Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Therapeutic Efficacy of Bovine Basic Fibroblast Growth Factor Combined with Ultrapulsed Fractional CO2 Laser in Acne Scars: Randomized Controlled Trial
Authors Yuan C, Li J, Wang H, Gao L, Zheng Y, Ailan L
Received 28 June 2023
Accepted for publication 14 September 2023
Published 10 October 2023 Volume 2023:16 Pages 2813—2819
DOI https://doi.org/10.2147/CCID.S428017
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Chunying Yuan, Jianhua Li, Haiying Wang, Laiqiang Gao, Youyou Zheng, Li Ailan
Department of Dermatology, Dongying People’s Hospital, Dongying, Shandong, 257100, People’s Republic of China
Correspondence: Jianhua Li, Email [email protected]
Objective: To observe the therapeutic efficacy of ultrapulsed fractional CO2 laser combined with bovine basic fibroblast growth factor (bFGF) on acne scars, so as to provide clinical evidence for future treatment of acne scars.
Methods: One hundred and twenty patients with acne scars admitted between October 2021 and August 2022 were selected as the research participants, of which 60 cases treated with bFGF plus ultrapulsed fractional CO2 laser were regarded as the research group (RG) and 60 cases with ultrapulsed fractional CO2 laser therapy alone were set as the control group (CG). The clinical efficacy, Échelle d’évaluation clinique des cicatrices d’acné (ECCA) score, and scar base depth before and after treatment were comparatively analyzed, and changes in skin pore value, texture value and skin barrier function were detected. Finally, the duration of redness, scabbing and erythema after treatment and the incidence of adverse reactions after treatment were counted.
Results: A higher overall response rate was determined in RG versus CG (P< 0.05). Besides, RG was lower than CG in post-treatment ECCA score, scar base depth, skin pore value, texture value and transepidermal water loss (TEWL), and higher in skin water and epidermal oil content (P< 0.05). Moreover, the duration of redness, scabbing and erythema was shorter and the incidence of adverse reactions was lower in RG than in CG after treatment (P< 0.05).
Conclusion: The combination of bFGF and ultrapulsed fractional CO2 laser is highly effective and safe in the treatment of acne scars, which reserves widespread use in clinical practice.
Keywords: bovine basic fibroblast growth factor, ultrapulsed fractional CO2 laser, acne scars, safety, skin barrier function
Introduction
Acne is a chronic inflammatory skin disease in pilosebaceous units, with skin lesions commonly found in cheeks, forehead and mandible and can also involve the trunk; it is clinically characterized by pimples, papulae, and pustules and is often accompanied by sebum overflow, which is common in young men and women aged 15–25.1 For severe acne without targeted intervention, there may be serious skin infections that induce dermal and epidermal defects, which further develop into uneven skin and pigmentation, eventually forming acne scars and affecting facial appearance.2 Severe acne scarring can cause social and psychological obstacles to patients and affect their quality of life.3 With the development of the economy and the improvement of people’s cognition, acne patients have higher and higher requirements for facial beauty. Currently, there are various treatments for acne scars, such as scar removers, grinding, fat filling, micro-needle therapy, surgery, and traditional Chinese medicine, but the effect is not ideal.4 In 2004, researchers proposed that fractional laser could produce thermal damage to the treatment area through photothermal effect without damaging the surrounding normal tissues, and create a thermal bridge between the thermal damage area and the surrounding normal tissues, thus initiating the skin wound repair mechanism.5 The gradual improvement of fractional laser has made it widely used in the treatment of acne scars.6 Among them, ultrapulsed fractional CO2 laser has a remarkable effect. Different from the previous fractional laser, this laser therapy is more powerful with a better therapeutic effect on deep-seated and sunken scars. Meanwhile, it can pinch off the hyperplastic blood vessels, exerting a good therapeutic effect on the corresponding redness.7 However, a growing number of studies have pointed out that ultrapulsed fractional CO2 laser treatment of acne scars may lead to facial burning, pain, edema, erythema, scab and persistent pigmentation, with obvious adverse reactions.8,9 Therefore, it is urgent to find a reliable intervention measure to improve the safety of ultrapulsed fractional CO2 laser therapy.
Bovine basic fibroblast growth factor (bFGF), a biological agent that promotes the repair and regeneration of cells derived from mesoderm and ectoderm, is often used clinically in combination with laser therapy to reduce adverse reactions.10,11 We believe that the combination of bFGF can not only improve the safety of ultrapulsed fractional CO2 laser, but also provide a more reliable guarantee for therapeutic efficacy. But there’s a dearth of research to test our claims.
In view of this, this study analyzes the therapeutic effect of bFGF combined with ultrapulsed fractional CO2 laser on acne scars, so as to provide a more reliable reference for its future clinical application.
Materials and Methods
Research Population
From October 2021 to August 2022, 120 patients with acne scars were selected as study participants for a randomized controlled trial based on inclusion and exclusion criteria. This study met the requirements of the Medical Ethics Committee and was approved by Dongying people’s hospital Ethics Committee. All the study subjects were divided into 2 groups according to the random number table method, among them, 60 patients treated with bFGF + ultrapulsed fractional CO2 laser therapy and another 60 cases with ultrapulsed fractional CO2 laser treatment alone were regarded as the research group (RG) the control group (CG), respectively. This study will be conducted in strict compliance with the Declaration of Helsinki, and all study subjects signed an informed consent form.
Criteria for Patient Enrollment and Exclusion
All the patients included had moderate or severe facial acne scars, no coagulation dysfunction, no recent treatment history nor no scar constitution. Patients meeting any of the following criteria were excluded: epilepsy, melanocytic skin tumor, lupus erythematosus, pregnancy, herpes zoster, or vitiligo; seminal trauma at the treatment site and hereditary photosensitive diseases like xeroderma pigmentosum; history of mental illness; severe heart, liver and kidney diseases; intolerance to the treatment methods in this paper; patients who did not participate in the entire study.
Treatment Methods
Ultrapulsed fractional CO2 laser (Wuhan Huada Laser Equipment Co., Ltd., HD-230) therapy: Compound lidocaine cream was applied to the scar of the patient for surface anesthesia, and the face was routinely cleaned after being wrapped with plastic wrap (face-dedicated) for about 30 minutes. Then, the ultrapulsed fractional CO2 laser therapeutic instrument was used, and appropriate treatment parameters were selected according to the patient’s symptoms. The power, pulse time and dot spacing were set to 25–30W, 2 ms, and 1.2 cm, respectively. After treatment, ice packs were applied to the affected area to eliminate pain. Laser treatment was performed 1 time/month for a total of 3 treatments, and bFGF (Zhuhai Essex Bio-Technology, SFDA Approval No. S20040001, 21000IU (5g)/piece) was coated 30 min after laser treatment. bFGF was also required to be coated twice daily when laser treatment was not performed (once in the morning and once in the evening).
Endpoints
Efficacy was evaluated as follows by referring to the guidelines for the treatment of acne scars:12 marked response: most of the scars were flattened after treatment with the scar color close to the surrounding normal skin and high patient satisfaction; response: about half of the scars became flattened, with obviously reduced concave-convex scars and uneven colors after treatment, and the patients were satisfied with the treatment; nonresponse: the acne scar was not improved obviously, with the presence of new scars, and the patient was not satisfied with the treatment; overall response rate (ORR) = (marked response+response) cases/total cases ×100%. Before and after treatment, the Échelle d’évaluation clinique des cicatrices d’acné (ECCA) score of the two groups was compared (evaluated based on the weight of the scar nature; V-shaped punctate scars with a diameter < 2 mm: 15 points; U-shaped scars with a diameter of 2–4 mm and sheer edges: 20 points; M-shaped scars with irregular edges and a diameter > 4 mm: 25 points. Quantitative scoring based on scar quantity: 1, 2, and 3 points for a small number, a limited number, and a large number of scars, respectively; the total score is the product of scar nature and quantity scores). Changes in scar base depth before and after treatment were evaluated by confocal laser scanning microscope. Photos were saved before and after intervention, the observation points were marked, and the mean value was taken after 3 records. Additionally, the skin pore value and texture value were measured by skin detector to evaluate the skin condition of patients; the smaller the score, the better the skin condition. We also used a skin moisture tester to test the skin barrier function of both groups before and after treatment, including skin water content, epidermal oil content and transepidermal water loss (TEWL). Finally, the duration of redness, scabbing and erythema after treatment and the incidence of adverse reactions (redness, scab, acneiform rash, and pigmentation) after treatment were counted.
Statistical Methods
Statistical analyses of data were made by SPSS23.0. Quantitative data, represented by ( ), were analyzed by the independent sample t-test between groups and the paired t-test before and after treatment. The inter-group difference of categorical data expressed by [n(%)] was identified by the chi-square test. The statistical significance level was set to P<0. 05.
), were analyzed by the independent sample t-test between groups and the paired t-test before and after treatment. The inter-group difference of categorical data expressed by [n(%)] was identified by the chi-square test. The statistical significance level was set to P<0. 05.
Results
Comparison of Clinical Data
We first compared patients’ clinical baseline data to ensure the reliability of the experimental results. No statistical difference was found in age, sex and course of disease between RG and CG (P>0.05), indicating comparability. Table 1
 |
Table 1 Table of Clinical Baseline Information |
Comparison of Clinical Efficacy
The ORR was found to be 93.33% in RG after treatment, higher compared with CG (P<0.05), suggesting better clinical efficacy of bFGF combined with ultrapulsed fractional laser for acne scars. Table 2
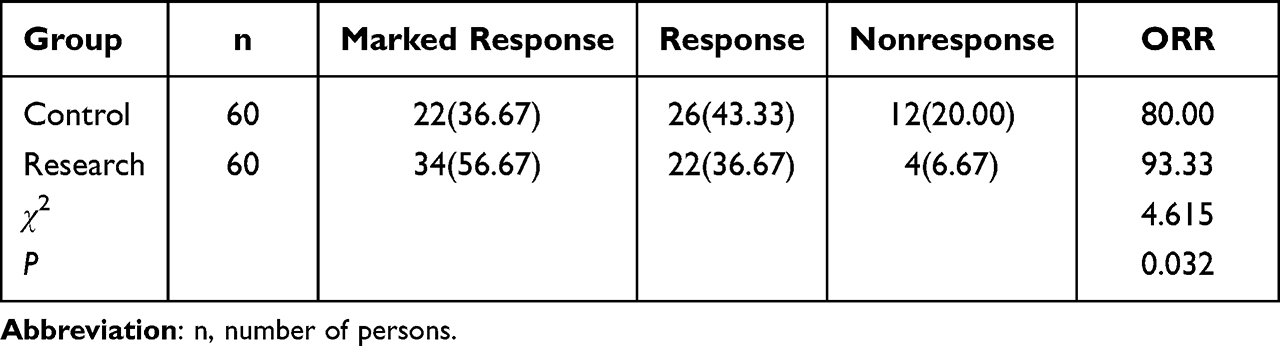 |
Table 2 Comparison of Clinical Efficacy |
Comparison of ECCA Score and Scar Base Depth Before and After Treatment
RG and CG did not differ much in pre-treatment ECCA score and scar base depth (P>0.05). The post-treatment ECCA score and scar base depth in RG decreased to (24.90±4.14) and (93.58±12.49) μm, respectively, both of which were lower compared with CG (P<0.05). Figure 1
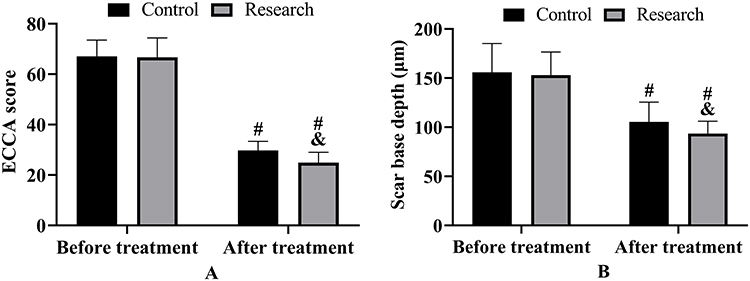 |
Figure 1 Comparison of ECCA score and scar base depth (there were 60 cases in each of research and control groups). (A) ECCA score before and after treatment. (B) Scar base depth before and after treatment. #: vs before treatment, P<0.05. &: vs control group, P<0.05. |
Comparison of Pre- and Post-Treatment Skin Condition
The pore and texture values of the skin were measured by a skin detector before and after treatment. Reductions in skin pore and texture values were observed in both cohorts two after treatment (P<0.05); the post-treatment pore value and texture value in RG were (60.87±6.26) and (49.93±6.31), respectively, both lower versus CG (P<0.05). Figure 2
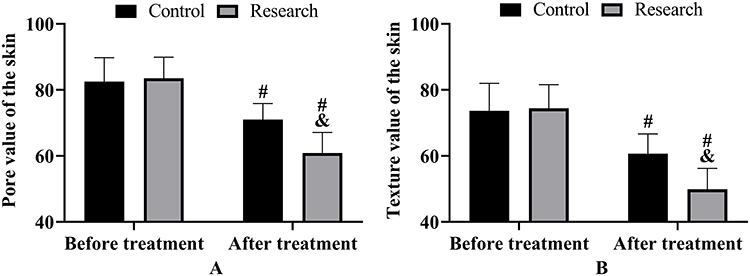 |
Figure 2 Comparison of skin condition. (A) The pore value of the skin before and after treatment (there were 60 cases in each of research and control groups). (B) The texture value of the skin before and after treatment. #: vs before treatment, P<0.05. &: vs control group, P<0.05. |
Comparison of Recovery Time
Statistics showed that the duration of redness, scabbing, and erythema was further shortened in RG versus CG (P<0.01), indicating that bFGF + ultrapulsed fractional CO2 laser therapy can facilitate the recovery of patients after treatment. Figure 3
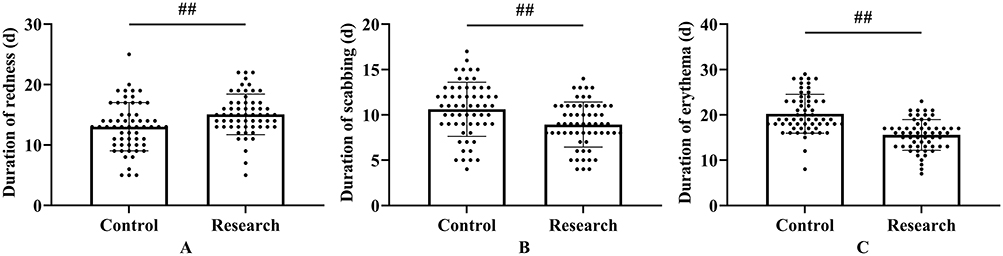 |
Figure 3 Comparison of recovery time (there were 60 cases in each of research and control groups). (A) Comparison of duration of redness. (B) Comparison of scabbing. (C) Comparison of erythema. ##P<0.01. |
Comparison of Pre- and Post-Treatment Skin Barrier Function
An increased skin water and epidermal oil content was identified in both groups after treatment, with an even higher value in RG; while the TEWL decreased, and the reduction was more significant in RG versus CG (P<0.05). Figure 4
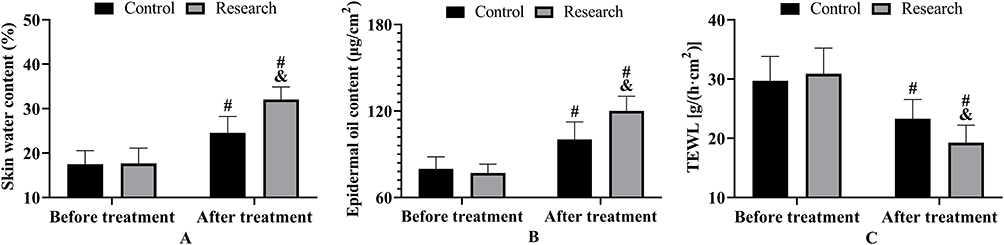 |
Figure 4 Comparison of skin barrier function (there were 60 cases in each of research and control groups). (A) Skin water content before and after treatment. (B) Epidermal oil content before and after treatment. (C) TEWL before and after treatment. #: vs before treatment, P<0.05. &: vs control group, P<0.05. |
Incidence of Adverse Reactions in Two Groups
Finally, the incidence of adverse reactions such as persistent erythema, dilated capillaries and pigmentation was calculated to be 10.00% in RG, which was markedly reduced compared with CG (P<0.05). Table 3
 |
Table 3 Incidence of Adverse Reactions |
Discussion
Acne scars are concave scarring formed by the destruction of hair follicles and surrounding dermal tissue by inflammatory responses, infections, or improper treatment during acne development, leading to the loss of dermal fibrous tissue, collagen, or elastin and the resulting inability to complete dermal tissue filling.13 In this study, we conducted a preliminary observation on the treatment of acne scars by bFGF + ultrapulsed fractional CO2 laser therapy. Compared with CG, the clinical efficacy was found to be evidently higher in RG, and the post-treatment ECCA score, scar base depth, skin pore value and texture value were lower, which fully demonstrates that the combination of bFGF and ultrapulsed fractional CO2 laser had a better effect on acne scars. This is also consistent with the research results of Yan et al,14 which can support our view. bFGF has been shown to inhibit fibroblast proliferation and scar tissue fibrosis, improve skin and mucosal blood irrigation of the local defect tissue, and promote blood vessel regeneration, thus accelerating repair and stabilizing the scar area.15,16 Therefore, in the application of ultrapulsed fractional CO2 laser, bFGF can further improve its therapeutic effect on acne scars. Moreover, we found that bFGF can activate natural killer T lymphocytes, reduce phagocytosis on mature fibroblasts, and inhibit scarring.17 This can ensure the long-term effectiveness and stability of scar treatment and better patient outcomes and rehabilitation.
On the other hand, in the comparison of the treatment and recovery, it can also be seen that the duration of redness, scabbing and erythema was further shortened in RG, and the skin barrier function was better, demonstrating that the use of bFGF can not only improve treatment effects, but also provide reliable safety for patients. Studies have shown that bFGF can induce basal membrane cells in the dermis that have not yet been completely differentiated, activate their regeneration function, and reduce the proliferation of fibroblasts and the fibrosis process of scar tissues through contact inhibition.18,19 In addition, bFGF can improve the blood flow irrigation of skin and mucosa in local defects, increase the absorption rate of apoptotic and necrotic scar cells, and stabilize the scar area to avoid spread.20 Therefore, the combined use of bFGF promotes dermal collagen proliferation and cell regeneration, increases dermal moisture and improves skin texture, while enhancing blood circulation and reducing tissue edema, which is more conducive to speeding up skin regeneration and repair, shortening recovery time and better repair of depressed acne scars. The inter-group comparison of adverse reactions also identified a lower incidence in RG, which can also verify the above viewpoint, testifying the excellent application value of bFGF. However, compared with the previous research on CO2 fractional laser, the adverse reactions of both groups in this study were fewer. This may be due to the fact that ultrapulsed fractional CO2 laser treatment for acne scars generally adopts a precise scanning mode, which uses photothermal action to stimulate dermal fibroblasts in the damaged part, promote dermal fibroblasts and collagen remodeling, and more effectively avoid normal tissue damage, thus reducing the incidence of adverse reactions and contributing to better efficacy than traditional laser therapy.21,22
However, the limited number of cases included in this study may result in statistical calculation contingency. Second, as we all know, the rehabilitation of acne scars takes a long time, so we still need to follow up the research participants for a longer period of time to evaluate the therapeutic effect of bFGF + ultrapulsed fractional CO2 laser therapy. Finally, further basic experimental analysis on the mechanism of action of bFGF can be carried out in the follow-up studies, so as to provide more comprehensive clinical references.
Conclusively, the combination of bFGF and ultrapulsed fractional CO2 laser therapy for acne scars can not only improve treatment safety, shorten recovery time and reduce prevent adverse reactions, but also further enhance treatment efficacy and patients’ facial beauty, which is worthy of widespread use in clinical practice.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethical Approval
This case has got approval from the Ethics Committee of Dongying People’s Hospital.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Oge LK, Broussard A, Marshall MD. Acne vulgaris: diagnosis and treatment. Am Fam Physician. 2019;100(8):475–484.
2. Baldwin H, Tan J. Effects of diet on acne and its response to treatment. Am J Clin Dermatol. 2021;22(1):55–65. doi:10.1007/s40257-020-00542-y
3. Habeshian KA, Cohen BA. Current issues in the treatment of acne vulgaris. Pediatrics. 2020;145(Suppl 2):S225–S230. doi:10.1542/peds.2019-2056L
4. Mohsin N, Hernandez LE, Martin MR, Does AV, Nouri K. Acne treatment review and future perspectives. Dermatol Ther. 2022;35(9):e15719. doi:10.1111/dth.15719
5. Xu Y, Deng Y. Ablative fractional CO2 laser for facial atrophic acne scars. Facial Plast Surg. 2018;34(2):205–219. doi:10.1055/s-0037-1606096
6. Sadick NS, Cardona A. Laser treatment for facial acne scars: a review. J Cosmet Laser Ther. 2018;20(7–8):424–435. doi:10.1080/14764172.2018.1461230
7. Zhang DD, Zhao WY, Fang QQ, et al. The efficacy of fractional CO(2) laser in acne scar treatment: a meta-analysis. Dermatol Ther. 2021;34(1):e14539. doi:10.1111/dth.14539
8. Amiri R, Khalili M, Mohammadi S, Iranmanesh B, Aflatoonian M. Treatment protocols and efficacy of light and laser treatments in post-acne erythema. J Cosmet Dermatol. 2022;21(2):648–656. doi:10.1111/jocd.14729
9. Barbieri JS, Spaccarelli N, Margolis DJ, James WD. Approaches to limit systemic antibiotic use in acne: systemic alternatives, emerging topical therapies, dietary modification, and laser and light-based treatments. J Am Acad Dermatol. 2019;80(2):538–549. doi:10.1016/j.jaad.2018.09.055
10. Ai JJ, Zha WF, Guo B, Song WM. A randomized Guinea pig study on external cell growth factors after fractional ultrapulsed CO(2) laser therapy. J Cosmet Laser Ther. 2013;15(4):219–224. doi:10.3109/14764172.2012.758370
11. Cecerska-Heryc E, Goszka M, Serwin N, et al. Applications of the regenerative capacity of platelets in modern medicine. Cytokine Growth Factor Rev. 2022;64:84–94. doi:10.1016/j.cytogfr.2021.11.003
12. Kurokawa I, Nakase K. Recent advances in understanding and managing acne. F1000Res. 2020;9:792. doi:10.12688/f1000research.25588.1
13. Heng AHS, Chew FT. Systematic review of the epidemiology of acne vulgaris. Sci Rep. 2020;10(1):5754. doi:10.1038/s41598-020-62715-3
14. Yan L, Wu W, Wang Z, et al. Comparative study of the effects of recombinant human epidermal growth factor and basic fibroblast growth factor on corneal epithelial wound healing and neovascularization in vivo and in vitro. Ophthalmic Res. 2013;49(3):150–160. doi:10.1159/000343775
15. Wang X, Qu M, Li J, Danielson P, Yang L, Zhou Q. Induction of fibroblast senescence during mouse corneal wound healing. Invest Ophthalmol Vis Sci. 2019;60(10):3669–3679. doi:10.1167/iovs.19-26983
16. Elbialy ZI, Assar DH, Abdelnaby A, et al. Healing potential of Spirulina platensis for skin wounds by modulating bFGF, VEGF, TGF-ss1 and alpha-SMA genes expression targeting angiogenesis and scar tissue formation in the rat model. Biomed Pharmacother. 2021;137:111349. doi:10.21037/apm-22-70
17. Zhang X, Li NL, Guo C, et al. A vaccine targeting basic fibroblast growth factor elicits a protective immune response against murine melanoma. Cancer Biol Ther. 2018;19(6):518–524. doi:10.1080/15384047.2018.1435223
18. Xie C, Shen X, Xu X, et al. Astrocytic YAP promotes the formation of glia scars and neural regeneration after spinal cord injury. J Neurosci. 2020;40(13):2644–2662. doi:10.1523/JNEUROSCI.2229-19.2020
19. Suzuki R, Kawai Y, Tsuji T, et al. Prevention of vocal fold scarring by local application of basic fibroblast growth factor in a rat vocal fold injury model. Laryngoscope. 2017;127(2):E67–E74. doi:10.1002/lary.26138
20. Tateya I, Tateya T, Sohn JH, Bless DM. Histological effect of basic fibroblast growth factor on chronic vocal fold scarring in a rat model. Clin Exp Otorhinolaryngol. 2016;9(1):56–61. doi:10.21053/ceo.2016.9.1.56
21. Galal O, Tawfik AA, Abdalla N, Soliman M. Fractional CO2 laser versus combined platelet-rich plasma and fractional CO2 laser in treatment of acne scars: image analysis system evaluation. J Cosmet Dermatol. 2019;18(6):1665–1671. doi:10.1111/jocd.12909
22. Lin L, Liao G, Chen J, Chen X. A systematic review and meta-analysis on the effects of the ultra-pulse CO2 fractional laser in the treatment of depressed acne scars. Ann Palliat Med. 2022;11(2):743–755.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.