Back to Journals » Clinical Ophthalmology » Volume 16
Thermal Pulsation with or without Dexamethasone Intracanalicular Insert for Meibomian Gland Dysfunction: A Prospective, Masked Trial
Authors Dierker DS ![]() , Hauswirth SG
, Hauswirth SG
Received 24 January 2022
Accepted for publication 28 April 2022
Published 12 May 2022 Volume 2022:16 Pages 1477—1485
DOI https://doi.org/10.2147/OPTH.S359719
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Damon S Dierker,1 Scott G Hauswirth2
1Eye Surgeons of Indiana, Indianapolis, IN, USA; 2Department of Ophthalmology, Sue-Anschutz-Rodgers Eye Center, University of Colorado School of Medicine, Aurora, CO, USA
Correspondence: Damon S Dierker, Eye Surgeons of Indiana, 9202 N Meridian St, #100, Indianapolis, IN, 46260, USA, Email [email protected]
Significance: Meibomian gland dysfunction (MGD) is among the most common causes of dry eye disease worldwide. Few studies have compared treatment options, and the basis for an evidentiary approach to MGD management is lacking. We have conducted a non-randomized trial evaluating the additive benefit of a recently developed therapy.
Purpose: To compare the efficacy of thermal pulsation therapy alone or combined with the dexamethasone intracanalicular insert (Dextenza) on the signs and symptoms of MGD.
Methods: This was a prospective, patient-masked, sham-controlled, non-randomized trial. All subjects underwent thermal pulsation therapy using the LipiFlow system. The dexamethasone intracanalicular insert was placed in the inferior canaliculus of the more symptomatic eye (DEX group), while sham punctal dilation of the fellow eye was performed to preserve patient masking (SHAM group). Key outcomes were improvement in meibum expressibility at 1, 4, and 12 weeks and patient treatment preference at week 12.
Results: Nineteen subjects underwent thermal pulsation therapy and received the DEX insert. Meibomian gland expressibility scores improved significantly in both groups at 1, 4, and 12 weeks, with significantly greater improvement in DEX eyes than SHAM eyes at 12 weeks (P=0.027). Improvement from baseline in TBUT was significant at all time points in DEX eyes and only at week 4 in SHAM eyes, with significantly greater improvement in DEX eyes over SHAM eyes at week 12 (P=0.028). Mean best-corrected visual acuity and intraocular pressure remained unchanged from baseline throughout follow-up in both groups, and no adverse events were noted. Combined therapy with DEX was preferred by 61% of subjects.
Conclusion: This study demonstrated a significant benefit of combining thermal pulsation therapy with the dexamethasone intracanalicular insert on signs of MGD including TBUT and meibomian gland expressibility score. Consequently, a majority of patients preferred combination therapy to thermal pulsation therapy alone.
Keywords: Dextenza, dexamethasone, LipiFlow, thermal pulsation therapy, meibomian gland dysfunction
Introduction
Meibomian gland dysfunction (MGD) is defined by the Tear Film and Ocular Surface Society (TFOS) as
a chronic, diffuse abnormality of the meibomian glands, commonly characterized by terminal duct obstruction and/or qualitative/quantitative changes in the glandular secretion … [that] may result in alteration of the tear film, symptoms of eye irritation, clinically apparent inflammation, and ocular surface disease
and may be the leading cause of dry eye disease throughout the world.1 Its prevalence ranges from ~4–20% in Caucasian populations and may affect more than 60% of some Asian populations.1
Due to a paucity of well-designed and appropriately powered clinical studies, the clinical approach to MGD is neither standardized nor evidence-based. Lid hygiene, coupled with lid warming and compression, are commonly recommended, but instructions by providers and techniques employed by patients vary significantly. Antibiotics with or without steroids are also commonly prescribed, with a meta-analysis demonstrating the benefits of topical azithromycin on short-term improvement of tear film quality2 and several studies demonstrating improvements in tear film inflammatory mediators, gland expressibility, and/or clinical symptoms with the use of topical corticosteroids.3–5
Integrated systems utilizing a combination of heat and directed pressure on the eyelids to facilitate expression of meibum from inspissated or blocked meibomian glands have been developed and commercialized for the treatment of MGD.6 One such system (LipiFlow, Johnson & Johnson) is designed to warm the lid to soften and liquify meibum and compress the lid with a series of peristaltic proximal-to-distal pulses to express liquified meibum from dysfunctional glands. In its pivotal trial and subsequent studies, this therapy significantly improved both meibomian gland function and clinical symptoms of ocular surface disease.6–10
We have conducted a prospective subject-masked trial to compare the effects of thermal pulsation therapy with the LipiFlow system with or without the dexamethasone intracanalicular insert (Dextenza, Ocular Therapeutix) on the signs and symptoms of MGD. The insert is a rod-shaped hydrogel matrix incorporating 0.4 mg preservative-free dexamethasone, is placed in the canaliculus, and provides sustained-release delivery of dexamethasone to the ocular surface for 30 days.11–13 It is currently approved in the United States for the control of postoperative pain and inflammation following ocular surgery.14
Methods
This was a single-center, open-label, prospective, non-randomized, subject-masked, sham-controlled trial. The protocol was reviewed and approved by the Western IRB on 7/2/2020. The study was registered at ClinicalTrials.gov (NCT04413279) on 6/2/2020. Participants were enrolled between 8/5/2020 and 4/14/2021; all participants provided written informed consent. The study was conducted in accordance with the tenets of the Declaration of Helsinki.15
Eligible subjects were adults aged 18 years or older with history of evaporative dry eye disease, meibomian gland dysfunction, and clinically significant inflammation as evidenced by ocular surface staining and/or conjunctival hyperemia and/or elevated MMP-9 levels. Exclusion criteria included ocular or nonocular infection, compromised nasolacrimal flow, or concurrent use of or contraindications to corticosteroids. Consecutive eligible subjects were invited to participate in the study.
All subjects underwent a clinical evaluation to establish eligibility consisting of uncorrected and best-corrected visual acuity (UCVA and BCVA), meibomian gland assessment, tear film osmolarity (TearLab) and matrix metalloproteinase 9 (MMP-9; Inflammadry, Quidel) assessment, corneal fluorescein and conjunctival lissamine green staining, tear break-up time (TBUT), intraocular pressure (IOP), and a dilated eye examination. Meibomian gland assessment mirrored the methodology in the pivotal LipiFlow trial10 and consisted of grading the quality of meibum expression from 15 glands along the lower eyelid, 5 each from the temporal, central, and nasal regions, and each graded on a 0–3 scale as follows: 3, clear liquid secretions; 2, cloudy liquid secretions; 1, inspissated/toothpaste consistency; and 0, no secretions. A composite meibomian gland expressibility score ranging from 0 to 45 (with lower scores representing worse disease) was tabulated by summing the grades of all 15 glands assessed. Corneal fluorescein staining was graded from 0 to 3 (none to heavy staining) in five regions (superior, inferior, nasal, temporal, and central) and summed for a corneal staining score. Conjunctival lissamine green staining was graded on the same 0–3 scale in 6 regions (3 nasal and 3 temporal) and summed for a conjunctival staining score. Corneal and conjunctival scores were summed to produce an overall ocular surface staining score. Subjects also completed the validated DEQ-5 Dry Eye Questionnaire, which characterizes the presence and severity of ocular discomfort, dryness, and watering; possible scores range from 0 to 22 with higher scores representing worse symptoms.16
Qualifying subjects underwent bilateral thermal pulsation therapy with the LipiFlow system 1–30 days later. The procedure has been described in detail previously8–10 and was performed in accordance with the manufacturer’s directions. Briefly, under topical anesthesia, the activator was placed on the eye such that the corneal shield rested on the ocular surface (vaulting the cornea to protect it from heat) and the inflatable bladder rested on the lid surface. Over a 12-minute treatment period, the lids were gently heated and expressed with repeated vectored pressure pulses. Following the procedure, the DEX insert was placed in the inferior canaliculus of the more symptomatic eye (the DEX group), and the inferior punctum of the fellow eye was dilated using a punctal dilator to mimic insert placement to achieve patient masking to treatment (the SHAM group). No anti-inflammatory therapy was applied to the SHAM eye during the study, although patients were permitted to continue warm compresses and lid scrubs in either or both eyes at their discretion, and to continue habitual dry eye treatments such as topical immunomodulators and/or oral omega fatty acid supplements. Subjects were re-evaluated 1, 4, and 12 weeks later, at which time all assessments listed above were repeated and safety assessed. Additionally at week 12, subjects completed the validated Comparisons of Ophthalmic Medications for Tolerability (COMTOL) questionnaire17 adapted for the treatments utilized in this study.
The first key outcome measure of this study was the change from baseline in meibomian gland expressibility scores at weeks 1, 4, and 12 and was compared between treatment groups using paired t-tests as between-group data were drawn from correlated fellow-eye pairs. The second key outcome measure was patient preference for therapy as measured by the COMTOL instrument at week 12. Secondary outcomes included mean changes in BCVA, tear film osmolarity, MMP-9 positivity rates, ocular surface staining scores, TBUT, and DEQ-5 scores from baseline to weeks 1, 4, and 12; these were also analyzed using paired t-tests except for the dichotomous MMP-9 parameter for which the Fisher Exact Test was utilized. Safety outcomes included the nature and incidence of adverse events. No formal power analysis was conducted a priori; rather, a convenience sample consistent with recent prior studies of similar design and purpose (40 eyes of 20 subjects) was selected.18–20
Results
Overall, 20 subjects were enrolled. No patients had previously undergone microblepharoexfoliation, thermal pulsation, or intense pulsed light therapy in the past 12 months. Their mean (standard deviation) age was 59.2 (11.1) years, 18/20 (90%) were female, and 19/20 (95%) identified themselves as white. DEX insertion was not possible in 1 subject who was excluded from all outcomes analyses; all other subjects completed the trial.
Mean meibomian gland expressibility scores and other outcomes data at each time point are given in Table 1. In DEX-treated eyes, significant improvements from baseline were seen in meibomian gland expressibility scores at post-treatment time points (P<0.0001), ocular surface staining scores at 1 (P=0.035) and 4 weeks (P<0.001), and TBUT at all time points (P<0.037). In SHAM-treated eyes, significant improvements from baseline were seen in expressibility scores at all time points (P<0.0001) and TBUT at week 4 (P=0.020). Significantly greater improvements were seen in DEX eyes compared to SHAM eyes for expressibility scores at 12 weeks (P=0.027), ocular surface staining score at 4 weeks (P=0.028), and TBUT at 12 weeks (P=0.028). In both treatment groups, the rate of MMP-9 positivity decreased by 16–46% across all visits; these were not significant changes within or between groups. Significantly greater improvements in SHAM eyes compared to DEX eyes were not seen for any parameters at any time point.
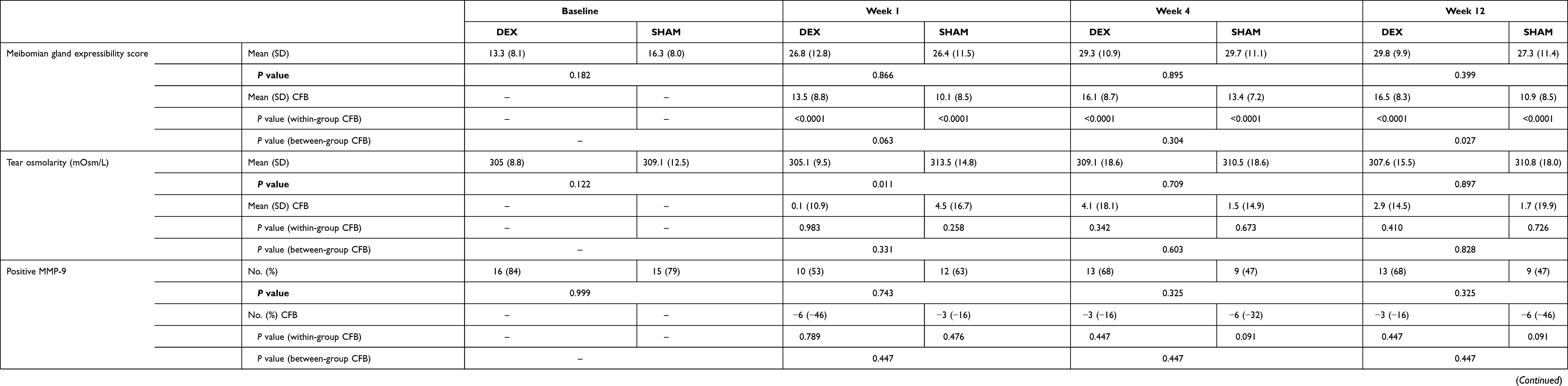 |
Table 1 Meibomian Gland Expressibility Scores and Other Endpoint Data by Treatment Group and Time Point |
Symptom scores on the DEQ-5 improved from baseline at each post-treatment visit. Mean DEQ-5 scores were 12.3 (4.4) at baseline, 11.1 (4.7) at week 1 (P=0.132), 10.3 (5.1) at week 4 (P=0.078), and 9.1 (5.9) at week 12 (P=0.019). The DEQ-5 is an individual-level and not eye-level instrument and cannot assess differences between eyes. The COMTOL instrument, however, is designed to compare treatment experiences in subjects exposed to both treatments. Of the 18 subjects reporting a treatment preference using the COMTOL instrument, 11 (61.1%) preferred LipiFlow with DEX and 7 (38.9%) preferred LipiFlow with SHAM. One subject reported no preference between treatments.
Both the thermal pulsation therapy and the DEX insert were safe and well tolerated in this sample. No adverse events were noted in either group. Mean BCVA and IOP remained stable throughout follow-up (Table 2). No patients had an IOP rise >10 mmHg; a single patient had an 8-mm IOP rise in the eye receiving DEX from 15 mmHg at baseline to 23 mmHg at week 4 that resolved without intervention.
 |
Table 2 Best-Corrected Visual Acuity (BCVA) and Intraocular Pressure (IOP) Safety Data by Treatment Group and Time Point |
Discussion
In this prospective, sham-controlled, non-randomized study, thermal pulsation therapy + DEX provided significantly greater improvement in meibomian gland expressibility and TBUT at 12 weeks and in ocular surface staining at 4 weeks compared to thermal pulsation therapy + SHAM. The majority (61%) of patients undergoing thermal pulsation lid therapy for symptomatic MGD preferred combined therapy with the DEX insert over sham therapy (39%). The interventions assessed in this study were safe and well tolerated by all study participants.
The therapeutic benefits of thermal pulsation lid therapy on symptomatic MGD have been thoroughly characterized in the literature6,8,10,21–41 and a meta-analysis demonstrated its superiority over warm compress treatment for treating dry eye disease.42 The benefit of corticosteroid therapy for MGD is less well characterized. In general, brief therapy with steroids are beneficial in the setting of acute inflammatory flares of ocular surface disease, while the long-term side effects of steroids—including elevated IOP and cataract formation—preclude their chronic use.43–45
The DEX insert is a formulation of dexamethasone designed for sustained-release drug delivery over a 30-day period.11–13 It is approved in the United States for the control of pain and inflammation following ocular surgery,14 and its role in postoperative care has been demonstrated following cataract extraction in adults11,12,46–48 and children,49 pars plana vitrectomy,20 as well as refractive surgical procedures.18,19,50 Phase 2 and 3 trials have also evaluated DEX for chronic inflammation associated with allergic conjunctivitis and reported short-term improvements in itching and conjunctival hyperemia.51–53 Given the role of inflammation in MGD, we hypothesized in this study that DEX may provide additional therapeutic benefit when combined with thermal pulsation therapy for MGD. The DEX insert has several features to support this hypothesis. First, it provides short-term pulsed therapy with a diminishing dose over time to minimize complications related to IOP and cataract formation54,55 and with minimal systemic absorption.56 Second, it is preservative-free, which is important given the pro-inflammatory nature of preservatives in ophthalmic formulations and their adverse effects on ocular surface disease.57 Third, its anti-inflammatory mechanism of action is complementary to that of thermal pulsation therapy, favoring additivity of efficacy.
In this study, both treatment groups demonstrated significant improvements in meibomian gland expressibility, but the improvement was significantly greater in eyes treated with thermal pulsation therapy + DEX. Similarly, TBUT was significantly improved in the DEX (but not the SHAM) group at 12 weeks, and ocular surface staining was improved in the DEX (but not the SHAM) group at week 4. All of the significant within-group changes from baseline indicated improvement, and all significant between-group differences favored combination therapy with DEX. This was an expected outcome of the study, as prior studies supported the benefits of corticosteroid therapy for MGD.3–5 Thus it is likely that patient preference favored combination therapy given the better outcomes in this group.
Strengths of this study include its prospective nature as well as the use of sham therapy for subject masking. Limitations include both a relatively small sample size and a short study duration given the chronic nature of MGD.
In summary, we have demonstrated a significant benefit of combining thermal pulsation therapy with the dexamethasone intracanalicular insert on signs of MGD including TBUT and meibomian gland expressibility score. Consequently, the majority of patients preferred combination therapy to thermal pulsation therapy alone.
Data Sharing Statement
The investigators will consider reasonable requests for sharing of the de-identified data set upon request to the corresponding author.
Funding
Sponsorship for this study was provided by Ocular Therapeutix.
Disclosure
Dr Damon S Dierker reports grants and personal fees from Ocular Therapeutix, during the conduct of the study; personal fees from Aerie, Alcon, Allergan, Azura, Bio-Tissue, Eyevance, Johnson & Johnson, Kala Pharmaceuticals, Lumenis, Novartis, Oyster Point Pharma, Quidel, ScienceBased Health, Scope, Sight Sciences, Sun Pharma, Tarsus, TearLab, and Thea Pharmaceuticals, outside the submitted work. Dr Scott G Hauswirth reports personal fees from Ocular Therapeutix, during the conduct of the study; personal fees from Dompe, Kala Pharmaceuticals, Sun Pharmaceuticals, Takeda, Oyster Point, Sight Sciences, Horizon Pharmaceuticals, and NuSight Medical; non-financial support from TearRestore and Science Based Health for advisory work, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Nichols KK, Foulks GN, Bron AJ, et al. The international workshop on meibomian gland dysfunction: executive summary. Invest Ophthalmol Vis Sci. 2011;52(4):1922–1929. doi:10.1167/iovs.10-6997a
2. Tao T, Tao L. Systematic review and meta-analysis of treating meibomian gland dysfunction with azithromycin. Eye. 2020;34(10):1797–1808. doi:10.1038/s41433-020-0876-2
3. Ko JS, Seo Y, Chae MK, Jang SY, Yoon JS. Effect of topical loteprednol etabonate with lid hygiene on tear cytokines and meibomian gland dysfunction in prosthetic eye wearers. Eye. 2018;32(2):439–445. doi:10.1038/eye.2017.213
4. Lee H, Chung B, Kim KS, Seo KY, Choi BJ, Kim TI. Effects of topical loteprednol etabonate on tear cytokines and clinical outcomes in moderate and severe meibomian gland dysfunction: randomized clinical trial. Am J Ophthalmol. 2014;158(6):1172–1183 e1. doi:10.1016/j.ajo.2014.08.015
5. Akyol-Salman I, Azizi S, Mumcu UY, Ates O, Baykal O. Comparison of the Efficacy of Topical N-Acetyl-Cysteine and a Topical Steroid-Antibiotic Combination Therapy in the Treatment of Meibomian Gland Dysfunction. J Ocul Pharmacol Ther. 2011;1:43. doi:10.1089/jop.2010.0110
6. Tauber J, Owen J, Bloomenstein M, Hovanesian J, Bullimore MA. Comparison of the iLUX and the LipiFlow for the Treatment of Meibomian Gland Dysfunction and Symptoms: a Randomized Clinical Trial. Clinical Ophthalmology (Auckland, NZ. 2020;14:405–418. doi:10.2147/OPTH.S234008
7. Finis D, Konig C, Hayajneh J, Borrelli M, Schrader S, Geerling G. Six-month effects of a thermodynamic treatment for MGD and implications of meibomian gland atrophy. Randomized Controlled Trial. Cornea. 2014;33(12):1265–1270. doi:10.1097/ICO.0000000000000273
8. Greiner JV. Long-term (12-month) improvement in meibomian gland function and reduced dry eye symptoms with a single thermal pulsation treatment. Clin Exp Ophthalmol. 2013;41(6):524–530. doi:10.1111/ceo.12033
9. Greiner JV. A single LipiFlow(R) Thermal Pulsation System treatment improves meibomian gland function and reduces dry eye symptoms for 9 months. Current Eye Research. 2012;37(4):272–278. doi:10.3109/02713683.2011.631721
10. Lane SS, DuBiner HB, Epstein RJ, et al. A new system, the LipiFlow, for the treatment of meibomian gland dysfunction. Cornea. 2012;31(4):396–404. doi:10.1097/ICO.0b013e318239aaea
11. Tyson SL, Bafna S, Gira JP, et al. Multicenter randomized Phase 3 study of a sustained-release intracanalicular dexamethasone insert for treatment of ocular inflammation and pain after cataract surgery. J Cataract Refract Surg. 2019;45(2):204–212. doi:10.1016/j.jcrs.2018.09.023
12. Walters T, Bafna S, Vold S, et al. Efficacy and Safety of Sustained Release Dexamethasone for the Treatment of Ocular Pain and Inflammation after Cataract Surgery: results from Two Phase 3 Studies. J Clin Exp Ophthalmol. 2016;7:1–11.
13. Lee A, Blair HA. Dexamethasone Intracanalicular Insert: a Review in Treating Post-Surgical Ocular Pain and Inflammation. Drugs. 2020;80(11):1101–1108. doi:10.1007/s40265-020-01344-6
14. Ocular Therapeutix, Inc. Dextenza. Highlights of Prescribing Information. Available from: https://www.dextenza.com/wp-content/uploads/2019/06/NDA-208742-S001-Dextenza-labeling-19Jun19.pdf.
15. World Medical A. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
16. Chalmers RL, Begley CG, Caffery B. Validation of the 5-Item Dry Eye Questionnaire (DEQ-5): discrimination across self-assessed severity and aqueous tear deficient dry eye diagnoses. Cont Lens Anterior Eye. 2010;33(2):55–60. doi:10.1016/j.clae.2009.12.010
17. Barber BL, Strahlman ER, Laibovitz R, Guess HA, Reines SA. Validation of a questionnaire for comparing the tolerability of ophthalmic medications. Ophthalmology. 1997;104(2):334–342.
18. Greenwood MD, Gorham RA, Boever KR. A Randomized Fellow-Eye Clinical Trial to Evaluate Patient Preference for Dexamethasone Intracanalicular Insert or Topical Prednisolone Acetate for Control of Postoperative Symptoms Following Bilateral Femtosecond Laser in Site Keratomileusis (LASIK). Clinical Ophthalmology (Auckland, NZ. 2020;14:2223–2228. doi:10.2147/OPTH.S265311
19. Larsen J, Whitt T, Parker B, Swan R. A Randomized, Controlled, Prospective Study of the Effectiveness and Safety of an Intracanalicular Dexamethasone Ophthalmic Insert (0.4 Mg) for the Treatment of Post-Operative Inflammation in Patients Undergoing Refractive Lens Exchange (RLE). Clinical Ophthalmol. 2021;15:2211–2217. doi:10.2147/OPTH.S311070
20. Suner IJ, Peden MC. Dexamethasone Sustained-Release Intracanalicular Insert for Control of Postoperative Inflammation After Pars Plana Vitrectomy. Clinical Ophthalmology (Auckland, NZ. 2021;15:3859–3864. doi:10.2147/OPTH.S330255
21. Park J, Yoo YS, Shin K, et al. Effects of Lipiflow Treatment Prior to Cataract Surgery: a Prospective, Randomized, Controlled Study: lipiflow prior to cataract surgery. Am J Ophthalmol. 2021;1:34. doi:10.1016/j.ajo.2021.04.031
22. Chan AYY, Chuang JC, Wong VWY. Evaluation of Meibomian Gland Dysfunction Among Ophthalmic Healthcare Workers. Clinical Ophthalmology (Auckland, NZ. 2021;15:1201–1206. doi:10.2147/OPTH.S299338
23. Zhao Y, Li J, Xue K, et al. Preoperative Management of MGD with Vectored Thermal Pulsation before Cataract Surgery: a Prospective, Controlled Clinical Trial. Semin Ophthalmol. 2021;36(1–2):2–8. doi:10.1080/08820538.2021.1881567
24. Fallah S, Loer CJ. Effects of Vectored Thermal Pulsation on Objective Tear Film Measures. Cornea. 2021;12:76. doi:10.1097/ICO.0000000000002714
25. Li B, Fu H, Liu T, Xu M. Comparison of the therapeutic effect of Meibomian Thermal Pulsation LipiFlow(R) on obstructive and hyposecretory meibomian gland dysfunction patients. Int Ophthalmol. 2020;40(12):3469–3479. doi:10.1007/s10792-020-01533-y
26. Hura AS, Epitropoulos AT, Czyz CN, Rosenberg ED. Visible Meibomian Gland Structure Increases After Vectored Thermal Pulsation Treatment in Dry Eye Disease Patients with Meibomian Gland Dysfunction. Clinical Ophthalmol. 2020;14:4287–4296. doi:10.2147/OPTH.S282081
27. Matossian C. Impact of Thermal Pulsation Treatment on Astigmatism Management and Outcomes in Meibomian Gland Dysfunction Patients Undergoing Cataract Surgery. Clinical Ophthalmology (Auckland, NZ. 2020;14:2283–2289. doi:10.2147/OPTH.S263046
28. Tauber J. A 6-Week, Prospective, Randomized, Single-Masked Study of Lifitegrast Ophthalmic Solution 5% Versus Thermal Pulsation Procedure for Treatment of Inflammatory Meibomian Gland Dysfunction. Cornea. 2020;39(4):403–407. doi:10.1097/ICO.0000000000002235
29. Hagen KB, Bedi R, Blackie CA, Christenson-Akagi KJ. Comparison of a single-dose vectored thermal pulsation procedure with a 3-month course of daily oral doxycycline for moderate-to-severe meibomian gland dysfunction. Clinical Ophthalmology (Auckland, NZ. 2018;12:161–168. doi:10.2147/OPTH.S150433
30. Godin MR, Stinnett SS, Gupta PK. Outcomes of Thermal Pulsation Treatment for Dry Eye Syndrome in Patients With Sjogren Disease. Cornea. 2018;37(9):1155–1158. doi:10.1097/ICO.0000000000001621
31. Blackie CA, Coleman CA, Nichols KK, et al. A single vectored thermal pulsation treatment for meibomian gland dysfunction increases mean comfortable contact lens wearing time by approximately 4 hours per day. Clinical Ophthalmology (Auckland, NZ. 2018;12:169–183. doi:10.2147/OPTH.S153297
32. Epitropoulos AT, Goslin K, Bedi R, Blackie CA. Meibomian gland dysfunction patients with novel Sjogren’s syndrome biomarkers benefit significantly from a single vectored thermal pulsation procedure: a retrospective analysis. Clinical Ophthalmology (Auckland, NZ. 2017;11:701–706. doi:10.2147/OPTH.S119926
33. Schallhorn CS, Schallhorn JM, Hannan S, Schallhorn SC. Effectiveness of an Eyelid Thermal Pulsation Procedure to Treat Recalcitrant Dry Eye Symptoms After Laser Vision Correction. J Refract Surg. 2017;33(1):30–36. doi:10.3928/1081597X-20161006-05
34. Kim MJ, Stinnett SS, Gupta PK. Effect of thermal pulsation treatment on tear film parameters in dry eye disease patients. Clinical Ophthalmology (Auckland, NZ. 2017;11:883–886. doi:10.2147/OPTH.S136203
35. Gibbons A, Waren D, Yesilirmak N, et al. Ocular Surface Parameters Predicting Patient Satisfaction After a Single Vectored Thermal Pulsation Procedure for Management of Symptomatic Meibomian Gland Dysfunction. Cornea. 2017;36(6):679–683. doi:10.1097/ICO.0000000000001196
36. Zhao Y, Veerappan A, Yeo S, et al. Clinical Trial of Thermal Pulsation (LipiFlow) in Meibomian Gland Dysfunction With Preteatment Meibography. Eye Contact Lens. 2016;42(6):339–346. doi:10.1097/ICL.0000000000000228
37. Blackie CA, Coleman CA, Holland EJ. The sustained effect (12 months) of a single-dose vectored thermal pulsation procedure for meibomian gland dysfunction and evaporative dry eye. Clinical Ophthalmology (Auckland, NZ. 2016;10:1385–1396. doi:10.2147/OPTH.S109663
38. Greiner JV. Long-Term (3 Year) Effects of a Single Thermal Pulsation System Treatment on Meibomian Gland Function and Dry Eye Symptoms. Eye Contact Lens. 2016;42(2):99–107. doi:10.1097/ICL.0000000000000166
39. Satjawatcharaphong P, Ge S, Lin MC. Clinical Outcomes Associated with Thermal Pulsation System Treatment. Optom Vis Sci. 2015;92(9):e334–41. doi:10.1097/OPX.0000000000000670
40. Blackie CA, Carlson AN, Korb DR. Treatment for meibomian gland dysfunction and dry eye symptoms with a single-dose vectored thermal pulsation: a review. Current Opinion in Ophthalmology. 2015;26(4):306–313. doi:10.1097/ICU.0000000000000165
41. Finis D, Hayajneh J, Konig C, Borrelli M, Schrader S, Geerling G. Evaluation of an automated thermodynamic treatment (LipiFlow(R)) system for meibomian gland dysfunction: a prospective, randomized, observer-masked trial. Randomized Controlled Trial. Ocul Surf. 2014;12(2):146–154. doi:10.1016/j.jtos.2013.12.001
42. Pang SP, Chen YT, Tam KW, Lin IC, Loh EW. Efficacy of Vectored Thermal Pulsation and Warm Compress Treatments in Meibomian Gland Dysfunction: a Meta-Analysis of Randomized Controlled Trials. Cornea. 2019;38(6):690–697. doi:10.1097/ICO.0000000000001907
43. Sabeti S, Kheirkhah A, Yin J, Dana R. Management of meibomian gland dysfunction: a review. Survey of Ophthalmology. 2020;65(2):205–217. doi:10.1016/j.survophthal.2019.08.007
44. Thode AR, Latkany RA. Current and Emerging Therapeutic Strategies for the Treatment of Meibomian Gland Dysfunction (MGD). Drugs. 2015;75(11):1177–1185. doi:10.1007/s40265-015-0432-8
45. Geerling G, Tauber J, Baudouin C, et al. The international workshop on meibomian gland dysfunction: report of the subcommittee on management and treatment of meibomian gland dysfunction. Invest Ophthalmol Vis Sci. 2011;52(4):2050–2064. doi:10.1167/iovs.10-6997g
46. Gira JP, Sampson R, Silverstein SM, Walters TR, Metzinger JL, Talamo JH. Evaluating the patient experience after implantation of a 0.4 mg sustained release dexamethasone intracanalicular insert (Dextenza): results of a qualitative survey. Patient Preference and Adherence. 2017;11:487–494. doi:10.2147/PPA.S126283
47. Walters T, Endl M, Elmer TR, Levenson J, Majmudar P, Masket S. Sustained-release dexamethasone for the treatment of ocular inflammation and pain after cataract surgery. J Cataract Refract Surg. 2015;41(10):2049–2059. doi:10.1016/j.jcrs.2015.11.005
48. Stephenson PDG. Real-world evaluation of postoperative in-office Dexamethasone intracanalicular insert administration for control of postoperative inflammation following cataract surgery. J Clin Ophthalmol. 2020;4(3):273–278.
49. Trivedi RH, Wilson ME. A sustained-release intracanalicular dexamethasone insert (Dextenza) for pediatric cataract surgery. J AAPOS. 2021;25(1):43–45. doi:10.1016/j.jaapos.2020.10.001
50. Ibach MJ, Shafer BM, Wallin DD, et al. and Safety of Dextenza 0.4 mg for the Treatment of Postoperative Inflammation and Pain in Patients After Photorefractive Keratectomy: the RESTORE Trial. J Refract Surg. 2021;37(9):590–594. doi:10.3928/1081597X-20210610-05
51. McLaurin EB, Evans D, Repke CS, et al. Phase 3 Randomized Study of Efficacy and Safety of a Dexamethasone Intracanalicular Insert in Patients With Allergic Conjunctivitis. Am J Ophthalmol. 2021;229:288–300. doi:10.1016/j.ajo.2021.03.017
52. Kenyon KR, McLaurin E, Silverstein S. Phase 3 Trial Evaluating an Intracanalicular Dexamethasone Insert (0.4 mg) for the Treatment of Patients with Allergic Conjunctivitis.
53. Torkildsen G, Abelson MB, Gomes PJ, McLaurin E, Potts SL, Mah FS. Vehicle-Controlled, Phase 2 Clinical Trial of a Sustained-Release Dexamethasone Intracanalicular Insert in a Chronic Allergen Challenge Model. J Ocul Pharmacol Ther. 2017;33(2):79–90. doi:10.1089/jop.2016.0154
54. Blizzard C, Desai A, Driscoll A. Pharmacokinetic Studies of Sustained-Release Depot of Dexamethasone in Beagle Dogs. J Ocul Pharmacol Ther. 2016;32(9):595–600. doi:10.1089/jop.2016.0025
55. Driscoll A, Blizzard C. Toxicity and Pharmacokinetics of Sustained-Release Dexamethasone in Beagle Dogs. Adv Ther. 2016;33(1):58–67. doi:10.1007/s12325-015-0280-7
56. Blizzard C, McLaurin EB, Driscoll A, et al. Plasma Pharmacokinetic Parameters of Dexamethasone Following Administration of a Dexamethasone Intracanalicular Insert in Healthy Adults. Clinical Ophthalmology (Auckland, NZ. 2021;15:2055–2061. doi:10.2147/OPTH.S307194
57. Goldstein MH, Silva FQ, Blender N, Tran T, Vantipalli S. Ocular benzalkonium chloride exposure: problems and solutions. Eye. 2021;1:56. doi:10.1038/s41433-021-01668-x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.