")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 16
Therapeutic Potential of Ixekizumab in the Treatment of Ankylosing Spondylitis: A Review on the Emerging Clinical Data
Authors Benucci M, Damiani A, Li Gobbi F , Grossi V, Infantino M, Manfredi M, Niccoli L, Cantini F
Received 19 January 2020
Accepted for publication 8 March 2020
Published 16 April 2020 Volume 2020:16 Pages 287—297
DOI https://doi.org/10.2147/TCRM.S228880
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Maurizio Benucci,1 Arianna Damiani,2 Francesca Li Gobbi,1 Valentina Grossi,3 Maria Infantino,3 Mariangela Manfredi,3 Laura Niccoli,4 Fabrizio Cantini4
1Rheumatology Unit, Hospital S. Giovanni di Dio, Azienda USL-Toscana Centro, Florence, Italy; 2Rheumatology Unit, University of Florence, Florence, Italy; 3Immunology and Allergology Laboratory Hospital S. Giovanni di Dio, Azienda USL-Toscana Centro, Florence, Italy; 4Rheumatology Unit, S. Stefano Hospital, Azienda USL-Toscana Centro, Prato, Italy
Correspondence: Maurizio Benucci
Rheumatology Unit, Azienda Sanitaria USL-Toscana Centro, Hospital S. Giovanni di Dio, Via Torregalli 3, Florence 50143, Italy
Tel +39-055-6932636
Fax +39-055-6932099
Email [email protected]
Abstract: Over the last 20 years, the greatly improved knowledges of underlying pathogenic mechanisms of AS, including the role of tumor necrosis factor (TNF), the interleukin 23/Th17 axis, and interleukin-17 (Il-17), constituted the rationale to develop biologics selectively inhibiting these pathways. For more than 10 years, anti-TNF biologics were successfully employed to treat AS, with marked improvement of signs and symptoms in around 60% of the patients. Recent knowledge of the pathophysiology of spondyloarthritis has highlighted the emerging role of the IL-17/IL-23 axis. New therapies with selective biological drugs have emerged in the treatment of this pathology. In this review, we evaluated the effects of ixekizumab, a new anti–IL-17A, that was licensed both by EMA and FDA in August 2019 for the treatment of ankylosing spondylitis. The review highlights the efficacy and safety data of the 3 randomized controlled trials (COAST V-COAST W-COAST X) and those of the extension to 52 weeks of COAST V and COAST W.
Keywords: ixekizumab, ankylosing spondylitis, randomized control trials
Introduction
Ankylosing spondylitis (AS) is a relatively common, chronic, immune-mediated, inflammatory rheumatic disease which affects the axial skeleton leading, in more severe cases, to complete spinal ankylosis (bamboo spine), with consequent marked impairment of vertebral column physiological range of movement.1 AS occurrence is strongly conditioned by the inheritance of HLA-B27, and several subtypes, including B*2702, B*2703, B*2704, B*2705 and B*2710 were found to significantly increase the risk.2 Currently, AS is included, together with non-radiographic axial spondyloarthritis (ax-SpA), in the axial-SpA group and it has been renamed as radiographic ax-SpA.3 In the absence of validated diagnostic criteria, the 1984 modified New York classification criteria for AS are employed for diagnostic purpose in clinical practice.4 This set of criteria requires as obligatory condition the presence of bilateral grade 2 or unilateral grade 3 sacroiliitis, thus resulting in inadequate to capture patients with early axial-SpA. Over the last 15 years, the use of magnetic resonance showing periarticular bone edema has permitted to diagnose sacroiliitis in early phase of axial-SpA, thus defining non-radiographic ax-SpA (nr-ax-SpA).5 Until the early 2000s, due to the inefficacy of conventional synthetic disease-modifying antirheumatic drugs (csDMARDs), AS was treated with non-steroidal anti–inflammatory drugs (NSAIDs) and physical therapy, with good efficacy in terms of relief of symptoms, but unsatisfactory results regarding the disease progression, and the long-term tolerability.6–8 Over the last 20 years, the greatly improved knowledges of underlying pathogenic mechanisms of AS, including the role of tumor necrosis factor (TNF), the interleukin 23/Th17 axis, and interleukin-17 (Il-17), constituted the rationale to develop biologics selectively inhibiting these pathways.9 For more than 10 years, anti-TNF biologics were successfully employed to treat AS, with marked improvement of signs and symptoms in around 60% of the patients.10 Moreover, these biologics were demonstrated to inhibit the radiographic progression of AS when employed in early phase of the disease.11 However, the safety profile anti-TNFs, characterized by increased risk of infection and latent tuberculosis reactivation,12,13 represented an important concern. Recently, the pivotal pathogenic role of IL-17 in AS was demonstrated,14 and, randomized controlled trials (RCTs) evidenced the efficacy and safety of secukinumab, an anti–IL-17 targeted monoclonal antibody.15 In two recent RCTs, ixekizumab, an anti–IL-17a monoclonal antibody, resulted highly efficacious and safe for the treatment of AS.16 The present review was focused on the pharmacological characteristics of ixekizumab, the peculiarity of its mechanism of action, the efficacy and safety, and its place in therapy of AS.
Methods
The literature on the existing evidence on the efficacy and safety of anti–IL-17 ixekizumab in AS was analysed. The literature review was made using PubMed, Scopus and EMBASE databases to identify English-language articles related to the previously mentioned topic. The research was performed by crossing the following key terms: ankylosing spondylitis, ixekizumab, mechanism of action, pharmacology, anti–IL-17, efficacy, safety, discontinuation, survival, adverse events, infections, tuberculosis, opportunistic infections, adverse events (AE), serious adverse events (SAE). Due to the few available studies, the manuscript was structured as narrative review. The literature review was extended to December 15, 2019.
The Pathogenesis of Ankylosing Spondylitis and the Role of IL-17
AS manifestations should account for a common pathogenetic pattern, maybe lying on a common predisposing genetic and immunologic field. Rising from an old epidemiologic observation, the correlation with HLA-B27 expression and AS development is well known, and it has been deeply investigated to understand its molecular basis. Two theories are mainly available about HLA-B27 way of inducing AS: firstly, the “arthritogenic peptide theory”, assuming that the presentation of pathogen peptides by HLA-B27 or self-mimicking HLA-B27-binding peptides from bacteria could induce an immune reaction leading to AS.17 This could explain why most forms of reactive arthritis develop in HLA-B27+ patients, and it gives AS a hint of autoimmunity. Secondly, the “unfolded protein response” hypothesis states that HLA-B27 has a defect in the protein folding process and tends to be stored in the endoplasmic reticulum, determining cellular damage, activation of NFKB pathway and cytokines releasing, mainly IL-23. Here, AS is mostly seen as an autoinflammatory disease. IL-23 trigs Th17 response, driving to IL-17 expression, frequently observed in AS. The two hypotheses around HLA-B27 established a link between the classical pure genetic predisposing field and the more recently discovered immunologic milieu characterizing AS. Moreover, going back again from cytokines to genes, a large number of SNPs and other genetic marks regarding IL-12/23 and IL-17 related signaling pathways have been lately found in patients suffering from AS.18 Furthermore, some authors suggested that HLA-B27 in spondylarthritis may act on cells containing killer cell immunoglobulin-like receptor 3DL2 (KIR3DL2). KIR3DL2 is a NK cell receptor for HLA-B27 homodimer (that is HLA-B27 heavy chain not associated with β2-microglobulin, a unique structural conformation of this specific HLA haplotype) and it is highly expressed on NK cells and CD4 T cells in patients with spondylarthritis and enthesitis-related arthritis. The binding of HLA-B27 homodimers to KIR3DL2-positive cells can stimulate IL-17 production.19 IL-17’s family includes various isoforms, from A to F, produced by different cells; they bind to five receptor subtypes (IL-17RA to IL-17RE). The most studied isoform is IL-17A, whose production depends on TH-17, CD8+T cells, ILC3 and γδ T cells, involving both innate and adaptative immune systems. Its main role is to protect against parasite infections, thus justifying the predominant presence of IL-17 producing cells in the mucosal barriers like skin and gut. IL-17 acts principally during the effector phase of an inflammatory response, enhancing T cell priming and stimulating the production of proinflammatory mediators (as IL-1, IL-6, TNF-a and chemokines) in fibroblasts, endothelial cells, macrophages and epithelial cells. As previously stated, IL-17 production is in turn stimulated from IL-23, a member of the IL-12 cytokine family produced mainly by activated myeloid cells, endothelial and epithelial cells. While IL-12 has been shown to have a dominant role in the development of Th1 cells, IL-23 seems to stimulate Th17 cell. Physiologically, IL-17 secretion is crucial in cutaneous and mucosal defenses against various microbiologic agents as in the constitution of a normal mucosal immunity, able to be tolerant against resident microbiota. But IL-17 effects are claimed to be involved in human diseases, such as in psoriasis, multiple sclerosis, IBD and SA itself. In fact, at bone level, IL-17A can activate osteoclasts by interacting with RANKL, determining bone erosions, osteopenia and osteoporosis, typically seen in AS patients. IL-17 also exerts direct effects on osteoclasts, upregulating the expression of RANK on their surfaces.20 Additionally, IL-17 has pro-inflammatory actions on bone cells, inducing the production of TNF, IL-1 and IL-6 by stromal cells and macrophages which in turn promote osteoclastogenesis. Furthermore, IL-17A can stimulate osteoblasts differentiation from human mesenchymal stem cells21 acting on JAK2/STAT3 system with an increase of bone production and osteophytes formation. In fact, IL-17A is thought to be also involved in bone-repairing process after fractures.22 Anyway, other data support an inhibitory role for IL-17A on osteoblasts,23 thus leaving space for further investigations on this topic.24 Talking about SA extra-articular manifestations, a role of IL-17 in uveitis pathogenesis is quite probable; high levels of IL-17A have been found in aqueous, vitreous and serum of patients with anterior uveitis.25 Moreover, γδ T cells have been detected in the ciliary body of SA mice models and the same finding was made at the side of the cardiac valves. Some authors suggest that IL-17 producing γδ T cells, typically resident in a continually stimulated environment as the gut mucosa, are recruited also in mechanically stressed tissues as enthesis, cardiac valves and ciliary body and they can contribute to trigger and maintain inflammation in predisposed subjects.26,27 Unfortunately, IL-17 blockers such as secukinumab, that successfully resolves enthesitis, did not show any effect in treating SA-related anterior uveitis, reserving for TNFa inhibitors a major role for patients suffering from this manifestation. This could lead to considerations about the existence of different pathways underlying these conditions. Of extreme interest is the role of IL-17 in gut immune system and in IBD pathogenesis. ILC and γδ T are very important in the genesis of bowel immune barrier and in the maintenance of tolerance against gut microbiota.28 Alteration in this balance, induced by pathogens or immune dysregulations maybe due to environmental stressor in the presence of genetic predispositions, leads to inflammatory processes that can become chronic. IL-12/23 axis is known to be altered in IBD as it is IL-17 expression. By the way, biologic therapy targeting IL12/23 demonstrated efficacy in these diseases, while RCT of IL-17 inhibitors failed to reach the endpoints and, in some cases, leads to concerns about these drugs' implications in IBD development. Even if the association between gut and osteoarticular system is well known and it is demonstrated by the existence of IBD-related spondylarthritis and by the high frequency of clinical or subclinical bowel inflammation in AS patient, molecular basis of this connection is yet unknown. An interesting observation is the one from Gracey et al29 about mucosal-associated invariant T (MAIT) cells. MAIT cells are innate-like lymphocytes found preferentially in the gut lamina propria, but they can also be found in peripheral blood. They are able to produce various inflammatory cytokines, with a high expression of IL-17, and to stimulate TH17 differentiation. The authors found a reduced number of MAIT cells in peripheral blood samples of AS patients, with an increased IL-17 producing MAIT cells in the same patients’ synovial fluid. Similar findings have been described by Ciccia et al about the presence of expanded IL-17 producing ILC not only in the gut but also in bone morrow and synovial fluid of patients affected by AS.30 Besides, both Gracey’s and Ciccia’s groups found out a role for IL-7 in promoting IL-17 secretion. These evidences could suggest a homing mechanism justifying the migration of a pathologic process from the gut side to the joints. Moreover, it can explain how a genetic alteration inducing the immune responses against mucosal pathogens can predispose to osteoarticular (and systemic) diseases. Although the fascinating world of immune system is far from being completely revealed, innovative, selective, available therapies are a demonstration of the scientific progress and an incentive to a never-ending study.
Licensed Anti-IL-17 Biologics for the Treatment of AS
To date, two monoclonal antibody biologics targeted against IL-17, secukinumab and ixekizumab have been licensed for the treatment of AS. Secukinumab (Cosentyx®), at the dose of 150 mg/sc/4 weeks, was firstly approved for the treatment of AS by the European Medical Agency (EMA) in March 2015,31 and by Food and Drug Administration (FDA) in January 2016.32 Secukinumab is a fully human monoclonal antibody of IgG1/κ isotype, and exerts its pharmacological action by binding to IL-17a with consequent inhibition of interaction with the IL-17 receptor.33 The efficacy of secukinumab in AS at the dose of 150 mg/sc/was demonstrated in 5 RCTs of MEASURE program.15 Overall, the drug significantly reduced the disease activity, improved the quality of life, with slowing down of the structural damage both in naïve and anti-TNF refractory AS patients.15 A few studies from real-life clinical practice, on a limited number of patients, confirmed the results of RCTs.15 Secukinumab safety profile was satisfactory, with a slight increased risk for infections,31 no increased risk of latent tuberculosis (TB) reactivation.34 Due to the physiological protective role exerted by IL-17 on mucosae,35 and on gut microbiome,36 a special attention was reserved to the risk of opportunistic infections and increased occurrence of inflammatory bowel diseases induced by IL-17 inhibition. As expected, an increased occurrence of candidiasis was observed in secukinumab-exposed, but not requiring the drug withdrawal,37 while the risk of IBD development was low or absent.38 Ixekizumab (Taltz®), a monoclonal antibody directed against interleukin 17A, was licensed both by EMA and FDA in August 2019 for the treatment of ankylosing spondylitis.39,40 According to the objective of present review, the pharmacology of ixekizumab, and its efficacy and safety in the treatment of AS will be discussed in the following headings.
Pharmacological Features of Ixekizumab
Mechanism of Action
Ixekizumab is an IgG4 monoclonal antibody that binds with high affinity (<3 pM) and specificity to interleukin 17A (both IL-17A and IL-17A/F). IXE selectively binds to IL-17A cytokine to inhibit interaction with IL-17 receptor thus inhibiting the release of pro-inflammatory cytokines and chemokines by target cells with downstream effects on cellular elements. In vitro binding tests have confirmed that Ixe does not bind to human Fcγ I, IIa and IIIa receptors or to the complement component C1q.41
Pharmacodynamics after a single subcutaneous dose of ixekizumab in patients with psoriasis, mean peak concentrations were reached within 4–7 days, within a dose range of 5 to 160 mg. The mean (SD) of the maximum plasma concentration (Cmax) of ixekizumab, after the initial dose of 160 mg, was 19.9 (8.15) μg/mL. After the initial 160 mg dose, steady state was reached by week 8 at a dose of 80 mg every 2 weeks (q2W). The mean (SD) estimates for Cmax, ss, and C trough, ss are 21.5 (9.16) μg/mL and 5.23 (3.19) μg/mL. After switching from the 80 mg dose every 2 weeks (q2W) to the 80 mg dose every 4 weeks (q4W) at week 12, the steady state would be reached after about 10 weeks. The estimated mean (SD) Cmax, ss and C trough, ss are 14.6 (6.04) μg/mL and 1.87 (1.30) μg/mL. Among the analyzes carried out, the average bioavailability of ixekizumab after subcutaneous administration was between 54% and 90%.41 From population pharmacokinetic analyzes, the mean total distribution volume at steady state was 7.11 L.
Elimination
IXE is likely broken down into small peptides and amino acids through catabolic pathways. The mean systemic clearance was 0.39 L/day. Clearance and volume of distribution increase as body weight increases. In the population pharmacokinetic analysis (PK), the average serum clearance was 0.0161 L/hour. Clearance is dose-independent. The mean elimination half-life, as estimated from the population pharmacokinetic analysis, is 13 days in patients with plaque psoriasis.41
Effectiveness Data of IXE in Ankylosing Spondylitis
Three RCTs of Patients with as Evidenced the Efficacy of IXE (See Table 1)
COAST-V42 was a randomized, double-blind, active and placebo-controlled Phase III study evaluating the safety and efficacy of IXE in patients with active radiographic axSpA who have not previously been treated with biological disease-modifying antirheumatic drugs (bDMARD). The study included 341 patients who randomized into four different groups in a 1:1:1:1 manner. Patients had the following characteristics: age over 18 years, established diagnosis of axSpA and fulfillment of the SpondyloArthritis international Society (ASAS) criteria for axSpA5 radiographic (modified New York Criteria 4 sacroiliitis and characteristic ≥1 SpA), active disease defined by Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) ≥4 and total numerical scale of back pain ≥4 and inadequate response to at least 2 NSAIDs or intolerance to NSAID therapy. 38% of the patients initially screened failed to meet the modified New York criteria. Finally, 341 patients were randomized to the following arms: 87 placebo patients, 90 patients with 40 mg adalimumab (ADA) as an active comparator, 83 patients with 80 mg of IXE q2w and 81 patients with 80 mg of IXE q4w. Patients assigned to IXE treatment regimens were randomly assigned (1:1) to receive an initial dose of 80 or 160 mg IXE at week 0. The percentages of completion of the 16-week blinded treatment administration period were 86 out of 87 for placebo (99%), 88 out of 90 for ADA (98%), 79 out of 83 for IXE q2w (95%) and 78 out of 81 for IXE q4w (96%). Nine patients stopped the trial before week 16. The primary end point was the ASAS40 response at week 16. The primary-secondary endpoints were ASAS20, BASDAI 50 (≥50% improvement in BASDAI score from baseline) and inactivity score of ankylosing spondylitis disease (ASDAS) (ASDAS <1.3) Secondary endpoints included change from baseline at week 16 in: ASDAS, bath ankylosing spondylitis functional index (BASFI), spinal column MRI assessed with SPARCC (SpA Research Consortium of Canada) score,43 summary of physical components at 36 elements in short form (SF-36 PCS) and ASAS Health Index (ASAS-HI).44 The mean baseline age, the percentage of men and women, the race was similar in the 4 groups. Mean duration of axSpA symptoms, mean duration from axSpA diagnosis, number of patients using NSAIDs at baseline and mean disease scores (ASDAS, BASDAI, BASFI, ASAS-HI and SF-36 PCS) and baseline SPARCC MRI scores were comparable across all groups. The primary end point, ASAS40 response at week 16, was achieved by a larger number of patients treated with IXE q2W (43 out of 83 [52%], p <0.0001) and IXE q4W (39 out of 81 [48%], p <0.0001) compared to those who received placebo (16 of 87 [18%]). The percentage of patients who achieved the ASAS20 response at week 16 was higher with IXE q2W (57 of 83 [69%], p = 0.0002) and IXE q4W (52 of 81 [64%], p = 0.0015) compared placebo (35 of 87 [40%]). The ADA group also showed significant improvements over placebo for ASAS40 (32 out of 90 [36%], p = 0.0053) and ASAS20 (53 out of 90 [59%], p = 0.0075) at week 16. Significant improvements in IXE groups were noted as early as 1 week after treatment. BASDAI 50 response was achieved by patients who received IXE q2w 43% (p <0.0001) and IXE q4W 42% (p <0.0001) compared to those who received 17% placebo. Inactive ASDAS disease (<1.3) at 16 weeks was achieved by patients who received IXE q2W 11% (p <0.01) and IXE q4W 16% (p <0.01) compared to those who received placebo 2% Patients who received one of the two IXE regimens showed significantly greater improvements at week 16 in the SPARCC spine scores compared to placebo. Patients treated with IXE q2w had a variation of −9.6 compared to baseline SPARCC score (p <0.001) and IXE q4w had a variation of −11.0 (p <0.001) while for those who received placebo the variation was only −1.5. The starting dose of 160 versus 80 mg at week 0 did not lead to an improvement in the results observed at week 16. Compared to placebo, patients who received one of the two active regimens showed significantly greater improvements for all other secondary endpoints such as ASDAS, BASFI, SF −36 PC and ASAS-HI at week 16.42
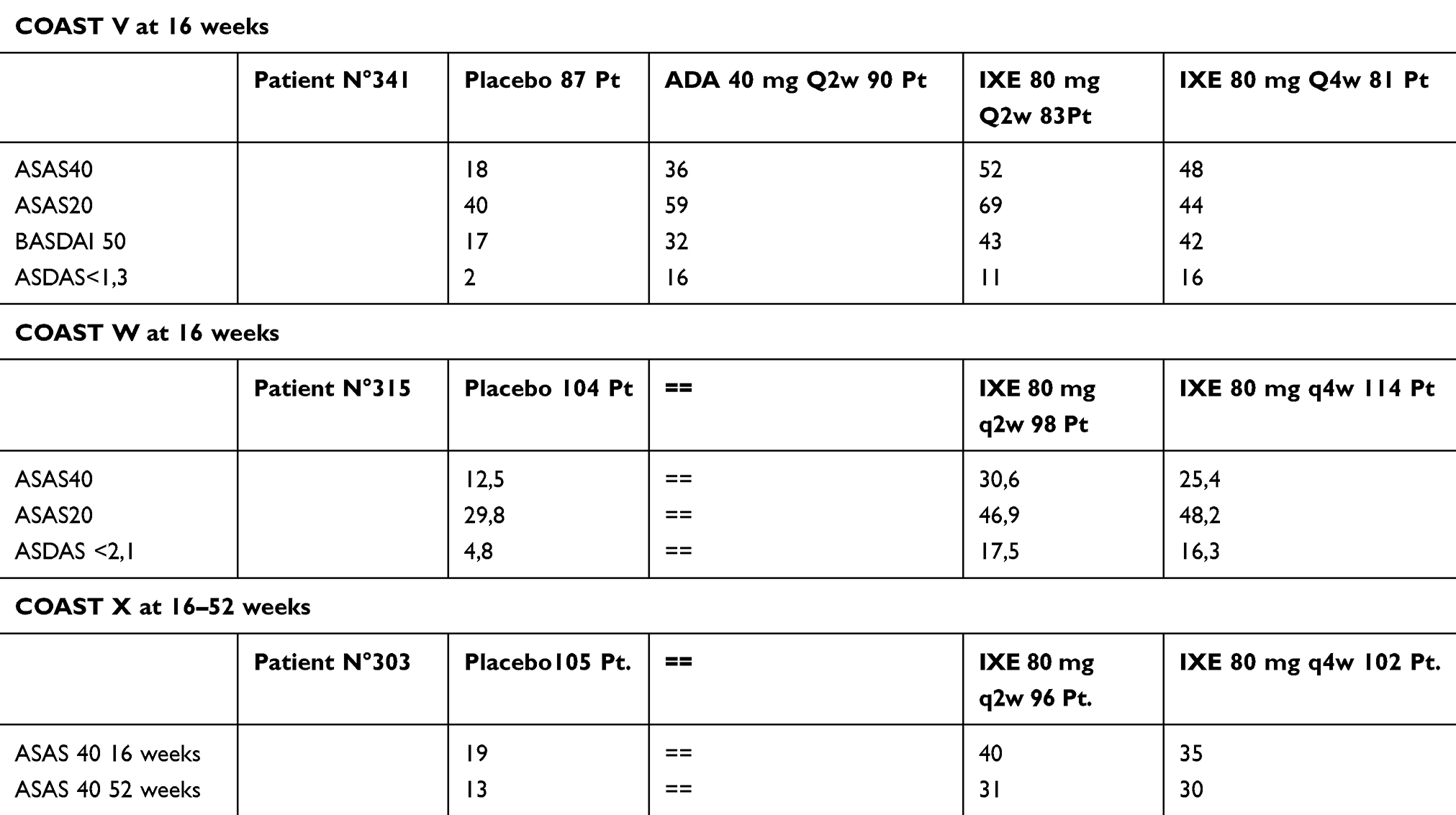 |
Table 1 Percentage of Achievement of the Primary End-Points in Three RCTs of IXE in AS |
COAST-W45 was a randomized, double-blind, placebo-controlled phase III study to evaluate safety and efficacy in patients with active radiographic axSpA with inadequate response to one or two TNFi or intolerance to TNFi. The study includes 315 patients who were randomized to three different arms. The inclusion criteria were: age over 18 years, established diagnosis of axSpA and meet the ASAS criteria for radiographic axSpA 44 (sacroiliitis using modified New York Criteria 4 and ≥1 SpA), active disease defined by BASDAI ≥4 and numerical scale of total back pain ≥4 and with previous inadequate response to one or two TNFi after at least 12 weeks of therapy or intolerance to TNFi. The exclusion criteria in COAST-W were total ankylosis of the spine, the current or previous history of the past 5 years of malignancy and the current or previous history of the use of bDMARDs. Three hundred fifteen patients were randomly assigned in the following arms: 104 patients on placebo, 98 patients at 80 mg IXE q2w and 114 patients at 80 mg IXE q4w. The completion rates were as follows: 92 (89.4%) of 104 for the placebo, 90 (91.8%) of 98 for IXE q2w and 99 (86.8%) of 114 for IXE q4w. The primary end point was the percentage of achievement and improvement of ASAS40 in disease activity at week 16. The secondary endpoints were ASAS20 and spondylitis disease activity score (ASDAS <2.1). Other important secondary endpoints included change from baseline to week 16 in: ASDAS, BASFI, BASDAI, MRI of the spine assessed with SPARCC score, PCS SF-36 and ASAS-HI. SPARCC MRI spine and SI joint scores were analyzed using covariance analysis based on the observed case. The basic demographics and characteristics of the disease were similar between the treatment groups. Average duration of axSpA symptoms, average duration since diagnosis of axSpA, number of patients with prior baseline TNFi treatment and average disease scores (ASDAS, BASDAI, BASFI, ASAS-HI, SF-36 PCS) and SPARCC MRI scores at the baseline were comparable across all groups. The primary end point, the ASAS40 response at week 16, was achieved by a larger number of patients treated with IXE q2w (30 of 98 [30.6%], p = 0.003) and IXE q4w (29 of 114 [25, 4%], p = 0.017) compared to those who received placebo (13 out of 104 [12.5%]). The percentage of patients who achieved the ASAS20 response at week 16 was higher with IXE q2w (46 of 98 [46.9%], p <0.05) and IXE q4w (55 of 114 [48.2%], p < 0.001) compared to placebo (31 of 104 [29.8%]). Patients who received one of the two IXE regimens showed significantly greater improvements at week 16 in the SPARCC spine scores compared to placebo. Patients who received IXE q2w had a variation of −4.0} 1.5 compared to baseline SPARCC score (p <0.001) and IXE q4w had a variation of −3.0} 1.4 (p <0, 01) while those who received placebo the variation was +3.3} 1.4. The initial dose of 160 compared to 80 mg at week 0 did not lead to an improvement in efficacy observed at week 16. I patients who received one of the two active regimens showed significantly greater improvements at week 16 for all major secondary endpoints such as ASDAS, BASDAI, BASFI, SF-36 PCS and ASAS-HI.45
In the extension of the two studies to 52 weeks, adults with active r-axSpA were randomized from 1:1:1:1 (n = 341) to 80 mg of ixekizumab every 2 (IXE q2W) or 4 weeks (IXE q4W), placebo (PBO) or 40 mg of adalimumab q2W (ADA) in COAST-V and 1:1: 1 (n = 316) at IXE q2W, IXE q4W or PBO in COAST-W. At week 16, patients treated with IXE continued the assigned treatment; patients who received PBO or ADA were re-randomized from 1:1 to IXE q2W or IXE q4W (PBO/IXE, ADA/IXE) until week 52. In COAST-V, Assessment of SpondyloArthritis international Society 40 (ASAS40) response rates (intent-to-treat population, unanswered imputation) at weeks 16 and 52 were 48% and 53% (IXE q4W); 52% and 51% (IXE q2W); 36% and 51% (ADA/IXE); 19% and 47% (PBO/IXE). The corresponding ASAS40 response rates in COAST-W were 25% and 34% (IXE q4W); 31% and 31% (IXE q2W); 14% and 39% (PBO/IXE). Both IXE regimens supported improvements in disease activity, physical function, objective markers of inflammation, QoL, overall health and function for up to 52 weeks. Improvements in patient function at week 16 (change from baseline in BASFI) were sustained for up to 52 weeks in patients continuously treated with IXE, as well as improvements in QoL measurements (change from baseline in SF-36 PCS) and health functioning (change from baseline to ASAS HI). Week 16 improvements in spinal magnetic resonance imaging and objective inflammation were sustained up to 52 weeks for SPARCC spine and sacroiliac joint scores (assessed beyond week 16 in COAST-V only) and changes from baseline in CRP.46
COAST-X was a 52-week, randomized, double-blind, placebo-controlled parallel group study. Eligible participants were adults (aged ≥18 years) with active axial spondyloarthritis without defined radiographic sacroiliitis (non-radiographic axial spondyloarthritis), objective signs of inflammation (via magnetic resonance or C-reactive protein) and an inadequate response or intolerance to non-steroidal drugs anti–inflammatories (NSAIDs). Patients were randomly assigned (1:1:1) to receive 80 mg of IXE subcutaneously every 4 weeks (q4W) or every 2 weeks (q2W) or placebo. The primary endpoints were evaluation of the response of SpondyloArthritis International Society-40 (ASAS40) (defined as a 40% improvement or more and an absolute improvement from baseline of 2 units or more [range 0–10] in at least three of the four domains [overall patient, spinal pain, function and inflammation] without worsening in the remaining domain) at weeks 16 and 52. 303 patients (105 on placebo, 96 at IXE q4W and 102 at IXE q2W) were enrolled. Both primary endpoints were achieved: ASAS40 at week 16 (IXE q4W: 34 [35%] on 96, p = 0.0094 vs placebo; IXE q2W: 41 [40%] on 102, p = 0.0016; placebo: 20 [19%] of 105) and ASAS40 at week 52 (IXE q4W: 29 [30%] of 96, p = 0.0045; IXE q2W: 32 [31%] of 102, p = 0.0037; placebo: 14 [13%] of 105). Study results showed that IXE was superior to placebo for improving signs and symptoms in patients with non-radiographic axial spondyloarthritis at weeks 16 and 52.47
Safety of Ixekizumab in AS
Safety outcomes reported in IXE studies are summarized in Table 2. Subcutaneous IXE 80 mg was generally well tolerated in COAST-V42,46 e COAST-W43,46 studies for Ax-SpA, and COAST-X.47 All kinds of adverse events were evaluated: infections, injection site reactions, neutropenia, anterior uveitis, inflammatory bowel diseases, cerebrocardiovascular events, depression, immunogenicity, malignancies, deaths. In COAST-V42 the treatment-emergent adverse events (TEAEs) were similar in all groups (from 40% to 49%), and the most frequent were nasopharyngitis and upper respiratory tract infections (in more than 5% of patients in IXE groups). In COAST-W45 TEAEs were slightly more frequent in the IXE groups, without differences in the q2W and q4W groups (60–64%) with respect to placebo (49%). The events were usually mild or moderate, and upper respiratory tract infections and injection site reactions were most frequently observed. Similar percentages of TEAEs resulted in COAST-X47 where the most common were nasopharyngitis (16% and 1% in IXE q2W and q4W, respectively) and injection site reactions (25% and 19% in IXE q2W and q4W, respectively). In COAST-V and COAST-W long-term extension trials (LTE),46 TEAEs occurred in 61.1% and in 63.7% of patients, respectively. Serious adverse events were rare and similar in all groups of the 3 trials, as well as discontinuations. Looking to infections, no case of TB occurred in all studies; one case of Herpes zoster in the IXE q4W group of COAST-W43 study and two cases of Herpes Zoster in the IXE q4W group in COAST-X47 were recorded; although mucocutaneous Candida infections have previously been described in clinical studies of IXE in psoriasis and psoriatic arthritis,5,8,42 in these trials Candida infection was extremely rare, with 2 cases of candida (esophageal and genital) in COAST-W45 and 2 cases in COAST-V LTE46 and COAST-W LTE;46 no Candida infections in COAST-V42 and COAST-X47 occurred. Very few serious infections occurred in the IXE groups in COAST-V42 (1 gastroenteritis and 1 urinary tract infection) and in IXE q4W group in COAST-W45 (1 peritonitis and 1 pharyngitis). All these patients continued the trials. In COAST-V-LTE46 1 cellulitis, 1 pneumonia and 1 tonsillitis were reported; in COAST-W-LTE46 one gastroenteritis, one pneumonia and one sinusitis occurred. Injection site reactions (ISR) are one of the most frequent TEAEs in IXE treated groups in all trials, but very often they are mild, decrease over time and rarely led to discontinuations42,45-47 We know that IL-17A antagonism is involved in neutrophils trafficking and granulopoiesis,48 so a decrease in neutrophils count with IXE could be expected. However, during IXE therapy neutropenia has been described in small percentages of patients, usually grade 1 (1.5–2.0 x 109 cells/liters), rarely grade 2 (1.0–1.5 x 109 cells/liters).42,45-47 There was only one case of neutropenia grade 4 (<0.5 x 109 cells/liters) in COAST-W in patients with acute promyelocytic leukemia (PML), that occurred 4 weeks post baseline (this patient had a genetic risk factor for PML).45 There have been reports of new onset or exacerbations of inflammatory bowel diseases (IBD) in patients treated with secukinumab.11 In IXE studies there is the description of some cases of IBD, both Crohn’s disease and ulcerative colitis, but they are often mild or moderate, adjudicated “probable”, rarely “definitive” and overall they are not frequent in all the studies: COAST-V,42 COAST-W,45 COAST-V ETP,46 COAST-X.47 Even no IBD cases were described in COAST-W ETP46 (Table 2). The incidence of anterior uveitis during IXE treatment was described and, such as IBD, was something higher in patients affected by Ax-SpA with prior inadequate response or intolerance of 1 or 2 TNF inhibitors (COAST-W45) than in bDMARD-naive Ax-SpA patients (COAST-V42). It seems that some comorbidities, like IBD and anterior uveitis, could be associated with longer disease duration.49 In many cases, patients had a pre-existing history of anterior uveitis and were HLA B27+45 About malignancies, there was only one case of acute promyelocytic leukemia (PML) few weeks after IXE started in a patient with genetic predisposition in COAST-W45 and a bladder cancer in COAST-V LTE.46 About cerebrocardiovascular events, there was one case of atrial fibrillation in IXE q2W group in COAST-W,45 two cases of cerebrocardiovascular events in COAST-V ETP46 and one major cardiovascular event (acute myocardial infarction) in COAST-W ETP.46 There was no death in all the trials. There are some reporting of depression, but it is more frequent in the placebo groups and in patients affected by pre-existing anxiety.45,47 Few cases of psoriasis occurred in COAST-W45 (1 patient with previous history) and in COAST-W ETP46 (4 patients). About immunogenicity, antidrug antibodies (ADA) were detected in less than 5% of patients of IXE groups, but none neutralising in COAST-V42 and in less than 9% of patients of IXE groups in COAST-W.45 In COAST-W45 they were considered neutralising in 1% of patients. In most patients, they were at low titres. No association was identified between treatment-emergent ADA positivity and ASAS response, ISRs or potential allergic/hypersensitivity events.42,45,46 During the 52-week ETP of COAST-V and COAST-W, the authors looked at the pooled exposure-adjusted incidence rate per 100 patients years (EAIR). Among IXE patients the EAIRs for serious infections was 2.0. The pooled EAIRs for Candida infections, IBD and grade 3–4 neutropenia were ≤1 event/100 patient-years. EAIR for anterior uveitis is similar to the upper limit of the range reported for patients treated with TNF-inhibitors (2.6–3.5), remembering that COAST-W included anti-TNF-experienced population.46
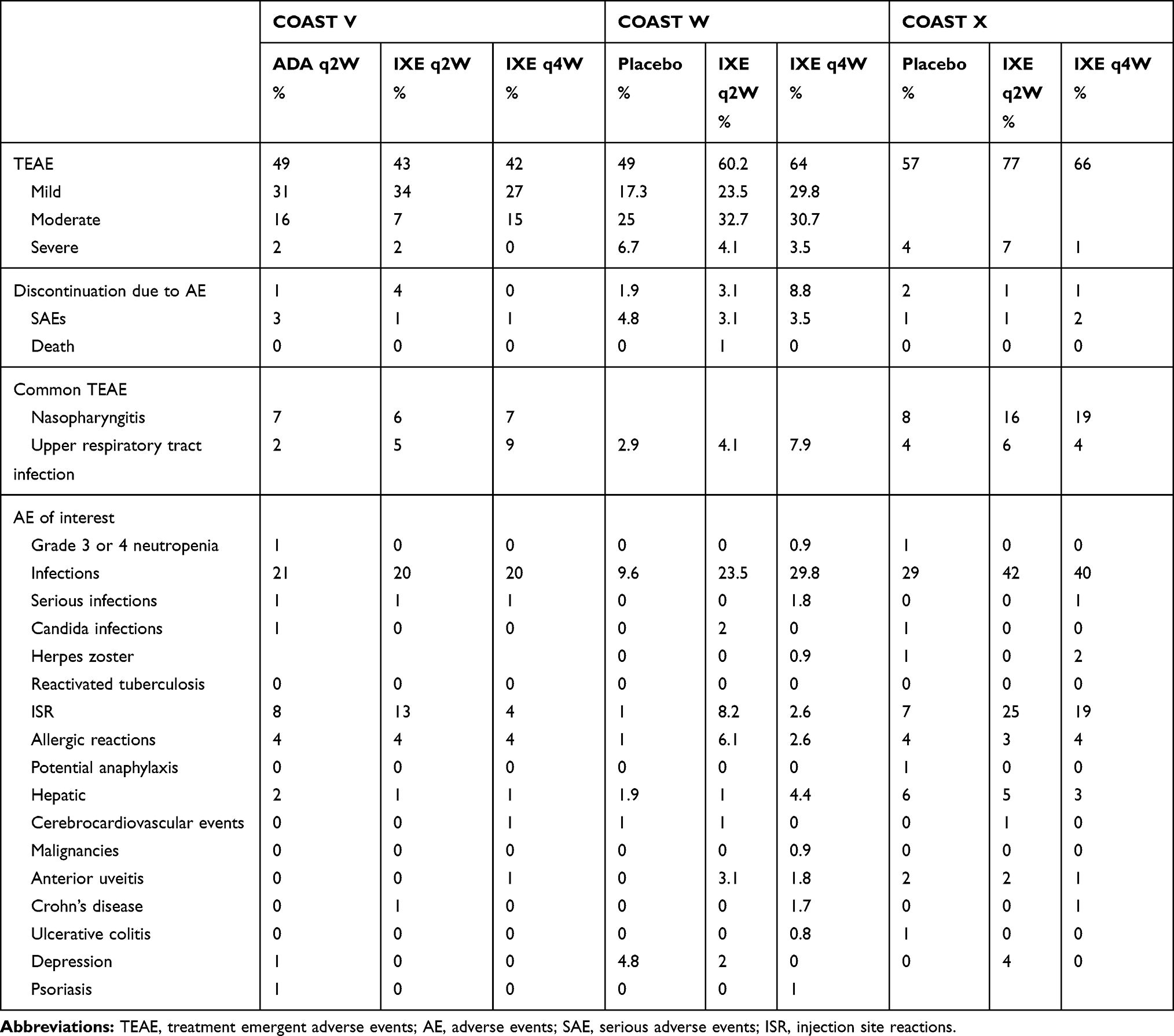 |
Table 2 Percentage of Adverse Events in the 3 RCTs |
Which Features of IXE Can Guide Its Choice When Using an Anti-IL-17
The recent American College of Rheumatology guidelines for the treatment of AS and nrx-axSpA indicate anti-TNFs as first-line therapy in patients with no relief by taking NSAIDs.50 Anti–Il-17 secukinumab and IXE are placed as second choice in patients resistant or intolerant to anti-TNFs. However, the nature itself of recommendations/guidelines does not allow to indicate the more appropriate therapeutic intervention for the single patient. In other words, in current clinical practice clinicians should evaluate the characteristics of biologics in terms of efficacy and safety, and the patient-related variables driving the therapeutic choice. As previously underlined,51 some differences exist among biologics in terms of efficacy on extra-articular manifestations, including enthesitis, dactylitis, anterior uveitis and inflammatory bowel diseases. The same is true in terms of infection risk,51 and TB reactivation risk.34 Data from 3 RCTs of IXE, enrolling a cumulative number of 959 patients with AS, demonstrated a good safety profile, with a low increased risk of mild to moderate infections, and no case of TB reactivation. These results seem to be related, unlike TNFα, to the negligible role played by IL-17a in systemic immunity,52 and TB granuloma integrity maintenance.34 Regarding the persistence, which is directly related to the efficacy and safety, the only information on IXE are provided by the 52-week LTE studies of COAST-V and COAST-W trials.46 In the first trial, 20 (5.9%) out of 341 patients discontinued the treatment. Notably, 12 (60%) patients withdrew the consent to prosecute the trial, and only 8 abandoned for adverse events or lack of efficacy. In the second trial, 31 patients (9.8%) discontinued the treatment, mostly for lack of efficacy (11 patients) or adverse events (10 patients). The increased percentage of discontinuations in COAST-W trial may be attributed, at least in part, to the enrollment of patients who previously were exposed to 1 or more anti-TNF. However, long-term studies from real-life are required to better address the persistence of IXE in the treatment o fax-SpA. Surprisingly, important clinical features of ax-SpA such as enthesitis and dactylitis were not assessed in IXE trials. In a recent report,53 these clinical manifestations were observed in 33.4% and 9.8% out of 407 patients from the CORRONA registry. Comparable percentages resulted in a meta-analysis from Europe.54 Nevertheless, based on the efficacy data on dactylitis and enthesitis in patients with psoriatic arthritis,55 we believe that a history of, or current enthesitis and dactylitis occurrence may represent a relevant variable to drive the choice toward IXE, instead of anti-TNFs. To conclude, in view of the need for a personalized therapy, available data support a relevant role for IXE as first-line therapy for patients at high infection and TB risk, those with enthesitis and dactylitis. On the contrary, the drug seems contraindicated in patients with anterior uveitis and inflammatory bowel diseases associated SpA.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sieper J, Poddubnyy D. Axial spondyloarthritis. Lancet. 2017;390(10089):73–84. doi:10.1016/S0140-6736(16)31591-4
2. Simone D, Al Mossawi MH, Bowness P. Progress in our understanding of the pathogenesis of ankylosing spondylitis. Rheumatology (Oxford). 2018;57(suppl 6):vi4–vi9. doi:10.1093/rheumatology/key001
3. Khan MA, van der Linden S. Axial spondyloarthritis: a better name for an old disease: a step toward uniform reporting. ACR Open Rheumatol. 2019;1(5):336–339. doi:10.1002/acr2.11044
4. Van der Linden SM, Valkenburg HA, Cats A. Evaluation of diagnostic criteria for ankylosing spondylitis: a proposal for modification of the New York criteria. Arthritis Rheum. 1984;27:361–368. doi:10.1002/art.1780270401
5. Rudwaleit M, van der Heijde D, Landewé R, et al. The development of Assessment of Spondyloarthritis International Society classification criteria for axial spondyloarthritis part II: validation and final selection. Ann Rheum Dis. 2009;68(6):777–783.
6. Wanders A, Heijde D, Landewé R, et al. Nonsteroidal antiinflammatory drugs reduce radiographic progression in patients with ankylosing spondylitis: a randomized clinical trial. Arthritis Rheum. 2005;52(6):1756–1765. doi:10.1002/art.21054
7. Balazcs E, Sieper J, Bickham K, et al. A randomized, clinical trial to assess the relative efficacy and tolerability of two doses of etoricoxib versus naproxen in patients with ankylosing spondylitis. BMC Musculoskelet Disord. 2016;17(1):426. doi:10.1186/s12891-016-1275-5
8. Kristensen LE, Jakobsen AK, Askling J, Nilsson F, Jacobsson LT. Safety of etoricoxib, celecoxib, and nonselective nonsteroidal antiinflammatory drugs in ankylosing spondylitis and other spondyloarthritis patients: a Swedish National Population-Based Cohort Study. Arthritis Care Res (Hoboken). 2015;67(8):1137–1149. doi:10.1002/acr.v67.8
9. Lories RJ. Advances in understanding the pathophysiology of spondyloarthritis. Best Pract Res Clin Rheumatol. 2018;32(3):331–341. doi:10.1016/j.berh.2018.12.001
10. Dubash S, McGonagle D, Marzo-ortega H. New advances in the understanding and treatment of axial spondyloarthritis: from chance to choice. Ther Adv Chronic Dis. 2018;9(3):77–87. doi:10.1177/2040622317743486
11. Haroon N, Inman RD, Learch TJ, et al. The impact of tumor necrosis factor α inhibitors on radiographic progression in ankylosing spondylitis. Arthritis Rheum. 2013;65(10):2645–2654. doi:10.1002/art.38070
12. Minozzi S, Bonovas S, Lytras T, et al. Risk of infections using anti-TNF agents in rheumatoid arthritis, psoriatic arthritis, and ankylosing spondylitis: a systematic review and meta-analysis. Expert Opin Drug Saf. 2016;15(sup1):11–34. doi:10.1080/14740338.2016.1240783
13. Baddley JW, Cantini F, Goletti D, et al. ESCMID Study Group for Infections in Compromised Hosts (ESGICH) consensus document on the safety of targeted and biological therapies: an infectious diseases perspective (Soluble immune effector molecules [I]: anti-tumor necrosis factor-α agents). Clin Microbiol Infect. 2018;24(Suppl 2):S10–S20. doi:10.1016/j.cmi.2017.12.025
14. Taams LS, Steel KJA, Srenathan U, Burns LA, Kirkham BW. IL-17 in the immunopathogenesis of spondyloarthritis. Nat Rev Rheumatol. 2018;14(8):453–466. doi:10.1038/s41584-018-0044-2
15. Blair HA. Secukinumab: a review in ankylosing spondylitis. Drugs. 2019;79(4):433–443. doi:10.1007/s40265-019-01075-3
16. Kiwalkar S, Beier S, Deodhar A. Ixekizumab for treating ankylosing spondylitis. Immunotherapy. 2019;11(15):1273–1282. doi:10.2217/imt-2019-0094
17. Benjamin R, Parham P. HLA-B27 and disease: a consequence of inadvertent antigen presentation? Rheum Dis Clin North Am. 1992;18(1):11–21.
18. Burton PR, Clayton DG, Cardon LR, et al. Association scan of 14,500 nonsynonymous SNPs in four diseases identifies autoimmunity variants. Nat Genet. 2007;39:1329–1337.
19. Kollnberger S, Chan A, Sun MY, et al. Interaction of HLA-B27 homodimers with KIR3DL1 and KIR3DL2, unlike HLA-B27 heterotrimers, is independent of the sequence of bound peptide. Eur J Immunol. 2007;37(5):1313–1322. doi:10.1002/eji.200635997
20. Adamopoulos IE, Chao CC, Geissler R, et al. Interleukin-17A upregulates receptor activator of NF-κB on osteoclast precursors. Arthritis Res Ther. 2010;12:R29. doi:10.1186/ar2936
21. Huang H, Kim HJ, Chang EJ, et al. IL-17 stimulates the proliferation and differentiation of human mesenchymal stem cells: implications for bone remodeling. Cell Death Differ. 2009;16(10):1332–1343. doi:10.1038/cdd.2009.74
22. Nam D, Mau E, Wang Y, et al. T- Lymphocytes enable osteoblast maturation via IL-17F during the early phase of fracture repair. PLoS One. 2012;7(6):e40044. doi:10.1371/journal.pone.0040044
23. Kim YG, Park JW, Lee JM, et al. IL-17 inhibits osteoblast differentiation and bone regeneration in rat. Arch Oral Biol. 2014;59:897–905. doi:10.1016/j.archoralbio.2014.05.009
24. McGonagle DG, McInnes IB, Kirkham BW, Sherlock J, Moots R. The role of IL-17A in axial spondyloarthritis and psoriatic arthritis: recent advances and controversies. Ann Rheum Dis. 2019;78(9):1167–1178. doi:10.1136/annrheumdis-2019-215356
25. Weinstein JE, Pepple KL. Cytokines in uveitis. Curr Opin Ophthalmol. 2018;29(3):267–274. doi:10.1097/ICU.0000000000000466
26. Reinhardt A, Yevsa T, Worbs T, et al. Interleukin-23–dependent γ/δ T cells produce interleukin-17 and accumulate in the enthesis, aortic valve, and ciliary body in mice. Arthritis Rheumatol. 2016;68(10):2476–2486. doi:10.1002/art.39732
27. Lories RJ, Haroon N. Evolving concepts of new bone formation in axial spondyloarthritis insights from animal models and human studies. Best Pract Res Clin Rheumatol. 2017;31(6):877–886. doi:10.1016/j.berh.2018.07.007
28. Lee JS, Tato CM, Joyce-shaikh B, et al. Interleukin-23-independent IL-17 production regulates intestinal epithelial permeability. Immunity. 2015;43(4):727–738. doi:10.1016/j.immuni.2015.09.003
29. Gracey E, Qaiyum Z, Almaghlouth I, et al. IL-7 primes IL-17 in mucosal-associated invariant T (MAIT) cells, which contribute to the Th17-axis in ankylosing spondylitis. Ann Rheum Dis. 2016;75(12):2124–2132. doi:10.1136/annrheumdis-2015-208902
30. Ciccia F, Guggino G, Rizzo A, et al. Type 3 innate lymphoid cells producing IL-17 and IL-22 are expanded in the gut, in the peripheral blood, synovial fluid and bone marrow of patients with ankylosing spondylitis. Ann Rheum Dis. 2015;74(9):1739–1747. doi:10.1136/annrheumdis-2014-206323
31. European Medicine Agency. EMEA/H/C/003729. Cosentyx: EPAR – Summary for the public. March 2, 2015. Available fom: https://www.ema.europa.eu/en/documents/overview/cosentyx-epar-summary-public_en.pdf.
32. Novartis receives two new FDA approvals for Cosentyx to treat patients with ankylosing spondylitis and psoriatic arthritis in the US. Jan 15, 2016. Available fom: https://novartis.gcs-web.com/novartis-receives-fda-approvals-for-secukinumab-in-as-and-psa.
33. Blair HA, Dhillon S. Secukinumab: a review in ankylosing spondylitis. Drugs. 2016;76(10):1023–1030. doi:10.1007/s40265-016-0598-8
34. Cantini F, Nannini C, Niccoli L, Petrone L, Ippolito G, Goletti D. Risk of tuberculosis reactivation in patients with rheumatoid arthritis, ankylosing spondylitis, and psoriatic arthritis receiving non-anti-TNF-targeted biologics. Mediators Inflamm. 2017;2017:8909834. doi:10.1155/2017/8909834
35. Li J, Casanova JL, Puel A. Mucocutaneous IL-17 immunity in mice and humans: host defense vs. excessive inflammation. Mucosal Immunol. 2018;11(3):581–589. doi:10.1038/mi.2017.97
36. Manasson J, Wallach DS, Guggino G, et al. IL-17 Inhibition in spondyloarthritis associates with subclinical gut microbiome perturbations and a distinctive IL-25-driven intestinal inflammation. Arthritis Rheumatol. 2019. doi:10.1002/art.41169
37. Winthrop KL, Mariette X, Silva JT, et al. ESCMID Study Group for Infections in Compromised Hosts (ESGICH) consensus document on the safety of targeted and biological therapies: an infectious diseases perspective (soluble immune effector molecules [II]: agents targeting interleukins, immunoglobulins and complement factors). Clin Microbiol Infect. 2018;24 Suppl 2(Suppl 2):S21–S40. doi:10.1016/j.cmi.2018.02.002
38. Yamada A, Wang J, Komaki Y, Komaki F, Micic D, Sakuraba A. Systematic review with meta-analysis: risk of new onset IBD with the use of anti-interleukin-17 agents. Aliment Pharmacol Ther. 2019;50(4):373–385. doi:10.1111/apt.15397
39. European Medicine Agency. EMEA/H/C/003943. Taltz: EPAR summary for the public. April 25, 2016. updated August 28, 2019. Available from: https://www.ema.europa.eu/en/documents/overview/taltz-epar-summary-public_en.pdf.
40. Eli-Lilly press release. FDA approves Taltz for treatment of ankylosing spondylitis. Available from: https://investor.lilly.com/news-releases/news-release-details/lilly-receives-us-fda-approval-taltzr-ixekizumab-treatment. August 26, 2019.
41. Taltz (Ixekizumab), packager insert. Mechanism of Action, Pharmacodynamics and Pharmacokinetics of IXE. IN, USA: Eli Lilly and Company; 2018.
42. Van der heijde D, Wei JC, Dougados M, et al. Ixekizumab, an interleukin-17A antagonist in the treatment of ankylosing spondylitis or radiographic axial spondyloarthritis in patients previously untreated with biological disease-modifying anti-rheumatic drugs (COAST-V): 16 week results of a Phase III randomised, double-blind, active-controlled and placebo-controlled trial. Lancet. 2018;392(10163):2441–2451. doi:10.1016/S0140-6736(18)31946-9
43. Maksymowych WP, Wichuk S, Chiowchanwisawakit P, Lambert RG, Pedersen SJ. Development and preliminary validation of the spondyloarthritis research consortium of Canada magnetic resonance imaging sacroiliac joint structural score. J Rheumatol. 2015;42(1):79–86. doi:10.3899/jrheum.140519
44. Zochling J. Measures of symptoms and disease status in ankylosing spondylitis: Ankylosing Spondylitis Disease Activity Score (ASDAS), Ankylosing Spondylitis Quality of Life Scale (ASQoL), Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), Bath Ankylosing Spondylitis Functional Index (BASFI), Bath Ankylosing Spondylitis Global Score (BAS-G), Bath Ankylosing Spondylitis Metrology Index (BASMI), Dougados Functional Index (DFI), and Health Assessment Questionnaire for the Spondylarthropathies (HAQ-S). Arthritis Care Res (Hoboken). 2011;63(Suppl 11):
45. Deodhar A, Poddubnyy D, Pacheao-tena C, et al. Efficacy and safety of ixekizumab in the treatment of radiographic axial spondyloarthritis: sixteen-week results from a Phase III randomized, double-blind, placebo-controlled trial in patients with prior inadequate response to or intolerance of tumor necrosis factor inhibitors. Arthritis Rheumatol. 2019;71(4):599–611. doi:10.1002/art.40753
46. Dougados M, Wei JC, Landewé R, et al.; COAST-V and COAST-W Study Groups. Efficacy and safety of ixekizumab through 52 weeks in two Phase 3, randomised, controlled clinical trials in patients with active radiographic axial spondyloarthritis (COAST-V and COAST-W). Ann Rheum Dis. 2020;79(2):176–185.
47. Deodhar A, van der Heijde D, Gensler LS, et al.; COAST-X Study Group. Ixekizumab for patients with non-radiographic axial spondyloarthritis (COAST-X): a randomised, placebo-controlled trial. Lancet. 2020;395(10217):53–64.
48. Krstic A, Mojsilovic S, Jovcic G, Bugarski D. The potential of interleukin-17 to mediate hematopoietic response. Immunol Res. 2012;52(1–2):34–41. doi:10.1007/s12026-012-8276-8
49. Varkas G, Vastesaeger N, Cypers H, et al. Association of inflammatory bowel disease and acute anterior uveitis, but not psoriasis, with disease duration in axial spondyloarthritis: results from two Belgian nationwide axial spondyloarthritis cohorts. Arthritis Rheumatol. 2018;70:1588–1596. doi:10.1002/art.40551
50. Ward MM, Deodhar A, Gensler LS, et al. 2019 Update of the American College of Rheumatology/Spondylitis Association of America/Spondyloarthritis research and treatment network recommendations for the treatment of ankylosing spondylitis and nonradiographic axial spondyloarthritis. Arthritis Care Res (Hoboken). 2019;71(10):1285–1299. doi:10.1002/acr.v71.10
51. Cantini F, Niccoli L, Nannini C, et al. Tailored first-line biologic therapy in patients with rheumatoid arthritis, spondyloarthritis, and psoriatic arthritis. Semin Arthritis Rheum. 2016;45(5):519–532. doi:10.1016/j.semarthrit.2015.10.001
52. Blauvelt A. Safety of secukinumab in the treatment of psoriasis. Expert Opin Drug Saf. 2016;15(10):1413–1420. doi:10.1080/14740338.2016.1221923
53. Mease PJ, Heijde DV, Karki C, et al. Characterization of patients with ankylosing spondylitis and nonradiographic axial spondyloarthritis in the US-based corrona registry. Arthritis Care Res (Hoboken). 2018;70(11):1661–1670. doi:10.1002/acr.23534
54. de Winter JJ, van Mens LJ, van der Heijde D, Landewé R, Baeten DL. Prevalence of peripheral and extra-articular disease in ankylosing spondylitis versus non-radiographic axial spondyloarthritis: a meta-analysis. Arthritis Res Ther. 2016;18(1):196. doi:10.1186/s13075-016-1093-z
55. Mease PJ, van der Heijde D, Ritchlin CT, et al. Ixekizumab, an interleukin-17A specific monoclonal antibody, for the treatment of biologic-naive patients with active psoriatic arthritis: results from the 24-week randomised, double-blind, placebo-controlled and active (adalimumab)-controlled period of the phase III trial SPIRIT-P1. Ann Rheum Dis. 2017;76(1):79–87. doi:10.1136/annrheumdis-2016-209709
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.