Back to Journals » OncoTargets and Therapy » Volume 11
Therapy-related myeloid neoplasms: clinical perspectives
Authors Fianchi L, Criscuolo M, Fabiani E ![]() , Falconi G
, Falconi G ![]() , Maraglino AME, Voso MT, Pagano L
, Maraglino AME, Voso MT, Pagano L ![]()
Received 14 August 2017
Accepted for publication 19 May 2018
Published 17 September 2018 Volume 2018:11 Pages 5909—5915
DOI https://doi.org/10.2147/OTT.S101333
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Samir Farghaly
Luana Fianchi,1 Marianna Criscuolo,1 Emiliano Fabiani,2 Giulia Falconi,2 Alessio Maria Edoardo Maraglino,1 Maria Teresa Voso,2 Livio Pagano1
1Department of Radiological Sciences, Radiotherapy, and Hematology, Fondazione Policlinico Universitario A. Gemelli, IRCCS, Rome, Italy; 2Department of Biomedicine and Prevention, Università di Roma Tor Vergata, Rome, Italy
Abstract: Therapy-related myeloid neoplasms (t-MNs) are a complication of cytotoxic treatment for primary tumors and autoimmune diseases. t-MNs result from a complex interaction between individual predisposition and exposition to toxic agents. Some different biological and clinical characteristics can be recognized according to the type of anticancer drug. Compared to de novo myeloid neoplasms, prognosis of t-MN is dismal. Age and karyotype are the most important prognostic factors for t-MN, which should be treated with frontline chemotherapy treatments that are appropriate for patients with myelodysplastic syndrome (MDS) and de novo acute myeloid leukemia (AML) with similar disease characteristics. Allogeneic stem cell transplantation should be considered particularly for unfavorable karyotypes and younger patients with aggressive disease.
Keywords: therapy-related myeloid neoplasm, leukemia, prognosis, secondary leukemia, secondary myelodysplastic syndrome
Introduction
Therapy-related myeloid neoplasms (t-MNs) are a group of hematologic diseases that arise after chemotherapy and/or radiation therapy for a previous cancer or rarely autoimmune diseases.1 The improvement in therapeutic strategies for curing hematologic and solid tumors has led to a prolongation of life expectancy of patients; in consequence, the prevalence of later side effects of treatment is increasing, although the progress of standard therapies has been made.2
The most frequent side effects of anticancer therapy are cardiac and pulmonary chronic diseases, but a second cancer is unfortunately not rare. The damage to DNA is a direct consequence of the mechanism of action of many anticancer drugs and can determine permanent bone marrow modifications.3 Exposition to other toxic events, such as environmental pollution or recreational habits, may cause cellular damages. Accumulation of genomic damages may overcome the mechanisms of intracellular repair; clonal bone marrow modifications may arise and determine an overt hematologic neoplasm such as myelodysplastic syndrome (MDS) and acute myeloid leukemia (AML).
A diagnosis of t-MN has a dismal impact on the quality of life and prognosis of cancer survivors: it represents the most dangerous long-term side effect of anticancer therapies and the most heavy barrier to cancer cure.4,5
Pathogenesis
t-MNs represent a rare complication of anticancer treatment. Since less than 10% of even heavily pretreated patients with cytotoxic drugs develop a t-MN, individual susceptibility has also been suggested2,6–9; t-MN result from a complex interaction between individual predisposition and exposition to toxic agents being the pathogenesis possibly determined by a progressive acquisition of somatic mutations and epigenetic modifications in a variable timeline.
Some clinical characteristics known to be associated with an increased risk of t-MN are higher total chemotherapy dose, combination chemo-radiotherapy, use of myeloid growth factors, older patient age, and longer duration of cytotoxic therapy.
Some data suggest that harboring heterozygous gene mutation in a FANC gene, which is implicated in DNA repair, could determine a predisposition for developing a t-MN, after exposition to either environmental or iatrogenic factor that can activate DNA repair enzymes.10
Moreover, polymorphic enzymes involved in apoptosis, folate metabolism, and synthesis of nucleotides had a role in the t-MN development even if not completely defined, considering the complex interaction between different metabolic pathways.11,12
As a consequence of persistent self-renewal potential, bone marrow stem cells may accumulate DNA mutations in a stochastic way and some mutated cells can acquire, under the pressure of chemo-/radiotherapy, a growth advantage compared to non-mutated cells and favor the expansion of clonal hematopoietic cells in otherwise normal subjects.
A number of studies are reported on clonal hematopoiesis in older subjects.13–16 In particular, sequencing DNA from the peripheral blood of adult patients without hematologic disease, two different groups identified somatic mutations of genes involved in MDS and AML development, such as DNMT3A, TET2, ASXL1, TP53, JAK2, and SF3B1.17,18 Prevalence of mutations varies with age: <1% in patients younger than 50 years and up to 18% in 90-year-old patients; on the other hand, harboring a mutation at high allelic fraction increases the risk of developing a hematologic neoplasm of 0.5%–1% per year only.
Mutations of TP53, associated with unfavorable karyotype and worse outcome, are particularly frequent in t-MN (around 21%–38%), whereas other common somatic mutations identified in de novo AML and MDS are more rare, with the solely exception of those affecting the spliceosome machinery gene SRSF2.19
Wong et al20 sequenced the genomes of seven patients at the time of t-MN diagnosis and during the follow-up for previous cancer. In four patients TP53 mutation was detectable before t-MN diagnosis: among them 2 patients acquired one more mutation at t-MN diagnosis; in other 2 patients TP53 mutation was detectable in the bone marrow sample before the chemotherapy for primary cancer was started; one acquired complex chromosomal abnormalities after drugs exposition. Subsequently, the authors studied the peripheral blood of 19 noncancer patients aged 68–89 years and detected a TP53 mutation in nine cases, with a variant allelic fraction between 0.01% and 0.37% demonstrating that TP53 mutation can develop in normal hematopoietic cells as a consequence of aging process.
Otherwise, some driver mutations in de novo AML, such as NPM1 and DNMT3A, are less frequent in t-MN.20 Lindsley et al showed that eight genes involved in splicing, methylation, and transcriptional regulation, which are frequently mutated in MDS, are mutated mainly in secondary AML.21 TP53 mutations identified a group of AMLs characterized by higher prevalence of complex karyotype and aggressive clinical course.21
Recently, two studies were published from two large US oncology referral centers, reporting the results of their genomic analyses (ie, whole-exome sequencing and targeted resequencing of relevant myeloid neoplasia-associated genes) of serial blood samples obtained from patients treated for cancer who either did or did not subsequently develop t-MN. Both studies found that the presence of even a small myeloid clone that was detectable after the treatment for the primary neoplasm increased the likelihood of subsequent development of t-MN and confirmed as expected that TP53 mutations were the most commonly detected clonal changes in those patients who went on to develop t-MN.22,23
Our group studied the mutational profile of 13 patients with t-MN at diagnosis and at previous time points during the follow-up for primary hematologic malignancy. We identified eight common somatic mutations in 7 out of 13 t-MN patients (54%). Somatic mutations were detectable in the bone marrow harvested at the primary diagnosis, prior to any cytotoxic treatment in three patients, while they were not detectable and apparently acquired by the t-MN clone in five patients. Our data showed that clonal evolution in t-MN was a heterogeneous process and somatic mutations in critical genes may precede and favor leukemic development or may be induced by the cytotoxic treatment.24
Epidemiology and prognosis
In 2008 World Health Organization (WHO) classification defined as t-MN, AMLs (t-AML) and myelodysplastic syndromes (t-MDS) occurring in patients treated with radiotherapy and/or chemotherapy for cancer or autoimmune diseases.1 t-MNs had been included in the group of AMLs and remain as a distinct category also in the recent 2016 revision of the WHO classification of myeloid neoplasm and acute leukemia.25
The latency between exposition to anticancer drugs and development of t-MN may vary from some months up to 10 years, even considering the age at diagnosis of the primary malignancy, the kind of cytotoxic treatment previously used, and the cumulative dose and dose intensity.26,27
Some different biological and clinical characteristics, including karyotype, latency, and disease history, can be recognized according to the use of an alkylating agent or radiotherapy and topoisomerase II inhibitor.
Nowadays, a combination of different drugs is used to treat the vast majority of tumors, but variable effects have been reported depending on the mechanism of action of these drugs. Alkylating agents, which can induce t-MN after a median latency of 4–7 years, can determine dysplasia of single or multiple lineages through modification of cellular differentiation, and eventually an overt leukemic evolution, which is frequently associated with abnormalities of chromosome 5 (−5/del[5q]) and chromosome 7(−7/del[7q]).28
Currently, a combination of different topoisomerase II inhibitor-related t-MNs has a relatively shorter latency between exposure to drugs and onset (median of 2–3 years), and patients with this subtype often present with overt AML without the features of preceding MDS; a high incidence of balanced translocations involving chromosomal segments 11q23, 17q21, and/or 21q22 is observed in these cases.29,30
An Italian multicentric cohort of 277 patients confirmed that the median latency after exposition to alkylating agents was significantly longer than that after exposition to a combination therapy including topoisomerase II inhibitors (8.4+1.1 vs 6+0.5 years, P=0.002). In the same study, it was confirmed that the latency of t-MN following radiation therapy was considerably longer than that following chemotherapy alone or combination of chemo/radiation therapy (11.2+1.8 vs 7.1+0.4 years, P=0.0005).31
Epidemiology
In most cases, t-MNs are related to breast cancer and lymphoproliferative disease treatment.2,5,31 In a population-based survey of 426,068 adults treated with chemotherapy for cancer, Morton et al2 identified 801 t-AML cases, translating into a 4.7-fold increased risk compared to the general population. For more than three decades, there has been an increase in t-AML risk following the treatment of non-Hodgkin lymphoma (NHL) and a decline in the risk of ovarian cancer, myeloma, and possibly lung cancer. This review also reported the emerging t-MN risk groups, which were coincident with the expanding use of chemotherapy for cancers of the esophagus, anus, cervix, endometrium, and prostate.2
In the Italian multicentric cohort, lymphoproliferative diseases represented the most frequent primary disease, accounting for 32% of cases with the frequency of Hodgkin lymphoma (HL) as primary tumor (6%), resulting slightly lower than that previously reported by the German–Austrian Acute Myeloid Leukemia Study Group (10%) and the Chicago series (25%).4,28,31 These data probably reflect the changes of HL treatment over time, with the recent tendency to avoid nitrogen mustards and reduce the number of chemotherapy cycles and the extension of radiotherapy fields.
Four or more cycles of escalated bleomycin, etoposide, doxorubicin, cyclophosphamide, vincristine, procarbazine, prednisone were found as a significant t-MN risk factor in a retrospective study on 106 t-MN cases in 11,952 HL patients (0.9%) treated within the German Hodgkin Study Group between 1993 and 2009.32 Recently, a study was conducted to describe the characteristics and outcome of 80 t-MNs consecutively diagnosed in the 1997–2012 period after the treatment of lymphoid malignancies (NHL, HL, T-cell lymphoma [TCL], and chronic lymphocytic leukemia [CLL]). t-MNs accounted for 2.3% of all AML cases, which occurred 60 months after lymphoproliferative disease diagnosis, and were characterized by a high frequency of acute erythroid leukemia according to French-American-British classification AML and poor-risk cytogenetic abnormalities. Time to t-MN diagnosis was influenced by patient age, type of lymphoproliferative diseases, and treatment.33
The risk of t-MN was recently evaluated among 115 consecutive patients receiving radioimmunotherapy with yttrium-90 ibritumomab tiuxetan during 1987–2012 for follicular lymphoma. Nine of these patients (8%) developed t-MN at a median of 41.4 months (range 5–89). The estimated 10-year risk of t-MN in all patients was 15%, but interestingly this resulted significantly higher in fludarabine-treated patients (29%) vs non-fludarabine-treated patients (13%; P=0.012).34
In a population-based study on Swedish Acute Leukemia Registry, t-MN represented the 7.7% of all cases of AML (259/3,363 adult patients with AML).5 In this series, breast cancer and lymphoproliferative diseases represented the primary malignancy in 21% and 19% of cases, respectively. Interestingly, some common types of malignancies such as lung cancer and prostate cancer were heavily underrepresented among t-MNs compared to their frequency in the general population.35 The median latency between the diagnosis of the primary disease and the diagnosis of t-MN was 6.2 years overall (5.8 and 14.3 years for malignancies and nonmalignant diseases, respectively).
In a retrospective study of an oncological institution in North Portugal, over a 10-year-period, 38 t-AML cases were identified among 231 diagnoses of AML. The mean latency time was 3 years, and t-MN was related to solid cancer treatment in >70% of cases; breast cancer was the most frequent solid tumor identified (39.5% of all solid tumors diagnosed).36
Incidence and risk factors for the development of t-MN among a total of 13,810 lymphoma patients who received autologous (n=9,963) or allogeneic (n=3,847) hematopoietic cell transplantation (HCT) between 1,985 and 2,012 patients were recently retrospectively analyzed. At a median overall survival (OS) of 52 and 46 months in autologous and allogeneic HCT groups, respectively, lymphoma patients receiving autologous HCT (1.38% at 3 years after autologous HCT) had a significant risk for developing t-MN compared to allogeneic HCT (0.37% at 3 years after allogeneic HCT, P<0.001). Significant risk factors for the development of t-MN after autologous and allogeneic HCT were high-stage risk at HCT (P=0.04) or secondary malignancies (P<0.001) and receiving cord blood stem cell (P=0.03) or involved-field radiotherapy (P=0.002), respectively.37
Prognosis
t-MNs represent about 10%–20% of all myeloid neoplasms (including AML, MDS, and myelodysplastic/myeloproliferative neoplasms). Compared to de novo myeloid neoplasms, prognosis of t-MN is dismal: OS is <10% at 5 years due to different factors. Advanced age, higher number of comorbidities, previous chemotherapy, and possible long-lasting complications may limit an optimal treatment.
Moreover, t-MNs are considered biologically aggressive because of higher percentage of complex karyotype specifically monosomy of chromosomes 5 and 7; however, as in de novo myeloid neoplasms, recurrent cytogenetic translocations are prognostically more favorable.4,38 In the Italian multicentric study, cytogenetic abnormalities were very frequent, with single or multiple abnormalities in 64% of evaluable cases. Karyotype was unfavorable in 39% of patients and involved chromosome 5 or 7 deletions in most cases. Interestingly, no differences were found in the distribution of karyotype abnormalities according to treatment, probably due to the fact that most of the patients received combinations of different drugs.31
Quintás-Cardama et al39 proposed a score, which was able to identify three prognostically different t-MN groups in a retrospective collection of 279 t-MDSs. Negative factors at baseline were as follows: age>65 years, Eastern Cooperative Oncology Group (ECOG) performance status over 1, monosomy 7 or complex karyotype, refractory anemia with ringed sideroblasts (RARSs) or refractory anemia with excess blast types 1 and 2 (RAEB-1/2), hemoglobin below 11 g/dL, platelet counts below 50×109/L, and transfusion dependency.
Interestingly this prognostic score resulted in predictive of significant differences in OS and leukemia-free survival also in a series of t-MN patients treated with azacitidine (AZA).40
Ornstein et al, from the Cleveland University, published a prognostic model for OS in 58 t-MN patients treated with cytarabine.27 Unfavorable cytogenetics (according to Cancer and Leukemia Group B), antecedent hematologic or autoimmune disease vs solid tumor, age>60 years, and platelet counts below 30×109/L at t-MN diagnosis were associated with inferior survival.26 Patients with no or only one risk factor had a median OS of 37.6 months, while patients with two to four risk factors had a poor outcome with only 6.4 months of OS.3 This “Cleveland score” has been validated in a larger population of t-MN in the Italian report, including a retrospective and a prospective patient cohort, and by stratifying the analysis for treatment type.31
The survival analysis adjusted for recruitment (retrospective vs prospective) identified the following as significant prognostic factors for OS: age at t-MN diagnosis, platelet counts below 30×109/L, hemoglobin level, adverse karyotype, and allogeneic stem cell transplantation compared to best supportive care. The multivariable analysis stratified for treatment type identified the following as independent prognostic factors: age, hemoglobin as continuous variable, and unfavorable karyotype.
Accordingly, a clinical prognostic score was developed attributing 1 point to age>60 years and 1 point to unfavorable karyotype. This resulted into three prognostic groups including patients with 0, 1, or 2 adverse factors. Patients with score 0 had a significantly better survival when compared to patients with 1 or 2 poor-risk features (median OS not reached vs 14 and 8.9 months, respectively, P<0.0001).
Interestingly, no survival differences were observed in Italian registry comparing t-MDS to t-AML, and really these data were confirmed by the WHO 2016 revision, where the author underlined the importance of cytogenetics in spite of the bone marrow blast count when considering prognosis and therapeutic options.31
Significant differences in outcome according to age and karyotype are known for de novo AML, where mutations of FLT3, NMP1, and CEBPalfa have been shown to improve survival prediction.41 In t-MN, FLT3, NPM1, and epigenetic and spliceosome mutations have been shown to occur in a minority of patients indicating that in these diseases karyotype has a dominant role.8,10
In the Portuguese study, the OS time was observed to be significantly poorer among individuals with t-AML (P<0.001).36 However, in younger patients (age<50 years), there was no difference between the OS time of patients with t-AML and that of patients with de novo AML (P=0.983). In addition, patients with promyelocytic leukemia possess a good prognosis, even when AML occurs as a secondary event (P=0.98). All these data confirmed, as suggested by Larson,42 that cytogenetics, not just previous therapy, determines the course of t-MN.
OS according to prognostic scores identified in epidemiological studies on t-MN patients is presented in Table 1.
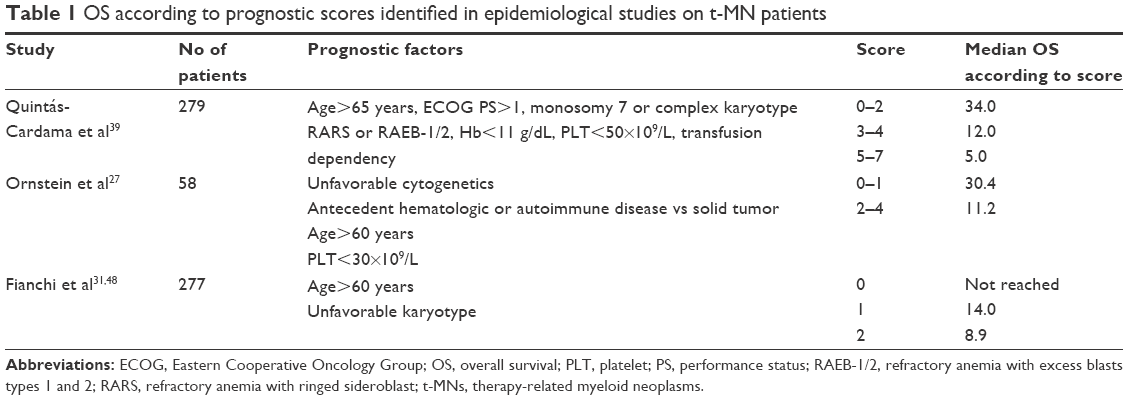 | Table 1 OS according to prognostic scores identified in epidemiological studies on t-MN patients |
Treatment
As for de novo myeloid neoplasms, therapeutic options of t-MN include supportive care, demethylating agents, and conventional chemotherapy: the only curative option is allogeneic bone marrow transplantation. Unfortunately, intensive treatment is not applicable in the majority of cases because of clinical conditions.
The heterogeneous treatments generally used for t-MN in retrospective studies, ranging from best supportive care to intensive chemotherapy (IC), hypomethylating agents, (HMAs), and stem cell transplantation, do not allow definite conclusions on the best treatment choice in t-MN, mostly typical of elderly patients. Treatment recommendations for t-MN should be based on performance status and karyotype, so these patients should be enrolled into frontline chemotherapy trials that are appropriate for patients with MDS and de novo AML with similar disease characteristics.4,37,43,44 A multicenter study showed that t-MN patients with good performance status, enrolled in conventional GIMEMA trials, had treatment response rates similar to de novo AML.44
In t-MN with recurrent cytogenetic translocations, conventional chemotherapy may induce the percentage of response similar to de novo AML, particularly in acute promyelocytic leukemia.43,45
Allogeneic stem cell transplantation should be considered for unfavorable karyotypes, including monosomal karyotype; younger patients with aggressive disease are expected to undergo allogeneic bone marrow transplantation, even if the outcome could be inferior than what has been seen in de novo myeloid neoplasms in case some mutations such as TP53 were present.46
Encouraging results have been obtained in MDS and oligoblastic AML using HMAs.47,48
Among 50 t-MN patients receiving 5-AZA, an overall response rate of 42% with a median OS of 21 months was reported, similar to results obtained in de novo high-risk MDS treated with AZA at standard doses and also favorably compared to conventional therapy in t-MN.26,43,47–49
Recently, decitabine, also in refractory/relapsed AML, showed to induce a significantly higher overall response in patients with t-MN and secondary AML compared to those with de novo AML (70% vs 30%; P=0.02) with median survival in patients with t-MN or secondary AML of 12.4 months compared to 8 months in those with de novo AML (P=0.20).50 These data could be probably related to the advantage of this drug suggested by a recent study, where a 10-day course of decitabine showed an OS rate in patients with AML and MDS who had cytogenetic abnormalities associated with unfavorable risk and/or TP53 mutations similar to those patients with AML who had an intermediate-risk cytogenetic profile.51 It is, however, to underline that these results have been obtained in an uncontrolled trial and should be confirmed in larger prospective studies to draw any conclusion about a specific therapeutic approach based on hypomethylating agents in this clinical context.
Recently, a study about the outcomes of 931 older patients with newly diagnosed secondary AML according to treatment was published.52
Patients were grouped into five treatment cohorts: patients receiving high- or intermediate-dose cytarabine-based IC; patients receiving HMA or HMA combinations; patients receiving low-dose cytarabine combinations; patients receiving CPX-351, and patients receiving investigational (INV) agents. Complete remission rates were lower in the HMA (36%) and INV groups (16%) in comparison with the IC group (46%; P=0.03 and P=0.001, respectively). However, an OS analysis performed for patients with t-MN by therapy regimen (ie, IC regimen vs epigenetic and low-dose cytarabine regimens) did not demonstrate a statistically significant difference in OS (6 vs 5.6 months; P=0.92), while patients who received a transplant (7.1%) had superior outcomes in terms of median OS in comparison with patients who did not proceed to transplantation after chemotherapy (16.2 vs 5.5 months, respectively; P<0.001), confirming the importance of allogeneic transplantation, if applicable, in the treatment of t-MN.52
Conclusion
t-MNs represent a distinct category of myeloid neoplasms apart from de novo MDS and AML. However, it is important to underline that t-MN “per se” should not be considered as a prohibitive factor for standard therapy, since some t-MNs are not biologically unfavorable.
Cytogenetics and molecular data represent the important prognostic factors, so treatment recommendations for t-MN should be based on these parameters in addition to performance status; patients with t-MN should be treated with frontline chemotherapy trials that are considered appropriate for patients with MDS and de novo AML with similar disease characteristics and performance status.
Disclosure
The authors report no conflicts of interest in this work.
References
Vardiman JW, Thiele J, Arber DA, et al. The 2008 revision of the World Health Organization (WHO) classification of myeloid neoplasms and acute leukemia: rationale and important changes. Blood. 2009;114(5):937–951. | ||
Morton LM, Dores GM, Tucker MA, et al. Evolving risk of therapy-related acute myeloid leukemia following cancer chemotherapy among adults in the United States, 1975–2008. Blood. 2013;121(15):2996–3004. | ||
Greim H, Kaden DA, Larson RA, et al. The bone marrow niche, stem cells, and leukemia: impact of drugs, chemicals, and the environment. Ann N Y Acad Sci. 2014;1310(1):7–31. | ||
Kayser S, Döhner K, Krauter J, et al; German-Austrian AMLSG. The impact of therapy-related acute myeloid leukemia (AML) on outcome in 2853 adult patients with newly diagnosed AML. Blood. 2011;117(7):2137–2145. | ||
Hulegårdh E, Nilsson C, Lazarevic V, et al. Characterization and prognostic features of secondary acute myeloid leukemia (AML) in a population based setting: a report from the Swedish acute leukemia registry. Am J Hematol. 2015;90(3):208–214. | ||
Easton DF, Pooley KA, Dunning AM, et al; SEARCH Collaborators; kConFab; AOCS Management Group. Genome-wide association study identifies novel breast cancer susceptibility loci. Nature. 2007;447(7148):1087–1093. | ||
Knight JA, Skol AD, Shinde A, et al. Genome-wide association study to identify novel loci associated with therapy-related myeloid leukemia susceptibility. Blood. 2009;113(22):5575–5582. | ||
Voso MT, Fabiani E, Fianchi L, et al. Mutations of epigenetic regulators and of the spliceosome machinery in therapy-related myeloid neoplasms and in acute leukemias evolved from chronic myeloproliferative diseases. Leukemia. 2013;27(4):982–985. | ||
Seedhouse C, Russel N. Advances in the understanding of susceptibility to treatment related acute myeloid leukaemia. Br J Haematol. 2007;137(6):513–529. | ||
Voso MT, Fabiani E, Zang Z, et al. Fanconi anemia gene variants in therapy-related myeloid neoplasms. Blood Cancer J. 2015;5(7):e323. | ||
Fabiani E, Fianchi L, Falconi G, et al. The BCL2L10 Leu21Arg variant and risk of therapy-related myeloid neoplasms and de novo myelodysplastic syndromes. Leuk Lymphoma. 2014;55(7):1538–1543. | ||
Criscuolo M, Chiusolo P, Giammarco S, et al. Methylenetetrahydrofolate reductase polymorphisms in myelodysplastic syndromes and therapy-related myeloid neoplasms. Leuk Lymphoma. 2014;55(12):2942–2944. | ||
Champion KM, Gilbert JG, Asimakopoulos FA, Hinshelwood S, Green AR. Clonal haemopoiesis in normal elderly women: implications for the myeloproliferative disorders and myelodysplastic syndromes. Br J Haematol. 1997;97(4):920–926. | ||
Jacobs KB, Yeager M, Zhou W, et al. Detectable clonal mosaicism and its relationship to aging and cancer. Nat Genet. 2012;44(6):651–658. | ||
Busque L, Patel JP, Figueroa ME, et al. Recurrent somatic TET2 mutations in normal elderly individuals with clonal hematopoiesis. Nat Genet. 2012;44(11):1179–1181. | ||
Xie M, Lu C, Wang J, et al. Age-related cancer mutations associated with clonal hematopoietic expansion. Nat Med. 2014;20(12):1472–1478. | ||
Jaiswal S, Fontanillas P, Flannick J, et al. Age-related clonal hematopoiesis associated with adverse outcomes. N Engl J Med. 2014;371(26):2488–2498. | ||
Genovese G, Jaiswal S, Ebert BL, McCarroll SA. Clonal hematopoiesis and blood-cancer risk. N Engl J Med. 2015;372(11):1071–1072. | ||
Shih AH, Chung SS, Dolezal EK, et al. Mutational analysis of therapy-related myelodysplastic syndromes and acute myelogenous leukemia. Haematologica. 2013;98(6):908–912. | ||
Wong TN, Ramsingh G, Young AL, et al. Role of TP53 mutations in the origin and evolution of therapy-related acute myeloid leukaemia. Nature. 2015;518(7540):552–555. | ||
Lindsley RC, Mar BG, Mazzola E, et al. Acute myeloid leukemia ontogeny is defined by distinct somatic mutations. Blood. 2015;125(9):1367–1376. | ||
Gillis NK, Ball M, Zhang Q, et al. Clonal haemopoiesis and therapy-related myeloid malignancies in elderly patients: a proof-of-concept, case-control study. Lancet Oncol. 2017;18(1):112–121. | ||
Takahashi K, Wang F, Kantarjian H, et al. Preleukaemic clonal haemopoiesis and risk of therapy-related myeloid neoplasms: a case-control study. Lancet Oncol. 2017;18(1):100–111. | ||
Fabiani E, Falconi G, Fianchi L, et al. Clonal evolution in therapy-related neoplasms. Oncotarget. 2017;8(7):12031–12040. | ||
Arber DA, Orazi A, Hasserjian R, et al. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood. 2016;127(20):2391–2405. | ||
Leone G, Fianchi L, Voso MT. Therapy-related myeloid neoplasms. Curr Opin Oncol. 2011;23(6):672–680. | ||
Ornstein MC, Mukherjee S, Mohan Elson P, et al. Predictive factors for latency period and a prognostic model for survival in patients with therapy-related AML. Am J Hematol. 2014;89(2):168–173. | ||
Smith SM, Le Beau MM, Huo D, et al. Clinical-cytogenetic associations in 306 patients with therapy-related myelodysplasia and myeloid leukemia: the university of Chicago series. Blood. 2003;102(1):43–52. | ||
Pedersen-Bjergaard J, Philip P. Balanced translocations involving chromosome bands 11q23 and 21q22 are highly characteristic of myelodysplasia and leukemia following therapy with cytostatic agents targeting at DNA-topoisomerase II. Blood. 1991;78(4):1147–1148. | ||
Olney HJ, Mitelman F, Johansson B, Mrózek K, Berger R, Rowley JD. Unique balanced chromosome abnormalities in treatment-related myelodysplastic syndromes and acute myeloid leukemia: report from an international workshop. Genes Chromosomes Cancer. 2002;33(4):413–423. | ||
Fianchi L, Pagano L, Piciocchi A, et al. Characteristics and outcome of therapy-related myeloid neoplasms: report from the Italian network on secondary leukemias. Am J Hematol. 2015;90(5):E80–E85. | ||
Eichenauer DA, Thielen I, Haverkamp H, et al. Therapy-related acute myeloid leukemia and myelodysplastic syndromes in patients with Hodgkin lymphoma: a report from the German Hodgkin study group. Blood. 2014;123(11):1658–1664. | ||
Bertoli S, Sterin A, Tavitian S, et al. Therapy-related acute myeloid leukemia following treatment of lymphoid malignancies. Oncotarget. 2016;7(52):85937–85947. | ||
Epperla N, Pham AQ, Burnette BL, et al. Risk of histological transformation and therapy-related myelodysplasia/acute myeloid leukaemia in patients receiving radioimmunotherapy for follicular lymphoma. Br J Haematol. 2017;178(3):427–433. | ||
Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136(5):E359–E386. | ||
Espitito Santo AE, Chacim S, Ferreira I, et al. Effect of therapy-related acute myeloid leukemia on the outcome of patients with acute myeloid leukemia. Oncol Lett. 2016;12(1):262–268. | ||
Yamasaki S, Suzuki R, Hatano K, et al. Therapy-related acute myeloid leukemia and myelodysplastic syndrome after hematopoietic cell transplantation for lymphoma. Bone Marrow Transplant. 2017;52(7):969–976. | ||
Kern W, Haferlach T, Schnittger S, et al. Prognosis in therapy-related acute myeloid leukemia and impact of karyotype. J Clin Oncol. 2004;22(12):2510–2511. | ||
Quintás-Cardama A, Daver N, Kim H, et al. A prognostic model of therapy-related myelodysplastic syndrome for predicting survival and transformation to acute myeloid leukemia. Clin Lymphoma Myeloma Leuk. 2014;14(5):401–410. | ||
Breccia M, Fianchi L, Lunghi M, et al. Newly proposed therapy-related myelodysplastic syndrome prognostic score predicts significant differences in overall survival and leukemia-free survival in patients treated with azacitidine. Leuk Lymphoma. 2013;54(8):1786–1787. | ||
Döhner H, Estey E, Grimwade D, et al. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood. 2017;129(4):424–447. | ||
Larson RA. Cytogenetics, not just previous therapy, determines the course of therapy-related myeloid neoplasms. J Clin Oncol. 2012;30(19):2300–2302. | ||
Larson RA, Le Beau MM. Prognosis and therapy when acute promyelocytic leukemia and other “good risk” acute myeloid leukemias occur as a therapy-related myeloid neoplasm. Mediterr J Hematol Infect Dis. 2011;3(1):e2011032. | ||
Pagano L, Pulsoni A, Vignetti M, et al; GIMEMA. Secondary acute myeloid leukaemia: results of conventional treatments. Experience of GIMEMA trials. Ann Oncol. 2005;16(2):228–233. | ||
Duffield AS, Aoki J, Levis M, et al. Clinical and pathologic features of secondary acute promyelocytic leukemia. Am J Clin Pathol. 2012;137(3):395–402. | ||
Bejar R, Stevenson KE, Caughey B, et al. Somatic mutations predict poor outcome in patients with myelodysplastic syndrome after hematopoietic stem-cell transplantation. J Clin Oncol. 2014;32(25):2691–2698. | ||
Klimek VM, Dolezal EK, Tees MT, et al. Efficacy of hypomethylating agents in therapy-related myelodysplastic syndromes. Leuk Res. 2012;36(9):1093–1097. | ||
Fianchi L, Criscuolo M, Lunghi M, et al. Outcome of therapy-related myeloid neoplasms treated with azacitidine. J Hematol Oncol. 2012;5:44. | ||
Fenaux P, Mufti GJ, Hellstrom-Lindberg E, et al; International Vidaza High-Risk MDS Survival Study Group. Efficacy of azacitidine compared with that of conventional care regimens in the treatment of higher-risk myelodysplastic syndromes: a randomised, open-label, phase III study. Lancet Oncol. 2009;10(3):223–232. | ||
Khan N, Hantel A, Knoebel RW, et al. Efficacy of single-agent decitabine in relapsed and refractory acute myeloid leukemia. Leuk Lymphoma. 2017;58(9):1–7. | ||
Welch JS, Petti AA, Miller CA, et al. TP53 and decitabine in acute myeloid leukemia and myelodysplastic syndromes. N Engl J Med. 2016;375(21):2023–2036. | ||
Boddu PC, Kantarjian HM, Ravandi F, et al. Characteristics and outcomes of older patients with secondary acute myeloid leukemia according to treatment approach. Cancer. 2017;123(6):3050–3060. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.