Back to Journals » Infection and Drug Resistance » Volume 19
Thoracic Extension of an Odontogenic Deep Neck Space Infection: A Case of Carbapenem-Resistant Acinetobacter baumannii (CRAB) Empyema in an Immunocompetent Patient
Authors Aljbawi H ![]() , Senjab A
, Senjab A ![]() , Saif MAA, Hesso M, Darwish B
, Saif MAA, Hesso M, Darwish B
Received 17 December 2025
Accepted for publication 30 January 2026
Published 3 February 2026 Volume 2026:19 589625
DOI https://doi.org/10.2147/IDR.S589625
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hazrat Bilal
Hussein Aljbawi,1 Alaa Senjab,1 Mohammad Abd Alrahman Saif,2 Mohammad Hesso,2 Bassam Darwish2
1Faculty of Medicine, Damascus University, Damascus, Syrian Arab Republic; 2Al-Mouwasat University Hospital, Faculty of Medicine, Damascus University, Damascus, Syrian Arab Republic
Correspondence: Alaa Senjab, Faculty of Medicine, Damascus University, Fayez Mansour Street, Al Mazzah, Damascus, Syrian Arab Republic, Tel +963 940 450 703, Email [email protected]
Background: Deep neck space infections (DNSIs) of odontogenic origin are serious infections that may extend into mediastinal and thoracic compartments, causing life-threatening complications. Empyema secondary to carbapenem-resistant Acinetobacter baumannii (CRAB) in an immunocompetent patient is extremely rare and illustrates the therapeutic challenges posed by multidrug-resistant pathogens.
Case Presentation: A 22-year-old previously healthy Arab male presented to the emergency department with fever, left facial swelling, trismus, and dysphagia following untreated dental caries. Examination and imaging revealed a descending infection from deep neck space abscess toward the thoracic cavity. Despite incision and drainage of the buccal abscess, from which Acinetobacter baumannii was isolated, he developed respiratory distress. Chest imaging confirmed a large left-sided pleural empyema, and drainage yielded 1000 mL of purulent fluid. Pleural cultures identified CRAB, resistant to all tested agents except colistin. The patient was treated with chest drainage, intravenous colistin, and repeated wound irrigation. Clinical status improved with resolution of fever, normalization of inflammatory markers, and radiological reduction of the empyema. He was discharged with portable chest drains and referred for thoracic follow-up.
Discussion: This case underscores the aggressive nature of odontogenic DNSIs and their potential for thoracic extension even in immunocompetent young adults. It also highlights that highly drug-resistant organisms such as CRAB may occasionally be encountered in severe infections outside classical intensive-care environments, particularly in settings with extensive antibiotic exposure and limited access to newer agents. Early diagnosis, multidisciplinary management, and culture-guided therapy were key to a favorable outcome.
Conclusion: Odontogenic DNSIs complicated by empyema represent a rare but severe condition. The unusual involvement of CRAB in this context emphasizes both the clinical severity and the therapeutic limitations associated with multidrug-resistant pathogens and underlines the need for timely drainage and appropriate, susceptibility-guided antibiotic therapy.
Keywords: deep neck space infection, odontogenic infection, pleural empyema, carbapenem-resistant Acinetobacter baumannii, case report
Introduction
Pleural effusion is a relatively common medical case with an annual incidence of 0.32%.1 Even though empyema represents only 5–10% of all parapneumonic effusions, empyema-related hospitalizations are rising.2,3 Empyema is the presence of purulent material within the pleural cavity, commonly as a complication of pneumonia, chest wall trauma, or thoracic surgeries.4 Odontogenic infections are a rare source of intrathoracic complications, and clinical awareness is needed due to their potentially significant morbidity and mortality.5 While aerobic bacteria- primarily Streptococcus spp., Staphylococcus aureus- are the principal etiological agents reported in such infections,6 anaerobes are also significant etiological agents, they are less frequently reported, largely due to limitations in culture facilities and the technical complexity required for their accurate isolation and identification.7 Acinetobacter baumannii is implicated in a wide range of infections, and Carbapenem-resistant Acinetobacter baumannii (CRAB) represents a pressing public health challenge.8 It is widely recognized as a top-priority pathogen for the development of new antibiotics on a global scale.9 Treatment options for pleural empyema vary based on the stage of the disease and range from non-surgical approaches, such as antibiotic therapy and chest tube drainage, to more invasive interventions, including thoracoscopic or open surgical procedures.10 This case adds to the literature by documenting a rare descending odontogenic deep neck space infection complicated by pleural empyema due to community-acquired carbapenem-resistant Acinetobacter baumannii in an immunocompetent young adult without preceding pneumonia, highlighting the need for early repeat chest imaging, culture-guided therapy, and timely drainage.
Case Presentation
We report the case of a 22-year-old Syrian male who presented to the emergency department with swelling of the left cheek, erythema, and localized warmth. He also reported fever, trismus, and dysphagia. The patient disclosed a history of dental caries and persistent toothache over the preceding week.
The patient was on 1 g/day of IM ceftriaxone prescribed by his dentist for his dental carries for four days. He had no known history of chronic medical conditions, drug allergies, or hereditary diseases. His past surgical history included an appendectomy and an inguinal hernia repair.
Vital signs on presentation were: temperature 38°C, Blood Pressure: 120/70 mmHg, Heart Rate: 127, Respiratory Rate: 28, PO2: 95% on room air. Head and neck exam showed a red, swollen area on the left lower cheek, extending to the mandibular angle. Intraoral examination showed fluctuant abscess with a spontaneous drainage opening, along with soft tissue swelling extending toward the left tonsillar region.
The patient was conscious, alert, and in no acute distress. Respiratory examination revealed fine crackles at the base of the left lung. Cardiovascular, Abdominal, and Neurological tests were unremarkable.
Laboratory investigations showed leukocytosis (WBC 16,400/µL) with neutrophilic predominance (neutrophils 94%, lymphocytes 6%) and markedly elevated C-reactive protein (CRP) at 211 mg/L.
Bedside incision and drainage of the buccal abscess under local anesthesia were performed, yielding approximately 100 mL of purulent material, which was collected for culture and sensitivity testing. The culture grew Acinetobacter baumannii. The abscess cavity was then irrigated and packed. Blood cultures obtained were negative.
A contrast-enhanced head and neck CT demonstrated a gas-containing, multiloculated left buccal/masticator space collection consistent with an odontogenic abscess (Figure 1A and B). A baseline chest radiograph showed no pleural effusion or focal pulmonary consolidation, with no radiographic evidence of thoracic complications at that time (Figure 2).
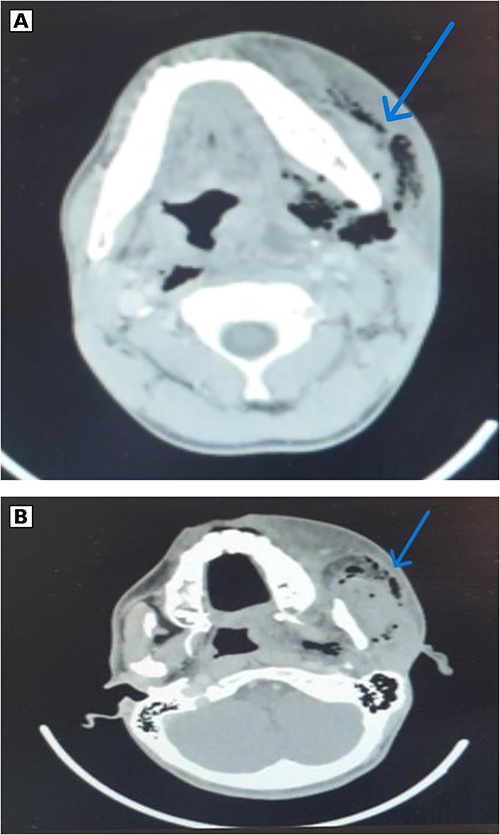 |
Figure 1 (A) Contrast-enhanced neck CT (axial view) demonstrating a multiloculated hypodense collection within the left submandibular and parapharyngeal spaces with surrounding soft-tissue edema, consistent with a deep neck space abscess. No vascular thrombosis or bony involvement is evident. The arrow indicates the gas-containing component consistent with a left deep neck space abscess (submandibular/parapharyngeal collection). (B) Additional axial neck CT slice showing the extent of the hypodense collection in the left submandibular/parapharyngeal spaces with associated soft-tissue swelling. The arrow indicates the gas-containing component consistent with a deep neck space abscess (submandibular/parapharyngeal collection). |
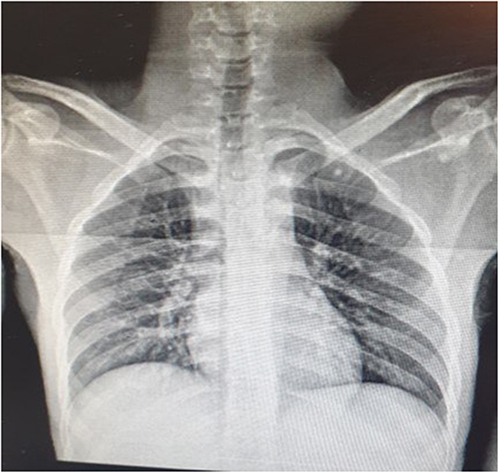 |
Figure 2 Admission chest radiograph (frontal view) showing no pleural effusion or acute thoracic complication at presentation. |
The patient was started on broad-spectrum antimicrobial coverage of IV Piperacillin-Tazobactam, Vancomycin, and Clindamycin, in addition to antiseptic mouthwash.
Subsequently, the patient developed dyspnea and tachypnea. A repeat chest radiograph demonstrated a new large left-sided pleural effusion with near-complete opacification of the left hemithorax, consistent with complicated parapneumonic effusion/empyema (Figure 3). A contrast-enhanced chest CT confirmed a large, loculated left pleural fluid collection with compressive atelectasis of the adjacent lung (Figure 4). These findings correlated with the clinical suspicion of an odontogenic deep neck space infection with thoracic extension.
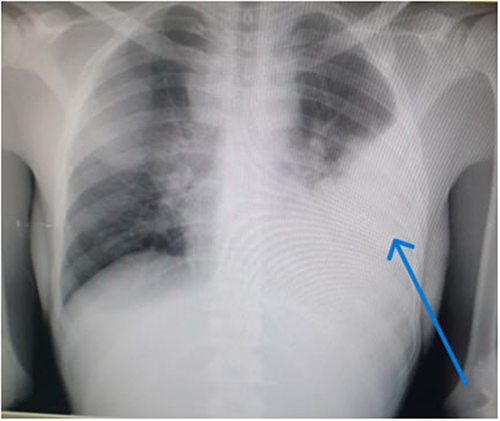 |
Figure 3 Chest radiograph (frontal view) obtained after onset of respiratory symptoms demonstrating a large left pleural opacity/effusion occupying most of the left hemithorax with blunting of the left costophrenic angle and rightward mediastinal shift, consistent with a large pleural collection. The arrow indicates a large left-sided pleural opacity/effusion. |
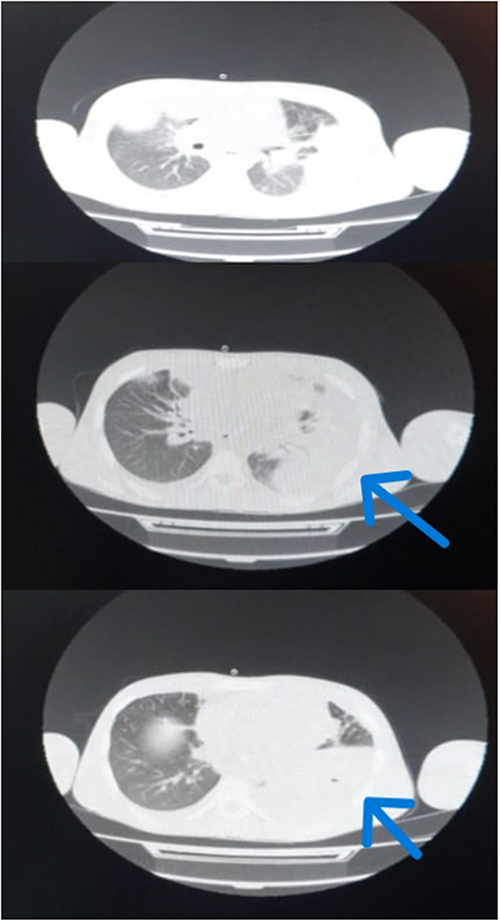 |
Figure 4 Contrast-enhanced chest CT demonstrating a large, loculated left pleural fluid collection with compressive atelectasis of the adjacent lung, consistent with pleural empyema. The arrows indicate a large, loculated left pleural fluid collection, consistent with pleural empyema. |
Definitive surgical drainage of the deep neck spaces under general anesthesia was recommended; however, the patient refused because of anxiety about anesthesia-related complications and opted for a conservative approach.
A chest drainage procedure was performed under local anesthesia (tube thoracostomy), yielding approximately 1000 mL of purulent fluid. A sample was sent for microbiological analysis, which identified carbapenem-resistant Acinetobacter baumannii (CRAB). Intravenous Colistin was administered. The patient’s condition improved significantly following the thoracostomy, repeated local wound care, and continued antibiotic therapy. His fever subsided, and his clinical condition stabilized.
Given the unusual isolation of CRAB in an immunocompetent young adult, Investigations for underlying immunodeficiency were conducted. Serological markers for hepatitis B and C, as well as Human Immunodeficiency Virus, were negative. HbA1c was 4.7%, ruling out diabetes mellitus.
Repeat laboratory tests showed improved inflammatory markers: WBC 9200/µL (neutrophils 80%), CRP 62 mg/L. Other laboratory parameters were within reference range.
The patient was discharged after completing antimicrobial therapy and demonstrating marked clinical, radiological, and laboratory improvement; follow-up chest radiography showed near-complete resolution of the left pleural effusion with re-expansion of the left lung and only minimal residual basilar changes (Figure 5). He was discharged with portable chest drains in place, with instructions to follow up at the thoracic surgery clinic once drainage ceases.
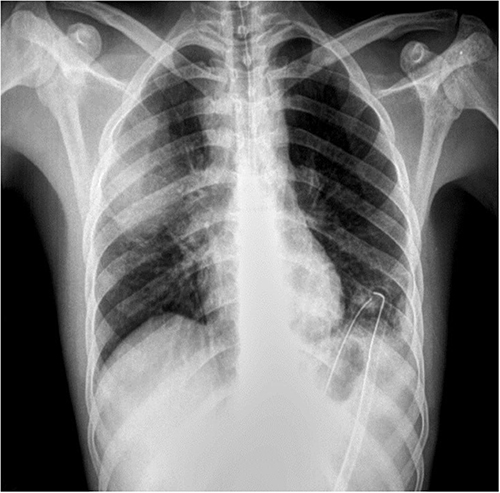 |
Figure 5 Follow-up chest radiograph showing marked interval reduction of the left pleural collection with improved aeration; the thoracostomy tube is visible in situ. |
Discussion
General Discussion
Odontogenic infections constitute the primary etiological source of maxillofacial space infections and can progress to life-threatening complications.10,11 Extensions to the thorax such as mediastinitis, empyema, jugular vein thrombosis, septic venous emboli, pericarditis, epidural abscess, and carotid artery erosion, though uncommon, have been reported, and these conditions are often associated with poor clinical outcomes.12 Delayed recognition and management of these cases are associated with significant morbidity and mortality.13
Over the past decades, Acinetobacter baumannii has emerged worldwide as a highly problematic nosocomial pathogen, particularly in immunocompromised or elderly patients. Its clinical relevance is largely driven by its remarkable capacity to acquire and upregulate diverse resistance determinants, making it one of the most successful multidrug-resistant organisms that threaten current antibiotic therapy.14 As we conducted our literature review, we identified several reports of deep neck infections caused by A. baumannii, such as Marioni et al (2010), who described a deep neck abscess due to A. baumannii infection in an immunocompetent yet elderly patient, and Jain et al (2008), who reported trauma-triggered cervicofacial necrotizing fasciitis by the same pathogen secondary to an odontogenic infection.15,16 There have also been reports of thoracic extension of deep neck infections causing necrotizing descending mediastinitis due to A. baumannii in an outpatient.17 While empyema caused by A. baumannii has been described in the literature, it has typically occurred in immunocompromised patients or been preceded by pneumonia.18–20 To our knowledge, the present case combines these previously described patterns, representing an odontogenic deep neck infection that extended into the thoracic cavity and resulted in pleural empyema due to CRAB in an immunocompetent young adult without preceding pneumonia.
Diagnostic Process
Microbiological identification and susceptibility testing were performed using the BD Phoenix NMIC/ID-431 system and interpreted according to CLSI criteria; colistin susceptibility was assessed by Kirby–Bauer disk diffusion per the local laboratory protocol, as colistin minimum inhibitory concentration data were not available.
Negative admission blood cultures, together with isolation of A. baumannii from both the neck abscess and pleural fluid, supports a contiguous (descending) spread from the odontogenic deep neck infection rather than an unrelated primary pulmonary source, while acknowledging that prior antibiotics may reduce blood-culture yield.
Early recognition of thoracic extension is crucial in patients with odontogenic deep neck infections. In our patient, the initial chest radiograph obtained at admission was unremarkable, consistent with a process confined to the cervical region. The subsequent onset of dyspnea and tachypnea under in-hospital observation prompted repeat chest imaging and led to the early identification of a large pleural effusion. This sequence highlights the importance of maintaining a low threshold for chest imaging in patients with deep neck infections who develop new respiratory symptoms or persistent systemic inflammation despite apparently adequate therapy.
Diagnosis of pleural empyema relies on a combination of clinical evaluation and radiological findings. Dyspnea, fever, and pleuritic chest pain are frequent but non-specific manifestations.21 Chest radiography provides a simple first-line tool to detect pleural opacification, whereas computed tomography offers superior anatomical detail, allowing differentiation between simple parapneumonic effusion and empyema and demonstrating loculations or associated lung collapse. In our case, contrast-enhanced CT of the chest confirmed a large, loculated pleural collection with compressive atelectasis and guided the decision to proceed with tube thoracostomy. A systematic review has emphasized that early diagnosis of pleural empyema depends on a high index of suspicion combined with informative pleural imaging findings.2 Our experience is in line with these observations, as prompt reassessment and repeat imaging were pivotal in altering the clinical course of this deep neck infection at risk of thoracic spread.
Therapeutic Approach and Emerging Treatments
Management options for pleural empyema range from chest tube drainage and intrapleural therapies to video-assisted thoracoscopic surgery (VATS) and open decortication. Current recommendations favor early VATS for organized or loculated empyema, as it is associated with higher success rates and shorter hospital stay compared with repeated tube thoracostomy alone.4,22,23 In our patient, definitive surgical drainage of the deep neck spaces and thoracic cavity under general anesthesia was advised; however, the patient refused the procedure because of anxiety regarding anesthesia-related complications. Consequently, a conservative strategy based on chest tube drainage, close clinical monitoring, and escalation of antimicrobial therapy was adopted.
The initial empirical regimen (piperacillin–tazobactam, vancomycin, and clindamycin) was chosen to provide broad coverage for deep neck infections of odontogenic origin. Once culture and sensitivity testing of the pleural fluid identified carbapenem-resistant Acinetobacter baumannii (CRAB), therapy was de-escalated to intravenous colistin as the only agent with in vitro activity in our setting. Colistin remains a key drug in the treatment of CRAB infections, but its use is limited by potential nephrotoxicity and by uncertainty regarding optimal dosing and the benefit of combination regimens.24 Newer agents such as cefiderocol, sulbactam–durlobactam, and eravacycline have shown promising activity against CRAB and have been approved by the US Food and Drug Administration;9 however, these options were not available in Syria at the time of treatment.
The patient’s condition improved significantly following chest drainage, colistin therapy, and continued local wound care, with resolution of systemic inflammation and normalization of laboratory markers. This favorable outcome should be interpreted with caution: tube thoracostomy and conservative management cannot be regarded as equivalent to guideline-recommended early VATS for all patients with empyema. Rather, our case illustrates that, in selected patients who refuse surgery or in whom advanced surgical options and newer anti-CRAB drugs are not accessible, prompt drainage and culture-guided antibiotic therapy, combined with close multidisciplinary monitoring, may still achieve clinical and radiological resolution.
An additional stewardship-relevant point is the patient’s outpatient exposure to intramuscular ceftriaxone prior to admission. In severe odontogenic deep neck infections, early source control and guideline-concordant empiric therapy are essential; partial or suboptimal antibiotics may delay definitive management, reduce culture yield, and exert selection pressure that favors resistant pathogens. Although causality cannot be confirmed, particularly as A. baumannii is often healthcare-associated, this highlights the need to avoid inappropriate antibiotic courses in dental practice and to ensure early referral when severe infection is suspected.
Limitations
This report has several limitations. First, definitive surgical source control both for the deep neck spaces and for the pleural empyema could not be pursued, as the patient declined procedures under general anesthesia; therefore, management relied on tube thoracostomy and close monitoring, which may not reflect outcomes achievable with early VATS or decortication in organized/loculated empyema. Second, antimicrobial options for carbapenem-resistant Acinetobacter baumannii were constrained in our setting, and treatment was limited to colistin as the only agent with in vitro activity; this approach is inherently limited by concerns regarding nephrotoxicity and uncertainties around optimal dosing and the value of combination regimens. Third, newer anti-CRAB agents (eg, cefiderocol, sulbactam–durlobactam, eravacycline) were unavailable locally at the time of care, which may limit the generalizability of our therapeutic strategy to settings where these agents are accessible. Finally, Colistin MIC data were not available, and colistin activity was assessed by disk diffusion per the local laboratory protocol.
Conclusion
This case illustrates the rare but serious progression of an odontogenic infection into the deep neck spaces with subsequent development of empyema caused by carbapenem-resistant Acinetobacter baumannii (CRAB) in an immunocompetent patient. It highlights the importance of early imaging, vigilant clinical assessment, and prompt multidisciplinary management when deep neck infections are accompanied by respiratory symptoms. Our findings suggest that highly resistant pathogens such as CRAB may occasionally be encountered in severe infections outside classical intensive-care environments, especially in regions with extensive antimicrobial use and limited access to newer agents. Timely drainage of purulent collections and tailored antibiotic therapy based on culture and susceptibility results remain critical for successful outcomes in such complex cases.
Declaration of Generative AI and AI-Assisted Technologies in the Manuscript Preparation Process
During the preparation of this work the author(s) used ChatGPT in order to improve the writing style. After using this tool/service, the author(s) reviewed and edited the content as needed and take(s) full responsibility for the content of the published article.
Data Sharing Statement
All data generated or analyzed during this case report are included in this published article.
Ethics Approval and Consent to Participate
Not applicable. As this is a single case report, ethical approval was not required in accordance with institutional policies.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Marel M, Zrůstová M, Stasný B, Light RW. The incidence of pleural effusion in a well-defined region. epidemiologic study in central Bohemia. Chest. 1993;104(5):1486–9. doi:10.1378/chest.104.5.1486
2. Zettinig D, D’Antonoli TA, Wilder-Smith A, Bremerich J, Roth JA, Sexauer R. Diagnostic accuracy of imaging findings in pleural empyema: systematic review and meta-analysis. J Imaging. 2021;8(1):3. doi:10.3390/jimaging8010003
3. Grijalva CG, Zhu Y, Nuorti JP, Griffin MR. Emergence of parapneumonic empyema in the USA. Thorax. 2011;66(8):663–668. doi:10.1136/thx.2010.156406
4. Redden MD, Chin TY, van Driel ML. Surgical versus non-surgical management for pleural empyema. Cochrane Database Syst Rev. 2017;3(3):CD010651. doi:10.1002/14651858.CD010651.pub2
5. Moncada R, Warpeha R, Pickleman J, et al. Mediastinitis from odontogenic and deep cervical infection. Anatomic pathways of propagation. Chest. 1978;73(4):497–500. doi:10.1378/chest.73.4.497
6. Dyrhovden R, Nygaard RM, Patel R, Ulvestad E, Kommedal Ø. The bacterial aetiology of pleural empyema. A descriptive and comparative metagenomic study. Clin Microbiol Infect. 2019;25(8):981–986. doi:10.1016/j.cmi.2018.11.030
7. Patel S, Hanfe H, Khurana AK, Bhadade A, Nema S. Unilateral complicated pleural empyema in a patient with bronchial asthma due to clindamycin-resistant Prevotella buccae. Archiv Clin Cases. 2023;10(4):150–152. doi:10.22551/2023.41.1004.10263
8. Ibrahim S, Al-Saryi N, Al-Kadmy IMS, Aziz SN. Multidrug-resistant Acinetobacter baumannii as an emerging concern in hospitals. Mol Biol Rep. 2021;48(10):6987–6998. doi:10.1007/s11033-021-06690-6
9. Shields RK, Paterson DL, Tamma PD. Navigating available treatment options for carbapenem-resistant Acinetobacter baumannii-calcoaceticus complex infections. Clin Infect Dis. 2023;76(Suppl 2):S179–S193. doi:10.1093/cid/ciad094
10. Zeitoun IM, Dhanarajani PJ. Cervical cellulitis and mediastinitis caused by odontogenic infections: report of two cases and review of literature. J Oral Maxillofac Surg. 1995;53(2):203–208. doi:10.1016/0278-2391(95)90404-2
11. Green AW, Flower EA, New NE. Mortality associated with odontogenic infection! Br Dent J. 2001;190(10):529–530. doi:10.1038/sj.bdj.4801024
12. Economopoulos GC, Scherzer HH, Gryboski WA. Successful management of mediastinitis, pleural empyema, and aortopulmonary fistula from odontogenic infection. Ann Thorac Surg. 1983;35(2):184–187. doi:10.1016/s0003-4975(10)61458-0
13. Miller CR, Von Crowns K, Willoughby V. Fatal Ludwig’s Angina: cases of lethal spread of odontogenic infection. Acad Forens Pathol. 2018;8(1):150–169. doi:10.23907/2018.011
14. Peleg AY, Seifert H, Paterson DL. Acinetobacter baumannii: emergence of a successful pathogen. Clin Microbiol Rev. 2008;21(3):538–582. doi:10.1128/CMR.00058-07
15. Marioni G, Marchese-Ragona R, Boldrin C, et al. Deep neck abscess due to Acinetobacter baumannii infection. Am J Otolaryngol. 2010;31(4):304–307. doi:10.1016/j.amjoto.2009.02.018
16. Jain S, Nagpure PS, Singh R, Garg D. Minor trauma triggering cervicofacial necrotizing fasciitis from odontogenic abscess. J Emerg Trauma Shock. 2008;1(2):114–118. doi:10.4103/0974-2700.43197
17. Cherrabi K, Ouattassi N, Tinni O, Kamal D, Elalami MN. et al. Necrotizing descending mediastinitis by Acinetobacter baumannii in an out-patient: a case report. Egypt J Otolaryngol. 2021;37(1):94. doi:10.1186/s43163-021-00155-0
18. Yang S, Wei C. Extensively drug-resistant Acinetobacter baumannii lung abscess and empyema in a patient with fulminant mycoplasma pneumoniae pneumonia. Respir Med Case Rep. 2024;53:102150. doi:10.1016/j.rmcr.2024.102150
19. Chai M, Yusufu P, Chen Y, et al. Empyema caused by Peptoniphilus asaccharolyticus and complicated by secondary pulmonary infection from Acinetobacter baumannii: a case report. Infect Drug Resist. 2024;17:4531–4537. doi:10.2147/IDR.S485235
20. Passerotto RA, Lamanna F, Farinacci D, et al. Ventilator-associated pneumonia (VAP) and pleural empyema caused by multidrug-resistant Acinetobacter baumannii in HIV and COVID 19 infected patient: a case report. Infect Med. 2023;2(2):143–147. doi:10.1016/j.imj.2023.02.004
21. Jany B, Welte T. Pleural effusion in adults-etiology, diagnosis, and treatment. Dtsch Arztebl Int. 2019;116(21):377–386. doi:10.3238/arztebl.2019.0377
22. Chambers A, Routledge T, Dunning J, Scarci M. Is video-assisted thoracoscopic surgical decortication superior to open surgery in the management of adults with primary empyema? Interact Cardiovasc Thorac Surg. 2010;11(2):171–177. doi:10.1510/icvts.2010.240408
23. Rana MA, Rahman BA, Mady AF, et al. Intra-pleural colistin methanesulfonate therapy for pleural infection caused by carbapenem-resistant Acinetobacter baumannii: a successful case report. Infect Dis Rep. 2014;6(3):5413. doi:10.4081/idr.2014.5413
24. Centers for Disease Control and Prevention (CDC). Antibiotic resistance threats in the United States. Atlanta: US Department of Health and Human Services; 2019.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.