advancements in technology and management optimization are expected to establish this technology as a core tool for security prevention and control in smart hospitals. This study is a preliminary exploration in this field.
Keywords: violence against healthcare workers, geographic information system, hospital safety protection, risk warning model
Introduction
Violence against healthcare workers is a global public health and safety concern.1 The risks of violence encountered by medical staff in healthcare settings have drawn considerable international scholarly attention. Most existing studies emphasize the distribution of violent incidents across hospital departments, the influence of healthcare workers’ perceptions of violence on medical practices, and the evaluation of violent behaviors in the healthcare sector.2–4 The risk of workplace violence(WPV) experienced by healthcare workers worldwide has garnered significant attention from scholars. Research in Singapore indicates that WPV has been increasing recently, with verbal and physical abuse being the primary concerns.5 The risk of violence faced by healthcare workers in the United States is higher than average, prompting calls for the country to adopt national strategies, including legislation, to reduce the occurrence of violent incidents.6 In Nepal, research on violence against healthcare workers has revealed that this issue is caught in a vicious cycle. To explain this, researchers have proposed a system dynamics model of violence.7 Studies from countries such as Saudi Arabia and Italy have shown that WPV has become a significant public health and safety issue in the healthcare sector.8,9 Additionally, WPV can negatively affect the physical and mental health, job satisfaction, and fatigue levels of medical staff.10,11 Although these studies contribute to post-incident management from sociological, criminological, and psychological perspectives, they generally lack a proactive focus on pre-incident early warning.
A Geographic Information System (GIS) is an integrated technical framework for spatial data collection, storage, management, analysis, and visualization. Its main advantage lies in combining geographic locations with diverse attribute data to uncover distribution patterns, relationships, and changes through spatial correlations, thereby providing scientific support for decision-making.12 At present, GIS has been widely applied in urban public safety management—such as crime hotspot mapping and crime prediction—alongside environmental governance, ecological conservation, and broader spatial governance. In South Korea, GIS is utilized to enhance the development of safe cities by optimizing the patrol routes of urban security personnel through the analysis of safety facility locations, crime data, and vulnerable areas within the city.13 Based on GIS models, extreme events such as natural disasters can be assessed and predicted, enabling the development of improved emergency evacuation plans and risk mitigation strategies.14 In other countries and regions, GIS has played a vital role in ecological environment security monitoring,15 natural environment protection,16 and risk warning assessment.17 These applications clearly demonstrate the significant advantages of GIS in early warning systems.
However, the application of GIS in internal hospital security, particularly for micro-scale violence risk early warning, remains limited and exploratory. Conventional hospital security systems primarily rely on access control, video surveillance, and intrusion alarms.18,19 These measures mainly serve recording and post-incident investigation purposes and do not fully exploit the potential of the spatial data they generate. It is entirely possible to integrate these spatial data with GIS technology and leverage its advantages in processing spatial data for risk warning.
It is therefore feasible to develop a spatially predictive early warning model for violence against healthcare workers by leveraging GIS predictive capabilities and integrating hospital-related big data, both internal and external. The extensive use of GIS technology significantly enhances the decision-making capabilities of hospital management departments in addressing WPV. Its spatiotemporal modeling technology can process multi-source heterogeneous data; however, it also has certain limitations.20 It depends heavily on the completeness of historical observation data, and large-scale spatiotemporal analyses require high-performance computing power, resulting in relatively high initial investment costs.
This model conceptualizes the hospital as a complex micro-geographic environment, mining data from past violent incidents involving healthcare staff. By combining spatiotemporal analysis and statistical modeling techniques with hospital spatial data—such as departmental layouts, patient flow, and waiting environments—the model can reveal intrinsic links between violent incidents and hospital spaces, identify high-risk areas and time periods, and enable precise and dynamic risk forecasting. Ultimately, this approach strengthens the proactive defense capacity of hospital public safety systems.
Methods
The framework for constructing an early warning model proposed in this study is derived from the integration and innovation of methods across multiple fields, including public safety spatial early warning, environmental criminology, and hospital management. The model construction follows systematic steps to ensure its scientific rigor, operability, and verifiability.
This research does not require approval from an institutional review board or ethics committee. The reason is that the warning model presented in the manuscript is purely a theoretical design and discussion, and does not involve real-world data. The data used for the heatmap are entirely from simulations of the model, intended to demonstrate its usability. Future research, when the model is applied in practice, will require approval from an ethics committee and will comply with data privacy policies. Therefore, for the current research, an ethics committee review report is not necessary.
The construction of the early warning model consisted of four steps: data collection and integration, spatiotemporal analysis and modeling, model development and validation, and system integration and testing.
Step 1 - Multi-Source Data Collection and Integration
The first step involved collecting data from both within and around the hospital. The internal data encompass five key aspects: 1. A historical database of violence against healthcare workers. This database records details such as the timing, department or room number, type of incident, information about the individuals involved, and the sequence of events for each case of violence. 2. Detailed spatial and geographic information of the hospital. GIS coordinates and spatial relationships of key locations—including various departments, consultation rooms, corridors, entrances and exits, nursing stations, waiting areas, and pharmacies—are obtained through Building Information Modeling. 3. Real-time dynamic data of the hospital. This includes time-specific registration volumes, patient queuing times, crowd density heatmaps in waiting areas, and real-time locations of security personnel on patrol. 4. Early-warning indicators for doctor-patient disputes. These include patient complaint records, medical dispute mediation cases, and identification of high-risk patients with a history of violence. 5. Healthcare staff workload data. Key metrics for assessing workplace pressure—such as doctor-to-nurse ratios, working hours, and patient-to-nurse ratios across departments—are extracted from the Hospital Information System.
The peripheral data consist of three components: 1. Medical-related police incident data, which include medical-related alarm records from police departments. These records require geocoding and correlation with police dispatch times and handling outcomes. 2. Environmental data, encompassing population density around the hospital (recommended to be defined within a 500–1000 meter buffer zone outside the hospital’s physical boundary, adjustable based on hospital size and urban context), day and night pedestrian and vehicular flow, and traffic congestion indices. 3. Socio-economic data, obtained from publicly available government sources, providing indicators such as average income levels and unemployment rates in surrounding communities.
Data Cleaning and Preprocessing. All collected raw data underwent rigorous processing, which primarily involved the following five steps: 1. Standardization and Formatting. This step unified time formats, coordinate systems, and data units across all datasets. 2. Geocoding. Non-spatial address information was converted into spatial coordinates using address-matching techniques. 3. Handling Outliers and Missing Values. Statistical methods were employed to identify, correct, or remove outliers. For randomly missing data, mean imputation was applied, while spatially missing data was designated for subsequent spatial interpolation. 4. Spatiotemporal Alignment. Data from diverse sources with varying sampling frequencies were integrated by interpolating or aggregating them into consistent spatiotemporal grid units, such as 15-minute intervals combined with departmental zones. 5. Privacy Protection. All personally identifiable information, including patient IDs and healthcare staff names, was anonymized prior to data integration.
All data were subjected to rigorous cleaning, geocoding, and standardized preprocessing before integration into a unified spatiotemporal database. The data collection approach for Step-1 is illustrated in Figure 1.
 |
Figure 1 Step 1 – Multi-Source Data Collection and Integration: Brief Architecture Diagram. |
Step 2 - Spatiotemporal Analysis and Spatial Modeling
Based on the constructed spatiotemporal database, multi-level spatial analyses were conducted to identify patterns of violent incidents against medical personnel. For spatiotemporal pattern recognition, Spatiotemporal Point Process (STPP) models and Kernel Density Estimation (KDE) were applied to analyze the clustering of historical incidents, producing hotspot maps to visually highlight high-risk areas. For event risk factor analysis, spatial regression models, such as Geographically Weighted Regression (GWR), were employed to quantify the localized effects of various environmental and operational variables on the probability of violence occurrence. Independent variables included department functional type (eg, emergency room, pediatrics), real-time crowd density, average queuing time, distance to nursing stations, healthcare staff workload index, and surrounding environmental complexity. This step aimed to elucidate key risk-driving factors and their spatial heterogeneity.
The methods and models used for data modeling in Step 2, along with the data analysis goals to be achieved, are illustrated in Figure 2.
 |
Figure 2 Step 2 – Spatiotemporal Analysis and Spatial Modeling: Methods and Concepts. |
Step 3 - Predictive Model Development and Validation
Machine learning algorithms, such as Random Forest, were used to construct predictive models for violence probability, incorporating the extracted risk factors as feature variables. By integrating temporal cycles (eg, weekday peak hours) with spatial units, the model generated fine-grained predictions of risks associated with specific times and locations. For areas with monitoring blind spots, spatial interpolation techniques such as Kriging were employed to provide reasonable estimates, ensuring continuity across the prediction surface.
Specifically, the model takes the feature data of spatiotemporal grid cells as input and outputs the probability of violence risk for each cell over a specified future period. To address data monitoring blind spots, the Kriging spatial interpolation method is employed to generate a continuous risk probability surface through reasonable estimation. Next, using techniques such as time-based cross-validation, the historical data is divided into training and testing sets, and the model’s predictive performance is evaluated using metrics including accuracy, precision, recall, F1 score, and the area under the ROC curve. Finally, to enhance the model’s generalizability, a calibration framework must be established. When applied to a new hospital, it is necessary to connect to the hospital’s local data source and use its historical data to recalibrate the model’s key parameters. This involves adjusting the weights of environmental variables or incorporating new localized features based on the hospital’s architectural layout, departmental configuration, and characteristics of its service population. The content discussed in Step 3 is primarily illustrated in Figure 3.
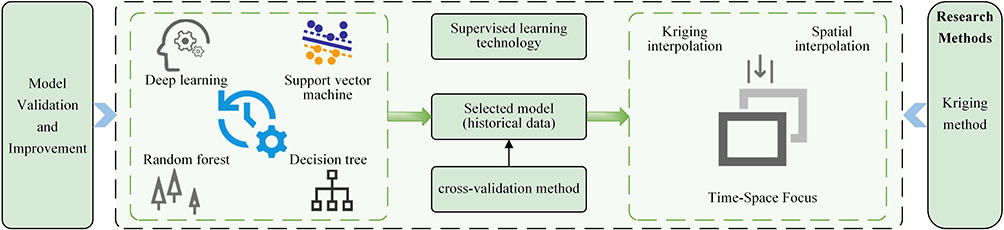 |
Figure 3 Step 3 – Schematic Diagram of Predictive Model Development Technology and Goals. |
Step 4 - System Integration and Testing
The validated predictive model was encapsulated and developed into an integrated early warning platform. The development and implementation process comprised three key phases.
1. System Functionality Implementation. The platform features a visually interactive interface that displays hospital-wide real-time and predicted risk distributions using dynamic heatmaps. It supports drill-down queries by department and time period. We simulated and generated a spatial heatmap visualizing the distribution of hospital violence risk, as shown in Figure 4. The system allows configuration of risk thresholds, enabling high, medium, and low-level early warnings. Alert messages are automatically sent to the security command center and relevant department heads via the hospital’s internal communication system when triggered.
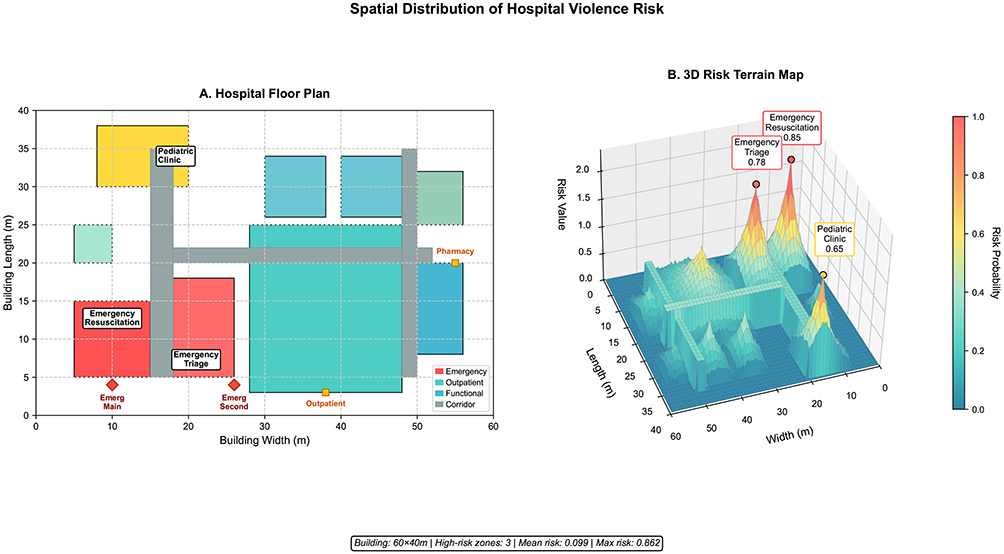 |
Figure 4 Spatial visualization of the distribution of hospital violence risk. Notes: (A) Flat View of Violence Risk Distribution in the Hospital. (B) 3D Visualization Hotspot Map of Violence Risk Distribution. |
*Image caption. (A) Planar layout of the hospital floor showing departmental distribution, corridors, and access points. Emergency areas are highlighted in red, outpatient areas in teal, and functional areas in blue. Emergency entrances are marked with red diamonds, with corresponding labels clearly positioned below each marker. (B) Three-dimensional terrain map of violence risk probability, where elevation represents risk values (0–1) and the color gradient indicates risk intensity from low (blue) to high (red). Three distinct risk peaks are observed: E-Resus (0.85, top-left), E-Triage (0.78, bottom-right), and Pediatric Clinic (0.65, top-center). Labels are vertically offset to ensure clarity, using abbreviated names for emergency departments to avoid clutter. The color bar is positioned with adequate spacing from the main plot to improve readability. The coordinate system represents building dimensions in meters.*
2. Pilot Implementation and Validation. One or two representative hospitals were selected for pilot deployment. The implementation was led by the Hospital Safety Management Committee, with joint participation from the Information Technology and Security Departments. Throughout the pilot phase, active collaboration with police departments was emphasized to gather practical experience and collect feedback. Their assessments of risk scenarios and suggestions for optimizing the alert response workflow were incorporated into system refinements.
3. Iterative System Optimization. During the pilot phase, data on the system’s warning accuracy, response timeliness, and end-user feedback were systematically collected. Based on this information, continuous adjustments were made to model features, algorithm parameters, and system functionalities. This iterative process ensured that the platform remained closely aligned with the hospital’s practical safety operation needs.
The concept of system integration in Step 4 is illustrated in Figure 5. PGIS in the figure stands for the Police Geographic Information System. The future model should be designed to be embedded within the mobile policing app, creating a compact platform that police officers and public safety personnel can access at any time.
 |
Figure 5 Step 4 – System Integration and Testing: Brief Diagram. |
The four steps outlined above introduce specific research methods and models. Since each method and model has its own advantages and disadvantages in practical research,21–23 they should be integrated organically into the model proposed in this study to complement one another and address potential issues of unsuitability in practical applications. To better illustrate the fundamental principles and interrelationships of each method and model, Table 1 is provided to enhance readability.
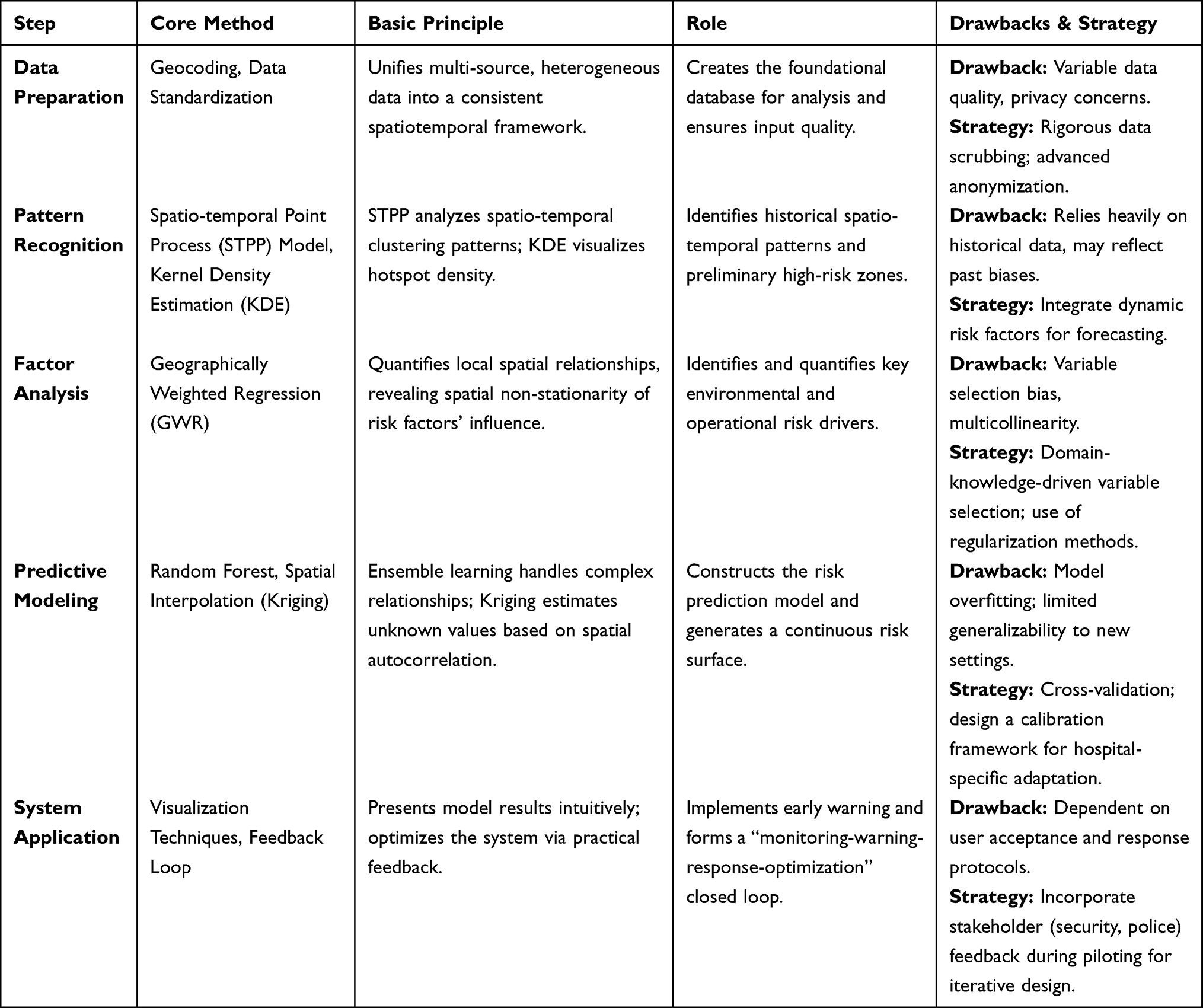 |
Table 1 Key Methods, Principles, and Interrelationships in the Early Warning Model |
Data Privacy, Security, and Ethical Standards
This study involves sensitive medical and personal behavioral data, requiring strict adherence to ethical research standards. Before deploying the model, the following prerequisites must be met.
1. Anonymization Techniques: All direct personal identifiers will be permanently deleted before data integration. For quasi-identifiers (eg, combinations of age and department), k-anonymity techniques will be applied to ensure that no single record can be distinguished from at least k-1 other records in the dataset. For data queries related to aggregate statistics or model training, differential privacy techniques will be explored. By adding calibrated noise, this approach aims to maximize data utility while protecting individual privacy.
2. Data Security Protocols: All data will be stored in encrypted databases within the hospital, protected by strict, layered access controls. Only authorized researchers and security management personnel, authenticated through two-factor authentication, will have access to the de-identified analytical data. Data sharing will occur only in aggregated forms or as derived indicators that have undergone rigorous privacy processing.
3. Regulatory Compliance. The data processing protocols for this study are designed to strictly comply with relevant laws and regulations, such as the Personal Information Protection Law. They also adhere to international standards, including the Privacy and Security Rules of Health Insurance Portability and Accountability Act (HIPAA) concerning the handling of Protected Health Information (PHI). Particular attention will be given to ensuring compliance when processing spatial data that may indirectly identify patient locations and behavioral trajectories.
4. Ethical Review. The study protocol will be submitted to the hospital’s Institutional Review Board (IRB) for approval to ensure that the informed consent process and privacy rights of both patients and healthcare workers are fully protected.
Discussion
Model Value and Innovation
The primary value of this early warning model lies in its capacity to provide proactive alerts regarding violence against healthcare workers. It shifts hospital security management from passive response toward proactive prevention, offering critical lead time for intervention measures such as the deployment of security personnel. This enhances the scientific foundation of decision-making in hospital safety management.24 The model facilitates a transition from experience-driven to data-driven approaches, making hidden spatial risks explicit through visualization tools. Such tools support precise resource allocation and environmental optimization, for instance, by improving hospital layouts or enhancing lighting conditions.
From a methodological perspective, the model represents an integrative innovation. By combining STPP, machine learning, and spatial interpolation techniques, it provides an interdisciplinary framework for predicting violent incidents within the micro-environment of hospitals.
Potential Challenges in Model Implementation
Several challenges may arise during practical implementation. A key issue involves addressing data silos and privacy concerns. Medical and security data are often maintained under separate systems, complicating integration. In addition, data collection encompasses sensitive personal information that must be strictly anonymized and de-identified to comply with ethical standards and privacy regulations. Fortunately, appropriate technical solutions already exist to achieve this.25–27 By adopting advanced technologies such as k-anonymity and differential privacy, and processing data under strict protocols that comply with regulations like HIPAA, it is possible to achieve a balance between protecting privacy and maximizing the value of data.
Another challenge concerns ensuring the model’s generalizability. Given that hospitals differ in architectural layouts, patient demographics, and management systems, a single model cannot be universally applied. Localized calibration and retraining are required. By retraining with local data and fine-tuning parameters, the model can adapt to diverse environments, from large general hospitals to small specialized institutions. Furthermore, system development entails significant investment in hardware, software infrastructure, and technical expertise, which imposes high demands on the financial and technical capacity of hospitals. The initial investment is relatively high, however, it can be positioned as the core component of the “security center” in smart hospitals, integrated with existing systems, and its costs can be shared. Actively incorporating feedback from security and law enforcement personnel during the pilot program is essential for enhancing the system’s practicality and user acceptance.
Implications for Future Research
This research direction holds significant potential for the advancement of smart hospitals.28 By embedding the early warning model as the “security hub” of the hospital’s intelligent management system and linking it with outpatient scheduling, bed management, and logistics/security platforms, hospitals can establish a closed-loop management cycle of “early warning – response – intervention – feedback”.29,30
It also expands the role of artificial intelligence in hospital safety management. Previous studies have applied time-series prediction models, such as Long Short-Term Memory (LSTM) networks, to forecast patient flow peaks at both hospital-wide and department-specific levels.31,32 Integrating these predictive models with the GIS-based early warning framework will enable extended risk forecasting. Furthermore, this research can promote the development of standardized hospital safety data protocols, privacy protection frameworks, and early warning response procedures, thereby laying the groundwork for widespread adoption of such technologies across the healthcare sector.
Conclusion
This study demonstrates that constructing an early warning model for violence against healthcare workers based on GIS technology is both theoretically feasible and practically necessary, with strong potential for application. By systematically integrating multi-source spatiotemporal data and applying spatiotemporal analysis, machine learning, and spatial interpolation techniques, the model can effectively identify and predict hospital violence hotspots, offering a robust technical tool and decision-making support for hospital security management.
Although challenges remain in data acquisition, ethics, and cost, with the continuous advancement of technology and the progressive development of smart hospitals, GIS-based early warning models are likely to become a central component of efforts to establish safe and harmonious healthcare environments. This study illustrates the value of interdisciplinary collaboration between public safety and clinical medicine, highlighting innovative directions for the future of hospital security management.
Patient Consent
The data in this study has been obtained with individual informed consent.
Funding
This study was supported by the Fundamental Research Funds for the Central Universities (2024JKF31). This study was supported in part by the “Double First-Class” innovative research project in criminology at the People’s Public Security University of China (2023SYL03).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rehan ST, Shan MS, Shuja SH, et al. Workplace violence against healthcare workers in Pakistan; call for action, if not now, then when? A systematic review. Global Health Action. 2023;16(1):2273623. doi:10.1080/16549716.2023.2273623
2. Fliegauf G, Dora EV, Guti T, et al.Workplace violence at the Heim Pál National Institute of pediatrics: (With a special focus on employee situation assessment, violence perception and emergency care). Medical Weekly. 2025;24(166):930–10. doi:10.1556/650.2025.33324
3. Bojaj G, Spahiu A, Bojaj B, Gokdemir O. Violence against health workers durıng the COVID-19 pandemic in Kosovo: a cross-sectional study. J Family Med Primary Care. 2025;14(5):1992–1999. doi:10.4103/jfmpc.jfmpc_1613_24
4. Goel A, Dyaram L, Dayaram K. Patient-perpetrated violence against healthcare workers in the Asia-Pacific Region: scoping review and research agenda. Asia Pac J Hum Resour. 2025;63(3):E70015. doi:10.1111/1744-7941.70015
5. Sing P, Lau ACH. A scoping review of workplace violence against healthcare workers in Singapore. Front Public Health. 2025;13:1624191. doi:10.3389/fpubh.2025.1624191
6. Kumar Wasan M. National strategies to reduce violence against health care workers. Am J Med. 2025;138(10):1317–1318. doi:10.1016/j.amjmed.2025.05.006
7. Ghimire A. Violence against healthcare workers in Nepal: a system dynamics perspective on a growing crisis. Front Public Health. 2025;13:1615231. doi:10.3389/fpubh.2025.1615231
8. Alhomoud F. “That’s Enough”-workplace violence against physicians, pharmacists, and nurses in Saudi Arabia: a systematic review of prevalence, causes, and consequences. Risk Management Healthcare Policy. 2025;18:373–408. doi:10.2147/RMHP.S509895
9. Bianco L, Oliva S, Grassi F, et al. Violence against healthcare workers in a university hospital of central italy: how risk management interventions can help change a trend. Healthcare. 2025;13(4):409. doi:10.3390/healthcare13040409
10. Lin Q, Liu LF, Fu MX, et al. Research hotspots and trends in workplace violence among healthcare professionals: a bibliometric and visualization analysis based on web of science. J Multidisciplinary Healthcare. 2025;18:2111–2129. doi:10.2147/JMDH.S508935
11. Cannizzaro D, Saguatti I, Caleffi D, Rovesti S, Ferri P. Physical and psychological consequences on nurses affected by workplace violence: a scoping review protocol. BMJ Open. 2025;15(7):e105171. doi:10.1136/bmjopen-2025-105171
12. Dean E, Taylor MJ, Francis H, et al. A methodological framework for geographic information systems development. Syst Res Behav Sci. 2017;34(6):759–772. doi:10.1002/sres.2417
13. Lee J, Lee JH, Im J, Jang J. Enhancing urban safety: optimal patrol route strategies for volunteer security squads based on integrated BIM-GIS data. Buildings. 2024;14(10):3074. doi:10.3390/buildings14103074
14. Celik KT, Kurdoglu BC. A GIS-based model for determining safety indices to evaluate the post-disaster usability of urban open and green spaces in Amasya City Center, Turkiye. Int J Disaster Risk Reduct. 2024;106:104439. doi:10.1016/j.ijdrr.2024.104439
15. Youssef M, El-Sorogy AS, Al Otaibi S, et al. Deciphering spatial patterns of potential toxic elements using GIS and multivariate statistics for sustainable development in some areas of MENA region. Toxicol Res. 2025;14(6). doi:10.1093/toxres/tfaf166
16. Zhang HR, Fu X, Huang J, et al. Multi-scale spatiotemporal dynamics of ecosystem services and detection of their driving mechanisms in Southeast Coastal China. Land. 2025;14(11):2101. doi:10.3390/land14112101
17. Allalou R, Hebib R, Bersi M, Lefkir A. BIM-GIS integrated hydrodynamic modeling for road flood risk assessment: a case study in Algeria’s Chiffa Wadi. Reliab Eng Syst Saf. 2025;267:111906. doi:10.1016/j.ress.2025.111906
18. DING jiadong. Design and application of security system in smart hospital cases. Application IC. 2024;41(10):428–430. doi:10.19339/j.issn.1674-2583.2024.10.205
19. Yang GAO, Ze-wei ZHU. The design of the security prevention system for smart hospital. Intelligent Building Smart City. 2025;S1):175–178. doi:10.13655/j.cnki.ibci.2025.S1.051
20. Dong Z, Guo C. A literature review of spatio-temporal data analysis. J Phys Conf Ser. 2021;1792(1):012056. doi:10.1088/1742-6596/1792/1/012056
21. Gan ZX, Liang T, Yang RX. Identifying temporal variations in accessibility inequity to healthcare services across different travel strategies. J Transport Health. 2024;38:101838. doi:10.1016/j.jth.2024.101838
22. Wang YF, Chen X, Xue F. A review of bayesian spatiotemporal models in spatial epidemiology. ISPRS Int J Geo-Information. 2024;13(3):97. doi:10.3390/ijgi13030097
23. Diggle PJ. Spatio-temporal point processes: methods and applications. Monographs Statistics Applied Probability. 2007;107:1–45.
24. Ming Y, Meehan R. Patient safety perception within hospitals: an examination of job type, handoffs and information exchange, and hospital management support. J Patient Safety. 2023;19(6):369–374. doi:10.1097/PTS.0000000000001128
25. Song FG, Ma TH, Tian Y, et al. A new method of privacy protection: random k-anonymous. IEEE Access. 2019;(7):75434–75445. doi:10.1109/ACCESS.2019.2919165
26. Guo P, Xu SL, Liang WF. A cloud-assisted anonymous and privacy-preserving authentication scheme for internet of medical things. Computers Secutrity. 2025;(157):e104614. doi:10.1016/j.cose.2025.104614
27. Faraj GH, Shahtalebi K, Mala H. An anonymous authenticated key agreement scheme for telecare medical information systems. Cryptography. 2024;8(4). doi:10.3390/cryptography8040052
28. Zhang GW, Gong MC, Li HJ. The “Trinity” smart hospital construction policy promotes the development of hospitals and health management in China. Front Public Health. 2023;(11):e1219407. doi:10.3389/fpubh.2023.1219407
29. Xia X, Ma YL, Luo Y. Research and exploration of data centre construction in smart hospital stage. J Computational Method Sci Engineer. 2023;23(4):1847–1858. doi:10.3233/JCM-226768
30. Shu C, Chen YY, Yang HY. Investigation and countermeasures research of hospital information construction of tertiary class-a public hospitals in China: questionnaire study. JMIR Format Res. 2023;(7). doi:10.2196/41820
31. Baten RB. How are US hospitals adopting artificial intelligence? Early evidence from 2022. Health Affairs Scholar. 2024;2(10):qxae123. doi:10.1093/haschl/qxae123
32. Pham P, Zhang HL, Gao WL. Determinants and performance outcomes of artificial intelligence adoption: evidence from US Hospitals. J Business Res. 2024;
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.