Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Thermoresponsive Hydroxybutyl Chitosan–Assisted Carteolol Delivery with Pulsed Dye Laser for Superficial Infantile Hemangiomas: An Exploratory Randomized Study
Authors Chen Z ![]() , Tang Y, Zheng M, Lin J, Xu J, Zhang C, You C, Wu J, Cao N
, Tang Y, Zheng M, Lin J, Xu J, Zhang C, You C, Wu J, Cao N ![]()
Received 17 April 2026
Accepted for publication 20 June 2026
Published 15 July 2026 Volume 2026:19 617690
DOI https://doi.org/10.2147/CCID.S617690
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Jeffrey Weinberg
ZeHui Chen, YiYan Tang, MeiLian Zheng, JieChao Lin, JiaBo Xu, CuiMei Zhang, CaiLian You, JinHong Wu, Ning Cao
Department of Plastic and Aesthetic Surgery, Zhangzhou Affiliated Hospital of Fujian Medical University, Zhangzhou, Fujian, People’s Republic of China
Correspondence: Ning Cao, Email [email protected]
Purpose: To preliminarily evaluate a thermoresponsive hydroxybutyl chitosan (HBC)-assisted topical carteolol delivery regimen combined with pulsed dye laser (PDL), compared with conventional carteolol wet-compress therapy combined with PDL, in infants with superficial infantile hemangiomas.
Patients and Methods: This single-center, open-label, randomized exploratory study included 40 infants with superficial IHs, who were assigned to an HBC group or a control group at a 1:1 ratio. Both groups received PDL. The HBC group received immediate post-laser topical application of the optimized HBC–carteolol mixture, whereas the control group received conventional topical carteolol wet-compress therapy after PDL. The predefined efficacy assessment was performed at the 6-month visit, while clinical follow-up continued for 6 to 12 months as routine clinical follow-up. The primary endpoint was the number of PDL treatment sessions completed during the 6-month treatment period. Secondary outcomes included 6-month Hemangioma Activity Score (HAS), change in HAS from baseline to 6 months, and treatment-related complications.
Results: At the predefined 6-month assessment, the HBC group required fewer treatment sessions than the control group during the 6-month treatment period (3.5 ± 0.6 vs 4.7 ± 0.7, P < 0.001). The 6-month HAS was numerically lower in the HBC group than in the control group, but the difference was not statistically significant (0.3 ± 0.4 vs 0.4 ± 0.4, P = 0.272). The HAS change score also did not differ significantly between groups (4.6 ± 0.5 vs 4.5 ± 0.5, P = 0.440). The aggregate treatment-related local complication rate was lower in the HBC group than in the control group (5.0% vs 35.0%, P = 0.048).
Conclusion: In this single-center exploratory randomized study, the HBC–carteolol–PDL regimen was associated with fewer treatment sessions and complications than conventional carteolol wet-compress therapy combined with PDL. Further component-controlled studies are needed to determine the independent effect of HBC.
Keywords: thermoresponsive hydroxybutyl chitosan, carteolol, pulsed dye laser, superficial infantile hemangiomas
Introduction
Infantile hemangioma (IH), the most common benign vascular tumor of infancy, affects approximately 4–5% of infants in population-based estimates. Reported risk is higher among female infants, premature or low-birth-weight infants, and White/Caucasian infants.1 The natural history of IH exhibits distinct chronological phases. The tumor typically appears within the first weeks of life, followed by a rapid proliferative phase throughout the first year of life. Subsequently, IH enters a spontaneous regressive stage, which may persist for 5 years or longer. Although most IH resolve spontaneously, approximately 10% of cases require intervention to prevent complications arising from the location of the tumor, including hemorrhage, ulceration, disfigurement, functional impairment and life-threatening complications.2
IHs are classified into superficial IH, mixed IH, deep IH, and IH with minimal or arrested proliferation.3 Superficial IH is predominantly composed of benign proliferation of vascular endothelial cells (VECs) derived from the mesoderm,2 which present as bright red macules/papules (strawberry-like) with a smooth surface and palpable local warmth clinically.3,4
β-Blockers are the first-line pharmacotherapy for IH. Oral propranolol remains the standard systemic therapy for problematic or high-risk IHs, whereas topical β-blockers have been widely used for selected small, thin, or superficial lesions. In particular, topical timolol is recommended by the American Academy of Pediatrics as an option for select small, thin, superficial IHs.1 Several clinical studies have also evaluated topical timolol for superficial IHs. Chan et al reported that 0.5% timolol maleate gel was safe and effective for small superficial IHs in a randomized controlled trial.5 A systematic review and meta-analysis including 31 studies and 691 patients further suggested that topical timolol was associated with clinical improvement in small IHs and was generally well tolerated, although the quality of evidence remained limited.6 More recently, Muñoz-Garza et al showed that topical timolol was well tolerated in early proliferative IHs, but its benefit in achieving complete or near-complete resolution was limited.7 Timolol has also been reported in the topical management of ulcerated IHs. Chakhunashvili et al described rapid healing of an ulcerated anogenital hemangioma after topical timolol combined with mupirocin, with complete healing within 4 weeks.8 Although this evidence was derived from a case report and combined topical antibiotic therapy, it indicates that timolol is clinically relevant not only to superficial IHs but also to selected ulcerated lesions.
Carteolol is another non-selective β-blocker that has been explored as a topical treatment for superficial IHs. Available clinical evidence suggests that topical carteolol may be effective and generally well tolerated in selected superficial IHs, particularly in young infants.9,10 Because it is applied locally, topical carteolol may reduce systemic exposure compared with oral β-blocker therapy; however, systemic β-blocker-related adverse effects cannot be excluded and should be actively monitored in future studies. Long-term topical application may still cause local irritation or other skin-related reactions; therefore, treatment duration and monitoring should be individualized according to lesion characteristics and clinical response.9,10 Previous studies demonstrated that 0.5% carteolol gel achieved an efficacy rate of 85–90% in treating superficial IH, particularly those located on periorbital and facial regions.11 However, long-term application of carteolol might cause irritation to the skin or abnormal growth of the hair, which required adjustments to the treatment duration on the basis of the lesion depth.9
Laser therapy destroys abnormally proliferating vascular structures within the hemangiomas through selective photothermolysis. The 595 nm pulsed dye laser (PDL) is the most commonly used laser for treating superficial IH. PDL selectively targets hemoglobin in blood vessels, resulting in photothermal coagulation of vascular endothelium while causing minimal collateral damage to surrounding normal tissues.11 PDL demonstrates significant efficacy in treating early erythematous phase or thin-walled IH through reducing ulceration occurrence and improving aesthetic outcomes.9 However, laser therapy has some limitations, including limited penetration depth, suboptimal efficacy for deep or mixed IHs, the need for repeated treatment sessions, and risks of scarring, hyperpigmentation, skin atrophy, hemorrhage, or secondary infection in selected lesions.11,12 Thus, laser therapy is commonly employed as an adjunctive approach to β-Blockers or utilized for repairing residual telangiectasias during the involuting phase. The combination of topical β-blockers and laser therapy has also been investigated. Tawfik and Alsharnoubi compared topical timolol solution with laser therapy for IHs.13 Asilian et al further reported in a double-blind randomized controlled trial that PDL combined with topical timolol gel achieved better outcomes than PDL alone.14 These studies indicate that topical β-blocker therapy and PDL may have complementary roles in selected IHs. However, the optimal topical formulation, local drug-retention strategy, dosing frequency, and post-laser delivery platform remain incompletely defined.
Innovative applications of biomaterials have provided new avenues for IH therapy. Chitosan, owing to its exceptional biocompatibility and enhanced permeability, is employed to construct drug delivery systems, such as chitosan-propranolol nanoparticles.15 This material enhances drug retention in the skin and provides sustained drug release, thereby improving local therapeutic efficacy while reducing dosing frequency.15 Furthermore, thermosensitive hydrogel-based delivery systems, such as Poloxamer 407/PF127-based hydrogels, have been investigated as local drug-delivery platforms capable of improving lesion-site retention and enabling sustained release. Their integration with photothermal strategies has also been explored in local tumor therapy, supporting the broader feasibility of hydrogel-assisted localized treatment approaches.16
Therefore, the novelty of this study lies in evaluating an integrated HBC–carteolol–PDL regimen as a local drug-delivery and post-laser protective strategy for superficial IHs. In this exploratory randomized study, we compared this HBC-based regimen with conventional carteolol wet-compress therapy combined with PDL.
Materials and Methods
Study Subjects
Forty eligible pediatric patients with superficial IHs were enrolled and randomly assigned to either the HBC group or the control group at a 1:1 ratio. All participants underwent clinical follow-up for 6 to 12 months, with outcome assessment performed at the 6-month visit. All randomized patients were scheduled to complete follow-up until at least the 6-month assessment. Patients who achieved sufficient clinical improvement before 6 months discontinued repeated PDL sessions but continued clinical follow-up until the 6-month assessment. Loss to follow-up, withdrawal of consent, and discontinuation of intervention were recorded for construction of the participant flow diagram. The participant flow from screening to final analysis is shown in Figure 1.
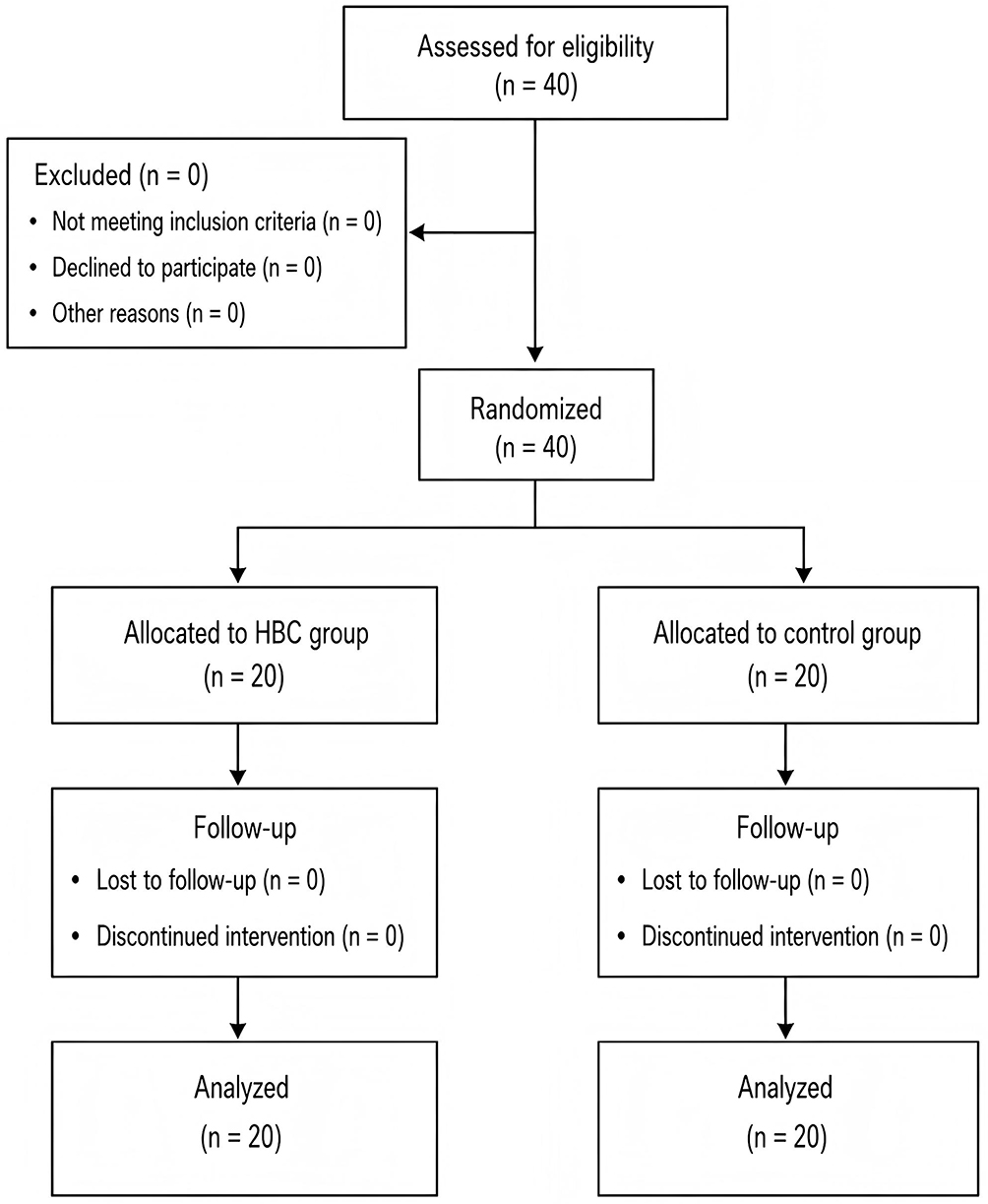 |
Figure 1 Flow diagram of participant randomization, follow-up, and analysis. The diagram shows the allocation of randomized infants to the HBC group or control group, completion of follow-up, and inclusion in the final analysis. |
Baseline demographic and lesion-related characteristics, including sex, age, lesion location, baseline HAS, follow-up duration, number of treatment sessions, and treatment-related complications, were collected. The study protocol was approved by the Institutional Ethical Committee of Zhangzhou Affiliated Hospital of Fujian Medical University (No. 2022KYB190, approval date: August 2022), and written informed consent was obtained from the guardians of all participants.
Inclusion criteria required: ① Diagnosis of IH during the proliferative phase (age less than 6 months) confirmed by clinical presentation and ISSVA 2018 Classification standards, with ultrasound or MRI showing lesion thickness of 2 to 5 mm and diameter less than 5 cm; ② No prior therapeutic interventions for IH.
Exclusion criteria included: ① Lesions in the involuting phase or without functional/cosmetic impact; ②History of prior IH-targeted therapy; ③ Contraindications such as local infection, recent vaccination (within 1 week), or systemic/cardiac disorders (eg, hypertension, sinus bradycardia, heart failure). The participant flow from screening to final analysis is shown in Figure 1.
Baseline Lesion Characterization
Baseline lesion-related characteristics were summarized using variables available in the original study database, including lesion location and baseline Hemangioma Activity Score. In addition, the eligibility criteria restricted enrollment to superficial infantile hemangiomas with a maximum lesion diameter of <5 cm and imaging-confirmed lesion thickness of 2–5 mm. Exact baseline lesion diameter, exact lesion thickness, lesion morphology, and color-intensity grading were not systematically recorded for all participants and therefore were not included as formal comparative baseline variables.
Randomization, Allocation Concealment, and Blinding
Randomization was performed at a 1:1 ratio using a random-number table prepared by an investigator who was not involved in patient enrollment, treatment delivery, or outcome assessment. Allocation was concealed using sequentially numbered, opaque, sealed envelopes. After eligibility confirmation and written informed consent, the envelope was opened by a study coordinator, who assigned the participant to the corresponding treatment group. Because the HBC–carteolol dressing and conventional carteolol wet-compress therapy differed in appearance, application procedure, and dosing frequency, blinding of caregivers and treating physicians was not feasible. Outcome assessors were blinded to treatment allocation.
Mixing Ratio Optimization of Thermosensitive Hydroxybutyl Chitosan Dressing with 2% Carteolol
A 1 mL aliquot of thermosensitive hydroxybutyl chitosan wound dressing (Medical Device Reg. No. Jing 20102140315) was mixed with varying volumes of 2% carteolol ophthalmic solution. Gelation temperature was determined using a standardized test tube inversion protocol: samples in 10×100 mm tubes were equilibrated at 4°C for ≥10 minutes, then heated in a water bath from 10°C with 1°C/min increments. After 60-second incubation at each temperature, tubes were inverted to identify the endpoint—defined as complete solidification along the tube wall with central tremor but no movement. Mixture homogeneity, precipitation, color, and transparency were simultaneously assessed to establish the optimal ratio range.
For clinical simulation, mixtures within the optimal ratio range were extruded onto a 30°-tilted beaker preheated to target temperatures (37°C, 40°C, 42°C, 45°C) in a water bath. Flow behavior (eg, gelation latency, dripping tendency) was recorded to validate applicability under physiological and post-laser hyperthermia conditions. Based on the formulation-screening results, the HBC-to-2% carteolol ratio of 10:6 (v/v) was selected as the final clinical formulation. This ratio corresponded to 1.0 mL of thermosensitive HBC wound dressing mixed with 0.6 mL of 2% carteolol ophthalmic solution. The selected formulation was used consistently in all patients assigned to the HBC group.
Treatment Protocol
The Vbeam™ pulsed dye laser system (Candela Corp., USA) was operated at a wavelength of 595 nm with a 10-mm spot size, fluence of 6–8 J/cm2, pulse duration of 1.5–40 ms, and dynamic cooling device settings of 40/20 ms cryogen spray cooling, corresponding to a 40-ms spray duration and a 20-ms spray-to-laser delay. The 40-ms value referred to the cryogen spray duration only and did not indicate a 40-ms spray plus a 40-ms delay. After standard skin cleansing and ocular protection, parameters were adjusted based on lesion characteristics, including location, color, and thickness, and patient factors, including age and skin phototype. Vertical irradiation was applied until mild purpura, defined as Grade 1–2 duskiness without epidermal graying, appeared.
All participants were scheduled for clinical reassessment at 4-week intervals after each PDL session. The 4-week interval was used as a uniform retreatment interval for both groups according to our institutional treatment protocol, allowing sufficient time for post-laser skin recovery and clinical evaluation of residual hemangioma activity. Repeat PDL treatment was performed when residual active superficial IH was present, including persistent erythema, residual swelling or elevation, or a HAS score >0, provided that the epidermis had recovered and there was no unresolved ulceration, blistering, infection, or severe dermatitis. PDL treatment was withheld in the presence of unresolved local complications and was discontinued when sufficient clinical improvement was achieved, defined as marked fading and flattening of the lesion without clinically active proliferation, or when the predefined 6-month treatment period was completed. The same retreatment interval and retreatment/stopping criteria were applied to both groups.
Post-treatment interventions were as follows: HBC group, immediate topical application of the optimized hydroxybutyl chitosan–carteolol mixture; control group, local ice-pack cooling for 15–30 min followed by erythromycin ointment. All patients were instructed to maintain wound dryness and avoid sun exposure, friction, and scratching.
Topical Application Protocol of Carteolol: The HBC group received once-daily topical application of the selected 10:6 HBC–carteolol formulation, while the control group underwent wet compress therapy with 2% carteolol ophthalmic solution three times daily. Specifically, medical gauze (6-layer thickness) was trimmed to match the hemangioma size, saturated with 2% carteolol ophthalmic solution (National Drug Approval No. H10970025; Otsuka Pharmaceutical Co., Ltd., Tokyo, Japan) until fully soaked but not dripping, applied directly to the hemangioma surface, covered with plastic wrap for occlusive sealing, and maintained for 0.5 hours per session. This procedure was repeated three times daily.
Outcome Measures and Assessment
The primary endpoint was the number of PDL treatment sessions required during the predefined 6-month treatment period. Repeated PDL sessions were discontinued when the retreatment/stopping criteria were no longer met, including marked fading and flattening of the lesion without clinically active proliferation, or when the predefined 6-month treatment period was completed. For patients who achieved sufficient clinical improvement before 6 months and discontinued repeated PDL sessions, clinical follow-up was continued, and the fixed 6-month visit remained the efficacy assessment time point. These patients were included in the 6-month HAS analysis and were not treated as missing, censored, or excluded observations. Early clinical improvement was reflected by the total number of PDL sessions completed during the predefined 6-month treatment period rather than analyzed as a separate time-to-endpoint outcome.
Secondary endpoints included the Hemangioma Activity Score (HAS) at 6 months, the change in HAS from baseline to 6 months, and treatment-related complications. The change in HAS was calculated as the baseline HAS minus the 6-month HAS. HAS was used as an activity-based follow-up measure to evaluate dynamic clinical changes during treatment, including changes in lesion color, swelling, and ulceration.
All participants underwent clinical follow-up for 6 to 12 months. The predefined efficacy assessment was performed at the 6-month visit, and the 6-month data were used for the main efficacy analysis. Follow-up beyond 6 months was conducted as routine clinical follow-up and was not used as the primary efficacy time point. Rebound growth after treatment cessation was not prospectively defined or systematically assessed using standardized criteria.
Treatment outcomes were assessed using standardized clinical photographs and HAS scoring. Prior to treatment, all lesions were photographed using the same standardized protocol. Follow-up evaluations were performed to assess changes in lesion color, clinical activity, HAS score, and complications. Two experienced clinicians who were not involved in treatment delivery independently reviewed the coded photographs. Before formal assessment, the assessors were calibrated using representative photographs not included in the final analysis. The assessors were blinded to treatment allocation, and disagreements were resolved by consensus.
Treatment-related complications were defined as ulceration, blistering, eczema, xerotic dermatitis, infection, pigmentation change, or scarring.
Statistical Analysis
Statistical analyses were performed using SPSS. Continuous variables are presented as mean ± standard deviation (SD) for descriptive purposes. For HAS-related outcomes and the number of PDL treatment sessions, distributional statistics, including median, interquartile range (IQR), and range, were additionally reported. Because the number of PDL treatment sessions and HAS scores were ordinal or non-normally distributed variables, between-group comparisons were performed using the Mann–Whitney U-test. Categorical variables were compared using the chi-square test or Fisher’s exact test, as appropriate. A two-sided P value < 0.05 was considered statistically significant.
This study was designed as a single-center exploratory randomized study. No formal a priori sample-size calculation was performed. The sample size of 40 patients was determined based on feasibility, the expected number of eligible infants during the study period, and the exploratory nature of the study.
Results
Formulation Optimization Results
The formulation-screening results are summarized in Supplementary Table 1. HBC-to-2% carteolol ratios from 10:1 to 10:6 produced homogeneous mixtures without visible precipitation and showed thermoresponsive gelation, with gelation temperatures ranging from 18°C to 26°C. In contrast, higher carteolol proportions, particularly 10:7–10:8, showed impaired or absent gelation at 37°C and were therefore considered unsuitable for clinical application. The 10:6 ratio was selected as the final clinical formulation because it represented the highest carteolol-containing ratio that maintained homogeneous mixing, absence of visible precipitation, and stable gel-forming capability.
Baseline Characteristics
A total of 40 patients were included in this study, with a mean age of 35.0 ± 7.7 days. Among them, 31 patients were female (77.5%) and 9 were male (22.5%). Baseline demographic and lesion-related characteristics are summarized in Table 1. No statistically significant differences were observed between the two groups in sex, age, lesion location, potentially higher-risk anatomical location, or baseline HAS. All enrolled lesions met the predefined eligibility criteria of superficial infantile hemangioma with maximum lesion diameter <5 cm and imaging-confirmed lesion thickness of 2–5 mm. Because exact baseline lesion diameter and thickness were not systematically recorded for all participants, these lesion-size variables were presented as eligibility-defined criteria rather than quantitative baseline measurements.
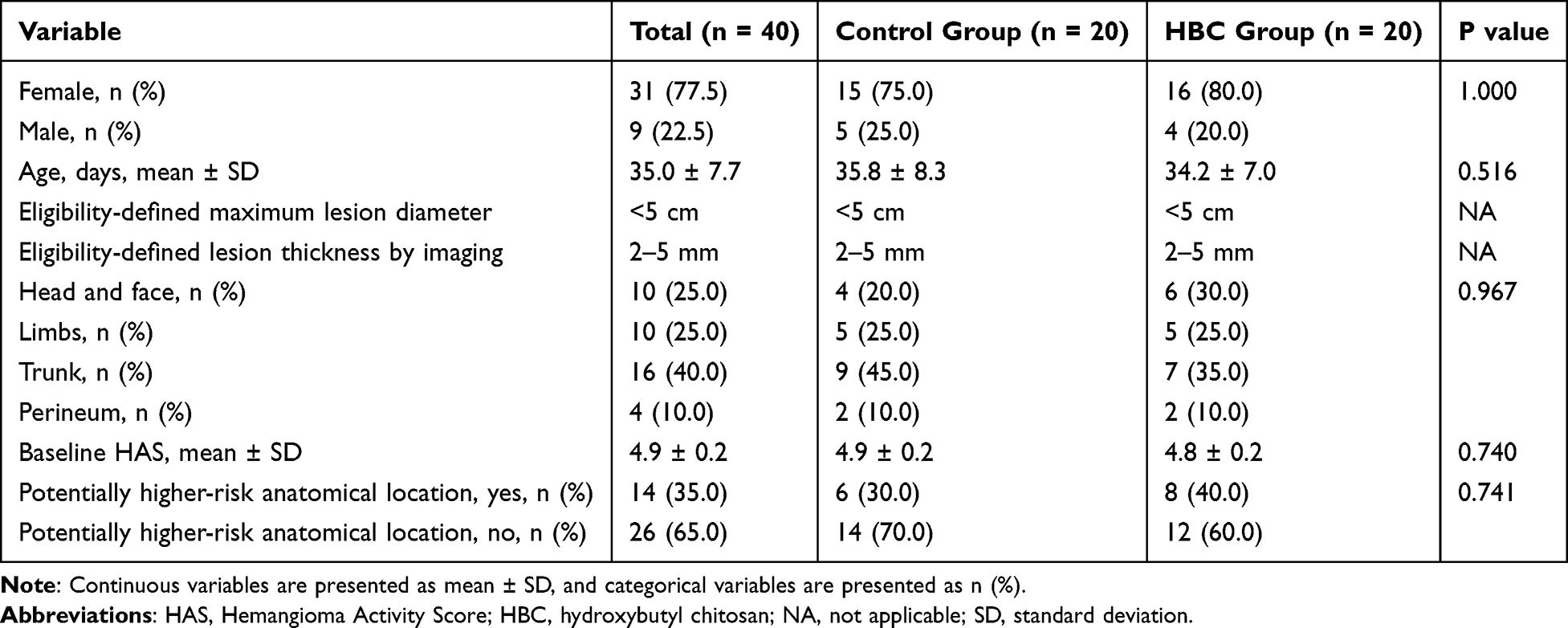 |
Table 1 Baseline Characteristics of the Study Participants |
Participant Flow and Protocol Adherence
All 40 randomized infants received the allocated intervention and completed the predefined 6-month efficacy assessment. Twenty patients were assigned to the HBC group and 20 to the control group, and all were included in the final analysis. No patient withdrew consent, was lost to follow-up before the 6-month assessment, discontinued treatment because of adverse events, or received additional IH-directed therapy outside the study protocol. No major protocol deviations occurred during the study period.
Follow-Up Duration and Timing of Outcome Assessment
The predefined efficacy assessment was performed at the fixed 6-month visit for all randomized patients. All patients in both groups completed the 6-month HAS assessment. Patients who achieved sufficient clinical improvement before 6 months discontinued repeated PDL sessions but continued scheduled follow-up until the fixed 6-month visit; therefore, they were included in the 6-month HAS analysis and were not treated as missing, censored, or excluded observations. The overall follow-up duration ranged from 6 to 12 months, with a mean duration of 8.9 ± 2.1 months. The 6-month data were used for the main efficacy analysis, including HAS-related outcomes and the number of PDL treatment sessions during the 6-month treatment period.
Efficacy Analysis
HAS changes and treatment outcomes during the 6-month treatment period are summarized in Table 2. All randomized patients completed the fixed 6-month HAS assessment and were included in the final analysis. Patients who achieved sufficient clinical improvement before 6 months discontinued repeated PDL sessions but continued scheduled follow-up until the fixed 6-month visit; therefore, they were not treated as missing, censored, or excluded observations.
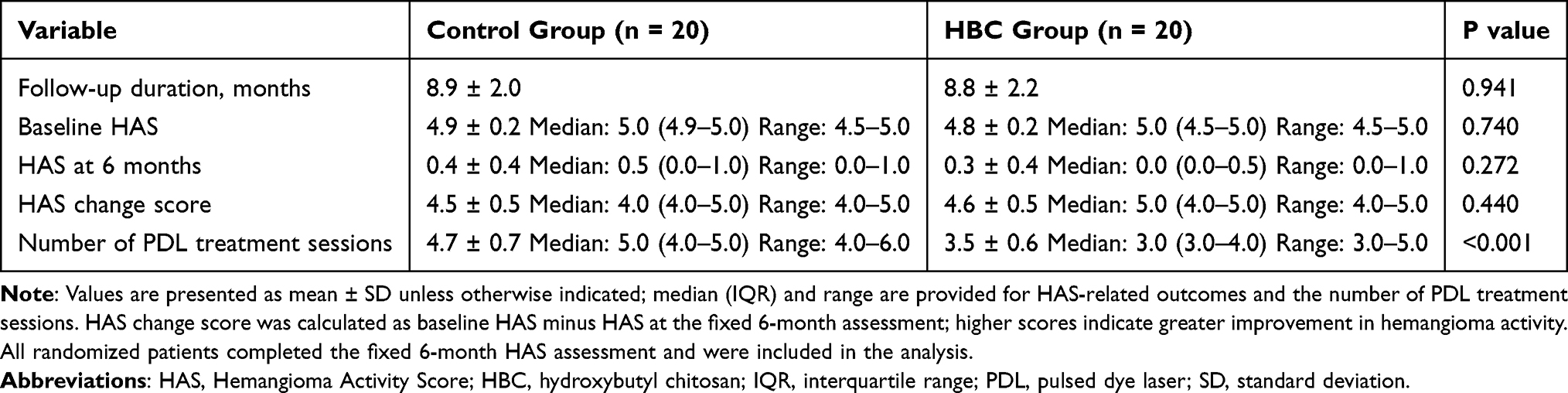 |
Table 2 HAS Changes and Treatment Outcomes During the 6-Month Treatment Period |
The HBC group required fewer PDL treatment sessions than the control group during the 6-month treatment period. The mean number of PDL sessions was 3.5 ± 0.6 in the HBC group and 4.7 ± 0.7 in the control group. The corresponding median values were 3.0 (IQR, 3.0–4.0) and 5.0 (IQR, 4.0–5.0), respectively, confirming that the HBC group required fewer treatment sessions (P < 0.001; Table 2 and Figure 2).
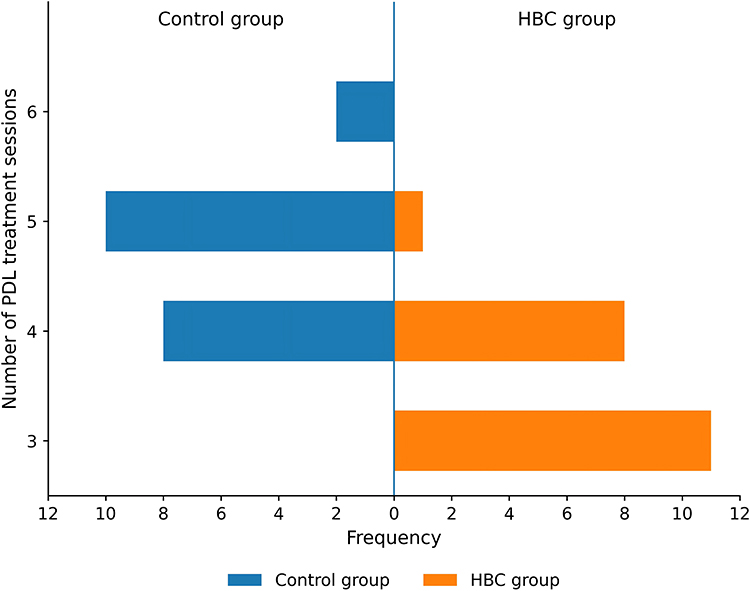 |
Figure 2 Distribution of PDL treatment sessions during the 6-month treatment period. The mirrored frequency plot shows the distribution of the number of PDL treatment sessions completed by infants in the HBC group and the control group during the predefined 6-month treatment period. |
The 6-month HAS was numerically lower in the HBC group than in the control group, but the between-group difference was not statistically significant [0.3 ± 0.4; median, 0.0 (IQR, 0.0–0.5) vs 0.4 ± 0.4; median, 0.5 (IQR, 0.0–1.0), P = 0.272; Table 2]. The HAS change score, calculated as baseline HAS minus HAS at the fixed 6-month assessment, was 4.6 ± 0.5 in the HBC group and 4.5 ± 0.5 in the control group, with no statistically significant between-group difference (P = 0.440; Table 2).
Safety Analysis
Available safety data are summarized in Table 3. Recorded treatment-related local complications occurred in 1 of 20 infants in the HBC group and 7 of 20 infants in the control group, corresponding to aggregate recorded local complication rates of 5.0% and 35.0%, respectively (P = 0.048; Table 3 and Figure 3). No treatment discontinuation due to adverse events was recorded during the 6-month treatment period. Because local complications were recorded at the aggregate level, event subtype, onset time, severity grade, duration, management details, and event-level attribution could not be reliably reconstructed. Systemic beta-blocker-related adverse effects were not assessed using a predefined active monitoring protocol.
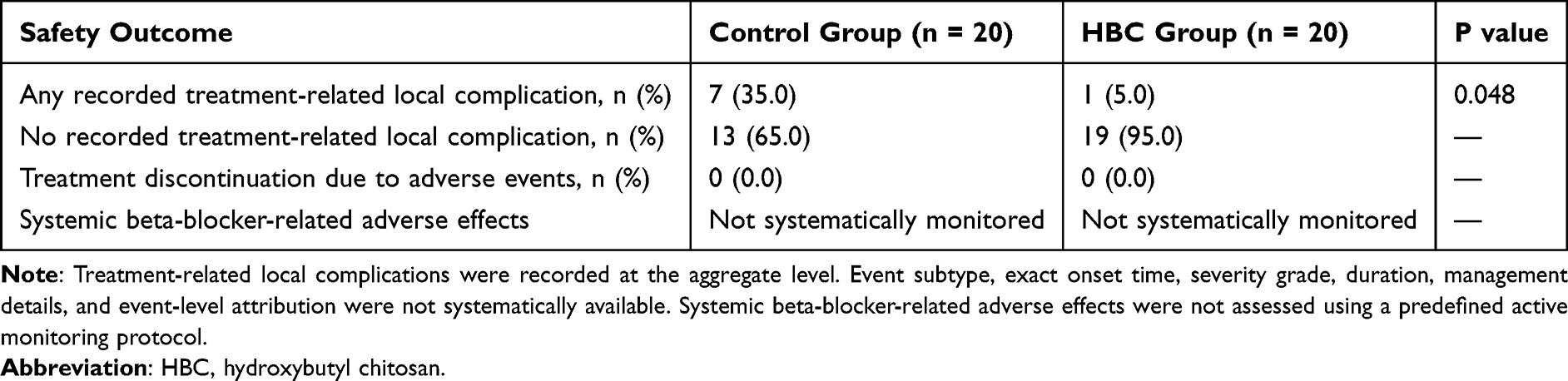 |
Table 3 Summary of Available Safety Data During Treatment and Follow-Up |
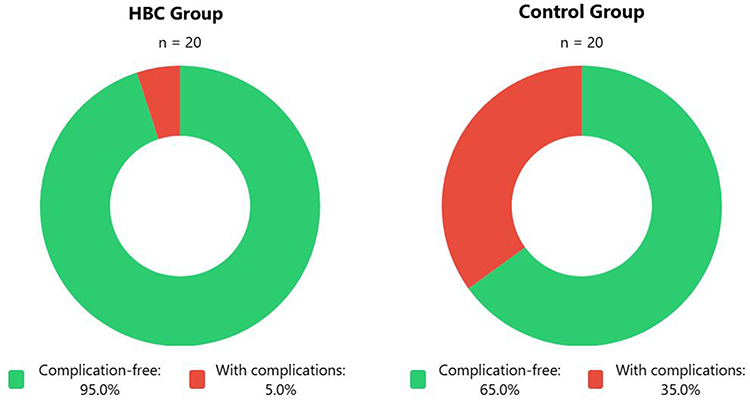 |
Figure 3 Recorded treatment-related local complications during treatment and follow-up. The donut charts show the proportions of infants with and without recorded treatment-related local complications in the HBC group and control group. χ2 = 3.906 P = 0.048. |
Representative Clinical Outcome
Representative clinical photographs showed satisfactory improvement after treatment with the HBC–carteolol–PDL regimen (Figure 4).
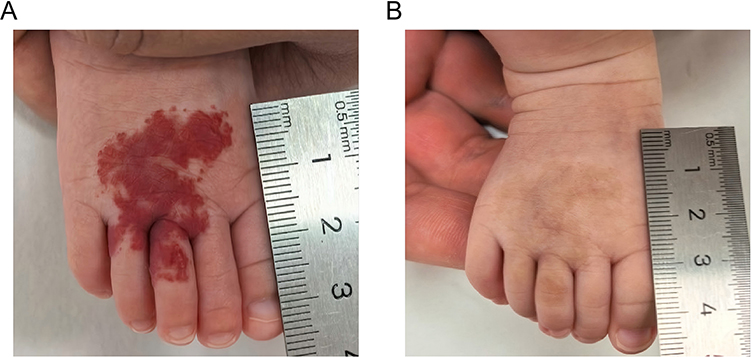 |
Figure 4 Representative clinical photographs of a superficial infantile hemangioma before and after HBC–carteolol–PDL treatment. (A) Before treatment. (B) After three treatment sessions. |
Discussion
In this exploratory randomized study, we evaluated whether a thermoresponsive HBC–carteolol formulation could serve as a local delivery and post-laser care strategy for superficial infantile hemangiomas. The HBC–carteolol–PDL regimen was associated with fewer PDL treatment sessions and a lower recorded rate of local treatment-related complications than conventional carteolol wet-compress therapy combined with PDL. In contrast, 6-month HAS and HAS change score were comparable between the two groups. This pattern of results suggests that the clinical value of the HBC-based regimen may be mainly reflected in reducing treatment burden and improving local post-treatment tolerability, which is relevant to the practical management of superficial IHs requiring repeated laser-based treatment.
Topical β-blockers are already an established therapeutic option for selected superficial IHs, and previous studies have mainly focused on timolol, propranolol, and carteolol-based topical regimens. In this field, β-blocker–laser combination therapy has also been explored, indicating that vascular-selective laser treatment and topical anti-angiogenic therapy may have complementary clinical roles.15 Therefore, the contribution of the present study is not the general concept of topical β-blocker therapy or β-blocker–PDL combination therapy, but the evaluation of a thermoresponsive HBC-based carteolol formulation as a possible local delivery and post-laser care strategy. From a biomaterial perspective, chitosan-based thermoresponsive gels have been reported to undergo sol–gel transition at body temperature and may improve local coverage and drug retention in topical delivery systems.15 In our study, the HBC–carteolol formulation was selected through practical formulation screening, and the 10:6 HBC-to-carteolol ratio maintained homogeneous mixing, absence of visible precipitation, and thermoresponsive gelation, providing a formulation basis for clinical application. Previous studies have suggested that chitosan-based systems may support sustained drug release and improve local drug retention.15 However, because the present study did not include drug-release testing, skin-permeation assays, pharmacokinetic evaluation, or local carteolol concentration measurement, sustained release and enhanced penetration should be considered plausible explanations rather than demonstrated mechanisms.15 Chitosan-based materials have also been reported to possess wound-dressing-related properties, including biocompatibility and potential support for local tissue repair,15 which may partly explain the lower local complication rate observed in the HBC group, although this possibility requires further validation.
From a biological plausibility perspective, topical carteolol may inhibit β-receptor-related angiogenic activity and vascular endothelial cell proliferation, whereas HBC may theoretically function as a local carrier that prolongs contact between carteolol and the lesion surface.9,15 PDL selectively targets hemoglobin-containing superficial vascular structures and remains an established treatment modality for superficial vascular lesions.11 Thus, HBC–carteolol and PDL may have complementary clinical roles, with PDL providing vascular-selective photothermal effects and topical carteolol providing pharmacological suppression of residual angiogenic activity. Nevertheless, this study did not directly assess local drug penetration, endothelial apoptosis, VEGF expression, vascular remodeling, or tissue repair after treatment.11 Similarly, although chitosan-based materials have been associated with wound protection and tissue-repair effects,15 and carteolol has been discussed in relation to angiogenesis-related regulation,9 the present data cannot establish vascular normalization or microcirculatory reconstruction. Thermoresponsive chitosan hydrogels have been reported to have controlled-release potential,17 and chitosan derivatives may influence transdermal delivery through effects on the stratum corneum and local skin microenvironment,15 including possible charge-related interactions with biological interfaces18 and enhanced transdermal delivery in experimental systems.15 PDL-related vascular photothermolysis,11 angiogenesis-related pathways such as VEGF/ANGPT2,19 post-laser inflammatory responses,20 glycolytic regulation in IH biology,16 chitosan-related immunomodulatory effects21 and antibacterial properties22 may provide useful directions for future mechanistic research. However, these processes were not directly examined in the present clinical study and should therefore be described as literature-based hypotheses rather than confirmed mechanisms.
Several limitations should be acknowledged. This was a single-center exploratory randomized study with a relatively small sample size, which limited statistical power and subgroup analyses. Although outcome assessors were blinded, caregivers and treating physicians could not be blinded because the two regimens differed in appearance, application procedure, and dosing frequency; therefore, treatment-delivery decisions, including repeated PDL sessions, may have been influenced by the open-label design. In addition, the comparator was clinically pragmatic but not component-controlled, so the independent contribution of HBC cannot be determined. Baseline lesion size and color characteristics were not quantitatively standardized, and HAS is an activity-based clinical score rather than a fully objective lesion-size or colorimetric endpoint. Finally, although no clinically documented symptomatic bradycardia or hypoglycemia was observed, prospective monitoring of heart rate, blood pressure, and blood glucose was not standardized. Larger multicenter, component-controlled studies with objective lesion assessment and systematic safety monitoring are warranted.
In conclusion, the HBC–carteolol–PDL regimen was associated with fewer treatment sessions and fewer local complications than conventional carteolol wet-compress therapy combined with PDL in infants with superficial IHs. These findings suggest that thermoresponsive HBC may serve as a useful topical post-laser care and local carteolol delivery platform. Further well-designed studies are needed to confirm its independent contribution and clarify the underlying mechanisms.
Conclusion
The thermoresponsive HBC–carteolol–PDL regimen reduced treatment frequency and complication incidence compared with conventional carteolol wet-compress therapy combined with PDL in this single-center randomized study. These findings suggest that HBC may serve as a useful topical delivery and post-laser protective platform for superficial IHs. However, because 6-month HAS-related outcomes did not differ significantly between groups, these findings should be regarded as preliminary and hypothesis-generating. Larger, rigorously controlled trials are needed to confirm the clinical relevance of this regimen.
Data Sharing Statement
The datasets generated during the current study are available from the corresponding author on reasonable request.
Statement of Ethics
This study was conducted in accordance with the World Medical Association Declaration of Helsinki. Informed consents were obtained from the parents of the enrolled infants. The Ethics Committee of Zhangzhou Affiliated Hospital of Fujian Medical University approved this study (No. 2022KYB190, approval date 2022.08).
Funding
This study was funded by NSF grants of Fujian Province (no.2023J011814).
Disclosure
The authors declared no conflicts of interest in this work.
References
1. Krowchuk DP, Frieden IJ, Mancini AJ, et al. Clinical practice guideline for the management of infantile hemangiomas. Pediatrics. 2019;143(1). PMID: 30584062. doi:10.1542/peds.2018-3475
2. Macca L, Altavilla D, Di Bartolomeo L, et al. Update on treatment of infantile hemangiomas: what’s new in the last five years? Front Pharmacol. 2022;13:879602. PMID: 35721150. doi:10.3389/fphar.2022.879602
3. Rodríguez Bandera AI, Sebaratnam DF, Wargon O, Wong LF. Infantile hemangioma. Part 1: epidemiology, pathogenesis, clinical presentation and assessment. J Am Acad Dermatol. 2021;85(6):1379–12. PMID: 34419524. doi:10.1016/j.jaad.2021.08.019
4. Leñero-Bardallo JA, Acha B, Serrano C, Pérez-Carrasco JA, Ortiz-álvarez J, Bernabéu-Wittel J. Thermography as a method for bedside monitoring of infantile hemangiomas. Cancers. 2022;14(21):5392. PMID: 36358809. doi:10.3390/cancers14215392
5. Chan H, McKay C, Adams S, Wargon O. RCT of timolol maleate gel for superficial infantile hemangiomas in 5- to 24-week-olds. Pediatrics. 2013;131(6):e1739–1747. PMID: 23650294. doi:10.1542/peds.2012-3828
6. Khan M, Boyce A, Prieto-Merino D, Svensson Å, Wedgeworth E, Flohr C. The role of topical timolol in the treatment of infantile hemangiomas: a systematic review and meta-analysis. Acta Derm Venereol. 2017;97(10):1167–1171. PMID: 28421234. doi:10.2340/00015555-2681
7. Muñoz-Garza FZ, Ríos M, Roé-Crespo E, et al. Efficacy and safety of topical timolol for the treatment of infantile hemangioma in the early proliferative stage: a randomized clinical trial. JAMA Dermatol. 2021;157(5):583–587. PMID: 33825828. doi:10.1001/jamadermatol.2021.0596
8. Chakhunashvili K, Kvirkvelia E, Chakhunashvili DG. Atypical development and swift resolution of an ulcerated hemangioma: a case report. J Med Case Rep. 2025;19(1):352. PMID: 40682105. doi:10.1186/s13256-025-05422-9
9. Sebaratnam DF, Rodríguez Bandera AL, Wong LF, Wargon O. Infantile hemangioma. Part 2: management. J Am Acad Dermatol. 2021;85(6):1395–1404. PMID: 34419523. doi:10.1016/j.jaad.2021.08.020
10. Gan LQ, Wang H, Ni SL, Tan CH. A prospective study of topical carteolol therapy in Chinese infants with superficial infantile hemangioma. Pediatr Dermatol. 2018;35(1):121–125. PMID: 29243341. doi:10.1111/pde.13361
11. Hashemi DA, Tao J, Wang JV, Geronemus RG. The 595-nm wavelength pulsed dye laser for pediatric port-wine birthmarks and infantile hemangiomas: A systematic review. Lasers Surg Med. 2025;57(1):27–36. PMID: 39682011. doi:10.1002/lsm.23864
12. Zou Y, Wu Z, Jin P, et al. Historical and contemporary management of infantile hemangiomas: a single-center experience. Front Pharmacol. 2024;15:1280948. PMID: 38370473. doi:10.3389/fphar.2024.1280948
13. Tawfik AA, Alsharnoubi J. Topical timolol solution versus laser in treatment of infantile hemangioma: a comparative study. Pediatr Dermatol. 2015;32(3):369–376. PMID: 25740672. doi:10.1111/pde.12542
14. Asilian A, Mokhtari F, Kamali AS, Abtahi-Naeini B, Nilforoushzadeh MA, Mostafaie S. Pulsed dye laser and topical timolol gel versus pulse dye laser in treatment of infantile hemangioma: a double-blind randomized controlled trial. Adv Biomed Res. 2015;4:257. PMID: 26918239. doi:10.4103/2277-9175.170682
15. Ma J, Wang Y, Lu R. Mechanism and application of chitosan and its derivatives in promoting permeation in transdermal drug delivery systems: a review. Pharmaceuticals. 2022;15(4):459. PMID: 35455456. doi:10.3390/ph15040459
16. Marques AC, Costa PC, Velho S, Amaral MH. Injectable poloxamer hydrogels for local cancer therapy. Gels. 2023;9(7):593. PMID: 37504472. doi:10.3390/gels9070593
17. Zhao J, Qiu P, Wang Y, et al. Chitosan-based hydrogel wound dressing: from mechanism to applications, a review. Int J Biol Macromol. 2023;244:125250. PMID: 37307982. doi:10.1016/j.ijbiomac.2023.125250
18. Egorov AR, Kirichuk AA, Rubanik VV, Rubanik VV, Tskhovrebov AG, Kritchenkov AS. Chitosan and its derivatives: preparation and antibacterial properties. Materials. 2023;16(18):6076. PMID: 37763353. doi:10.3390/ma16186076
19. Xiang S, Gong X, Qiu T, et al. Insights into the mechanisms of angiogenesis in infantile hemangioma. Biomed Pharmacother. 2024;178:117181. PMID: 39059349. doi:10.1016/j.biopha.2024.117181
20. Chelleri C, Monzani NA, Gelmetti C, et al. Residual lesions after pharmacological and dye-laser treatment of infantile hemangiomas: critical review of 432 cases. Lasers Surg Med. 2020;52(7):597–603. PMID: 31828809. doi:10.1002/lsm.23205
21. Tang W, Wang J, Hou H, et al. Review: application of chitosan and its derivatives in medical materials. Int J Biol Macromol. 2023;240:124398. PMID: 37059277. doi:10.1016/j.ijbiomac.2023.124398
22. Thirupathi K, Raorane CJ, Ramkumar V, et al. Update on chitosan-based hydrogels: preparation, characterization, and its antimicrobial and antibiofilm applications. Gels. 2022;9(1):35. PMID: 36661802. doi:10.3390/gels9010035
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.